acog tumor
DESCRIPTION
acog american obstetrics gynaecology tumor anatomy physiology pathology cancerTRANSCRIPT

Case PresentationsHonduras 2011
Pedro T. Ramirez, M.D.Professor
Director of Minimally Invasive Research & EducationDepartment of Gynecologic Oncology

Cervix

Case Presentation
28 year old G0 with irregular bleeding and CIN-III Medical: NegativeSurgical History: NegativeOBGYN: Menses normal. Paps-History CINIIPelvic exam: No gross cervical lesion
Adnexa normalCone: Adenocarcinoma 3mm invasion + margins
Points of Discussion
• Standard of care
• Options for fertility preservation
• Surgical approach
• Intraoperative decisions

2010 NCCN Guidelines

Surgery
Exploratory laparotomy
Radical trachelectomy
Lymphatic mapping
Bilateral pelvic lymphadenectomy
Frozen: No residual tumor present



Surgical Specimen

Points of Discussion
• Risk of no chance of fertility
• Postoperative complications
• Obstetrical outcomes
• Oncologic outcomes
• Long-term follow up


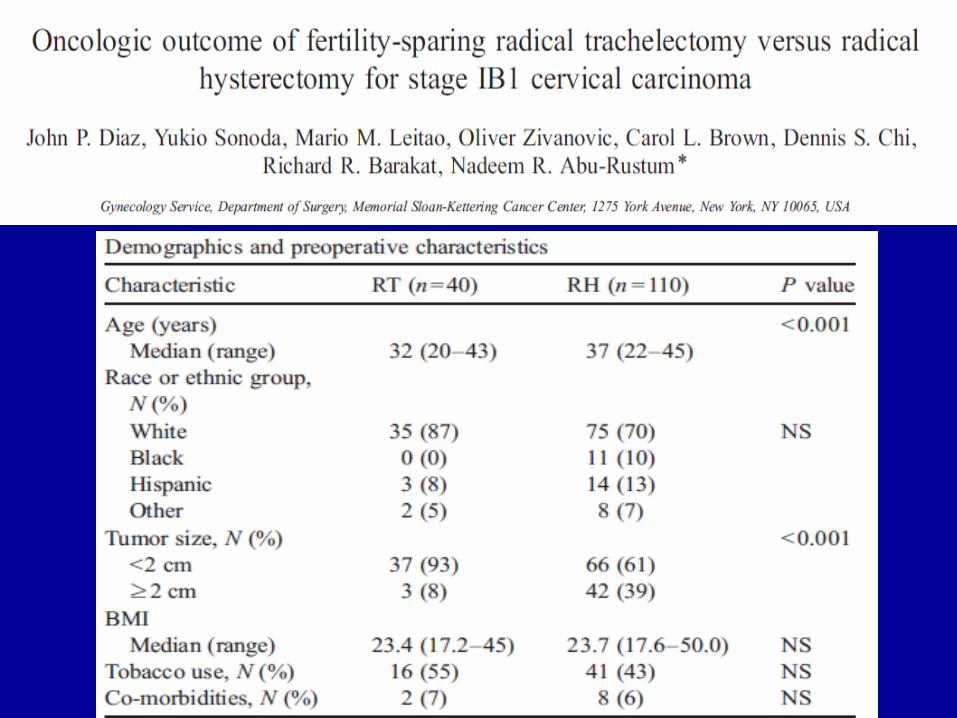


Conclusion:
Radical trachelectomy has similar oncologic outcome to radical hysterectomy
DFS OS

Case Presentation
34 year old G0 with history of stage IIB cervical cancer s/p chemotherapy and radiation
Presentation: Cough
Medical: NegativeSurgical History: NegativePelvic exam: Normal s/p radiation changes
Adnexa and rectal normal

Imaging Studies

Points of Discussion
• Discussion of prognosis
• Role of supportive care
• Options for treatmentGOG-179
GOG-204
• Ongoing trialsGOG-240
Uterine


Case Presentation
46 year old G3P2 obese female with irregular bleeding
Medical: Diabetes & HypertensionSurgical History: CholecystectomyPelvic exam: No gross cervical lesion
Adnexa normalDifficult due to body habitus

Pathology & Imaging Studies
Endometrial biopsy: Complex hyperplasia with atypia

Surgery
Robotic hysterectomy
Bilateral salpingo-oophorectomy
Frozen: G1 endometrioid adenocarcinoma
No invasion
FINAL: G1 endometrioid adenocarcinoma in CAH
No invasion
Points of Discussion
• Preoperative evaluation
• Discussion according to patient age
• Surgical approach
• Intraoperative options
• Postoperative hormone replacement

Case Presentation
38 year old G4P2 female with pelvic pain and bladder pressure
Medical: NegativeSurgical History: Myomectomy-FibroidPelvic exam: 26 cm irregular uterus
Adnexa non-palpableCervix normal

Imaging Studies

Surgery
Exploratory laparotomy
Total abdominal hysterectomy
Bilateral salpingo-oophorectomy
Frozen:
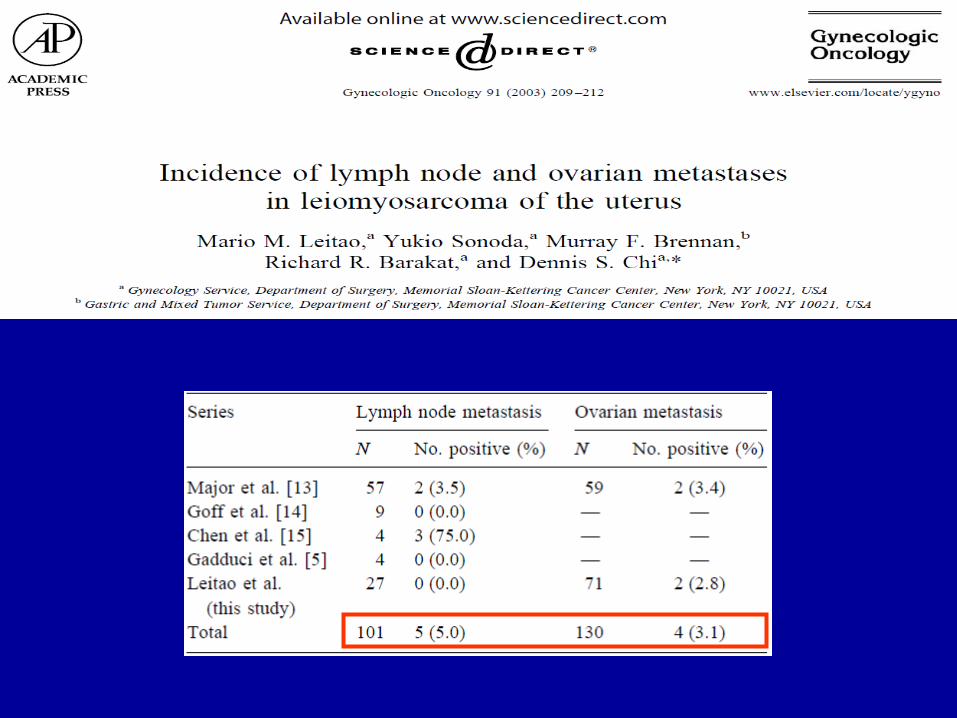
FINAL: Uterine leiomyosarcoma
Tumor size: 24 cms
R ovary-leiomyosarcoma

Points of Discussion
• Preoperative evaluation
• Surgical approach
• Role of intraoperative frozen section
• Indications for lymphadenectomy
• Postoperative therapy


Ovary

Case Presentation
30 year old G0 with dyspareunia. Medical and Surgical History: NegativeOBGYN: Menses normal. No STDs. Paps NormalPelvic exam: Bilateral adnexal masses
Cervix normal

Imaging and Laboratory Studies
CA125: 13.3 U/mL (<35)
AFP: 2.9 ng/mL (<5)
Inhibin B: 123 pg/mL (<139)
LDH: 449 IU/L (313-618)

Surgery
May 23, 2011Exploratory laparotomy
R salpingo-oophorectomy
L cystectomy

Points of Discussion
• Differential diagnosis
• Options for follow up vs. surgery
• Surgical approach
• Intraoperative options
• Postoperative counseling

Case Presentation
68 year old G0 with abdominal bloating and worsening shortness of breath.
Medical: Congestive heart failure and emphysemaSurgical History: Bilateral salpingo-oophorectomyExam: Decreased breath sounds L
Abdomen distended and firmPelvis: Firm nodularity in cul-de-sac

Imaging and Laboratory Studies
CA125: 1,043 U/mL (<35)
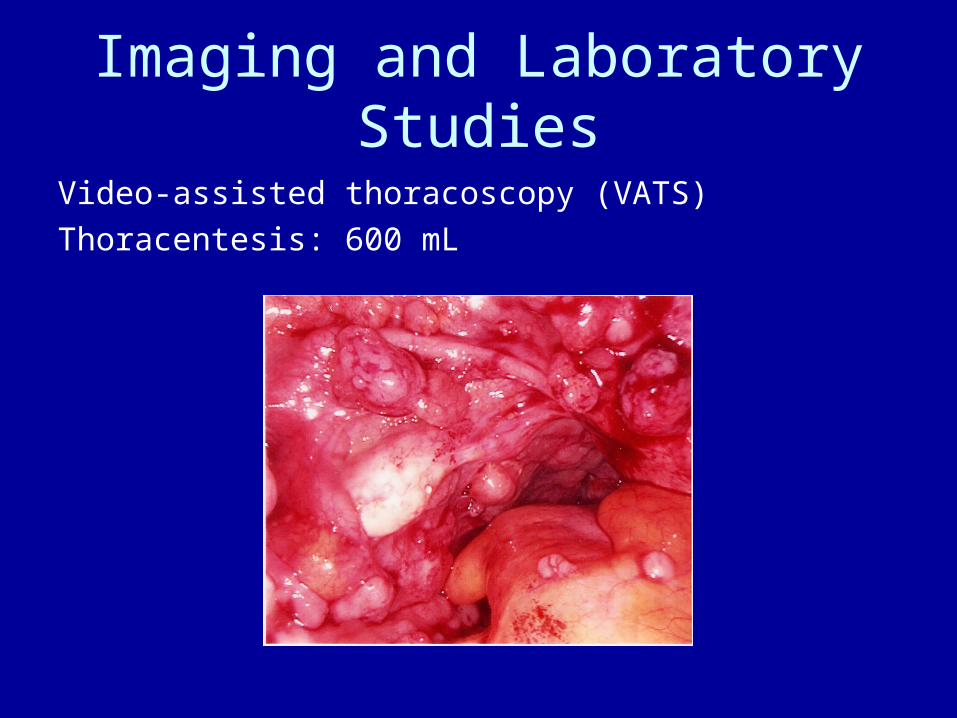
Imaging and Laboratory Studies
Video-assisted thoracoscopy (VATS)
Thoracentesis: 600 mL

Pathology
CT-Guided biopsy:
HG papillary serous carcinoma consistent with mullerian primary
Interval Cytoreductive Surgery• Chemotherapy followed by surgery
3 cycles---Surgery---3 cycles
• Patients who are NOT good surgical candidates -Multiple liver or lung metastases-Suprarenal lymph nodes-Mesenteric adenopathy
• Recent European study shows NO difference in survival

Points of Discussion
• Considerations of work-up evaluation
• Options offered to the patient
• Treatment implementation
• Strategies for follow up

Case Presentation
32 year old G0 with R pelvic pain. Medical: History of breast cancer at age 30.Surgical History: AppendectomyExam: Abdominal tenderness in R to deep palpation
Pelvis: Mobile palpable mass in pelvis ~12 cmsSocial: Patient due to be married in 6 weeks

Imaging and Laboratory Studies
CA125: 78 U/mL (<35)

Surgery
Exploratory laparotomy
R salpingo-oophorectomy
Pelvic and para-aortic lymphadenectomy
Omental biopsy
Peritoneal biopsies
Frozen:

Points of Discussion
• Considerations of work-up evaluation• Options offered to the patient• Risk factor discussion for ovarian cancer• Subset of histopathologic subtypes:
-non-invasive implants
-invasive implants
-micropapillary pattern
• Indications for treatment• Discussions on recurrent disease
Case Presentation
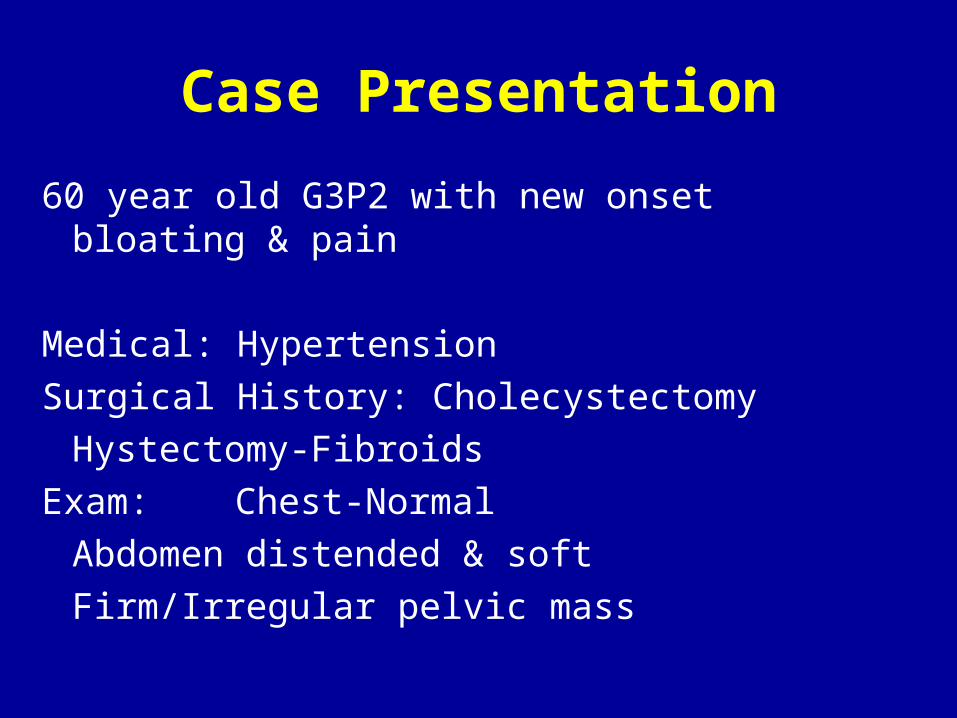
60 year old G3P2 with new onset bloating & pain Medical: HypertensionSurgical History: Cholecystectomy
Hystectomy-FibroidsExam: Chest-Normal
Abdomen distended & softFirm/Irregular pelvic mass

Imaging and Laboratory Studies
CA125: 1,565 U/mL (<35)

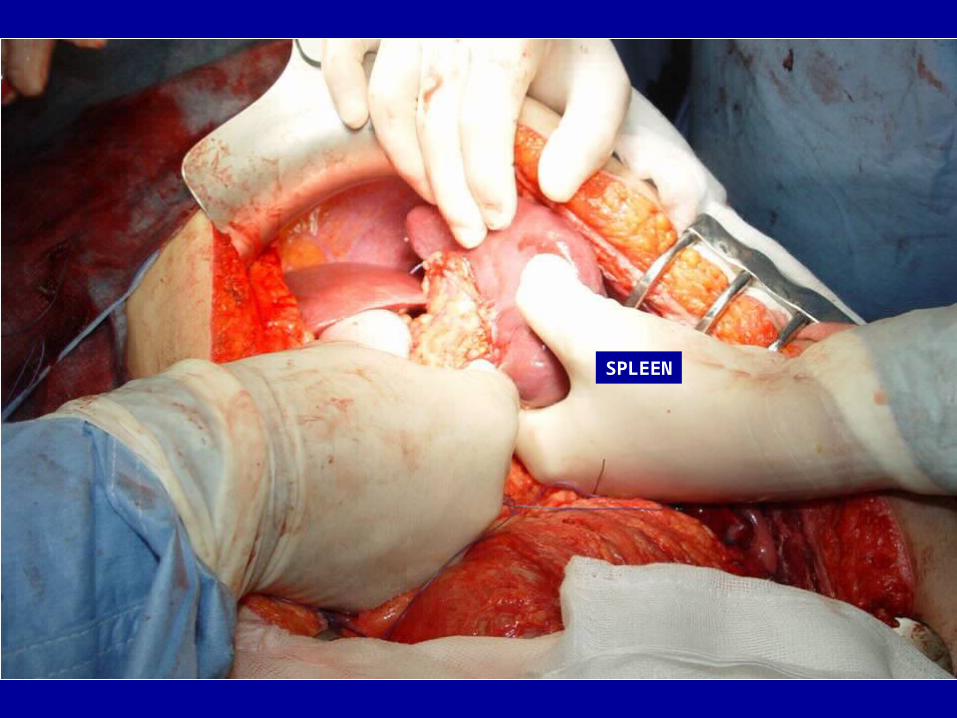
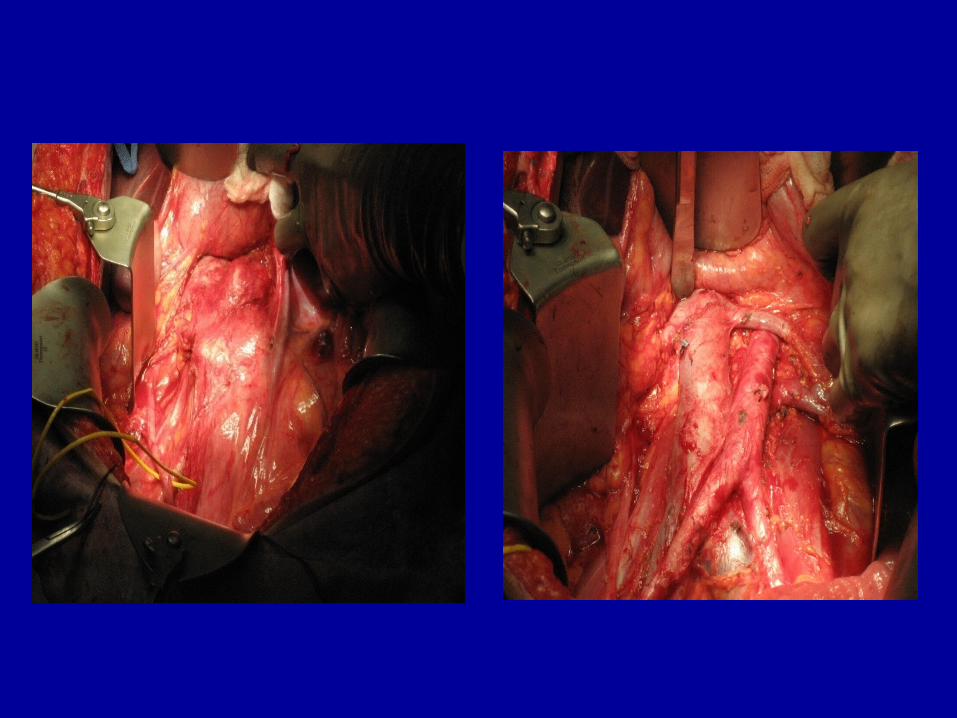
Surgery
Exploratory laparotomy
Bilateral salpingo-oophorectomy
Omentectomy
Splenectomy
Partial liver resection
Para-aortic radical lymphadenectomy
Diaphragmatic stripping
Recto-sigmoid resection with re-anastomosis
Frozen: HG serous neoplasm


SPLEEN



Points of Discussion
• Role of gynecologic oncologist
• Preparation for surgery-Multidisciplinary
• Extent of surgery-Intraoperative decisions
• Treatment implementation-IV vs IP
• Role of consolidation therapy
• Strategies for follow up

Post-operative CoursePOD # 4
Increasing acute abdominal pain and vomiting
Fever and elevated WBC count
Significant abdominal
tenderness

MD Anderson Cancer Center