acute coronary syndromes quinn capers iv, md associate dean for admissions director of peripheral...
TRANSCRIPT

Acute Coronary Syndromes
Quinn Capers IV, MDAssociate Dean for AdmissionsDirector of Peripheral Vascular [email protected]

Objectives
1. Understand the biology of coronary plaque rupture2. Understand the the relationship between the intracoronary pathological
findings and the clinical presentations in acute coronary syndromes3. Understand the differences between “stable” and “vulnerable” coronary
plaques4. Describe methods for changing the vulnerable plaque to a stable plaque5. Describe the concept of risk stratification in acute coronary syndromes6. Be familiar with the pathogenesis of coronary thrombosis7. Be able to calculate the TIMI risk score in ACS patients8. Compare and contrast the two major modes of reperfusion therapy in
acute ST elevation MI (STEMI)


• Life-threatening episodes of abrupt decrease in coronary blood flow in the patient with coronary atherosclerotic heart disease
• Continuum (clinical): from unstable angina to ST segment elevation myocardial infarction (STEMI)
• Clinical continuum correlates with degree of coronary artery obstruction, from partial to complete.
Acute Coronary Syndromes Definition
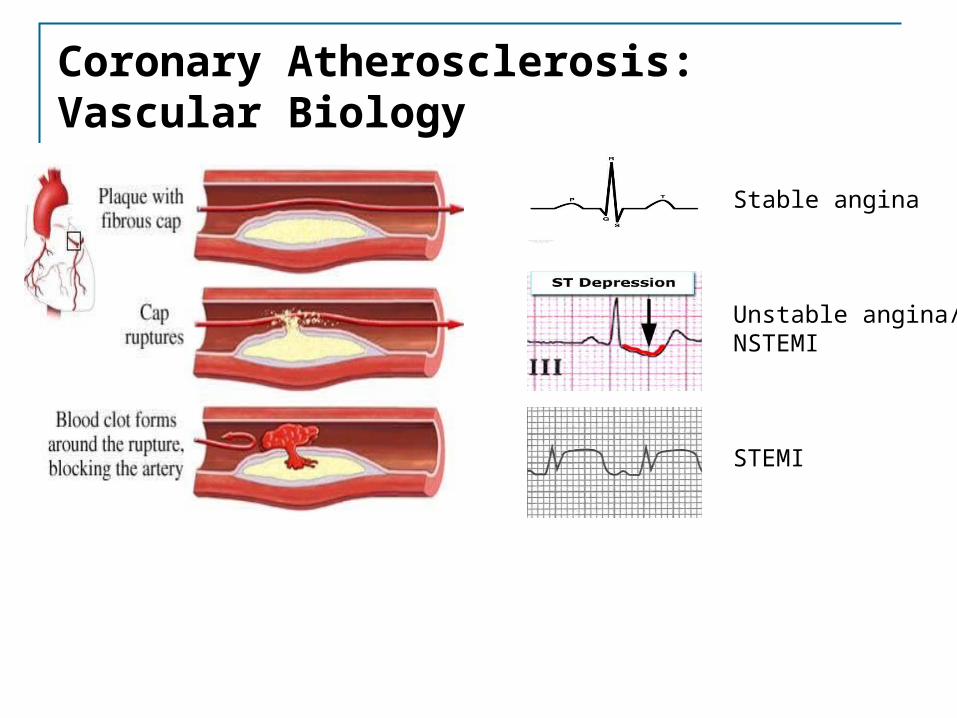
Stable angina
Unstable angina/NSTEMI
STEMI
Coronary Atherosclerosis: Vascular Biology
• Stable plaque:• Chronic, stable exertional angina pectoris• Low inflammatory state
• “Chronic coronary syndromes”
• Unstable or “vulnerable” plaque:• Unstable angina, acute MI• High systemic inflammatory state (CRP, ESR, IL1)• “Acute coronary syndromes”
Acute Coronary SyndromesBiological/Clinical Correlation
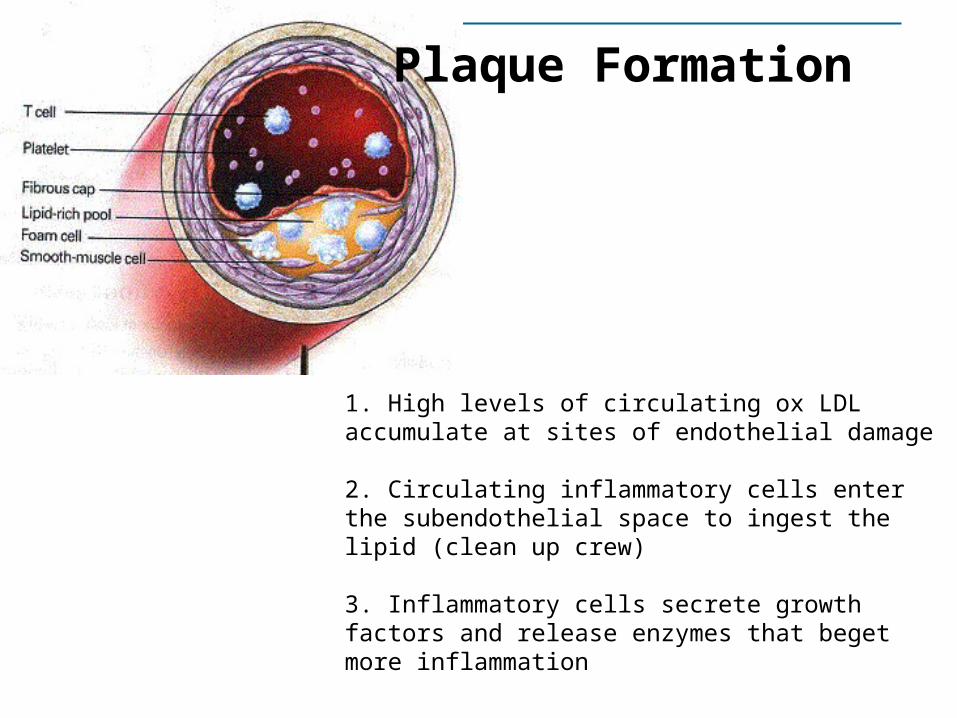
1. High levels of circulating ox LDL accumulate at sites of endothelial damage
2. Circulating inflammatory cells enter the subendothelial space to ingest the lipid (clean up crew)
3. Inflammatory cells secrete growth factors and release enzymes that beget more inflammation
Plaque Formation

4. Plaque grows slowly over the years
5. Fibrous cap weakens from enzymatic damage from inflammatory cells and fatique from mechanical forces
6. One fateful day, the fibrous cap bursts, allowing subendothelial gruel to come in contact with flowing blood
Plaque Formation

7. Causes instantaneous thrombosis
8. If thrombus partially occludes artery: USA/NSTEMI
9. If thrombus completely occludes artery: STEMI
Plaque Formation

1. : Excess circulating LDL cholesterol gets sub-endothelial and becomes oxidized, stimulating an inflammatory response.
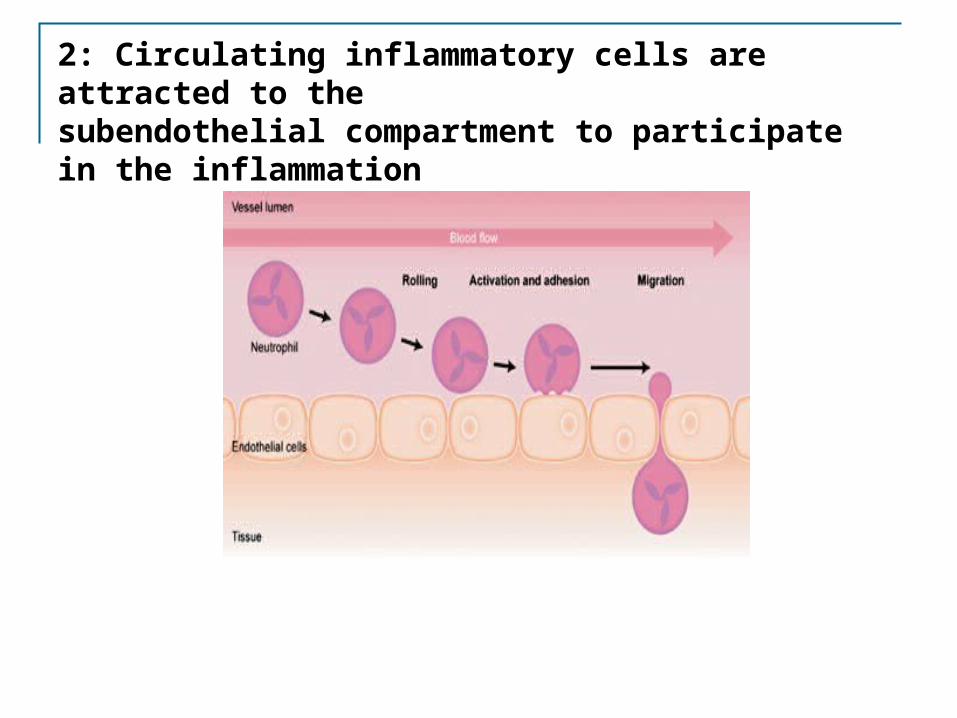
2: Circulating inflammatory cells are attracted to the subendothelial compartment to participate in the inflammation

3: Once in the subendothelial compartment, the macrophagesingest the lipid, becoming “foam cells”

4: Accumulation of foamcells make up the early atheroscleroticlesion: the “fatty streak”

5: Plaque progression.Over 20 to 40 years, the plaque continues To grow, until …

Coronary Artery Plaque/Rupture

Stable and Unstable Plaque
How can a coronary angiogram differentiate between these two?
Stable plaque: responsible for stable, exertional angina
Unstable or vulnerable plaque: upon rupture, responsible for acute MI and sudden death
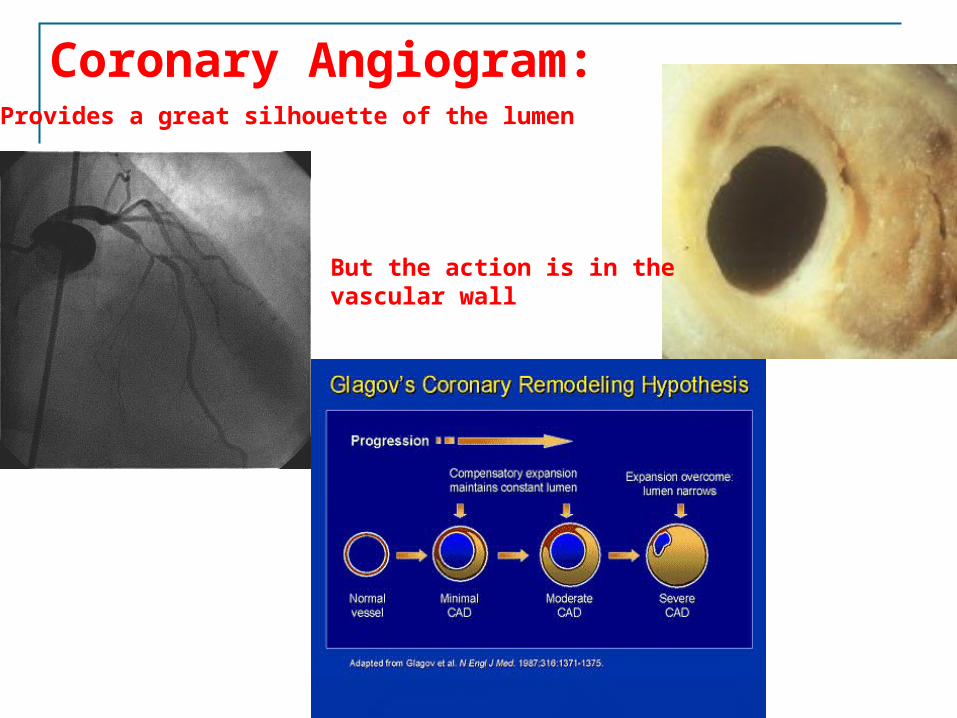
Provides a great silhouette of the lumen
But the action is in the vascular wall
Coronary Angiogram:

Coronary ImagingIntravascular Ultrasound (IVUS)

Unstable vs Stable Plaque

Unstable/Vulnerable Plaque vs Stable Plaque
Thickness of fibrous cap covering plaque
Lipids, WBC’s and enzymes within plaque
Connective tissue within plaque
Risk of rupture
Associated clinical sydromes
Stable plaque
Thick Small amt Large amt Low Stable exertional angina
Unstable/vulnerable plaque
Thin Large amt Small amt High Acute coronary syndromes, sudden death

Acute Coronary SyndromesBiological/Clinical Correlation Changing the vulnerable plaque to a quiescent, stable
plaque is major focus of treatment of CAD patients Statins (lipid lowering drugs) BP control Inhibition of renin angiotensin system Tobacco avoidance

Lower levels of circulating LDL cholesterol
Less oxidized LDL infiltrating the arterial wall
Fewer macrophages infiltrating the arterial wall
Fewer enzymes to degrade the cap of the plaque
Plaque less likely to rupture
Lower risk of myocardial infarction
Plaque STABILIZATION is the major benefit of aggressive lipid lowering

Acute Coronary SyndromesPathogenesis of Coronary Thrombosis
Fibrin strandsPlatelets
RBC’s
WBC’s

Acute Coronary SyndromesPathogenesis of Coronary Thrombosis
Thrombin (enzyme and cellular agonist) formed at sites of vacular injury (i.e., plaque rupture, endothelial erosion, balloon injury)
Thrombin cleaves soluble fibrinogen to fibrin strands
Fibrin strands make up “meshwork” of the clot
Platelets become activated by agents released from the plaque
Activated platelets express IIb/IIIa receptors, which link platelets to fibrin strands, propagating and strengthening the clot

Acute Coronary SyndromesPathogenesis of Coronary Thrombosis
Clot begets Clot (vicious cycle) Activated platelets provide cell membrane surface for more thrombin
formation (“Prothrombinase complex”)
Thrombin stimulates platelet activation
Platelets and thrombin mediate vasoconstriction, reducing blood flow to and from ruptured plaque. Low flow stimulates thrombus formation
Natural antithrombotic tendency of artery wall (tPA, antithrombin, nitric oxide, etc) becomes overwhelmed

Coronary Thrombosis: Clot begets Clot
Thrombin stimulates
platelet activation
Activated platelets
accelerate thrombin formation
Ruptured plaquepromotes thrombin
formation and recruits platelets
to site

Thrombin stimulates
platelet activation
Activated platelets
accelerate thrombin formation
Ruptured plaquepromotes thrombin
formation and recruits platelets
to site
Antiplatelet drugsAntithrombin drugs
Antiplatelet drugsAntithrombin drugs
Antiplatelet drugsAntithrombin drugs
Coronary Thrombosis: Clot begets Clot

Keys to breaking the “Vicious Cycle” of Coronary Thrombosis
Antiplatelet drugs Aspirin Clopidogrel Prasugrel IIb/IIIa glycoprotein receptor antagonists
Antithrombin drugs Unfractionated Heparin Low molecular weight heparins Bivalirudin Argatroban

Acute Coronary SyndromesClinical Presentation Unstable angina
New onset angina or change in pattern of angina Angina at lower workloads More severe in quality or occurring more frequently Takes longer to go away or increased NTG requirements
EKG changes may or may not be present
Physical exam often normal

Acute Coronary SyndromesClinical Presentation Non ST segment elevation MI (NSTEMI)
Prolonged angina, shortness of breath, or both
Evidence of myocardial necrosis (elevated cardiac enzymes in bloodstream)
EKG changes usually present ST segment depression T wave inversions

Acute Coronary SyndromesClinical Presentation ST segment elevation MI (STEMI)
Severe angina, shortness of breath, or both
Physical exam can separate high from low risk pt Rales on lung auscultation, gallops on cardiac auscultation, tachycardia,
low BP
EKG: ST segment elevation in at least two contiguous leads
Acute Coronary Syndromes (USA/NSTEMI):Treatment Principles Restore normal coronary blood flow as soon as
possible
Address coronary thrombosis, interrupt cycle Optimize myocardial oxygen demand-supply ratio (Decrease
HR, BP, wall tension) Interrupt sympathetic nervous system/catecholamine
stimulation of heart In sickest patients, immediate cardiac cath/reperfusion

Acute Coronary SyndromesTreatment:USA/NSTEMI Statins
Reduce inflammation inside culprit plaques and other plaques throughout the body.
Beta blocker Decrease HR, BP, myocardial oxygen demand
Nitrates Decreases myocardial oxygen demand by decreasing preload, wall
tension Improves coronary perfusion directly by dilating coronary arteries

Acute Coronary SyndromesTreatment:USA/NSTEMI Clopidogrel/Prasugrel/Ticlopidine/Ticagrelor
Inhibits ADP-induced platelet activation
Aspirin Inhibits thromboxane A2-mediated platelet activation
IIb/IIIa platelet receptor antagonists Inhibits final common pathway of platelet aggregation Reduces composite of death and MI in ACS pts
Unfractionated Heparin or Low molecular weight Heparin Inhibits thrombin

Acute Coronary Syndromes Treatment: USA/NSTEMI When or whether to perform cardiac catheterization with
coronary angiography?
If pain persists despite maximal medical treatment, urgent cardiac cath with revascularization (coronary stent placement or CABG) is indicated
If pain resolves with medical treatment, but patient with high risk markers, cardiac cath and revascularization before hospital discharge (High TIMI Risk Score)
Very low risk patients without recurrent symptoms can be managed conservatively, with cardiac catheterization performed only for recurrent symptoms

(Thrombolysis in Myocardial Ischemia)TIMI Risk ScoreClassification system of risk stratifying ACS pts with clinical variables Age > or = 65 History of known CAD Use of ASA in last 7 d At least 3 CAD risk factors ST segment changes (depression or elevation) > or = 2 episodes of rest angina in last 24 hrs Elevated cardiac enzymes
Each of the above has a value of 1 point; add the points up to get the patient’s TIMI score

TIMI Risk Score allows the doctor to assess pt’s risk for death/MI in next 14 days

TIMI Risk Score: Example
73 year old woman, works as part time bus driver
PMHx: HTN, tobacco, hyperlipidemia
CAD (cardiac cath 7 years ago: 60% RCA stenosis)
3 episodes rest angina since last night
Medications: ASA, Atorvastatin, Metoprolol
CXR: enlarged cardiac silhouette
Troponin, CK and CKMB all normal
Her EKG
What is her TIMI Risk Score? What is her risk of death or MI in next 14 d?

73 year old woman, works as part time bus driver
PMHx: HTN, tobacco, hyperlipidemia,
CAD (cardiac cath 7 years ago: 60% RCA stenosis)
3 episodes rest angina since last night
Medications: ASA, Atorvastatin, Metoprolol
CXR: enlarged cardiac silhouette
Troponin, CK and CKMB all normal
Her EKG
What is her TIMI Risk Score? Answer: 6What is her risk of death or MI in next 14 d? Answer: Approx 40%
TIMI Risk Score: Example

Lumen
Thrombus
Complex plaque
Acute Coronary Syndromes:Treatment: STEMI

Acute Coronary Syndromes:Treatment: STEMI
Immediate reperfusion therapy (coronary balloon angioplasty/stent placement or fibrinolytic drug therapy )
Restore normal coronary blood flow ASAP (“Time is muscle”)
Just like USA and NSTEMI, beta blockers, nitrates, antiplatelets, anti-thrombins, and statin drugs are indicated
Acute Coronary SyndromesSTEMI Fibrinolytic therapy
Plasmin: enzyme that digests fibrin strands of a clot, effectively “lysing” the clot
Plasminogen: Pro-enzyme of plasmin. Needs to be cleaved to plasmin
Plasminogen activators: enzymes that cleave plasminogen to plasmin:
Streptokinase (rarely used in US) Tissue type plasminogen activator (tPA) Tnk-tPA (modified tPA with longer half-life) rPA (modified tPA with longer half-life) Others (urokinase, APSAC, vampire bat saliva, etc.)

Fibrinolytic therapy: (Plasminogen activators that cleave plasminogen to plasmin)
Plasmin: digests fibrin strands, rendering clot unstable
Antiplatelet agents: prevent further platelet aggregation
Antithrombin agents: prevent production of more fibrin strands
Clot
Clot

STEMI: Percutaneous Coronary Intervention (PCI)
Catheter introduced into femoral, Brachial, or radial artery
Advanced up to heart
X ray dye injected into coronaryarteries to identify blocked artery
Blocked artery opened with tinyballoon and stent

STEMI

Stepwise Approach:
Step 1: Thrombectomy catheter(physical removal of thrombus)
Step 2: Delivery of anticoagulant/Antiplatelet drug into the lesion to Disrupt/dissolve residual thrombus
Step 3: Balloon and Stent
STEMI

Coronary Angiogram

Immediate Reperfusion in STEMI: Fibrinolytic Therapy vs PCI Fibrinolytic drug tx
Improves survival in STEMI pts
Works within 90 min of initiation of tx
Initial success in 65-75% of pts
20-30% of pts reocclude artery
Intracranial bleed in approx 1%
Artery often left with moderate or severe residual stenosis
Available in most, if not all hospitals
Percutaneous intervention
Improves survival in STEMI pts
Works within 30 min of initiating cath
Initial success in >95% of pts
<1% of pts reocclude artery
Intracranial bleed risk <0.1%
Artery usually left with 0% residual stenosis
Available in <1/3 of hospitals

STEMI Treatment: Fibrinolytic Therapy vs Percutaneous Coronary Intervention (PCI) In multiple head-to-head studies, PCI (balloon angioplasty with stent
placement) in STEMI pts proved superior to fibrinolytic drug therapy (better survival, better myocardial salvage, lower complication rates)
Most hospitals do not have an interventional cath lab
If pts present to hospitals without cath lab, they have better outcomes if they can be transported to a cath lab and have PCI within 90 minutes

Treatment of STEMI:Coronary Stenting vs Fibrinolytic therapy
Bottom line:
Stenting >>>fibrinolytic therapy>>>nothing

Acute Coronary Syndromes:Treatment:STEMI Whether treating the STEMI pt with fibrinolytic therapy or
mechanical revascularization, patients who receive the treatment early (2-3 hrs from pain onset) have ½ the mortality of people who receive the treatment late (>6 hrs after pain onset)
This is a major problem, with delays at several steps: Patient delays seeking medical help (denial, poor access, social
issues) Delay in ER staff performing EKG Delay in EKG being presented to MD for interpretation Delay in drugs being mixed in pharmacy and administered to pt Delay in transporting pt from ER to cath lab or from one hospital to
another Delay in cath lab staff coming in from home

• Acute coronary syndromes range from unstable angina without infarction, to STEMI.
• Stable plaques are filled with connective tissue, are metabolically inactive, and cause stable exertional angina
• Unstable or “vulnerable” plaques are lipid-filled, tense, metabolically active, and prone to rupture, causing acute coronary syndromes
• A main focus of treating CAD pts is transforming vulnerable plaques to stable plaques. Statins are the drugs with the most evidence supporting this.
Acute Coronary Syndromes: Summary

• Coronary thrombosis is a hallmark of acute coronary syndromes
• Much of the therapy for ACS is directed at interrupting the vicious cycle of thrombosis (e.g., ASA, clopidogrel, heparin, IIb/IIIa blockers)
• In STEMI, emergent reperfusion can be life-saving, the sooner the better
• In STEMI patients, PCI (coronary stenting) results in greater myocardial salvage and better survival than fibrinolytic therapy, but only if it can be performed expeditiously. If no cath lab is available, do not delay giving fibrinolytic therapy, which is also a life-saving therapy
Acute Coronary Syndromes: Summary

1. Understand the biology of coronary plaque rupture2. Understand the the relationship between the intracoronary pathological
findings and the clinical presentations in acute coronary syndromes3. Understand the differences between “stable” and “vulnerable” coronary
plaques4. Describe methods for changing the vulnerable plaque to a stable plaque5. Describe the concept of risk stratification in acute coronary syndromes6. Be familiar with the pathogenesis of coronary thrombosis7. Be able to calculate the TIMI risk score in ACS patients8. Compare and contrast the two major modes of reperfusion therapy in
acute ST elevation MI (STEMI)
Acute Coronary Syndromes: Objectives

Acute Coronary SyndromesSample Questions A 71 year old woman is admitted to your service for treatment of a non ST
elevation acute MI. She is now free of chest pain, and her EKG which initially showed ST segment depression, has normalized. She has a high TIMI risk score of 5. Her current medications include ASA, clopidogrel, a IIb/IIIa antagonist, and a beta blocker. A coronary angiogram is planned for tomorrow. Which of the following classes of medications should be added to address the pathophysiology and prevent further ischemic episodes?
A) Morphine
B) An antithrombin drug (unfractionated or low molecular weight heparin)
C) A fibrinolytic drug
D) Prasugrel

Acute Coronary SyndromesSample Questions One of your patients is a physician who recently had a CT coronary
angiogram, which provides an image of the lumen of the coronary artery. The only abnormality seen was a 65% stenosis in the proximal LAD. He is concerned, and wants you to provide him with detailed information on his risk for an acute MI. Which of the following would you recommend?
A) A cardiac cath with coronary angiography
B) A fasting determination of his total cholesterol level
C) A coronary angiogram accompanied by intravascular ultrasound or some form of imaging of the coronary wall
D) Reassure him that no further testing is necessary

Acute Coronary SyndromesSample Questions You are the ER attending at a hospital equipped with a 24 hour on
call cath lab team with interventional capability. You take a call from a paramedic transporting a pt having a massive STEMI; the pt is hypotensive and may be going into cardiogenic shock. The ambulance is 5 minutes away from a hospital that does not have a cath lab; your hospital is 2 hours away by ambulance. You advise her to:
A) Proceed to your hospital; multiple head to head trials have shown that percutaneous coronary intervention is the preferred method of treatment for STEMI
B) Proceed to the nearest hospital for fibrinolytic therapy right away
C) Begin aspirin and heparin and continue driving to your hospital
D) Begin high dose IV nitroglycerin and beta blockers and proceed to the nearest hospital. The doctors at the local hospital will be able to assess the pt and decide on further options.

Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey