acute&kidney&injury& - spr club · nephsap*september*2007* uehlinger etal# ndt&2005...
TRANSCRIPT
Acute Kidney Injury
Dr S Mathavakkannan Consultant Nephrologist

Scope
1. Defini@on 2. Epidemiology 3. Physiology 4. Markers of Injury 5. Survival 6. Treatment 7. AKI Preven@on
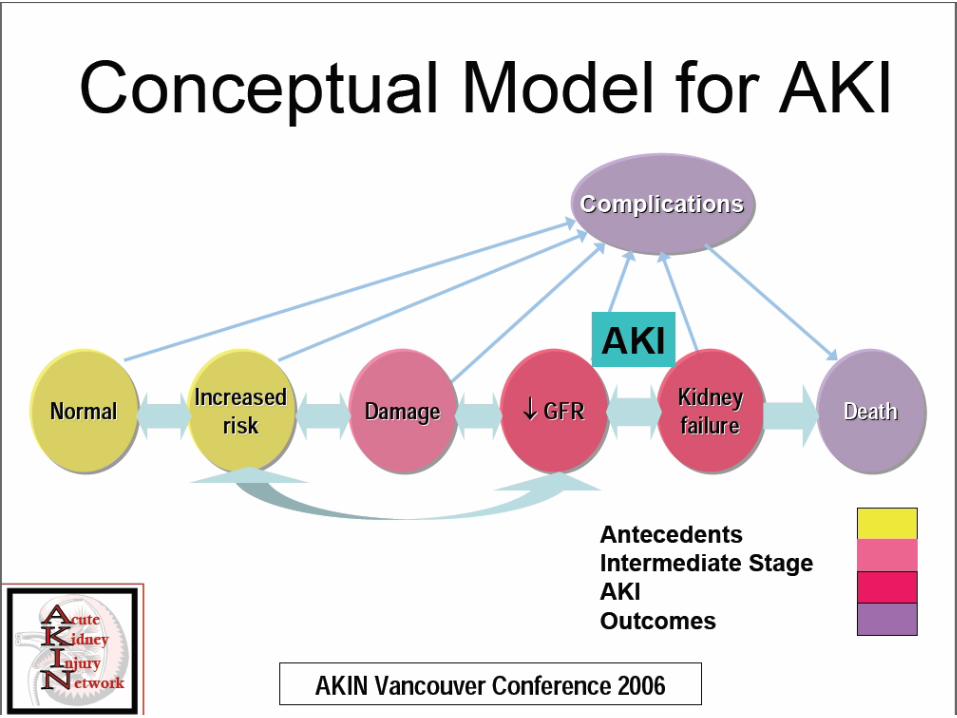
Defini@on(s): 1. ADQI
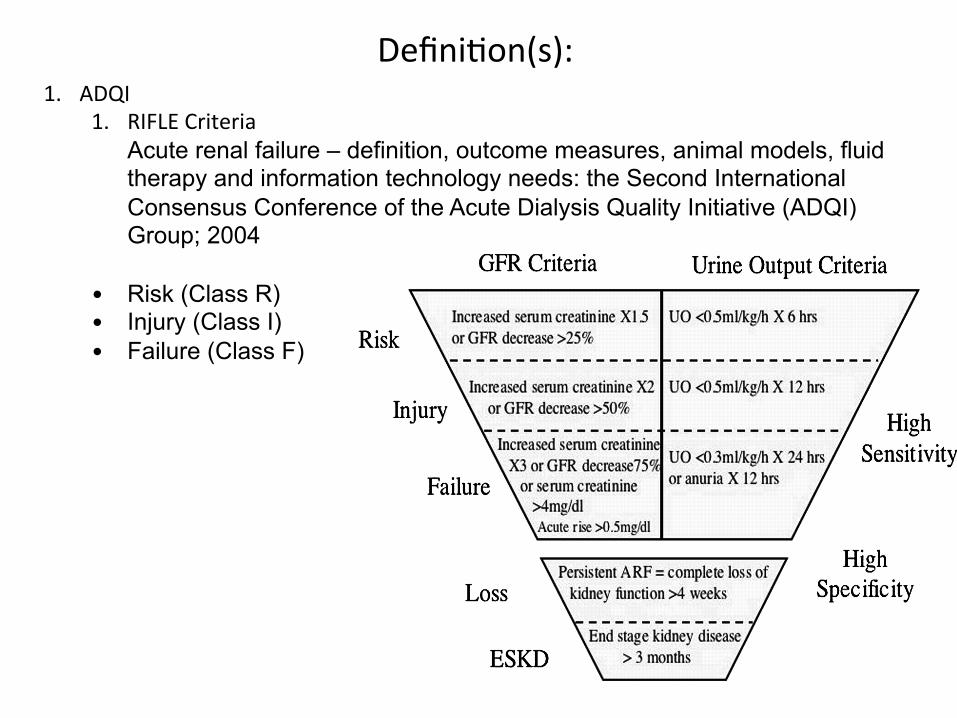
1. RIFLE Criteria Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group; 2004
• Risk (Class R) • Injury (Class I) • Failure (Class F)
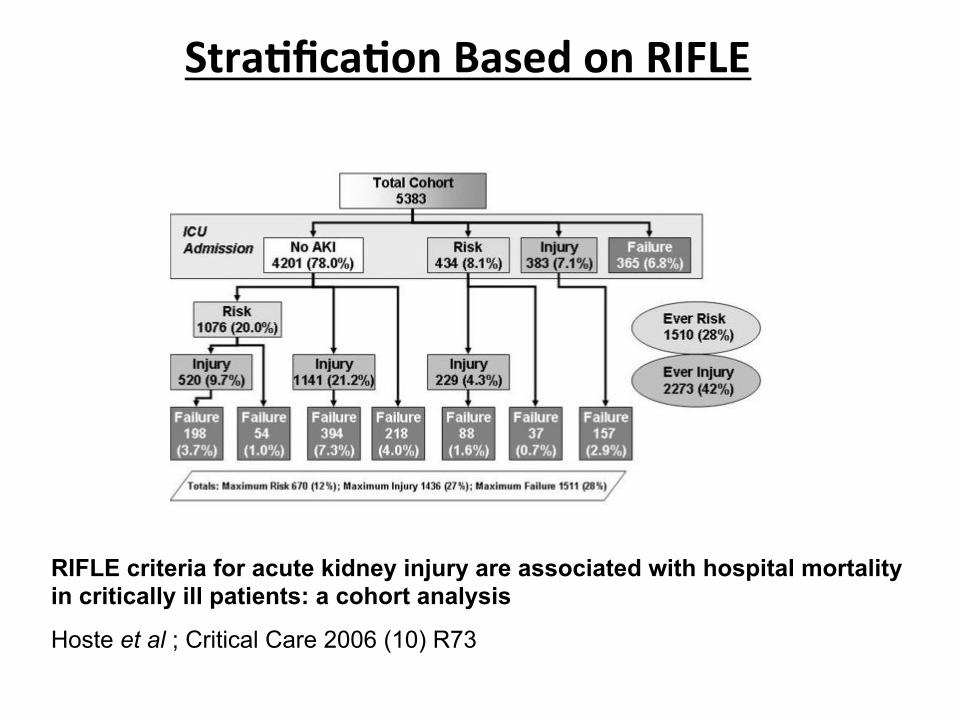
Stra%fica%on Based on RIFLE
RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis
Hoste et al ; Critical Care 2006 (10) R73

Outcomes of all Patients based on RIFLE Class

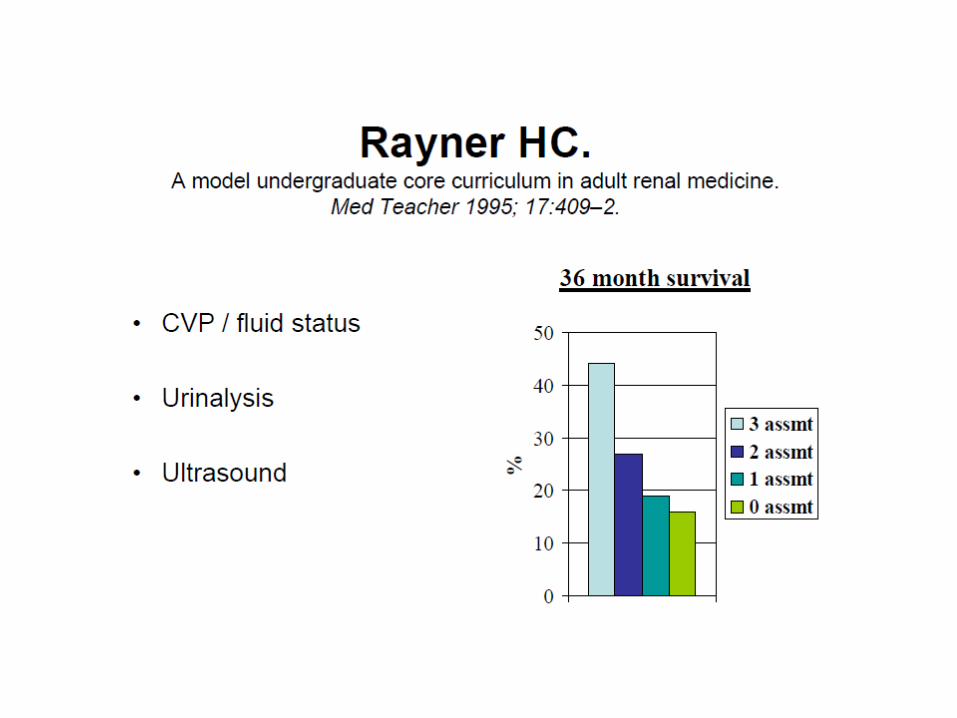
Survival: Based on RIFLE Categorisation
Defini@on(s):
1. ADQI 1. RIFLE Criteria
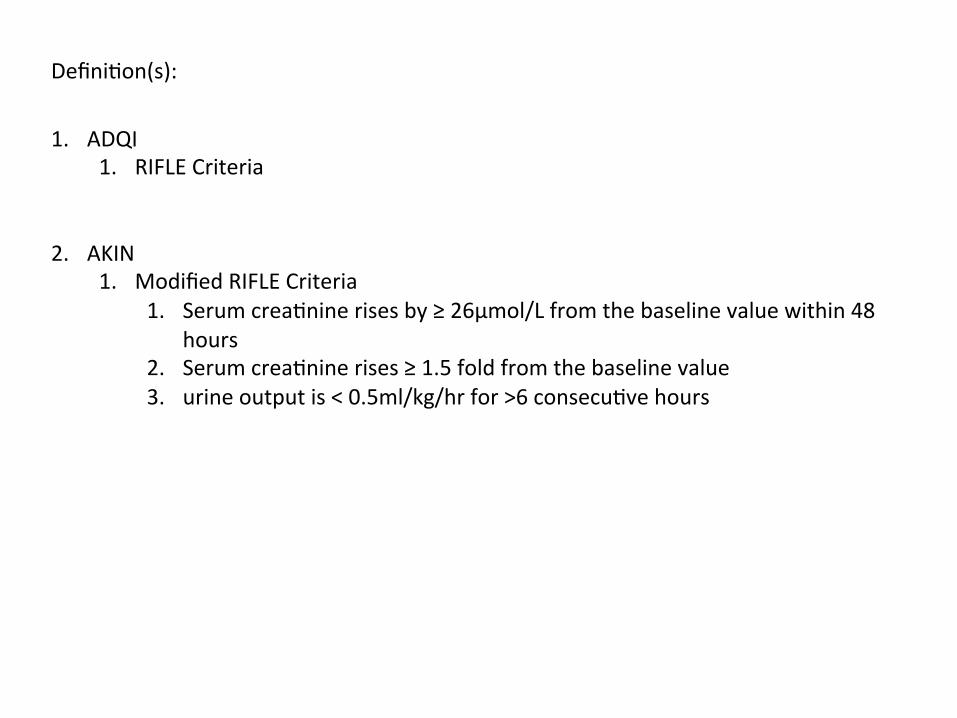
2. AKIN
1. Modified RIFLE Criteria 1. Serum crea@nine rises by ≥ 26µmol/L from the baseline value within 48
hours 2. Serum crea@nine rises ≥ 1.5 fold from the baseline value 3. urine output is < 0.5ml/kg/hr for >6 consecu@ve hours

Ques@ons in AKI


Incidence of AKI 1. US:
1. 1% 2. 7.1%
2. UK: 1. 172pmp 2. 486-‐630pmp 3. AKI-‐RRT: 20-‐203pmp
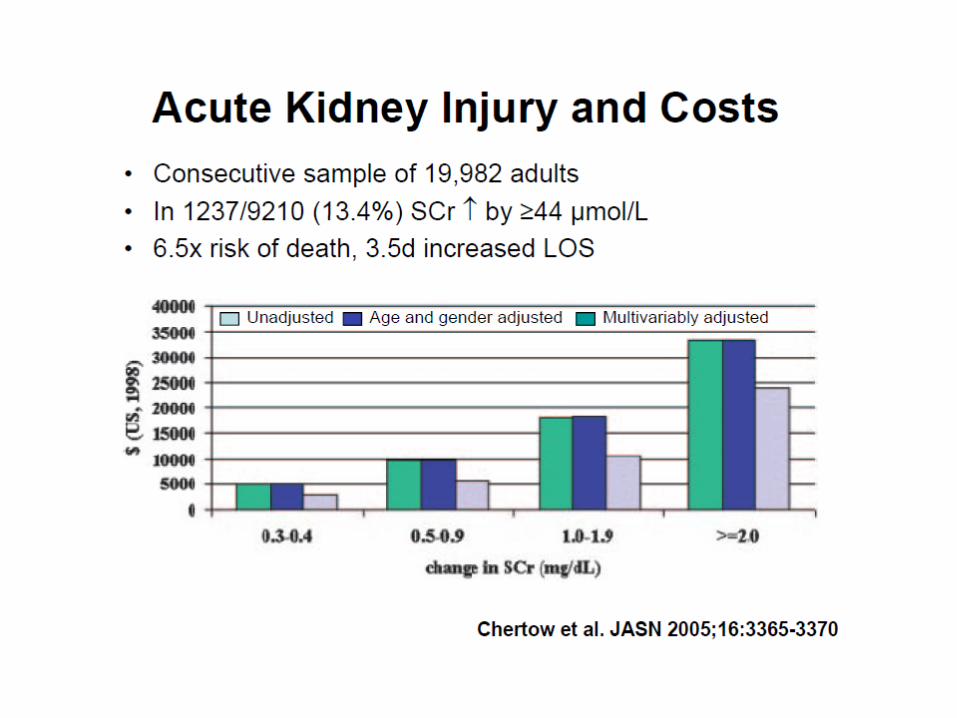
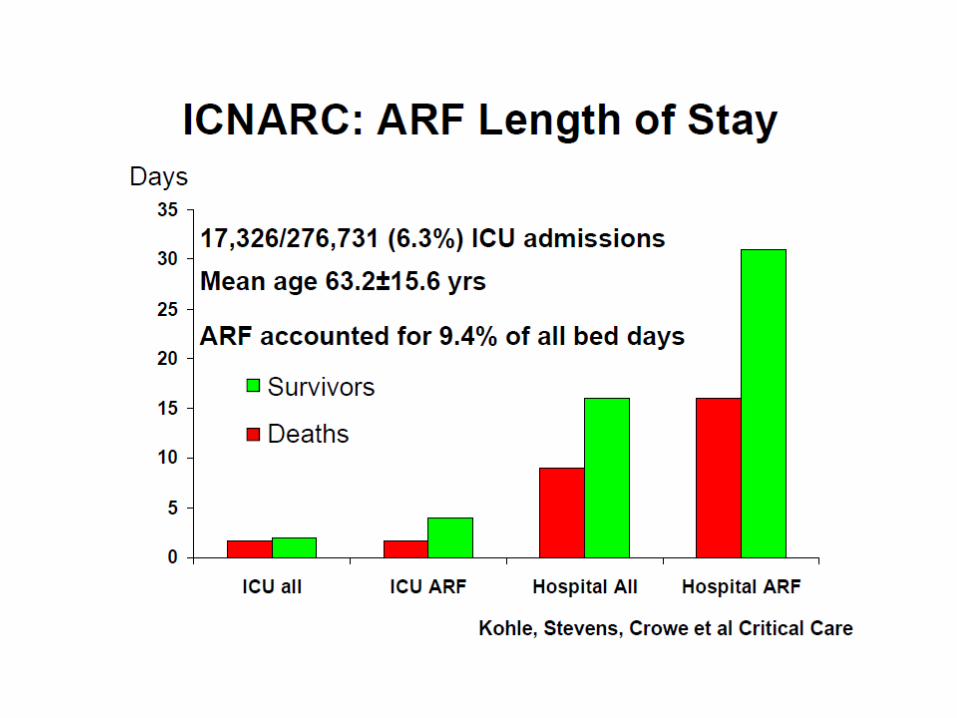
3. Cri@cal Care: 1. 5-‐20% of pa@ents develop AKI 2. 4.9% of admissions require RRT 3. AKI accounts 10% Hospital Days
4. AKI in Hospital: 1. 10-‐80% mortality 2. Uncomplicted AKI: Mortality of 10% 3. AKI in mul@-‐organ failure: 50% 4. AKI requiring RRT in Mul@-‐organ failure : 80%

Study overview
Proposed by the Renal Associa4on • Prevalent and serious problem amongst hospitalised pa@ents
• All hospital pa@ents, regardless of specialty, are at risk of AKI
• It is unknown to what degree strategies to reduce the risk of AKI are implemented
Primary aim
To examine the process of care of pa@ents
who died in hospital with AKI, in order to
iden@fy remediable factors in the care
received by these pa@ents

Data returns

Key findings
• Only 50% of AKI care considered good • Poor assessment of risk factors • Unacceptable delay in recogni@on of post-‐admission in AKI in 43%
• 22 pa@ents died with a primary diagnosis of post-‐admission AKI which was predictable and avoidable
• Complica@ons missed (13%), avoidable (17%) or badly managed (22%)

NCEPOD Report 2009
Comprehensive Assessment in AKI
3. poten@al causes for AKI including 3. reduced fluid intake 4. increased fluid losses 5. urinary tract symptoms 6. recent drug inges@on 7. sepsis
4. systemic clinical features 4. fever 5. rash 6. joint pains
1. pa@ent notes 2. AKI risk factors
1. age > 75 yrs 2. chronic kidney disease
(CKD, eGFR < 60 mls/min/1.73m2)
3. Cardiac failure 4. Atherosclero@c peripheral
vascular disease 5. Liver disease 6. Diabetes mellitus 7. Nephrotoxic medica@ons

Comprehensive Assessment in AKI • general
– rash – uvei@s – joint swelling
• assessment of volume status – core temperature – peripheral perfusion – heart rate – blood pressure – jugular venous pressure
• signs of renovascular disease – audible bruits – impalpable peripheral pulses
• abdominal examina@on – palpable bladder
Inves@ga@ons:AKI • biochemistry
– Urea and electrolytes • haematology
– FBC • urinalysis (± microscopy) • microbiology
– urine culture (if infec@on is suspected)
– blood culture (if infec@on is suspected)
• renal immunology • urinary biochemistry
– electrolytes – osmolality
• ECG • chest x-‐ray • abdominal x-‐ray • renal tract ultrasound
(within 24hrs if obstruc@on suspected)
• kidney biopsy
Measurement of Crea%nine
1. Poor Biomarker 1. Jaffe Reac@on (1886) 2. Inter-‐laboratory varia@ons and analy@cal interference
3. Interference 1. Protein, glucose, ascorbate, pyurvate, cephalosporins
2. Bilirubin 4. Enzyma@c Assays
1. Crea@ninase, cre@nase, sarcosine oxidase 5. Calibra@on against IDMS
Urine Microscopy
• Proteinuria (3+ or >) • Haematuria • Lucocyturia • Eosinophiluria • Crystalluria
– EG – TLS – S, AcyC, IndinV, TriamT, Cathar@cs
• Myoglobinuria
Urine Electrolyte Es@ma@on
1. FENa 2. FEUrea 3. Urinary Sodium Excre@on 4. Free water clearence 5. Crea@nine Clearence 6. Blood Urea:Crea@nine Ra@os
1. Pre-‐Renal Azotemia
2. ATN 3. Hepatorenal Syndrome
Biomarkers of AKI
1. NGAL 2. KIM-‐1 3. Cysta@n C 4. IL-‐8 5. NAG 6. L-‐FABP
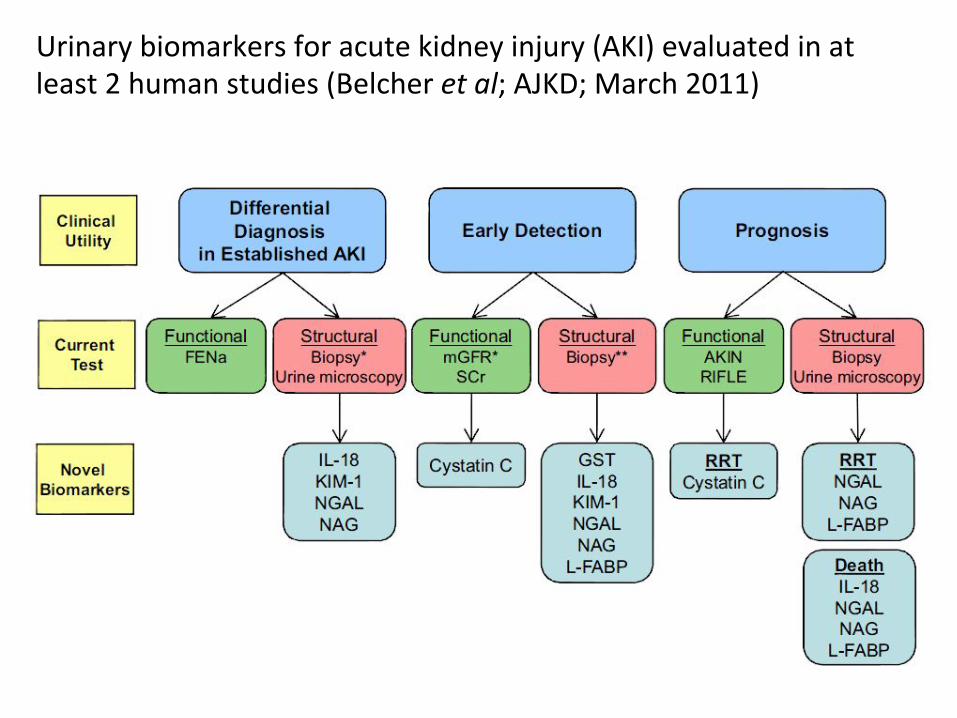
Urinary biomarkers for acute kidney injury (AKI) evaluated in at least 2 human studies (Belcher et al; AJKD; March 2011)
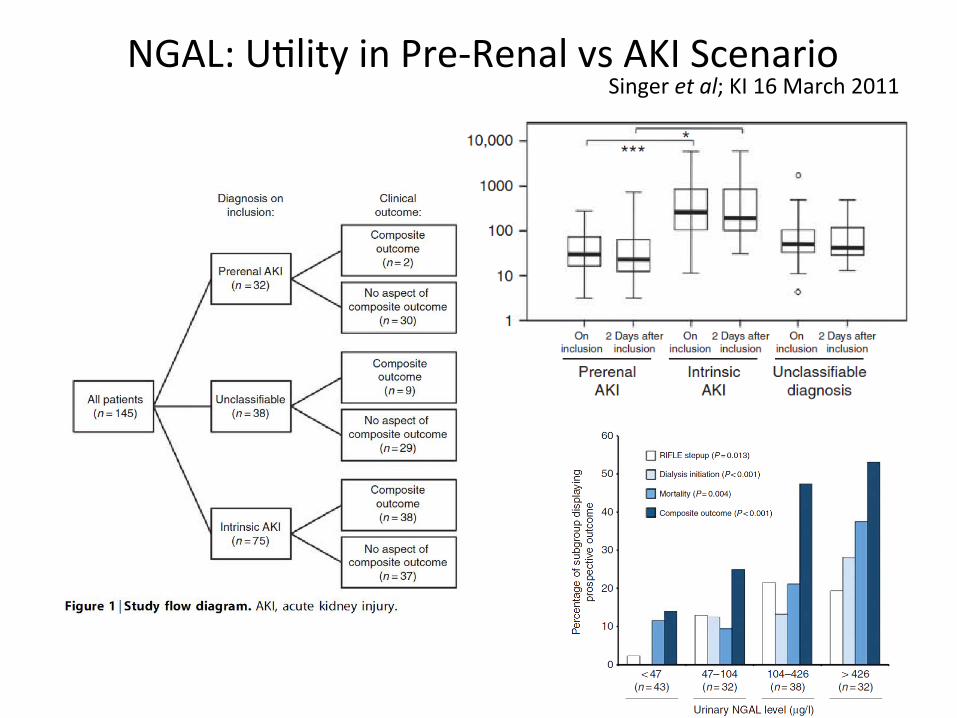
NGAL: U@lity in Pre-‐Renal vs AKI Scenario Singer et al; KI 16 March 2011
AKI-‐Preven@ve Strategies
• Major Surgery • Sepsis: SIRS v CARS; EGDT; Volume and Pressor support; euglycemia; Low Tidal Vol
• CI-‐AKI • Rhabdomyolysis

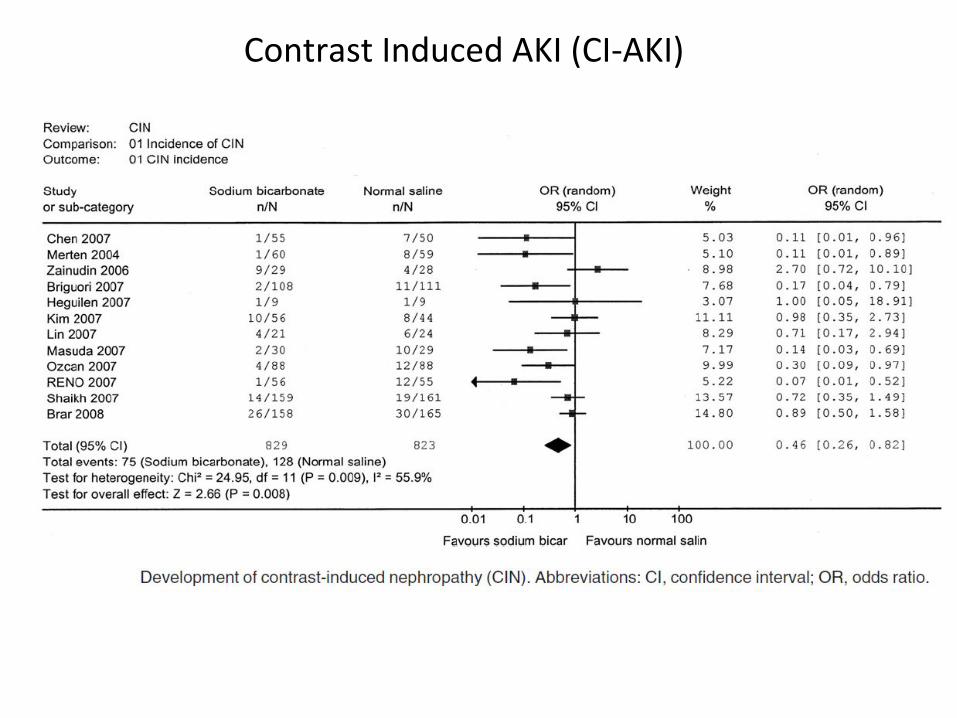
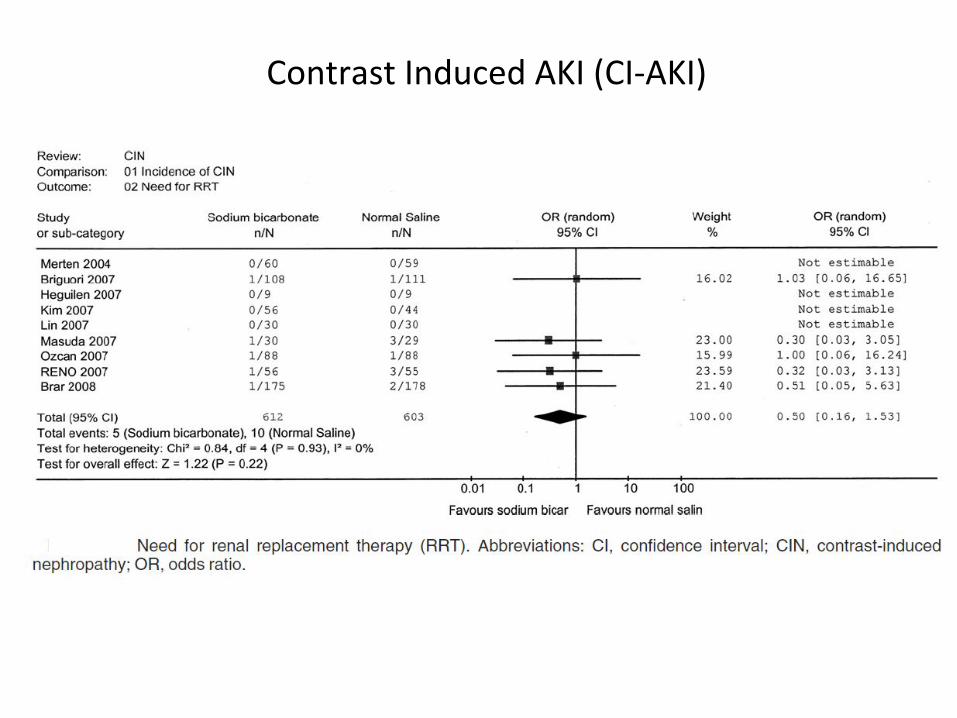
AKI: Preven@on Strategies Contrast Induced AKI (CI-‐AKI)
Parameter Number Number in Total n=12; 1854 Preven@on of CI-‐AKI using bicarbonate n = 12; 1652; OR 0.46 (0.28-‐0.82) Need for RRT n=9; 1215; OR 0.5 Survival n=11; 1640; OR 0.51 Bicarbonate use in CCF No difference in Survival; no excessive
LVF episodes
Compare with REMEDIAL (NS+NAC v NaHCO3+NAC v NAC+Vit C+NS
Hoste et al AJKD 2009
Brer et al JASN
Contrast Induced AKI (CI-‐AKI)
Contrast Induced AKI (CI-‐AKI)

Flowchart of meta-analysis.
Brar S S et al. CJASN 2009;4:1584-1592
©2009 by American Society of Nephrology
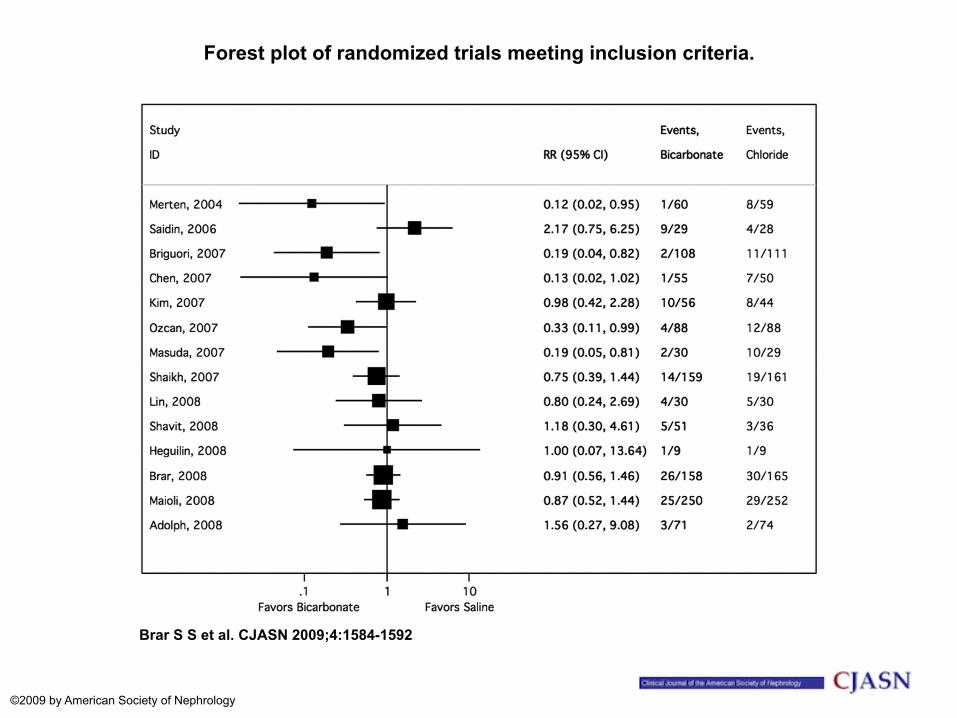
Forest plot of randomized trials meeting inclusion criteria.
Brar S S et al. CJASN 2009;4:1584-1592
©2009 by American Society of Nephrology
AKI-‐ Rhabdomyolysis
Factors 1. Trauma 2. Burns 3. Compartment Syndrome 4. Drugs
1. Sta@ns 2. Coccaine 3. Ecstasy
Management 1. Volume Assessment 2. Aggressive hydra@on 3. Alkalinisa@on
1. UO 100ml/hr 2. Urine pH>6.5
General Management
1. Fluid Resuscita@on
1. Crystalloid vs Colloid 2. Oliguric vs Non-‐Oliguric AKI
2. Pharmacological Therapy
1. Frusemide: 2. Dopamine 3. Fenoldopam 4. ANP
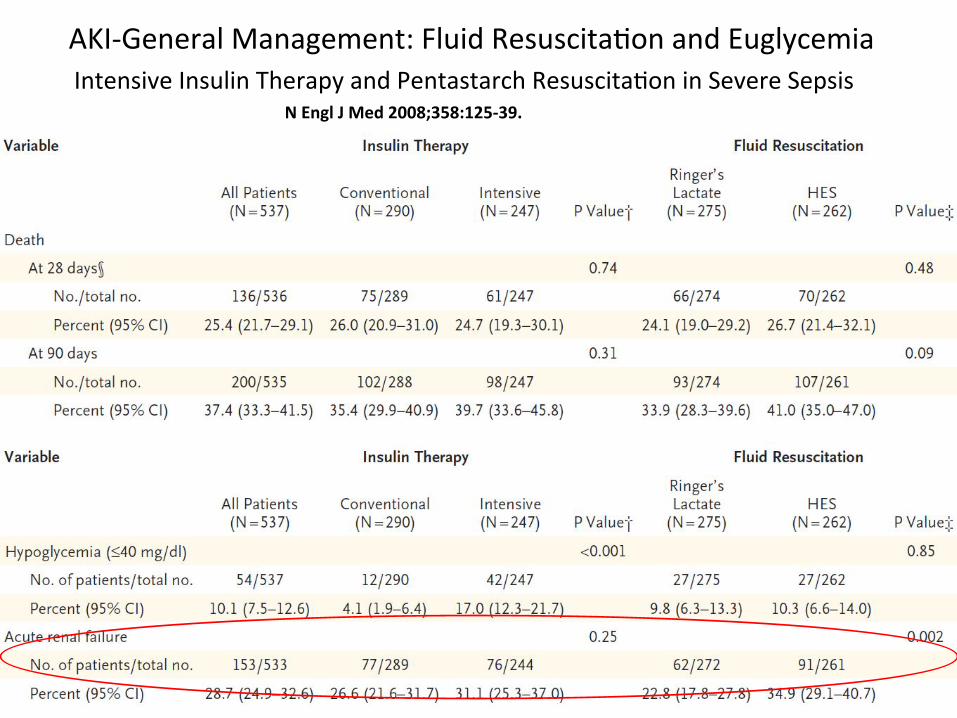
AKI-‐General Management: Fluid Resuscita@on and Euglycemia
N Engl J Med 2008;358:125-‐39. Intensive Insulin Therapy and Pentastarch Resuscita@on in Severe Sepsis
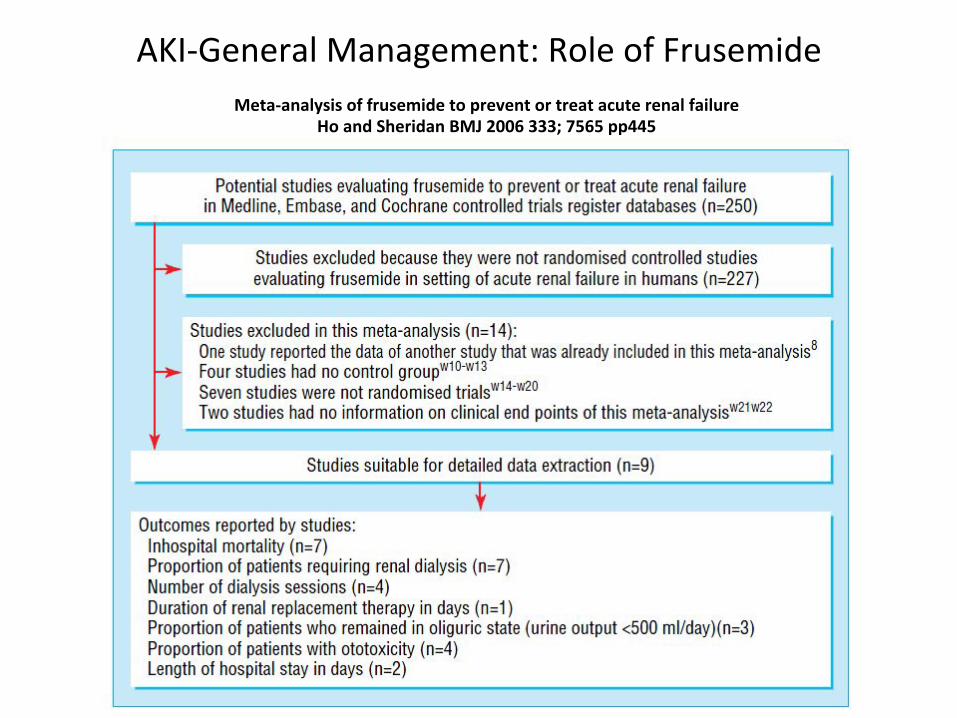
AKI-‐General Management: Role of Frusemide Meta-‐analysis of frusemide to prevent or treat acute renal failure
Ho and Sheridan BMJ 2006 333; 7565 pp445
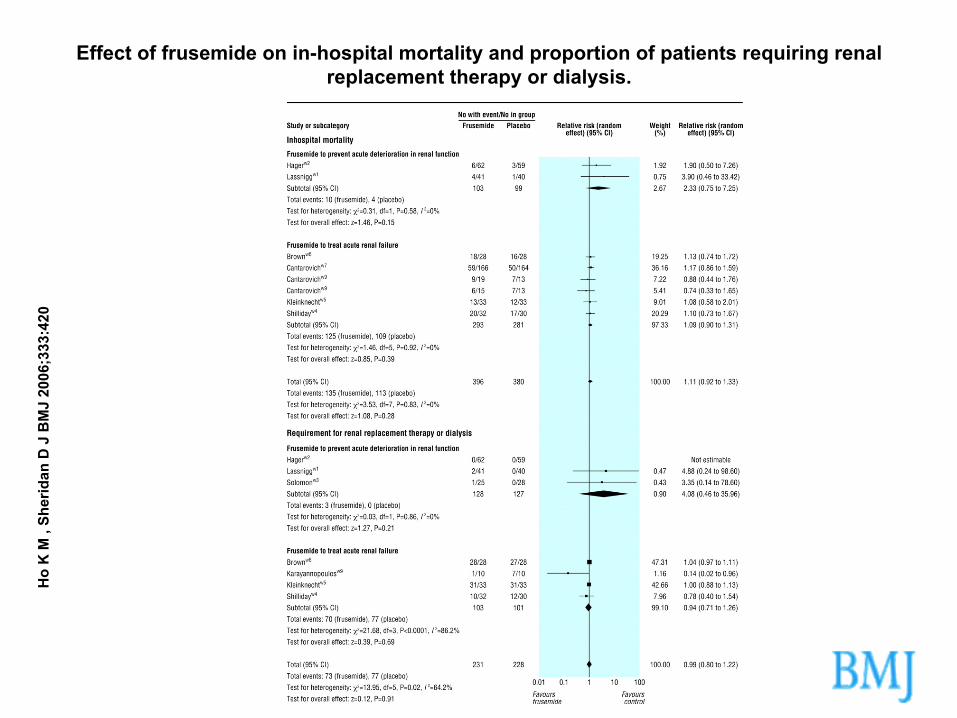
Effect of frusemide on in-hospital mortality and proportion of patients requiring renal replacement therapy or dialysis.
Ho
K M
, Sh
erid
an D
J B
MJ
2006
;333
:420
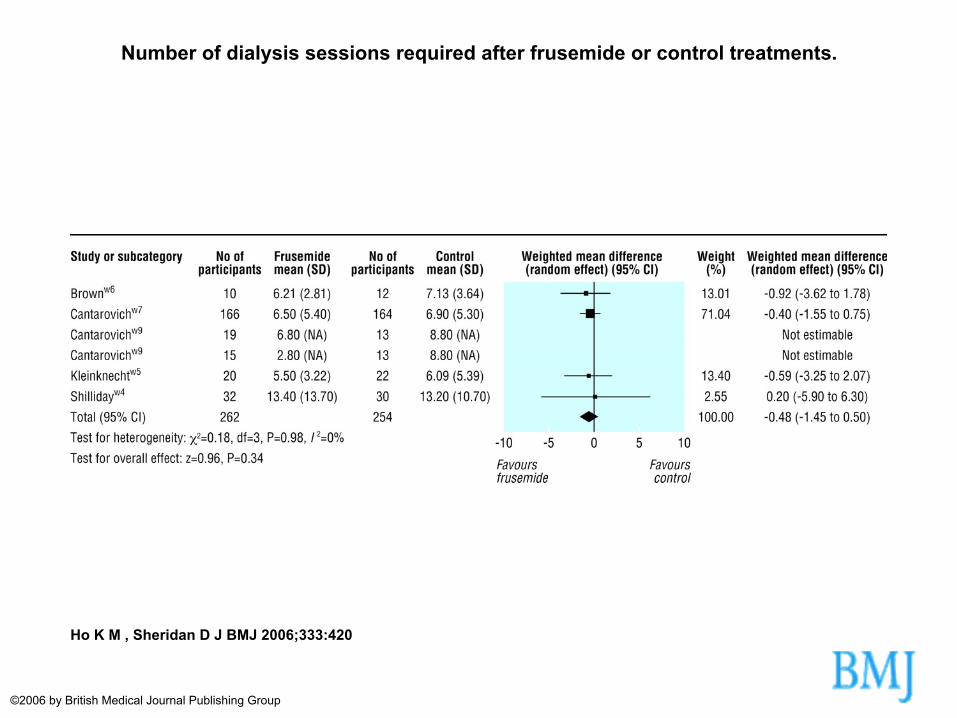
Number of dialysis sessions required after frusemide or control treatments.
Ho K M , Sheridan D J BMJ 2006;333:420
©2006 by British Medical Journal Publishing Group
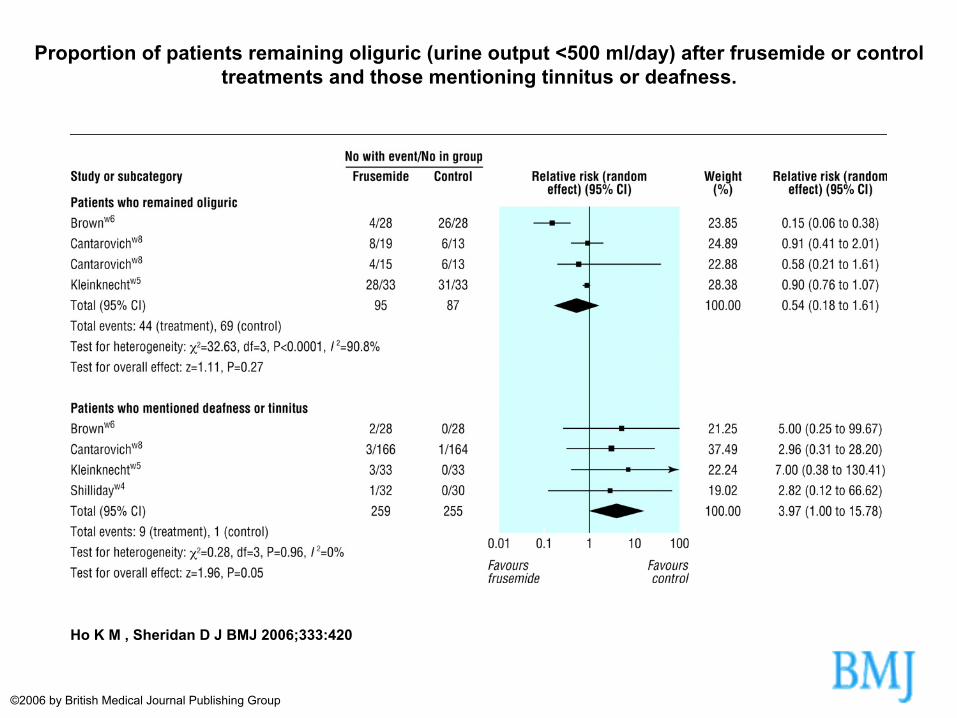
Proportion of patients remaining oliguric (urine output <500 ml/day) after frusemide or control treatments and those mentioning tinnitus or deafness.
Ho K M , Sheridan D J BMJ 2006;333:420
©2006 by British Medical Journal Publishing Group
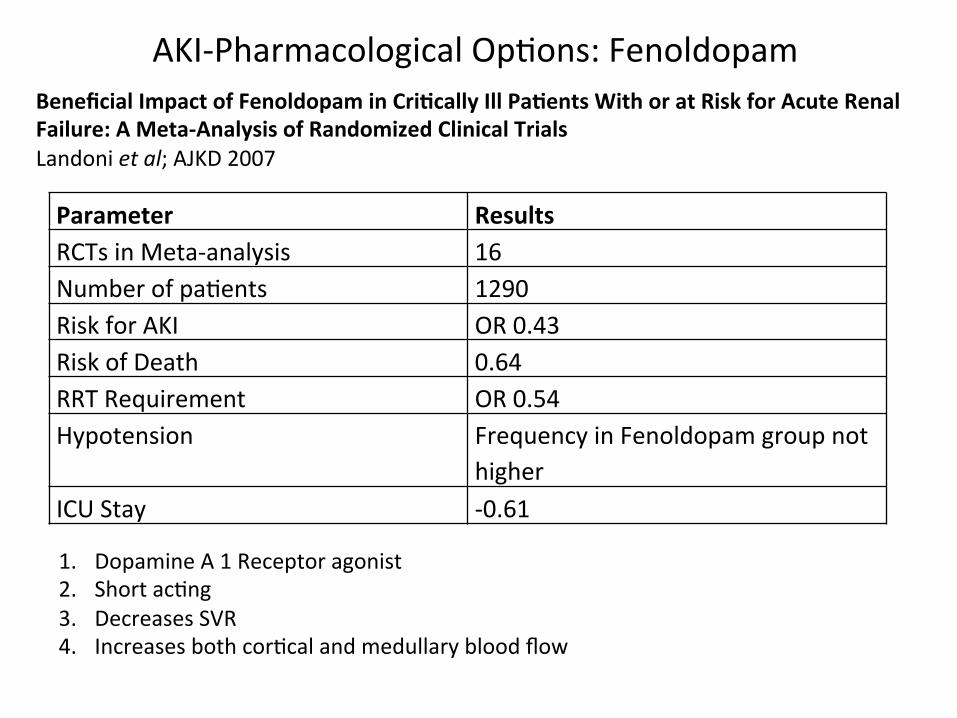
AKI-‐Pharmacological Op@ons: Fenoldopam Beneficial Impact of Fenoldopam in Cri%cally Ill Pa%ents With or at Risk for Acute Renal Failure: A Meta-‐Analysis of Randomized Clinical Trials Landoni et al; AJKD 2007
Parameter Results RCTs in Meta-‐analysis 16 Number of pa@ents 1290 Risk for AKI OR 0.43 Risk of Death 0.64 RRT Requirement OR 0.54 Hypotension Frequency in Fenoldopam group not
higher ICU Stay -‐0.61
1. Dopamine A 1 Receptor agonist 2. Short ac@ng 3. Decreases SVR 4. Increases both cor@cal and medullary blood flow

AKI-‐Pharmacological Op@ons: ANP
CJASN 2009; Nigwekar et al; 19 Trials 1861 patients
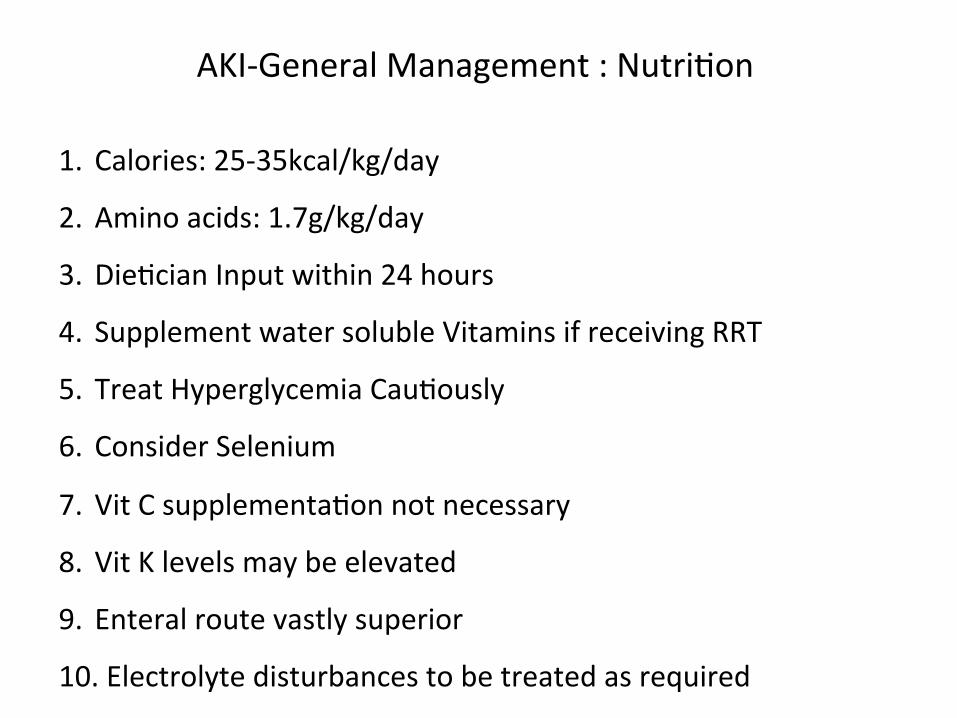
AKI-‐General Management : Nutri@on
1. Calories: 25-‐35kcal/kg/day 2. Amino acids: 1.7g/kg/day
3. Die@cian Input within 24 hours 4. Supplement water soluble Vitamins if receiving RRT
5. Treat Hyperglycemia Cau@ously
6. Consider Selenium
7. Vit C supplementa@on not necessary
8. Vit K levels may be elevated
9. Enteral route vastly superior 10. Electrolyte disturbances to be treated as required
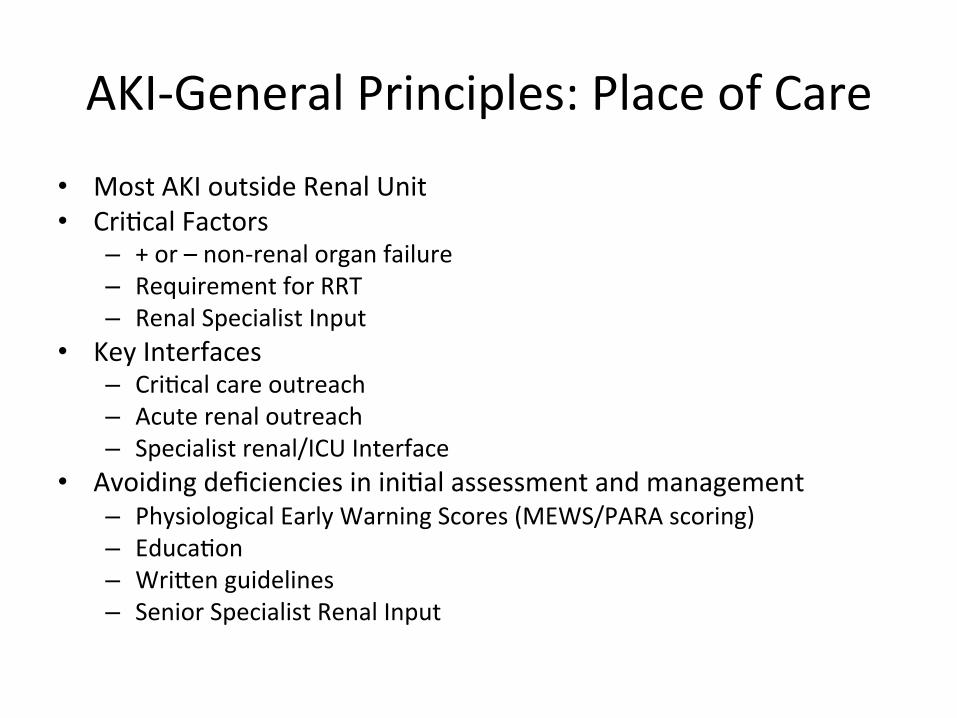
AKI-‐General Principles: Place of Care
• Most AKI outside Renal Unit • Cri@cal Factors
– + or – non-‐renal organ failure – Requirement for RRT – Renal Specialist Input
• Key Interfaces – Cri@cal care outreach – Acute renal outreach – Specialist renal/ICU Interface
• Avoiding deficiencies in ini@al assessment and management – Physiological Early Warning Scores (MEWS/PARA scoring) – Educa@on – Wrisen guidelines – Senior Specialist Renal Input

AKI-‐General Principles: Place of Care
1. Pa@ent flow from cri@cal care to renal services: a year-‐long survey in a cri@cal care network (Wright et al QJM Aug 2008) 1. 219/527 pa@ents survived 2. Incidence of RRT in ICU 234 pmp/year 3. Dura@on of RRT in ICU: 4 DAYS 4. 127/219 required renal support outside ICU 5. 74/129 were provided RRT in ICU as for single organ failure 6. 113 ICU days u@lised to provide this support
2. Kanagasundaram NS, Jones KE. Transfer of pa@ents with acute kidney injury to specialist
renal services-‐-‐physiological early-‐warning systems, applied prior to transfer from outside hospitals, can iden@fy those at risk of deteriora@on. QJM 2008;101:249-‐250 • SOFA Score to assess need for escala@on
Suppor@ve Management in AKI Principles
ü Volume ü Acid-‐base, electrolytes ü Nutri@on ü Adequate medica@on dosing
if fails……
RRT
CRRT vs
IHD
Hybrid Therapies
Which
When
How much
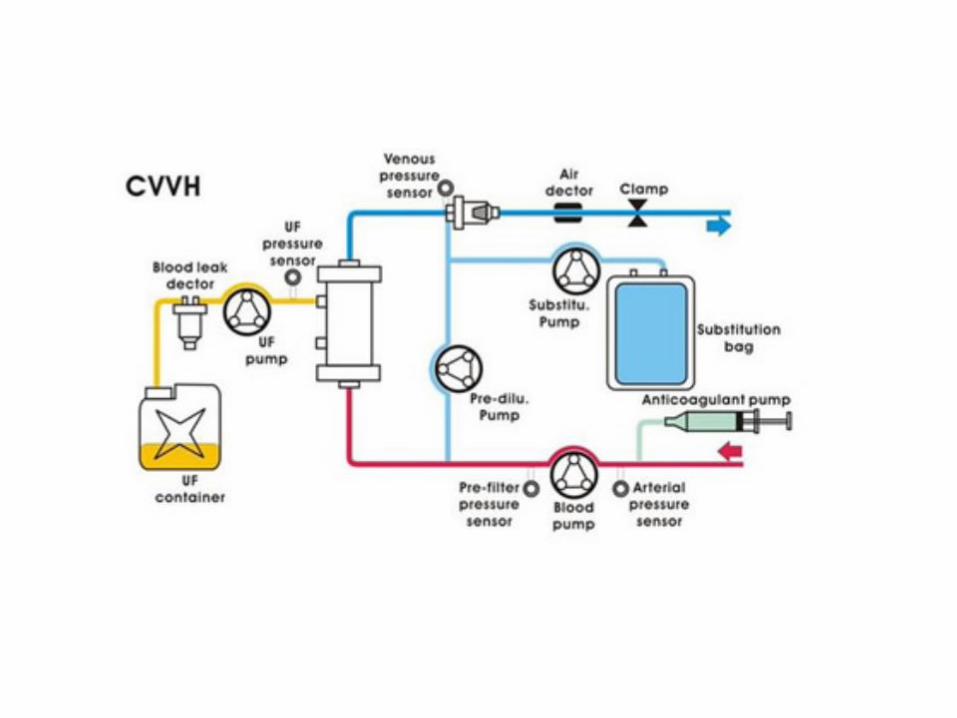

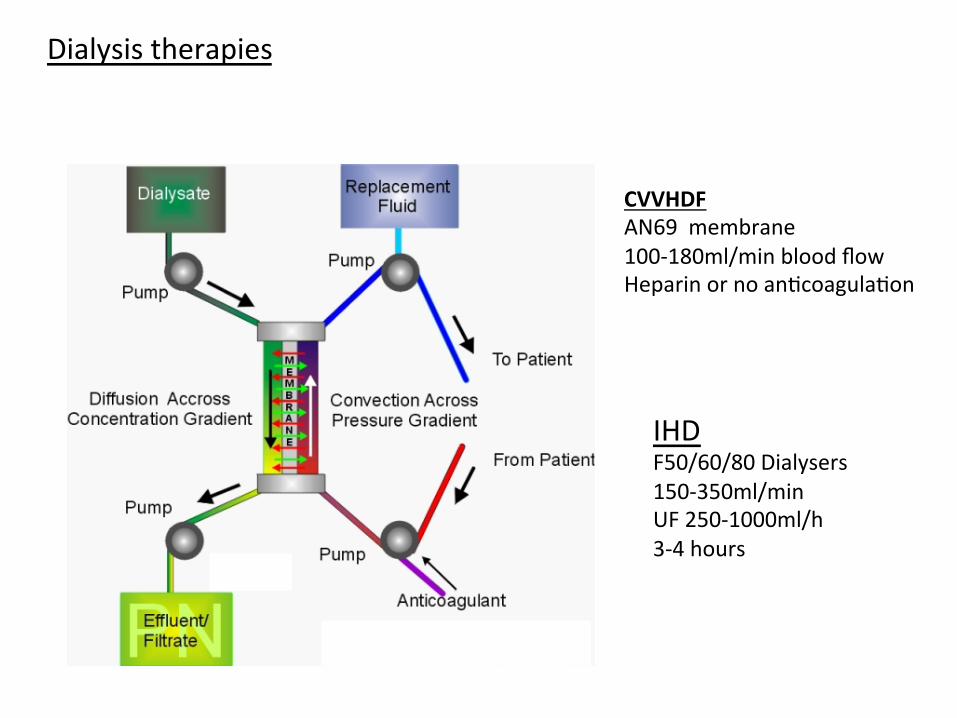
Dialysis therapies
CVVHDF AN69 membrane 100-‐180ml/min blood flow Heparin or no an@coagula@on
IHD F50/60/80 Dialysers 150-‐350ml/min UF 250-‐1000ml/h 3-‐4 hours

Story of beser haemodynamic stability in CRRT vs IHD
Authors/Setting n Outcome ITU/1993/Davenport et al 32 combined AKI/hepatic
failure Intermittent vs CAVH/CAVHD 35 vs 25 treatments Increased ICP, decreased CO, decreased DO2
Van der Scheuren 1996 N=11 IHD increases systemic O2 consumption
Heering 1997 N=33 Cytokine removal with CVVH, improvement in CV haemodynamics
Misset 1996 N=27 CAVH vs HD; MAP changes similar in both groups
John and Griesbach 2001 N=30 (20 cvvh 10 hd) CVVH vs HD in sepsis; drop in HR, slight increase BP, splanchnic perfusion parameters unchanged
Kumar 2000 N=42 (25 EDD, 17 CVVH) 367 vs 117 treatment days, 7.5 vs 19.5 hours,
Kielstein JT N= 39, (CVVH 19, EDD 20) Earlier correction of acidosis, less heparin
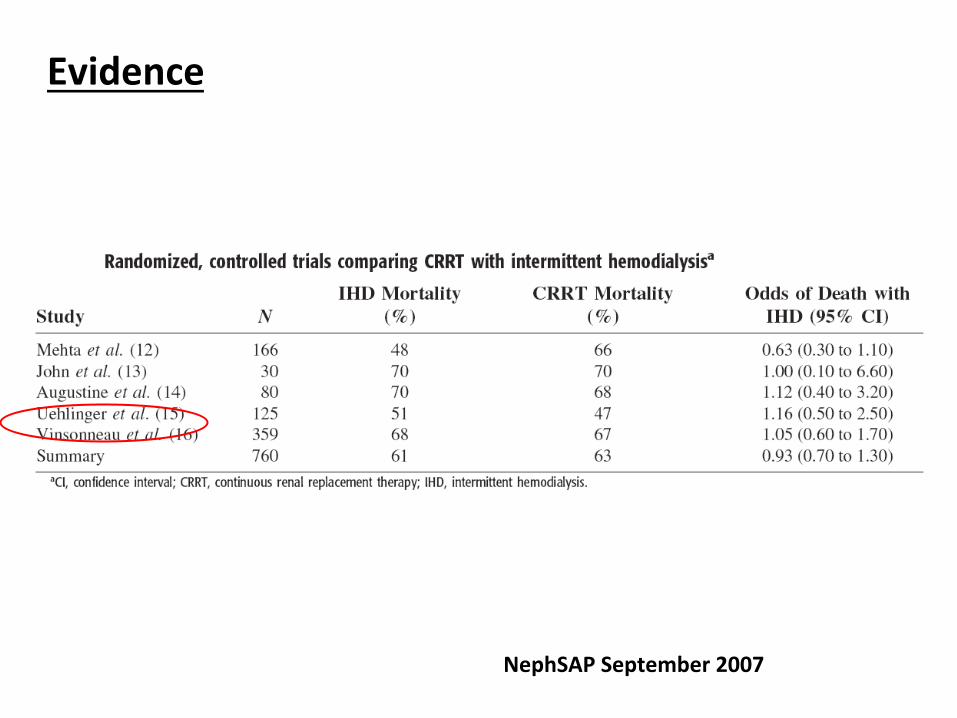
Evidence
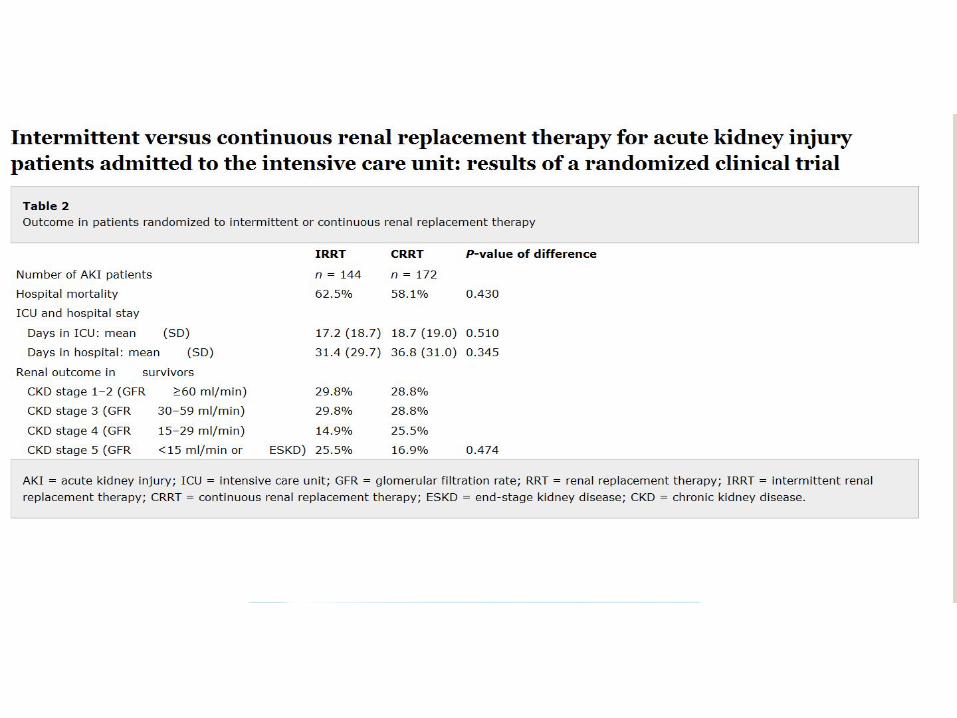
NephSAP September 2007
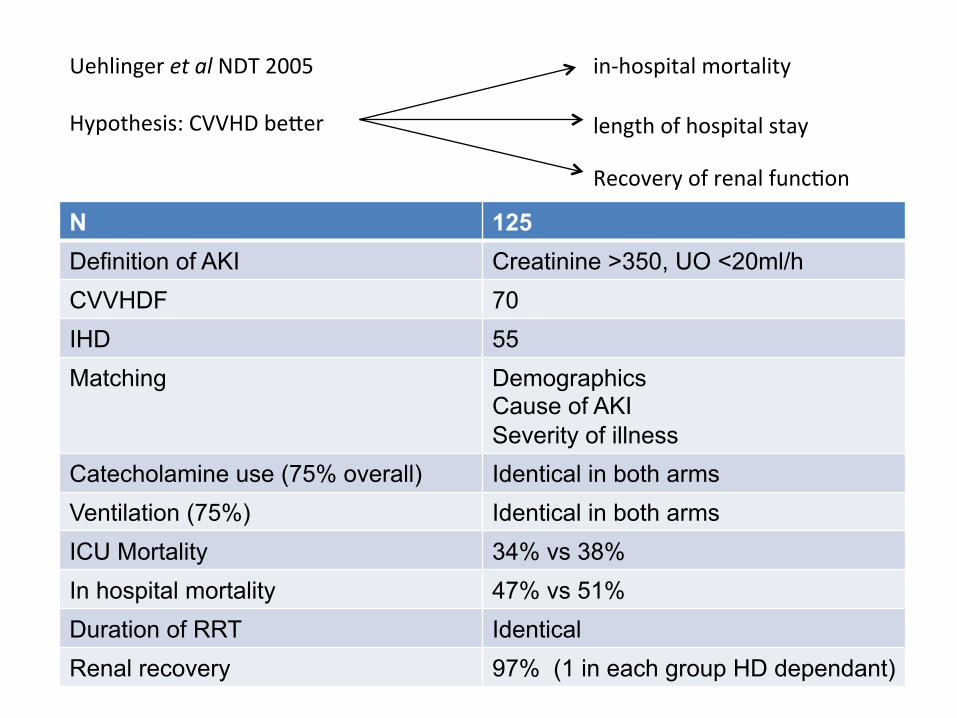
Uehlinger et al NDT 2005 Hypothesis: CVVHD beser
N 125 Definition of AKI Creatinine >350, UO <20ml/h CVVHDF 70 IHD 55 Matching Demographics
Cause of AKI Severity of illness
Catecholamine use (75% overall) Identical in both arms Ventilation (75%) Identical in both arms ICU Mortality 34% vs 38% In hospital mortality 47% vs 51% Duration of RRT Identical Renal recovery 97% (1 in each group HD dependant)
in-‐hospital mortality
length of hospital stay
Recovery of renal func@on

Blood pressure and dura@on of modali@es during ICU stay
CVVHDF vs IHD
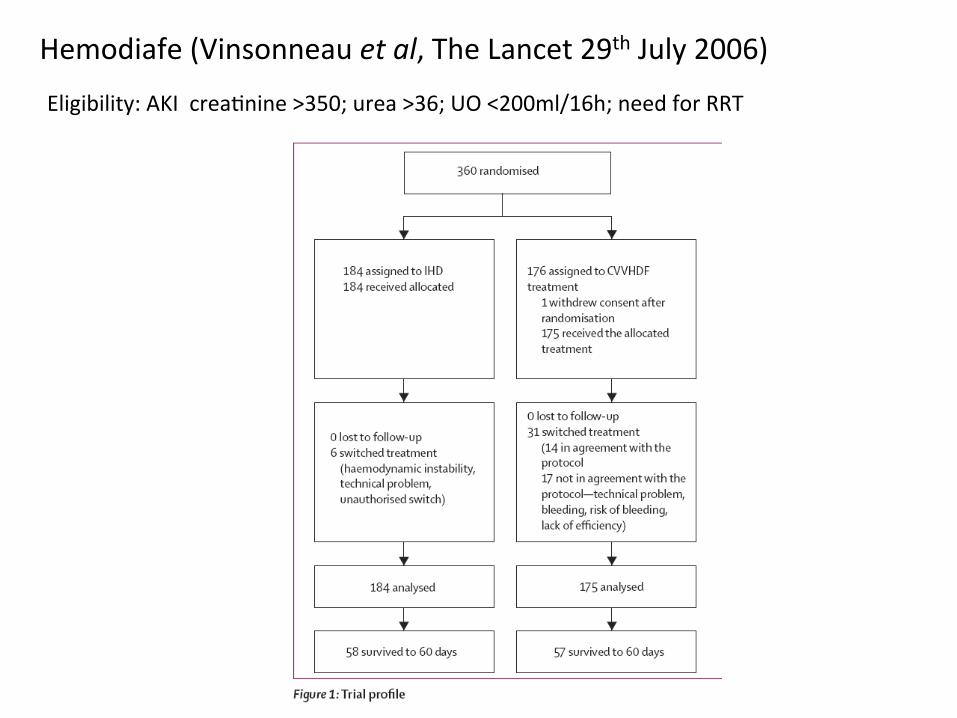
Hemodiafe (Vinsonneau et al, The Lancet 29th July 2006)
Eligibility: AKI crea@nine >350; urea >36; UO <200ml/16h; need for RRT

Survival: 32.6% vs 31.5% IHD survival improved through trial period ? CVVHDF dose inadequate
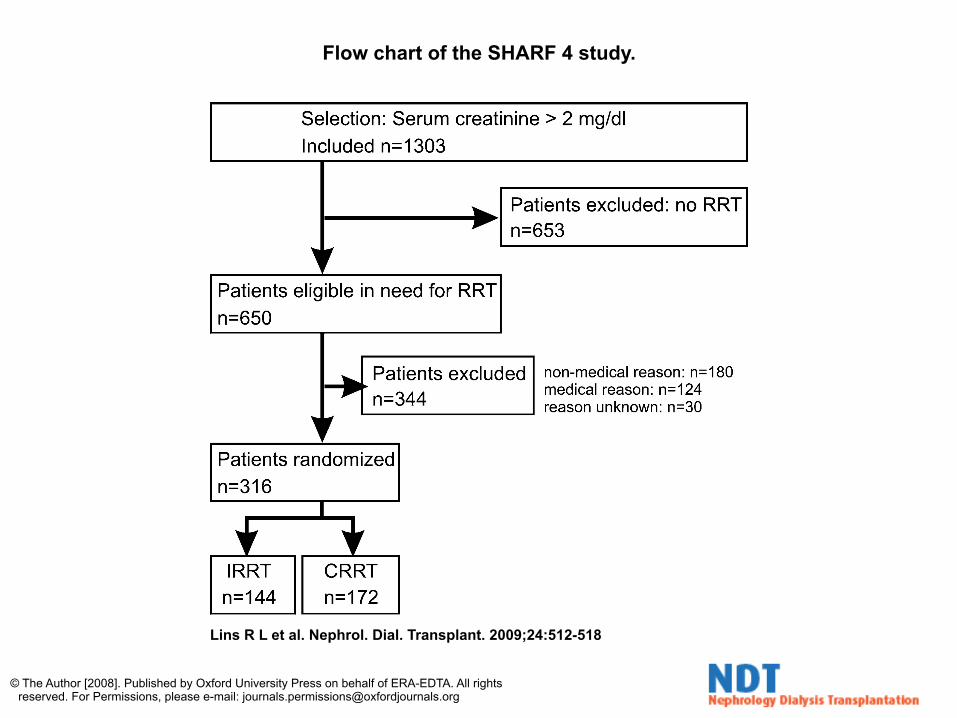
Flow chart of the SHARF 4 study.
Lins R L et al. Nephrol. Dial. Transplant. 2009;24:512-518
© The Author [2008]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please e-mail: [email protected]
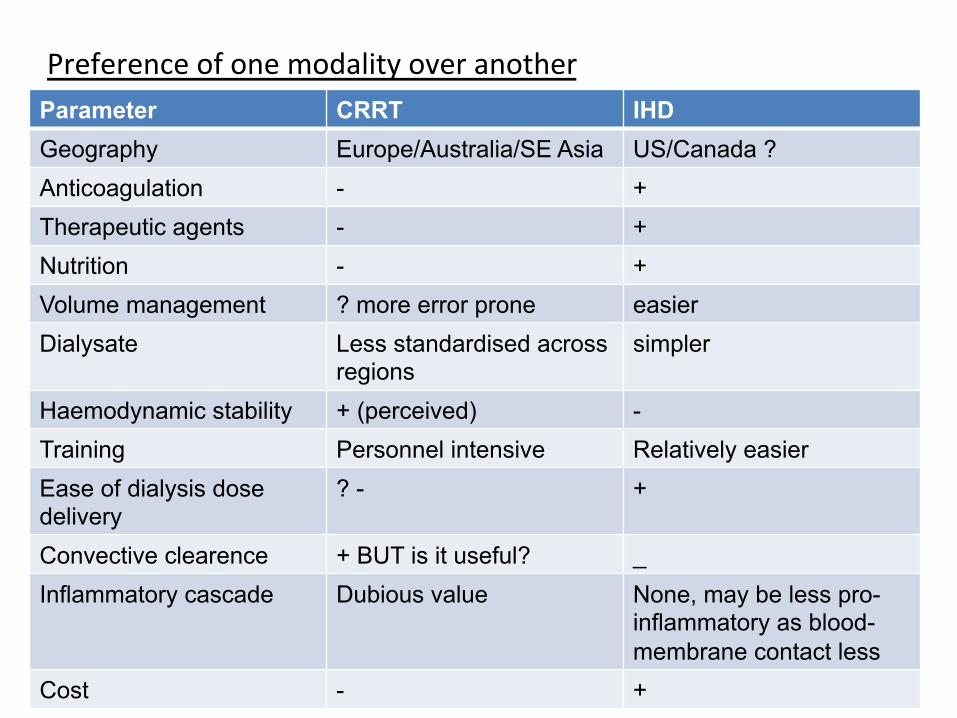
Preference of one modality over another q IHD modality of choice for managing AKI in ICU (Mehta et al)
q Local preferences; >97% of treatments for AKI in Australia are CRRT
q Haemodynamic stability governs choice of therapy
q Con@nuous removal of inflammatory cytokines beser (?)
q Blood membrane contact is pro-‐inflammatory
Parameter CRRT IHD Geography Europe/Australia/SE Asia US/Canada ? Anticoagulation - + Therapeutic agents - + Nutrition - + Volume management ? more error prone easier Dialysate Less standardised across
regions simpler
Haemodynamic stability + (perceived) - Training Personnel intensive Relatively easier Ease of dialysis dose delivery
? - +
Convective clearence + BUT is it useful? _ Inflammatory cascade Dubious value None, may be less pro-
inflammatory as blood-membrane contact less
Cost - +
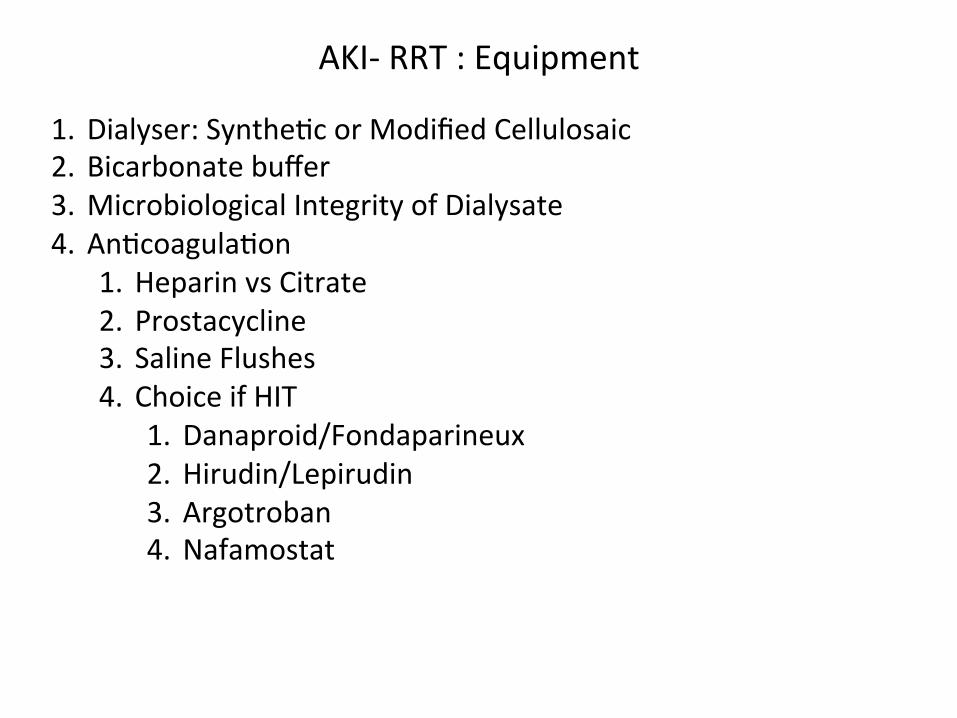
AKI-‐ RRT : Equipment
1. Dialyser: Synthe@c or Modified Cellulosaic 2. Bicarbonate buffer 3. Microbiological Integrity of Dialysate 4. An@coagula@on
1. Heparin vs Citrate 2. Prostacycline 3. Saline Flushes 4. Choice if HIT
1. Danaproid/Fondaparineux 2. Hirudin/Lepirudin 3. Argotroban 4. Nafamostat

AKI-‐ Dose of RRT Kt/V ~ 1.2 URR > 65%
Evidence:
1. Veteran Affairs/Na@onal Ins@tute of Health Acute Renal Failure Trial Network 2. Randomised Evalua@on of Normal Versus Augmented Level Renal Replacement
Therapy (RENAL)

How much? Ronco et al Lancet July 2000 Efficacy of three different doses of CVVH
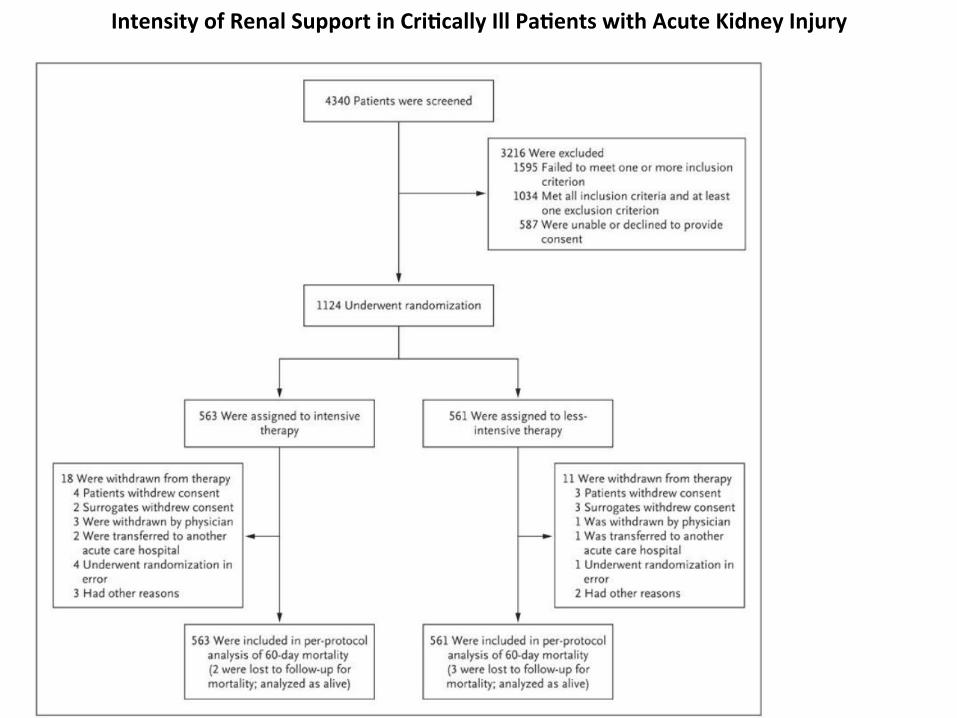
Intensity of Renal Support in Cri%cally Ill Pa%ents with Acute Kidney Injury
Intensity of Renal Support in Cri%cally Ill Pa%ents with Acute Kidney Injury
• Intense vs Conven@onal – IHD/SLED 6 @mes/week – CVVH at 35ml/kg/hour
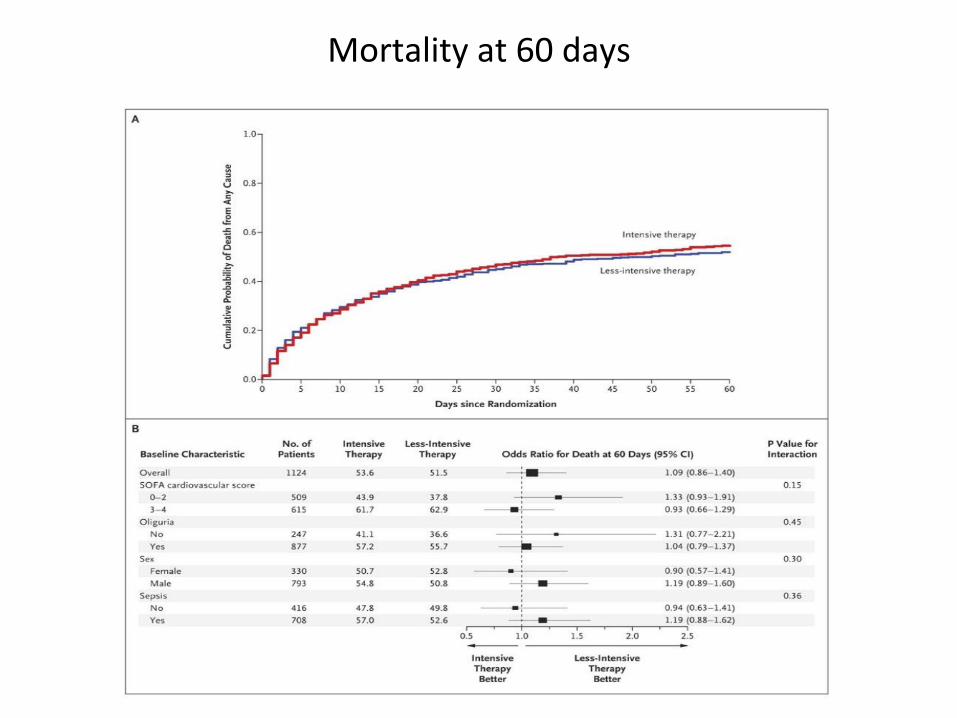
Mortality at 60 days

RENAL Study Design
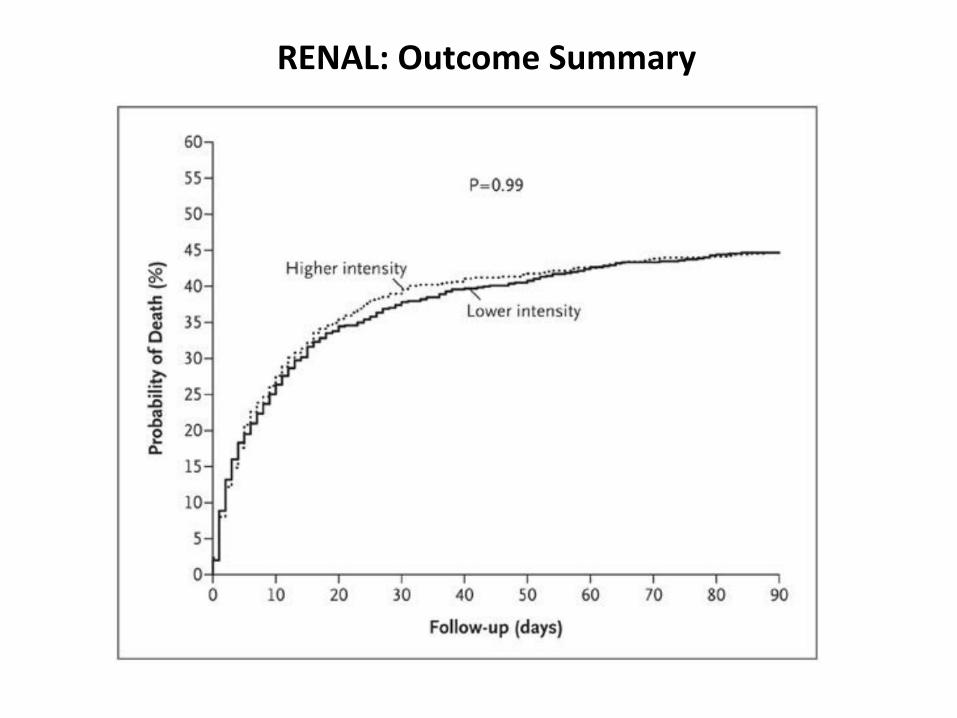
RENAL: Outcome Summary
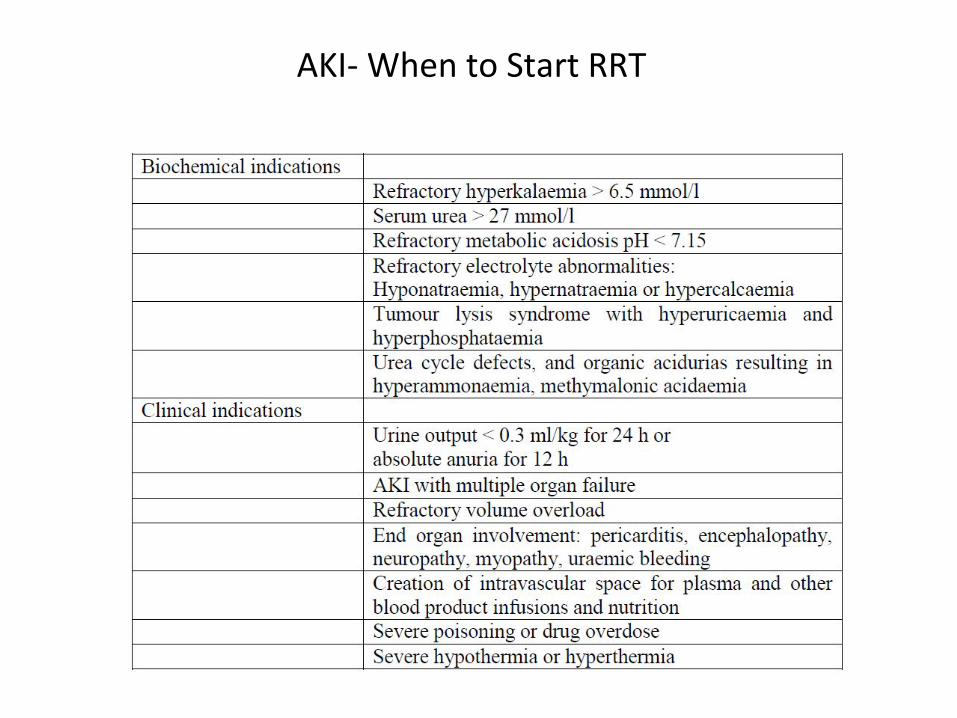
AKI-‐ When to Start RRT

Era Number Criteria 1960s/1970s/1980s 3 BUN 90-100mg/dl 1990s At least 2 of importance
n=100; higher survival in early initiation n= 64, Cardiac ITU, 22 vs 43:: early/late
<60 BUN group vs >60 8 hr oliguria / >84mg/dl
PICARD n=243 Survival 80 & 65 (early) 75 & 59 (late) RR 1.85 (co-variate adj) RR 2.07 (propensity sco)
<76mg/dl vs >76mg/dl
BUT Urea cannot be a surrogate for dura@on of AKI AND spontaneous recovery or death without RRT
AKI-‐ When to Start RRT • Early start a ‘good idea’
• How early is early – Perhaps Stage 3 of AKIN
• Balance Early start with – Morbidity associated with RRT – ? Delays recovery from AKI – Many pa@ents pull back from brink with suppor@ve therapy
– Urea of 28mmol/L a cut off? 21.5mmol/l? UO <100ml/8hr
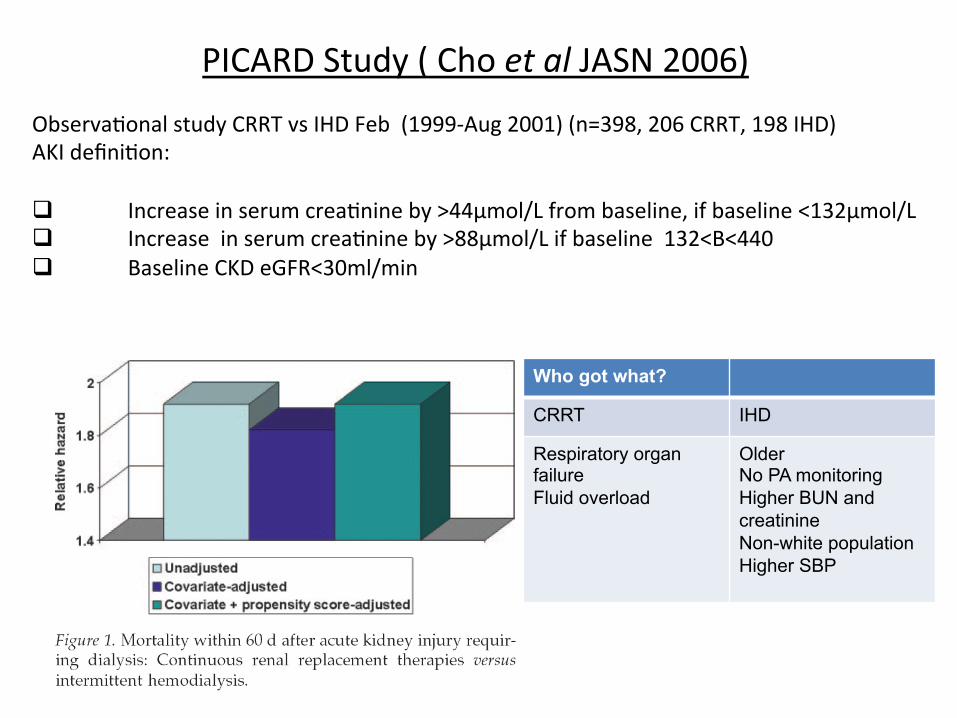
PICARD Study ( Cho et al JASN 2006) Observa@onal study CRRT vs IHD Feb (1999-‐Aug 2001) (n=398, 206 CRRT, 198 IHD) AKI defini@on: q Increase in serum crea@nine by >44μmol/L from baseline, if baseline <132μmol/L q Increase in serum crea@nine by >88μmol/L if baseline 132<B<440 q Baseline CKD eGFR<30ml/min
Who got what?
CRRT IHD
Respiratory organ failure Fluid overload
Older No PA monitoring Higher BUN and creatinine Non-white population Higher SBP
AKI-‐ Timing of RRT
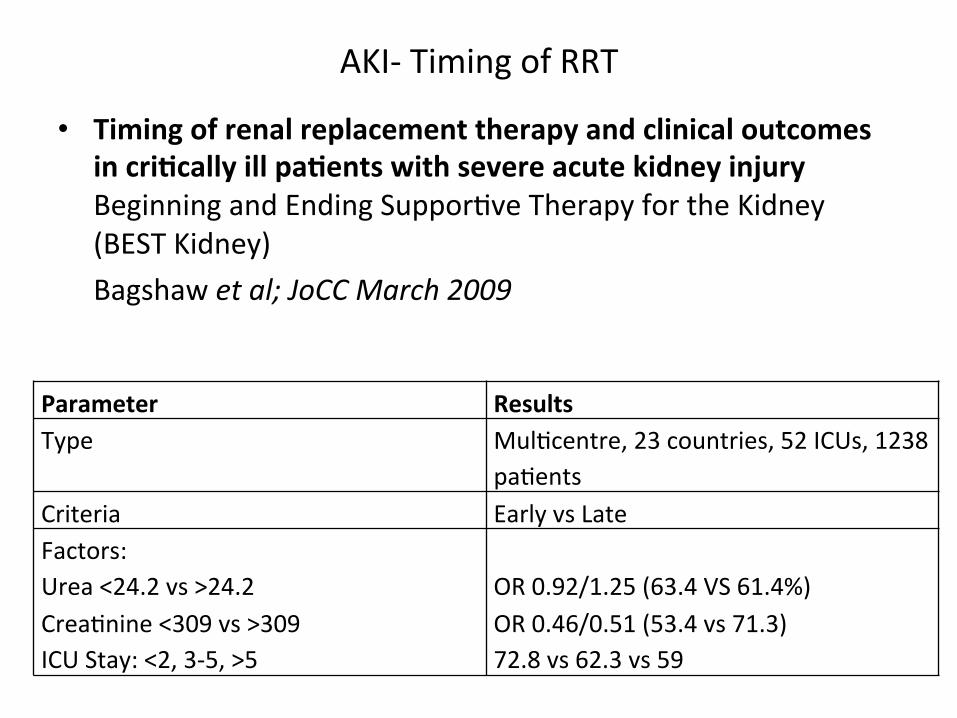
• Timing of renal replacement therapy and clinical outcomes in cri%cally ill pa%ents with severe acute kidney injury Beginning and Ending Suppor@ve Therapy for the Kidney (BEST Kidney) Bagshaw et al; JoCC March 2009
Parameter Results Type Mul@centre, 23 countries, 52 ICUs, 1238
pa@ents Criteria Early vs Late Factors: Urea <24.2 vs >24.2 Crea@nine <309 vs >309 ICU Stay: <2, 3-‐5, >5
OR 0.92/1.25 (63.4 VS 61.4%) OR 0.46/0.51 (53.4 vs 71.3) 72.8 vs 62.3 vs 59
AKI-‐Educa@on