acute flaccid paralysis
TRANSCRIPT

ACUTE
FLACCID
PARALYSISby Nur Hanisah Zainoren(062)

ACUTE
FLACCID
PARALYSIS
Rapid in onset
ACUTE
FLACCID
PARALYSIS
Drooping
without spasticity

ACUTE
FLACCID
PARALYSISLoss of ability to move a body part

What is AFP?

What is AFP?
a clinical syndrome

What is AFP?
a clinical syndromecharacterized by
rapid onset of weakness including
(less frequently) weakness of the muscles of
respiration & swallowing
progressing to maximum severity within
several days to weeks

What is AFP?In Global Polio Eradication Initiative, AFP is defined as
any case of AFP in a child aged <15 yr
or
any case of paralytic illness in any person of any age when polio is suspected

“Result from involvement at any point
in the motor unit”
Common causes
of AFP:
Nonpolioenteroviral
illnesses
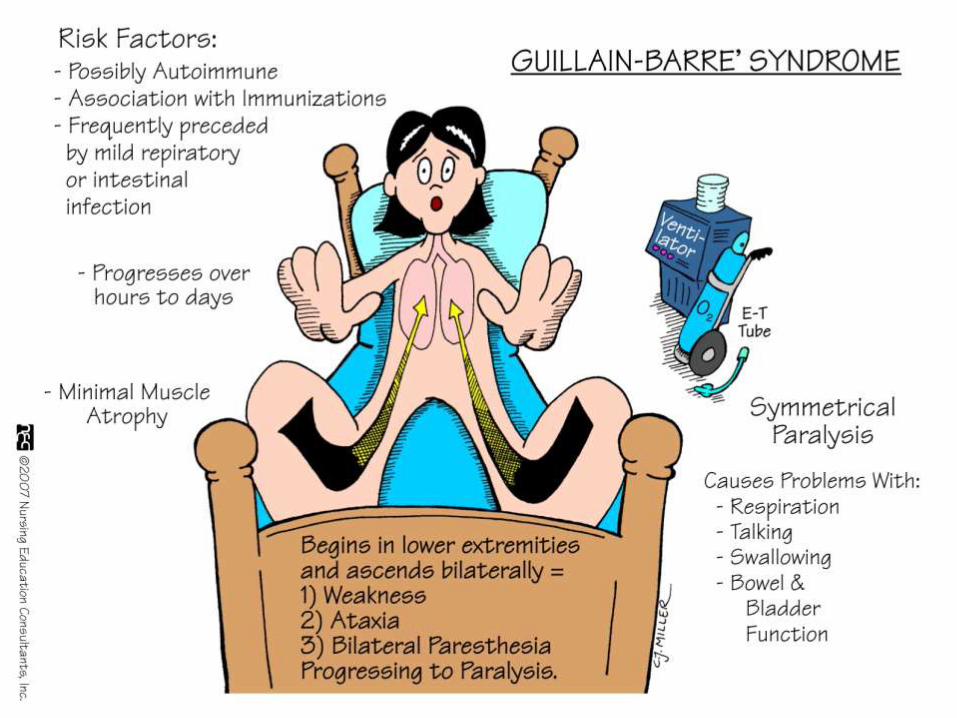
Guillain-Barrésyndrome
Poliomyelitis
Transverse myelitis
Traumatic neuritis
Postdiphtericneuropathy

“Result from involvement at any point
in the motor unit”
Common causes
of AFP:
Nonpolioenteroviral
illnesses
Guillain-Barrésyndrome
Poliomyelitis
Transverse myelitis
Traumatic neuritis
Postdiphtericneuropathy

Caused by the destruction of myelin (demyelination)
Common cause of AFP in children
Guillain-Barré Syndrome

“Result from involvement at any point
in the motor unit”
Common causes
of AFP:
Nonpolioenteroviral
illnesses
Guillain-Barre syndrome
Poliomyelitis
Transverse myelitis
Traumatic neuritis
Postdiphtericneuropathy

Poliomyelitis
Highly infectious viral disease, which mainly affects young children.
Viral transmitted mainly through the faecal-oral route multiplies in the intestine invade the nervous system cause paralysis.
There is no cure for polio, it can only be prevented by immunization.
• Initial symptoms of polio include Fever
Fatigue
Headache
Vomiting
Stiffness in the neck
Pain in the limbs
In a small proportion of cases, the disease causes paralysis, which is often permanent.

“Result from involvement at any point
in the motor unit”
Common causes
of AFP:
Nonpolioenteroviral
illnesses
Guillain-Barre syndrome
Poliomyelitis
Transverse myelitis
Traumatic neuritis
Postdiphtericneuropathy

Transverse Myelitis
• disorder caused by inflammation of the spinal cord
• Characterized by symptoms and signs of neurologic dysfunction in motor and sensory tracts on both sides of the spinal cord.
• Produce altered sensation, weakness and sometimes urinary or bowel dysfunction.

Transverse Myelitis
• disorder caused by inflammation of the spinal cord
Characterized by symptoms and signs of neurologic dysfunction in motor and sentracts on both sides of the spinal cord.
duce altered sensation, weakness and sometimes urinary or bowel dysfunction.

• The cause of 60% of TM cases may remain unknown
• However, the remaining 40% is associated with autoimmune disorder such as:– multiple sclerosis
– neuromyelitis optica
– systemic lupus erythematous
– Sjogren’s syndrome
– sarcoidosis

four classic symptoms of transverse myelitis:
• weakness in the arms/legs
• sensory symptoms such as numbness or tingling
• pain and discomfort
• bladder dysfunction and/or bowel motility problems

“Result from involvement at any point
in the motor unit”
Common causes
of AFP:
Nonpolioenteroviral
illnesses
Guillain-Barre syndrome
Poliomyelitis
Transverse myelitis
Traumatic neuritis
Postdiphtericneuropathy

Traumatic neuritis
• Inflammation of a nerve following an injury.
• Sciatic nerve injury leading to paralysis of the foot and permanent sequelae following intramuscular injection in the gluteal region has been recognised since long
• 75% of polio cases have received injections for fever with paralysis following from 24-48 hours later.


Rationale
Poliomyelitis is targeted for eradication
Highly sensitive surveillance including immediate case investigation and specimen collection are critical for the detection of wild poliovirus circulation
Critical for documenting the absence of poliovirus circulation for polio-free certification

All patients with acute flaccid paralysis should be reported to Surveillance Medical Officer of World Health Organization.
Every case of AFP within the last 6 months has to be reported
Additionally, other conditions which need notification are:• Isolated facial palsy• Isolated bulbar palsy• Unproved hypokalemia• Neck flop• Floppy baby• Flaccid hemiplegia• Encephalitis• Postictal weakness (Todd’s paralysis)• Postdiphretic polyneuritis

Cases are investigated immediately, usually
within 48 hrs of notification, by a trained
medical officer
Detailed medical history, examination & investigations are done :
- Collection & transportation of
stool specimen
- Search for additional cases &
outbreak response in affected
community
- 60 days follow up examination
- Analysis of laboratory result
- Case classsification
Aft
er
con
firm
ing
the
cas
es
as A
FP
Stool Specimen Collection
• Important aspect of polio eradication strategy
• For every cases of AFP,
2 stool specimen is collected (at least 24 hours apart)
**Ideally within 14 days of onset of paralysis
(optimal time period for detection of polio virus)
**Should also be collected in any late-reported AFP case upto 60 days from the day of paralysis onset
**>60 days, the likelihood for detecting poliovirus is very low

• Voided stool sample is preferred
• Other methods:
– Digital extraction (when child is constipated or dies)
– Postmortem stool collection (contents of large intestine)
– Use of rectal tube
• Each specimen should be 8 g each • Enema or purgatives is not recommended•Collected in a clean, dry, screw-capped container•Labeled and transported in the ‘cold chain’

Poliovirus Isolation
• 2 types of cell lines are used:
– RD cell lines (derived from human rhabdomyosarcoma; favour the growth of all enteroviruses)
– L20B cell lines (favour the growth of only poliovirus)
• If cytopathic effects appears in L20B cell line, the isolate then goes for neutralization test to determine the serotype (type 1,2 or 3) of the poliovirus by using appropriate antisera

• If cytopathic effects appears in L20B cell line, the isolate then goes for neutralization test to determine the serotype (type 1,2 or 3) of the poliovirus by using appropriate antisera
• Intratypic differentiation test is done to determine wetherthe particular isolate is wild poliovirus or vaccine poliovirus
• All wild poliovirus isolates also undergo genetic sequencing
• A case is classsified as polio if wild poliovirus is isolated from the stool specimen.
• Cases with inadequate stool specimens and having residual weakness, who have died or are lost to followup undergo additional investigation & are presented for review by the National Expert Review Committee (classifies the case as compatible with polio or discarded as nonpolio AFP)

