access to tb drugs and diagnostics gregg gonsalves open society foundations division of the...
TRANSCRIPT
Access to TB Drugs and Diagnostics
Gregg GonsalvesOpen Society Foundations
Division of the Epidemiology of Microbial Diseases, Yale School of Public HealthDepartment of Global Health and Social Medicine, Harvard Medical School
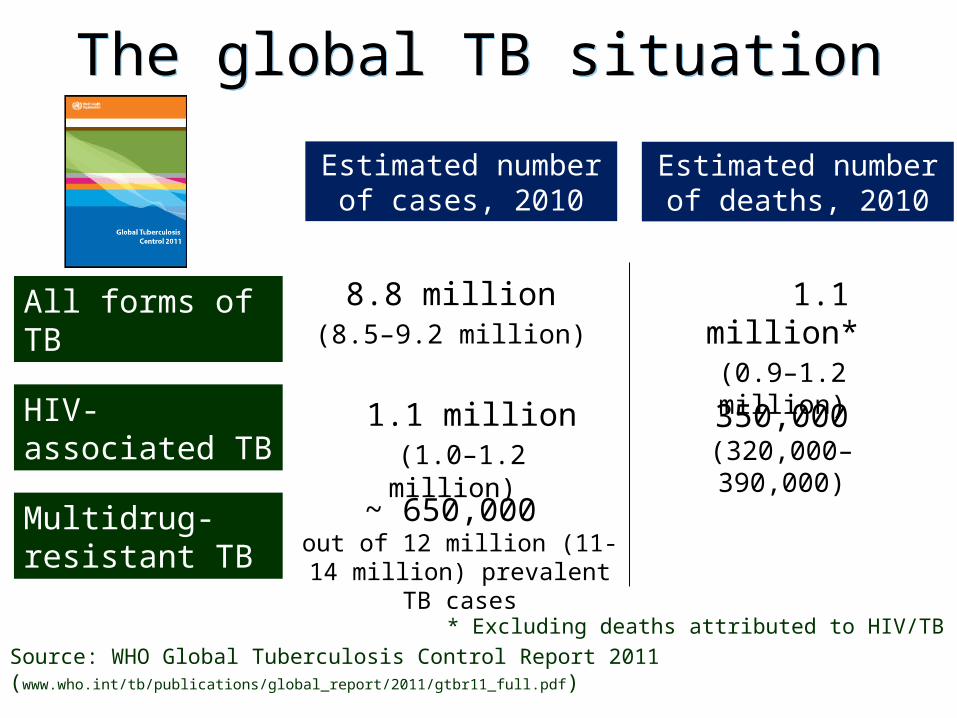
The global TB situationThe global TB situation
Estimated number of cases, 2010
Estimated number of deaths, 2010
1.1 million*(0.9–1.2 million)
8.8 million(8.5–9.2 million)
~ 650,000 out of 12 million (11-14 million)
prevalent TB cases
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (1.0–1.2 million)
350,000(320,000–390,000)
Source: WHO Global Tuberculosis Control Report 2011 (www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf)* Excluding deaths attributed to HIV/TB
0–24
25–49
50–99
100–299
>300
No estimate
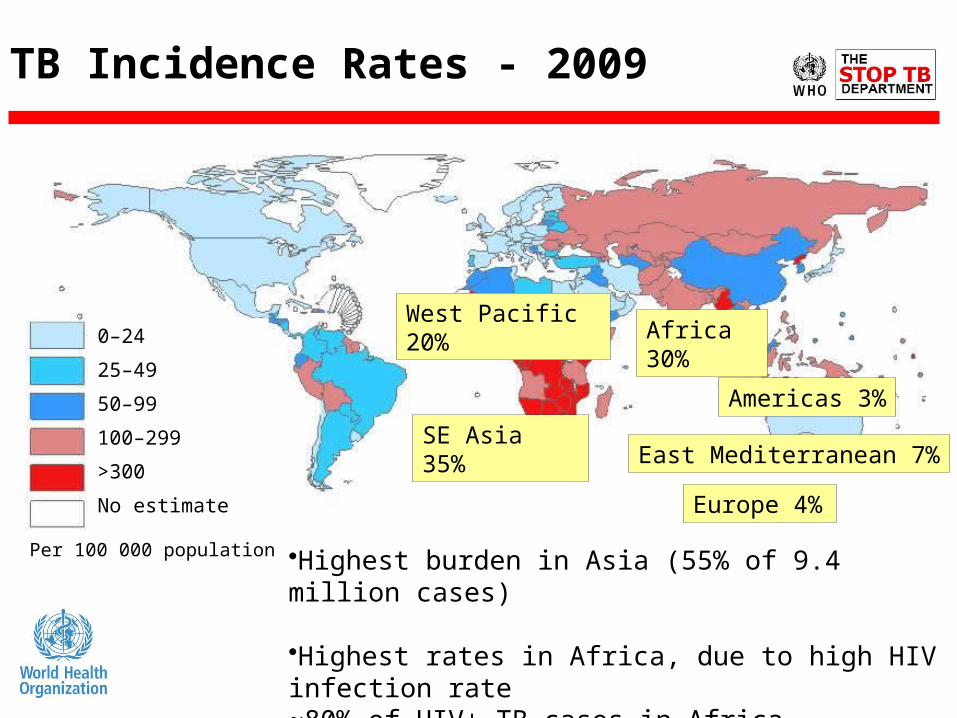
•Highest burden in Asia (55% of 9.4 million cases)
•Highest rates in Africa, due to high HIV infection rate~80% of HIV+ TB cases in Africa
Per 100 000 population
TB Incidence Rates - 2009
Africa 30%
West Pacific 20%
SE Asia 35%
Europe 4%
East Mediterranean 7%
Americas 3%

Impact of HIV on TB in Africa
Notified cases per 100,000 pop. 1980-2008
•79% of all TB/HIV cases world-wide are in Africa•50% of all TB/HIV cases world-wide in 9 African countries•23% of the estimated 2 million HIV deaths due to TB

Time trends in MDR-TBTime trends in MDR-TBAvailable data from 74 countries and territories with measurements for at least two years could not answer the question of whether the proportion of previously untreated TB cases with MDR was increasing, decreasing or stable over time at a global or regional level.

Proportion of MDR among new TB cases Latest available data, 1994-2010
0-<3
3-<6
6-<12
12-<18
>18
No data available
Subnational data only
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines
for which there may not yet be full agreement. WHO 2011. All rights reserved

0-<6
6-<12
12-<30
30-<50
>50
No data available
Subnational data only
Proportion of MDR among previously treated TB cases Latest available data, 1994-2010
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines
for which there may not yet be full agreement. WHO 2011. All rights reserved

Countries that had reported at least oneXDR-TB case by Oct 2011
Argentina Burkina Faso Estonia Japan Namibia Republic of Korea The Former Yugoslav Republic of MacedoniaArmenia Bhutan France Kazakhstan Nepal Republic of Moldova TogoAustralia Cambodia Georgia Kenya Netherlands Romania TunisiaAustria Canada Germany Kyrgyzstan Niger Russian Federation TurkeyAzerbaijan Chile Greece Latvia Norway Slovenia UkraineBangladesh China India Lesotho Pakistan South Africa United Arab EmiratesBelarus Colombia Indonesia Lithuania Peru Spain United KingdomBelgium Czech Republic Iran (Islamic Rep. of) Mexico Philippines Swaziland United Republic of TanzaniaBenin Dominican Republic Ireland Mongolia Poland Sweden United States of AmericaBotswana Ecuador Israel Mozambique Portugal Tajikistan UzbekistanBrazil Egypt Italy Myanmar Qatar Thailand Viet Nam
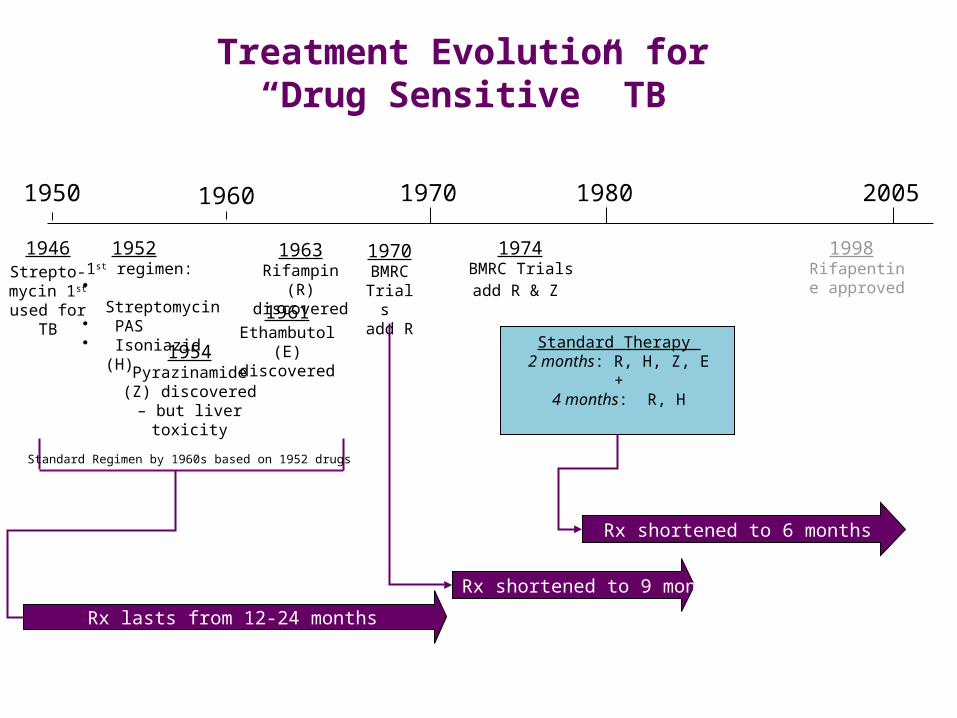
Treatment Evolution for“Drug Sensitive” TB
1950 2005
1952 1st regimen:
• Streptomycin• PAS• Isoniazid (H)
1963 Rifampin (R) discovered
1974 BMRC Trials add R & Z
1970
1954Pyrazinamide (Z)
discovered – but liver toxicity
Rx lasts from 12-24 months
Standard Regimen by 1960s based on 1952 drugs
1970BMRC Trials add R
Rx shortened to 9 months
Standard Therapy 2 months: R, H, Z, E
+4 months: R, H
Rx shortened to 6 months
19801960
1946Strepto-mycin 1st
used for TB
1998 Rifapentine approved
1961 Ethambutol (E)
discovered
9

The Burden of Therapy for Multi-drug Resistant TB
Example of a typical regimen for MDR-TB•Intensive phase of 6-9 months – aim to directly observe 6 days/week:
– Six drug combination, one given by injection•Continuation phase of 18 months:
– Four drugs•A patient may need longer therapy if sputum is not clear of TB at month 4
Note: If the patient has HIV, he/she may need to take 3 additional anti-retroviral drugs
10

The Burden of Therapy for Multi-drug Resistant TB
• The price of four medicines in particular weigh heavily in the overall cost of a DR-TB regimen. Overall costs of the DR-TB regimen are particularly driven by capreomycin, moxifloxacin, PAS, and cycloserine.
• For most DR-TB drugs, patents are not typically a factor in causing high prices, because the medicines were developed so long ago that patents on most have long run out. However, moxifloxacin is a notable exception—until now, Bayer’s monopoly has kept prices high.
• Some DR-TB drug prices have increased considerably between 2001 and 2011, including for the medicines procured through the GDF for GLC-approved treatment programs. This is true of the prices of amikacin (the most affordable source in 2011 costs eight times more the most affordable source in 2001), kanamycin (six times more), cycloserine, and capreomycin (both three times more). 1
1

MDR-TB Drug Prices

► Significant improvements in therapy are needed for all patient populations
Patient Population
CurrentTherapy
UnmetNeeds
Drug-Susceptible TB 4 drugs; ≥6 month therapy Shorter, simpler therapy
Drug-ResistantM(X)DR-TB
Few drugs (including injectables); ≥18 months therapy; toxicities
Totally oral, shorter, more efficacious, safer and lower cost therapy
TB/HIVCo-Infection
Drug-drug interactions with HIV medications
Ability to co-administer TB regimens with ARVs
Latent TBInfection 6-9 months of treatment Shorter, safer therapy
Children 4 drugs; ≥6 month therapyShorter, simpler therapy with pediatric-friendly dosing
Current TB Therapy and Unmet Needs
13

The Global TB Development Pipeline
From the Stop TB Partnership Working Group on New Drugs
14

Tuberculosis Diagnosis: Then and Now


The Future of TB Diagnostics
– Xpert MTB/RIF :• Level of the Health system: Peripheral laboratory,
at district and sub-district level (intended for use in secure facilities with a reliable source of electricity)
• For LICs and MICs FIND negotiated a 75% reduction relative to the market price:
• $16.86 per cartridge• $17,000 - $17,500 per Instrument• But• Not the POC diagnostic that is needed.
Xpert MTP/RIF
• Point-of-care: easy to perform in peripheral health centres
• Detect active TB in adults regardless of HIV status• Improved diagnosis of TB in children• Result that allow decision on treatment initiation • Patient can receive result on the same day
The TB Test We Need

2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Dis
tanc
e fr
om P
atien
ts
Intermediate level Lab
Reference level
New SS+ case definition
2-specimen approaches
POC test (detection)
Peripheral level
AbbreviationsDST: Drug susceptibility testNAAT: Nucleic acid amplification testLTBI: Latent TB infectionPOC: Point of careMODS: Microscopic observation drug-susceptibilityNRA: Nitrate reductase assayCRI: Colorimetric redox indicator assayLED: Light-emitting diodeLPA: Line probe assay
Technologies or methods endorsed by WHO
Rapid speciation
Liquid culture & DST
LPA for MDR-TB
Non-commercial culture & DST (MODS, NRA,CRI)
LPA for XDR-TB
10-40%
70%
95%
% Access aft
er 5 years
Predictive LTBI
Xpert MTB/RIF
Rapid colorimetric
DST
Manual NAAT 1st generation
Manual NAAT 2nd generation
Technologies at late stages of development
Technologies at early stages of development
LED microscopy
Same-day diagnosis

Tonight! From 7-8PM
Meet in Hotel Lobby(with guest Salmaan Keshavjee, Harvard Medical
School/Partners in Health)
Let’s Start a Campaign to Drop the Price of MDR-TB Drugs!