addendum no. 1 - cook county health and hospital · pdf filethe rfp question cchhs response 1...
TRANSCRIPT

Page 1 of 12
ADDENDUM NO. 1 May 27, 2016 Real-Time Provider Connectivity for CountyCare Health Plan RFP # H16-0015
1. General
This addendum revises RFP documents. This addendum is issued to respondents of record prior to execution of contract, and forms a part of contract documents and modifies previously issued documents. Insofar as previously issued contract documents are inconsistent with modifications indicated by this addendum, modifications indicated by this addendum shall govern. Where any part of the contract documents are modified by this addendum, all unaltered provisions shall remain in effect.
2. Addendum Acknowledgement Form
Acknowledge receipt of this addendum in the space provided on the Addendum Acknowledgement Form. Proposers must include the signed form with their response. Failure to do so will subject Proposers to disqualification.
3. Changes and Clarifications
a. Responses to Vendor Questions are provided below.
4. Attachments
a. Pricing Proposal attached
NEXT PAGE

Page 2 of 12
Responses to Vendor Questions
ID Section of
the RFP Question CCHHS Response
1 The RFP asks for expansion of alerts to include services provided by …….. a. can you be specific about the types of alerts that CCHS is looking b. what are the existing alert types, what new alerts are being requested
As noted in ‘Purpose’ on page 5 of the RFP, the on-line system is to provide real-time alerts to medical homes, other providers, care coordination teams and outreach/linkage teams of acute care inpatient and emergency department admissions and discharges. Expansion of these, as allowed by law, would include admission/discharge notification by select mental health providers, substance abuse providers, immediate and urgent care centers, and CCHHS’ correctional health services.
2 Can you itemize the number of users and organizations that require on-line access
Users at over 180 different locations have on-line access to the existing system. Assuming an average of three users/site, there are over 540 user logins. It can be assumed that roughly one-third (150) access the system at any one time. CCHHS expects the proposed solution to have proven scalability to this level (i.e. examples of site stress testing or actual use). A detailed listing of sites needing access will be defined during contracting.
3 Regarding integration of data feeds: could you please indicate what systems, data sets and providers you seek to do the integration from
Eleven participating hospital organizations send data from 21 institutions through HL7 messaging to the online system. Additional data (e.g. claims, pharmacy claims, eligibility) are sent in either industry-standard formats (e.g. 837, 834) or through mutually agreed upon formats by CCHHS and/or its designee.
4 Finally, could you provide an extension on the due date to allow us to provide a proposal the properly covers the requirements as specified in the RFP?
No extensions to the RFP will be provided.
5 2 Please provide more details about where CCHHS sits in its NCQA compliance journey. Does CCHHS hold any NCQA certifications today?
CCHHS’ Medicaid health plan, CountyCare, is working towards NCQA Health Plan Accreditation by July, 2017. The health system does not hold any other NCQA accreditations.
6 4 How many end users are on the current system? (Please break down by number of sites and types of provider if possible)
See question #2 above.
7 4 Please provide a high-level system architecture diagram.
See diagram on Page 11 below.
8 4 Please provide a description of each of the systems used today (names, versions, description)?
The currently used system is MHNConnect, a proprietary system of the Medical Home Network (MHN).
9 4 How many records/messages/events flow back and forth on a daily basis?
About 500.

Page 3 of 12
ID Section of
the RFP Question CCHHS Response
10 4 How much data (TB/GB) is shared on a daily basis?
Around 50 MB
11 4 How many users are expected to be on the new system? (Please break down by number of sites and types of provider if possible)
See question #2 above.
12 4 How much user growth do you expect over the length of the contract?
As noted in Sections #4, #5.3.2 and #8.1 of the RFP, Proposers are expected to outline and discuss the development, implementation and management of an incentive program that increases utilization of the on-line portal. CCHHS expects this incentive program will result in increased use of the portal to levels consistent with the service utilization of the provider’s assigned membership.
13 4 Please provide any specific use cases you may have for the new platform. Which use cases will be on mobile versus a desktop/laptop platform?
CountyCare’s care coordination model is centered at the point of care, not centralized in a typical health plan call center environment. For this reason, mobile access, including manual data input to the application, is necessary.
14 4 Does the solution need to support languages other than English (e.g. Spanish)?
No. The software is not member facing.
15 4 What analytics/reports will need to be implemented?
Analytics/reporting is not a specified requirement in the RFP. General reports on system utilization, including impact of an incentive program, however, are expected.
16 4 Will the solution need to support ad-hoc and custom reporting?
See question #15 above.
17 5.1.3 Is CCHHS open to a public cloud-based solution (e.g. Amazon Web Services) for hosting?
Yes, as long as they are deemed HIPAA-compliant. Proposers should address this if they are recommending this as a solution.
18 5.1.3 Are you looking to migrate your existing platform to the new platform?
No.
19 5.1.10 Will the solution need to support bi-directional data feeds? Would users be able to write to source systems/databases?
Bi-directional data feeds are not required. End-user, manual data entry may be needed depending on the proposed solution.
20 5.1.10 What standards are used for messaging in the existing platform (HL7, API, or others?)
HL7 messaging.
21 5.1.10 In what format are the data feeds from your TPAs (after hours, crisis lines, etc.)
See question #3 above. Integration of non-standard format, flat file data (e.g. after hours nurse hotline, crisis lines, etc.) is out of scope, yet proposers are encouraged to consider this level of integration in their responses as a value-added service.

Page 4 of 12
ID Section of
the RFP Question CCHHS Response
22 5.1.10 Please list the interfaces that exist in today’s solution.
There are four major data feeds today: Description Source Format
Medical Claims
CCHHS or designee
Standard file format (835, 837) or mutually-agreed upon format (flat file, etc.)
Rx Claims CCHHS or designee
Standard file format (835, 837) or mutually-agreed upon format (flat file, etc.)
Member Eligibility
CCHHS or designee
Standard 834 file format
ADT Data Participating hospitals
HL7 message
23 5.1.10 Do you have access to a claims data warehouse from the health plan?
Yes.
24 5.1.10 If so, how many years of claims history do you have?
Three.
25 3 In Section 3 (Schedule), the Proposal Due Date is mentioned as June 3, 2016. We request that the proposal due date be extended by 2 weeks to June 17, 2016. Can you please confirm this extension?
No extensions to the RFP will be provided.
26 4 The CountyCare Health Plan has an existing online notification system for its contracted network of providers. Please provide details of this existing system including the implementation vendor.
MHNConnect is the current tool. It is the proprietary software of Medical Home Network who oversees its implementation.
27 4 The CountyCare Health Plan has an existing online notification system for its contracted network of providers. As part of this RFP, does CountyCare wish to replace the existing system with a new system?
It is CCHHS’ desire to continue offering a connectivity solution beyond the term of the current agreement.
28
4 The CountyCare Health Plan has an existing online notification system for its contracted network of providers. This includes all network PCPs (over 180 access points), 14 community-based hospitals and 3 academic medical centers. In addition, what are the other providers in the CountyCare network who need to be covered by the new system?
All of the CountyCare PCPs have on-line access to the system. A majority of acute care hospitals in the CountyCare network provide ADT feeds to the system. CountyCare desires an expansion of these ‘suppliers’ of data to select mental health providers, substance abuse providers, immediate and urgent care centers, and CCHHS’ correctional health services. Finalization of these providers will be done jointly by CountyCare and the successful proposer.

Page 5 of 12
ID Section of
the RFP Question CCHHS Response
29 4 Who is CountyCare's contracted TPA? What IT system is the TPA currently using?
Valence Health is CountyCare’s TPA (as of 4/1/2016). Their proprietary IT systems are Vision, vCare and vQuest.
30 4 Our understanding is that the scope of the project is restricted to the 170,000 CountyCare members. Please confirm. Will the scope of real-time data from provider systems be limited to CountyCare members, or potentially include the full panel of patients for the provider?
The scope of the project is limited to CountyCare’s current membership. Real-time data from identified acute care and other provider types to the portal will be for assigned CountyCare members only.
31 4 Please provide the list of vendors who will perform care management and/or linkage services for CountyCare members and will need to have access to the proposed solution.
CountyCare has three delegated care management vendors (CCHHS, MHN ACO and La Rabida Care Coordination) and one contracted linkage services provider (TASC, Inc.).
32 4 Does CountyCare have an inventory of EHRs (acute and ambulatory) currently installed at its provider network? Are these EHRs ONC 2014 certified, and do they meet interoperability requirements for CCDA exchange?
Only acute care hospital EHRs are feeding the portal and are doing so through HL7 messaging. Full CCDA exchange is out of scope for this RFP. Proposers, however, may include this functionality as a value-added service to their proposal.
33
4 Has CountyCare developed a set of rules to apply to real-time data feeds to generate alerts?
Yes.
34 4 What is the expectation regarding integration of alerts with EHRs used by providers? Is the intent to use secure messaging, CCD exchange, or even API-level integration with EHRs?
Integration of ADT alerts into EHRs used by CountyCare providers is out of scope. Proposers, however, may include this functionality as a value-added service to their proposal.
35 4 Are data feeds from commercial laboratories and imaging centers expected to be included in real-time feeds?
Integration of data feeds from commercial laboratories and imaging centers is out of scope. It is expected that these data will be available through the claims data provided by CCHHS. Proposers, however, may include this functionality as a value-added service to their proposal.
36 5.1.10 The RFP mentions about interfaces to systems listed in the Current State (Technology). What are these external systems that we need to interface with?
See question #3 above.
37 6.15 The RFP mentions That "The Pricing Format is attached to this PDF file." We could not locate the pricing format with the RFP document. Please provide the pricing format.
A copy of the pricing format is included with this addendum.

Page 6 of 12
ID Section of
the RFP Question CCHHS Response
38 1 Is the CountyCare contracted provider network (all CCHHS facilities, every FQHC and more than 30 hospitals) already fully integrated with the existing system?
See question #28 above.
39 4 Regarding the existing system, is the vision to integrate with it or replace it?
It is CCHHS’ desire to continue offering a connectivity solution beyond the term of the current agreement.
40 4 Does the existing system capture all admissions and discharges satisfactorily? How? Is it through a system to system mechanism, manual data entry at a web interface, or some combination?
Yes, the existing system is capturing all admissions and discharges satisfactorily through automated HL7 messaging with participating acute care hospitals.
41 4 If the vision is to integrate with the existing system, how would we get access to the data? Is it in an RDBMS that we can access? A REST API?
It is CCHHS’ desire to continue offering a connectivity solution beyond the term of the current agreement.
42 4 If the vision is to replace the existing system, how does it capture the data? What are the interfaces?
Data are captured by the online system through HL7 messaging by participating hospitals that are linked with eligibility and claims data files provided by CCHHS (or its designee).
43 4 If the vision is to replace the existing system, can we get copies of its full specification and/or access to it?
CCHHS will provide the necessary specification information for any selected proposer to be successful with the RFP requirements.
44
4 Can you provide details of the mental health providers, substance abuse providers, immediate and urgent care centers and CCHHS correctional health services that you want capture data from? Can you provide any details about their interface points?
The overarching goal of the online notification system is to improve the health outcomes and health care utilization of CountyCare members. CCHHS believes this can be enhanced by expanding the ‘supply’ of ADT data to the portal beyond the current acute care hospital settings. Prioritizing these providers will be done jointly with CountyCare leadership. The interface points would be expected to mirror those for the acute care setting.
45 4 What does "Integration of data feeds from CountyCare's contracted TPA" mean?
Specifically, this references receipt of membership eligibility (i.e. 834) and claims payment files (i.e. 837 or other agreed-up format) for integration into the notification system.
46 5.1.1 Can you provide a list of all systems that the solution is expected to interface with?
See #22 above
47 5.1.1a Can we assume that all users have existing clients (PCs, tablets, mobile devices, etc.) with required connectivity, that provision of clients is not a part of the bid?
Yes.

Page 7 of 12
ID Section of
the RFP Question CCHHS Response
48 5.1.8b Is there any requirement (or desire) to integrate with an existing IdP for some or all users?
We currently want to ensure all devices connected into our environment are current on Anti-Virus. All wireless devices must be registered via our helpdesk
49 5.1.8e Is the focus of this system administrators and developers provided by the proposer and its subs?
Yes.
50 5.1.9 Can the solution rely on customer provided VPN endpoints, such as an ASA or an SSH tunnel endpoint?
Yes.
51 5.1.10a Interfaces to what systems? Does this mean out of the box interfaces?
Out-of-the-box interfaces with HL7 messaging to link the participating providers to the proposed on-line system.
52 5.1.10i Is there a list of minimum interfaces that are desired or required?
CountyCare expects to retain, at minimum, the current levels of access to the system. This includes all primary care provider groups, and 11 hospitals (21 separate feeds).
53 5.3.1 From what system can we obtain member demographics, health history, health care utilization, CM assignment and CM? How do we link patients? Is there a standard key?
All member demographics and utilization data, including CM assignment, is provided by CCHHS. The standard key to link members is the State-issued Medicaid Recipient Identification Number (RIN).
54 5.3.1a Is there a list of organizations that the solution must collect data from? Is anything known about their interfaces?
See #2. All data are collected through HL7 exchange.
55 5.3.1c Is it envisioned that outreach personnel will manually enter updates/documentation into the system, not via a system to system interface?
This may occur in either format.
56 5.3.1e Is the permissions model well understood? Are roles identified along with corresponding permissions?
Permission models are primarily defined based on member PCP assignment, and/or CCHHS-designated access for contracted partners (e.g. care management entity). Data suppression for confidential information is expected to transcend permission models and follow universal protocols.
57 5.3.1g Can you provide a list of the required systems and interface specifications?
Interface specifications will be developed during contracting.
Care Management: Consensus, MHNConnect, Syntranet and any other system utilized by a future contracted CME.
TPA: ValenceHealth
EHRs: major electronic health record systems in our network include Epic, Centricity, Alliance Centricity, Cerner, NextGen, and Athena.
Page 8 of 12
ID Section of
the RFP Question CCHHS Response
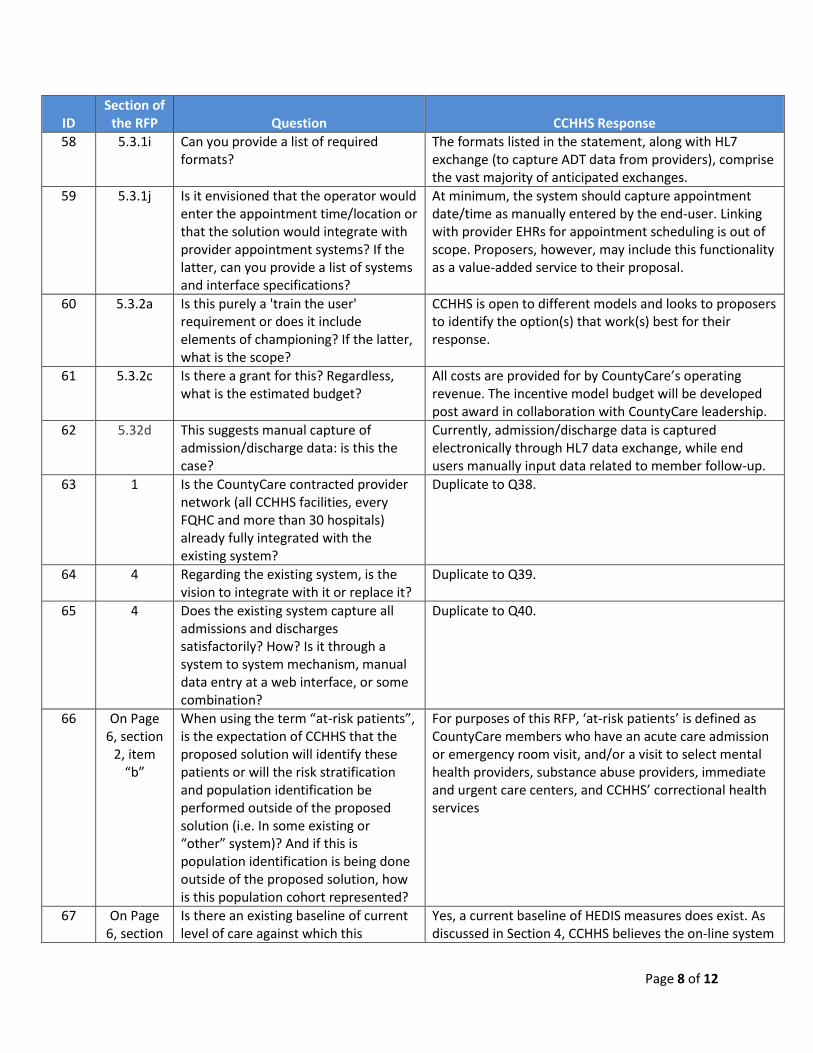
58 5.3.1i Can you provide a list of required formats?
The formats listed in the statement, along with HL7 exchange (to capture ADT data from providers), comprise the vast majority of anticipated exchanges.
59 5.3.1j Is it envisioned that the operator would enter the appointment time/location or that the solution would integrate with provider appointment systems? If the latter, can you provide a list of systems and interface specifications?
At minimum, the system should capture appointment date/time as manually entered by the end-user. Linking with provider EHRs for appointment scheduling is out of scope. Proposers, however, may include this functionality as a value-added service to their proposal.
60 5.3.2a Is this purely a 'train the user' requirement or does it include elements of championing? If the latter, what is the scope?
CCHHS is open to different models and looks to proposers to identify the option(s) that work(s) best for their response.
61 5.3.2c Is there a grant for this? Regardless, what is the estimated budget?
All costs are provided for by CountyCare’s operating revenue. The incentive model budget will be developed post award in collaboration with CountyCare leadership.
62 5.32d This suggests manual capture of admission/discharge data: is this the case?
Currently, admission/discharge data is captured electronically through HL7 data exchange, while end users manually input data related to member follow-up.
63 1 Is the CountyCare contracted provider network (all CCHHS facilities, every FQHC and more than 30 hospitals) already fully integrated with the existing system?
Duplicate to Q38.
64 4 Regarding the existing system, is the vision to integrate with it or replace it?
Duplicate to Q39.
65 4 Does the existing system capture all admissions and discharges satisfactorily? How? Is it through a system to system mechanism, manual data entry at a web interface, or some combination?
Duplicate to Q40.
66 On Page 6, section
2, item “b”
When using the term “at-risk patients”, is the expectation of CCHHS that the proposed solution will identify these patients or will the risk stratification and population identification be performed outside of the proposed solution (i.e. In some existing or “other” system)? And if this is population identification is being done outside of the proposed solution, how is this population cohort represented?
For purposes of this RFP, ‘at-risk patients’ is defined as CountyCare members who have an acute care admission or emergency room visit, and/or a visit to select mental health providers, substance abuse providers, immediate and urgent care centers, and CCHHS’ correctional health services
67 On Page 6, section
Is there an existing baseline of current level of care against which this
Yes, a current baseline of HEDIS measures does exist. As discussed in Section 4, CCHHS believes the on-line system

Page 9 of 12
ID Section of
the RFP Question CCHHS Response
2, item “e”
“improvement” will be measured, or is the baseline measurement expected by CCHHS to be part of the proposed solution? And what specific data point(s) will be being measured/monitored?
can improve health plan performance on HEDIS goals, namely timely follow-up from discharge and access to primary care.
68 Page 7, section 4
In describing the “Current & Future Scope of Work”, there is no indication of what the current system(s) actually is/are. What does the current application/data environment consist of, in terms of software, processes, connections, data/information sources etc.? And what sort of interoperability is expected between these existing solutions and the proposed solution?
Simply, the current system aggregates CountyCare member eligibility, historical claims data (medical and pharmacy), and inpatient and ED admission/discharge data (ADT) from participating acute care hospitals into an on-line tool that is used by providers of care to manage and improve member outcomes, namely timely follow-up from discharge and access to primary care. The interoperability is limited to membership, claims data and ADT exchange.
69 Page 7, section 4
How does CCHHS currently identify/validate patient identities across the multiple care settings (i.e. Is there any sort of County Enterprise Master Patient Identity (EMPI) solution currently deployed/maintained)?
Member identity is confirmed using the State-issued Medicaid Recipient Identification Number (RIN).
70 On Page 7, section
4
The described “current” state indicated that currently there are “connections” to the network of care settings, but does not indicate what the data form/format or nature of these information delivery pathways take. What types of data is being delivered (i.e. “X12 Post Adjudicated Claims”, “CCD”, “HL7v2.x messages”, “Fixed Format CSV file”, etc.)? And in what delivery methodology (i.e. “Nightly Batch File”, “Message traffic over secured TCP/IP connection”, “DIRECT secure protocol email”, etc.)?
Data from participating hospitals are delivered through a real-time HL7 ADT interface.
71
On Page 13,
section 5.3.1,
item “f”
Is the expectation of the proposed solution to include a secure bi-directional mobile application, or a read-only mobile application?
CCHHS expects proposed mobile solution(s) to include end-user data entry functionality appropriate to the system’s needs.
72 How is this proposed project being funded (i.e. Federal Grant, County funds, State funds, Self-funded from CCHHS operating budgets, etc.)?
All funds come from CountyCare’s operating revenue.

Page 10 of 12
ID Section of
the RFP Question CCHHS Response
73 Respectfully requesting a 2 week extension on RFP# H16-0015 proposal submission due date
No extensions to the RFP will be provided.
74 Who is currently the incumbent? Medical Home Network (MHN)
75 Will there be consideration for a well-funded start up with revolutionary, disruptive technology?
Proposers must meet the eligibility criteria as listed in Section 8.1 (verified in section 6.5[a]).
76 Can we have vendor conference? No vendor conference will be held for this RFP.
77 Can we extend the date?...the RFP was posted on May 9th and closes June 3rd...which is less than a month
No extensions to the RFP will be provided.

Page 11 of 12
#7: Please provide a high-level system architecture diagram.

Page 12 of 12
ADDENDUM ACKNOWLEDGEMENT FORM
As required by the RFP, Proposers must submit this acknowledgement form with their response. One acknowledgement form per response, listing all addenda, is appropriate. Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Company Name: _____________________________________________________________ Representative’s Name: ____________________________________________________________ Signature: ______________________________________________________________ Date: ______________________________________________________________
END OF ADDENDUM