aco partnerships · mssp ltc aco vs institutional special needs plan • only one regulatory agency...
TRANSCRIPT
ACO PartnershipsCreating Effective SNF Engagement
with and within Accountable Care Organizations
December 10, 2019

ACO Partnerships
• Mike Hensley Owner & Chief Marketing Officer –Burgess Square Healthcare Centre
• Jason FeuermanPresident – LTC ACO SVP – Genesis Healthcare
Canaries in the Coal MineEngagement in ACO and APM Partners
Mike Hensley, Managing Partner, Burgess Square Healthcare Centre
Burgess Square’s ACO JourneyTake care of the residents, patients, staff and families and the rest will take care of itself
• Burgess Square is an independently owned SNF in the suburban Chicago area.o Average skilled census is 75 with approximately 115 admissions and 115 discharges per month.o Average length of stay is 14 dayso 500% increase in new admissions since 2009o 114th out of 15,000 facilities in the country for Medicare volume
• The ACO market became active in our area in 2011-2012. • By 2016, Burgess Square was participating in 4 different ACOs and 3 different BPCI
programs. • By 2018, Burgess Square had 3 day waiver participation agreements with 2 ACOs.• At the end of 2018, Burgess Square and one of the ACOs terminated the ACO agreement
due to lack of alignment with mutual goals.
How Did We Get There?
• Investment in Qualityo 5 Stars across the boardo Deficiency free survey in 2019o Low readmission scores o AHCA Quality award program
• Stable leadership and staff• Strong clinical systems
o Rounding specialistso Pulmonary program
• Culture of patient and staff engagement
Successful Collaboration with an ACO“Yes, it is possible”
• Take time to understand the ACOs goals and objectives. Demonstrate to the ACO that the SNF is invested in helping the ACO meet their goals.
• Educate the ACO on SNF operations and how best to align the SNF and ACO. ACOs often do not understand SNF RoPs.
• Keep track of your own data and share your findings with the ACO. If there is something that the SNF feels is important and the ACO doesn’t track, track it for them.
• Identify mutual opportunities for improvement.• Don’t be afraid to professionally challenge an ACOs decision or
recommendation.
Data is King
• Know your organization’s data:oReadmission RatesoLength of StayoCost per beneficiaryoPatient satisfaction scoresoReferrals to ACOs preferred organizations
• Identify and report flaws in ACOs data collection and reporting:oQuestion ACO data that does not match your dataoExplain outliers
Challenges and Barriers
• Multiple APM partners with different data collection methods and protocols.
• One sided partnership• Lack of shared values• Volatility• Inaccurate data• Liability
Navigating a Challenging ACO
• If the ACO gives directives that do not integrate well within the SNF organization, evaluate the purpose of the directive and make recommendations on alternative solutions that work for the SNF and still achieve the desired outcome for the ACO.
• Stand behind your outcomes. If the SNF meets or exceeds benchmarks and goals set by the ACO, it gives the SNF leverage and credibility when working with the ACO.
• Don’t be afraid to professionally disagree with the ACO. • Work diligently to create a collaborative relationship rooted in respect and trust.• Always act in the best interest of the patient, even if it does not align with a
directive from the ACO.
Positioning Your SNF as an Attractive Partner
• Produce exceptional outcomes. ACOs want to partner with facilities that have good star ratings, low readmission scores and high satisfaction rates.
• Demonstrate innovation. Consider offering value added services that set your facility apart (sleep studies, pulmonary programs etc.).
• Volunteer to be part of quality improvement projects at the hospital or ACO. • Know your weaknesses before the ACO identifies them. Have processes in
place to make improvements. • Be a good partner. Provide data that the ACO asks for and keep them updated
on the status of their patients.
Engagement
• Look for opportunities everywhere.• Vertically integrate to prepare for volatile
times.• Engage physicians. • Don’t abandon traditional community
based efforts.• Streamline processes to manage high
volume. Volume drives conversation and engagement.
• Don’t be afraid to be a disrupter. Disrupters solve hidden problems.

The Medicare Shared Savings Program in the Long-Term Care SettingDirect Participation in Value-Based Payment Models
Jason Feuerman – President, LTC ACO & SVP Strategic Development / Managed Care, Genesis Healthcare
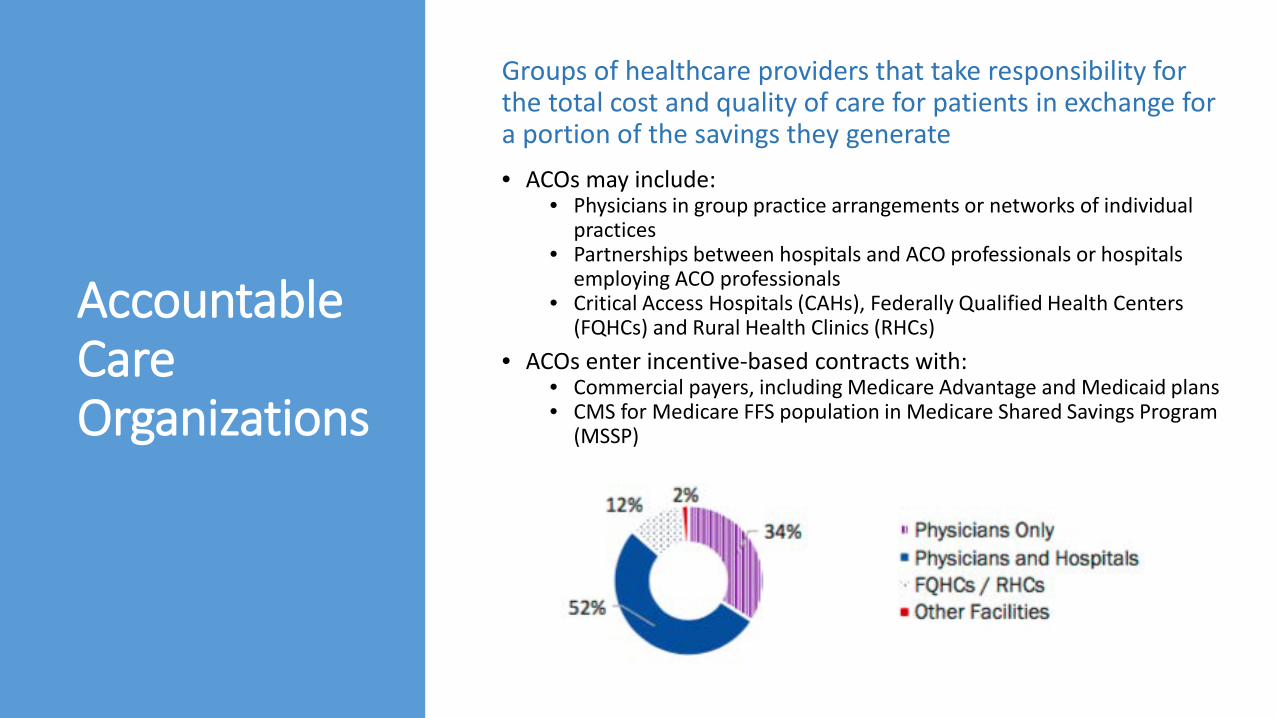
Accountable Care Organizations
Groups of healthcare providers that take responsibility for the total cost and quality of care for patients in exchange for a portion of the savings they generate• ACOs may include:
• Physicians in group practice arrangements or networks of individual practices
• Partnerships between hospitals and ACO professionals or hospitals employing ACO professionals
• Critical Access Hospitals (CAHs), Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs)
• ACOs enter incentive-based contracts with:• Commercial payers, including Medicare Advantage and Medicaid plans• CMS for Medicare FFS population in Medicare Shared Savings Program
(MSSP)

Mechanics of Shared Savings Programs
Shared Savings PaymentBonuses or penalties levied based on variance of expenditures from target and achievement of quality goals
4
AssignmentPatients assigned to ACO based on plurality of primary care costs
1
ComparisonTotal cost of care for assigned population compared to risk-adjusted target expenditures
3
BillingProviders bill Medicare normally, receive standard fee-for-service payments
2
Shared Savings Payment Cycle
Actual Spend > Projected Spending: No bonus for ACO, potential penalty if contract has downside risk
Year 1 Year 2 Year 3
Projected Spend Actual Spend
Projected Spending > Actual Spend: Shared savings bonus awarded to ACO
How Savings and Penalties are Calculated
MSSP Program
Basics
• Beneficiary assignment: Prospective or retrospective, based on physician/APP delivery of the plurality of primary care services, as determined using Medicare claims data
• Total cost of care model: ACOs manage all Medicare A + B costs, including hospice
• Benchmark: • Based on a blend of 3 years of ACO historical costs +
regional costs• Annually adjusted for healthcare cost inflation and changes
in the ACO’s population risk (HCC scores)• Shared Savings:
• Average cost for assigned population vs Adjusted Benchmark
• % shared is based on election of risk assumption• Final shared savings amount is adjusted based on the
ACO’s quality score and sequestration• Five year contract period with annual settlements for
savings/losses
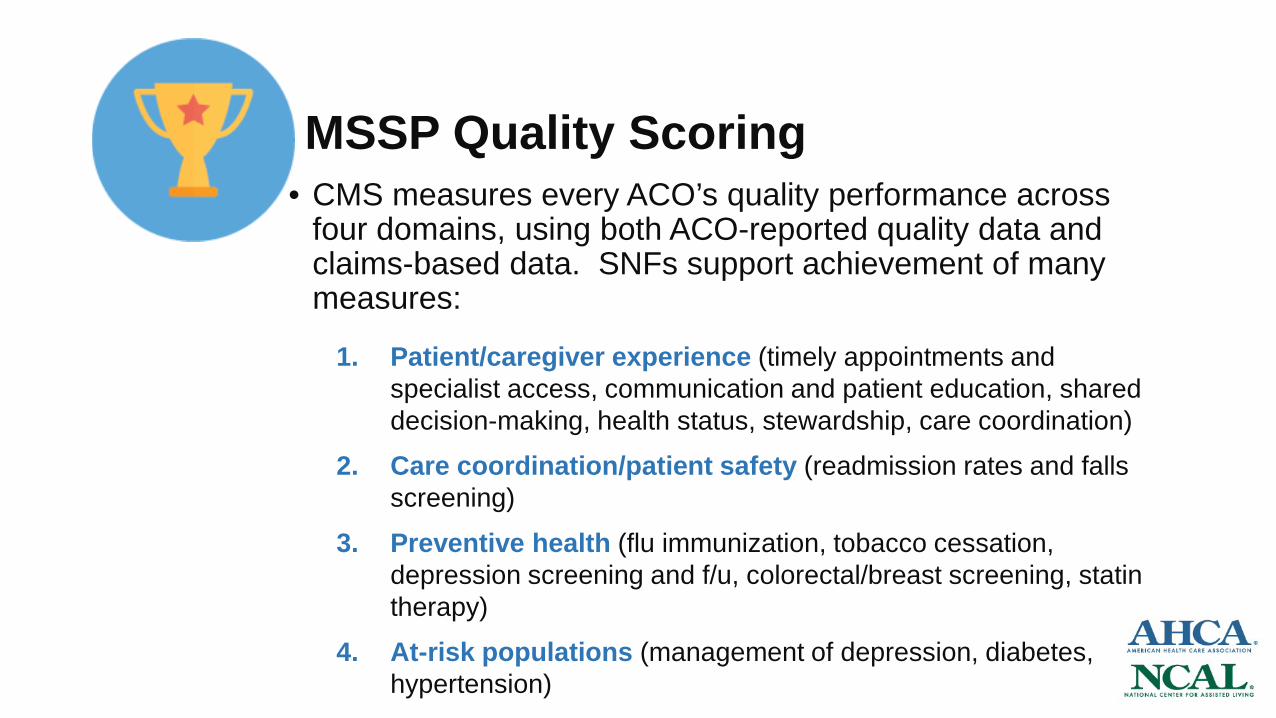
MSSP Quality Scoring• CMS measures every ACO’s quality performance across
four domains, using both ACO-reported quality data and claims-based data. SNFs support achievement of many measures:
1. Patient/caregiver experience (timely appointments and specialist access, communication and patient education, shared decision-making, health status, stewardship, care coordination)
2. Care coordination/patient safety (readmission rates and falls screening)
3. Preventive health (flu immunization, tobacco cessation, depression screening and f/u, colorectal/breast screening, statin therapy)
4. At-risk populations (management of depression, diabetes, hypertension)
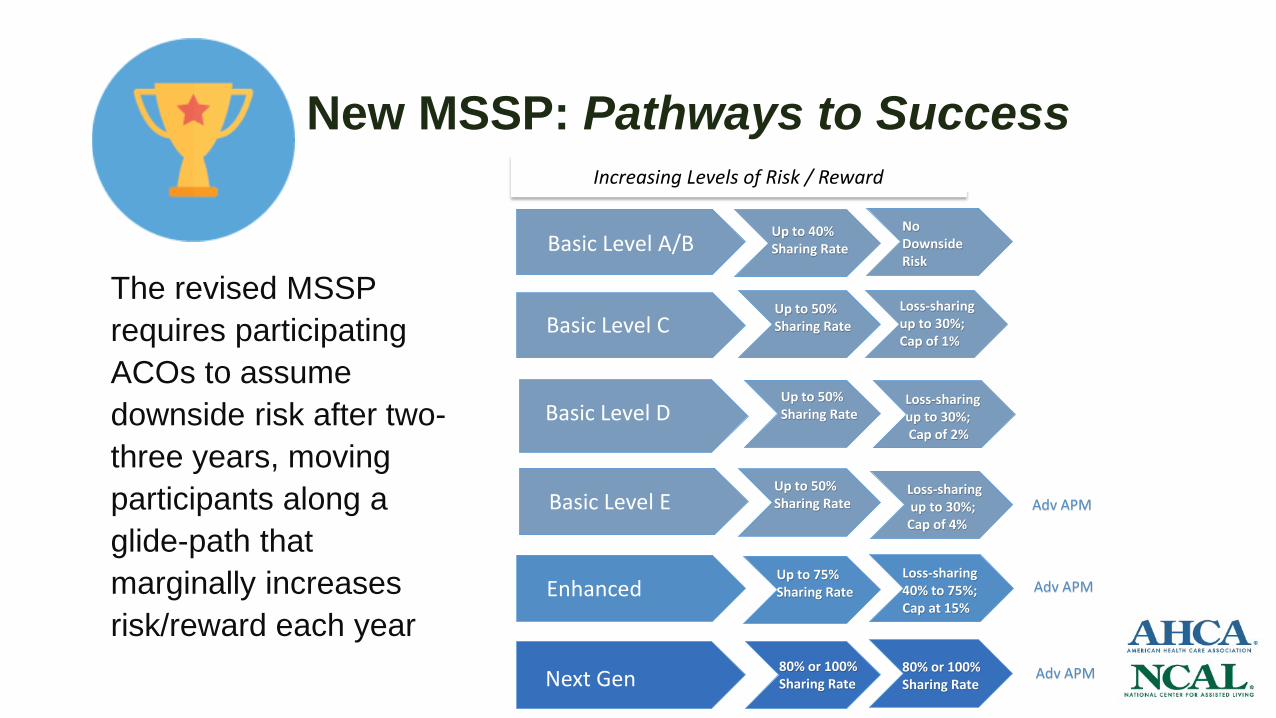
New MSSP: Pathways to Success
The revised MSSP requires participating ACOs to assume downside risk after two-three years, moving participants along a glide-path that marginally increases risk/reward each year
Increasing Levels of Risk / Reward
Basic Level C
Basic Level A/B Up to 40% Sharing Rate
Basic Level D
Basic Level E
Enhanced
Next Gen
Up to 50% Sharing Rate
Up to 50% Sharing Rate
Up to 50% Sharing Rate
Up to 75% Sharing Rate
80% or 100% Sharing Rate
Adv APM
Adv APM
Adv APM
No Downside Risk
Loss-sharing up to 30%; Cap of 1%
Loss-sharing up to 30%;Cap of 2%
Loss-sharingup to 30%;
Cap of 4%
Loss-sharing40% to 75%;Cap at 15%
80% or 100% Sharing Rate

Accountable Care Within the Nursing Facility
• Genesis Healthcare ACO entered MSSP in 2016 as an ACO serving solely nursing facility residents with Traditional Medicare coverage.
• Now has over 6,000 assigned beneficiaries with primary care delivered by 500+ employed and contracted providers across 200 Genesis centers
• Achieved $2.3 million in shared savings in 2018, its third year in the MSSP
• In July 2019, entered a new 5-year agreement in the Enhanced Model, assuming downside risk and the potential for up to 75% participation in shared savings.
• Rebranded to LTC ACO and expanded to include residents in unaffiliated nursing facilities, with participating providers and nursing facilities eligible to receive a portion of shared savings earned to create full alignment in improving quality, patient care and healthcare efficiencies.
• Advocacy for quality metrics, risk adjustment methodologies and waiver eligibility (e.g. 3-day hospital stay) to ensure MSSP aligns appropriately with LTC population requirements.
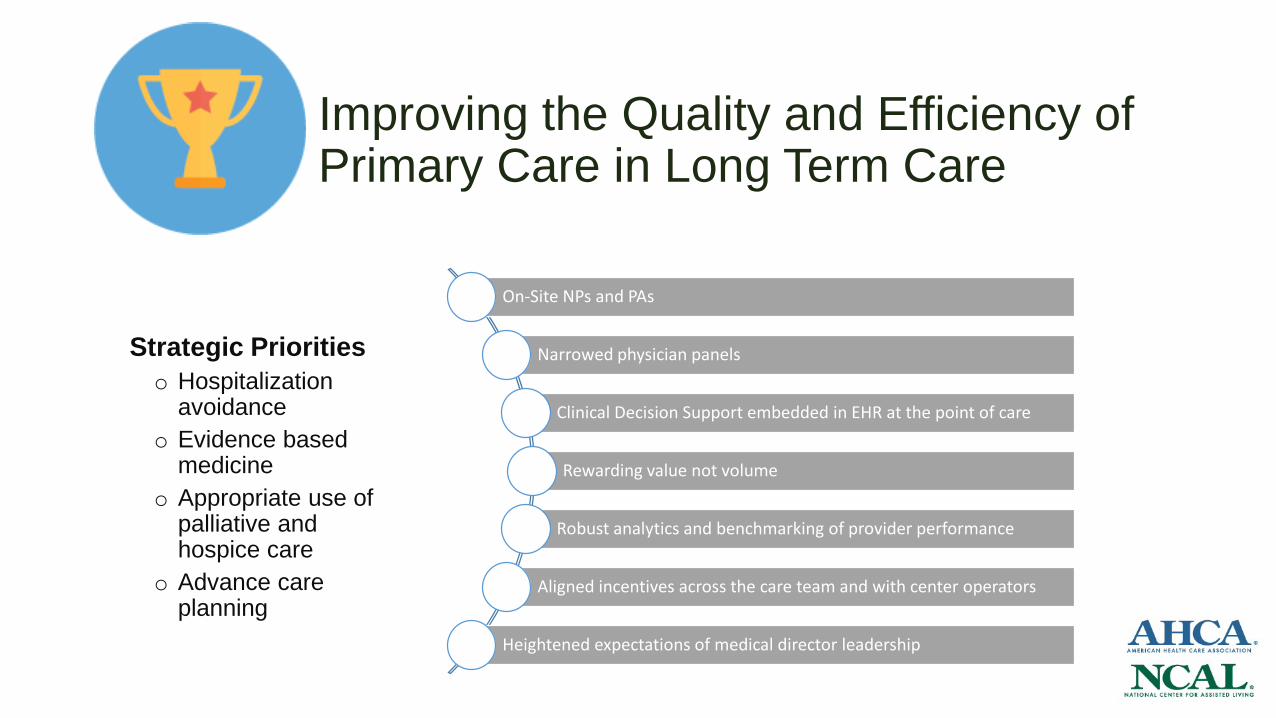
Improving the Quality and Efficiency of Primary Care in Long Term Care
On-Site NPs and PAs
Narrowed physician panels
Clinical Decision Support embedded in EHR at the point of care
Rewarding value not volume
Robust analytics and benchmarking of provider performance
Aligned incentives across the care team and with center operators
Heightened expectations of medical director leadership
Strategic Prioritieso Hospitalization
avoidanceo Evidence based
medicineo Appropriate use of
palliative and hospice care
o Advance care planning

Why Partner with an LTC ACO?• Participation in shared savings provides a new revenue source as the
proportion of Traditional FFS Medicare patients declines and Medicaid mix increases
• Creates a competitive advantage in the recruitment of attending physicians and APPs by allowing an opportunity to participate in both shared savings and an Advanced Alternative Payment Model (APM) that qualifies them for 5% MACRA bonus for their entire Medicare patient billings
• Aligns medical providers with nursing facility goals for improved quality outcomes, including avoidable hospitalizations, and supports evolution of clinical practices, care coordination and quality initiatives
• Enables and supports opportunities for partnership with community-based ACOs based on improving the delivery of efficient, high-quality care
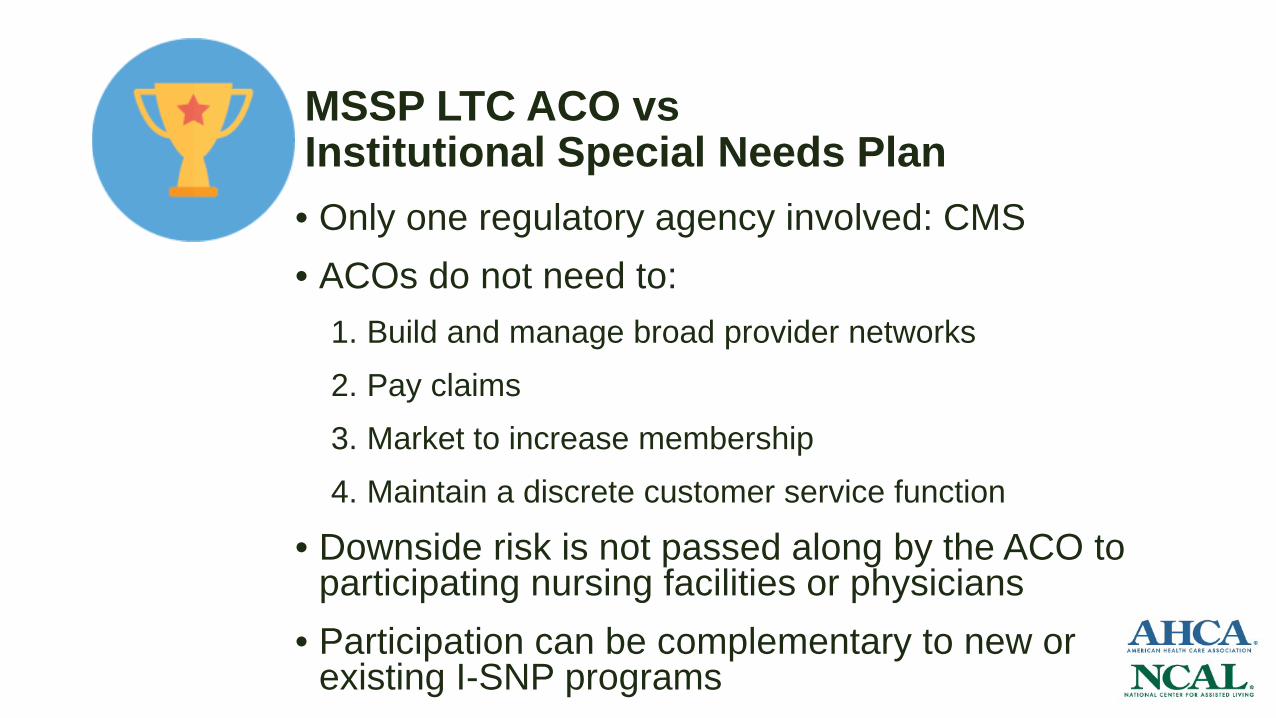
MSSP LTC ACO vs Institutional Special Needs Plan• Only one regulatory agency involved: CMS• ACOs do not need to:
1. Build and manage broad provider networks2. Pay claims3. Market to increase membership4. Maintain a discrete customer service function
• Downside risk is not passed along by the ACO to participating nursing facilities or physicians
• Participation can be complementary to new or existing I-SNP programs
Other Partnership Opportunities Health system partners: Participation in value-based programs
like MSSP increases alignment and improves the SNF profile as hospitals review and update their post acute networks.
• Health plan partners: Commercial payers struggle for ways to identify high quality providers. Participation enables SNFs to better articulate their value proposition from both an outcomes perspective as well as a quality perspective with Medicare Advantage plans, given the high degree of similarity between the two programs. Community-based ACOs: As ACO’s populations age into skilled
nursing and long-term care, the LTC ACO offers an opportunity for partnership across populations to improve outcomes.

Questions?
