adhd, tics and tourette’s disorder - media-ns.mghcpd.org...
TRANSCRIPT

www.mghcme.org
ADHD, Tics and Tourette’s DisorderChild and Adolescent Psychopharmacology
March 4, 2018Barbara J. Coffey, MD, MS
Division Chief, Child and Adolescent Psychiatry
Professor, Department of Psychiatry and Behavioral Sciences
University of Miami Miller School of Medicine
www.mghcme.org
ADHD, Tics and Tourette’s Disorder:Learning Objectives
• At the end of this session, the participant should be able to:– Review evidence for the bidirectional overlap of
ADHD and tic disorders– Describe a systematic approach to disentangling
ADHD and tic disorder symptoms to prioritize target symptoms for treatment
– Interpret relevance of recent research findings for application to treatment of youth and adults with ADHD and tics
– Select approved and off label treatments for comorbid ADHD and tic disorders

www.mghcme.org

www.mghcme.org
Epidemiology: Bi-Directional Overlap of ADHD and Tic Disorders
• Rates of tic disorders are higher (10-30%) in children with
Attention Deficit Hyperactivity Disorder (ADHD) than in
children without ADHD (1-10%). (Spencer T., Biederman, J. Coffey, B. et al.,
Arch Gen Psych; 1999, 56: 842-84)
• ADHD is the most highly prevalent (50-75%) comorbid
disorder in clinically referred children with Tourette’s
Disorder (TD). (Coffey, B. Biederman, J. et al. J Nerv Ment Dis; 2000;188:583-588; Freeman,
TS International Data base Consortium; Eur Child Adolesc Psych 2007; 16 [suppl; 1];1/15-1/23)
• In a recent large community sample, by parent report,
more than 60% of children diagnosed with TD had also
been diagnosed with ADHD. (National Survey of Children’s Health Study, US, 2007)

www.mghcme.org
Gilles de la Tourette Syndrome Robertson et al. (2017)

www.mghcme.org
A National Profile of Tourette Syndrome, 2011-2012(Bitsko, R. et al. (2015) Journal of Behavioral Pediatrics; 35 (5);
317-322)
Method: Data on 65, 540 US children age 6-17 years from the 2011-2012 National Survey of Children’s Health.
Parents reported whether they had ever been told by a clinician that their child had Tourette Syndrome or another neurobehavioral health condition.
Results: 0.19% of US children had current TS; average age of diagnosis was 8.1 years. 0.28% were ever diagnosed with TS.
Compared to those without TS, children with TS were more likely to have co-occurring neurobehavioral health conditions.
Conclusion: TS is characterized by frequent co-occurring neurobehavioral health conditions.

www.mghcme.org
Prevalence of Lifetime Diagnosis: Tourette Syndrome
(Scahill, L. et al; Morbidity and Mortality Weekly Report CDC; 2009)
(National Survey of Children's Health, United States, 2007)
•† Selected Diagnoses age 6-17: Among children ever diagnosed with TS, 79% also had been diagnosed with at least one other selected diagnosis.

www.mghcme.org
TD and ADHD: Neurobiology(Seidman, L. et al; Biol Psychiatry; 2005; 57; 1263-1272; Sukhodolsky, D. et al; Eur Child Adolesc Psychiatry 2007; Leckman, J.
et al; JCAP, 2010; 20 (4); 237-247; Dickstein, S. et al; J Child Psych; 2006: 47: 10. 1051-1062)
• Inhibition is a core deficit in both disorders
• Executive functions abnormalities in both are thoughtto result from fronto-striatal and frontal-parietalnetwork dysfunction
• TD+ADHD: CTSC misguided neural oscillations mayresult in basal ganglia disinhibition, worsened by frontalhypoactivity in ADHD.
• Both TD and ADHD tend to improve with time, whichmay be a result of increased myelinization of prefrontalregions.

www.mghcme.org
Tourette Syndrome and Comorbid ADHD: Causes and Consequences. Eur J Pediatr. Malhany, N. Gulisano, M. et al 2014.

www.mghcme.org
Pre- and Perinatal Complications in Relation to Tourette Syndrome and Co-Occurring OCD and ADHD
(Abdulkadir, M. et al. Journ Psych Res 82 (2016); 126-135)
Aim: To investigate role of pre- and perinatal complications in TS, andcomorbid OCD and ADHD clinical phenomenology
Method: N=1113 participants in TIC Genetics study. 586 had chronic ticdisorder (CTD) and 527 were unaffected family controls.
Results: Prenatal complications i.e. premature birth (OR 1. 72) andmorning sickness requiring medical attention (OR 2.57) were associatedwith CTD. Total number of pre- and perinatal complications was associatedwith CTD.
Delivery complications were only related to OCD (OR 1.49).
Neonatal complications were related to presence (OR 1.46) and severity(b=2.27) of co-occurring OCD and ADHD severity (b=1.09)
Conclusion: Early exposure to adversity during pregnancy is related to CTD.Exposure at a later stage, at birth or in the neonatal period, is associated
with co-occurring OCD and ADHD.

www.mghcme.org
Tourette Syndrome and Comorbid ADHD: Causes and Consequences. Eur J Pediatr Malhany, N. Gulisano, M. et al 2014.

www.mghcme.org
Comorbidity in Clinical Samples:Clinical and Demographic Characteristics of Non-
specialized and Specialized Clinic Patients with TD
Non-specialized Clinic patients
(N=92)
Specialized Clinic patients
(N=103)
Overall Significance
Mean SD Mean SD p
Current Age 10.8 3.23 10.8 3.62 0.89
SES 2.0 1.13 2.2 1.24 0.42
N % N % p
Past GAS 47.9 7.50 48.6 7.57 0.54
Current GAS 51.3 7.32 51.9 6.52 0.55
% Male 82 90 81 80 0.06
Informativeness of Structured Diagnostic Interviews in the Identification of Tourette’s Disorder in Referred Youth(Coffey B, Biederman J, Spencer T et al. J Nerv Ment Dis. 2000;Sep;188 (9):583-588)

www.mghcme.org
Disruptive Behavior Disorders
Non-specialized Clinic Patients
Specialized Clinic Patients
Overall
Significance
(N = 92) (N = 103)
Diagnosis N % N % p
ADHD 76 84 74 72 .053
Conduct Disorder 18 20 14 14 .25
Oppositional Defiant Disorder
63 69 58 57 .91
Any Disruptive Disorder 83 91 86 84 .14
Informativeness of Structured Diagnostic Interviews in the Identification of Tourette’s Disorder in Referred Youth (Coffey B, Biederman J, Spencer T et al. J Nerv Ment Dis. 2000;Sep;188 (9):583-588)

www.mghcme.org
Phenotype Development in Adolescents with Tourette Syndrome: A Large Clinical Longitudinal Study
(Groth, C. Mol Debes, N. et al ; Journal of Child Neurol; 2017; 32 (3) 1047-1057)
Aim: Description of development of phenotypes in TS and tic-relatedimpairment in a large longitudinal study of 226 children and adolescentsfollowed up after 6 years.
Methods: Participants examined for tic severity, impairment, OCD andADHD.
Results: Phenotype development changed toward less comorbidity:
40% had TS only (no OCD or ADHD) at baseline and 55% at follow up.
Tic related impairment scores did not reflect tic decline.Sex, vocal and motor tics, and OCD and ADHD severity were highlysignificantly correlated with impairment score.
Conclusion: Knowledge of phenotype development may be useful inclinical settings.

www.mghcme.org

www.mghcme.org

www.mghcme.org

www.mghcme.org

www.mghcme.org
Chronic Tic Disorders (CTD) in Children with ADHD(Poh, W., Payne, J. et al. Arch Dis Child; 2018; 0; 1-6)
Aim: To examine 1) prevalence of chronic tics in a community based cohortin children with ADHD compared to children with non-ADHD at ages 7 and10 and 2) additional psychiatric and functional burden of CTD in childrenwith ADHD.Methods: N=179 children age 6-8 with ADHD and 212 controls recruitedthrough 43 schools using parent and teacher Conners followed by caseconfirmation with DISC-IV. Baseline and 36 month follow up evaluationsincluded measures of tics, CBCL, academic performance and quality of life.
Results: Compared with controls, children with ADHD were 4 times morelikely to have CTD at age 7 and 5.9 times more likely at age 10. Childrenwith ADHD + CTD experienced higher rates of internalizing, externalizingdisorders, peer problems and poorer quality of life than those with ADHDalone.
Conclusions: Clinicians should be aware of and manage both symptoms.

www.mghcme.org

www.mghcme.org

www.mghcme.org

www.mghcme.org
Course of ADHD and Tic Disorders: What Happens to
Tics in the Context of ADHD Over Time? (Spencer, T. Biederman, J. Coffey, B. et al. Arch Gen Psych 1999, 56: 842-847)
• Design: Prospective ADHD Follow-up • Objective: To evaluate the prevalence and impact of tic
disorders at baseline and at follow-up on the course of ADHD.
• Methods: N=128 boys with ADHD; N=110 controls. Duration of follow-up: 4 years.
• Results: – Proportion of ADHD youth with tics: 34%– Remission rate for tics over 4 years: 65%– Remission rate for ADHD: 20%
• Conclusion: Tic remission rate is independent of ADHD Tic disorders did not impact ADHD course

www.mghcme.org
Onset of ADHD and Tic Disordersin ADHD Probands
Age in Years0 5 10 15 20 250
ADHD
Tic Disorders
10
20
30
40
50
60
70
80
90
100
Tic Disorders
ADHD

www.mghcme.org
Offset of ADHD and Tic Disordersin ADHD Probands
Age in Years
00 5 10 15 20 25
Tic Disorders
ADHD
10
20
30
40
50
60
70
80
90
100
Tic Disorders
ADHD

www.mghcme.org
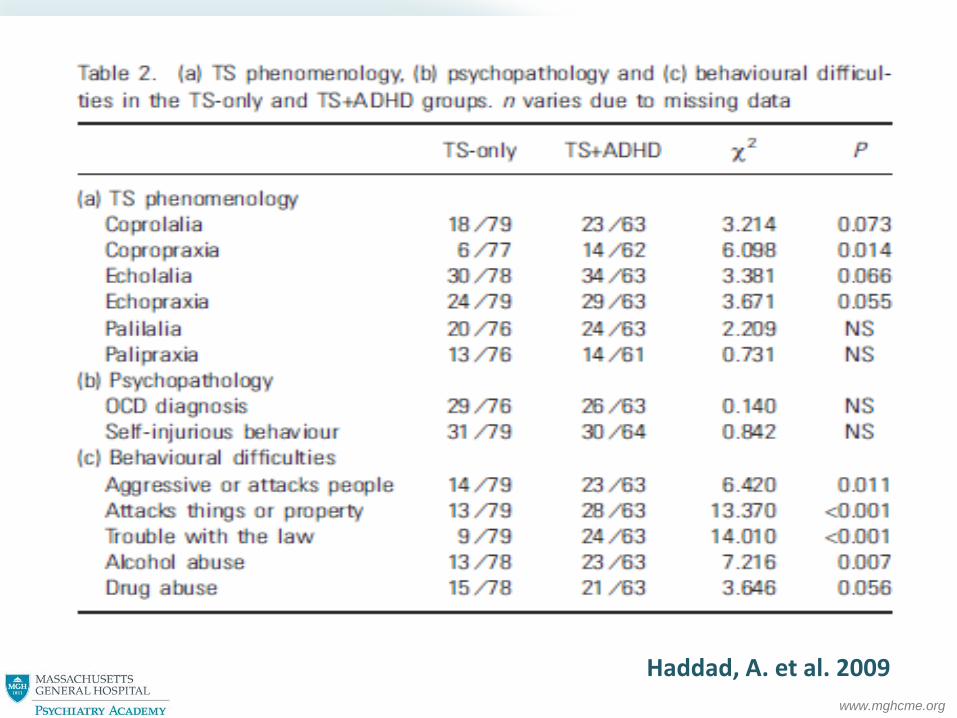
What About Adults?Adults with Tourette Syndrome with and without Attention Deficit
Hyperactivity Disorder(Haddad, A. Umoh, B. Robertson, M. Acta Psychiatr Scand; 2009; 120; 299-307)
• Design: N=80 adults with TS only were compared to 64 with TS+ADHD in a clinical interview and standardized measures of depression, anxiety and OCD
• Results: No differences noted in tic severity. • TS+ADHD had significantly more depression, anxiety,
OCD and behavioral problems than TS only. • Differences in ADHD family history.• Conclusion: More overall behavioral problems and
psychopathology was found in adults with TS+ADHD vs. TS only is consistent with findings in children.
• ADHD treatment in childhood may prevent development of behavioral problems later in life.

www.mghcme.org
Haddad, A. et al. 2009
www.mghcme.org
Haddad, A. et al. 2009

www.mghcme.org
Mount Sinai / Presentation Slide / December 5, 2012
30

www.mghcme.org
Diagnostic Evaluation: Tics and ADHD
• Structured diagnostic interviews, such as the Children'sSchedule for Affective Disorders and Schizophrenia (K-SADS) can improve classification and assessment ofcomorbidity.
• Standardized rating scales have improved diagnosticreliability in research studies; helpful in clinical care.
• The Yale-Global Tic Severity Scale (YGTSS) (Leckman,Riddle, Hardin, Ort, Swartz, Stevenson, et al., 1989) isconsidered the “gold standard.” The YGTSS assessesdomains of: tic number, frequency, intensity, complexityand interference (0-50), and tic related impairment (0-50).
• SNAP and Conners (Parent and Teacher) are helpful forquantitative evaluation of ADHD symptoms.

www.mghcme.org

www.mghcme.org

www.mghcme.org
Tics/Tourette’s Disorder: Pharmacotherapy Overview
Only formally approved (labeled) treatments for TD:
– D2 dopamine antagonists: conventional neuroleptics
– Haloperidol (Haldol) and pimozide (Orap)
(Physicians Desk Reference, 2017)
Haloperidol: effective for tics, superior to placebo
(Shapiro et al. 1968, 1978)
Pimozide: effective for tics, superior to placebo and haloperidol
(Shapiro et al. 1983, 1984; Sallee et al; 1997)
Aripiprazole: effective for tics, superior to placebo (Yoo et al 2013)
Other interventions
– Psychoeducation; referral to the Tourette Association of America
– **Habit reversal therapy (Comprehensive Behavioral Intervention for Tics)
– Individual and family therapy
– Educational consultation

www.mghcme.org
The Challenges of Treating Tics! Roessner et al. Eur Child Adolesc Psychiatry (2011); 20:173-196
What’s new in treatment of tics? Rounding up the usual suspects………

www.mghcme.org
www.mghcme.org
TD/Tics + ADHD: Treatment Overview
• Pharmacotherapy is cornerstone.
• Tics: Most patients with mild tic symptoms need only monitoring, education, and guidance.
• ***ADHD: Since ADHD symptoms are more likely to persist and cause significant functional impairment, treatment is usually necessary.
• Behavioral treatment of tics (Comprehensive Behavioral Intervention for Tics (CBIT)) is now established.
• There are no published studies of comorbid ADHD and tic disorders of combination pharmacotherapy and behavioral treatment.

www.mghcme.org
Daily Doses of Frequently Prescribed Tic Medications(Egolf, A. Coffey, B. Current Pharmacotherapeutic Approaches to the Treatment of Tourette Syndrome: Drugs Today; 2014 Feb; 50 (2):159-79. doi: 10.1358/dot.2014.50.2.2097801).
Medication Range of daily dosing
Haloperidol 0.25-4.0mg
Pimozide 0.5-8.0mg
*Risperidone 0.125-3.0mg
Aripiprazole 1.0-15.0mg
*Clonidine 0.025-0.4mg
*Guanfacine 0.25-4.0mg

www.mghcme.org
ADHD and Tics/TD: Can We Treat with Stimulants?
• Old studies suggested that stimulants increase tics, (Lowe
et al. 1980) and pharmaceutical labeling states tics are a contraindication for stimulants (PDR, 2017)
• Long term methylphenidate treatment did not worsen tics in children with ADHD and multiple tic disorders (Castellanos et al, 1997)
• More recent studies demonstrated that some TD patients with significant ADHD may be candidates for methylphenidate (MPH) when no other treatments have been effective (Gadow, Nolan, Sverd. 1992; Gadow et al. 2007)


www.mghcme.org
Meta Analysis: Risk of Tics Associated with Stimulant Use in Randomized, Placebo-Controlled Trials
=Design: Meta-analysis of RCTs of stimulants in treatment of ADHD. Results: N=22 studies with 2385 children with ADHD.New onset or worsening of tics were commonly reported with stimulants (5.7%) and placebo groups (6.5%). Risk of new onset or tic worsening associated with stimulants was similar to that of placebo (risk ratio=0.99, p=.962).
(Cohen, S. Mulqueen, J. Ferracioli-Oda, E. Stuckelman, Z. Coughlin, C,Leckman, J. Bloch, M. JAACAP; 2015; 54(9); 728-736)

www.mghcme.org
Meta Analysis: Risk of Tics Associated with Stimulant Use in Randomized, Placebo-Controlled Trials
Results: Stimulant type, dose, duration and age did not affect risk. Cross over studies were associated with a significantly greater risk than parallel group trials.Conclusion: There is no evidence for support of an association between new onset or worsening of tics with stimulant use in patients with ADHD.
(Cohen, S. Mulqueen, J. Ferracioli-Oda, E. Stuckelman, Z. Coughlin, C,Leckman, J. Bloch, M. JAACAP; 2015; 54(9); 728-736)

www.mghcme.org
ADHD, Stimulants and Tics: What Clinical Data is Needed to Weigh Risks and Benefits in Individual
Patients?
To what degree is the ADHD associated with distress and/or impairment in the child or adolescent?
Important factors in the clinical history:
Age of child?
Prior treatments?
Past history of tics?
Family history of tics, Tourette’s Disorder and/or Obsessive Compulsive Disorder?
Previous exposure to stimulants? If so, what class (amphetamines or methylphenidate) and what response?

www.mghcme.org
Practical Tips on Treating ADHD and Tics/TD with Stimulants
• Methylphenidates (MPH) are recommended
• Initiate treatment with very low doses: for example, for pre-pubertal children:
• Start with 2.5 mg bid
• Titrate to 5 mg AM, 2.5 mg PM
• Increase to 5 mg bid
• If tolerated, switch to 10mg equivalent long- acting delivery system, ie extended release MPH 10 mg or 18 mg OROS

www.mghcme.org
Practical Tips on Treating ADHD and Tics/TD with Stimulants
• Methylphenidates (MPH) are recommended
• For adolescents, MPH can be initiated at 10 mg and titrated upward gradually.
• If tics increase along the way, if ADHD symptoms have improved, hold the dose and monitor, or temporarily reduce the dose and titrate back upward.
• Guanfacine or clonidine can be added if tic increase is sustained.

www.mghcme.org
How To Decide? Systematic Review: Pharmacological Treatment of Tic Disorders: Efficacy of Antipsychotic and Alpha 2 Agonist Agents
• Design: Meta-analysis of RCTs in treatment of chronic tic disorders and examination of moderators
• Results: Significant benefit of antipsychotics vs. placebo. SMD=0.58. No significant difference in efficacy of risperidone, pimozide, haloperidol and ziprasidone.
• Significant benefit of alpha 2 agonists vs. placebo. Significant moderating effect of comorbid ADHD.
• With comorbid ADHD SMD:0.68. No ADHD: 0.15.
• Conclusion: Significant benefits of both medication types, but alpha 2 agonists may have minimal benefit in patients without ADHD.
(Weisman, H. Qureshi, I. Leckman, J. Scahill, L. Bloch, M. Neuroscience and Biobehavioral
Reviews; 2013; 37; 1162-1171)

www.mghcme.org

www.mghcme.org
Extended-Release Guanfacine (GXR) Does Not Show a Large Effect on Tic Severity in Children with Chronic Tic Disorders
(CTD)(Murphy T, Fernandez T, Coffey B, et al. JCAP. 2017;27(9):762–770.)
• Methods: 8-week RCT in N=34 youth ages 6 to 17 years (mean = 11.1) with CTD.
• Results: At baseline, mean YGTSS total score was 26.3 for GXR group vs. 27.7 for placebo. • GXR group: (mean final daily dose 2.6 mg.); mean YGTSS total score declined to 23; • p = 0.08; effect size = 0.35.• PBO group: declined to 24.7; p = 0.08; effect size = 0.38.
• There was no significant difference in the rate of positive response on CGI-I between GXR and PBO (19% vs. 22%; p = 1.0).
• Adverse Effects (AE): Most common: fatigue, drowsiness, dry mouth, headache, and irritability. Two subjects on GXR discontinued due to AE (depressed mood) and one for of lack of efficacy; two subjects on PBO discontinued for lack of efficacy.
• Conclusion: This pilot study did not confirm a clinically meaningful effect size within GXR group. These results do not support the launch of a larger efficacy trial for tics in youth with CTD.

www.mghcme.org
Extended-Release Guanfacine (GXR) Does Not Show a Large Effect on Tic Severity in Children with Chronic Tic Disorders
(CTD)(Murphy T, Fernandez T, Coffey B, et al. JCAP. 2017;27(9):762–770.)

www.mghcme.org
FIG. 2. YGTSS total score, motor, and phonic; guanfacine versus placebo. YGTSS, Yale Global Tic Severity
Scale.
Extended-Release Guanfacine (GXR) Does Not Show a Large Effect on Tic Severity in Children with Chronic Tic Disorders
(CTD)(Murphy T, Fernandez T, Coffey B, et al. JCAP. 2017;27(9):762–770.)

www.mghcme.org
Atomoxetine Treatment in Children and Adolescents with ADHD and Comorbid Tic Disorders
(Allen, A. Kurlan, R. Gilbert, D. Coffey, B. et al Neurology 2005; 65; 1941-1949)
Study Design: Randomized controlled trial; non-inferiority hypothesis.
Subjects: Children and adolescents 7-17 years old and weighing 20 - 80 kg
Met DSM-IV criteria for ADHD and had concurrent Tourette’s Disorder or chronic motor tic disorder
Two-week screening and washout period followed by a 3-week dose-titration phase and a 15-week acute treatment phase.
Subjects were randomly assigned to double-blind treatment with either placebo or atomoxetine (0.5 - 1.5 mg/kg/day)

www.mghcme.org
ADHD Rating Scale (ADHD RS)
Total ScoreInattentive Subscale
Hyperactive/Impulsive Subscale
-12
-10
-8
-6
-4
-2
0
Mea
n C
han
ge f
rom
Bas
elin
e
Atomoxetine
Placebo
Baseline 38.9 35.0 21.6 20.5 17.2 14.6
p=.019
p=.002
p=.002
**
***
Reduction in Symptoms

www.mghcme.org
Yale Global Tic Severity Scale (YGTSS)Tourette’s subjects Only
Baseline: 23.0 23.6 13.6 13.2 9.4 10.4 22.7 21.4
Total Motor PhonicOverall
Impairment
-7
-6
-5
-4
-3
-2
-1
0
Mea
n C
han
ge f
rom
Bas
elin
e
Atomoxetinee
Placebop=.027
p=.039p=.126
p=.019*
*
*
Reduction in
Symptoms

www.mghcme.org
A Multicenter Randomized Placebo-controlled Clinical Trial of Pramipexole for Tourette Syndrome
(Kurlan, R. Crespi, G. Coffey, B. et al. Mov Disord. 2012 May;27(6):775-8
• Design: 6 week multicenter randomized controlled study; N=63 children and adolescents
• Results: No difference between pramipexole and placebo in reduction of tics on YGTSS Total Tic score or CGI-improvement
• In patients with ADHD, there was significantly more improvement in DuPaul ADHD score compared to placebo
• Conclusion: There was no evidence that pramipexole was efficacious in tic reduction. Pramipexole may improve ADHD symptoms in comorbid ADHD and tics.

www.mghcme.org
A Multicenter Randomized Placebo-controlled Clinical Trial of Pramipexole for Tourette Syndrome
(Kurlan, R. Crespi, G. Coffey, B. et al. Mov Disord. 2012 May;27(6):775-8
)

www.mghcme.org
Evidence Based ADHD/Tics/TD Treatment Algorithm
ADHD + TD or Persistent Tic Disorder
ADHD Primary Tics Primary
Alpha AgonistStimulant (MPH)
Effective
Monitor
Tics Increase
Add Alpha-Agonist or Switch to Atomoxetine
Effective
Monitor
Intolerable or Inadequate
Consider atomoxetine+stimulant or pramipexole

www.mghcme.org

www.mghcme.org
Summary and Take Home Points: ADHD, Tics and Tourette’s Disorder
**There is bi-directional overlap of ADHD and Tic Disorders, including common neural substrates and phenomenology.
Prevalence of ADHD in TD in clinically referred samples is 50-75%, and tics in ADHD patients 10-30%.
ADHD symptoms tend to persist, but tic symptoms tend to remit over time. In children with TD, ADHD symptoms reduced over time in one large longitudinal study.
Much of the associated psychopathology (behavioral, neurocognitive) in Tourette’s Disorder is secondary to ADHD.
Children with ADHD + CTD are more likely to have psychopathology and reduced quality of life than those without CTD.
An alpha agonist is recommended as initial pharmacotherapy for ADHD + tics when tics are the primary issue. Start with a stimulant If ADHD is the primary issue.
Stimulants are effective in treatment of ADHD in children with ADHD and tics, and there is not evidence they produce or increase tic severity in the short run.
Tune in next year!!

www.mghcme.org
• ACKNOWLEDGEMENTS
Icahn School of Medicine at Mount Sinai Tics and Tourette’s Clinical and Research Program
• Wayne Goodman, M.D. Former Professor and Chair, Department of Psychiatry, Icahn School of Medicine at Mount Sinai
• Vilma Gabbay, M.D. M.SAssociate Professor, Department of Psychiatry, Director, Pediatric Mood and Anxiety and Disorders Clinical Research Program
• Dorothy Grice, M.D.Professor, Department of Psychiatry, Director, Pediatric OCD Program
• Ariz Rojas, Ph.D. Assistant Professor, Department of Psychiatry
• Maxwell Luber, B.A. Research Coordinator • Melissa Fluehr, B.A. Clinical Coordinator• Saniya Saleem, B.A. Research Intern