actualités sur l’hyperphosphatémie et le métabolisme ... · actualités sur...
TRANSCRIPT

Actualités sur l’Hyperphosphatémie et
le Métabolisme Minéralo-Osseux de
l’Insuffisance Rénale Chronique
Dr Pablo Ureña TorresClinique du Landy23, rue du Landy. 93400 Saint [email protected]

Phosphate Metabolism
Phosphorus
- One of the most abundant anions in the body
(500 to 800 g or 20-30 moles)
- Mostly bound to oxygen (PO4 or Phosphate)
Functions- Mineral : Teeth/Bone. Hydroxyapatite (Ca10(PO4)6(OH)2
85% in bone (500 à 800 g)- Reserve and transfer of energy (ATP)- pH regulation- Intracellular signal transduction (second messenger)- Cellular membrane composition (phospholipids)- Nucleic acids constituent- Oxygen dissociation from Hb (2-3 DPG),NAD coenzyme, etc

Phosphate Distribution
Bone
500
0
1000A
mo
un
t (g
)
Cells(Intracellular)
Fluids(Extracellular)
600 g20 000 mmol
63 g 0.5 g
- The most abundant anion in the body (700 g = 23 000 mmol)- Intracellular (80-120 mmol/l IC and only 1-1.5 mmol/l plasma)
- Minimum needs in a healthy adult : 300 mg/day
85-90 %
Plasma = 0.02% = 130 mg
Hydroxyapatite
9 % 1 %

De Boer IH, et al., NHANES III. AJKD 53:399-407, 2009
Serum Phosphate Concentration
0,80 0,80 0,80 0,80 –––– 1,45 mmol/L1,45 mmol/L1,45 mmol/L1,45 mmol/L (2.6 to 4.6 m/dL)(2.6 to 4.6 m/dL)(2.6 to 4.6 m/dL)(2.6 to 4.6 m/dL)Inorganic Phosphate =Orthophosphate et pyrophosphosphate
Total Plasma Phosphate = 3,9 mmol/l
15,513 subjects
3.2
3.7
Fasting
Non fasting
Serum phosphorus (mg/dL)
Morning Afternoon Evening
3.3
3.4
3.5
3.6

Serum Phosphate Concentration
De Boer IH, et al., NHANES III. AJKD 53:399-407, 200915,513 subjects
NHW
Serum phosphorus (mg/dL)
3.2
NHB
Age Gender Race/Ethnicity
3.3
3.4
3.5
3.6
H
Men
Women20-29
30-39
40-49
50-5960-69
70-79
80-90
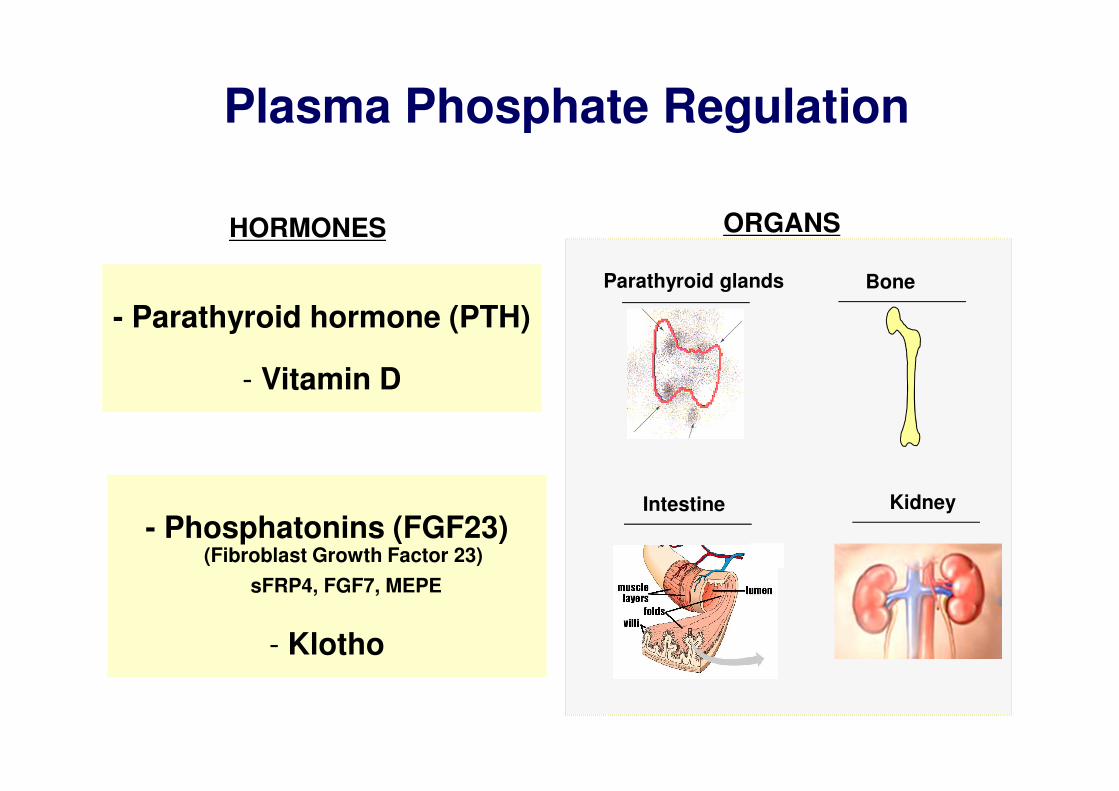
Plasma Phosphate Regulation
- Parathyroid hormone (PTH)
- Vitamin D
HORMONES
- Phosphatonins (FGF23)(Fibroblast Growth Factor 23)
sFRP4, FGF7, MEPE
- Klotho
ORGANS
Bone
Intestine Kidney
Parathyroid glands

Plasma Phosphate Regulation
Intestine
1400 mg/d(Diet)
500 mg(Feces)
1100 mg
200 mg
900 mg(Net
absorption )
ExtracellularPool 550 mg
(Plasma pool130 mg or
0.80-1.45 mmol/L)
60-70%
(NPT2b)
?2Na+
HPO42-
85%
15%
PO4
Kidney
Bone
FGF23
Parathyroid glands
PTH
Active Vitamin D
NPT2aNPT2cKlotho
1400 mg900 mg(Urine)
NET INTESTINAL PO4 ABSORPTION
mmol/day
0 10 20 30 40 50 60 70 80 90 100
0
-10
-20
10
20
30
40
50
60
70
NET IN
TESTINAL PO4 ABSORPTION
mg/day
-500
0
500
1000
1500
2000
DIET PO4, mg/day
0 500 1000 1500 2000 2500 3000
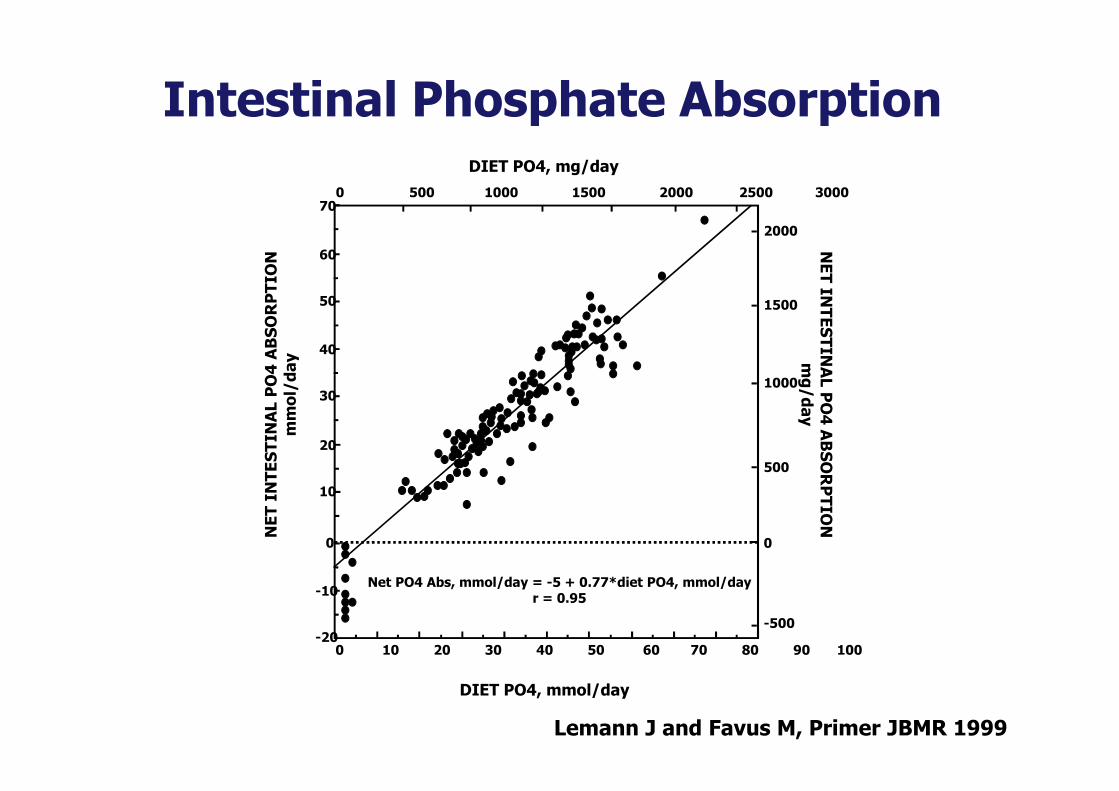
Net PO4 Abs, mmol/day = -5 + 0.77*diet PO4, mmol/dayr = 0.95
DIET PO4, mmol/day
Lemann J and Favus M, Primer JBMR 1999
Intestinal Phosphate Absorption

Rufino M., et al., Nephrol Dial Transplant 61:94, 1998
Relationship between Protein Intake and Phosphate Intake
APPORTS PHOSPHATES
(mmol/jour)
0 50 100 150 200 250 300 350
0
20
40
60
80
100
120
140
y = 0,4316xR2 = 0,8252N = 559
APPORTS PROTIDIQUES(g/jour)
100 g protéines = 43 mmol phosphates

Phosphate Intake,
Demography, Cardiovascular Risk Factors, and Kidney Function Explain Only
12% of Variation in Serum
Phosphate Levels
(NHANES III)
De Boer IH, et al., AJKD 53:399-407, 200915,513 subjects

Frequence of Hyperphosphatemia in CKD Patients
PTH > 60 pg/ml Hb < 11.0 g/dL Bicarbonate < 22 mM Potassium > 5.0 mM Phosphate > 1.38 mM
Moranne O. , and the Nephrotest Study Group. JASN 2008
25 %

Hyperphosphatemia in CKD Patients
Martinez I et al. Am J Kidney Dis 1997;29:496–502
*P < 0.05, compared with CrCl ≥ 50 mL/min
0
mm
ol/
L
Creatinine clearance (mL/min)
0.75
1.00
1.25
1.50
Serum ionized calcium
Phosphorus
0.50
0
5.4
10.8
16.2
21.6
pm
ol/
L
iPTH
*
*** *
*
Creatinine clearance (mL/min)
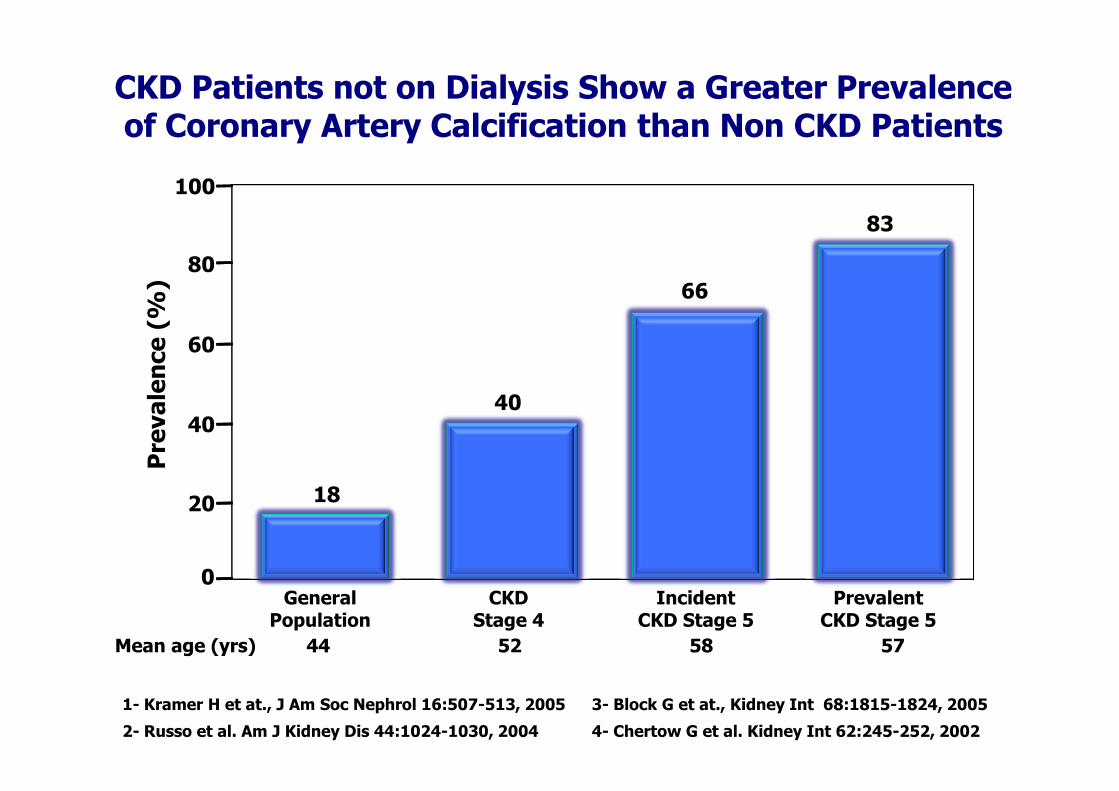
CKD Patients not on Dialysis Show a Greater Prevalence of Coronary Artery Calcification than Non CKD Patients
1- Kramer H et at., J Am Soc Nephrol 16:507-513, 2005
2- Russo et al. Am J Kidney Dis 44:1024-1030, 2004
Prevalence (%)
0General
Population
20
40
60
80
CKDStage 4
IncidentCKD Stage 5
PrevalentCKD Stage 5
100
18
40
66
83
Mean age (yrs) 44 52 58 57
3- Block G et at., Kidney Int 68:1815-1824, 2005
4- Chertow G et al. Kidney Int 62:245-252, 2002

Serum Phosphate Levels and Coronary Artery Calcification
Tomiyama C et al. Nephrol Dial Transplant 21:2464-2471, 2006
Serum Phosphate Levels (mg/dL)
5.5
3.0
3.5
4.0
4.5
5.0
CACS ≤ 400n = 74
3.7 mg/dL(1.20 mmol/L
4.2 mg/dL(1.40 mmol/L
P = 0.013
CACS ≥ 400N = 22
Patients with CKD Stages 2-4

- Nishioka et al. N Engl J Med349:e12, 2003
- Phosphatemia and CAC ScoreTomiyama C et al. NDT 21:2464-2471, 2006
Hyperphosphatemia and Vascular Calcifications

CKD Patients not on Dialysis Are More Likely to Die than Progress to ESRD Dialysis Therapy
RRT = Renal Replacement Therapy
Keith D et al., Arch Intern Med 164:659-663, 2004

High Serum Phosphate Levels are Associted with Increased Risk of Mortality in CKD Patients not on Dialysis
Kestenbaum B et al., J Am Soc Nephrol 16:520-528, 2005

L’Axe Fibroblast Growth Factor 23-
Klotho dans l’Homéostasie du
Phosphate en Cas de MRC
Rein : FGF23/Klotho/NPT2a
Intestin : NPT2b
Parathyroïde : Klotho/FGFR1/FGF23

L’Axe Fibroblast Growth Factor 23-
Klotho dans l’Homéostasie du
Phosphate en Cas de MRC
Rein : FGF23/Klotho/NPT2a
Intestin : NPT2b
Parathyroïde : Klotho/FGFR1/FGF23

Circulating FGF23 Molecules
Urena P et al. Kidney Int 73:102-107, 2008Dr D. Prié, personal data
- Circulating at low concentration in normal subjects
0 10 20 30 40 50
FGF-23 intact (pg/ml)
% of subjets
0
5
10
15
20
25
30
Intact FGF23 by ELISA from Kainos Lab.Normal mean values : 29 ± 28 pg/ml
Normal range 0-40 pg/ml
C-terminal FGF23 by ELISA from Immutopics Lab.Normal mean values : 57 ± 43 rU/ml
Normal range 0-130 rU/ml
50
75
25
0
100
FGF23 (rU/ml)
C-Terminal FGF-23

Circulating FGF23 in CKD is Mainly the Intact Molecules
Shimada et al. WCN-ERA-EDTA 2009. Unpublished data
Dr D. Prié, personal data
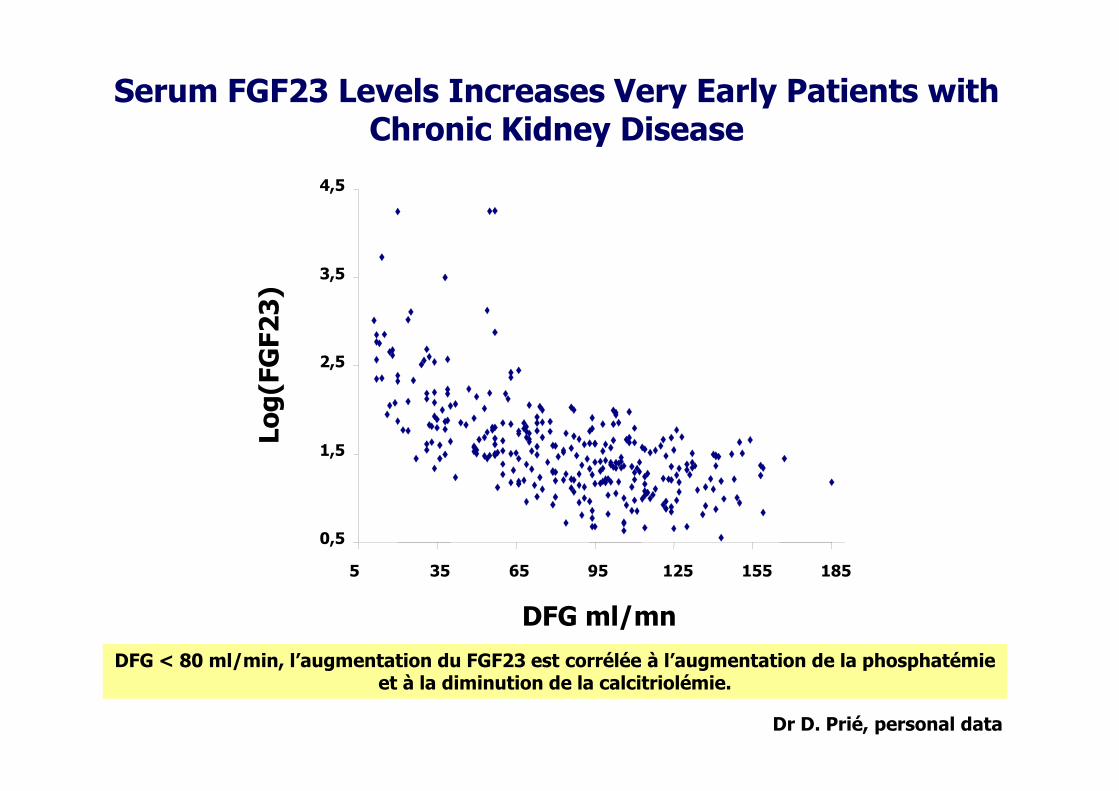
DFG < 80 ml/min, l’augmentation du FGF23 est corrélée à l’augmentation de la phosphatémie et à la diminution de la calcitriolémie.
Serum FGF23 Levels Increases Very Early Patients with Chronic Kidney Disease
Log(FGF23)
DFG ml/mn
0,5
1,5
2,5
3,5
4,5
5 35 65 95 125 155 185

The Renal Expression of Klotho mRNA isDown-Regulated in CKD Patients
Koh N et al. BBRC 280:1015-1020, 2001
RNAse protection assay
kl s = secreted formKl m : membrane form
F1-F9 = CRF kidneysC1-C3 : Control kidneys
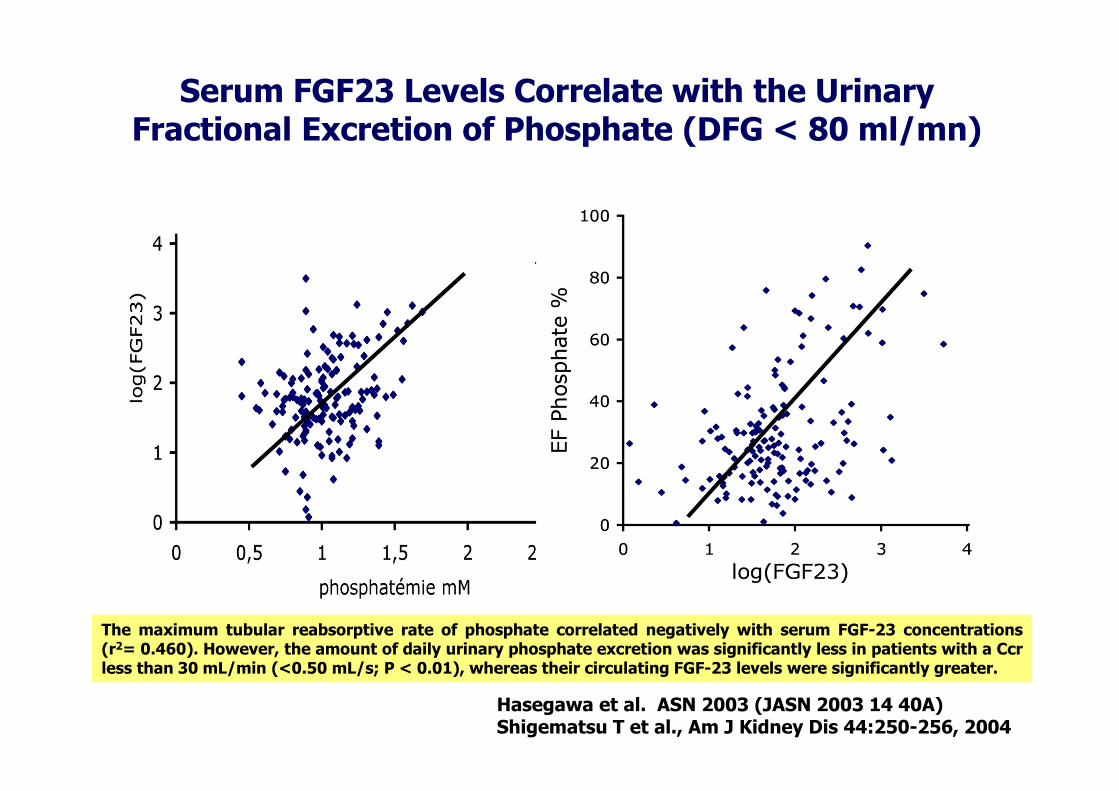
Hasegawa et al. ASN 2003 (JASN 2003 14 40A)Shigematsu T et al., Am J Kidney Dis 44:250-256, 2004
Serum FGF23 Levels Correlate with the Urinary Fractional Excretion of Phosphate (DFG < 80 ml/mn)
The maximum tubular reabsorptive rate of phosphate correlated negatively with serum FGF-23 concentrations(r2= 0.460). However, the amount of daily urinary phosphate excretion was significantly less in patients with a Ccrless than 30 mL/min (<0.50 mL/s; P < 0.01), whereas their circulating FGF-23 levels were significantly greater.

In CKD animals the injection of antibodies against FGF-23 normalizes serum calcitriol levels
Serum FGF23 Levels Correlate Negatively with Calcitriol and Positively with PTH (DFG < 80 ml/mn)
Hasegawa et al. ASN 2003 (JASN 2003 14 40A)

Manipulating Serum Phosphate with Phosphate Binders Can Reduce Serum FGF23 Levels in Uremic Rats
Nagano N et al. Kidney Int 69;531-537, 2006

Mineral Metabolism in Patients with Mild Chronic Kidney Disease: Origin of Secondary Hyperparathyroidism
Isakova T et al. JASN, 2008
PTH
CKD II-III
Calcemia
Normal
FE Ca
FGF23Normal = 50 pg/mlCKD II-III = 75 pg/ml

Non Progressors Progressors
FGF23 35± 58 69± 70
(pg/ml)
Phosphate 1.04 ± 0.38 1.25 ± 0.27
(mmol/ml)
PTH 6± 5 22 ± 20
(pg/ml)
Fliser D et al. JASN 18:2601-2608, 2007

L’Axe Fibroblast Growth Factor 23-
Klotho dans l’Homéostasie du
Phosphate en Cas de MRC
Rein : FGF23/Klotho/NPT2a
Intestin : NPT2b
Parathyroïde : Klotho/FGFR1/FGF23

NPT2b and Intestinal Phosphate Absorption in CKD
Phosphate (P32) Uptake NPT2b mRNA
Marks J et al. Kidney Int 72:166-173, 2007

Sabbagh Y et al., ASN 2008
Intestinal Phosphate Absorption in NPT2b-/-Mice
[SA-FC343] Importance of Npt2b in Phosphate Homeostasis: Characterization
of the Conditional Npt2b Knockout MouseYves Sabbagh, Stephen P. O'Brien, Wenping
Song, Adam Stockmann, Cynthia Arbeeny, Susan C. Schiavi. Renal Sciences, Genzyme Corporation,Framingham, MA
Standard diet (0.6% of Phosphate)NPT2b-/- mice have : - hypophosphatemia
- hypophosphaturia2 folds more phosphate in the feces than the WT mice
Under low phosphate diet (0.02% of Phosphate), after intestinal administration of 1.6 M of phosphate
- NPT2b-/- mice absorb 40-50% less phosphate than WT- Nicotinamide decrease by 40% intestinal phosphateabsorption in WT mice but have no effect in NPT2b-/-

Nicotinamide Decreases Serum Phosphate Concentration in Dialysis Patients
Takahashi Y et al. Kidney Int 65:1099-1104, 2004
Eto N et al., Nephrol Dial Transplant 20:1378-1385, 2004
2Na+
HPO42-
?
(NPT2b)
2Na+HPO42-
SGLT-1

Evidence For a Intestinal Phosphate Sensor
Berndt T et al. PNAS 104:11085-11090, 2007

L’Axe Fibroblast Growth Factor 23-
Klotho dans l’Homéostasie du
Phosphate en Cas de MRC
Rein : FGF23/Klotho/NPT2a
Intestin : NPT2b
Parathyroïde : Klotho/FGFR1/FGF23

FGF23/FGFR1/Klotho on Parathyroid Glands
Ben-Dov I et al. JCI 117:4003-4008, 2007

Diminution de l’Expression de la Protéine Klotho dans les Glandes Parathyroïdes
Komabe, Fugakawa, et al. WCN-ERA-EDTA 2009. Unpublished data
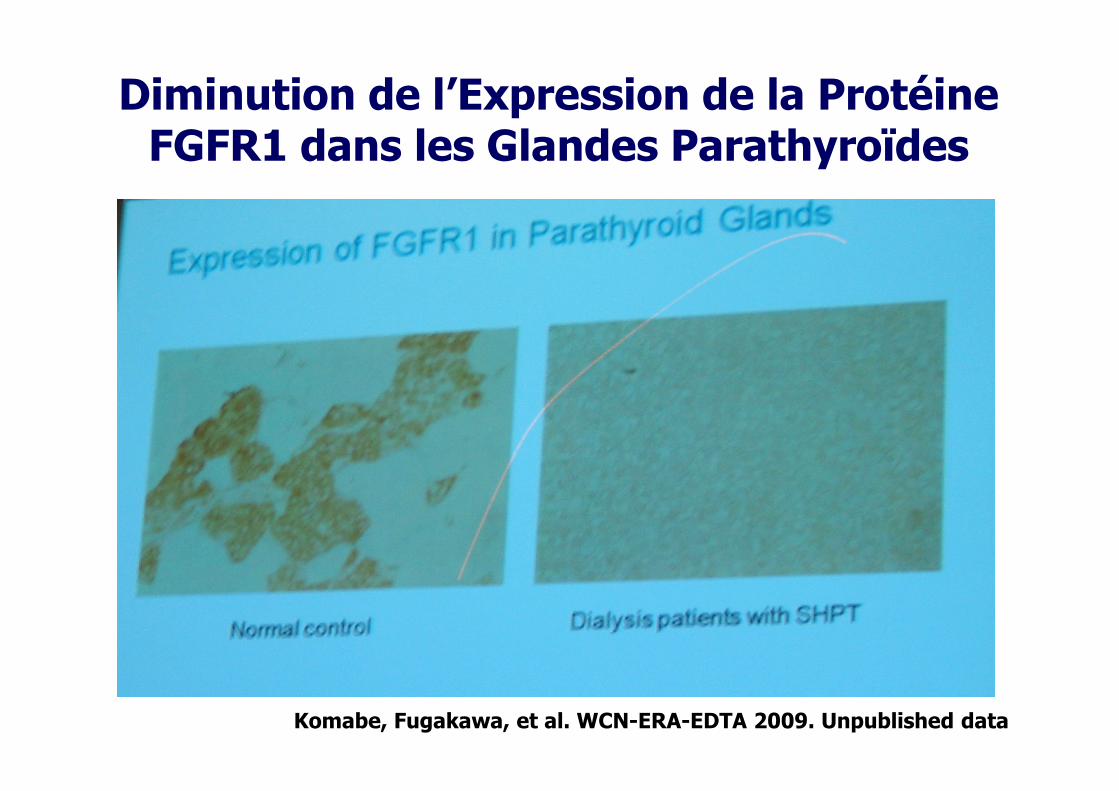
Diminution de l’Expression de la Protéine FGFR1 dans les Glandes Parathyroïdes
Komabe, Fugakawa, et al. WCN-ERA-EDTA 2009. Unpublished data

Serum FGF23 Levels Predict the Severity of Secondary Hyperparathyroidism and Its Response to Vitamin D
100 patients followed for 2 years
Nakanishi et al. Kidney Int 67:1171, 2005
62 patients
24 weeks of calcitriol
treatment
FGF23 before treatment
Response + -
Kazama et al. Kidney Int 67:1120, 2005

Schematic Representation of Factors Regulating Serum Phosphate Levels
Urena P., el al.Kidney Int 71:730-737, 2007
Parathyroids
Kidney
Intestine
Bone
Phosphorus
PhosphorusElimination
PTH
FGF23
?

DominiquePrié Marie
Courbebaisse
ChristineSalaün Alice
RousseauChristineLeroy
DavidDeBrauwere
ValérieBoitez
LaurentBeck
GérardFriedlander
PabloUreña

END