act enhanced exposure handout version
TRANSCRIPT

4/8/14
1
Integra(ng Acceptance and Commitment Therapy with Exposure Therapy to Enhance the Treatment of
Obsessive-‐Compulsive Disorder
Kim Rockwell-‐Evans, Ph.D. ADAA, 2014
Disclosure
Co-‐author of: Handling your OCD: A=ack of the Brain Monster
My Mission Today
• To provide you with a case example demonstraGng ACT enhanced exposure
Evidence Based Treatment for OCD
ERP is the gold standard • Outcomes – 60 – 85% effecGve
AND • 15 -‐ 40% don’t respond • 25 -‐ 50% disconGnue treatment prematurely or relapse in the long term
• 15 -‐ 25% refuse to parGcipate in ERP What can we do with these sufferers?
Ra(onale for Enhancing ERP with ACT
• ACT is transdiagnosGc – Comorbidity impacts treatment outcomes • 50% have experienced at least one depressive disorder • GAD, panic disorder, social phobia – range from 30 – 45%
• Emphasis on psychological flexibility targeGng the ACT core processes can help clients live a CBT lifestyle
Ra(onale for Enhancing ERP with ACT
Consistent with recent research suggesGng that: • Inhibitory learning is at the heart of fear exGncGon – Original associaGon between the condiGoned sGmulus and uncondiGoned sGmulus remain, while alternaGve associaGon is being formed
• Within session habituaGon is not a reliable indicator of learning
• HabituaGon is not a predictor of outcome
Craske, et. al 2008
4/8/14
2
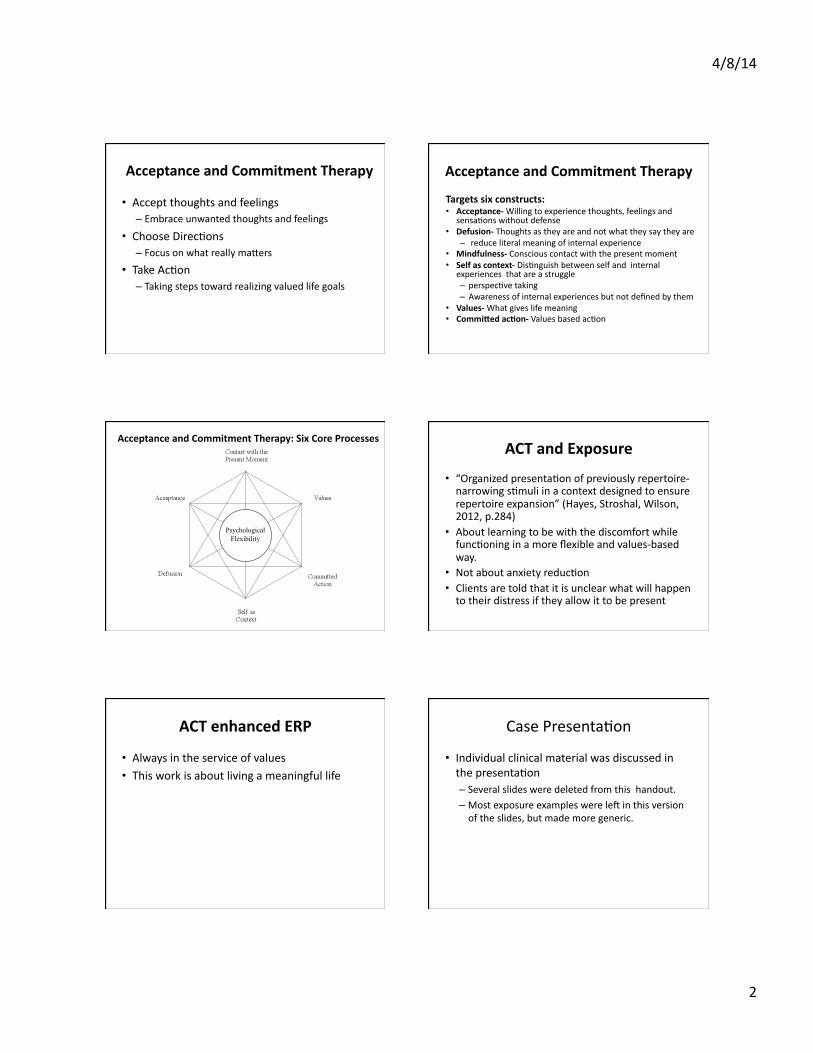
Acceptance and Commitment Therapy
• Accept thoughts and feelings – Embrace unwanted thoughts and feelings
• Choose DirecGons – Focus on what really ma=ers
• Take AcGon – Taking steps toward realizing valued life goals
Acceptance and Commitment Therapy
Targets six constructs: • Acceptance-‐ Willing to experience thoughts, feelings and
sensaGons without defense • Defusion-‐ Thoughts as they are and not what they say they are – reduce literal meaning of internal experience
• Mindfulness-‐ Conscious contact with the present moment • Self as context-‐ DisGnguish between self and internal
experiences that are a struggle – perspecGve taking – Awareness of internal experiences but not defined by them
• Values-‐ What gives life meaning • CommiQed ac(on-‐ Values based acGon
Psychological Flexibility
Acceptance and Commitment Therapy: Six Core Processes ACT and Exposure
• “Organized presentaGon of previously repertoire-‐narrowing sGmuli in a context designed to ensure repertoire expansion” (Hayes, Stroshal, Wilson, 2012, p.284)
• About learning to be with the discomfort while funcGoning in a more flexible and values-‐based way.
• Not about anxiety reducGon • Clients are told that it is unclear what will happen to their distress if they allow it to be present
ACT enhanced ERP
• Always in the service of values • This work is about living a meaningful life
Case PresentaGon
• Individual clinical material was discussed in the presentaGon – Several slides were deleted from this handout. – Most exposure examples were lef in this version of the slides, but made more generic.

4/8/14
3
Developing Crea(ve Hopelessness
• Goal: Help clients see the uselessness of their control agenda
• Clients can consider giving up strategies where their experience says “this doesn’t work”
• Explore client’s experience of what hasn’t been working – What have your tried? – How has it worked for you? – What has it cost you?
• Opens up to doing something new • Precursor to willingness
Introducing Treatment with a Finger Trap
• Pulling away from anxiety just gets you stuck – More effecGve to lean in to
anxiety
• Seems logical to pull away • Pulling away from anxiety
is restricGng • “Don’t think of a pink
elephant” – Paradoxical effect of
thought suppression
Effec(ve Strategy is Counterintui(ve
• Ahtude of curiosity • Expect anxiety to occur • Seek out opportuniGes to pracGce embracing what anxiety wants you to avoid
• Rigid a=empts to control anxiety is the problem, not the soluGon
• A=empts to end doubt and distress just increase it
Examining the Effects of Anxiety Control Efforts
Tug of War with the Monster
Window to Your Values
Family Marriage
Is there room for your loved ones when you are in the struggle?
Exposure Ideas What behaviors come to mind that are like dropping the rope?
• Looking at children and a=racGve women
• Thinking disturbing thoughts on purpose • Allowing doubt to sit • Not asking for reassurance or confessing • Using knives around wife • InteracGng with children • Not locking bedroom door and placing chairs at the door
when visiGng family
A detailed list with specific exposure tasks was generated

4/8/14
4
Homework
• Watch “Demons on the boat” you tube video • ConGnue informal mindfulness task
• Reassurance/confession book – Write thoughts and confessions in a book and have wife review it and write a one sentence response every two days
– Observe thoughts, sensaGons, feelings
Metaphor: Demons on the Boat Targets all six ACT processes
Russ Harris and Joe Oliver
Willingness as an Alterna(ve to Control • Lack of willingness will undermine the therapy • Clients must give up the control agenda – Fully embrace and open up to what shows up
• Are you willing to experience anxiety without defense if that means _______ ?
• Willingness scale of 0 to 10 – 0 = Completely closed to experiencing thoughts, feelings and sensaGons as they are
– 10 = Completely open to experiencing thoughts, sensaGons and feelings as they are • Directly without changing it • Avoiding it • ManipulaGng it
• If Willingness is not at a 10, rethink strategy • Precursor to acceptance
Willingness as an AlternaGve to Control
• Two sides of a card • “Are you willing to have these thoughts and feelings in order to have the relaGonship you want with your wife and family?”
• “It’s unlikely that you can have one without the other”
• “Is it worth it to you?”
“I might be a child molester” “I might harm my family” “I might give my wife AIDS”
Anxiety feelings and sensaGon
Marriage and Family
Surfing Anxiety
• “Surf” with the ups and downs of the anxiety
• Stay with it • Observe sensaGons, thoughts and feelings
In Session Exposure Example Doubt Induc(on Task
• Say these thoughts on purpose with varying tempo: – “I might be a child molester” – “I’ll never know for sure” – “Maybe I’m a child molester, maybe I’m not, there is no way to be sure”
– “I’m going to be with this uncertainty” • Then, state thoughts while looking at photos of wife and family,
• Lastly, he wrote “I might be a child molester” on a small sheet of paper and put it in his pocket for the rest of the session
Observe sensaGons, feelings and thoughts

4/8/14
5
In Session Exposure Example
• Exposure task was connected to values • Willingness raGng obtained prior to exposure • Exposure was described as being a way to pracGce being with the anxiety related to obsessions without doing compulsions
• Stay in the moment with the experience • Seek out discomfort and describe in detail • Obtained SUDS raGng for the purpose of introducing a more challenging task
Imaginal Exposure
• Write a newspaper arGcle about being caught for molesGng a child
• Imagery scripts – Client is very creaGve – Had thought: “the script was so easy, it must mean I molested a child and didn’t know it.”
– Did a doubt inducGon script on that • “Maybe because it was so easy to write the exposure script, I’m a child molester and molested a child without knowing it. Being creaGve and finding this easy doesn’t prove whether or not I’m a molester. Maybe it means I’m a child molester, and maybe not. I’m going to take a risk and embrace this uncertainty.”
Intrusive Thought Exposure
• Write down intrusive thoughts and read them out loud • Make a digital recording with intrusive thoughts – Thoughts were at random intervals ranging from 5 to 120 seconds
– Vary tempo and volume when saying the thoughts – Listen to recording with a headset for one hour a day while doing a variety of acGviGes and in a variety of sehngs • Running • Doing chores • Reading • Surfing internet • Driving
Addi(onal Exposure Examples
• Sca=er photos of children all over the house. Think “I’m a child molester” when looking at the photos.
• Do not put chair in the way of the bedroom door while sleeping when visiGng family.
• Leave bedroom door slightly opened while sleeping when visiGng family.
• Allow children to sit on his lap.
Physicalizing Exercise Convert subjec(ve experiences into an object
Mental compulsion: like a hurdler with an endless amount of hurdles
Acceptance: Bring it on
What would a sculpture of what you are doing right now look like?
What would willingness look like?
Chessboard Metaphor
• Client says “I’m so stupid to have believed all these thoughts”
• Targets self as context process in ACT • Chess pieces represent thoughts, feelings, sensaGons
• Board holds the pieces and isn’t invested in the outcome

4/8/14
6
Keep in mind-‐
• This case presentaGon is a summary of the highlights of 15 sessions
• ACT is not: – a canned approach – just a bag of tricks
• ACT is: – an experienGal approach – flexible
• Case example is just one way of applying it
• ACT can enhance ERP
ERP and ACT Similari(es
Both target: • Building flexible behaviors • ExperienGal avoidance Both emphasize:
• Experiencing anxiety on purpose • Giving up compulsions
Key Differences: ACT and ERP • ACT focuses on willingness to experience discomfort rather than habituaGon
• ERP is a very effecGve, focused treatment, where ACT is transdiagnosGc
• ACT measures outcome by moving in a valued direcGon rather than anxiety reducGon
• Values are directly linked to exposures in ACT • Concepts are introduced with metaphor or experienGal exercises rather than explanaGons
Take Home Points
• ACT is a flexible, individualized approach that can prepare clients for exposure, enhance exposure, and treat co-‐morbid condiGons
• Research on ACT and OCD is limited, but promising
• ACT is consistent with recent research on inhibitory learning
Future Implica(ons • Research on inhibitory learning can inform our treatment approach (Craske, et. al.) – It’s a game changer! – Consistent with ACT
• We need to review our ERP procedures – Not everyone habituates – HabituaGon doesn’t predict good outcome – SystemaGcally working with a graded hierarchy may not be the most efficient approach
– Focus on toleraGng anxiety instead of reducing it • Maybe we can achieve be=er long term outcomes by doing ACT enhanced ERP?
References • Abramowitz, J.S. (2006). Obsessive-‐compulsive disorder. Cambridge, Massachuse=s:
Hogrefe. • Abramowitz, J.S. & Arch, J.J. (2014). Strategies for improving long-‐term outcomes in
cogniGve behavioral therapy for obsessive-‐compulsive disorder: Insights from learning theory. CogniGve and Behavioral PracGce, 21, 20-‐31.
• Craske, M.G., Kircanski, K., Zelikowsky, M., Mystkowski, J., Chowdhury, N., & Baker, A. (2008). OpGmizing inhibitory learning during exposure therapy. Behaviour Research and Therapy, 46, 5-‐27.
• Eifert, G.H. & Forsyth, J.P. (2009). Acceptance and commitment therapy for anxiety disorders: Three case studies exemplifying a unified treatment protocol. CogniGve and Behavioral PracGce. 16, 368-‐385.
• Eifert, G.H. & Forsyth, J.P. (2005). Acceptance and commitment therapy for anxiety disorders. Oakland, California: New Harbinger PublicaGons, Inc.
• Forsyth, J.P. & Eifert, G.H. (2007). The mindfulness and acceptance workbook for anxiety. Oakland, California: New Harbinger PublicaGons, Inc.
• Grayson, J. (2003). Freedom from obsessive-‐compulsive disorder. New York: Penguin Group, Inc.
• Harris, R. (2008). The happiness trap: How to stop struggling, and start living. Boston, Massachuse=s: Trumpeter Books.
• Hayes, S.C. (2005). Get out of your mind and into your life. Oakland, California: New Harbinger PublicaGons, Inc.
• Hayes, S.C., Strosahl, K.D. & Wilson, K.G. (2012). Acceptance and commitment therapy. The process and pracGce of mindful change. (2nd ediGon). New York, New York: Guilford Press.
• Siegel, R.D. (2010). The mindful soluGon. New York, New York: Guilford Press.

4/8/14
7
References
• Twohig, M.P. (2012). The basics of acceptance and commitment therapy. CogniGve and Behavioral PracGce, 19, 499-‐507.
• Twohig, M.P., Hayes, S.C., Plumb, J.C., Prui=, L.D., Collins, A.B., Hazle=-‐Stevens, H., & Woidneck, M.R. (2010). A randomized clinical trial of acceptance and commitment therapy vs. progressive relaxaGon training for obsessive compulsive disorder. Journal of ConsulGng and Clinical Psychology, 78, 705-‐716.
• Twohig, M.P., Hayes, S.C., & Masuda, A. (2006). Increasing willingness to experience obsessions: Acceptance and commitment therapy as a treatment for obsessive compulsive disorder. Behavior Therapy, 37, 3-‐13.
• Twohig, M.P. (2009). The applicaGon of acceptance and commitment therapy to obsessive-‐compulsive disorder, 16, 18-‐28.
• Twohig, M.P., Moran, D.J., & Hayes, S.C. (2007). A funcGonal contextual account of obsessive-‐compulsive disorder. In Understanding behavior disorders. Oakland, California: Context Press.
• Vervliet, B., Craske, M.G. & Hermans, D. (2013). Fear exGncGon and relapse: State of the art. Annual Review of Clinical Psychology, 9, 215-‐248.
Contact Informa(on:
Kim Rockwell-‐Evans, Ph.D. 375 Municipal Drive, Suite 230
Richardson, Texas 75080
214-‐368-‐6999