acls ii sept 25 students copy 2003
TRANSCRIPT
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 1/63
CORE ACLS
CONCEPTS
ADVANCED
CARDIAC LIFE SUPPORT
3/2/2012

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 2/63
Core ACLS Concepts “The chain of survival” has 4 links applied to
all CPR settings (hospital, ER (A&E), ICU,
CCU, or community)
Early Early Early Early
Access CPR Defibrillation Advanced care
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 3/63
Advanced Cardiovascular/Cardiac Life Support
Is a training program that generally aims to
develop the knowledge and skills of health
care providers as they make effective use of
themselves when assisting in a code
situation.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 4/63
Definition of Terms:
ACLS – Iincludes the knowledge and skills
necessary to provide the appropriate early
treatment for cardiopulmonary current which
reduces BLS and use of adjunctive
equipment and special technique to establish
and maintain ventilation and circulation.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 5/63
Terminologies
Cardioversion - The discharge of electrical energy synchronized on
the R wave of the electrocardiogram.
Defibrillation - use of unsynchronized electrical energy for revision of
cardiac arrhythmias.
Algorithm – sets of step-by-step procedure guides to assist caregiversin making informed decisions regarding the diagnosis and treatment
of disease.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 6/63
ECC – (Emergency Cardiac Care) includes all responses necessary to deal with
sudden and often life threatening events affecting the cardiovascular andpulmonary system.
Megacode - situation wherein the algorithm will be applied and an individual
will be tested on his ability to recite the exact sequences of an algorithm.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 7/63
Resuscitation (Code Red)
General Policy:
The Cardiac Code team’s goals are to preserve life, restore health, relieve
suffering and limit disability. These goals shall be carried out promptly with
patient safety foremost in the mind.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 8/63
A team is composed of :
1. Person for chest compression
2. Ventilator
3. Person to insert IV lined and will administer medications.
4. Person to monitor the cardiac and will do the defibrillation .
5. Recorder
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 9/63
Role of the Nurses:
1.Prepares and set-up all equipments necessary for resuscitation.
2. Regular checking of E-cart (every shift before
receiving the endorsement)
3.Document Checklist
4,Location of E-cart
5.Administer assist BLS measure
6.Carries out Doctor’s order and record the chronological event
using the CPR Record Form

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 10/63
.7. Arranges all matters pertinent to the ad
mission and transfer of patient whennecessary
8.Arranges all matters pertinent to the discharge
of patient(expired patient)
9. Autopsy, DOA, HAMA
10. REPLENISHES AND CHARGES ALL ITEMS
USED
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 11/63
GENERAL GUIDELINES FOR ALL TEAMS
Maintain quiet, orderly and professional
environment
Patient should be automatically hooked to EKG,
cardiac monitor,defibrillator and pulse oximeter
State vital signs every 5 minutes / PRN
State each medication given
Document
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 12/63
GENERAL GUIDELINES FOR ALL TEAMS
Maintain quiet, orderly and professional
environment
Patient should be automatically hooked to EKG,
cardiac monitordefibrillator and pulse oximeter
State vital signs every 5 minutes of PRN
State each medication given
Document
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 13/63
Request clarification of any order if not clearly
understood
Limit traffic
Comfort relatives and advise to stay outside the room

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 14/63
EQUIPMENT
E-cart
Pulse oximeter
Cardiac monitor with defibrillator
Ambu-bag
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 15/63
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 16/63
DOCUMENTATION
CPR Record Form
Nurse fills up the data and activities
Team leader documents the CPR outcome
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 17/63
The algorithm Approach Emergency Cardiac
Care(ECC)
The following clinical recomendations apply to all
treament algorithms
First, treat the patient not the monitor.
Algorithms for cardiac arrest presume that thecondition under discussion continually persists, that
the patient remains in cardiac arrest, and that CPR is
always perform.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 18/63
Apply different interventions whenever appropriate indications
exist.
The flow diagrams present mostly
Class I(acceptable, definitely effective)recomendations.
The footnotes present Class IIa(acceptable, probably effective),
band Class Iib (acceptable, possibly effective), and
Class III (not indicated, may be harmful) recomendations.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 19/63
Adequate oxygenation,airway, ventilation,. Chest
compressions, and defibrillation are more important
than administration of medications and takes
precedence over initiating an intravenous line or
ejecting pharmacologic agents.
Several medications (epinephrine. Lidocaine, and
atropine) can be administered via the endotracheal
tube but the dose must be 2 – 2.5 times the
intravenous dose. (use a catheter or suction tip which
be passed beyond the tip of the endoctracheal tube.)
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 20/63
With a few exceptions, intravenous medications
should always be administered rapidly, in bolus
method.
After each intravenous medication, give a 20-30
ml bolus of intraveus fluid and immediately
elevate the extremity. This will enhance the
delivery of drugs to the central circulation, whichmay take 1-2 minutes.
Last, treat the patient, not the monitor.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 21/63
Core ACLS Concepts The Most Important Goal : > Cerebral resuscitation
The Patients :
u For Many >> Their hearts should be too good to die.
u For Some >> The last heartbeat should be the last.
Treat the patient, not the monitor
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 22/63
Cardio-pulmonary-cerebral resuscitation Primary purpose : to return the
patient to his/her best possible
neurological outcome.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 23/63
Arrythmia Recognition
Important in any ACLS/ CPR sequence
All algorithms start with identifying rhythm
Cannot identify arrhytthmais- cannot mange
corrrectly
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 24/63
The Beating Heart – ElectrophysiologyElectrical Stimulation & Contraction
BEFORE THE HEART CONTRACTS
IT MUST BE ELECTRICALLY STIMULATED
DEPOLARIZATION
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 25/63
Pacemaker impulses are initiated in the SA node,
travelling through atrial pathways, at frequenciesbetween 60-100bpm
There is the presence of a P wave, followed by a
QRS complex at a regular rate
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 26/63
Normal Sinus Rhythm
Look at the P waves ;
rate is 60-100/min
Cycle length do not vary by 10%
PR interval is 0.12 – 0.20sec.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 27/63
During ACLS/BLS:
• Patient is hooked to cardiac monitor/ defibrillator
•Patient’s heart rate is automatically detected
•Normal HR = 60 to 100 bpm
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 28/63
MANAGEMENT:
A. No specific drug treatment
B. Identification of cause
C. Treatment of underlying cause
D. Check hemodynamics
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 29/63
Characterized by tachycardia with a narrow QRS complex
Sudden onset and termination
150-250 beats/min (180-200 bpm in adults)
Regular rhythm
QRS complex is normal in contour and duration
No P waves
•P waves are generally buried in the QRS complex
•Often, P wave is seen just prior to or just after the end of the QRS and cause a subtle
alteration in the QRS complex that results in pseudo- s or pseudo - r
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 30/63
A. Cardiovert the patient!
B. Defibrillate the patient!
C. Give Verapamil!
D. Check hemodynamics
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 31/63
Prematurely occurring complex
Wide, bizarre looking QRS complex
Usually no preceding P waves
T wave opposite in deflection to the QRS complex
Complete compensatory pause following every premature beat
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 32/63
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 33/63
• Adult (1 to 2L) bag and the provider should deliver
approximately 600 ml of tidal volume sufficient to produce chest
rise over 1 second
•Open the airway adequately with a head tilt-chin lift, lifting the
jaw against the mask and holding the mask against the face,
creating a tight seal
•During CPR give 2 breaths (each 1 second) during a brief (
about 3 to 4 seconds) pause after every 30 chest compr essions.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 34/63
Use of 100% inspired oxygen (FiO2 1.0) as soon as it becomes
available is reasonable during resuscitation from cardiac
arrest (Class IIa, LOE C)
Titrate oxygen administration to achieve arterial
oxyhemoglobin saturation > 94%
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 35/63
To facilitate delivery of ventilations with a bag-mask device,
the nasopharyngeal airway can be used in patients with a
compromised airway
In the presence of known or suspected basal skull fracture or
severe coagulopathy, an oral airway is preffered (Class II a,
LOE C)
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 36/63
ADVANTAGES
Keeps airway patent
Permits suctioning of airway secretions
Enables delivery of a high concentration oxygen
Provides an alternative route for administration of some
drugs
Facilitates delivery of a selected tidal volume
With use of a cuff, may protect the airway from
aspiration
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 37/63
Epinephrine
Lidocaine
Vasopressin
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 38/63
Endotracheal intubation is frequently associated with
interruption of compressions for many seconds
Placement of a supraglottic airway is a reasonable
alternative to endotracheal intubation and can be done
successfully without interrupting chest compressionsa
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 39/63
Rescuer should record the depth of the tube as marked
at the front of the teeth and secure it.
Providers should verify correct placement of all
advanced airways after insertion and whenever the
patient is moved.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 40/63
VENTILATION
Chest x-ray
Rationale: Confirm secure airway and detect
causes or complications of arrest:
pneumonitis, pneumonia, pulmonary edema.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 41/63
VENTILATION
After ROSC, routine hyperventilation leading to hypocapnia
should be avoided to prevent additional cerebral ischemia.
CONTROLLED OXYGENATION
There is insufficient evidence to support or refute the use of
titrated inspired oxygen content in the early care of cardiac
arrest patients following sustained ROSC
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 42/63
VENTILATION
Mechanical Ventilation
o Rationale: Minimize acute lung injury, potential oxygen
toxicity
o Tidal volume – 6 – 9ml/kg
o Titrate minute ventilation to
- PETCO2 – 35- 40 mm Hg
- PaCO2 – 40- 45 mm Hg
o Reduce FiO2 as tolerated to keep SpO2 or SaO2 > 94%

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 43/63
ELECTRICAL THERAPIES
DEFIBRILLATION & CARDIAC PACING
PHA Council on CPR

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 44/63
Electrical Therapies
Defibrillation
Cardioversion
Cardiac Pacing
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 45/63
Key Challenges (2010 Guidelines)
Improve time for Defibrillator Availability
- Immediate AED availability
- Improve response time and training
Decrease interruptions in chest
compressions pre and post shocks
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 46/63
DEFIBRILLATION
Is the therapeutic use of electric current delivered in large
amounts over very brief periods of time.
Temporarily “stuns” an irregularly beating heart and allows
more coordinated contractile activity to resume.
Termination of VF for at least 5 seconds follwing the shock.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 47/63
AUTOMATED EXTERNAL DEFIBRILLATORS
Sophisticated, reliable computerized devices that use voice and
visual prompts to guide lay rescuers and health care providers to
safely defibrillate VF SCA
Recorded information about frequency and depth of chest
compressions during CPR.
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 48/63
BIPHASIC WAVE FORM DEFIBRILLATORS
Defibrillation with biphasic waveforms uses relatively low
energy ( < 200 J ) that is safe and has equivalent or higher
efficacy for termination of VF than monophasic waveform
shocks (class llb)
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 49/63
SYNCHRONIZED CARDIOVERSION
Synchronization avoids shock delivery during the
relative refractory portion of the cardiac cycle, when a
shock could produce VF.
The energy (shock dose) used for a synchronized shock
is lower than that used for unsynchronized shocks
(defibrillation)

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 50/63
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 51/63
CARDIAC PACING
Deliver an electric stimulus through electrodes to
the heart causing electrical depolarizations and
subsequent cardiac contraction
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 52/63
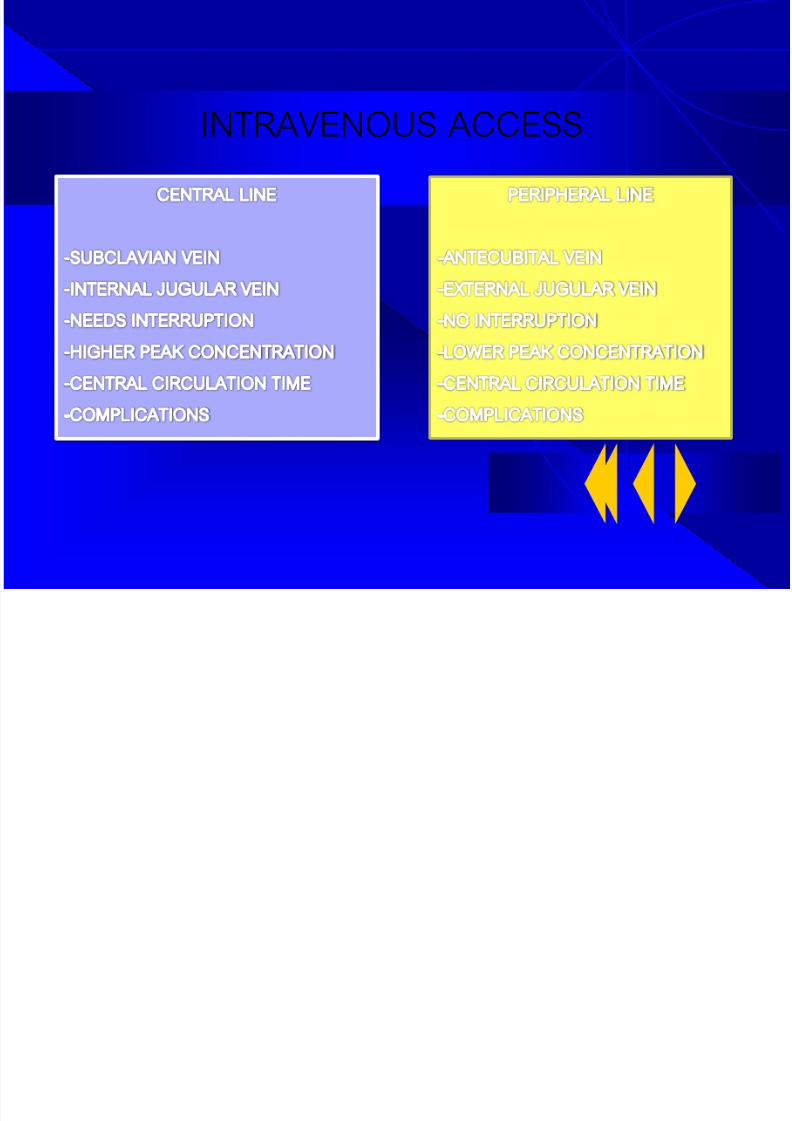
INTRAVENOUS ACCESS
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 53/63
PERIPHERAL IV SITE
Administer drugs by Bolus
20cc of saline or distilled water
Elevate the extremity for 10-20
seconds
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 54/63
Tracheal Drug Administration
NAVEL (Naloxone, Atropine, Vasopressin, Epinephrine,
Lidocaine)
Administer 2 to 2.5 times the recommended IV dose
diluted in 10ml NSS or distilled water
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 55/63
ACLS DRUGS
Agents used to Optimize Agents used to treat Arrhythmias
Cardiac Output and blood pressure
Cardiac Arrest Shock Heart Failure/ Tachycardia Bradycardia
Pulmonary Edema, Misc;
buffers
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 56/63
MONOPHASIC WAVE FORM DEFIBRILLATORS
Deliver current of one polarity
Monophasic damped sinusoidal waveforms (MDS) returns to zero
gradually, whereas the Monophasic truncated exponential
waveform current is abruptly returned to baseline to zero current
flow.
Initial shock is 360J and if VF persists, the subsequent shocks
should be 360J
Time Sequence &
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 57/63
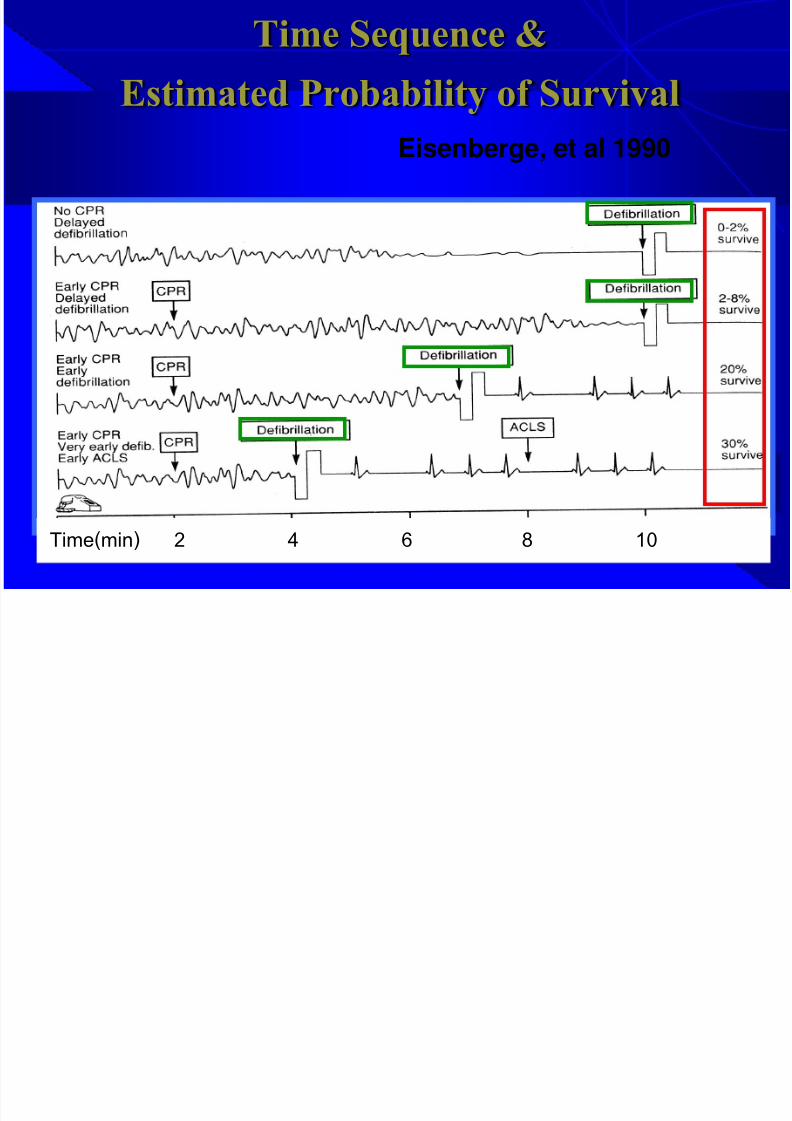
Time Sequence &
Estimated Probability of Survival
Eisenberge, et al 1990
Time(min) 2 4 6 8 10
CPR T & O i i
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 58/63
CPR Team & Organization
BLS & ACLS
Training &
Retraining,
CPR Code
Organization,
Performance
Evaluation &
Peers R eview
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 59/63
Core ACLS Concepts Classification of Therapeutic Interventions
in CPR & ECC
Class I : acceptable, definitely effective
Class II : acceptable, uncertain efficacyII a > probably effective
II b > possibly effective & not harmful
Class III : inappropriate & may beharmful
The Algorithm Approach
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 60/63
in ACLS & ECC
Treat the patient, not the monitor
Continue CPR (include defibrillation) is moreimportant than the procedure and pharmacologicagents
Flow diagrams: mostly class I,footnotes: class IIa, IIb, or III
Most ACLS medications(but few exceptions) shouldbe given as iv. bolus
“2
nd
Syringe Technique” for 20-30 ml. iv. bolus aftereach iv. medications
Epinephrine, lidocaine, atropine, etc can be given viaET tube at 2-2.5 times of iv. Route
Summary :

8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 61/63
Summary : Ten Commandments for ACLS
1. Do good CPR : do CPR whenindicated, not do when not indicated,and do well
2. Highest priority is the primary C A-B--D* survey & hunt for VF
3. The next highest priority is thesecondary CA-B--D** survey
4. Know the defibrillator! : familiarizeand daily maintenance check
5. Search for reversible or treatable causes.
Summary :
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 62/63
Summary : Ten Commandments for ACLS
6. Know the ECC medications : “Why?”,“When?”, “How?”, and “Watch out?!?”
7. Be a good team : conductor ormember
8. Practice the phase responseresuscitation format :anticipation/entry/resuscitation/maintenance/ family notification/transfer/critique
9. Determined “code status” in advance
Summary :
8/2/2019 ACLS II Sept 25 Students Copy 2003
http://slidepdf.com/reader/full/acls-ii-sept-25-students-copy-2003 63/63
Summary : Ten Commandments for ACLS
10. Learn and practice the most difficultresuscitation skills*:
when not to start CPR
when to stop CPR
how to tell the family members
how to talk with your colleagues
Even though it’s the most difficult, but it’s
more important & more challenging!