acute umbilical complaints in the pediatric er or “my babies navel looks/smells funny”
TRANSCRIPT
Acute Umbilical Complaints in the Pediatric ER
Or
“my babies navel looks/smells funny”
2
Issues Umbilical - Case 1• 9 week girl infant. Presents to PLC-ER• Swelling of the umbilicus for ~5 hours• Erythema and a central Umbilical “lump”
noted• No fever• Some poor feeding with no vomiting for less
than a day• ~6 wet diapers past 24 hours
3
Issues Umbilical - Case 1• 5.11 kg, Cap refill <3 sec• T 36.4, R28, P 145, BP 78/49• Alert, no distress• N H&N• N chest and HS• Soft benign abdomen with no masses• Central, red umbilical bulge within skin cuff
(cushion)• Small volume thin purulent drainage?• Slight erythema 4-7o’clock? No induration or
demarcation
4
Issues Umbilical• Referred to ACH-ER with:
“? Umbilical hernia, R/O Omphalitis”
ACH ER exam similar overall• C&S of Umbilical “discharge”• CBC, Lytes• Felt likely to be Omphalitis• Referral to General Surgery• Ancef 25 mg/kg commenced
5
Issues Umbilical• CBC• WBC 9.7, Neuts 2.6• Hb 106, Platlets 522
• Na 138, Cl 103, K 4.7, HCO3 23
• Cr 17, Urea 2.2• U/A neg
6
Issues Umbilical• General Surgical Opinion (in the am!)• Likely omphalitis• Consider infected urachal remnant
• Admitted• Change to IV clindamycin• U/S booked
7
Issues umbilical• In Hospital course• Always remained afebrile• C&S umbilical discharge “scant skin flora
only”• U/S abdomen:• Swollen protruding umbilicus noted to be filled
with echogenic material. A sinus tract is identified which extends form the lower umbilicus and connects to the superior and anterior wall of the bladder in the midline. The appearance is consistent with a patent urachus.
8
Issues Umbilical• Day 4 • Discharged home for urgent elective repair
to be booked• Clindamycin oral course
9
Objectives of Naval Mission• Discuss omphalitis • Discuss common cord care• Understand the non-infectious
abnormalities that can occur in the umbilicus, notably in the infant
• Not to discuss • Umbilical hernia management• Case room cord examination and
implications
10
Normal Cord care• Policies vary greatly in developing vs
developed countries• Marked decrease in incidence of Omphalitis in
developed countries • ~0.7% vs up to 6 %
• In developed countries:• Cochrane review shows no form of cord
cleaning/antiseptic is better than dry cord care
• In developing countries antiseptics in cord care markedly decrease death and omphalitis (chlorhexidine, AgSulfadiazine, Triple dye…)
11
Cord Separation• Normal timing of ~1 week or less for
separation• Prolonged by certain agents• 70% alcohol: ~17 days• Triple dye: 3-8 weeks
• True “delayed” separation (without agent application) is in excess of 3 weeks
12
Umbilical infection• All cords are nearly immediately
colonized • Staph and other gm+ves within hours• Enteric organisms shortly thereafter
• Devitalized tissue is a good bacterial growth medium
• Mild discharge and absent inflammatory change, even with some odor is usually still a normal occurrence.• No proof for or against Rx with Alcohol, Bacitracin
or Mupirocin…but many choose this.
• When does this constitute early Omphalitis?
13
Omphalitis• Predominately Neonatal• Mean age of onset in term infants is 3.5
days• Infection of umbilicus and/or surrounding
tissues• Purulent (+/-bloody) drainage from stump• Surrounding induration, erythema,
tenderness
• BUT• Lethargy, fever, Irritability, poor feeding
suggest more severe infection/impending sepsis
14
Omphalitis
• Complications:• Sepsis / death• Septic umbilical arteritis/portal vein thrombosis• Peritonitis/liver abscess/intestinal gangrene• Small bowel evisceration• Necrotizing fasciitis
• Present-day Mortality: 7-15%
15
Case 2• 14 day infant girl transferred to ACH-ICU
for umbilical infection• 41 weeks GA• C/S for fetal distress• APGARs 81 & 95
• GBS+ve • Passed N mec. At 24 hours • No jaundice• Breast fed/BM 8x/day• Cord loss ~1 week of age
16
Case 2• Day 11• Some peri-umbilical redness, afebrile• Poor evening feeding
• Day 12• Worsening erythema, wider area• Abdomen appeared “puffy”• T = 38.50C• To local community hospital; blood-streaked stool in
ED, and with all serial later BMs• Much worse feeding and lethargy• Sepsis workup/LP/Ampicillin and Cefotaxime and
admitted
17
Case 2• Day 13• General progression of anorexia, and
increasing abdo wall abnormalities. • U/S abdomen, and transferred to ACH
overnight
• Day 14 ACH - PICU• Change to Flagyl, Meropenum, Clindamycin.
And Gentamycin• Surgery/Plastics consult
18
Case 2• Physical• 88/60, 153,100%RA, 37.5, 40, 4.0Kg• AF flat, no jaundice• CVS N save CRT “2-5 seconds”• No increased WOB• Mottled extremities• Distended abdomen. Black umbilicus,
surrounded by an inner purple and outer white halo, both non-blanching. Rt > Lt, ~30% of abdo wall
• Whole remainder of abdomen wall is erythematous
19
Case 2• Lab • WBC of 33.7• CRP 72.8• Hb 148, Platlets 501
• To ACH-OR for debridement, and bowel inspection for R/O NEC• Abdo wall biopsy and C&S• Bowel observed to be vital without NEC• Umbilicus and surrounding tissues resected
including necrotic skin and abdo. wall to healthy fascia
• Frozen section biopsy consistent with Nec Faciitis

20
Case 2: Intra-operative, Post Umbilical Resection

21
Case 2: Intra-operative, Post Umbilical Resection
22
Case 2• OR visits on PICU-days 1,2,4,6 and 8 for
serial lesser debridements and bowel inspection
• Wound closure PICU day 8 but subsequent dehisence day 19
• Change to tazocin/vancomycin day 7• Wound grew • Enterococcus faecalis• Coag neg Staph• Actinomyces
23
Case 2
• Day 12 - extubated• Day 13 - to the ward• Day 19 - Wound dehisced• Day 30 - discharged home• All Abx discontinued • planned delayed closure abdo. wall ~2
weeks later
24
Omphalitis• Risk factors• LBW• Prolonged labor• PROM• Non-sterile delivery• Umb.A. cathetrization• Home birth• Improper cord care
• (cow dung, bentonite clay)
• Immune abnormalities
• Poorer Prognosis• Male• Premature• “Septic delivery”
• (including un-planned home delivery)
• Temperature instability• Necrotizing fasciitis
• (up to 85% mortality)
25
Omphalitis/Any Soft Tissue Infection
• There is a continuum of severity:
CellulitisInfection of skin and S.C. fat
Necrotizing fasciitisInfection of skin, S.C. fat and superficial and deep fasciae
Myositis/myonecrosis
Deep muscle infection with muscle death
26
Omphalitis/Any Aggressive Soft Tissue Infection
• Should be presumed to be poly-microbial at outset• “the usual suspects” in Omphalitis:• Staph Aureus• Gp A Strep• Coag Neg Staph• Enterococci• Gm Negs: E Coli, Klebsiella P., Proteus Mirabilis…• Anerobes: Bacteroides, Clostridium
perfingens/tetani
27
Omphalitis• Pathology of infection is presumed to be
polymicrobial from the outset• Abx must cover for this, and include:
• Anti-stahpylococcal penicilin or vancomycin• Aminoglycoside• Probable Clinamycin or Metronidazole
Esp. if maternal chorioamnionitis and/or foul discharge, for anaerobic coverage
28
Omphalitis
• Necrotizing Fasciitis• Rare complication of omphalitis• Polymicrobial• Involves skin, subcutis, superficial and deep
fasciae• Rapid spread is typical• Bacteremia, systemic toxicity, and shock in
high proportion. Death 60-85%• Early aggressive surgical intervention, broad
spectrum antibiotics, and supportive ICU care
29
Case 3• 38 2/7 week boy• 30 yr G1P1 mother, N Vtx Vag delivery• APGARs 81 and 85
• Short ACH transfer Day 1-3 for ?ileal atresia…final Dx Meconium plug
• Day 13• Peri-umbilical redness noted by family
30
Case 3• Day 14• Admitted to local hospital• Dx Omphalitis• Ampicillin and Gentamycin
• Day 15• Increasing redness in abrupt fashion: 5cm
above and 3cm below umbilicus• Transfer to ACH ICU• Dx Omphalitis, R/O Necrotizing Fasciitis
31
Case 3• ICU:• Not toxic• Abdo wall is only abnormality of serious note• WBC 16.5, N diff, INR N, Lytes N and Neg AG• Urgent tissue biopsy• No Nec Fasciitis; consistent with cellulitis• Neg gram stain
• Neg blood and urine C&S.• Surface Umb C&S from Primary hospital• Coag neg staph, and enterococcus faecalis
32
Case 3• I.D. Service: Antibiotics changed to • Meropenum, Clindamycin, and Gentamycin
• Day 16• Child improves sufficiently that ward transfer
is in process…..then oliguria unresponsive to fluids arises
• Scrotal swelling and severe progressive abdominal wall edema
• ICU stay maintained
33
Case 3• Day 17• 03:00 Resp failure/ETT• 05:00 dobutamine infusion• 05-10:00 progressive metabolic acidosis• 10:00 to OR• Abdominal exploration. Healthy bowel. • Abdo wall : Excision of navel and surrounding
tissue. Biopsy now positive for Necrotizing fasciitis
• Deterioration: • with coagulopathy, WBC up to 49.5, INR elevated,
ARDS / pulmonary hemorrhage
34
Case 3
• Day 17• Progressive deterioration and difficulty
ventilating. Rising Cr up to 180• 13:30 back to OR• Abdominal compartment syndrome• Bowel “eviscerates” under pressure and
ventilatability markedly improves…bowel seems healthy; Abdo Wall Margins still look healthy, and back to ICU with bowel encased in a “silo bag”
35
Case 3• Severe oliguria• Lines placed and dialysis commenced• Poor tolerance with repeated hypotension and need
for fluid bolusing
• Day 18• Several bradycardic arrests• Progressive instablilty and dialysis
discontinued• Family agree to discontinue all supportive Rx• 04:20 child pronounced
36
Case 3• C&S from initial umbilical ACH biopsy• Coag neg staph• Enterococcus faecalis• Clostridium sordellii
• Autopsy conclusion• Necrotizing faciitis of poly-microbial nature• Sepsis

37
Conclusion
Respect Omphalitis
38
Something is wrong with my babies Navel
• Umbilical Granuloma
• Omphalo-mesenteric duct remnants
• Urachal remnants
39
Case 4• 12 day infant girl
• 41 3/7 weeks, vacuum assisted SVD• GBS -ve• Thriving• Cord dehisced day 7• Umbilicus raw, oozing with sero-sanguinous
discharge since
40
Case 4• Looks well• P 165, R 26, T 37.1, BP 76/42• General Exam Normal• No peri-umbilical redness• Moist “nodule” of pinkish-red tissue over
stump site. Bleeds easily
• ?Umbilical Granuloma (vs some other developmental lesion)…Referred to Surgery Clinic DDR
41
Case 4• In clinic 1 month later• Major lump had “fallen off” and moist base
was cauterized with AgNO3
• Re seen 3 weeks later:• Area dry and fully healed
• Diagnosis:
Umbilical Granuloma
42
Umbilical Granuloma• Most common cause of umbilical mass
and umbilical drainage• Usually post cord separation• Persistent drainage of serous or sero-
sanguinous fluid around the umbilicus• A mass of pink granulation tissue at
umbilical base• Moist• Pink• Friable• Soft• Often pedunculated • Usually 3-10 mm
43
Umbilical Granuloma• Treatment:
• AgNO3 local Rx 1-2 x per week
• If it persists post 3-4 Rx sessions • Can be ligated (be sure its not a polyp!) or
referred to general surgery for formal excision
44
Omphalo-mesenteric Duct Remnants
• Omphalo-mesenteric duct (Viteline duct):
• Connects the developing GI tract to yolk sack
• Regresses by ~9th week GA• Disruption of this regression causes the list
of abnormalities:
45
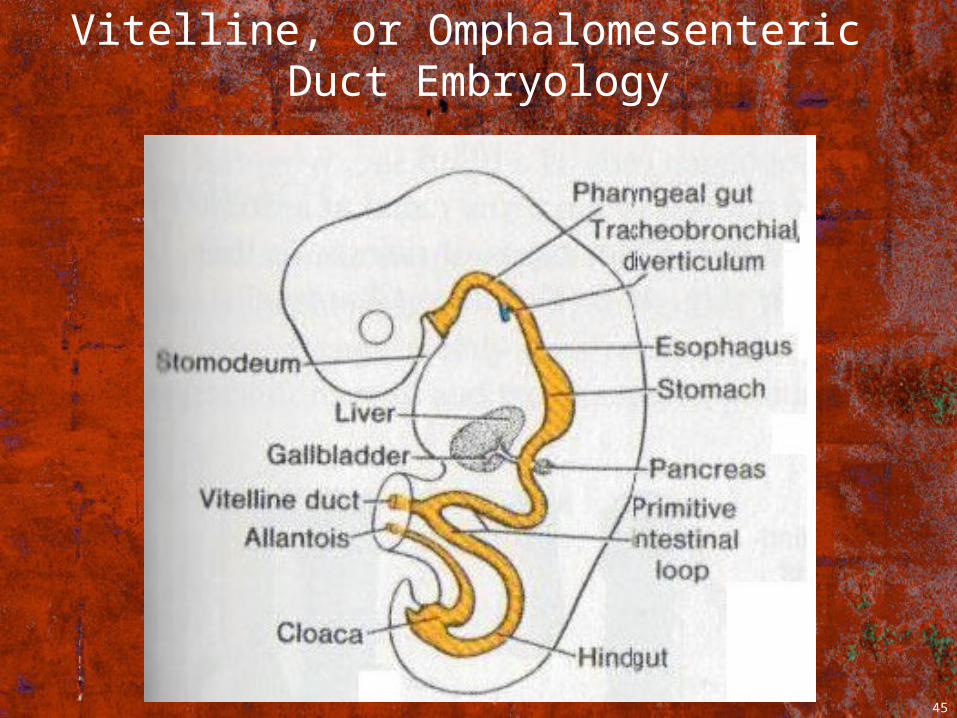
Vitelline, or Omphalomesenteric Duct Embryology
46
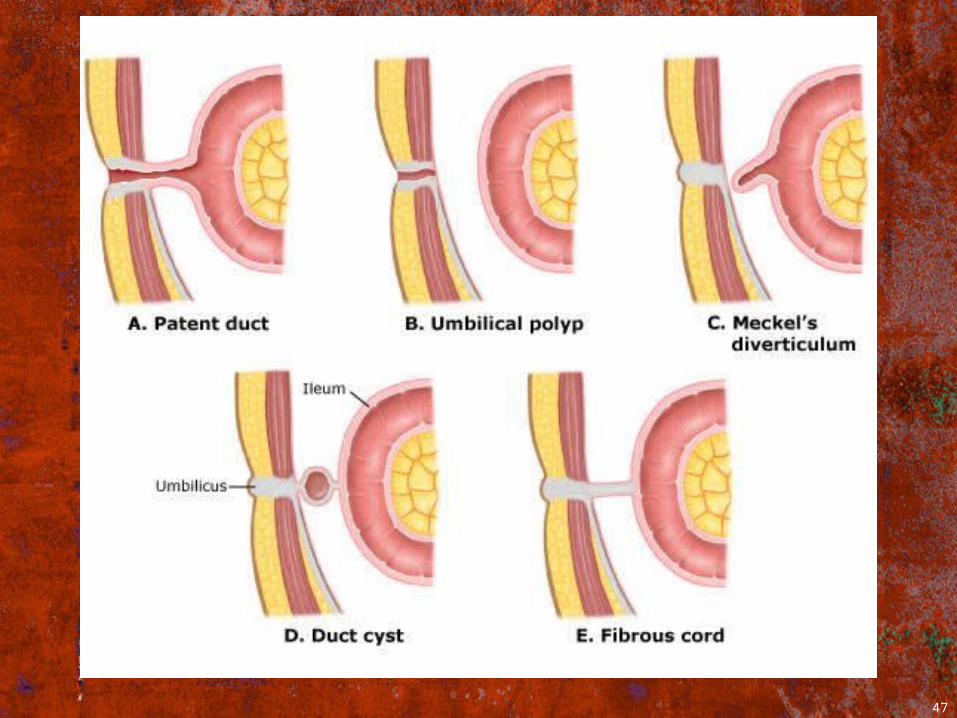
OMD Remnants• Umbilical fistula• Complete patency of OMD with stoma-like
connection to the terminal ileum
• Partial persistence of OMD• Fibrous band umbilicus to ileum• “Distal” remnant - OMD-enteric cyst• “Proximal” remnant - Meckel’s diverticulum• Umbilical polyp - a mucosal remnant in the
umbilical stump
47
48
OMD remnants• Fibrous band • can cause volvulus; obstruction and/or volvulus
are most common infant presentation
• Umbilical Polyp• Usually enteric, but occasionally urachal origin.
Rarely pancreas, liver• Firm masses. No response to AgNO3,and must be
surgically excised
• OMD cyst • often asymptomatic, or may be an umbilical or
abdominal mass; occasionally infected
49
Urachal Remnants• Urachus is the embryologic descendant
of the allantois.
• Allantois is the most distal projection of the primitive gut, projecting into the extra-embryonic cord. Of it’s Intra-embryonic portions:• The bladder = proximal portion.• The urachus = more distal portion.
50
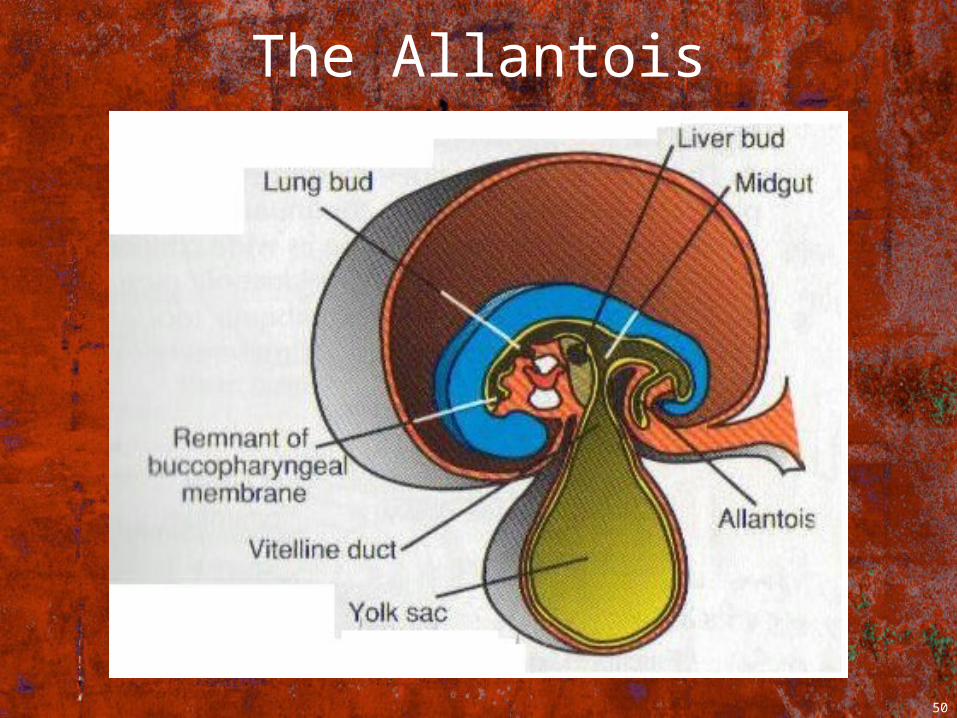
The Allantois
51
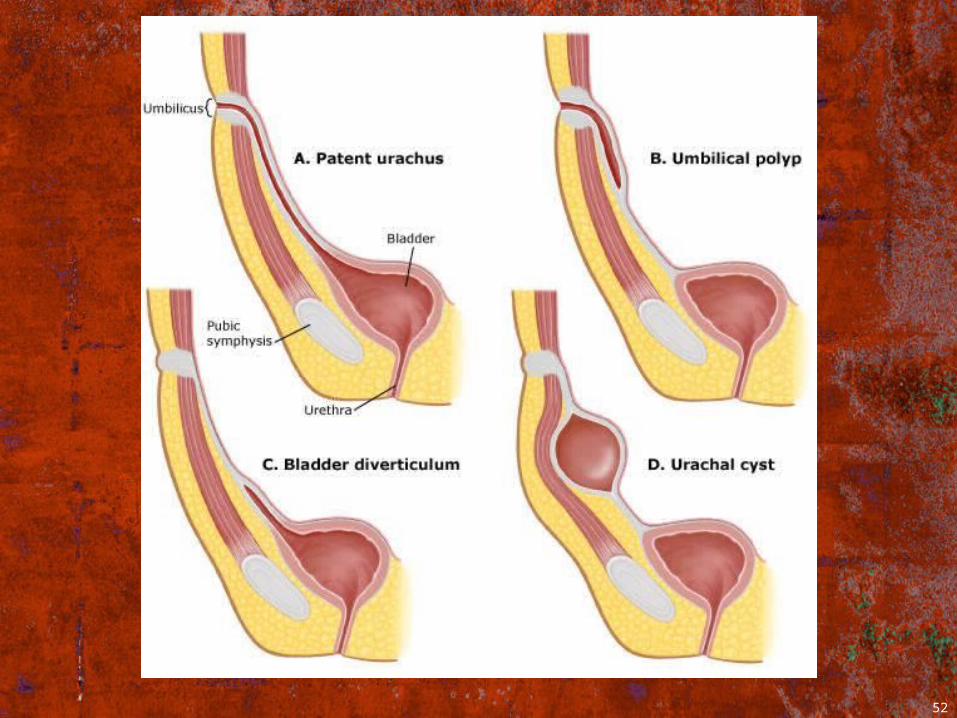
Urachal Remnants• Urachal fistula - complete patency of the
urachus• Urachal cyst - remnant along tract
(usually lower 1/3)
• Urachal sinus Blind umbilical tract, unconnected to the bladder
• Vesico-urachal diverticulumAntero-superior midline bladder dome
• Umbilical (urachal) polyp
52
53
Urachal Remnants• Ultrasound is the ideal investigation for
initial definition
• Sinogram for patent urachus (“fistula”) or urachal sinus are other options
• Renal U/S and VCUG have also been recommended
54
Urachal Remnants• Presentations:• May be subtle with erythema +/- drainage
• Umbilical discharge or Omphalitis spectrum
• Umbilical pain or retraction on micturition
• Umbilical mass or cyst
• Peri-umbilical pain
55
Urachal Remnants• All need to be excised
• In adults, 50% have malignant (adneocarcinoma) changes at the time of excision (nil in children)
• Cuff of normal bladder mucosa is excised during resection

56
Questions?
57
References1) Vane D.W. et al “Viteline Duct Abnormalities:
Experience with 217 Childhood Cases Arch surg122:542, 1987
2) Pomeranz A. “Anomalies, Abnormalities and Care of the Umbilicus” Pediatric Clinics of N.A. 51:819, 2004
3) Rescorla F. J. “Hernias and Umbilicus” in Principles and Practice of Pediatric Surgery, volume 2, 2005
4) Cilento B. G. et al “Urachal Anomalies: Defining the Best Diagnostic Modalitiy” Urology52:120, 1998.
5) Ashley R.A. et al “Urachal Anomalies: a Longitudinal Study of Urachal Remnants in Children and Adults” J Urol 178:1615, 2007
6) Cushing A.H. “Omphalitis: A Review”Pediatr Infect Dis 2:282, 1985
58
References7) Sawardekar K.P. “changing Spectrum of Neonatal
Omphalitis” Pediatr Infect Dis J 23:22, 20048) Mason W.H.et al “Omphalitis in the Newborn
Infant”Pediatr Inf Dis J 8:521, 19899) Kosloske A.M. “Cellulitis and Necrotizing Fasciitis of the
Abdominal Wall in Pediatric Patients”. J Pediatric Surg 16:246-251, 1981
10)Simon N.P. “Changes in Newborn Bathing Practices may Increase the Risk for Omphalitis” Clin Pediatr 43>763-767, 2004
11) Louie J.P. “Essential Diagnosis of Abdominal Emergencies in the First Year of Life”Emer Med. Clinics of N A 25:1009-1040
12) Zupan J. et al “Topical Umbilical Cord Care at Birth(Review)”Cochrane Library 2008, Issue 3
59
References13) Mullany L.C et al “Development of a Clinical Sign Based
Algorithm for Community Based Assessment of Omphalitis” Arch Dis. Child. Fetal Neonatal Ed. 91:F91-F104, 2006
14) Mullany, L.C. “Topical Applications of Chlorhexidine to the Umbilical Cord for Prevention of Omphalitis and Neonatal Mortality n Southern Nepal: a Community-based, Cluster-randomized Trial” Lancet 367:910, 2006
15) Hseih, W.S. et al “Neonatal Necrotizing Fasciitis: A report of Three Cases abd Review of the Literature” Pediatrics103:e53, 1999
16) Iacono, G. “Red Umbilicus”:a Diagnostic Sign of Cow’s Milk Protein Intolerance. J. Ped.Gastro. And Nutr. 42:531-534, 2006
17) Burd R.S. et al “Evaluation and Initial Management of Miscellaneous Pediatric Surgical Problems”Pediatric Annals30:752-759, 2001