acid base balance & perinatal implications s arulkumaran professor emeritus obstetrics &...
TRANSCRIPT
Acid base balance & Perinatal Implications
S ArulkumaranProfessor Emeritus
Obstetrics & GynaecologySt George’s University of London
Perinatal Implications of asphyxia
• Intrapartum or immediate NN death
• Cerebral palsy / Neurological deficits
• Admission to NNU with HIE (Gr 1-3)
• Low Apgar scores & metabolic acidosis
• Concepts of hypoxaemia, hypoxia, asphyxia
Definition of a fetus in jeopardy
1. A normal state.
2. Hypoxaemia (relative lack of O2 in the blood).
3. Hypoxia (decreased oxygenation of tissues) .
4. Asphyxia (Hypoxia + Metabolic acidosis in tissues due to anaerobic metabolism).
Acid base balance
• Respiratory or metabolic or mixed acidosis (lactic acid + carbonic acid)
• pH and base excess/ base deficit
• pH and hydrogen ions (negative logarithmic relationship)
• Base excess and buffers – bicarbonate, Hb, plasma proteins

Progression of anaerobic metabolism
1. Accumulation of organic acids that slowly cross the placenta in contrast to CO2 which rapidly crosses the placenta.
2. Asphyxia results from the combination of metabolic acidosis and hypoxia.
3. Injury and death of the cell, tissues, organs and finally to the organism due to the stoppage of cellular enzymes at certain pH level.
Examples of Cell Dysfunction
1. Heart failure.
2. Pneumocytes type 2 injury lead to less surfactant factor.
3. GI system “necrotizing enterocolitis”
4. Renal failure.
5. Endothelial damage leads to DIC.
6. CNS cerebral oedema, seizures and cell death leads to cerebral palsy.
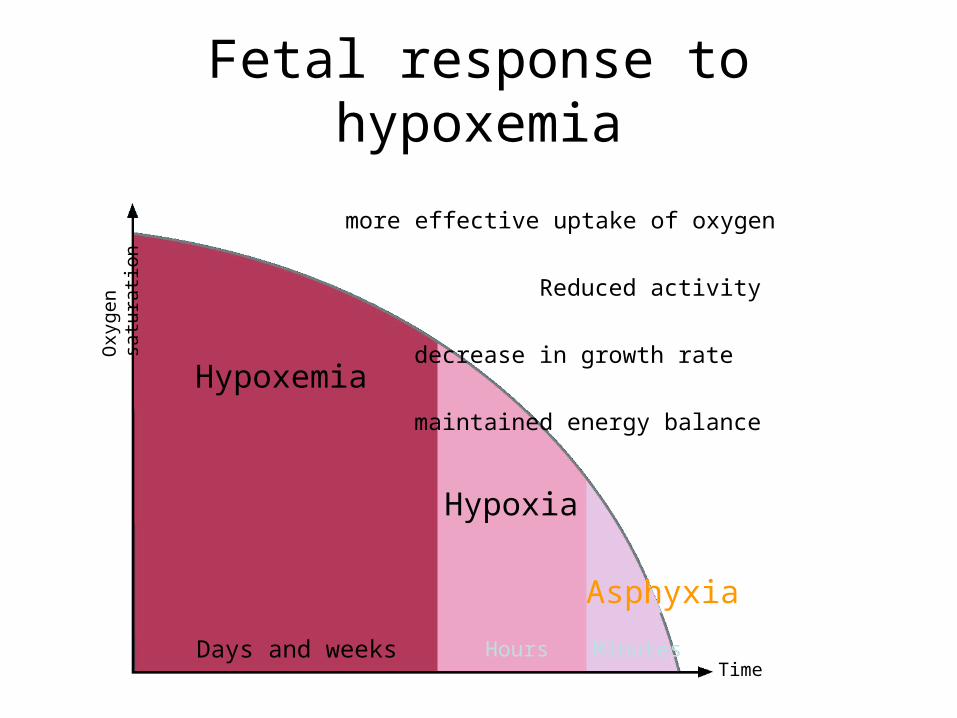
Fetal response to hypoxemia
Time
Oxygen
satu
rati
on
Days and weeks Hours Minutes
Hypoxemia
Hypoxia
Asphyxia
more effective uptake of oxygen
Reduced activity
decrease in growth rate
maintained energy balance

The fetal response to hypoxia
Time
Oxygen
satu
rati
on
Days and weeks Hours Minutes
Hypoxemia
Hypoxia
Asphyxia
surge of stress hormones
redistribution of blood flow
anaerobic metabolism in the peripheral tissues
maintained energy balance

Fetal response to asphyxia
Time
Oxygen
satu
rati
on
Days and weeks Hours Minutes
Hypoxemia
Hypoxia
Asphyxia
Alarm reaction
anaerobic metabolism in peripheral tissues
brain and heart organ failure

Fetal monitoring goals :
1. To identify a fetus in jeopardy in timely fashion so that we can intervene and prevent permanent damage or death.
2. To identify a normal fetus so that we can safely continue expectant management to avoid unnecessary interventions (CS or IVD).

Umbilical artery A/B
Sequential Changes in Tests of Fetal well being
Growth
Fetal sizeless than5th centile
Aortic Aortic blood blood flowflow
Cerebral blood flow
AbnormalAbnormalvenousvenousflowflow
AbnormalFHRTrace
AFI Oligohydramnios
ModerateModerateseveresevereredistribnredistribn
4’th December 2014



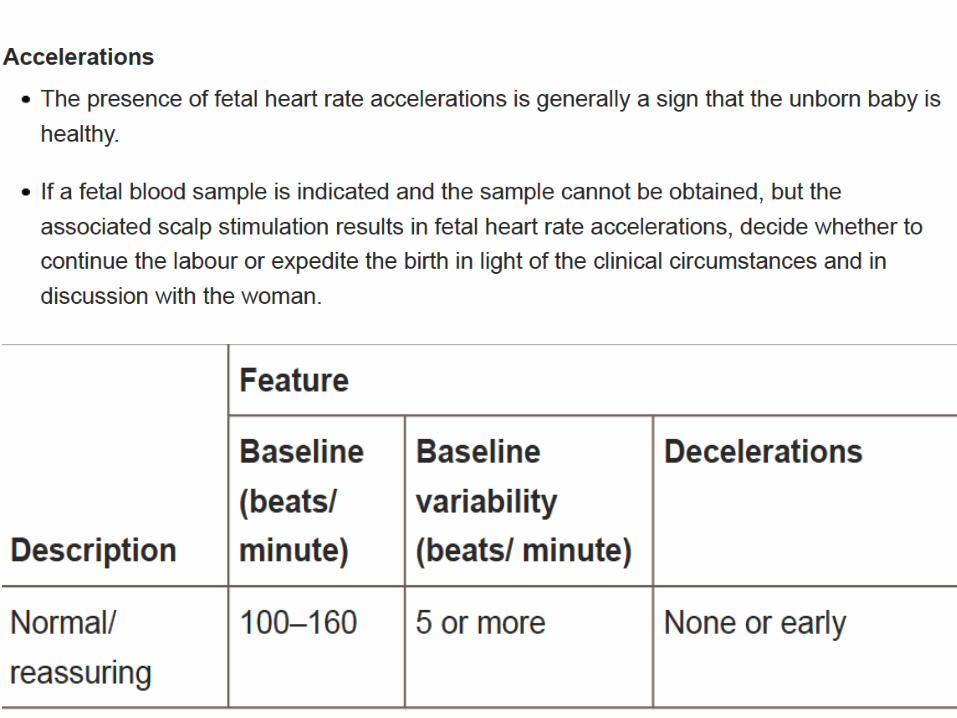


GREEN – Normal & Reassuring

Non reassuringNeed for Conservative Measures

Abnormal & needs Comservative measures+ Additional Testing
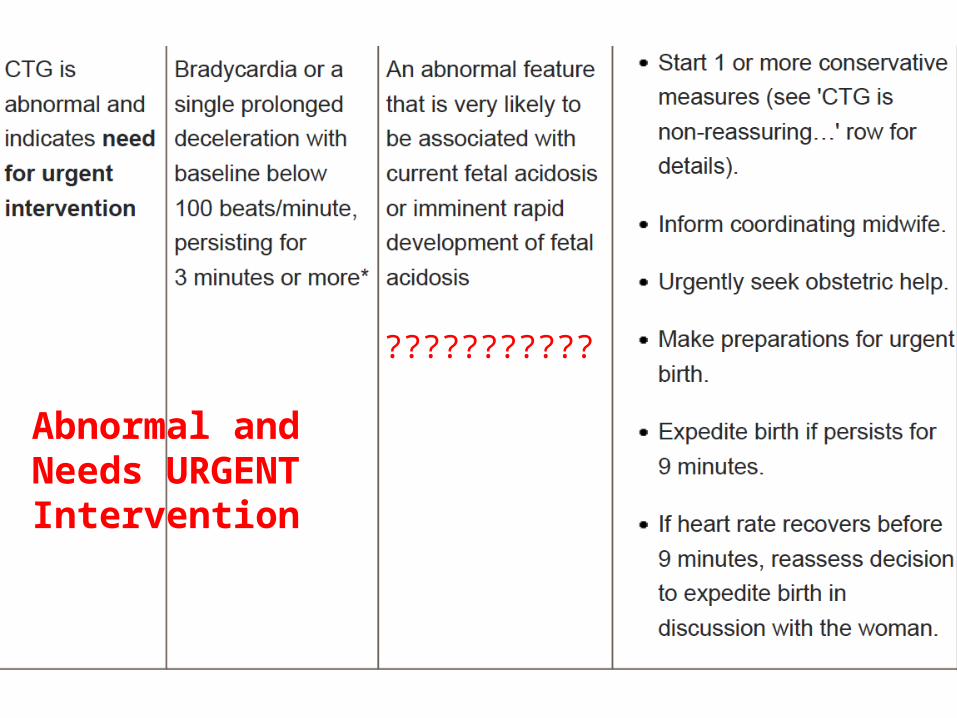
Abnormal and Needs URGENTIntervention
???????????






Fetal blood sampleFetal blood sample (FBS) result (pH)
=> 7.25
Subsequent action
FBS should be repeated if the FHR abnormality persists
7.21 – 7.24
Repeat FBS within 30 mins or consider delivery if rapid fall since last sample
< 7.20 Delivery indicated
All scalp pH estimations should be interpreted taking into account the initial pH measurement, the rate of progress in labour and the clinical features of the mother and baby
NICE – Recommendations for FBS
• Units employing EFM should have ready access to FBS facilities - A
• Where delivery is contemplated because of an abnormal FHR pattern in cases of suspected fetal acidosis, FBS should be undertaken in the absence of technical difficulties or any contraindications - A
NICE – Contraindications to FBS
• Maternal infection (e.g. HIV, Hepatitis, Herpes)• Fetal bleeding disorders (haemophilia)• Prematurity (34 weeks)• Where there is clear evidence of acute fetal
compromise (e.g. prolonged deceleration > 3 minutes

Umbilical cord A/V sampling
• Paired samples B
• Artery pH &BE as a minimum after ©
Em CS, IVD, FBS was done in labour, poor condition of the baby at birth

Cord blood samples
• Normal values Artery Vein• pH 7.05-7.38 7.17-7.48• pCO2 kPa 4.9 – 10.7 3.5 – 7.9• BD ecf m.mol/l -2.5 -10.0 -1.0 – 9.0
• pH should be atleast 0.03 units less in artery• pCO2 should be atleast 1.0 kPa higher in the
artery
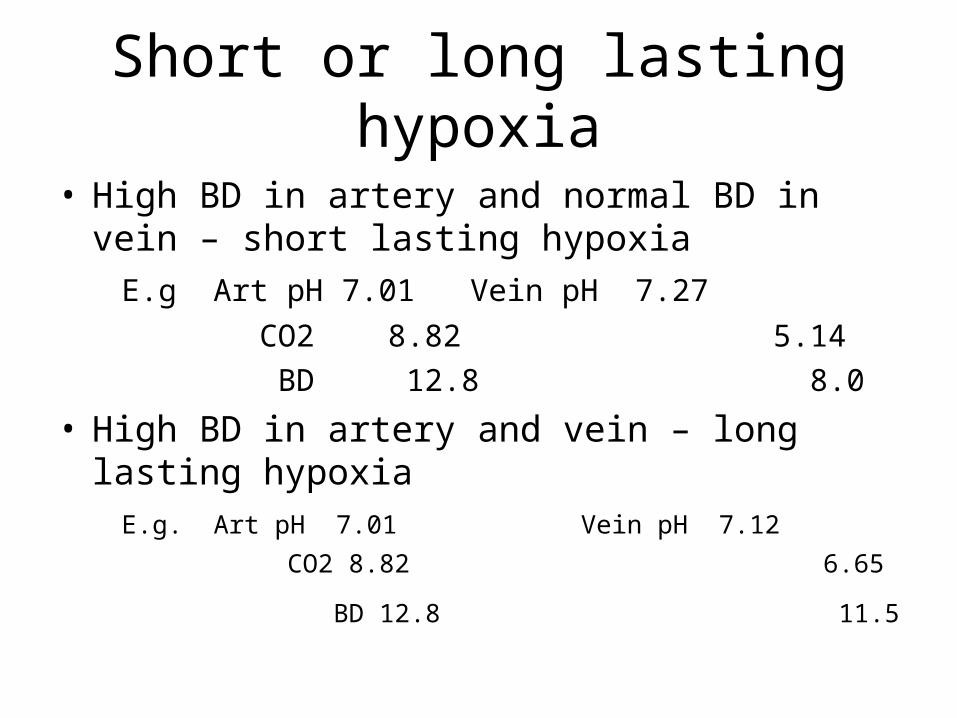
Short or long lasting hypoxia
• High BD in artery and normal BD in vein – short lasting hypoxia
E.g Art pH 7.01 Vein pH 7.27
CO2 8.82 5.14
BD 12.8 8.0
• High BD in artery and vein – long lasting hypoxia E.g. Art pH 7.01 Vein pH 7.12
CO2 8.82 6.65
BD 12.8 11.5
THANK YOU
THANKYOU