abstract id: iria - 1052. introduction among the widely used neuro imaging techniques ie computed...
TRANSCRIPT

Ring Enhancing Lesions Of The Brain.
Abstract Id: IRIA - 1052

IntroductionAmong the widely used neuro imaging
techniques ie computed topography and MRI, numerous etiologies may present as ring enhancing lesions. On non contrast images these lesions usually appear as hypodense or isodense. However on post contrast, there is a homogeneous disk like enhancement within the region of hypodensity and is usually associated vasogenic oedema.

CausesBACTERIAL- - Pyogenic abscess - Tuberculoma - Syphilis - Listeriosis
Contd..
Ring enhancement
Pyogenic Abscess

PARASITIC- - Neurocysticercosis - Toxoplasmosis - Amoebic brain abscess - Echinococcus - Cerebral sparganosis
Contd..
Neurocysticercosis

NEOPLASTIC - Metastasis - Primary brain tumour - Primary CNS lymphoma
Contd..
Metastasis

FUNGAL- - Cryptococcosis - Actinomycosis - Aspergillosis - Histoplasmosis - Nocardiosis - Zygomycosis
INFLAMMATORY AND DEMYELINATING - Multiple sclerosis - Acute disseminated encephalomyelitis - Sarcoidosis - Neuro Behects disease - Systemic lupus erythematosus
Radiographic featuresEnhancing wall characteristics - Thick and nodular is in favour of neoplasm - Thin and smooth favours abscess - Incomplete ring opened towards cortex
favours demyelination - Intermediate to low T2 signal capsule
favours abscess - Restricted diffusion of enhancing wall
favours GBM or demyelination.Contd..

Surrounding oedema - Extensive oedema relative to lesion size favours abscess - Increased perfusion favours neoplasmCentral fluid/ content - Restricted diffusion favours abscessNumber of lesions - Similar sized rounded lesions at grey white matter
favours metastasis/ abscess - Irregular mass with adjacent secondary lesions
embedded in the region of oedema favours GBM - Small (< 1-2 cm) lesions with thin walls and calcifications
are in favour of neurocysticercosis

Neoplasm The imaging features of both primary and metastatic tumors usually
manifest as rounded, well-circumscribed, ring enhancing lesions of variable sizes surrounded by a variable amount of vasogenic oedema. MRI reveals mild T1 hypointensity with T2 hyperintensity and fluid-attenuated inversion recovery hyperintensity at the site of lesion.
T1W T1W- ContrastT2W FLAIRT2W

Pyogenic abscessThe lesions are commonly located at the gray-white matter
junction. Non contrast MRI shows an isointense to slightly hyperintense capsule on T1 weighted images, and is hypointense on T2 weighted images. The ring enhancement on post-contrast images is usually thin and smooth and often thinner along the medial margin.
T1W T2W T2W FLAIR T1W- Contrast
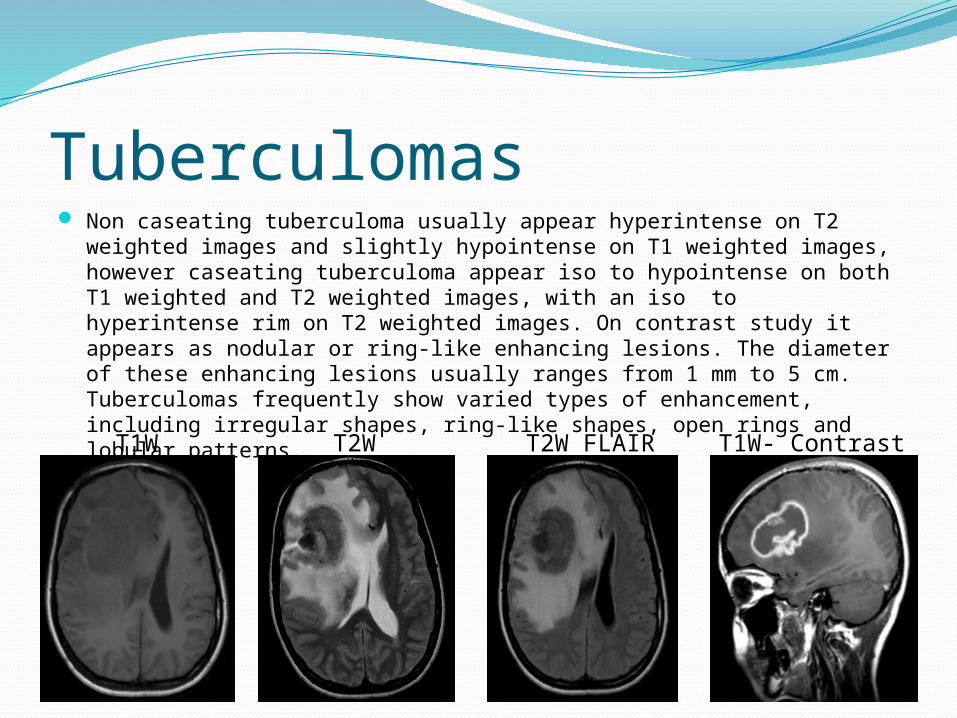
Tuberculomas Non caseating tuberculoma usually appear hyperintense on T2 weighted
images and slightly hypointense on T1 weighted images, however caseating tuberculoma appear iso to hypointense on both T1 weighted and T2 weighted images, with an iso to hyperintense rim on T2 weighted images. On contrast study it appears as nodular or ring-like enhancing lesions. The diameter of these enhancing lesions usually ranges from 1 mm to 5 cm. Tuberculomas frequently show varied types of enhancement, including irregular shapes, ring-like shapes, open rings and lobular patterns.
T1W T2W T2W FLAIR T1W- Contrast

Neurocysticercosis On MRI, the wall of the cysticercus granuloma (a colloid cyst stage)
becomes thick and hypointense and there is marked perilesional edema on T2 weighted images. Cysticercus granuloma shows a ring pattern of enhancement after contrast medium administration. Usually, the lesions are <20 mm in diameter. Calcified eccentric scolex is also often seen. The lesions are often multiple and most often do not have peri lesional oedema.
T1W T2W T2W FLAIR T1W- Contrast

Subacute Infarct T1W T2W
T2W FLAIR T1W- CONTRAST
DWI ADC

Demyelinating disorders Multiple enhancing ring lesions may be encountered. Enhancing
demyelinating lesions differ in size, shape or pattern, most demonstrating a nodular pattern whereas some demonstrate a ring enhancing pattern while few have other patterns. Presence of an open ring or incomplete ring lesion is also characteristic in differentiating demyelinating lesions from large brain tumors or infective lesions like brain abscess.
T1W T2W T2W FLAIR T2W- Contrast

Glioblastoma multiforme Glioblastoma multiforme usually appear as hypo to isointense mass within
white matter with a central heterogenous signal on T1 weighted images. On contrast its enhancement is variable showing a peripheral and irregular pattern with nodular components. On T2 / FLAIR it appears hyperintense surrounded by vasogenic oedema with occasional flow voids. There is a low intensity rim from blood product which is incomplete and irregular in 85% when present and is mostly located inside the peripheral enhancing component. There is no diffusion restriction, however, lower measured ADC than low grade gliomasT1W T2W T2W FLAIR T1W- Contrast

CNS Lymphoma It is typically hypointense to white matter on T1 weighted images.
On contrast study it shows strong homogenous enhancement for high grade tumours while low grade tumours have absent to moderate enhancement. T2 weighted images show iso to hypo intensity. Isointense 33%, hypointense 20% and hyperintense 15-47% which are more common in tumours with necrosis. DWI shows typical restricted diffusion.
T1W T2W T2W FLAIR DWI T1W- Contrast

ConclusionRing enhancing lesions caused by common
non-neoplastic and neoplastic disorders remain a diagnostic challenge inspite of clinical evaluation and a battery of tests. In a majority of such cases, biopsy of the lesion(s) remain the only option to establish a confirmative diagnosis.

References Schwartz KM, Erickson BJ, Lucchinetti C. Pattern of T2 hypointensity associated
with ring-enhancing brain lesions can help to differentiate pathology. Neuroradiology 2006;48:143-9.
Murphy FM, Rees JH, Schroeder JW. Patterns of contrast enhancement in the brain and meninges. Radiographics 2007;27:525-51.
Cortese I, Nath A. Case 11: a young woman with ring-enhancing brain lesions. Med Gen Med 2006;8:3.
Yamamoto M, Kawauchi T, Sakata I, Iwasaki Y, et al. Does supplementation of contrast MR imaging with thallium-201 brain SPECT improves differentiation between benign and malignant ring-like contrast-enhanced cerebral lesions? 2007;21:251-6.
Wasay M, Kheleani BA, Pui M, Hasan S, et al. Brain CT and MRI findings in 100 consecutive patients with intracranial tuberculoma. J Neuroimaging 2003;13:240-7.
Krabbe K, Gideon P, Wagn P, Thomsen C, Madsen F. MR diffusion imaging of human intracranial tumours. Neuroradiology 1997;39:483-9.
Parihar A, Nath K, Jaiswal S, Prasad KN, Husain N, et al. Comparative evaluation of fungal, tubercular, and pyogenic brain abscesses with conventional and diffusion MR imaging and proton MR spectroscopy. AJNR Am J Neuroradiol 2007;28:1332-8.

Thank You