adrenal disorders
TRANSCRIPT

ADRENAL DISORDERS
Anand Vaidya, MD MMSc
Director, Center for Adrenal Disorders
Division of Endocrinology, Diabetes, & Hypertension
Brigham and Women’s Hospital
Associate Professor of Medicine, Harvard Medical School

• Harvard Medical School
• Internal Medicine Residency @BWH
• Clinical Endocrinology Fellowship @BWH
• Cardiovascular Endocrinology Research Post-
Doc @BWH
• Director, Center for Adrenal Disorders @BWH
• Associate Professor of Medicine @HMS

Disclosures
Consulting: Mineralys, Corcept, HRA Pharma

Learning Objectives
1. Review the pathophysiology of adrenal insufficiency and how to
make the diagnosis
2. Review the approach to an adrenal mass and how to conduct a
biochemical evaluation for adrenal hormone excess
3. Review the high and unrecognized prevalence of primary
aldosteronism
• 28yoF presents to ER 6 weeks after having a baby
• Cannot breastfeed well
• Presents with progressive fatigue, dizziness, orthostasis, salt craving,
hyperpigmentation, anorexia, and weight loss
• BP=60/40 mmHg
• IV saline (8L) and BP improves
• Cortisol 0.80 mcg/dL (3-21)
• ACTH>1000pg/mL (15-75)
• (60mins after 250 mcg cosyntropin)= 1.0 mcg/dL
Case 1

Question 1
The most likely diagnosis is:
A) Primary adrenal insufficiency
B) Acute secondary adrenal insufficiency
C) Chronic secondary adrenal insufficiency
D) Ectopic ACTH syndrome
E) Cushing’s disease
Question 1
The most likely diagnosis is:
A) Primary adrenal insufficiency
B) Acute secondary adrenal insufficiency
C) Chronic secondary adrenal insufficiency
D) Ectopic ACTH syndrome
E) Cushing’s disease

Adrenal Cortex: Steroidogenesis
Cholesterol
DHEA
Androstenedione
Testosterone
Estradiol
Pregnenolone
Progesterone
11-Deoxycorticosterone
Corticosterone
Aldosterone
17-Hydroxypregnenolone
17-Hydroxyprogesterone
11-Deoxycortisol
Cortisol
Zona Glomerulosa Zona Fasciculata Zona Reticularis

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
CRH
POMC
• ACTH
• (MSH)
H
P
Cortisol
Cortisol
Adrenal
Glucocorticoid
Receptor
11βOH-steroid dehydrogenase 2
Inactivates cortisol to cortisone
Hypothalamic-Pituitary-Adrenal Physiology

Hypothalamic-Pituitary-Adrenal Physiology
1-20mcg/dL
1-20 ng/dL
Schiffer et al. JSBMB 2019

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
CRH
ACTH
H
P
Aldosterone
K+
Adrenal
AGT
Ang-I
Ang-II
Renin ACE
Hypothalamic-Pituitary-Adrenal Physiology

1) Cortisol secretion is entirely dependent on ACTH
2) Aldosterone is not dependent on ACTH. It is regulated in part by:
• Angiotensin II (Renin-angiotensin system)
• K+ balance
• ACTH
3) HPA axis responds to:
• Diurnal variation/clock
• “stress”: ACTH & cortisol secretion is augmented “relative” to the degree of stress
Hypothalamic-Pituitary-Adrenal Physiology

25
20
15
10
5
0
2400 0400 0800 1200 1600 2000 2400
TIME
Co
rtis
ol (µ
g/d
L)
Hypothalamic-Pituitary-Adrenal Physiology
Bhake et al. JCEM 2019

Testing the HPA axis
STATIC TEST (entire HPA axis):
•Morning cortisol (and ACTH)
•An “appropriate” AM cortisol should ideally be >14-18 µg/dL, reflecting a
morning peak, but values > 10 µg/dL probably OK when pre-test
probability is low
•An AM cortisol <5 mcg/dL is highly suggestive of adrenal insufficiency
•AM cortisol levels between 5-10 may be difficult to interpret and can be
repeated

Testing the HPA axis
STATIC TEST (entire HPA axis):
•Morning cortisol (and ACTH)
•An “appropriate” AM cortisol should ideally be >14-18 µg/dL, reflecting a
morning peak, but values > 10 µg/dL probably OK when pre-test
probability is low
•An AM cortisol <5 mcg/dL is highly suggestive of adrenal insufficiency
•AM cortisol levels between 5-10 may be difficult to interpret and can be
repeated
PROVOCATIVE TEST (adrenal glands):
•250 µg cosyntropin stimulation test
•Stimulated cortisol <14* mcg/dL highly suggestive of adrenal
insufficiency
*18 mcg/dL is the traditional cutoff. New cortisol immunoassays and LC-MS/MS assays have lower thresholds

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
Adrenal
CRH
ACTH
H
P
Cortisol
Aldosterone
Manifestations/Characteristics:
Labs:
• low cortisol
• high ACTH
• low aldosterone
-hyperkalemia, hyponatremia,
hypovolemia
Physical Exam:
• fatigue/lethargy/anorexia
• hypotension/orthostasis/salt craving
• weight loss
• hyperpigmentation
• abdominal pain
• many many more
Primary Adrenal Insufficiency
(Addison’s Disease)

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
Adrenal
CRH
ACTH
H
P
Primary Adrenal Insufficiency
(Addison’s Disease)
CosyntropinMorning
60 mins following
250 µg cosyntropin
Cortisol (µg/dL) 1.8 2.1
ACTH (pg/mL) 1100
Response to Cosyntropin:
• sub-optimal
EXAMPLE:
Cortisol

Causes:
• Autoimmune
• Infiltrative infections (TB, fungal)
• Hemorrhage
• Infiltrative malignancy
• Congenital adrenal hyperplasia
• adrenoleukodystrophy
Medications:
• Anti-fungal medications
• Heparin
• Etomidate
Primary Adrenal Insufficiency (Addison’s)

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
CRH
ACTH
H
P
ACUTE Secondary Adrenal Insufficiency
Cortisol
Manifestations/Characteristics:
Labs:
• low basal cortisol
• inappropriately low ACTH
• ± hyponatremia
• Normal K and aldosterone regulation
Physical:
• completely normal
• mild, progressive, fatigue at baseline
• severe fatigue, orthostasis,
hypotension, in situations of stress
Adrenal

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
CRH
ACTH
H
P
ACUTE Secondary Adrenal Insufficiency
Cortisol
Cosyntropin
Response to Cosyntropin:
• NORMAL
Morning60 mins following
250 µg cosyntropin
Cortisol (µg/dL) 2.2 26.0
ACTH (pg/mL) 10
EXAMPLE:
Adrenal

Target
Organ
Cell
Glucocorticoid
Receptor
Mineralocorticoid
Receptor
CRH
ACTH
H
P
CHRONIC Secondary Adrenal Insufficiency
Cosyntropin
With chronic ACTH deficiency, adrenal cortex
(ZF) will atrophy, and will progressively
respond less to cosyntropin stimulation
Morning60 mins following
250 µg cosyntropin
Cortisol (µg/dL) 2.2 4.5
ACTH (pg/mL) 10
EXAMPLE:
AdrenalCortisol

Causes:
• Pituitary mass: adenoma or metastatic lesion
• Pituitary infection
• Pituitary infiltration (granulomatous disease, iron)
• Pituitary trauma
Medications:
• Glucocorticoids
• Megesterol
• Opioids
Secondary Adrenal Insufficiency

• Diagnosed with primary adrenal insufficiency (Addison’s)
• Treated with IV saline (8L)
• IV hydrocortisone 100mg q8hrs initially
• Transitioned to PO hydrocortisone/fludrocortisone
• Educated regarding recognizing illness or trauma requiring stress
dosing
• Trained to use an IM injection of hydrocortisone for emergencies
Case 1
Case 2
• 46 year old pre-menopausal woman was in a car accident.
• No known medical conditions
• Brought to ER and complained of some abdominal pain. Had a
rapid unenhanced Abdominal CT that revealed no hemorrhage or
other injuries
• Incidental discovery of a 2.2 cm R adrenal mass, with 5 HU
unenhanced densityWhat, if anything, do you tell her about
the incidental adrenal mass??

Incidentally Disovered Adrenal Masses
• Adrenal tumors are incidentally discovered in 1-10% of adults who are scanned.
• A minority represent malignant entities (primary adrenal malignancy or extra-
adrenal metastasis)
• In contrast, ~10-15% of adrenal tumors autonomously secrete adrenal hormones.
These “functional” tumors are associated with an increased risk for
cardiometabolic outcomes, such as CV disease, diabetes, and
osteoporosis/fracture.
• Therefore, all incidentally discovered adrenal tumors should be carefully evaluated
to determine whether they are: 1) malignant and/or 2) functional.
Vaidya et al. Endocrine Practice 2019
Differential Diagnosis of Adrenal Mass
NON-FUNCTIONAL FUNCTIONAL
BENIGN
MALIGNANT

Differential Diagnosis of Adrenal Mass
NON-FUNCTIONAL
(85-95%)
FUNCTIONAL
(5-15%)
BENIGN
(~90-95%)
Adrenocortical Adenoma
Cyst
Ganglioneuroma
Hemangioma
Hemorrhage
Infections and granulomatous
disease (tuberculosis, fungi,
sarcoidosis)
Lymphangioma
Myelolipoma
Pheochromocytoma
Schwannoma
Adrenocortical Adenoma
Aldosterone producing
Cortisol producing
Micro- or Macro-nodular Disease
Aldosterone producing
Cortisol producing
Pheochromocytoma
Myelolipoma*
Ganglioneuroma*
MALIGNANT
(~5%)
Adrenocortical carcinoma
Metastatic cancer from a non-
adrenal primary
Neuroblastoma
Adrenocortical carcinoma
Pheochromocytoma

General Diagnostic Approach
1. Is there evidence for malignancy?
2. Is there adrenal hormone excess?
History and physical exam
for evidence of hormone
excess or malignancy
Laboratory evaluation for
evidence of adrenal
hormone excess
Radiographic evidence
supportive of a benign or
malignant mass
Biochemical
Characteristics
Clinical
CharacteristicsRadiographic
Characteristics

Clinical Characteristics
• Obesity/weight gain
• Lipodystrophy
oCentral adiposity
oSupraclavicular fat pads
oDorsocervical fat pad
oRounded face
• Hyperglycemia/Diabetes
• Hypertension
• Insomnia
• Mood disorder/Psychosis
• Osteoporosis
• Immunesuppression
• Platelet dysfunction
• Hypercoagulable state
• Myopathy
• Atrophic skin
Overt
Cortisol Excess
Overt
Catecholamine Excess
Overt
Aldosterone Excess
• Episodic symptoms
o Hypertension
o Palpitations
o Anxiety/Panic
o Sweats/Tremors
o Headache
o Arrhythmia
• Hypertension
• Hypokalemia

Case 2 – Clinical Phenotype
• No symptoms
• No signs to suggest Cushing syndrome,
pheochromocytoma,
hyperaldosteronism, or hirsutism.
• No evidence of weight loss, abdominal
distention, or androgen excess, to
suggest metastatic cancer or
hyperfunctioning adrenocortical
carcinoma
Unrevealing
Clinical
Phenotype

Case 2 – Radiographic Phenotype
Patient’s non-contrast CTNormal comparison
2.2cm right adrenal mass
5 Hounsfield units
Round, homogenous

Question 2
A 2.2 cm adrenal nodule with an unenhanced density of 5 HU on
CT is most suggestive of:
A)Myelolipoma
B)Adrenocortical adenoma
C)Pheochromocytoma
D)Metastatic lung cancer to the adrenal gland
E)Adrenocortical carcinoma

Question 2
A 2.2 cm adrenal nodule with an unenhanced density of 5 HU on
CT is most suggestive of:
A)Myelolipoma
B)Adrenocortical adenoma
C)Pheochromocytoma
D)Metastatic lung cancer to the adrenal gland
E)Adrenocortical carcinoma

Case 2 – Radiographic Phenotype
CharacteristicsLikely
BenignPotentiallyMalignant
Irregular Shape No Yes
Heterogeneous content No Yes
Necrosis or Calcifications No Yes
Rate of Growth < 1cm/y ≥1cm/y
Attenuation on unenhanced CT
<10 HU ≥ 10 HU
Contrast washout on CT protocol at 15 minutes
Absolute>60%Relative>40%
Absolute ≤60%Relative ≤40%
MRI chemical shift
suggestive of lipid-rich content
Yes No
FDG avidity on PET No Yes
Size < 4 cm ≥ 4-6 cm
Benign: Suggestive of
adrenocortical adenoma
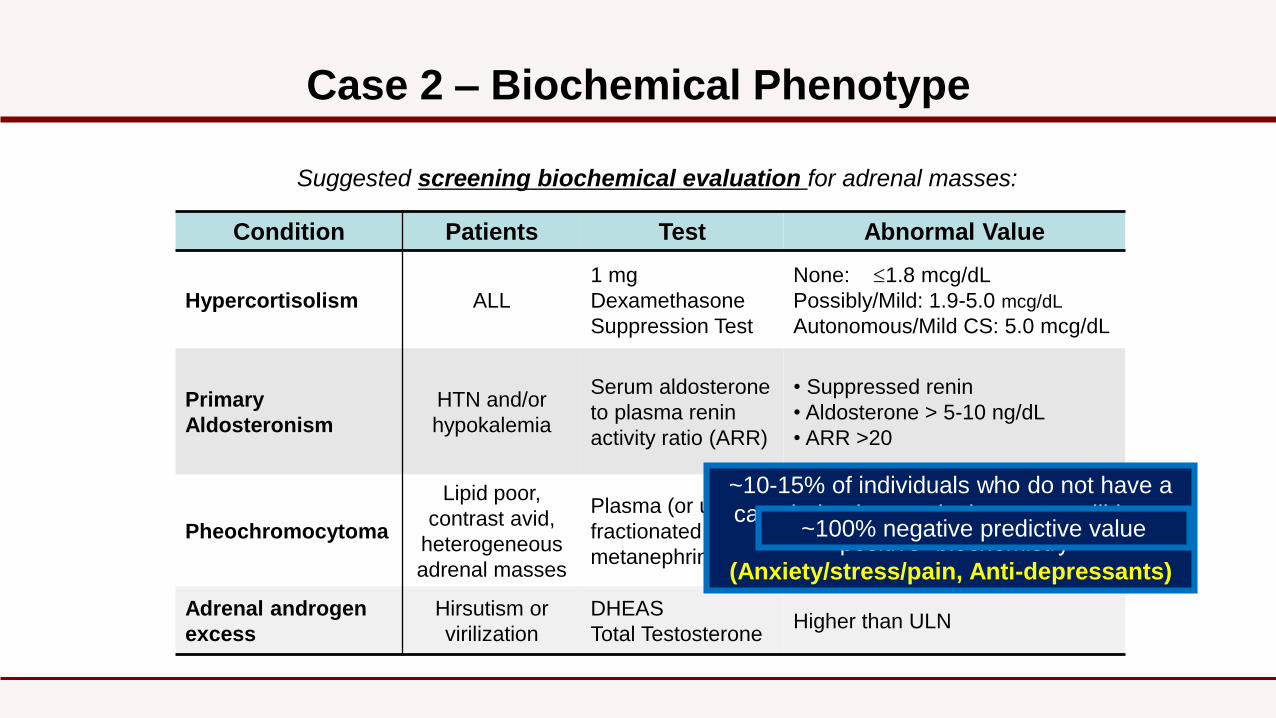
Case 2 – Biochemical Phenotype
Suggested screening biochemical evaluation for adrenal masses:
Condition Patients Test Abnormal Value
Hypercortisolism ALL
1 mg
Dexamethasone
Suppression Test
None: 1.8 mcg/dL
Possibly/Mild: 1.9-5.0 mcg/dL
Autonomous/Mild CS: 5.0 mcg/dL
Primary
Aldosteronism
HTN and/or
hypokalemia
Serum aldosterone
to plasma renin
activity ratio (ARR)
• Suppressed renin
• Aldosterone > 5-10 ng/dL
• ARR >20
Pheochromocytoma
Lipid poor,
contrast avid,
heterogeneous
adrenal masses
Plasma (or urinary)
fractionated
metanephrines
>> 2-4x ULRR
Adrenal androgen
excess
Hirsutism or
virilization
DHEAS
Total TestosteroneHigher than ULN
~10-15% of individuals who do not have a
catecholamine-producing tumor will have
“positive” biochemistry
(Anxiety/stress/pain, Anti-depressants)
~100% negative predictive value

Case 2 – Biochemical Phenotype
• 1mg DST #1 => cortisol: 8.0 µg/dL
• 1mg DST #2 => 7.8 µg/dL, ACTH<5 pg/mL, dex level normal
• 8mg DST => 8.1 µg/dL, ACTH<5 pg/mL
• 24h Urine Free Cortisol: 45 µg/24h (<45)
•Midnight Salivary Cortisol:
3.7, 3.9, 4.6, 4.3 nmol/L (<4.3)
• Random ACTH: <5 pg/mL
• DHEA-S: low
• Plasma metanephrines: normal
• Aldosterone/PRA: not suggestive
Suggestive of
autonomous and
ACTH-independent
hypercortisolism without
overt Cushing syndrome

• BP = 122/75 mmHg
• Fasting Blood Glucose = 99 mg/dL
• HbA1c = 5.8%
• Bone Mineral Density:
• Spine T= -3.2
• Femoral Neck T= -2.2
• Total Hip T= -2.0
Case 2 – Outcome
• Extensive work-up for secondary causes of osteroporosis: Negative

Case 2 – Clinical Diagnosis
Benign adrenocortical adenoma
Autonomous cortisol secretion
No overt clinical Cushing syndrome, but
unexplained osteoporosis
Should surgery be recommended?

• BP = 122/75 mmHg
• Fasting Blood Glucose = 99 mg/dL
• HbA1c = 5.8%
• Bone Mineral Density:
• Spine T= -3.2
• Femoral Neck T= -2.2
• Total Hip T= -2.0
Case 2 – Outcome
• Extensive work-up for secondary causes of osteroporosis: Negative
• INDIVIDUALIZED DECISION: Laparoscopic R adrenalectomy
• Pathology revealed 2.5 cm adrenal cortical adenoma
• Post-op AM cortisol 4 mcg/dL, ACTH<10 pg/mL (asymptomatic)
• 1 week post-op, morning cortisol = 17 µg/dL

Case 2 – Clinical Diagnosis
↑CVD
↑Mortality
↑Diabetes
↑osteoporosis/fracture
Autonomous Cortisol Secretion:
Lopez et al. Annals Int Med 2016
Elhassan e al Annals Int Med 2019
Kjellbom et al Annals Int Med 2021
Vaidya et al. Endocrine Practice 2019

Incidentally Discovered Adrenal Mass
Suspicious≥10 HU, contrast avid, heterogeneous, ≥4-6cm
Benign Appearing<10HU, <4cm, non-contrast avid,
homogeneous
No evidence/indication to support
longitudinal radiographic surveillance
If initially “nonfunctional”:
No indication to lab repeat testing unless new or
rapid comorbidities suspicious for hormone
excess
If autonomous cortisol secretion without
clinical syndrome:
• Individualized consideration for surgery based
on comorbidities and other factors.
• Consider longitudinal clinical/biochemical
surveillance
Biochemical Evaluation Radiographic CharacteristicsNonfunctional, or
Mild/autonomous cortisol secretion
without a clinical syndrome
Evaluate for Clinical Signs and Symptoms of Adrenal Hormone Excess
Biochemical Assessments & Evaluation of Radiographic Characteristics
Confirmation of Overt
Hormone Excess with Clinical
Syndrome
Surgery
Overt Hormone Excess
Concern for
metastases or
infection
Biopsy
Bilateral, history of
malignancy, or
immunesuppression?
Repeat Assessments in 3-6
mos•Growth>1 cm/year in any dimension
•Suspicious radiographic features
•New or worsening hormonal excess
Ambiguous results or
indecision regarding
surgery
Uncertainty?
UnilateralConsider confirmation on
alternative imaging such as CT
with washout, MRI, FDG-PET
Unilateral?
Unilateral
Suspicious
Mass
Suggested Diagnostic Algorithm for Incidentally Discovered Adrenal Mass
Vaidya et al. Endocrine Practice 2019
Case 3
Concerning for primary
aldosteronism!!
Clinical
Phenotype
• 60yo woman with hypertension
• Hypertension for ~30 years
• Currently on lisinopril, amlodipine, HCTZ
• BP 150-160/90-100 mmHg
– Resistant Hypertension
• K+ 2.5-3.5 for >10 years
• HCO3- 28-33 for >10 years

Case 3
• 60yo woman with hypertension
• Hypertension for ~30 years
• Currently on lisinopril, amlodipine, HCTZ
• BP 150-160/90-100 mmHg
– Resistant Hypertension
• K+ 2.5-3.5 for >10 years
• HCO3- 28-33 for >10 years
• PRA < 0.6 ng/mL/h
• PAC 15 ng/dL
Primary aldosteronism!!
Clinical
Phenotype
Treated with spironolactone;
BP controlled on 2 drugs

What is Primary Aldosteronism?
SYNDROME of Inappropriate, Relatively non-suppressible, Renin-independent
aldosterone production that results in excessive activation of the renal-MR, vicious
cycle of volume expansion => can increase BP, increases K+/H+ excretion, increases
risk for CV disease independent of BP (extra-renal MR)
Clinical Manifestations:
Reflect the severity and duration of the renin-independent aldosteronism
BP and potassium are dependent features
Hallmark Biochemical Diagnostics:
Suppression of Renin
Inappropriate/Dysregulated Production of Aldosterone
Vaidya et al. Endocrine Reviews 2018

Why should you care?
Part I: Preventable Cardiovascular Risk
Part II: Under-recognition
Part III: High Prevalence

Risk for Incident Composite Cardiovascular Events
Matched Idiopathic
Hypertension
Overt
Primary Aldosteronism
(No Targeted Therapy)
CAD ~2x -
Heart failure ~2x -
Stroke ~2.5x -
Afib ~3.5x -
LVH ~2.3x -
Monticone et al, The Lancet D&E 2018
↑CVD independent of BP

Risk for Incident Composite Cardiovascular Events
Hundemer et al, The Lancet D&E 2018
Bilateral PA
following Optimized
Medical Therapy
Idiopathic HTN
Years
Unilateral PA
following
Curative Surgery
0
20
40
0 2.5 5 7.5 10Cu
mu
lati
ve I
ncid
en
ce o
f C
om
po
sit
e C
V E
ven
ts (
%)
Primary Aldosteronism increases the risk for
CVD, and we have targeted therapies that
can mitigate this risk
How Common is the
Primary Aldosteronism Syndrome?

Prevalence of Primary Aldosteronism
Burrello et al. Hypertension 2020; Brown et al. Ann Int Med 2020
Resistant HTN ≥ 25%
Stage II HTN ≥ 10-15%
Stage I HTN ≥ 5-10%
HTN + hypokalemia ≥ 25%
HTN + severe hypokalemia ≥ 85%
In Reality…
Screening Rates Among Patients with R-HTN + Hypokalemia
<< 1 - 2%
Ruhle et al. Surgery 2019
Jaffe et al. Hypertension 2020
Liu et al. JAMA Surgery 2021
Cohen et al. Annals Int Med 2021

Primary Aldosteronism in the USA
Brown et al. Annals of Int Med 2020
N=1847
Oral Sodium Suppression Test
“gold standard” diagnostic

0
10
20
30
40
50
60
70
80
90
100
24
h U
rin
ary
Ald
os
tero
ne E
xc
reti
on
(m
cg
)
Number of Participants
Untreated
Normotension
Untreated
Stage I
Hypertension
Untreated
Stage II
Hypertension
12 mcg/24h =
Overt Primary Aldostronism
A severity spectrum of
non-suppressible,
renin-independent,
aldosterone production
(aka primary aldosteronism)
Brown et al. Annals of Int Med 2020
0 50 100 1500 50. 100 150. 200 0 50 0 50 100 150
Treated
Resistant
Hypertension
This is (milder) primary aldosteronism!!
Primary Aldosteronism in the USA

0
5
10
15
20
25
30
9.0%
15.7%
20.7%
24.0%
Cru
de P
revale
nce (
%)
Normotension Stage I HTN Stage II HTN Resistant Hypertension
Prevalence of Overt Primary Aldosteronism
Resistant Hypertension
% with Aldosterone < 10 ng/dL = 24%
Aldosterone production is pulsatile/variable
Aldosterone levels <10 ng/dL can still be inappropriate
Brown et al. Annals of Int Med 2020

Current and Future LandscapeAll Currently
Diagnosed PA
Resistant HTN
Prevalence of PA > 25%
< 1-2% of R-HTN + HypoK
are ever screened
< 1% ever diagnosed
All Currently
Diagnosed PA

Current and Future Landscape
Prevalence of PA
> 5-15%
<<< 1% ever
diagnosed
All HTN(>1 billion ppl)
Resistant HTN
All Currently
Diagnosed PA
True Prevalence of
Overt PA and
clinically-relevant
renin-independent
aldosteronism
amenable to
targeted therapy

Measure Plasma Renin and Aldosterone
Essential Indications
Severe or Resistant Hypertension
Any hypokalemia regardless of BP
HTN + adrenal mass or sleep apnea
Suggestive family history
Future Indications
Stage II hypertension?
New onset hypertension?
Indications to Screen for Primary Aldosteronism
Adapted from: Vaidya et al. JCEM 2020 & Endocrine Reviews 2018
Any time of day
No medication
changes
Do not miss your
chance!

Enhanced
Diagnostic
Pathway
Simplified Exclusionary PathwaySimplified Confirmatory Pathway
Renin Suppressed*
Aldosterone 5-15 ng/dL
POSITIVE SCREEN
Mild PA Likely
Marginal
Suppression
K+ < 3.5 mEq/L ?
Overt PA Likely
ConfirmedRepeat renin and aldosterone
on a future date to confirm
Yes
Consider repeat
evaluation after
cessation of certain
medications& if
applicable
Aldosterone >15 ng/dL
OVERTLY
POSITIVE SCREEN
Aldosterone <5 ng/dL
LIKELY
NEGATIVE SCREEN
PA UnlikelyRepeat renin and aldosterone on a
future date to confirm
MRA Therapy & Dietary
Sodium Restriction
Imaging
AVS to Determine
Potential for Unilateral
Adrenalectomy
Willing/able to undergo
more/advanced testing?
Aldosterone Suppression
Testing
Yes
No Empiric MR antagonist
therapy
Marked
Suppression
Clear Failure
of Suppression
Measure Plasma Renin and Aldosterone
Renin Not
Suppressed*
Adapted from: Vaidya et al. JCEM 2020 & Endocrine Reviews 2018
PRA <0.6 - 1.0 ng/mL/h
PRC <5 - 10 mU/L
MRAs & ENaCi
Rarely Others
Learning Objectives
1. Review the pathophysiology of adrenal insufficiency and how to
make the diagnosis
2. Review the approach to an adrenal mass and how to conduct a
biochemical evaluation for adrenal hormone excess
3. Review the high and unrecognized prevalence of primary
aldosteronism
ADRENAL DISORDERS
Anand Vaidya, MD MMSc
Director, Center for Adrenal Disorders
Division of Endocrinology, Diabetes, & Hypertension
Brigham and Women’s Hospital
Associate Professor of Medicine, Harvard Medical School