abstract of the thesis entitled an evidence-based energy … ping yan.pdf · for the degree of...
TRANSCRIPT
1
Abstract of the thesis entitled
An evidence-based energy-protein dietary program to improve the nutritional
status among TB patients
Submitted by
CHOW Ping Yan
For the degree of Master of Nursing
At the University of Hong Kong
In August 2015
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium
Tuberculosis. It typically affects the pulmonary system (pTB). The disease is spread in
the air when people who are sick with pulmonary TB expel bacteria, for example by
coughing. In Hong Kong, TB is the second high infectious disease; about 4800 people
got infected every year. Tuberculosis and nutrition is under a bidirectional relationship.
Under-nutrition increases the risk of TB and in turn TB can lead to malnutrition.
Nutritional state of TB patient is usually weakened during infection period; however,
there is currently no an evidence-based dietary program available to them.
This dissertation aims to assemble relevant research studies on the effectiveness
of energy-protein dietary program for improving the nutritional status and accelerate
the sputum sterilization in TB patients; to appraise, summarize and synthesize the
finding extracted from the selected studies; to formulate and evidence-based energy-
protein dietary program for improving the nutritional status and accelerate the sputum

2
sterilization in TB patients; to assess the implementation potential of the proposed
innovation in designed clinical setting and to develop and evaluation plan for the
proposed program.
Four electronic bibliographical databases including PubMed, British Nursing
Index, PsyInfo and CINAHL, and one searching engine: Google Scholar, were used to
identify studies that examined the effectiveness of dietary program and interventions
for TB patients. 96 relevant articles were searched. Six of those studies met the selection
criteria and were critically appraised using the methodology checklist designed by
Scottish Intercollegiate Guidelines Network (SIGN). After summarizing and
synthesizing the data, five dietary interventions with 1++ to 1+ level of evidence were
concluded as the most effective strategies for eradicating the clinical issue.
Following assessment of the implementation potential of the proposed innovation
in designated clinical setting in terms of transferability, feasibility and cost-benefit ratio,
an evidence-based energy-protein dietary program was developed. In order to facilitate
the change of practice and determine the effectiveness of the program, comprehensive
plans of communication with various stakeholders, pilot study and evaluation were also
subsequently established.
With this evidence-based program, the nutritional status and the rate of the sputum
sterilization of TB patients are believed to be enhanced.

3
An evidence –based energy-protein dietary program to improve the
nutritional status among TB patients
By
CHOW Ping Yan
BN, RN
A thesis submitted in partial fulfillment of the requirements for the
Degree of Master of Nursing at The University of Hong Kong
July 2015

4
Declaration
I declare that this thesis represents my own work, except where due acknowledgement
is made, and that it has been previously included in a thesis, dissertation or report
submitted to this University or to any other institution for a degree, diploma or other
qualifications.
A thesis submitted in partial fulfilment of the requirement for the Degree of Master of
Nursing at the University of Hong Kong
August, 2015

5
Acknowledgement
I would like to express sincere gratitude to my supervisor, Professor Felix Yuen,
for his guidance and enlightenment. I also deeply thank Dr. Daniel Fong and Dr. Patsy
Chau for giving tutorials of this dissertation. Without their insightful comments and
encouragement, this dissertation could not be completed.
Ultimately, I would like to give my heartfelt thanks to my parents, ward manager,
colleagues and friends, especially Shereen, for their understanding and generous
support throughout my studies.
…………………………………………..
CHOW Ping Yan
August, 2015

6
Contents
Declaration P. 4
Acknowledgement P. 5
Table of contents P. 6
List of appendices P. 12
CHAPTER 1: INTRODUCTION P. 14
1.1 BACKGROUND P. 15
1.1.1 Tuberculosis P. 15
1.1.2 Nutrition P. 16
1.1.3 Tuberculosis and Nutrition P. 16
1.2 AFFIRMING THE NEEDS P. 18
1.2.1 Local Setting P. 18
1.2.2 Current management for TB patients P. 19
1.2.3 Problem of the current practice P. 19
1.2.4 Potential Innovation P. 20
1.3 SIGNIFICANT OF THE STUDY P. 22
1.3.1 Patients’ view P. 22
1.3.2 Nurses’ view P. 22

7
1.3.3 Hospitals’ view P. 23
1.4 RESEARCH QUESTION P. 23
1.5 OBJECTIVES OF THE PROPOSAL P. 24
1.6 CONSLUSION P. 24
CHAPTER TWO: CRITICAL APPRAISAL P. 25
2.1 SEARCH & SEARCH STRATEGIES P. 25
2.1.1 Electronic Databases, Search Keywords P. 25
2.1.2 Inclusion/exclusion criteria P. 26
2.1.3 Data extraction P. 27
2.1.4 Appraisal strategies P. 27
2.2 RESULTS P. 28
2.2.1 Describe search history P. 28
2.2.2 Summary of study characteristics P. 28
2.2.3 Summary of Quality assessment and methodological issue P. 28
2.3 SUMMARY OF THE DATA p. 31
2.3.1 Patient Characteristics P. 32
2.3.2 Sample Size P. 32
2.3.3 Intervention P. 32

8
2.3.4 Comparison P. 33
2.3.5 Length of follow-up P. 34
2.3.6 Outcome measures P. 34
2.3.7 Results P. 35
2.4 SYNTHSIS OF THE DATA P. 36
2.4.1 Subjects P. 36
2.4.2 Assessment of nutritional status and counseling P. 36
2.4.3 Earlier initiation of nutrition support: High energy-protein
supplementation
P. 37
2.4.4 Outcomes measures P. 38
2.4.5 Closer outcomes monitoring P. 38
2.5 CONCLUSION P. 38
CHAPTER 3: RANSLATION AND APPLICATION P. 40
3.1 IMPLEMENTATION POTENTIAL P. 40
3.1.1 Target setting P. 40
3.1.2 Target audience P. 40
3.1.3 Transferability of the findings P. 41
3.1.4 Feasibility P. 42

9
3.1.5 Cost-benefit Ratio P. 46
3.2 EVIDENCE-BASED ENERGY-PROTEIN DIETARY PROGRAM TO
IMPROVE THE NUTITIONAL STATUS AMONG TB PATIENTS
P. 49
3.2.1 Background P. 49
3.2.2 Objectives P. 49
3.3.3 Target users P. 50
3.3.4 Target patient population P. 50
3.3.5 Rating Scheme for the Strength of the recommendation P. 50
3.3.6 Recommendations P. 50
CHAPTER 4: IMPLEMENTATION PLAN P. 55
4.1 COMMUNICATION PLAN P. 55
4.1.1 Hospital management P. 55
4.1.2 Frontline nursing staff P. 56
4.1.3 Respiratory specialists P. 57
4.1.4 Dietitians P. 57
4.1.5 Clerical staff P. 57
4.1.6 Patients and their caregivers P. 58
4.2 PILOT STUDY P. 58

10
4.2.1 Objectives P. 58
4.2.2 Target setting and target audience P. 59
4.2.3 Study design P. 59
4.2.4 Ethical consideration P. 59
4.2.5 Evaluation of the pilot study P. 60
4.3 CONCLUSION P. 61
CHAPTER 5: EVALUATION PLAN P. 62
5.1 OUTCOME MEASURES P. 62
5.1.1 Patient outcome P. 62
5.1.2 Healthcare provider outcome P. 63
5.1.3 System outcome P. 63
5.2 NATURE AND NUMBER OF INVOLVED CLIENTS P. 63
5.3 DATA COLLECTIO AND ANALYSIS P. 64
5.3.1 Patient outcome P. 64
5.3.2 Healthcare provider outcome P. 64
5.3.3 System outcome P. 65
5.4 CRITERIA FOR THE EFFECTIVE CHANGES P. 65
5.5 CONCLUSION P. 66

11
CHAPTER 6: CONCLUSION P. 67
CHAPTER 7: REFERENCES P. 68

12
List of appendices
Appendix A Search Strategies and Search History P. 76
Appendix B PRISMA 2009 Flow Diagram P. 77
Appendix C Tables of Evidence P. 78
Appendix D Critical Appraisals P. 84
Appendix E Level of evidence hierarchy developed by the SIGN P. 96
Appendix F Assessment form of Target TB Patient P. 97
Appendix G The content of the program briefing session P. 99
Appendix H Tables of the Costs P. 100
Appendix I Table of the operation cost of the two programs: briefing
sessions
P. 102
Appendix J SIGN 50: A guideline developer’s handbook P. 103
Appendix K Nursing Procedure Audit Form for Evidence-based
energy-protein dietary program
P. 104
Appendix L Nurse Satisfaction Survey for Evidence-based energy-
protein dietary program Questionnaire
P. 105
Appendix M Patient Satisfaction Survey for Evidence-based energy-
protein dietary program Questionnaire
P. 107

13
Appendix N Timeframe for the implementation of Evidence-based
energy-protein program
P. 108

14
CHAPTER 1: INTRODUCTION
Tuberculosis (TB) is the major worldwide infectious disease. Under-nutrition is
highly prevalent among TB patients with the relationship between TB and nutrition has
long been recognized: TB causes weight loss and in turn being underweight acts as the
risk factor for developing active TB (Semba, Darnton-Hill & Pee, 2010; Gupta, Gupta,
Atreja, Verma & Vishvkarma, 2009; Cegielski & McMurray, 2004). World Health
Organization (WHO) (2014) indicated that under nutrition at the time of diagnosis of
active TB is a predictor of increased risk of death and TB relapse. Therefore, nutritional
care and support has played a prominent role in the prevention and treatment of TB. It
should be involved in the regular TB treatment.

15
1.1 BACKGROUND
1.1.1. Tuberculosis
Tuberculosis is the worldwide leading bacterial cause of death (Semba et al, 2010;
Young, Gideon & Wilkinson, 2009). It is caused by Mycobacterium Tuberculosis which
could further progress to an active respiratory disease. Its transmission route is from
person-to-person through the air. TB is a contagious disease related to poverty, under-
nutrition and poor immune function (WHO, 2014). Today, tuberculosis is still an
alarming global health issue. Approximately 8.6 million people have developed TB and
1.3 million TB patients passed away from the disease in 2012, the great number of TB
deaths is unacceptable as most are possibly preventable (WHO, 2013). According to
WHO Global Tuberculosis Report 2013, 6.1 million cases of TB were notified in 2012;
at the same year, the number of new TB cases occurred in Asia, accounting for 60% of
new cases around the world.
In Hong Kong, according to the statistics data from Centre for Health Protection in
2013, the total notified cases were 4773 while the notification rate was 66.41 per
100,000 population. Compared with other developed countries, such as US (3.0 per
100,000 population in 2013), UK (13.9 per 100,000 population in 2012) and Singapore
(40 per population in 2012), the notification rate of TB in Hong Kong is much higher
than them. Especially, among the aged above 65, the range of the notification rate was

16
from 110.43 to 309.13 per 100,000 population, which represents tuberculosis mostly
attacks the elder adults.
1.1.2. Nutrition
Nutrients are necessary to regulate body processes, tissue building and repairing,
thereby promote health and prevent diseases (WHO, 2013). Therefore, nutritional status
has greatly drawn an attention as it strongly influences the health and functioning of all
body systems, especially the immunity towards various infectious diseases.
Malnutrition is a general term of being under-nutrition or over-nutrition. Under-
nutrition is defined as a state when nutritional status of a person is suboptimal, which
can be in form of wasting and stunting (Semba et al, 2010). WHO (1999) has
reported under-nutrition is commonly associated with illness and infections such as TB,
pneumonia, and HIV.
1.1.3. Tuberculosis and Nutrition
As a matter of fact, the relationship between tuberculosis and nutrition is
bidirectional. The cell-mediated immunity (CMI) is the principle host defense against
TB, and is found to be impaired by malnutrition (Chandra, 1991; McMurray & Bartow,
1992).
On the flip side, due to the inflammatory state, tissue catabolism and the symptom
of poor appetite, the TB infection drives the nutritional status even worse and possibly

17
develops into active respiratory disease. Numerous studies revealed that nutritional
status is further affected and significantly poorer by active pulmonary tuberculosis
(Karyadi et al, 2000; Cegielski & McMurray, 2004; Dodor, 2008; Gupta et al, 2009;
Piva, Costa, Barreto & Pereira, 2013). As a result, a negative energy balance, nutrients
mal-absorption and changed metabolism leading to wasting are shown during the
infection period (Macallan et al, 1998; Paton, 2004; Dodor, 2008; Semba et al, 2010;
Mupere et al, 2014).
Wasting is one of typical symptoms of TB infection; and indicators of poor
nutrition status. Low body mass index (BMI) (< 18.5 kg/m2) and inadequate weight
gain with TB treatment are associated with TB relapse and delayed recovery (Ralph et
al, 2013; Khan, Sterling, Reves, Vernon & Horsburgh, 2006; Krapp, Véliz, Cornejo,
Gotuzzo & Seas, 2008; Shetty, Shemko, Vaz & D'Souza, 2006; Gupta et al,2009) and
an increased risk of death and adverse treatment outcome (Van Lettow et al, 2004;
Lönnroth, Williams, Cegielski & Dye, 2010; Hanrahan et al, 2010).

18
1.2 AFFIRMING THE NEEDS
1.2.1. Local Setting
The proposed innovation would be implemented in an adult isolation unit. The
target population is for the newly diagnosed TB patients. Those patients are generally
admitted from Accident & Emergency department; very few cases are transferred from
the respiratory units of other hospitals. The TB patients would be placed in a negative
pressure room to reduce the transmission of disease via air-borne route. TB patients are
not allowed to leave the isolation room and no visiting hour provided to their relatives
and friends. Private diets can be brought by the relatives to patients, however, a face to
face contact is never allowed in the isolation unit. Thanks to the restriction of isolation
policy, some patients might mainly consume the meals prepared by the kitchen of the
hospital.
Those TB patients commonly have a history of Chronic Obstructive Pulmonary
Disease (COPD) and a past or current smoking habit. Patients are not just Chinese, but
also other South-Asian people, such as Indians and Pakistani. Male TB patients are
dominated. Estimated above 50% of TB patients are aged above 40. Around 70% of
total TB patients are underweighted (BMI <18.5 kg/m2); they mainly live alone or in
residential care homes.
19
1.2.2. Current management for TB patients
For the newly diagnosed TB patients, they would be processed an ophthalmic
assessment, height and weight measurement for providing a baseline information for
dosage adjustment of TB medication. After that, they would be prescribed a
combination of antibiotics including isoniazid, rifampicin, pyrazinamide, ethambutol
and pyridoxine and notified as confirmed TB to Department of Health under the
Prevention and Control of Disease Ordinance.
Meanwhile, nurse would give a personal education about tuberculosis, treatment
and nutrition advice to all those TB patients. Usually, for those underweighted patients
(BMI<18.5 kg/m2), they would be encouraged for oral intake. Their meals size would
be enlarged or extra one glass of milk would be provided to them during tea-time. If the
patient’s BMI is too low, dietitian would be consulted for further nutritional
management.
1.2.3. Problem of the current practice
As mentioned, TB could cause under-nutrition because of loss of appetite and
increased utilization of energy and nutrition (Macallan, 1999; Macallan et al, 1995),
however, the current practice only targets on the underweighted patients and acts as an
acute intervention. The prevention of under-nutrition is as the same important in TB
treatment. Previous studies have demonstrated the newly diagnosed adult TB patients

20
were malnourished after starting TB treatment (Zachariah, Spielmann, Harries &
Salaniponi, 2002; Miller et al, 2000; Metcalfe, 2004).
There is no official protocols and guidelines of nutritional support developed for
TB patients, despite the evidence support of nutrition being an main factor in the
prophylaxis and treatment of TB. The management of patients’ nutritional problem is
various; it really depends on nurses’ clinical experience and preference.
Besides, after the baseline weight measurement, there is also no follow up of
monitoring patient’s nutritional status. Without the follow up, the nutrition status of
patients during receiving TB treatment is unknown. It is difficult to provide further
nutritional intervention to patient to recover and resume patients’ maximum health.
1.2.4. Potential Innovation
Historically, tuberculosis was recognized as a ‘consumption’ disease. The patients
on TB treatment were found their basal metabolic rate was 14% higher than the patients
with generally pulmonary diseases (Raj, D’Souza, Elia & Kurpad; 2006). Hence,
macronutrients, such as carbohydrate, protein and fat, are largely consumed during
infection. Hood (2013) reviewed the energy-protein malnutrition is one of the
prominent cause to the disease progression of TB in the domains severity, immune
function and medication efficacy. Daily energy requirement of a person varies
according to the individual’s sex, age, weight, height and health status, generally for at

21
least 2000 kcal/day for adults (Department of health, 2011). It is recommended TB
patients should consume approximately 15–30% of energy as protein, 25–35% as fat
and 45–65% as carbohydrate (Institute of Medicine, 2005). Studies pointed that
subjects who receive high energy-protein food supplements during TB treatment tend
to gain more weight; have an improvement on treatment completion and recovery and
significantly enhance the physical functioning and quality of life (Jahnavi & Sudha,
2010; Paton et al, 2014; Martins, Morris & Kelly, 2009; Sudarsanam et al, 2011; Hood,
2013).
22
1.3 SIGNIFICANT OF THE STUDY
1.3.1. Patients’ view
By providing the nutrition supports to the TB patients it could lead to immunologic
changes and further enhance the clearance of mycobacteria and alleviate infectiousness
of patient (Paton et al, 2004). Ultimately, it improves the health outcomes for the
tuberculosis patient. Weight loss or failure to gain weight during TB treatment would
contribute to other problems, like resistance to TB drugs and poor adherence (WHO,
2014). When the recovery is not delayed because of the nutritional problem, the
hospitalization period of patients might be shortened and the quality of life, hence,
might be improved. The rate of TB relapse might also be decreased. Jahnavi & Sudha
(2010) found that the patient who received food supplements had a significant increase
in body gain and physical function; improvements also can be observed in
psychological, physiological and social areas
1.3.2. Nurses’ view
In order to implement a holistic care to patients, nurses should pay an attention to
patients’ nutrition status, especially those with tuberculosis. With the restoration of
nutrition, their recovery and quality of life would be enhanced; the workload and stress
brought to nursing staff could be alleviated.

23
1.3.3. Hospitals’ view
Patient with tuberculosis is needed to be isolated in a negative pressure room with
air-borne precaution. Their hospitalization period is relative longer than those patients
with general medical problems. If the hospitalization of TB patients is shortened, the
health care and operation cost would be reduced.
1.4 RESEARCH QUESTION
Based on the affirming needs of current practice and concerned issue, the research
question is made; and the proposed innovation is formulated by applying the PICO
framework: "How effective is an energy-protein dietary program would be proposed to
improve the nutritional status among TB patients"; and
Patient – Tuberculosis patients
Intervention –Energy-protein dietary program
Comparison – Without the energy-protein dietary program
Outcomes – 1. Improving the nutritional status
2. Accelerate the sputum sterilization

24
1.5 OBJECTIVES OF THE PROPOSAL
The objectives of this evidence-based proposal are developed as below:
1. To assemble relevant research studies on the effectiveness of energy-protein dietary
program for improving the nutritional status and accelerate the sputum sterilization
in tuberculosis patients
2. To appraise, summarize and synthesize the findings extracted from the selected
studies.
3. To formulate an evidence-based energy-protein dietary program for improving the
nutritional status and accelerating the sputum sterilization in tuberculosis patients.
4 To assess the implementation potential of the proposed innovation in designated
clinical setting.
5 To develop an evaluation plan for the proposed program.
1.6 CONSLUSION
The purpose of the evidence-based dietary protocol is to help improve health
outcomes for people with TB through improved nutritional care and support. A
systematic and integrative review of literatures would be conducted to achieve the goal.

25
CHAPTER TWO: CRITICAL APPRAISAL
After identifying the affirming needs and significance, an evidence-based
nutritional supplement program will be developed through the process of gathering the
relevant research studies, summarizing and analyzing the identified data. The search
strategies, results, summary and synthesis of the extracted studies are described in this
chapter.
2.1 SEARCH & SEARCH STRATEGIES
2.1.1 Electronic Databases, Search Keywords
A systemic and thorough literature search about improving the nutritional status
and dietary in tuberculosis patients was conducted within the period of April 2014 to
August 2014 by utilizing four electronic bibliographical databases (PubMed, British
Nursing Index, PsycInfo and CINAHL) and one searching engine (Google Scholar).
Those were available in accessing in the Yu Chun Keung Medical Library of The
University of Hong Kong and Electronic Knowledge Gate (eKG) of the Hospital
Authority.
The keywords: 1. pulmonary tuberculosis, 2. mycobacterium tuberculosis, 3. diet,
4. dietary, 5. nutrition, 6. Energy-protein nutritional supplement, 7. under-nutrition, 8.
Wasting, 9. body mass index, 10. physical function and 11. body composition, were
searched respectively. Afterwards, the keywords were divided into three categories: 1,

26
2 and 3, 4, 5, 6 and 7, 8, 9, 10, 11. The keywords within the same group would be
searched again by using the ‘OR’ function with the result of those three categories
further combined with the ‘and’ function to narrow down the scope. To identify more
relevant studies, research journals retrieved from related citation or reference list were
considered with the inclusion and exclusion criteria being used as the filters for the
literature search. Search strategies, search history and flow diagram were illustrated in
details in Appendix A and Appendix B. In order to maximize the potential research
articles, there were no restrictions set on the language and date of publications in this
literature review. The titles and abstracts of all potential journals were screened
discreetly and the most relevant journals were then selected to have further analysis.
2.1.2. Inclusion/exclusion criteria
The systematic search of the evidence included all types of study designs, for
instance, systemic review, meta-analyses, randomized controlled trials, quasi-
experimental trials and cohort studies, about energy-protein nutritional interventions
towards the tuberculosis patients. Interventions were either natural food product or oral
fluid. Study participants included both male and female, aged 18 years or above, newly
diagnosed active pulmonary tuberculosis and currently receiving anti-TB treatment.
Studies with participants having parental or enteral feeding and pregnant women
were excluded. Suffering diabetes mellitus and multi-drug resistance TB were also

27
eliminated as these could be the cofounders that affect the results.
2.1.3. Data extraction
Data were extracted from the selected relevant research studies and presented in
form of a table of evidence with reference to the table of intervention studies of the
Scottish Intercollegiate Guidelines Network (SIGN) (Scottish Intercollegiate
Guidelines Network, 2012). Patient characteristics, study intervention and comparison,
length of follow-up, outcome measures and effect size of each selected study was
reported. The details of the tables of evidence of studies were shown in Appendix C.
2.1.4 Appraisal strategies
The methodological qualities of the selected studies were appraised critically by
using the appraisal checklist of the Scottish Intercollegiate Guidelines Network (SIGN)
(Scottish Intercollegiate Guidelines Network, 2012).
The appraisal checklists of randomized controlled trials and cohort studies were
used for assessing the studies. Both checklists were composed of two parts: internal
validity and overall assessment of the study. Ten methodological aspects were assessed
for each study in the section of internal validity; they were regarding the research
hypothesis, randomization method, concealment method, blinding, outcome
measurement, drop-out rate and data analysis. The latter section indicated how well the
study has done in minimizing bias or confounding by coding high quality (++),

28
acceptable (+) or unacceptable (0). The quality of the selected studies was rated from
2+ to 1++, and the details of each critical appraisal assessment were enclosed in
Appendix D. The guide for the level of evidence hierarchy developed by SIGN was in
Appendix E.
2.2 RESULTS
2.2.1. Describe search history
There were totally 96 relevant articles searched in English from the four electronic
databases and a searching engine. No study was retrieved in other languages. Through
manually screening topics, abstracts and the test contents, filtering according to the
mentioned inclusions and exclusion criteria, and eliminating the duplicated articles,
eventually there were 6 eligible studies assembled.
2.2.2. Summary of study characteristics
The six reviewed studies included five randomized control trials (RCTs) and one
cohort study. Those studies were conducted in India, Singapore, Mexico, Tanzania and
South Africa. 4 studies were funded by the universities and hospitals which had no role
in study design, data collection and analysis.
2.2.3. Summary of Quality assessment and methodological issue
For those selected 5 RCTs, they were at the level of evidence from high quality
(1++) to acceptable (1+). Only one of them was rated as 1++ (Martins et al, 2009),

29
whereas four of them were assessed to be 1+ (Jahnavi & Sudha, 2010; Paton et al, 2004;
Perez-Guzman et al, 2005; PrayGod et al, 2012). The cohort study was rated as 2+
(Rudolph et al, 2013). An appropriate and distinct focused question, study population,
intervention and outcomes were explicitly mentioned in all selected research studies.
Randomization controlled trials
For RCT, randomization is one of the prominent components for minimizing bias.
For those 5 studies, subjects have undergone the process of randomization before
allocating into either treatment or control group. Two studies addressed the details of
randomization procedure. Participants were allocated through a computer-generated
randomization sequence with varying Block size (Martins et al, 2009; PrayGod et al,
2012).
The remaining 3 studies only mentioned a brief (Jahnavi & Sudha, 2010; Paton et
al, 2004; Perez-Guzman et al, 2005). The randomizations of five studies have
demonstrated nearly 1:1 subject number for both treatment and control groups.
Regarding the concealment allocation, four trails have mentioned about recruiting
staff who were not directly involved in the studies to undertake the job of computer-
code generation and prepare the opaque and sealed envelopes. However, there was no
information about concealment method stated in Perez-Guzman et al (2005) study.
Keeping unawareness of the treatment implemented to subjects is recommended

30
in RCTs in order to minimize bias. Yet, it is not always feasible in every experimental
trial, especially for the dietary study. 4 RCTs mentioned no blinding performed in both
subjects and treatment providers. Only Perez-Guzman et al (2005) demonstrated double
blinding.
All trails reported the baseline background characteristics of the intervention and
control groups and they revealed insignificant discrepancies in both groups in relation
to gender, age, weight, BMI, income and smoking.
All studies have clearly illustrated the result measurement and the outcomes
variables were well defined. The indicators of result measurements were majorly in
anthropometry and sputum culture. A series of valid and reliable instruments and tools
were utilized: BMI measurement for the weight problem and Nicholas Manual muscle
Tester for measuring grip strength. Four trials (Jahnavi & Sudha, 2010; Paton et al,
2004; Martins et al, 2009; PrayGod et al, 2012) reported ranged 1.8%-19.1% drop out
rate before the studies were completed because of the death, poor compliance and cases
transferring to other clinics. Only two studies (Martins et al, 2009; PrayGod et al, 2012)
reported the sample size calculation using statistical power analysis with sufficient
power of 0.8.
A Cohort Study
The cohort study by Rudolph et al (2013) with the level of evidence of 2+ was to

31
assess the impact if a high prevalence of a fortified supplementary food in TB adult
patients. The research team took it as a pilot study. The outcome variable and the result
measurement method were clearly defined. The indicators were the clinical sign and
symptom of malnutrition, anthropometrical and biochemical measures. Owning to the
limited resource, its researcher team developed a longitudinal design without a placebo
controlled comparison group. Selection bias and Hawthorn effect may exist under this
design. Besides, as the given population is believed to have poor nutritional status, it
was deemed unethical to offer a placebo supplementary food (Rudolph et al, 2013).
Hence, only a single interventional group was designed, and the outcomes were
compared with the baseline data of subjects.
The drop out of that study was 6.9%, (Rudolph et al, 2013) reported the reasons
of dislike the invasive tests and the taste of ‘ePap’, inability to communicate with and
inform participants of data collection days and schedule conflicts with daytime data
collection.
2.3. SUMMARY OF THE DATA
These six studies were published from 2004-2013. 2 out of them were conducted
in hospital-based setting, while the remaining was in community clinic-based. Majority
studies were organized in Asian and African countries, there were Singapore, India,
South Africa and Tanzania, except one was in Mexico. Related to the difference of

32
culture and social-economic factors of the countries, there might be potential problems
of transferability and feasibility of implementing the dietary intervention to Chinese
population in Hong Kong.
2.3.1 Patient Characteristics
All subjects were the adult of both male and female with mean age ranged from
32.6-43.2 and newly diagnosis of pulmonary tuberculosis with anti-TB treatment, they
generally presented the typical signs and symptoms of TB. Four studies revealed
equilibrium proportion of genders, but the rest two were female dominance (Paton et
al, 2004; Perez-Guzman et al, 2005). Most subjects were wasting, with the
BMI<18kg/m2.
2.3.2. Sample Size
The sample size of six studies varied from 21-377 participants, and totally 891
confirmed TB patients got involved in those dietary research studies. Paton et al (2004)
and Perez-Guzman et al (2005) recruited relative small sample of 21 and 36 subjects.
The rest had got around at least 90 patients for their studies. Generalizability might be
the potential problem of the studies with small sample size.
2.3.3. Intervention
Among these six studies, the high energy-protein supplements were implemented
for 6 weeks to 32 weeks. Apart from the normal diet, the high energy-protein food

33
supplements were extra provided and served as snacks among 4 studies: Jahnavi &
Sudha (2010) provided sweet balls made from wheat flour, caramel, groundnuts and
vegetable ghee, which contained 600kJ energy and 6g protein every day; Patoon et al
(2004) served 2-3 packets of 200ml Ensure Plus, which contained 600-900kcal daily;
PrayGod et al (2012) provided six energy-protein biscuit bars daily which totally
consisted of 3690kJ energy and 29g protein. For the cohort study, Rudlop et al (2013)
gave 100g e’Pap’ daily which consisted of 1556kJ and 12.7g protein. Regarding the rest
two studies, they modified participants’ normal meals into high energy protein meals
(> 2500kal/day).
2.3.4. Comparison
Standard nutritional advices for TB patients were provided to the comparison
groups among four studies. PrayGod et al (2012) gave one energy-protein biscuit bar
to the control group patients daily. In the cohort study, as there was no comparison
group, the baseline data of the intervention group were utilized for comparison. In all
selected studies, the daily kilocalorie or energy intake of patients in intervention group
were briefly mentioned, however, none were shown to result in a total daily kilocalorie
intake for those in control group.

34
2.3.5. Length of follow-up
The length of follow-up among 6 studies varied from 8 weeks to 52 weeks.
Research teams continuously followed the participants until the intervention completed.
However, in two studies, the research teams particularly evaluated the outcomes after
the intervention ended for three to nine months (Jahnavi & Sudha, 2010; PrayGod et al,
2012)
2.3.6. Outcome measures
In order to monitor the nutritional status of TB participants, the anthropometrical
measures were generally considered which were easy to manage, non-invasive and not
costly. Basically, body weight, BMI and hand-grip strength were measured except in
Perez-Guzman et al (2005) study, they acted as the important marker of health and
nutritional status. The change in total lean mass, arm fat and muscle fat, which could
be an underestimate of the actual indicator in nutritional status, were also concerned.
Furthermore, some studies also put focus on the sputum conversion rate, treatment
completion rate and the rate of improvement of respiratory symptoms, which identified
if the dietary support influenced the recovery of TB (Jahnavi & Sudha, 2010; Martins
et al, 2009; Perez-Guzman et al, 2005).

35
2.3.7. Results
To summarize the results among six studies, body weight and BMI of the
intervention group had all significantly improvement except one did not revealed a
statically increase (PrayGod et al, 2012). For the inconsistent result, possible
explanations were illustrated. HIV-infected TB patients were included in that trial, as
TB and HIV infection are catabolic processes, the repletion of lean mass may need extra
protein and other nutrients to compensate for tissue impairment in anabolism. The food
supplement may increase the physical activities and energy requirements, rather than
increasing weight gain (PrayGod et al, 2012). The grip-strength of intervention group
patients consistently got significant increase among five studies. Regard of the sputum
conversion rate, it had found the mean duration for the sputum culture conversion of
intervention group was faster than the control group at the end of the intensive phase of
TB treatment (Jahnavi & Sudha, 2010; Martins et al, 2009; Perez-Guzman et al, 2005).
Jahnavi & Sudha (2010) reported a significant improvement in treatment completion
and Perez-Guzman et al (2005) found the sign and symptoms of respiratory diseases
have been improved, especially the sputum production got significantly alleviated after
completed the intervention.

36
2.4 SYNTHSIS OF THE DATA
2.4.1. Subjects
From the six included studies, the interventions were all applied to the patients
with active TB. Most patients also suffered from nutritional problem, like wasting,
which was similar to the targeted clinical setting. The mean age of the patients included
in the studies was about 30-40 which was slightly younger than that of patients in the
local setting. It was because most of the young adults in Hong Kong have been received
the BCG (Bacilli Calmette-Guerin) vaccine during their childhood. Due to aging and
the immunity changes, elder adults were probably attacked by mycobacteria
tuberculosis. Nevertheless, nutritional problem is a typical symptom of active TB, mild
discrepancy on age factor does not become a resistance for the transferability of the
evidence.
2.4.2. Assessment of nutritional status and counseling
In order to get an early nutritional picture of the active TB patients, they should
receive an assessment of their nutritional status. A target intake was calculated on the
basis of 35 kcal/day/kg body weight for each participant, and explained the important
of meeting the target. It encouraged the patients to achieve the adherence to the
nutritional TB treatment (Jahnavi & Sudha, 2010; Paton et al, 2004; Perez-Guzman et
al, 2005). Nutrition assessments, including anthropometric, biochemical and clinical

37
area, were a prerequisite for the provision of good nutritional care. An appropriate
counseling based on their nutritional status at diagnosis and throughout treatment was
recommended for the TB patient, it could have a positive influence to patient’s
nutritional status (Jahnavi & Sudha, 2010; Paton et al, 2004; Rudolph et al, 2013).
2.4.3. Earlier initiation of nutrition support: High energy-protein supplementation
An early initiation of nutritional support was proposed among the studies. High
energy protein dietary was provided as early as possible once the patient was diagnosed
as TB among all reviewed studies. Early restoration of nutritional status can cause the
immunologic changes and hence enhance the clearance of mycobacteria and alleviate
infectiousness of patients. The dietary diet should at least be taken in the intensive phase
of the anti-TB treatment, usually the first 2 months of starting TB antibiotics. During
the intensive phase of TB treatment, patients’ basal metabolic rate and energy
requirement increase rapidly. However, the energy-protein dietary after the intensive
phase of the treatment could be less advantaged as it greatly increased fat. It raised the
risk for later diabetes and cardiovascular disease (Paton et al, 2004).
For the food supplements, sweet balls, Ensure Plus, biscuit bar and e’Pap’ were
prepared for the subjects among these studies. Due to the non-tasty flavor of e’Pap’ and
the complicated preparation of sweet ball, Ensure Plus and biscuit bars would be the

38
favorable dietary strategies to accommodate the taste of different patients. These two
interventions will be incorporated in the proposed program.
2.4.4. Outcomes measures
According to the reviewed studies, evidence revealed the BMI, handgrip strength
and lean mass as the major indicators for nutritional status (Jahnavi & Sudha, 2010;
Paton et al, 2004; Martins et al, 2009; PrayGod et al, 2012; Rudolph, 2013).
Investigation of sputum culture and clearance of sputum smear were the indicators of
the bacteriologic sterilization (Martins et al, 2009; Perez-Guzman et al, 2005).
2.4.5. Closer outcomes monitoring
Paton et al (2004) and Perez-Guzman et al (2005) performed weekly monitoring
for the outcome measures for flexible adjustment of nutritional care. Paton et al (2004)
reviewed the subjects’ BMI weekly once implementing the high energy-protein
nutritional supplement to modify the content of the nutritional program. If the BMI got
improved and larger than 20kg/m2, the supplement were discontinued, otherwise the
supplementation continued and also stepped up the quantity.
2.5 CONCLUSION
Although there was no available study providing the most effective guideline for
energy-protein oral supplementation program to TB patients, several important
suggestions and elements have been identified via the literature review. Based on the

39
above analysis, the proposed program should have an assessment of nutritional status
and counseling before the implementation of nutritional intervention, and the
nutritional support should be early initiated with a close outcome monitoring.

40
CHAPTER 3: TRANSLATION AND APPLICATION
The implementation potential of the proposed program would be now assessed by
the transferability of the findings, feasibility and cost-benefit ratio in the target setting.
Every detail would be illustrated in this chapter.
3.1 Implementation Potential
3.1.1 Target setting
An isolation ward of a public hospital would be the target setting of the innovation.
24 beds in 14 rooms are in the target ward with all rooms under negative-pressure with
double door sealed designed.
3.1.2 Target audiences
According to the patient characteristics from the reviewed studies, the target
audience of the proposed innovation would be recruited the in-patients who are:
1. Aged 18 or above
2. Newly diagnosed active pTB (within 2 weeks)
3. Started on DOTS
4. Not diagnosed with multi-drug resistant TB
5. Not diagnosed with HIV infection and Dietetics Mellitus (DM)
6. BMI < 18.5 kg/m2
7. Allowed in oral feeding

41
3.1.3 Transferability of the findings
Target and audience
Among the reviewed trials, although two of them were conducted in the
community-based setting (Jahnavi & Sudha, 2010; Martins et al, 2009), the rest four
trails were organized in hospital or institutional-based setting, which is similar to the
proposed units. Furthermore, by comparing the patient’s age, gender, diagnosis,
treatment, nutritional status, and medical background, there are not much discrepancies
between those in reviewed studies and target audience. The ethnicities of all reviewed
studies were various, including Asian, White and Black; which is compatible to the
decided audience, as there are no restrictions of ethnicity in target unit. Therefore, based
on the high similarity of above components, it is highly transferable to the proposed
ward.
Underlying Philosophy of care
A new six point ‘stop TB strategy’ was developed to dramatically reduce the global
burden of TB in the future (WHO, 2014). Apart from pursuing high-quality DOTS
expansion and enhancement, addressing the needs for TB population, including
inadequate nutrient support is one of the focuses in the ‘stop TB strategy’.
The proposed innovation is well-match of the strategy developed by WHO. To
provide a holistic care, different aspects of care have to be considered to promote a
42
patient-centered care, a good prognosis of the disease, and hence enhance patient’s
quality of life.
Number of clients being benefited
In the target setting, an average 400 patients are newly diagnosis as TB in each
year and approximated 50% of them are with low BMI. By estimation, 219 patients
would benefit from the innovation.
Timeline of implementation and evaluation
Before implementing the program, about 3 weeks will be scheduled for
communication with multi-disciplines, program revision and the two training sessions.
Then, the 4-weeks pilot study would be initiated to the newly diagnosis patients with
DOTS prescribed. Patients’ outcomes would be evaluated weekly until discharge. The
implementation period would last for 12 weeks. At last, one week would be prepared
for the program evaluation. Totally 22 weeks would be reserved. The entire timeframe
is shown at Appendix N.
3.1.4 Feasibility
Organizational climate and administrative support
Organizational climate and administrative support definitely play the vital roles in
implementing changes. To get ready for a journey into a new era of health care system,
evidence-based practice (EBP) and continuous quality improvement scheme are highly
43
promoted and initiated in the target hospital in recent years. With the aim of eventually
leading hospital services into international healthcare standard, the target hospital is
facilitated by the hospital accreditation agency since 2009. At the same time, there are
various forms of engagement program provided for staff, for instance, seminars and
trainings with sponsorship and a cluster-based EBP development committee. It results
in a great contribution in boosting the nursing profession.
By focusing on the target unit, the evidence-based program of pressure ulcer
prevention and management and protocol of DOTS for TB patients have been
successively established and carried out.
Besides, based on the nutrition policy of the target hospital, which stipulates the
essential elements of nutrition care to ensure the optimal nutrition care should be
delivered to meet patients’ needs during their hospitalization journey. The
multidisciplinary and collaborative approach, for example, the physicians, nurses and
dietitians, are encouraged to provide efficient care delivery. Thus, it sounds possible to
gain approval of the implementation of innovation without much resistance from those
departments.
Therefore, new evidence-based innovations would be welcome and possibly
launched under such supportive circumstance.

44
Staff‘s acceptability
As the proposed innovation would be mainly operated by the nursing staff, their
acceptability is the key factor toward the success of the innovation. Nutritional problem
due to TB has been a concern in current nursing care. Wasting, weakened physical
function might adversely influent the prognosis of the disease and prolong the
hospitalization time. Instead of interfering with current staff functions, the innovation
could bring positive impacts to them, for instance, reducing workload and stress. To
implement this program, no specific skill or extra manpower is required. Some
additional work needed are performing a 10-min nutritional assessment for newly
diagnosed TB patients by using a designed form (Appendix F) and orientating a 10-min
nutrition program introduction to patient and patient’s relatives.
Nurses may lack confidence and feel stressed to implement the nutritional
interventions as they might not receive certain training of this knowledge field before.
To alleviate and clarify the misconceptions, routine nursing sharing sessions and journal
club are indispensable. They would become more confident in providing professional
nursing care with a latest evidence support. For the empowerment, two identical 45-
min briefing sessions (Appendix G) will be provided to all frontline nurses before the
implementation.

45
Availability of resources
Resources are available for staff training, including interview rooms, computers,
projectors and screens, printers and microphones. The designated energy-protein food
products and measuring tools, except the digital dynamometer for measuring the
handgrip strength, are available in the target setting. For the documentation forms, they
can be freely printed from printer by ward clerks.
Collaborations among various disciplines
Medical officers and dietitians would be the major collaborating partners. There
would not be much resistance from the medical officers as this innovation would not
create much changes of their practice. Moreover, they always concern about the
nutritional status of TB patients and would be appreciated if there is a systematic and
EBP to monitor and enhance patients’ needs.
In usual practice, all nutrition problems of patient would be referred to dietitian in
the target setting. However, there are many consultations every day in the target hospital,
for the non-urgent cases, the dietitians might assess the cases two days later since the
referral form was sent. If the program is initiated, the cases are filtered by nurses and
the primary nutrition problem of TB patients would be tackled. Therefore, it will
minimize the workload and save time for the dietitians. It is possible and feasible to get
a high degree of consensus obtained among these two cooperating parties.

46
3.1.5 Cost-benefit Ratio
Potential Benefits
As evidenced by the reviewed trails, most participants gained benefits from the
dietary program. Their BMI and physical function are significantly improved (Jahnavi
& Sudha, 2010; Paton et al, 2004; Martins et al, 2009; PrayGod et al, 2012; Rudolph,
2013). The sputum conversion rate is also significant enhanced which implies the TB
patients can be off isolation earlier and return to the community. Their quality of life
during the infection period was promoted (Jahnavi & Sudha, 2010; Paton et al, 2004;
Martins et al, 2009).
To the frontline nurses, it is also beneficial. Better compliance of TB treatment and
higher rate of improvement of respiratory symptoms can directly alleviate the workload
and stress of nurses. Furthermore, nurses are encouraged to pursue a greater autonomy
in independent decision making through implementing an EBP, thus better job
satisfaction could lower the turnover rate of the frontline staff.
To an organization, as the mean duration for the sputum culture conversion of TB
patients with nutritional program was about 14 days earlier than those in control group
(Jahnavi & Sudha, 2010; Perez-Guzman et al, 2005.). By calculation, the target ward
has to spend an extra operation fee $68,040 for each TB patient in these 14 days;
however, with implementing the innovation, the cost for energy-protein products and

47
staffing cost for managing one target patient maximally are $1270.7 (Appendix H). By
having a great reduction of healthcare cost, the target hospital would have much
potential resource to step up the healthcare development.
Potential material and non-material cost
Most of the hardware is available in target setting; the material cost will be only
the digital dynamometer ($1000) and the two staff training sessions which cost $4340.6
(Appendix I). Meanwhile, the non-material cost is harder to estimate. The possible non-
material cost is the friction from the nurses and patients’ non-compliance to the program.
As mentioned, nurse might feel insured and frustrated with the change at the beginning
stage, which could terminate the dietary problem or even absenteeism, so how do they
convince the patients to change their usual eating habit and complete the whole four
weeks programs?
To resolve the above challenges, a supportive and on-going appreciation and
training will facilitate the performance of the prior nursing staff.
For patients, apart from the detailed and clear introduction of the program, their
eligibilities and preferences of participating should be assessed and respected. A verbal
consent should be obtained before implementation.

48
Potential risks
There are two sides to every coin. First, some TB patient s might dislike the taste
of the energy-protein products and be allergic to the energy-protein products. Second,
Paton et al (2004) pointed that TB patients might not be beneficial after the early stages
of TB treatment; the over-consumption of energy-protein food products might increase
the risk of building fat and increase the risk of cardiovascular disease. Therefore,
the program would be lasted for 4 weeks (within the intensive phase) and the products
are carefully selected which they are low in saturated fat and cholesterol. The
intervention will be terminated once the adverse effect is shown or the patients decide
to withdraw. After the above modifications, it is believed that the program is safe to be
adopted.
To conclude, the proposed program is highly transferrable, feasible and cost
effective to be implemented. An evidence-bases energy-protein dietary program is
going to be developed.

49
3.2 Evidence-based energy-protein dietary program to improve the nutritional
status among TB patients
3.2.1 Background
Historically, TB is recognized as a ‘consumption’ disease. Nutritional support is
advocated as important part of the routine management of TB. Studies revealed a
negative energy balance; nutrients mal-absorption and altered metabolism would lead
to wasting, adverse treatment outcome and even increased risk of death. An evidence-
based energy-protein dietary program to improve the nutritional status among TB
patients is introduced.
3.2.2 Objectives
To provide an evidence-based clinical pathway to TB patient with wasting
To increase the nurses’ awareness of the importance of nutritional support for TB
patients
To improve patients’ nutritional status, including improved body weight, handgrip
strength and lean mass.
To promote the earliest bacteriologic sterilization of patient
To assist nurses to integrate the best available evidence into clinical practice
50
3.3.3 Target users
Nurses working in targeted isolation ward
3.3.4 Target patient population
Details were mentioned 3.1.2.
3.3.5 Rating Scheme for the Strength of the recommendation
This nutritional program is developed according to the reviewed studies and
synthesized from the SIGN methodology of SIGN 50: A guideline developer’s
handbook (SIGN, 2012). The guide of determining the level of evidence for studies is
attached in Appendix J.
3.3.6 Recommendations
Recruitment:
Recommendation 1: The energy-protein dietary program is not suggested to the
patients with HIV infection and DM.
A
Evidence:
Patients with a positive HIV antibody test or DM are excluded (Jahnavi &
Sudha, 2010; Paton et al, 2004; Perez-Guzman et al, 2005).
1+
HIV is a catabolic process, higher amounts of protein and other nutrients
to compensate for the impairment in anabolism which is associated with
infection (PrayGod et al, 2012).
1+
51
Assessment:
Recommendation 2: Nutritional assessment should be conducted for every
tuberculosis patient.
A
Evidence:
Nutritional status can influence the efficacy of anti-tubercular treatment
(Perez-Guzman et al, 2005).
1+
Under-nutrition or wasting attributed to loss of appetite that leads to low
daily food intake, and influenced metabolism as part of the inflammatory
and immune response (Jahnavi & Sudha, 2010; Paton et al, 2004; PrayGod
et al, 2012) .
1+
Recommendation 3: An individual counseling and education on dietary should
be provided to every TB patient.
A
Evidence:
Every TB patient was given verbal and written advice concerning the
types of locally available food that would constitute a balanced diet likely
to assist cure of TB (Martins et al, 2009).
1++
Individual counseling and education is necessary to calculate a target
energy and protein intake per day and explain the importance of meeting
1+

52
the target nutrient intake during TB infection (Jahnavi & Sudha, 2010;
Paton et al, 2004).
The compliance rate to the intervention will be higher as the TB patients
received more information about the nutrient support (PrayGod et al,
2012).
1+
Intervention:
Recommendation 4: Nutrition support, extra 600 kcal/day to 900 kcal/day,
should be started as early as possible and should be implemented in the
intensive phase (the first two months) of TB treatment. ).
A
Evidence:
The target patients with the energy-protein supplements (600 kcal/day to
900 kcal/day) were all newly diagnosed as pTB and started on anti-TB
therapy. (Jahnavi & Sudha, 2010; Paton et al, 2004; Perez-Guzman et al,
2005; Rudolph et al, 2013)
1+,
1+,
2+
Early provision of supplement produces a significant increase in body
weight and lean tissue; it also leads to immunologic changes that could
enhance the clearance of mycobacteria and reduce infectiousness of
patients. (Jahnavi & Sudha, 2010; Paton et al, 2004; Martins et al, 2009)
1+,
1+,
1++

53
Recommendation 5: The duration of energy-protein program is most
beneficially within the intensive phases, approximately for 4-6 weeks, but not
last for the whole TB treatment.
A
Evidence:
Patients’ nutritional status and the rate of sputum conversion were
improved significantly when the nutritional program implemented for 4-6
weeks. (Paton et al, 2004; Perez-Guzman et al, 2005; Rudolph et al, 2013)
1+,
1+,
2+
Continuing excess energy intake beyond the intensive phase is
questionable as the energy appeared to be deposited mainly as fat; which
promotes higher risk cardiovascular risk. (Paton et al, 2004; Perez-
Guzman et al, 2005)
1+
Evaluation:
Recommendation 6: On-going assessment should be performed during the
implementation.
A
Evidence:
Patient’s dietary intake and outcomes were reviewed weekly, since every
patient may have their own comments and condition changes during the
dietary program. (Paton et al, 2004; Perez-Guzman et al, 2005; Rudolph et
al, 2013)
1+,
1+,
2+

54
Recommendation 7: The nutritional status is compliance by measuring body
weight, handgrip strength and lean mass respectively.
A
Evidence:
The nutritional status could be assessed in the anthropometrical and
functional aspects. Body weight, handgrip strength and lean mass are
treated as the major indicators of nutritional status (Jahnavi & Sudha,
2010; Paton et al, 2004; Martins et al, 2009; PrayGod et al, 2012;
Rudolph, 2013)
1+,
1+,
1++
1+,
2+

55
CHAPTER 4: IMPLEMENTATION PLAN
A thorough implementation plan can make the journey smoother and without the
pressure of getting to the destination. With the establishment of the proposed innovation,
a communication plan and pilot study should be designed to facilitate the transition and
get the program at the right time and sequence for success.
4.1 COMMUNICATION PLAN
A clear communication plan is vital to the success of the innovation. It ensures all
stakeholders are equally informed so that so there is a consistent message to the target
patients. The major stakeholders identified for the proposed innovation and the ‘top-to-
down’ strategy are going to be discussed as below:
4.1.1 HOSPITAL MANAGEMENT
The department operation manager (DOM), ward specialist and ward manager are
the important people who approve the proposed program and provide adequate
resources and necessary support at the management level in the target setting. Ward
manager would be the first person to be persuaded, together with a summary of
literature review, current problem of the TB patients in the target setting, the details of
the proposed program, including objectives, implementation and evaluation plan, cost-
benefit analysis, obstacles and solutions and timeframe. After gaining the approval of
the ward manager, a precise presentation would be performed to DOM and ward

56
specialist in the monthly manager meeting. Apart from the above mentioned details of
the program, a clear budget plan is going to be shown. In order to enhance the feasibility
of the dietary problem, suggestions and ongoing refinement will be considered.
4.1.2 FRONTLINE NURSING STAFF
After being granted the permission from the management level, Nurses would be
the next target. Nursing staff involvement is extraordinary conspicuous in the program,
as they are the main user to carry out the program. As the climate in nursing profession
is rather traditional, extra effort is needed to make ‘changes’. To aim at gaining nurses
acceptance and corporation, they are invited to attend the orientating session, with the
content similar to that present to ward manager. The urge of the patient needs and the
benefits of this EBP should also be emphasized to them. The program can be
promulgated to nurses by organizing case conference and nursing sharing sessions
during working hour, an interactive discussion is encouraged. Then, their comments
would be collected through evaluation forms which are distributed in each orientation
sessions. Target frontline nurses might still get confused and question about the
proposed program, adequate inquiry time should be held for them to clarify their
concern and misconception. In addition to the Q&A period in the two orientating
sessions, they are welcome to share any point of views about the innovation via email.
57
4.1.3 RESPIRATORY SPECIALISTS
Doctors are responsible to manage the nutrition condition of advising on the
appropriate feeding mode of feeding. Due to the differential power relations between
doctor and nurse, medical support is need to minimize the potential resistance. After
approved by ward physician, the implementation plan will be conveyed in the monthly
respiratory meeting. An oral presentation would be performed at that time; the content
is similar to the one that was given to the nurses. The doctors’ role and the outcome of
the proposed dietary program would be indicated. Advices are always welcome.
4.1.4 DIETITIANS
Dietitian’s support is indispensable because the focus of the proposed innovation
is a dietary intervention. It is necessary to enhance the nurse-dietitians partnership
during the implementation period, the concept and details will be clearly explained at
the stage of confirming the feasibility of the program. Their opinions are definitely
valuable in the design of this innovation. The finalized logistics will be presented to the
Milk and Nutrition Committee when the approval attended.
4.1.5 CLERICAL STAFF
The clerical staff is taking part in arranging documents and procedures of diet
ordering, data collection and evaluation. A briefing would be given to them before the
implementation.

58
4.1.6 PATIENTS AND THEIR CAREGIVERS
Last but not least, the TB patients are the target of the proposed innovation. A well-
illustrated sheet, including the information of TB, potential adverse effects of the anti-
TB treatment, and outline of proposed dietary program would be provided to patients
and their caregivers with explanations. Written consent should be obtained before
initiating the program. Moreover, posters of this dietary program would be displayed
on the education board of the ward in order to raise the awareness of the visitors towards
the importance of nutrition care of TB patients.
4.2 PILOT STUDY
After communicating with various stakeholders, a pilot study should be conducted
to have a small-scale preliminary trial. It is crucial to test the feasibility of the program.
It can give an advance warming about whether the method or instruments are
appropriate or complicated; the acceptability and satisfaction of the staff and patients
getting involved in the program and any unexpected difficulties encountered in the trial.
Thus, appropriate modification could be made afterward.
4.2.1 OBJECTIVES
To determine the feasibility of the design of the energy-protein dietary program
To assess the adherence of target patients and compliance of nurses to the program
To assess the satisfaction level of the patients and nurses toward the program

59
To identify any unanticipated obstacles during actual implementation
To estimate the budget of implementation
4.2.2 TARGET SETTING AND TARGET AUDIENCE
These are as same as in the proposed program described in the chapter 3.
4.2.3 STUDY DESIGN
A 4-weeks pilot study will be conducted in a mixed isolation ward after the
completion of the briefing sessions. A one group quasi-experimental design will be
applied for the pilot test. Convenience sampling method would be adopted to recruit
the target subjects. The inclusion and exclusion criteria and the workflow constituted
for the actual implementation would be applicable to the pilot study. According to the
ward admission statistic record in 2014, approximately 4 eligible patients admitted to
the target ward weekly. With the highest dropout rate as about 20% (PrayGod et al,
2011), 20 samples will be expected to be recruited in the pilot study.
4.2.4 ETHICAL CONSIDERATION
The fundamental ethical principles in conducting medical research are developed
to protect the rights, dignity and welfare of research subjects, an ethical approval should
be obtained from the Hospital Clinical Research Ethic Committee. All eligible
participants taking part in the pilot study would receive the information sheets and
consent forms. The purpose of procedure, risks, benefits and the way to collect data of

60
pilot test would be illustrated by trained nurses. Patient’s written consent has to be
obtained before participating.
4.2.5 EVALUATION OF THE PILOT STUDY
Evaluation will be started after the first week of the pilot study. First, patient’s
daily input and output chart will be reviewed weekly for assessing the adherence to the
program. And a questionnaire (Appendix M) in a 6-point Likert Scale will be
distributed to patients upon the completion of the study to determine their satisfaction
level.
Second, to evaluate the program flow and nurses’ compliance, data will be collected via
bi-weekly evaluation by using the ‘self-designed audit form’ (Appendix K) and the
involved nurses would be invited to have a semi-structured group interview for further
feedback collection. Staff satisfaction level will be assessed by the ‘self-administrated
questionnaire’ at the end of the pilot (Appendix L).
In the pilot study, the time frame and the cost expenditure can be calculated and
can be a reference for the actual implementation. Any unexpected consumption of time
and money would be considered and discussed afterward for further refinement.
All data collected from the evaluation part will be transcribed in a written report
and taken as the recommendations to modify of the program. An evaluation report
would be subsequently distributed to the frontline nurse and respiratory specialists

61
through email, and presented in the managers meeting for final approval of the actual
implementation.
4.3 CONCLUSION
To ensure the successful translation of evidence into actual practice, it is important
to start with an implementation plan. It includes a well –prepared communication plan
and pilot study, which definitely contribute an effective implementation of the EBP
program in a long run.
62
CHAPTER 5: EVALUATION PLAN
A systematic evaluation plan is an essential component for implementation; it
determines the quality and effectiveness of a program, quantifies the effort of the
stakeholders and promotes continuous enhancement. Evaluation of outcome measures,
nature and number of involved client, data collection and analysis and criteria for
effective change are elaborated as follows.
5.1 OUTCOME MEASURES
The outcome measures would be evaluated from three aspects: patient, healthcare
providers and the system. Patients’ outcome weight heavily in evaluation because the
proposed program is designed for the TB patients in promoting their health during the
infection period.
5.1.1 Patient outcome
The objectives of the proposed program are to improve underweighted TB patients’
nutritional status and shorten the infection time. To determine the effectiveness of the
program, the nutritional status, including weight gain, improved handgrip strength and
lean mass, and the rate of clearance of sputum smears are assessed according to the
previous discussed studies. By summarizing the reviewed trials, patients’ adherence
level to the energy-protein oral supplement can be revealed by Input & Output chart
because the outcomes definitely correlate with patient’s consumption. To determine the

63
quality of care, the questionnaires in 6-point Likert scale would be given to each
participant to measure their satisfaction level. It also can indicate the reason of poor
compliance and withdrawal from the program.
5.1.2 Healthcare provider outcome
Nurses’ compliance level would be assessed by the self-designed audit form to
ascertain the application of the program and outcome measures. Besides, their
satisfaction level would be reflected by the self-administrated questionnaire.
5.1.3 System outcome
From the view of hospital, shortening the hospitalization period and cost control
are important in launching the dietary program, hence the length of stay in isolation of
eligible patients and the operation cost, including the cost of dietary products and
document printing, are going to be evaluated.
5.2 NATURE AND NUMBER OF INVOLVED CLIENTS
The characteristics of the patients recruited in the proposed program are designed
by taking reference of the reviewed studies. An outline computer program (Lenth,
2006-9) is utilized to calculate the sample size required in evaluation of this dietary
program. By taking a one sample t test with a power of 0.8, a standard deviation of
3.5kg of weight gain, significant level of 0.05 and with the estimation of 20% drop out
rate, the minimum sample size is 39. The proposed intervention will last for about 12

64
weeks.
5.3 DATA COLLECTION AND ANALYSIS
Time and frequency of review the measures would be various for different
parameters obtained. Within the 12 weeks evaluation, statistical analysis will be utilized
by the Statistical Package for Social Science (SPSS).
5.3.1 Patient outcome
Regarding patient outcomes, body weight, grip strength and lean mass will be
measured weekly, and the sputum would be sent for investigation of AFB smear every
two days. Concerning these totally four patient outcomes, they are the quantitative
variables which can be described by means and standard deviations and the first three
can be analyzed with one sample t test to measure any statistically significant
differences before and after implementing the dietary intervention.
5.3.2 Healthcare provider outcome
About the health care providers outcomes, their compliance rate and satisfactory
level are the major concerns. For the former one, a nursing compliance audit would be
conducted in the middle (week 6) and at the end of implementation period. The
compliance percentage is the number of items filled in will be over by the total number
of items in the audit form.
To determine the satisfaction level among nurses, every involved nurse will receive the
65
self-administrated questionnaire after the program accomplished. By having a mean
score of each item of the questionnaire, a textual data analysis will be presented in form
of the descriptive statistical method.
5.3.3 System outcome
The last but not least, to the system outcome, the length of stay in isolation ward
will be compared with the statistical figure of last three months before launching the
program by a two-tailed independent t-test. And the cost of dietary program will be well
controlled. These two outcomes would be evaluated at the end of the program.
5.4 CRITERIA FOR THE EFFECTIVE CHANGES
To determine the effectiveness of the proposed innovation, literatures were
reviewed to set the changes that are considered as effectives. For the main criteria for
the patient outcomes, 3.7-6.4 kg of weight gain, 3.2-6.3kg of grip strength and 1.3-3kg
of lean mass were found of the subjects in reviewed trials, so the program is deemed
effective if the body weight of eligible patients increases by over 5 kg during the
implementation period; the grip strength increase by 4.7 kg and the lean mass increase
by 2.1 kg during the implementation. And the duration of sputum clearance of AFB
smear is set to be within 14 days. Over 80% of the participants reveal good compliance
in having the energy-protein supplements. The mean value for each question should be
4 or above for patient satisfaction on the scale.

66
At least 85% compliance rate of nursing audit in the target setting and the mean
score of 4 or above for each item in the self-administrated questionnaire should be
targeted for the healthcare provider outcome.
Regarding the system outcome, the length of stay in isolation ward should be
reduced by 50% by comparing the usually stay; and the cost of program should maintain
at $150 per participants during implementation period.
5.5 CONCLUSION
Implementation and evaluation plans are required to assess the feasibility and
expected outcomes of the energy-protein oral supplement program. By considering and
getting prepared for the above aspects of the program, it would be promoted in a
successful way.

67
CHAPTER 6: CONCLUSION
Tuberculosis is a global health concern and the incident rate remains high in Hong
Kong. TB and nutrition is under an indivisibility relationship. Nutritional state of TB
patient is usually weakened during infection period; under-nutrition at the time of
diagnosis of active TB increases the risk of death and TB relapse. However, there is
currently no an evidence-based dietary program available to TB patients. In this
translational research, an evidence-based energy-protein dietary program for TB
patients was developed after systematic reviewing and critically appraising six high
quality research studies.
The program is going to be disseminated in the target setting, which is one
isolation ward in a public hospital in Hong Kong. The implementation potential of the
program is considered to be high while the implementation and evaluation plan are also
illustrated. With the implementation of the evidence-based program, the nutritional
status and the rate of the sputum sterilization of TB patients are expected to be enhanced.

68
CHAPTER 7: REFERENCES
Cegielski, J. P., & McMurray, D. N. (2004). The relationship between malnutrition
and tuberculosis: evidence from studies in humans and experimental animals. The
International Journal of Tuberculosis and Lung Disease, 8(3), 286-298.
Chandra, R. K. (1991). 1990 McCollum Award lecture. Nutrition and immunity:
lessons from the past and new insights into the future. The American Journal of Clinical
Nutrition, 53(5), 1087-1101.
Centre for Health Protection. (2014). Statistics on communicable disease:
Notifiable infectious diseases. Retrieved May 17, 2014, from
http://www.chp.gov.hk/en/data1/10/26/43/2210.html
Department of Health. (2011). Energy Requirement - Change 4 Health. Retrieved
July 17, 2014, from
http://www.change4health.gov.hk/en/healthy_diet/facts/calories_nutrients/calories_en
ergy/index_t.html
Dodor, E. A. (2008). Evaluation of nutritional status of new tuberculosis patients
at the effia-nkwanta regional hospital. Ghana Medical Journal, 42(1), 22-28.
Gupta, K. B., Gupta, R., Atreja, A., Verma, M., & Vishvkarma, S. (2009).
Tuberculosis and nutrition. Lung India, 26(1), 9-16.
Hanrahan, C. F., Golub, J. E., Mohapi, L., Tshabangu, N., Modisenyane, T.,

69
Chaisson, R. E., Gray, G. E., McIntyre, J. A., & Martinson, N. A. (2010). Body mass
index and risk of tuberculosis and death. AIDS, 24(10), 1501-1508.
Hood, M. L. H. (2013). A narrative review of recent progress in understanding the
relationship between tuberculosis and protein energy malnutrition. European Journal
of Clinical Nutrition, 67, 1122-1128
Institute of Medicine. (2005). Dietary reference intakes for energy, carbohydrate,
fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington, DC: National
Academies Press.
Jahnavi, G., & Sudha, C. H. (2010). Randomised controlled trial of food
supplements in patients with newly diagnosed tuberculosis and wasting. Singapore
Medical Journal, 51(12), 957-962.
Karyadi, E., Schultink, W., Nelwan, R. H., Gross, R., Amin, Z., Dlmans, W. M.,
van der Meer, J. W., Hautvast, J. G., & West, C. E. (2000). Poor Micronutrient Status
of Active Pulmonary Tuberculosis Patients in Indonesia. Journal of Nutrition, 130(12),
2953-2958.
Khan, A., Sterling, T. R., Reves, R., Vernon, A., & Horsburgh, C. R. (2006). Lack
of weight gain and relapse risk in a large tuberculosis treatment trial. American Journal
of Respiratory and Critical Care Medicine, 174(3), 344-348.
Krapp, F., Véliz, J. C., Cornejo, E., Gotuzzo, E., & Seas, C. (2008). Bodyweight

70
gain to predict treatment outcome in patients with pulmonary tuberculosis in Peru. The
International Journal of Tuberculosis and Lung Disease, 12(10), 1153-1159.
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [Computer
software]. retrieved May 15, 2015 from http://www.cs.uiowa.edu/~rlenth/Power/
Lönnroth, K., Williams, B. G., Cegielski, P., & Dye, C. (2010). A consistent log-
linear relationship between tuberculosis incidence and body mass index. International
journal of epidemiology, 39(1), 149-155.
Macallan, D. C. (1999). Malnutrition in tuberculosis. Diagnostic microbiology and
infectious disease, 34(2), 153-157.
Macallan, D. C., McNurlan, M. A., Kurpad, A. V., de Souza, G., Shetty, P. S.,
Calder, A. G., & Griffin, G. E. (1998). Whole body protein metabolism in human
pulmonary tuberculosis and undernutrition: evidence for anabolic block in tuberculosis.
Clinical Science. 94(3), 321-331.
Macallan, D. C., Noble, C., Baldwin, C., Jebb, S. A., Prentice, A. M., Coward, W.
A., Sawyer, M. B., McManus, T. J., & Griffin, G. E. (1995). Energy Expenditure and
Wasting in Human Immunodeficiency Virus Infection. The New England Journal of
Medicine, 333(7), 83-88.
Martins, N., Morris, P., & Kelly, P. M. (2009). Food incentives to improve
completion of tuberculosis treatment: randomized controlled trial in Dili, Timor-Leste.

71
British Medical Journal, 339:b4248. doi: 10.1136/bmj.b4248.
McMurray, D. N., & Bartow, R. A. (1992). Immunosuppression and alteration of
resistance to pulmonary tuberculosis in guinea pigs by protein undernutrition. The
Journal of Nutrition, 122(3), 738-743.
Metcalfe, N. (2004). A study of tuberculosis, malnutrition and gender in Sri Lanka.
Transactions of the Royal Society of Tropical Medicine and Hygiene, 99(2), 115-119.
Miller, L. G., Asch, S. M., Yu, E. I., Knowles, L., Gelberg, L., & Davidson, P.
(2000). A population-based survey of tuberculosis symptoms: how atypical are atypical
presentations? Clinical Infectious Disease, 30(2), 293-299.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA
Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
Mupere, E., Malone, L., Zalwango, S., Okwera, A., Nsereko, M., Tisch, D. J.,
Parraga, I. M., Stein, C. M., Mugerwa, R., Boom, W. H., Mayanja, H. K., & Whalen,
C. C. (2014). Wasting among Uganda men with pulmonary tuberculosis is associated
with linear regain in lean tissue mass during and after treatment in contrast to women
with wasting who regain fat tissue mass: prospective cohort study. BMC Infectious
Diseases, 14(24). doi: 10.1186/1471-2334-14-24.
Paton, N. I., Chua, Y. K., Earnest, A., Chee, C. B. (2004). Randomized controlled

72
trial of nutritional supplementation in patients with newly diagnosed tuberculosis and
wasting. American Society for Clinical Nutrition, 80(2), 460-465.
Pérez-Guzmán, C., Vargas, M. H., Quiñonez, F., Bazavilvazo, N., & Aguilar, A.
(2005). A cholesterol-rich diet accelerates bacteriologic sterilization in pulmonary
tuberculosis. Chest, 127(2), 643-651.
Piva, S. G., Costa, M. C., Barreto, F. R., Pereira, S. M. (2013). Prevalence of
nutritional deficiency in patients with pulmonary tuberculosis. Jornal de pneumologia,
39(4), 476-483.
PrayGod, G., Range, N., Faurholt-Jepsen, D., Jeremiah, K., Faurholt-Jepsen, M.,
Aabye, M. G., Jensen, L., Jensen, A. V., Grewal, H. M , Magnussen, P., Changalucha,
J., Andersen, A. B., & Friis, H. (2012). The effect of energy-protein supplementation
on weight, body composition and handgrip strength among pulmonary tuberculosis
HIV-co-infected patients: randomised controlled trial in Mwanza, Tanzania. The British
Journal of Nutrition, 107(2), 263-271.
Ralph, A. P., Waramori, G., Pontororing, G. J., Kenangalem, E., Wiguna, A., Tjitra,
E., Lolong, D. B., Yeo, T. W., Chatfield, M. D., Soemanto, R. K., Bastian, I., & Lumb,
R. (2013). L-arginine and Vitamin D Adjunctive Therapies in Pulmonary Tuberculosis:
A Randomised, Double-Blind, Placebo-Controlled Trial. Plos One, 8(8), e70032. doi:
10.1371/journal.pone.0070032

73
Raj, T., D’Souza, G., Elia, M., & Kurpad, A.V. (2006). Measurement of 24 h
energy expenditure in male tuberculosis patients. Indian Journal of Medical Research,
124, 665-676.
Rudolph, M., Kroll, F., Beery, M., Marinda, E., Sobiecki, J. F., Douglas, Geoffrey.,
& Orr, Gary. (2013). A Pilot Study Assessing the Impact of a Fortified Supplementary
Food on the Health and Well-Being of Crèche Children and Adult TB Patients in South
Africa. PloS one, 8(1), e55544. doi: 10.1371/journal.pone.0055544.
Scottish Intercollegiate Guidelines Network. (2012). Methodology Checklist 2:
Randomized Controlled Trials. Retrieved July 30, 2014 from
http://www.sign.ac.uk/guidelines/fulltext/50/checklist2.html
Scottish Intercollegiate Guidelines Network. (2012). SIGN 50: A guideline
eveloper’s handbook ANNEX B: key to evidence statements and grades of
recommendations. Retrieved July 19, 2014 from
http://www.sign.ac.uk/guidelines/fulltext/50/annexb.html
Semba, R. D., Darnton-Hill, I., & Pee, D. S. (2010). Addressing tuberculosis in
the context of malnutrition and HIV coinfection. Food and Nutrition Bulletin. 31(4),
345-364.
Shetty, N., Shemko, M., Vaz, M., & D'Souza, G. (2006). An epidemiological
evaluation of risk factors for tuberculosis in South India: a matched case control study.

74
The International Journal of Tuberculosis and Lung disease, 10(1), 80-86.
Sudarsanam, T. D., John, J., Kang, G., Mahendri, V., Gerrior, J., Franciosa, M.,
Gopal, S., John, K. R., Wanke, C. A., & Muliyil, J. (2011). Pilot randomized trial of
nutritional supplementation in patients with tuberculosis and HIV-tuberculosis
coinfection receiving directly observed short-course chemotherapy for tuberculosis.
Journal of tropical medicine and hygiene, 16(6):699-706.
van Lettow, M., Kumwenda, J. J., Harries, A. D., Whalen, C. C., Taha, T. E.,
Kumwenda, N., Kang'ombe, C., & Semba, R. D. (2004). Malnutrition and the severity
of lung disease in adults with pulmonary tuberculosis in Malawi. The International
Journal of Tuberculosis and Lung disease, 8(2), 211-217.
World Health Organization. (1999). Management of severe malnutrition: a manual
for physicians and other senior health workers. Geneva: World Health Organization
publication.
World Health Organization. (2013). Global Tuberculosis Report, Switzerland:
World Health Organization publication.
World Health Organization. (2014). Tuberculosis: Fact sheet. Retrieved May 17,
2014, from http://www.who.int/mediacentre/factsheets/fs104/en/
World Health Organization. (2014). Tuberculosis: The Stop TB Strategy. Retrieved
May 17, 2014, from http://www.who.int/tb/strategy/en/

75
Young, D. B., Gideon, H., & Wilkinson, R. J. (2009). Eliminating latent
tuberculosis. Trends Microbiology, 17, 183-188.
Zachariah, R., Spielmann, M. P., Harries, A. D., & Salaniponi, F. M. (2002).
Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated
with early death. Transactions of the Society of Tropical Medicine and Hygiene, 96(3),
291-294.

76
Appendix A: Search Strategies and Search History
Search Keywords Database
PubMed CINAHL PLUS
(EBSCOhost)
British Nursing
Index
PsyInfo
1 Pulmonary Tuberculosis 79647 847 23 235
2 Mycobacterium
Tuberculosis
56194 769 14 99
3 1 or 2 121772 1420 35 35
4 Diet 379284 19670 4918 21219
5 Dietary 501057 20434 1369 13278
6 Nutrition 298969 17953 7507 23054
7 Nutritional supplement 50095 76 177 745
8 Energy protein nutritional
supplement
4171 14 43 43
9 4 or 5 or 6 or 7or 8 702434 41887 8458 45132
10 Under-nutrition 18527 40 141 1616
11 Wasting 18190 339 46 596
12 Body mass index 144741 13459 958 12300
13 Physical function 927859 898 411 42119
14 Body composition 59584 3064 133 2534
15 10 or 11 or 12 or 13 or 14 1062243 16227 1587 57812
16 3 and 9 891 15 10 9
17 3 and 15 1238 20 6 3
18 3 and 9 and 15 149 2 2 1
Filtered by inclusion and
exclusion criteria
3 2 1 1
Studies retrieved from
related citation or reference
list
2 2 2 0
Number of studies recruited 5 4 (3 duplicated) 3 (All duplicated) 1 (Duplicated)
Total number of studies
recruited
6

77
Appendix B: PRISMA 2009 Flow Diagram
Records identified through
database searching
(n =154 )
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n
Additional records identified
through other sources
(n = 58 )
Records after duplicates removed
(n = 96 )
Records screened
(n = 28 )
Records excluded
(n = 36 )
Full-text articles assessed
for eligibility
(n =6 )
Full-text articles excluded,
with reasons
(n = 22 )
Studies included in
qualitative synthesis
(n = 6 )
Studies included in
quantitative synthesis
(meta-analysis)
(n = 6 )

78
Appendix C: Tables of Evidence

79

80
Citation (3) Study type Patient characteristics Intervention (s) Comparison Length of followC
up
Outcome measures Effect size
Martins et al
(2009)
Randomized
controlled
trial
- Aged ≥18 years
- Newly diagnosed active pTB
- Started on DOTS
Intervention group:
1. Age (yrs): 33.9± 14.2*
2. Male patients: 65%
3. Female patients: 35%
4. Weight(kg): 43.0± 7.3
5. BMI(kg/m2)<18.5: 79%
6. BMI(kg/m2)>18.5: 21%
Control group:
1. Age (yrs): 32.6± 13.4*
2. Male patients: 65%
3. Female patients: 35%
4. Weight(kg): 43.6± 7.6
5. BMI(kg/m2)<18.5: 80%
6. BMI(kg/m2)>18.5: 20%
(n=270)
High-energy food
supplement ( red
kidney beans, meat
and rice, about 1800kJ
energy) daily for 32
weeks
(n=137)
Standard nutritional
advice for TB patients
(n=133)
32 weeks Primary outcome:
1. Completion of
anti-TB
treatment
Secondary
outcomes:
2. Adherence to
treatment
3. Weight gain
(kg)
4. Clearance of
sputum smears
1. Intervention: 76%
Control: 78%
(RR: 0.98, p=0.7)
2. Intervention: 98.2±6.7
Control: 98.3±6.7
(RR: 0, p=1.0)
3. Intervention: 10±9.6
Control: 7.5±7.6
(RR: 2.6, p=0.04)
4. Intervention: 84%
Control: 80%
(RR: 1.05, p=0.4)
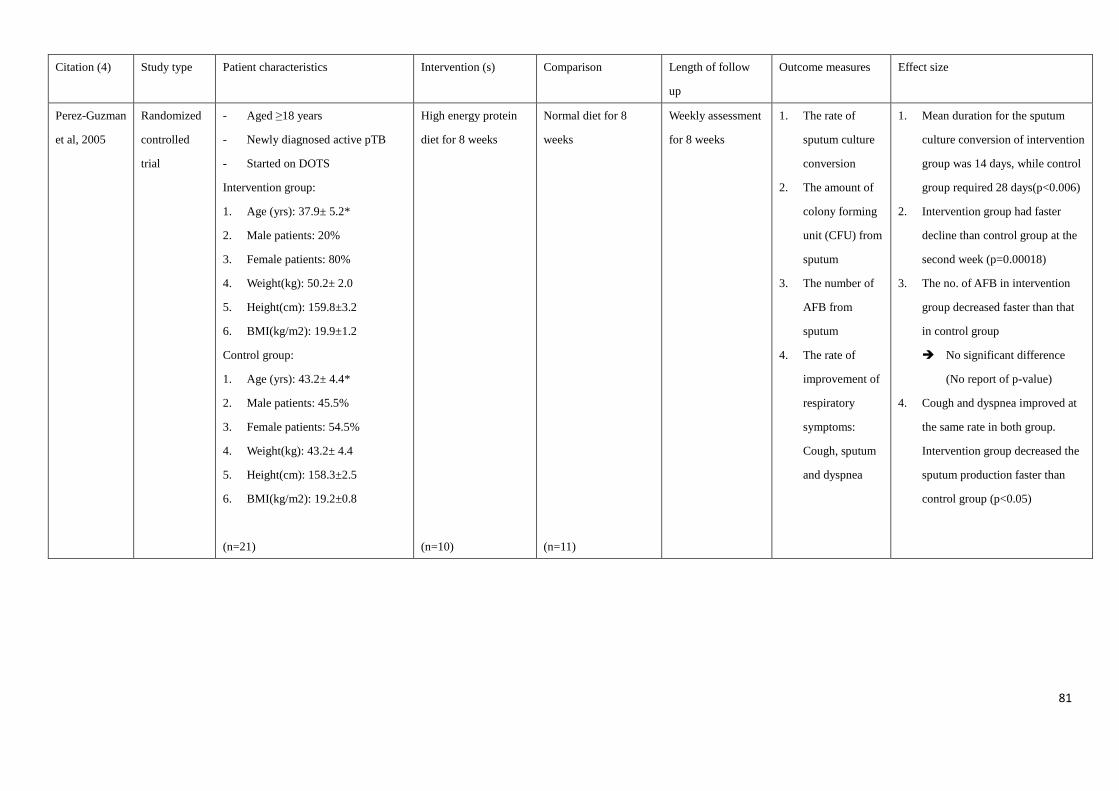
81
Citation (4) Study type Patient characteristics Intervention (s) Comparison Length of follow
up
Outcome measures Effect size
Perez-Guzman
et al, 2005
Randomized
controlled
trial
- Aged ≥18 years
- Newly diagnosed active pTB
- Started on DOTS
Intervention group:
1. Age (yrs): 37.9± 5.2*
2. Male patients: 20%
3. Female patients: 80%
4. Weight(kg): 50.2± 2.0
5. Height(cm): 159.8±3.2
6. BMI(kg/m2): 19.9±1.2
Control group:
1. Age (yrs): 43.2± 4.4*
2. Male patients: 45.5%
3. Female patients: 54.5%
4. Weight(kg): 43.2± 4.4
5. Height(cm): 158.3±2.5
6. BMI(kg/m2): 19.2±0.8
(n=21)
High energy protein
diet for 8 weeks
(n=10)
Normal diet for 8
weeks
(n=11)
Weekly assessment
for 8 weeks
1. The rate of
sputum culture
conversion
2. The amount of
colony forming
unit (CFU) from
sputum
3. The number of
AFB from
sputum
4. The rate of
improvement of
respiratory
symptoms:
Cough, sputum
and dyspnea
1. Mean duration for the sputum
culture conversion of intervention
group was 14 days, while control
group required 28 days(p<0.006)
2. Intervention group had faster
decline than control group at the
second week (p=0.00018)
3. The no. of AFB in intervention
group decreased faster than that
in control group
No significant difference
(No report of p-value)
4. Cough and dyspnea improved at
the same rate in both group.
Intervention group decreased the
sputum production faster than
control group (p<0.05)

82
Citation (5) Study type Patient characteristics Intervention (s) Comparison Length of follow up Outcome measures Effect size
PrayGod et al,
(2012)
Randomized
controlled
trial
- Aged ≥18 years
- Newly diagnosed or relapsed
active pTB
- Started on DOTS
- ± HIV infected
Intervention group:
1. Age (yrs): 34.7± 10.3*
2. Male patients: 50%
3. Female patients: 50%
4. BMI(kg/m2): 18.7 ± 2.9
5. BMI(kg/m2)<18.5: 51.6%
6. BMI(kg/m2)≥18.5: 48.4%
Control group:
1. Age (yrs): 36.2± 9.5*
2. Male patients: 51%
3. Female patients: 49%
4. BMI(kg/m2): 18.5 ± 2.8
5. BMI(kg/m2)<18.5: 56.4%
6. BMI(kg/m2)≥18.5: 43.6%
(n=377)
Six energy-protein
biscuit bars (totally
3690 kJ energy and
29g protein) daily for
two months
(n=189)
One energy-protein
biscuit bar daily for
two months
(n=188)
At the end of the
supplementation
period (2nd month)
and 5th month
Primary outcome:
1. Weight (kg)
Secondary
outcomes:
2. Arm fat area
(cm2)
3. Arm muscle
area (cm2)
4. Handgrip
strength (kg)
Intervention VS Control group
1. 2nd month:
Mean: +3.1 VS +2.8 (P=0.33)
5th month:
Mean: +6.4 VS +6.9 (P=0.75)
2. 2nd month:
Mean: +1.2 VS +1.4 (P=0.32)
5th month:
Mean: +3.3 VS +3.4 (P=0.66)
3. 2nd month:
Mean: +3.0 VS +2.3 (P=0.41)
5th month:
Mean: +6.6 VS +7.1 (P=0.63)
4. 2nd month:
Mean: +2.5 VS +2.5 (P=0.37)
5th month:
Mean: +6.3 VS +5.7 (P=0.07)
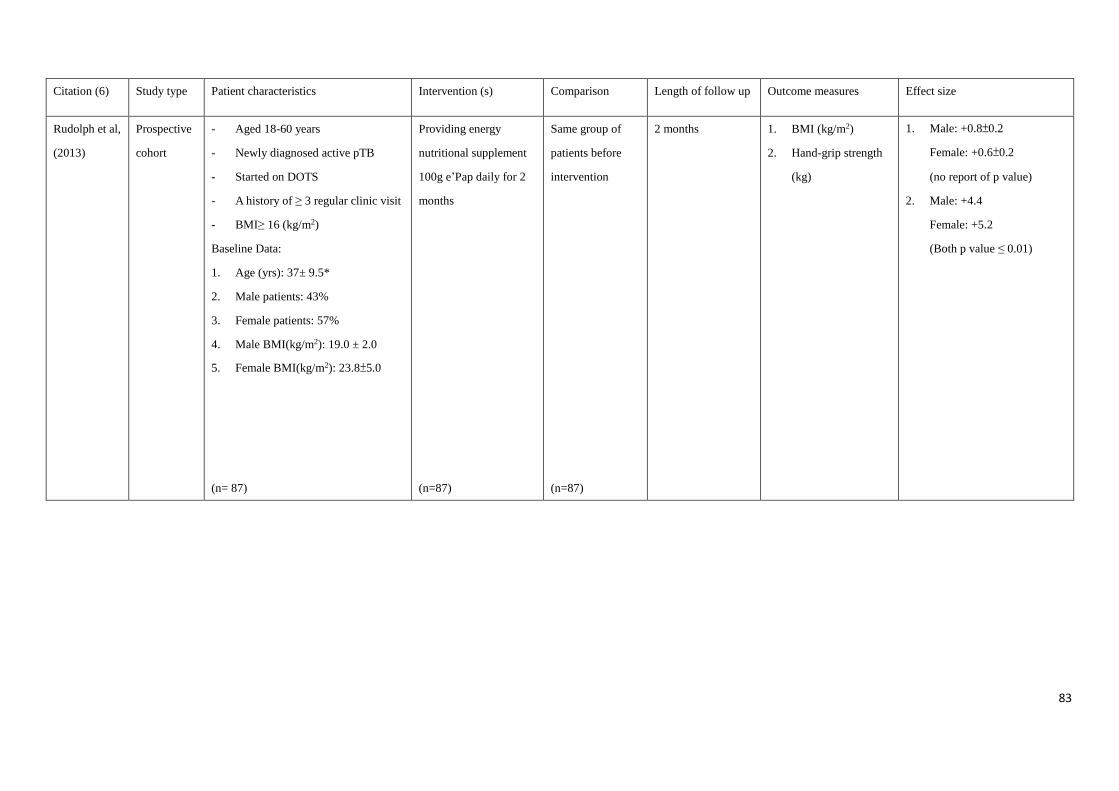
83
Citation (6) Study type Patient characteristics Intervention (s) Comparison Length of follow up Outcome measures Effect size
Rudolph et al,
(2013)
Prospective
cohort
- Aged 18-60 years
- Newly diagnosed active pTB
- Started on DOTS
- A history of ≥ 3 regular clinic visit
- BMI≥ 16 (kg/m2)
Baseline Data:
1. Age (yrs): 37± 9.5*
2. Male patients: 43%
3. Female patients: 57%
4. Male BMI(kg/m2): 19.0 ± 2.0
5. Female BMI(kg/m2): 23.8±5.0
(n= 87)
Providing energy
nutritional supplement
100g e’Pap daily for 2
months
(n=87)
Same group of
patients before
intervention
(n=87)
2 months 1. BMI (kg/m2)
2. Hand-grip strength
(kg)
1. Male: +0.8±0.2
Female: +0.6±0.2
(no report of p value)
2. Male: +4.4
Female: +5.2
(Both p value ≤ 0.01)

84
Appendix D: SIGN Critical Appraisals (Scottish Intercollegiate Guidelines Network,
2012)
Controlled Trials Checklist
Study identDification (1): Jahnavi, G., & Sudha, C. H. (2010). Randomised controlled trial of food supplement in patients with newly
diagnosed tuberculosis and wasting. Singapore medical Jounal, 51(12), 957-962.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and hypothesis
are clearly stated.
1.2 The assignment of subjects to treatment groups is randomised. Yes, but details of randomization
were not mentioned.
1.3 An adequate concealment method is used. Yes, patients were allocated by
drawing an opaque and sealed
envelope with respective group
stated.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No
1.5 The treatment and control groups are similar at the start of the trial. Yes, no significant differences
between groups were found.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes, measurements shown were
standard, valid and reliable.
1.8 What percentage of the individuals or clusters recruited into each treatment arm of
the study dropped out before the study was completed?
4%
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).
Yes, all subjects were
analyzed in their original group.
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.
Yes, study was carried out at 30
community centres
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (1+)

85
2.2 Taking into account clinical considerations, your evaluation
of the methodology used, and the statistical power of the
study, are you certain that the overall effect is due to the
study intervention?
No, power analysis was not used to calculate the
sample size.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes: Intake of food supplements can increase the body weight and physical function. Improvements were
observed in psychological, physiologically, socially and in the treatment outcomes.

86
Controlled Trials Checklist
Study identification (2): Paton, N. I., Chua, Y. K., Earnest, A., & Chee, C. B. E. (2004). Randomized controlled trial of nutritional
supplementation in patients with newly diagnosed tuberculosis and wasting. American Journal of Clinical Nutrition, 80(2), 460-465.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and hypothesis
are clearly stated.
1.2 The assignment of subjects to treatment groups is randomised. Yes, but details of randomization
were not mentioned.
1.3 An adequate concealment method is used. Yes, patients were allocated by
drawing an opaque and sealed
envelope with respective group
stated.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No
1.5 The treatment and control groups are similar at the start of the trial. Yes, no significant differences
between groups were found.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes, measurements shown were
standard, valid and reliable.
1.8 What percentage of the individuals or clusters recruited into each treatment arm of
the study dropped out before the study was completed?
5.6%
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).
Yes, all subjects were
analyzed in their original group.
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.
Does not apply, the study was carried
out at only one hospital.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (1+)
2.2 Taking into account clinical considerations, your evaluation
of the methodology used, and the statistical power of the
Yes, power analysis was used to calculate the
sample size.

87
study, are you certain that the overall effect is due to the
study intervention?
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Early nutritional intervention increases body weight, lean mass and physical function. Yet nutritional
intervention after the initial phase of TB treatment could be less beneficial as it mainly increases fat.
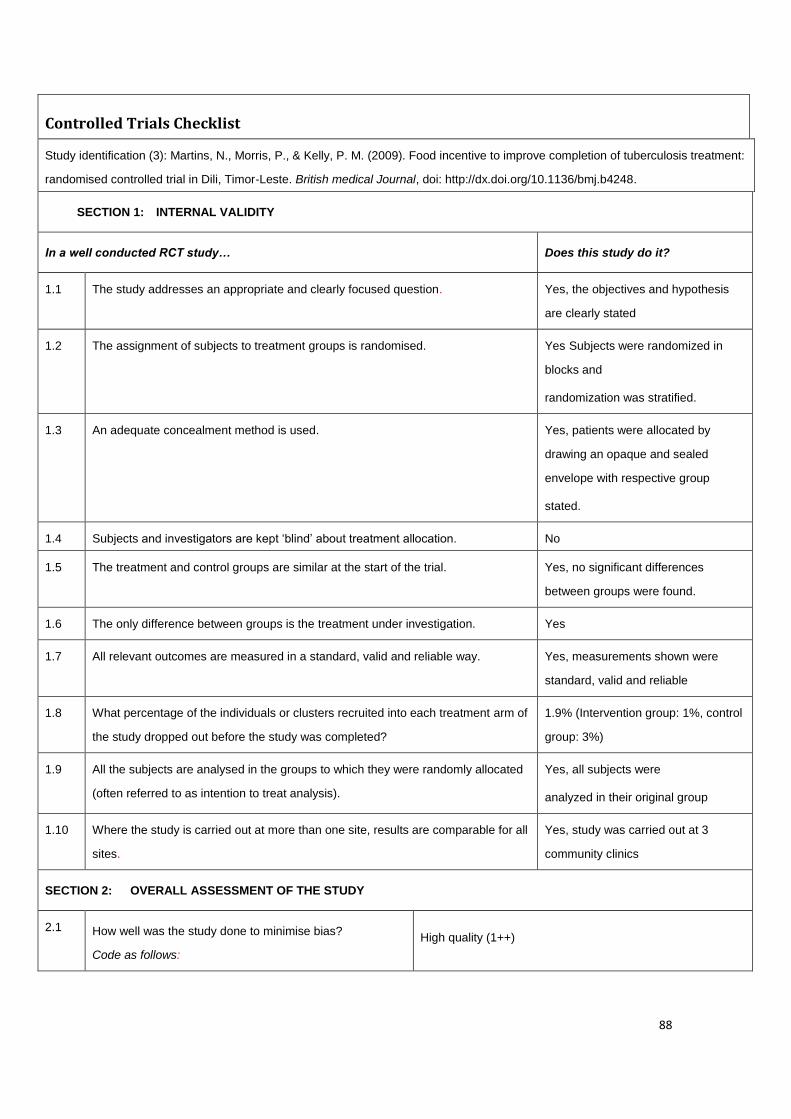
88
Controlled Trials Checklist
Study identification (3): Martins, N., Morris, P., & Kelly, P. M. (2009). Food incentive to improve completion of tuberculosis treatment:
randomised controlled trial in Dili, Timor-Leste. British medical Journal, doi: http://dx.doi.org/10.1136/bmj.b4248.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and hypothesis
are clearly stated
1.2 The assignment of subjects to treatment groups is randomised. Yes Subjects were randomized in
blocks and
randomization was stratified.
1.3 An adequate concealment method is used. Yes, patients were allocated by
drawing an opaque and sealed
envelope with respective group
stated.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No
1.5 The treatment and control groups are similar at the start of the trial. Yes, no significant differences
between groups were found.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes, measurements shown were
standard, valid and reliable
1.8 What percentage of the individuals or clusters recruited into each treatment arm of
the study dropped out before the study was completed?
1.9% (Intervention group: 1%, control
group: 3%)
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).
Yes, all subjects were
analyzed in their original group
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.
Yes, study was carried out at 3
community clinics
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (1++)
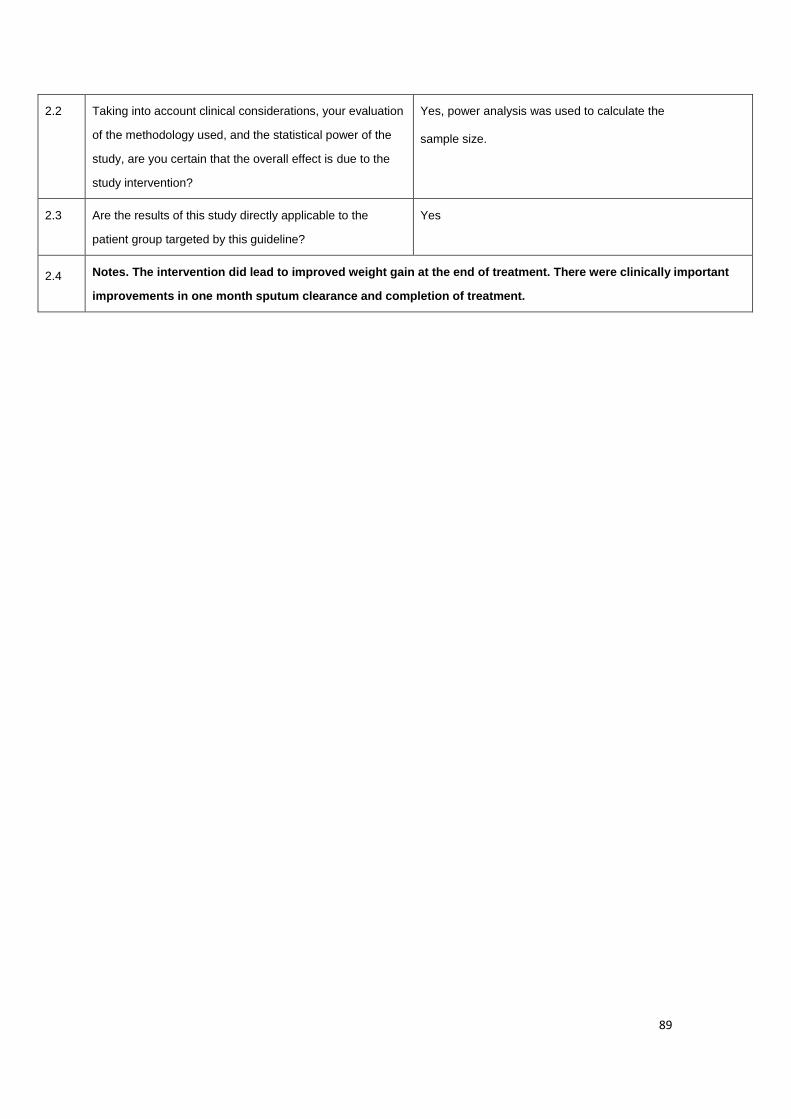
89
2.2 Taking into account clinical considerations, your evaluation
of the methodology used, and the statistical power of the
study, are you certain that the overall effect is due to the
study intervention?
Yes, power analysis was used to calculate the
sample size.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. The intervention did lead to improved weight gain at the end of treatment. There were clinically important
improvements in one month sputum clearance and completion of treatment.

90
Controlled Trials Checklist
Study identification (4): Perez-Guzman, C., Vargas, H. M., Quinonez, F., Bazavilvazo, N., & Aguilar, A. (2005). A Cholesterol-Rich
Diet accelerates bacteriologic sterilization in Pulmonary Tuberculosis. Chest, 127(2), 643-651.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and hypothesis
are clearly stated
1.2 The assignment of subjects to treatment groups is randomised. Yes, but details of randomization
were not mentioned.
1.3 An adequate concealment method is used. Not mentioned
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Double-Blinded
1.5 The treatment and control groups are similar at the start of the trial. Yes, no significant differences
between groups were found.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes, measurements shown were
standard, valid and reliable
1.8 What percentage of the individuals or clusters recruited into each treatment arm of
the study dropped out before the study was completed?
No drop out
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).
Yes, all subjects were
analyzed in their original group
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.
Does not apply, the study was carried
out at only one hospital.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (1+)
2.2 Taking into account clinical considerations, your evaluation
of the methodology used, and the statistical power of the
study, are you certain that the overall effect is due to the
study intervention?
No, power analysis was not used to calculate the
sample size.
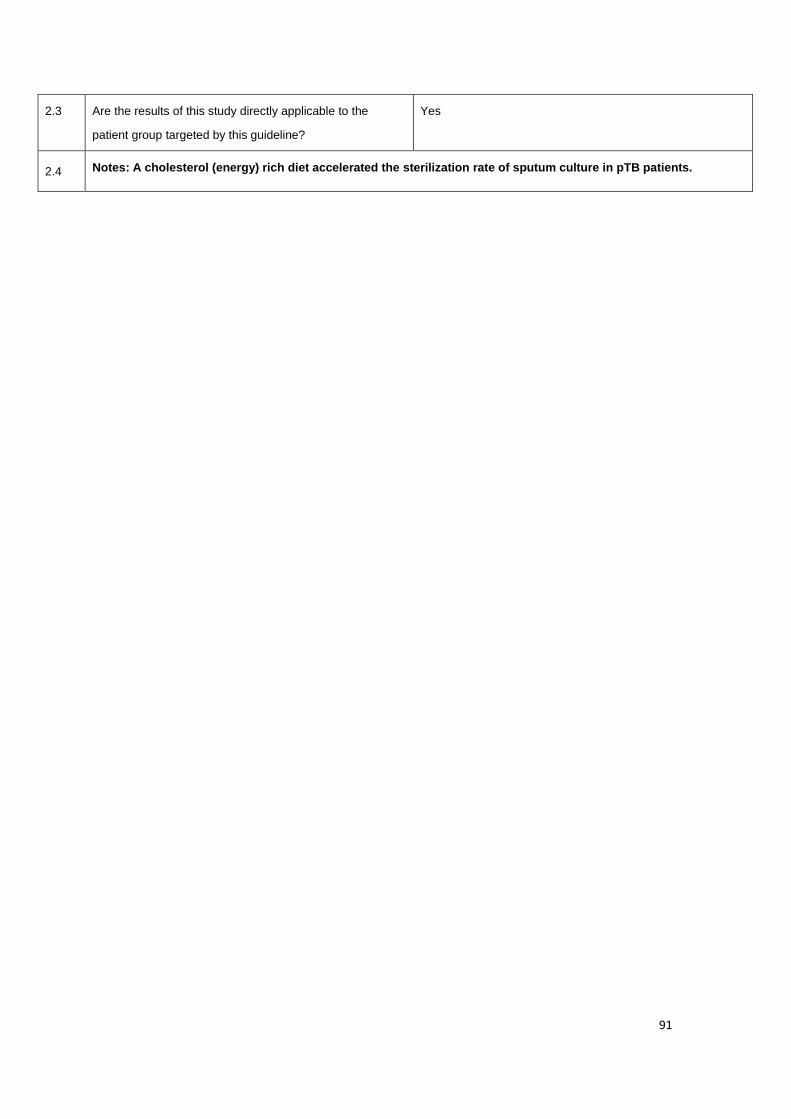
91
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes: A cholesterol (energy) rich diet accelerated the sterilization rate of sputum culture in pTB patients.

92
Controlled Trials Checklist
Study identification (5): PrayGod, G., Range, N., Faurholt-Jepsen, D., Jeremiah, K., Faurholt-Jepsen, M., Aabye, M. G., Jensen, L.,
Jensen, A., Grewal, H. M. S., Magnussen, P., Chanalucha, J., Andersen, A. B., & Friis, H. (2011). The effect if energy-protein
supplementation on weight, body composition and handgrip strength among pulmonary tuberculosis HIV-co-infected patient:
randomized controlled trial in Mwanza, Tanzania. British Journal of Nutrition, 107, 263-271.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and hypothesis
are clearly stated
1.2 The assignment of subjects to treatment groups is randomised. Yes Subjects were randomized in
blocks and
randomization was stratified.
1.3 An adequate concealment method is used. Yes, patients were allocated by
drawing an opaque and sealed
envelope with respective group
stated.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No
1.5 The treatment and control groups are similar at the start of the trial. Yes, no significant differences
between groups were found.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes, measurements shown were
standard, valid and reliable
1.8 What percentage of the individuals or clusters recruited into each treatment arm of
the study dropped out before the study was completed?
19.1%
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).
Yes, all subjects were
analyzed in their original group
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.
Yes, study was carried out at 3
community clinics
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
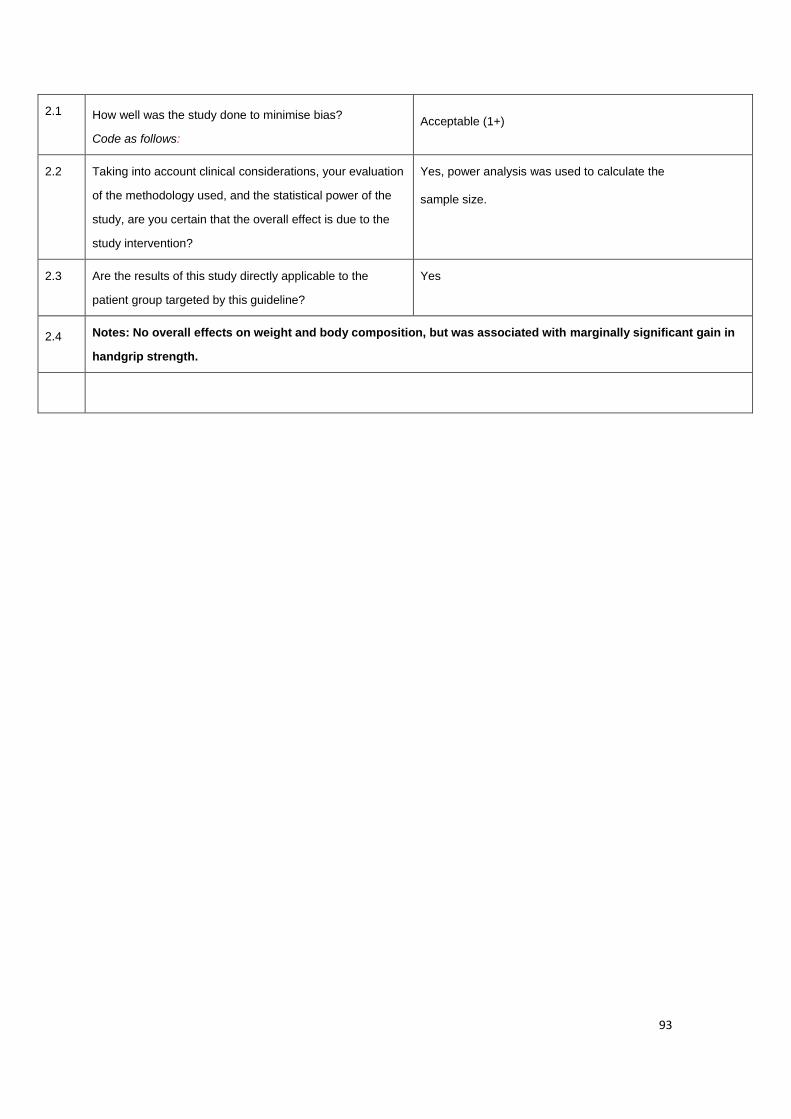
93
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (1+)
2.2 Taking into account clinical considerations, your evaluation
of the methodology used, and the statistical power of the
study, are you certain that the overall effect is due to the
study intervention?
Yes, power analysis was used to calculate the
sample size.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes: No overall effects on weight and body composition, but was associated with marginally significant gain in
handgrip strength.

94
Cohort studies Checklist
Study identification (6): Rudolph, M., Kroll, F., Beery., M., Marinda, E., Sobiecki, J. F., Douglas, G., & Orr, G. (2013). A Pilot study
Assessing the impact of a fortified supplementary food on the health and well-being of Creche children and adult TB patients in South
Africa. Plus one, 8(1), e55544. doi: 10.1371/journal.pone.0055544.
SECTION 1: INTERNAL VALIDITY
In a well conducted cohort study: Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes, the objectives and
hypothesis are clearly stated
SELECTION OF SUBJECTS
1.2 The two groups being studied are selected from source populations that are comparable in all
respects other than the factor under investigation.
Does not apply, there was no
comparison group.
1.3 The study indicates how many of the people asked to take part did so, in each of the groups
being studied.
Does not apply, there was no
comparison group.
1.4 The likelihood that some eligible subjects might have the outcome at the time of enrolment is
assessed and taken into account in the analysis.
No
1.5 What percentage of individuals or clusters recruited into each arm of the study dropped out
before the study was completed.
6.9%
1.6 Comparison is made between full participants and those lost to follow up, by exposure status. Does not apply there was
a single group study.
ASSESSMENT
1.7 The outcomes are clearly defined. Yes, the outcomes were
clearly specified and used in
the analysis.
1.8 The assessment of outcome is made blind to exposure status. If the study is retrospective
this may not be applicable.
Does not apply, there was
only one group
1.9 Where blinding was not possible, there is some recognition that knowledge of exposure
status could have influenced the assessment of outcome.
Yes

95
1.10 The method of assessment of exposure is reliable. Yes, measures used were
clearly defined
1.11 Evidence from other sources is used to demonstrate that the method of outcome assessment
is valid and reliable.
Yes, measures were
subjective and reliable.
1.12 Exposure level or prognostic factor is assessed more than once. Yes, it assessed twice
CONFOUNDING
1.13 The main potential confounders are identified and taken into account in the design and
analysis.
Yes
STATISTICAL ANALYSIS
1.14 Have confidence intervals been provided? Yes, 95% confidence
intervals
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise the risk of bias or confounding? Acceptable (2+)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the
statistical power of the study, do you think there is clear evidence of an association between
exposure and outcome?
Yes
2.3 Are the results of this study directly applicable to the patient group targeted in this guideline? Yes
2.4 Notes: There was a beneficial effect of e’Pap’ for adult TB patients. There is evidence to suggest statically
significant improvements in key micronutrient levels, well-being and energy, hand-grip strength.
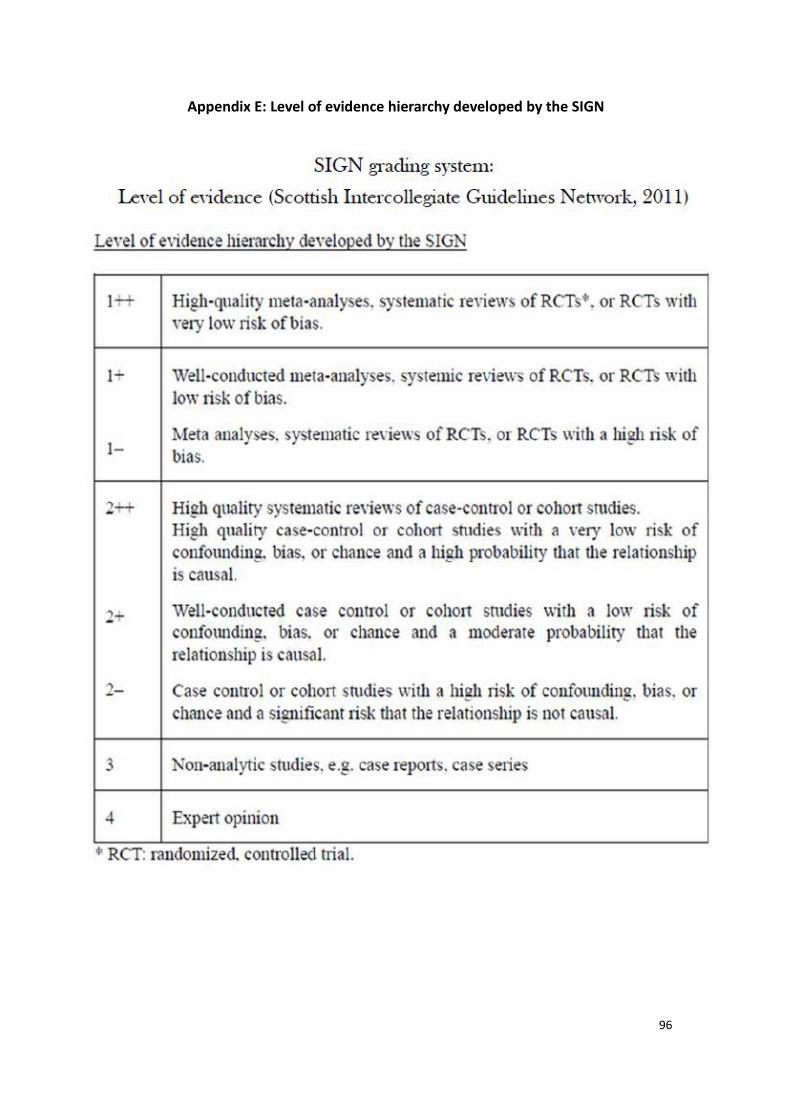
96
Appendix E: Level of evidence hierarchy developed by the SIGN

97
Appendix F: Assessment form of Target TB patient
An evidence-based
energy-protein dietary
program assessment form
Patient’s Gym Label
Medical Background:
Diagnosis:
__________________________________________________________________
Past History:
___________________________________________________________________
___________________________________________________________________
Current anti-TB antibiotics:
___________________________________________________________________
___________________________________________________________________
Measurements:
Week 0
Date: ______________
Body Weight: _________________
Body Height: _________________
BMI: _______________________
Handgrip Strength: _____________
Lean Mass: ___________________
Week 1
Date: ______________
Body Weight: ________________
Body Height: _________________
BMI: ____________________
Handgrip Strength: _____________
Lean Mass: ___________________
Week 2
Date: ______________
Body Weight: ________________
Body Height: _________________
BMI: ________________________
Handgrip Strength: _____________
Lean Mass: ___________________
Week 3
Date: ______________
Body Weight: ________________
Body Height: ________________
BMI: _______________________
Handgrip Strength: _____________
Lean Mass: ___________________

98
Performed by:
Name & Signature: _________________________
Rank: __________________
Date: __________________
Date of 1st positive AFB result / TB Sputum Culture: ___________
Date of 1st negative AFB result / TB Sputum Culture: ___________
Feeding method: ⃣ Oral ⃣ NG tube ⃣ TPN
Eligible for the “High energy-protein dietary program”
⃣ Yes ⃣ No
Selected food product:
⃣ Ensure (Vanilla/ Chocolate) 250ml -- 2 cans/day
⃣ Nutrition Vanilla Almond Crunch Protein Bar -- 2 bars/day

99
Appendix G: The content of the program briefing session
Items Duration Speakers Target participants
Literature Review 10 mins Investigator –
Advance Practice
Nurse (APN)
Registered Nurses
Program Introduction 25 mins
Question and Answer 10 mins
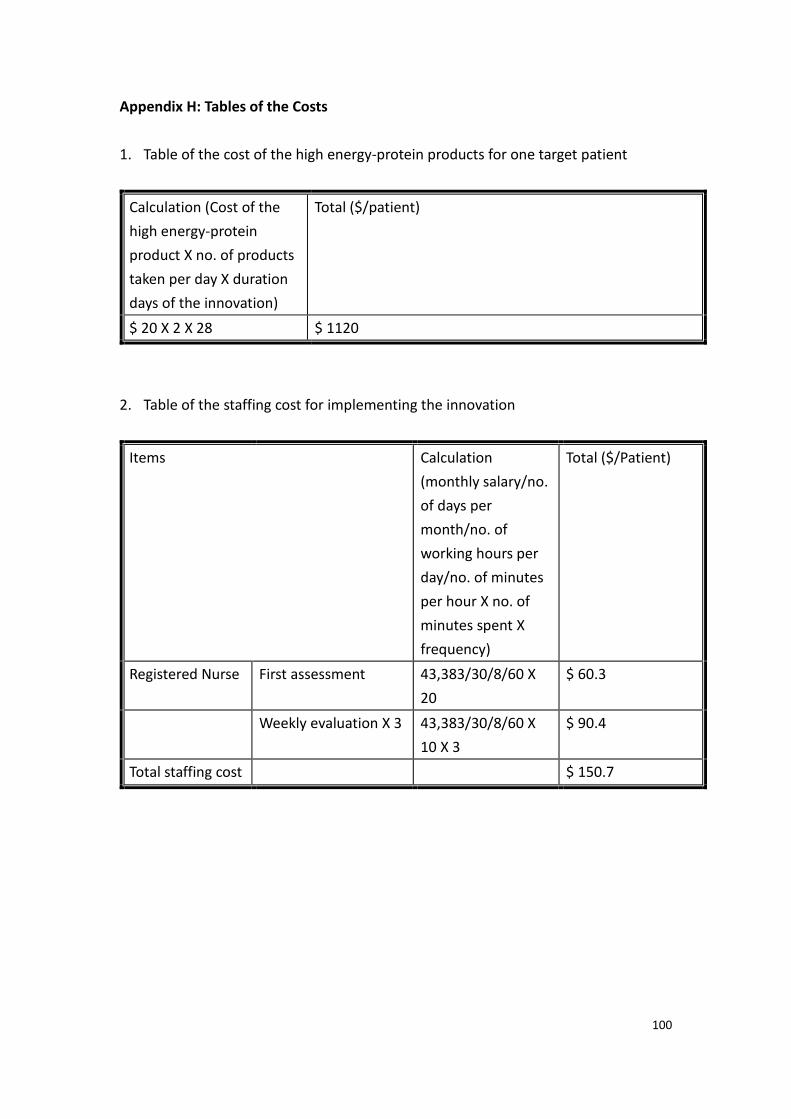
100
Appendix H: Tables of the Costs
1. Table of the cost of the high energy-protein products for one target patient
Calculation (Cost of the
high energy-protein
product X no. of products
taken per day X duration
days of the innovation)
Total ($/patient)
$ 20 X 2 X 28 $ 1120
2. Table of the staffing cost for implementing the innovation
Items Calculation
(monthly salary/no.
of days per
month/no. of
working hours per
day/no. of minutes
per hour X no. of
minutes spent X
frequency)
Total ($/Patient)
Registered Nurse First assessment 43,383/30/8/60 X
20
$ 60.3
Weekly evaluation X 3 43,383/30/8/60 X
10 X 3
$ 90.4
Total staffing cost $ 150.7

101
3. Table of the extra hospitalization cost of one target patient without receiving the
innovation
Calculation (Operating cost of an
isolation room X days of hospitalization)
Total ($/patient)
$4860 X 14 $68040

102
Appendix I: Table of the operation cost of the two program briefing sessions
Items Calculation
(monthly salary/no/of days per
month/no. of working hours per
day/no. of minutes per hour X no. of
minutes spent X no. of participants)
Subtotal ($)
Investigator(n=1) $ 57,275/30/8/60 X 90 $ 358.0
Registered Nurse
(n=22)
$ 43,383/30/8/60 X 45 X 22 $ 2982.6
Accommodation Free
IT equipment Free
Stationary Free
Total training cost $ 3340.6

103
Appendix J: SIGN 50: A guideline developer’s handbook

104
Appendix K: Nursing Procedure Audit Form for Evidence-
based energy-protein dietary program
*Please circle the appropriate source of information and tick as appropriate
Standard criteria Source of information Yes No N/A Remarks
Patient recruitment
1 Assess the body measurements
and physical function for every
newly diagnosed TB patients with
dedicated assessment form.
N / P / O / R
2 Complete all the items in the
assessment form accurately.
N / P / O / R
3 Include patients fulfilling the
recruitment criteria only.
N / P / O / R
4 Provide program introduction to
every eligible case.
N / P / O / R
5 Obtain written informed consent
before implementation.
N / P / O / R
Intervention
6 Serve the selected food product
according to the instruction.
N / P / O / R
Evaluation
7 Record all relevant data timely,
accurately and appropriately.
N / P / O / R
*Remarks: N: Nurse P: Patient O: Observation R: Record N/A: Not applicable
Ward: _________
Percentage of compliance: / 8= %
Name & Signature of auditor: _______________________
Date: ____________________

105
Appendix L: Nurse Satisfaction Survey for Evidence-based
energy-protein dietary program Questionnaire
Date: ________________ Name & Rank: ___________________
*Please circle the appropriate rating for the following aspects of the program
Item
No.
Strongly
disagree
Disagree Slightly
disagree
Slightly
agree
Agree Strongly
agree
1 The program has achieved
as stated objectives.
1 2 3 4 5 6
2 The information provided
in the briefing session is
clear, adequate and useful.
1 2 3 4 5 6
3 The tools for patients
assessment and outcome
measurement are
understandable and easy to
use
1 2 3 4 5 6
4 The workflow of the
program is reasonable and
acceptable.
1 2 3 4 5 6
5 The program can
effectively cut down
nursing workload in TB
patients
1 2 3 4 5 6
6 You are satisfied with the
program as a whole.
1 2 3 4 5 6
7. Which part of the program is most difficult to be operated? Why?
_____________________________________________________________________

106
_____________________________________________________________________
8. What additional patient information you would you like to be included in the
program?
_____________________________________________________________________
_____________________________________________________________________
9. Which area of the program could be further improved in the future any suggestion?
_____________________________________________________________________
_____________________________________________________________________

107
Appendix M: Patient Satisfaction Survey for Evidence-based
energy-protein dietary program
Questionnaire
Date: _____________ Name (Surname only): ____________________
*Please circle the appropriate rating for the following aspects of the program
Item
No.
Strongly
disagree
Disagree Slightly
disagree
Slightly
agree
Agree Strongly
agree
1 The program is useful to
improve nutritional status.
1 2 3 4 5 6
2 The program can make
you feel good during
infection period.
1 2 3 4 5 6
3 The food product is tasty
and acceptable.
1 2 3 4 5 6
4 The adverse effects of oral
supplement are minimal
and tolerated.
1 2 3 4 5 6
5 You will continue the
recommended diet at
home after discharge
1 2 3 4 5 6
6 You are satisfied with the
program as a whole.
1 2 3 4 5 6

108
Appendix N: Timeframe for the implementation of Evidence-based energy-protein dietary program
Tasks weeks
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Seek for approval from management level
Gain support from health care providers
Train the program coordinators
Conduct a pilot study of the proposed innovation
Amend the full-scale program as indicated
Implementation of energy-protein oral supplement program
Evaluation: Patient outcomes
Evaluation: Healthcare provider outcomes
Evaluation: System outcomes

109