access to health care for transgender patients asilomar faculty development conference october 3-6,...
TRANSCRIPT

Access to Health Care Access to Health Care for Transgender for Transgender
PatientsPatientsAsilomar Faculty Development ConferenceAsilomar Faculty Development Conference
October 3-6, 2004October 3-6, 2004
Sponsored by the Pacific AIDS Sponsored by the Pacific AIDS Education and Training CenterEducation and Training Center
Samuel LurieSamuel Lurie
www.tgtrain.orgwww.tgtrain.org

*Face-to-face informant interviews with providers around New England, f*Face-to-face informant interviews with providers around New England, funded with support of New England AIDS Education and Training Centerunded with support of New England AIDS Education and Training Center
Training Study FindingsTraining Study Findings2001-2002 Needs Assessment of 2001-2002 Needs Assessment of Healthcare Providers Showed*Healthcare Providers Showed*
Experience with a range of transgendered Experience with a range of transgendered expressions but lack of information on populations, expressions but lack of information on populations, terminology, differencesterminology, differences
Desire to treat TG patients respectfully but admitted Desire to treat TG patients respectfully but admitted discomfort and lack of tools for specific discomfort and lack of tools for specific interviewing/assessments.interviewing/assessments.
Concern and frustration with lack of information, Concern and frustration with lack of information, studies and researchstudies and research
*Face-to-face informant interviews with providers around New England, f*Face-to-face informant interviews with providers around New England, funded with support of New England AIDS Education and Training Centerunded with support of New England AIDS Education and Training Center
Training Study Findings (2)Training Study Findings (2)2001-2002 Needs Assessment of 2001-2002 Needs Assessment of Health Care Providers Showed*Health Care Providers Showed*
Concern and frustration with lack of treatment Concern and frustration with lack of treatment guidelines, referral contacts and ways to advocate guidelines, referral contacts and ways to advocate for transgender clients.for transgender clients.
Time constraints create an overarching barrier in Time constraints create an overarching barrier in building trusting relationships with clients, and building trusting relationships with clients, and trusting relationships are integral to quality care trusting relationships are integral to quality care


Four Steps to Providing Four Steps to Providing CareCare
1)1) Understand Understand rangerange of gender expressions of gender expressions and differences in desire for and access to and differences in desire for and access to surgical or hormonal interventions.surgical or hormonal interventions.
2)2) Recognize Recognize distinctionsdistinctions between gender between gender identity and sexual orientation and identity and sexual orientation and understand differences (and similarities) in understand differences (and similarities) in health care delivery needs.health care delivery needs.
3)3) Understand Understand access to careaccess to care is affected by is affected by negative experiences with providers and negative experiences with providers and role providers can play in improving role providers can play in improving quality of life for trans people.quality of life for trans people.
4)4) Making Making agenciesagencies more trans-friendly more trans-friendly
Recognize Range of Recognize Range of Expressions and DesiresExpressions and Desires
Terms:Terms: Transgender vs. Transgender vs.
TransexualTransexual FTM, TransmanFTM, Transman MTF, TranswomanMTF, Transwoman HormonesHormones
Pre-op, post-op, non-Pre-op, post-op, non-opop
IntersexIntersex Transition, SOFFATransition, SOFFA Read, clock, passRead, clock, pass
Many words to identify gender-variance, Many words to identify gender-variance, including:including:MTF, FTM, transman, transwoman, bi-gendered, MTF, FTM, transman, transwoman, bi-gendered, gender-blender, phallic woman, passing man, she-gender-blender, phallic woman, passing man, she-male, femme queen, non-op, boi, two-spirit, new male, femme queen, non-op, boi, two-spirit, new man, new woman, etc.man, new woman, etc.

Hormones OverviewHormones Overview Masculinizing hormones work much Masculinizing hormones work much
faster and more thoroughly than faster and more thoroughly than feminizing hormones. A few months feminizing hormones. A few months vs. a few years.vs. a few years.
Effects: change in body shape, facial Effects: change in body shape, facial and body hair, sex drive, emotions. and body hair, sex drive, emotions.
Maintenance of taking hormones is Maintenance of taking hormones is diagnostic of need for hormones. If not diagnostic of need for hormones. If not right, client will stop taking them.right, client will stop taking them.
Not a lot of studies; off-label usage.Not a lot of studies; off-label usage.

Range of Expressions Range of Expressions (continued)(continued)
Identities can and do changeIdentities can and do change, based on , based on context, culture, geography, and context, culture, geography, and individual’s place on their life journeyindividual’s place on their life journey
Hormones and surgical interventions may Hormones and surgical interventions may be desired in an order or degree other be desired in an order or degree other than what protocols dictate. than what protocols dictate.
Watch for pathologizing/medicalizing Watch for pathologizing/medicalizing situation (even words like “pre-op” and situation (even words like “pre-op” and “post-op” assume ““post-op” assume “opop” as final outcome. ” as final outcome. Also, emphasis is on genitals, not person.)Also, emphasis is on genitals, not person.)

Gender Identity and Sexual Gender Identity and Sexual Orientation are Different ThingsOrientation are Different Things Every individual has a biological sex, a Every individual has a biological sex, a
gender identity and a sexual orientation. gender identity and a sexual orientation. – All can be considered fluid. All can be considered fluid.
But being transgendered does not mean But being transgendered does not mean you’re gay and being gay does not mean you’re gay and being gay does not mean you’re transgendered. you’re transgendered.
– There is overlap, in part because gender variance There is overlap, in part because gender variance is often seen in gay context. is often seen in gay context.
– Masculine females and feminine males are Masculine females and feminine males are assumedassumedto be gay; to be gay;
– ““anti-gay” discrimination and violence often anti-gay” discrimination and violence often targets targets gender expression, not sexualitygender expression, not sexuality
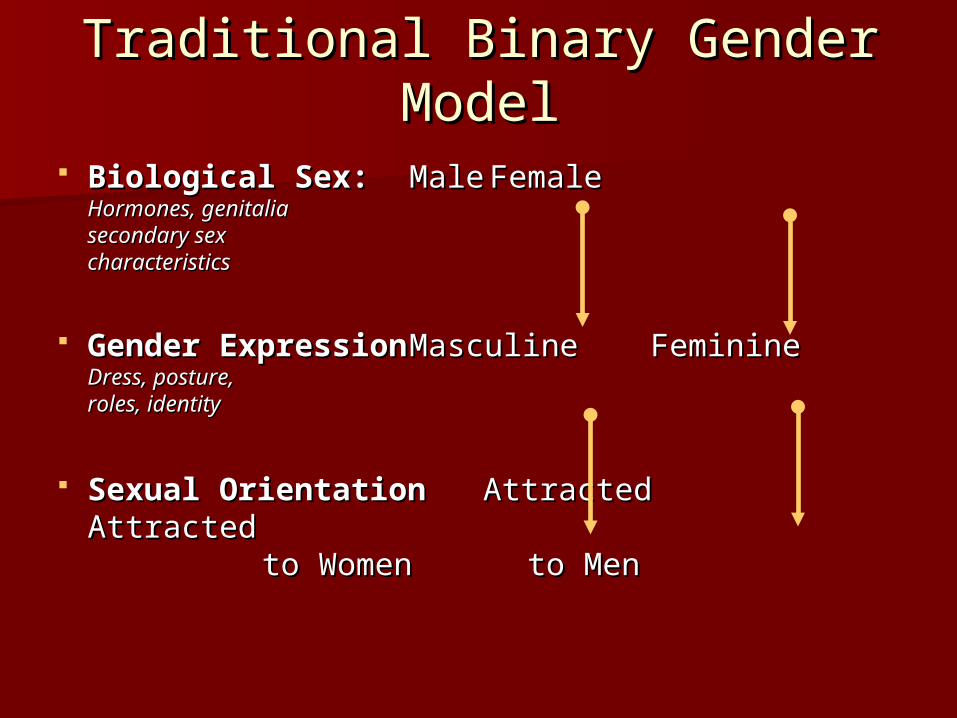
Traditional Binary Gender Traditional Binary Gender ModelModel
Biological Sex:Biological Sex: MaleMale FemaleFemaleHormones, genitaliaHormones, genitaliasecondary sex secondary sex characteristicscharacteristics
Gender ExpressionGender Expression MasculineMasculine FeminineFeminineDress, posture, Dress, posture, roles, identityroles, identity
Sexual Orientation Sexual Orientation AttractedAttracted AttractedAttracted to Women to Women to Men to Men

Revolutionary Gender ModelRevolutionary Gender Model
Biological Sex:Biological Sex: MaleMale IntersexedIntersexed FemaleFemaleHormones, genitaliaHormones, genitaliasecondary sex secondary sex characteristicscharacteristics
Gender ExpressionGender Expression Masculine Androgynous Masculine Androgynous FeminineFeminineDress, posture, Dress, posture, roles, identityroles, identity
Sexual OrientationSexual OrientationAttracted to:Attracted to: women men both neither women men both neither
other other

Revolutionary Gender ModelRevolutionary Gender ModelMany configurations are possibleMany configurations are possible
Biological Sex:Biological Sex: MaleMale IntersexIntersex FemaleFemaleHormones, genitaliaHormones, genitaliasecondary sex secondary sex characteristicscharacteristics
Gender ExpressionGender Expression Masculine Androgynous FeminineMasculine Androgynous FeminineDress, posture, Dress, posture, roles, identityroles, identity
Sexual OrientationSexual OrientationAttracted to:Attracted to: women men both neither otherwomen men both neither other
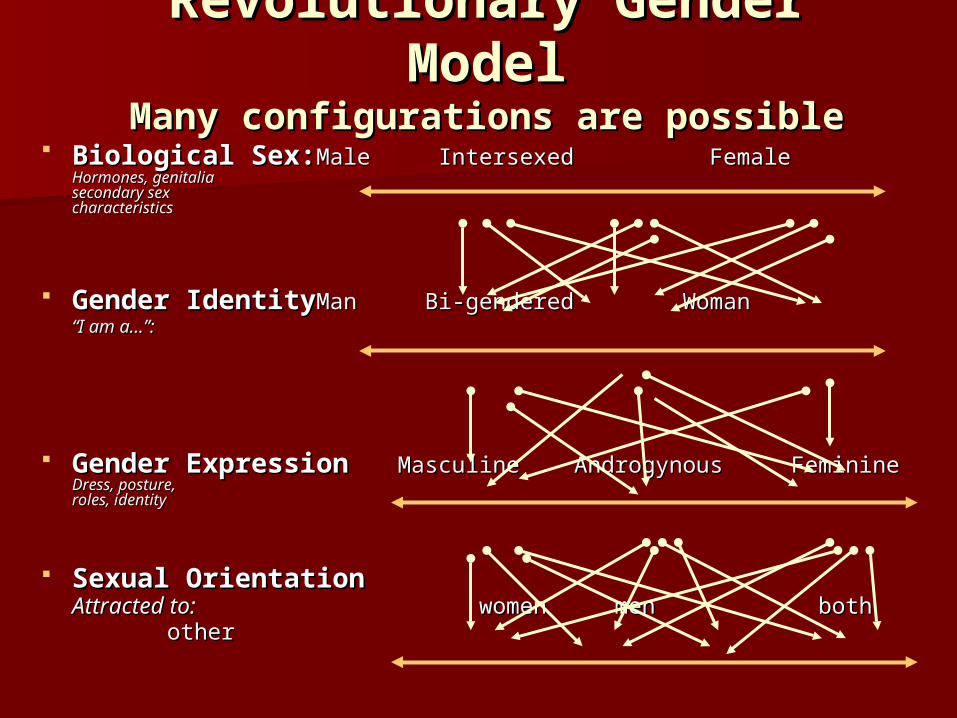
Revolutionary Gender Revolutionary Gender ModelModel
Many configurations are possibleMany configurations are possible Biological Sex:Biological Sex: MaleMale Intersexed Intersexed Female Female
Hormones, genitaliaHormones, genitaliasecondary sex secondary sex characteristicscharacteristics
Gender IdentityGender Identity ManMan Bi-gendered Woman Bi-gendered Woman ““I am a…”:I am a…”:
Gender ExpressionGender Expression Masculine Androgynous FeminineMasculine Androgynous FeminineDress, posture, Dress, posture, roles, identityroles, identity
Sexual OrientationSexual OrientationAttracted to:Attracted to: women men both women men both other other
RemindersReminders
Homophobia is different than Homophobia is different than TransphobiaTransphobia
Trans people are often outcast in G/L Trans people are often outcast in G/L context.context.
Pfc. Barry Winchell Pfc. Barry Winchell

Calpernia AdamsPhotos from her website at www.calpernia.com

Risks and NeedRisks and Need Not many studies, but all show painfully Not many studies, but all show painfully
high rates of HIV infectionhigh rates of HIV infection– From 22% in recent LA Study to 68% in 1993 From 22% in recent LA Study to 68% in 1993
study in Atlantastudy in Atlanta 35% in SF MTFs; 63% African-American 35% in SF MTFs; 63% African-American
MTFs MTFs (Clements-Nolle, Am. Journal of Public Health, June 2001)(Clements-Nolle, Am. Journal of Public Health, June 2001)
Often people don’t know they are Often people don’t know they are infected, or have no access to careinfected, or have no access to care– In SF study, 50% of those who knew status, not In SF study, 50% of those who knew status, not
receiving carereceiving care
CDC places TG people in MSM category CDC places TG people in MSM category for funding and prevention programsfor funding and prevention programs

Barriers to Care and TreatmentBarriers to Care and Treatment
Providers lack basic knowledge and have discomfortProviders lack basic knowledge and have discomfort Lack of research and informationLack of research and information Topic still derided by other professionalsTopic still derided by other professionals Not enough people doing the workNot enough people doing the work Extensive negative experiences with health careExtensive negative experiences with health care Medicalization and Pathologizing of Experience-Medicalization and Pathologizing of Experience-
judgmental, patronizing and humiliating treatmentjudgmental, patronizing and humiliating treatment In-take forms, office environment, alienating processIn-take forms, office environment, alienating process Insurance issues and long waiting listsInsurance issues and long waiting lists Workers and agencies come from a deficit Workers and agencies come from a deficit
perspectiveperspective

Trans LossesTrans Losses
Tyra Tyra HunterHunter
Photo by Mariette Pathy Allen
Robert Robert EadsEads
Billy Billy TiptonTipton
Photos from Remembering Our Dead, Photos from Remembering Our Dead, www.gender.org/rememberwww.gender.org/rememberAnd Transsexual, Transgender and Intersexed History, And Transsexual, Transgender and Intersexed History,
www.transhistory.org www.transhistory.org
Alexander John Alexander John GoodrumGoodrum
Protocols for HTProtocols for HT HBIGDA/Harry Benjamin Standards of HBIGDA/Harry Benjamin Standards of
Care: (Care: (www.hbigda.orgwww.hbigda.org))
Eligibility Criteria for Hormone TherapyEligibility Criteria for Hormone Therapy 1. 1. 18 years or older18 years or older 2.2. Demonstrable knowledge of social and medical risks and Demonstrable knowledge of social and medical risks and
benefits of hormonesbenefits of hormones 3. Either3. Either
A. Documented real life experience for at least 3 months A. Documented real life experience for at least 3 months or or B. Psychotherapy for at least 3 monthsB. Psychotherapy for at least 3 months
Readiness Criteria for Hormone TherapyReadiness Criteria for Hormone Therapy Real life experience or psychotherapy to further consolidate Real life experience or psychotherapy to further consolidate
gender identitygender identity Progress has been made toward the elimination of barriers to Progress has been made toward the elimination of barriers to
emotional well being and mental healthemotional well being and mental health Hormones are likely to be taken in a responsible mannerHormones are likely to be taken in a responsible manner

*San Francisco clinic incorporating hormone therapy as part of primary c*San Francisco clinic incorporating hormone therapy as part of primary care for low-income, homeless and at-risk people.are for low-income, homeless and at-risk people.
Initial Visits for Both:Initial Visits for Both:
Review history of gender experienceReview history of gender experience Document prior hormone useDocument prior hormone use Obtain sexual historyObtain sexual history Review patient goals Review patient goals Address safety concernsAddress safety concerns Assess social support systemAssess social support system Assess readiness for gender transitionAssess readiness for gender transition Review risks and benefits of hormone therapyReview risks and benefits of hormone therapy Obtain informed consentObtain informed consent Order screening laboratory studiesOrder screening laboratory studies Provide referralsProvide referrals
See Lori Kohler’s “Primary Care for Transgendered Patients” for information on drug See Lori Kohler’s “Primary Care for Transgendered Patients” for information on drug interactions and testsinteractions and tests..
Tom Waddell Clinic Protocols for CareTom Waddell Clinic Protocols for Care**

Agency-related issues to provide Agency-related issues to provide servicesservices
Don’t just add “T” without doing work to understand Don’t just add “T” without doing work to understand what it meanswhat it means
Train Train allall staff--receptionists, security guards, director staff--receptionists, security guards, director Make in-take forms trans friendly, i.e. include Make in-take forms trans friendly, i.e. include
“chosen name” not just legal name; include more “chosen name” not just legal name; include more than M/Fthan M/F
Don’t make assumptions about sexuality or goalsDon’t make assumptions about sexuality or goals Respect confidentiality, choices and Respect confidentiality, choices and fluidityfluidity Honor presenting gender and self-diagnosisHonor presenting gender and self-diagnosis Acknowledge limitationsAcknowledge limitations Challenge transphobia—in staff Challenge transphobia—in staff andand community community Have Unisex bathrooms!Have Unisex bathrooms!

Dr. Lori Kohler’s summaryDr. Lori Kohler’s summary
All trans people are medically All trans people are medically underservedunderserved
Hormone treatment is not optionalHormone treatment is not optional Providers who treat HIV disease have Providers who treat HIV disease have
unique opportunity to improve medical unique opportunity to improve medical care for trans peoplecare for trans people
While there are many unanswered While there are many unanswered questions about long-term effects, questions about long-term effects, benefits outweigh the risks for most benefits outweigh the risks for most patients.patients.
JoyJoy
“Working with someone going through
a gender transition is a joyous part
of medicine. It’s very similar to
feelings obstetricians have about
facilitating birth.”
-Edward Cheslow, MD

ResourcesResources Protocols for Hormonal Reassignment of GenderProtocols for Hormonal Reassignment of Gender from the from the
Tom Waddell Health Center, 2001, Tom Waddell Health Center, 2001, http://hivinsite.ucsf.edu/InSite.jsp?doc=2098.3d5ahttp://hivinsite.ucsf.edu/InSite.jsp?doc=2098.3d5a
Harry Benjamin International Gender Dysphoria Association Harry Benjamin International Gender Dysphoria Association (February 20, 2001). (February 20, 2001). Standards of Care for Gender Identity Standards of Care for Gender Identity Disorders,Disorders, Sixth Version Sixth Version. . http://www.hbigda.org/socv6.htmlhttp://www.hbigda.org/socv6.html
Oriel, K. A. (2000). Oriel, K. A. (2000). Medical care of transsexual patientsMedical care of transsexual patients. . Journal of the Gay and Lesbian Medical AssociationJournal of the Gay and Lesbian Medical Association 4(4): 185-193 4(4): 185-193
Post, P, (2002), Post, P, (2002), Crossing to Safety: Transgender Health and Crossing to Safety: Transgender Health and HomelessnessHomelessness,, Healing Hands: A publication of the Health Care Healing Hands: A publication of the Health Care for the Homeless Clinician’s Networkfor the Homeless Clinician’s Network, 6 (4), June 2002. , 6 (4), June 2002. http://www.nhchc.org/Network/HealingHands/2002/June2002Healihttp://www.nhchc.org/Network/HealingHands/2002/June2002HealingHands.pdfngHands.pdf
Bockting, W and Kirk S, editors, Bockting, W and Kirk S, editors, Transgender and HIV: Risks, Transgender and HIV: Risks, prevention and careprevention and care.. Bringhamton, NY: The Haworth Press Bringhamton, NY: The Haworth Press (2001) Originally published as a special issue of (2001) Originally published as a special issue of International International Journal of Trangenderism 3.1+2Journal of Trangenderism 3.1+2. Available online at . Available online at http://www.symposion/ijthttp://www.symposion/ijt

Resources (2)Resources (2) Clements-Nolle, K., Marx, R., Guzman, R., & Katz, M. (2001, June). Clements-Nolle, K., Marx, R., Guzman, R., & Katz, M. (2001, June).
“HIV prevalence, risk behaviors, health care use, and “HIV prevalence, risk behaviors, health care use, and mental health status of transgender persons: implications mental health status of transgender persons: implications for public health intervention.”for public health intervention.” American Journal of Public American Journal of Public Health, 91(6),Health, 91(6), 915-921. 915-921.
Keatley, J and Clements-Nolle, K. Keatley, J and Clements-Nolle, K. Factsheet: What are the Factsheet: What are the Prevention Needs of Male-to-Female Transgender Persons?Prevention Needs of Male-to-Female Transgender Persons? University of California, San Francisco, Center for AIDS Prevention University of California, San Francisco, Center for AIDS Prevention Studies, (2001) Studies, (2001) (English and Spanish versions) (English and Spanish versions) www.caps.ucsf.eduwww.caps.ucsf.edu
Gender Identity 101: A Transgender PrimerGender Identity 101: A Transgender Primerby Alexander John Goodrum, a publication of TGNet Arizona, by Alexander John Goodrum, a publication of TGNet Arizona, www.tgnetarizona.orgwww.tgnetarizona.org
Intersexed Society of North America; Intersexed Society of North America; www.isna.orgwww.isna.org, Advocacy and , Advocacy and educational organization founded and led by intersexed people.educational organization founded and led by intersexed people.
For a copy of the Needs Assessment “Identifying Training Needs For a copy of the Needs Assessment “Identifying Training Needs of Health Care Providers Related to Treatment and Care of of Health Care Providers Related to Treatment and Care of Transgendered Patients:Transgendered Patients:A Qualitative Needs Assessment” contact A Qualitative Needs Assessment” contact the author, Samuel Lurie, at [email protected] author, Samuel Lurie, at [email protected]