addressing obesity in the workplace | state of the evidence
TRANSCRIPT
Addressing Obesity in the WorkplaceState of the Evidence
George Washington University and ICF International Forum on Obesity Prevention in Worksites
January 21, 2015
Nico Pronk, Ph.D.HealthPartners and
HealthPartners Institute for Education and ResearchMinneapolis, Minnesota
Harvard UniversityBoston, Massachusetts
#GWICF2015

Prevalence
• Obesity has become highly prevalent
– More than 2.1 billion people—almost 30% of the global population—are overweight or obese
– Approximately 30% of the US workforce is obese
– Obesity has roughly doubled among US workers over the past 30 years
– Severe obesity is rising faster than other classes
Source: Pronk NP. Ann Rev Public Health, 2015 (in press)
Fig. Obesity prevalence of the US workforce, based on data from nationally representative samples
0%
100%
200%
300%
400%
500%
600%
700%
800%
900%
1000%
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
Perc
en
tag
e I
ncre
ase (
Baseli
ne 1
986)
bmi>30
bmi>35
bmi>40
bmi>45
bmi>50
#GWICF2015

Complexity
• The workplace is a complex social system
• Obesity is highly complex
• Single solutions are unlikely to generate success
• Multiple stakeholders working together is needed
• Aligning incentives and building cooperation is key
#GWICF2015

Costs
• Durden, et al (2008), estimates that the incremental combined direct medical and indirect costs for overweight, obese, and severely obese employees are:
– Overweight $1,550.92
– Obese $2,223.58
– Severely obese $3,391.52
• Finkelstein, et al (2010) found an annual attributable cost of obesity among full-time employees of $73.1 billion (based on 2006 Med Expend Panel Study and 2008 Nat’l Health and Welln Survey)
#GWICF2015
0
2
4
6
8
10
12
14
16
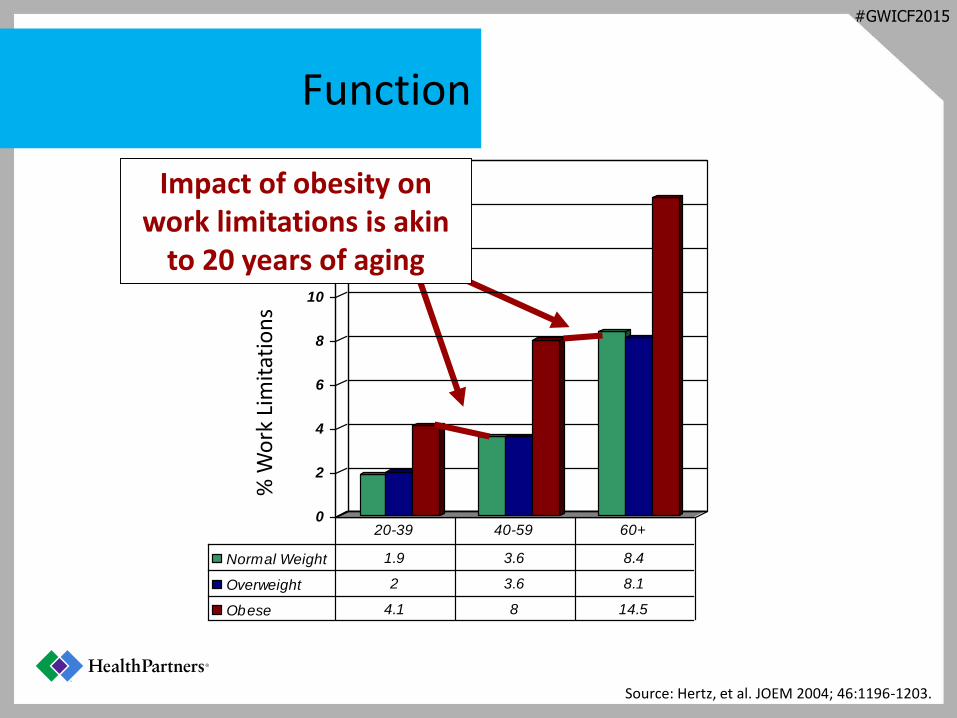
Normal Weight 1.9 3.6 8.4
Overweight 2 3.6 8.1
Obese 4.1 8 14.5
20-39 40-59 60+
Source: Hertz, et al. JOEM 2004; 46:1196-1203.
Impact of obesity on work limitations is akin
to 20 years of aging%
Wo
rk L
imit
atio
ns
Function
#GWICF2015
0
0.5
1
1.5
2
2.5
Increase in Number
of Chronic
Conditions
Decline in HRQOL
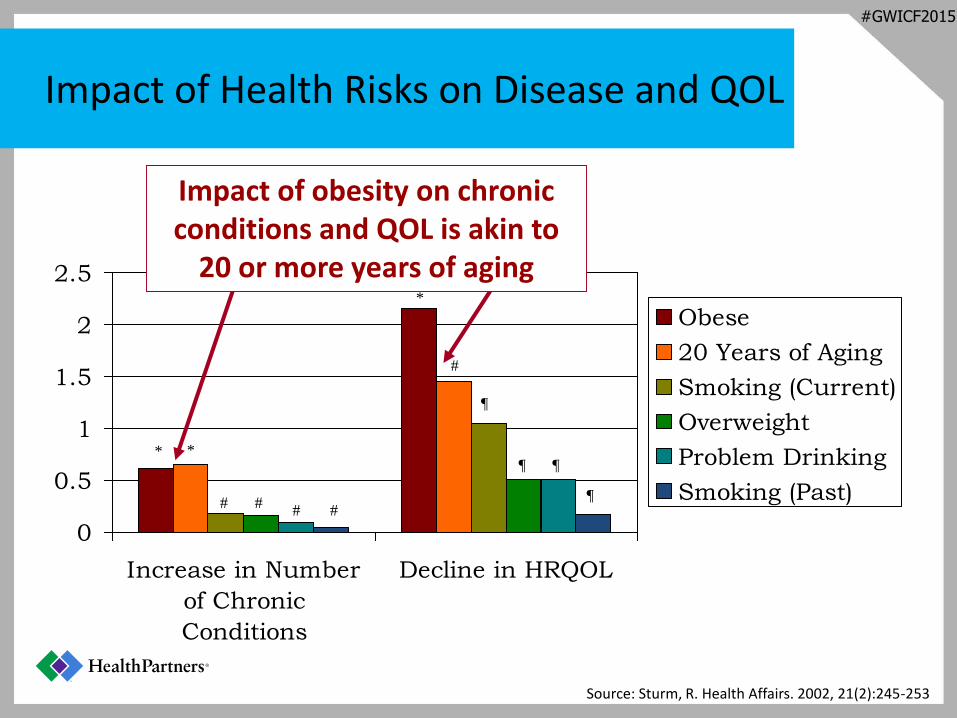
Obese
20 Years of Aging
Smoking (Current)
Overweight
Problem Drinking
Smoking (Past)
* *
*
# ## #
#
¶
¶ ¶
¶
Source: Sturm, R. Health Affairs. 2002, 21(2):245-253
Impact of obesity on chronic conditions and QOL is akin to
20 or more years of aging
Impact of Health Risks on Disease and QOL
#GWICF2015

-20
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
2
1 2 3 4 5 6
Weig
ht
Lo
ss (
kg
)
Exercise Alone
Diet + Exercise
Diet Alone
M eal Replacements
VLCD
Orlistat
Sibutramine
Advice Alone
6-mo 12-mo 24-mo 36-mo 48-mo
Source: Franz, et al. J Am Diet Assoc 2007;107:1755-1767.
Systematic Review of Weight Loss StudiesAverage Weight Loss of Subjects Completing a Minimum 1-Yr Weight Management Intervention80 Studies, 24, 698 Subjects, 16,823 Completers (68%)
#GWICF2015
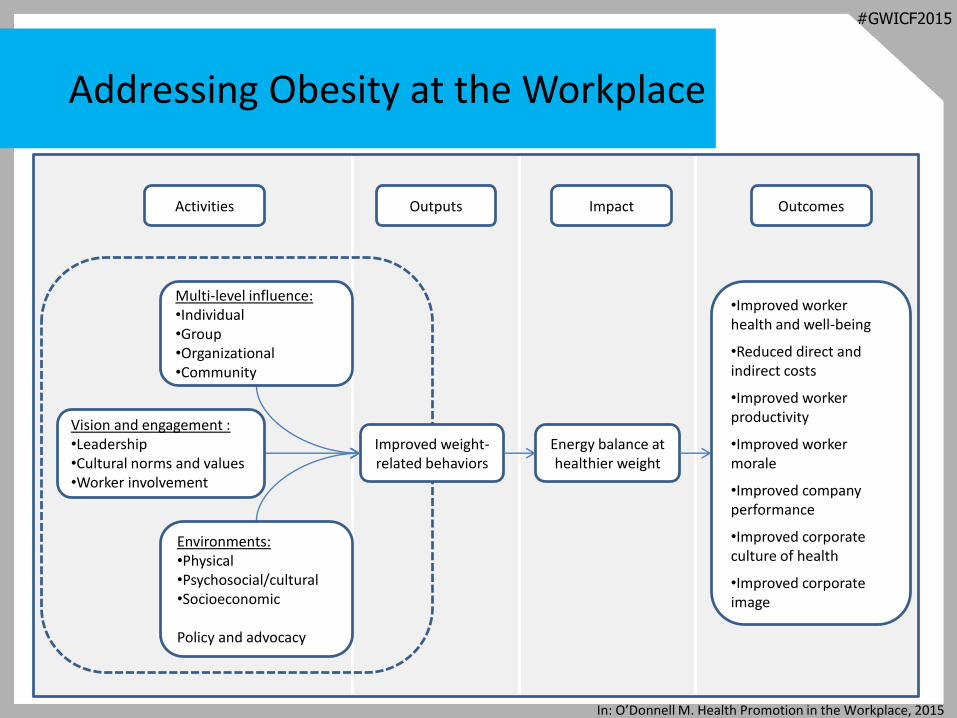
Addressing Obesity at the Workplace
In: O’Donnell M. Health Promotion in the Workplace, 2015
Improved weight-related behaviors
Energy balance at healthier weight
Environments:•Physical •Psychosocial/cultural•Socioeconomic
Policy and advocacy
Multi-level influence:•Individual•Group•Organizational•Community
Vision and engagement :•Leadership •Cultural norms and values•Worker involvement
•Improved worker health and well-being
•Reduced direct and indirect costs
•Improved worker productivity
•Improved worker morale
•Improved company performance
•Improved corporate culture of health
•Improved corporate image
Activities Outputs Impact Outcomes
#GWICF2015

Healthy Workplace, Healthy Community
e.g., meeting minimal regulatory standards for worker safety
e.g., corporate giving campaigns that enhance company brand, image
Compliance Charitable Strategic Systemic
e.g., core business and management systems deployed to generate health and business value
e.g., systemic solutions designed to intentionally generate population health, business value, and address social determinants of health
Schematic of the business case development continuum for employer engagement in community health
Source: Pronk, et al. In review
#GWICF2015

Conclusions
• Obesity prevalence is high, increasing, and very costly
• No single solutions will generate sufficient impact—only comprehensive, multi-level, multi-stakeholder solutions will work
• Don’t prioritize some programs over others—do as many as possible
• No single stakeholders owns the problem—partnerships are required
• Connections between employers and community are needed to create scalable, sustainable solutions to obesity
#GWICF2015

e.g., meeting minimal regulatory standards for worker safety
e.g., corporate giving campaigns that enhance company brand, image
Compliance Charitable Strategic Systemic
e.g., core business and management systems deployed to generate health and business value
e.g., systemic solutions designed to intentionally generate population health, business value, and address social determinants of health
-20
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
2
1 2 3 4 5 6
Weig
ht
Lo
ss (
kg
)
Exercise Alone
Diet + Exercise
Diet Alone
M eal Replacements
VLCD
Orlistat
Sibutramine
Advice Alone
6-mo 12-mo 24-mo 36-mo 48-mo
Thank You
Contact Information:
0%
100%
200%
300%
400%
500%
600%
700%
800%
900%
1000%
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
Perc
en
tag
e I
ncre
ase (
Baseli
ne 1
986)
bmi>30
bmi>35
bmi>40
bmi>45
bmi>50
#GWICF2015

To watch Dr. Nico Pronk’s presentation online, visit: www.icfi.com/ObesityPrevention-NicoPronk
#GWICF2015