adenomatous goiter - university of oregon · adenomatous goiter j. earl else, m.d. ... a study of a...
TRANSCRIPT

ADENOMATOSIS, OR THE DIFFUSEADENOMATOUS GOITER *
J. EARL ELSE, M.D.Assistant Professor and Chairman, Executive Committee, Department of
Surgery, University of Oregon Medical School
PORTLAND, ORE,
Under the term adenoma, there is described in theliterature two definite distinct pathologic entities, adeno-matosis, or the diffuse adenomatous goiter, and trueadenoma, which is a definite encapsulated growthbeginning from a single point and answering all therequirements of the benign tumors.
Adenomatosis of the thyroid is characterized by adiffuse new formation of acini usually involving theentire thyroid gland, beginning with the fetal type with-out secretion, but later assuming the adult or colloidtype, and giving rise to no symptoms at first, but laterto those of pure hyperthyroidism.
Wilson, in 1913, briefly described this condition andapplied the term adenomatosis. Goetsch, in 1920 and1921, described the early stage under the term diffuseadenomatosis, but he referred to the new formationof acini as "an abortive attempt at the formation ofyoung small alveoli." Plummer, in his writings, hasgrouped adenomatosis with the adenomas, treating themas a single entity. In addition to these references, Ihave referred to this condition in several communica-tions, but up to the present there has been no descrip-tion of the disease tracing it through its entire course.
PATHOLOGY
The pathlogic picture varies with the stage of thedisease.
Early Adenomatosis.—The thyroid gland is moder-ately enlarged, the surface is smooth, and the consis-tency is somewhat increased over the normal. On
*Freon the goiter clinic of the University of Oregon Medical Schooland the pathologic laboratory of Good Samaritan Hospital.
* Read before the Section on Surgery, General and Abdominal, atthe Seventy-Sixth Annual Session of the American Medical Association,Atlantic City, N. J., May, 1925.

2
section, the cut surface presents a more dense appeaiiance than in the normal gland ; and, while some coNiAis present, there is not the same semitranslue'eiiiappearance characteristic of the normal thyroid. j
is the early stage the gland s homogeneous, and nowhereis there to be seen any tendency toward nodular for-mation. On microscopic examination (Fig. 1), it isfound to contain both fetal acini and apparently normalor colloid acini. Between these two types of acini arefound all possible variations, the appearance beingindistinguishable from that of the mixed adenoma. Inother fields there may be an apparent increase in theinterstitial cells. In some areas these cells are arrangedin masses, many of them showing the definite beginningof acinus formation. It was these areas that Goetschreferred to as being abortive attempts at the formationof young small alveoli. A study of a series of cases,however, demonstrates that this is not an abortiveattempt, but is instead the real beginning of the newacini.
Late Adenoniatosis.—The gland shows a markedenlargement. The surface is more or less lobulated,often with very definite nodules projecting. On cutsection (Fig. 2), the nodular arrangement is still moremanifest. On close observation, these nodular massesare seen to be made up of groups of acini distendedwith colloid. Many of these masses have a thin, mem-branous capsule and can be enucleated, presenting anappearance not unlike that of an adenoma, but differingfrom an adenoma in that the capsule is only a thinmembrane instead of the well developed capsule of theadenoma (Fig. 3). Between these nodules is foundcompressed thyroid tissue. In some places degenera-tion has taken place, while in other areas there may bemarked connective tissue proliferation, marking thesite of a former degenerative process or a hemorrhage.Sometimes cystic formation is present, while hemor-rhagic areas, either into some of the nodules giving asharply circumscribed hemorrhagic mass, or infiltratingbetween the nodules, may be found. On microscopicexamination of the colloid nodules, the picture is verysimilar to that seen in a colloid adenoma. Sections madefrom the tissue between the nodules often show the sametype of structure, differing only in the amount of col-loid present in the acini. Solitary lymph follicles maybe found.

3
The blood supply in adenomatosis is increased, andin many cases there is a very definite increase in thecollateral circulation.
PATHOGENESIS
It is impossible to trace any one given thyroid glandthrough its course from the beginning new formationof Acini to the development of colloid adenomatosis, butby studying a series of cases, the method of develop-ment can be fairly well ascertained. The very firstevidence of the beginning of an adenomatosis is the
Fig. 1.—Early adenomatosis: thyroid only slightly enlarged, with nonodules; diffuse new formation of acini; fetal and adult acini presentthroughout thyroid.
formation of undifferentiated cells in masses (Fig. 4).These cells are probably identical with those describedby WOlfler as interstitial cells. They do not differfrom the appearance of the cells seen in the beginningof the development of new acini within old acini, asseen in compensatory hyperplasia (Fig. 5). Just asin well developed compensatory hyperplasia one seesin the center the undifferentiated cells, external to thisthe fetal acini, and next to the wall of the parent acinithe colloid acini, so in adenomatosis (Fig. 6) one findsfirst a group of the undifferentiated cells, then thenewly formed acini of the fetal type, and then the acinithat are taking on the power of secreting colloid. From
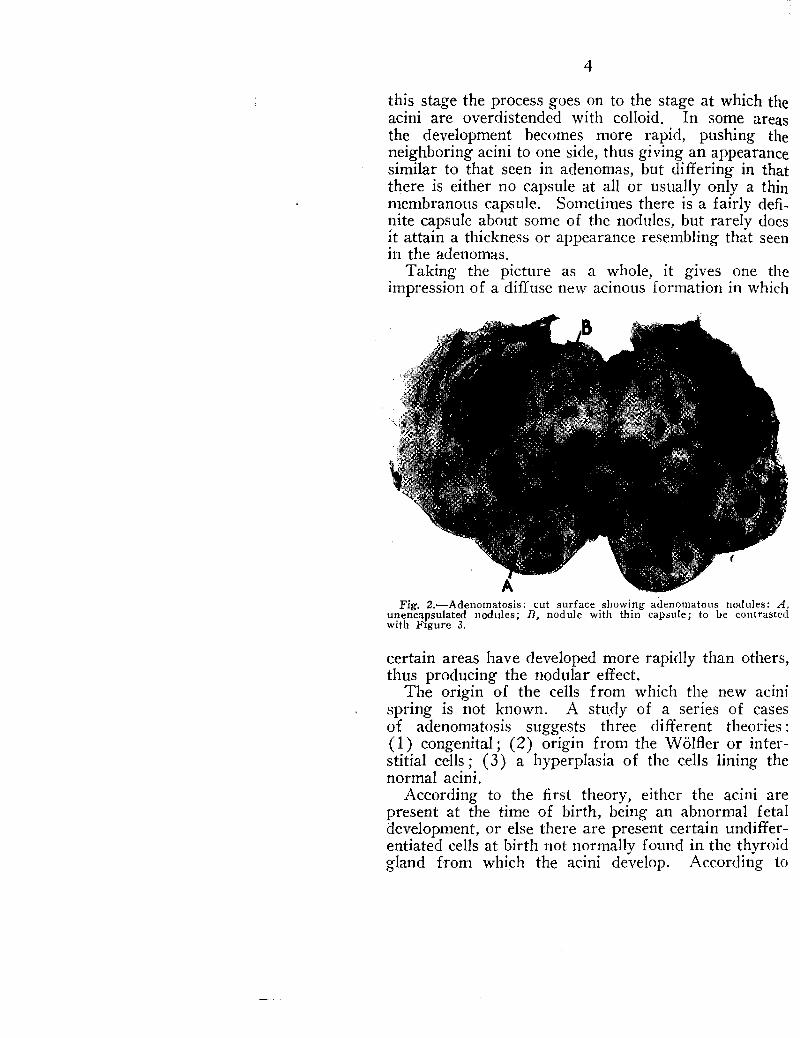
AFig. 2.—Adenotnatosis: cut surface showing adenoinatous nodules: A,
unencapsulated nodules; B, nodule with thin capsule; to be contrastedwith Figure 3.
4
this stage the process goes on to the stage at which theacini are overdistended with colloid. In some areasthe development becomes more rapid, pushing theneighboring acini to one side, thus giving an appearancesimilar to that seen in adenomas, but differing in thatthere is either no capsule at all or usually only a thinmembranous capsule. Sometimes there is a fairly defi-nite capsule about some of the nodules, but rarely doesit attain a thickness or appearance resembling that seenin the adenomas.
Taking the picture as a whole, it gives one theimpression of a diffuse new acinous formation in which
certain areas have developed more rapidly than others,thus producing the nodular effect.
The origin of the cells from which the new acinispring is not known. A study of a series of casesof adenomatosis suggests three different theories :(1) congenital; (2) origin from the WOlfler or inter-stitial cells ; (3) a hyperplasia of the cells lining thenormal acini.
According to the first theory, either the acini arepresent at the time of birth, being an abnormal fetaldevelopment, or else there are present certain undiffer-entiated cells at birth not normally found in the thyroidgland from which the acini develop. According to

5
the second theory, the new acini form from the inter-stitial cells of WOlfler, which are normally found inthe thyroid gland. The function of these cells is notdefinitely known, but it may be that they are for thepurpose of regeneration in thyroids that have beenpartially destroyed or removed, or in thyroids secretingan ,insufficient amount of thyroxin. In other organs,the regenerative ability is usually present. In the liver,for example, where there has been a slow destructionof the liver lobules, as in cirrhosis, there is often a newdevelopment of liver substance in adenomatous-likemasses sufficient to carry on the liver function so long
Fig. 3.—Multiple adenomas: three adenomas in one lobe; definitelyencapsulated. Difference from Figure 2 may be noted.
as the blood supply is not interfered with. This newformation in the liver probably develops from the bileradicles. The thyroid gland, not having ducts throughwhich the secretion may be discharged and from whichregeneration may take place, may have instead theso-called interstitial cells for this purpose, and fromthese, according to this theory, may come a diffuseatypical acinous formation.
The third theory is that a new formation of acinisimilar to that seen in compensatory hyperplasia maydevelop from the cells lining the old acini, but outsidethe walls of these acini instead of inside, as incompensatory hyperplasia.
It would appear from the glands studied that thetheory that these new acini develop from the inter-
r-ie
re
tal
tc

6
stitial cells was more tenable than any other theoryhowever, without the opportunity of studying a largonumber of thyroid glands of children or of the age o:adolescence, one cannot be certain that there may not b(some which show the characteristic findings of adeno-matosis from birth. Accepting the theory of th(development from the interstitial cells as being correct,the source of the interstitial cells is the next problem
Fig. 4.—Adenomatosis, showing transition from undifferentiated cellsto fetal acini.
in pathogenesis. These may be congenital, put therefor the purpose of regeneration, as stated, or it maybe that they spring from the epithelial cells of the acini,
ETIOLOGY
Three theories of causation are apparent : (1) thatit is congenital; (2) that it develops from uncuredadolescent goiter ; (3) that it is developed as the resultof a stimulus from the mild hypothyroidism due toiodin deficiency in the food and drink intake.

7
1. The congenital theory has already been discussedunder pathogenesis.
2. The patients having adenomatosis that I have seenmay he divided into three groups so far as a historyof adolescent goiter is concerned. The first group, byfar the largest, gives a history of having had an adoles-colt:goiter. The second group is uncertain whether agoiter was present or not during the adolescent period,and the third group, which is the smallest, is certain
Fig. 5.—Compensatory hyperplasia, showing manner of the developmentof new acini within old acini: A, undifferentiated cells; 13, fetal acini;C, intermediate "cells; D, adult acini.
that there was not a goiter ; but many if not all ofthese patients may be mistaken. The adolescent goiterprobably leaves the thyroid in a somewhat atypical statewith a reduced reserve, so that when increased demandis thrown on the thyroid gland in later life the changescharacteristic of adenomatosis take place. Patientswith other forms of goiter in adult life gave the samehistory regarding adolescent goiter ; hence, it appearsprobable that an uncured adolescent goiter may pre-dispose to the development of all types of adult goiter.

8
3. It is known that mild hypothyroidism due to adeficient iodin intake may result in : (1) an over-secretion of colloid, for the thyroid in its attempt tosecrete more thyroxin may secrete too much colloid;(2) a hyperplasia of the cells within the acini, as seenin hyperplastic adolescent goiters, in which the hyper-plasia may be either diffuse or localized and in the lattercase often mistaken for adenomas, and (3) the newformation of acini, as seen in compensatory hyper-plasia. To summarize our knowledge of the etiology,
Fig. 6.—Adenomatosis; A, undifferentiated cells; B, beginning fetalacinus formation; C, intermediate acini; D, adult acini.
it would seem that a simple nontoxic goiter, as the goiterof childhood, the adolescent goiter, or the colloidgoiter of adult life, but more especially the adolescentgoiter, predispose to the development of adenomatosis,and that an iodin deficiency in the food intake is animportant factor.
SYMPTOMATOLOGY
Early in the development of this disease, the onlyevidence of the presence of an adenomatosis is a slight

9
enlargement of the thyroid gland. It is probable thatconsiderable time elapses between the beginning of theadenomatosis and the beginning of the symptoms inthose that become toxic, the same as occurs in trueadenomas. The onset of the symptoms is insidious,so that the patient does not come seeking treatmentuntil the symptomatology has become fairly definite.At this time the most frequent complaints are tiringeasily, nervousness, shortness of breath, tachycardiaand palpitation. The appetite is usually very good,while the weight is variable, some patients losing andothers having no change. There is never a history ofacute symptoms as seen in exophthalmic goiter. Themost common clinical findings are tachycardia, tremor,moderate rise in the basal metabolic rate, moist skinand palms. The size, shape and consistency of thethyroid vary with the stage of the disease.
Early the gland is only moderately enlarged andsmooth ; later it may be markedly enlarged and nodular.The largest goiters that we have seen belonged to thistype. Increase in the systolic pressure occurs, followedgradually by an increase in the diastolic. The bloodpressure of adenomatosis, like that in toxic adenomasand compensatory hyperplasia, differs from that inexophthalmic goiter in that the diastolic pressure isusually not lowered or, if lowered, is lowered butslightly, while the systolic pressure rises, thus givingan increase in the pulse pressure characteristic of toxicgoiter. With the development of tachycardia andhypertension, cardiac hypertrophy takes place.
DIAGNOSIS
The diagnosis of hyperthyroidism is made on thehistory of tachycardia and palpitation, increased ner-vousness, tiring easily, increased sweating, increasedpulse pressure accompanying a tachycardia, and anincrease of the basal metabolic rate. The differentialdiagnosis between adenomatosis and toxic hyperplastic(exophthalmic) goiter is made, first, on the historyand, secondly on the clinical symptoms. In adenoma-tosis there is usually a history of a goiter having existedfor a considerable time. The onset of the symptomsis insidious. The most common complaints are tachy-cardia, palpitation, tiring easily and getting out ofbreath easily. There is a good appetite and usuallylittle disturbance with the weight, unless the patient is
1111111111C4 V V 21.1 • A. AO Gil ,

10
seen late in the disease. On physical examination, thegoiter is found to be small and smooth and fairly firmearly in the disease, and large, soft and lobulated latein the disease. There is an increase in pulse pressureresulting from a rise in the systolic pressure as a latesign. The diastolic pressure rises late in the diseasebut does not keep pace with the rise of the systolicpressure. Tremor is present. There is no exophthal-mos, lagging of the upper lids, or hyperthyroid crisis.The basal metabolic rate is moderately increased, beingfound usually between a plus 30 and a plus 50.
In the toxic hyperplastic goiter (exophthalmic) asseen in the first attack, there is a definite tachycardiawith fibrillation in the extreme cases, well markedtremor, evidence of a loss of weight, and lagging ofthe upper lids, with exophthalmos in the majority ofpatients. The skin is always moist, and the palms aresweaty. The patients give a history of being warmwithout a rise in temperature. Many of them wantthe living room cooler than other members of thefamily, and fewer covers at night. In a well markedattack, the basal metabolic rate is fairly high, usually50 or more. The patients are usually nervous, andmany of them talk rapidly. In secondary attacks, thefindings are not so definite. There is an increase inthe pulse pressure, resulting from a lowering of thediastolic, rather than to a raising of the systolic pres-sure. The systolic pressure may be normal, belownormal or occasionally above normal. The diastolicpressure is rarely above normal.
A differential diagnosis between adenomatosis andtoxic adenoma must be made by palpitation of thethyroid, as the clinical manifestations are the same.In the adenomas, there is one or at most two or threedefinitely isolated nodules. In adenomatosis, at firstthe gland shows only a diffuse enlargement withoutany nodular formations. Later the gland presents alobulated sensation to the examining fingers insteadof the definite isolated nodules of adenomas. In someinstances in which there has been a rapid developmentin some areas there may be fairly definite nodules, butthese are always accompanied by a more or lesslobulated gland.
PROG NOSI S
The prognosis varies with the intensity of the diseaseand the length of time elapsing after the toxic symp-

11
toms develop. The prognosis of cure with propertreatment so far as the hyperthyroidism is concernedis usually good. Early in the disease a good prognosisfor the relief of symptoms may be given, but afterdefinite cardiac hypertrophy has developed, after defi-nite hypertension has been established, and after thepatient has become distinctly nervous, the prognosis,so far as relief from symptoms is concerned, becomesless favorable.
In the cases showing a marked hypertension, thereis practically always a reduction in the blood pressurefollowing operation, but it usually does not go entirelyback to normal. A damaged heart muscle remains adamaged heart muscle. A badly disordered nervoussystem resulting from a prolonged or a pronouncedhyperthyroidism may not become entirely normal again.To give a good prognosis, the proper treatment mustbe instituted early.
TREATMENT
A cure can be obtained in only one way ; that is, earlyadequate removal of thyroid substance. Like allpatients with hyperthyroidism, each patient must becarefully studied in order to determine the treatmentfor that individual. Patients seen fairly early willstand the radical operation well. It has been our expe-rience that because of the increased collateral circula-tion, ligation of the superior thyroid poles is of littlevalue. Patients in whom the condition is moderatelysevere are put in bed, for a few days previous tooperation with an ice collar about the neck, sufficientsedatives, barbital or morphin, to keep ithem quiet, anddigalen, 10 minims (0.6 c.c.) intravenously or intra-muscularly every four hours if the pulse is over 120.In the severe cases we use the roentgen ray rather thansuperior pole ligation to decrease the activity of thethyroid in order to make the patient a safe risk. Onthe night before the operation, the patients are alwaysgiven barbital or morphin. There is no preoperativepreparation. The patient's rest is not disturbed, evenby giving an enema on the morning of operation.If the patient is found excessively apprehensive ornervous, the operation is postponed.
The operation must be a subtotal double lobectomy.We leave only the posterior capsule and a thin layerof thyroid gland adherent to it. If more is left there
ianu, tire., mar. irs, iuzu.

12
is danger of recurrence. It is possible with this typeof operation that there may be an occasional patientwho will show the evidence of hypothyroidism for ashort time, but we have never seen such a case. Witha careful study of each individual case and with theproper preliminary preparation of the patient, thereshould be only a very slight mortality.
CONCLUSIONS
1. Adenomatosis is a definite pathologic entity dif-fering from adenoma in that the process is diffuse anddoes not have a true capsule.
2. Adenomatosis produces a hyperthyroidism of thecardiovascular type.
3. It is important to differentiate between adenomaand adenomatosis because the former requires simpleenucleation of the tumor growth, while the latterrequires subtotal double lobectomy.
709 Stevens Building.
Reprinted from The Journal of the American Medical AssociationDecember 12, 1925, Vol. 85, pp. 1878-1882
Copyright, 1925American Medical Association, 535 N. Dearborn St., Chicago