adult measures of quality of life: the arthritis impact measurement scales (aims/aims2), disease...
TRANSCRIPT
Adult Measures of Quality of LifeThe Arthritis Impact Measurement Scales (AIMS/AIMS2), Disease RepercussionProfile (DRP), EuroQoL, Nottingham Health Profile (NHP), Patient GeneratedIndex (PGI), Quality of Well-Being Scale (QWB), RAQoL, Short Form-36 (SF-36),Sickness Impact Profile (SIP), SIP-RA, and World Health Organization’s Qualityof Life Instruments (WHOQoL, WHOQoL-100, WHOQoL-Bref)
Alison Carr
ARTHRITIS IMPACT MEASUREMENTSCALES (AIMS/AIMS2)General Description
Purpose. Disease-specific measure of physical,social, and emotional well-being designed as ameasure of outcome in arthritis (1).
Content. There are 9 scales: mobility, physicalactivity (walking, bending, lifting), dexterity,household activity (managing money andmedications, housekeeping), social activities,activities of daily living, pain, depression, andanxiety. AIMS2 includes arm function, socialsupport, and work.
Developer/contact information. AIMS wasdeveloped by Robert F. Meenan, Dean, BostonUniversity School of Public Health, 715 Albany St.,T-C-306, Boston, MA 02118. E-mail: [email protected].
Versions. There is an original version, shortenedversion, an expanded version (AIMS2), a short-form of the AIMS2 (AIMS2-SF), a child version,and a version for the elderly (Geri-AIMS). AIMShas been translated into many languages includingPortuguese, Canadian French, Italian, Spanish,French, Dutch, Swedish, Turkish, and Norwegian.
Number of items in scale. AIMS 45, ShortenedAIMS 18, AIMS2 101, and AIMS2-SF 26.
Subscales. AIMS 9 (listed above); shortenedAIMS 9; AIMS2 12.
Populations. Developmental/target. Developedin patients with rheumatoid arthritis andosteoarthritis to assess the outcome of health care.
Other uses. AIMS has been used in otherconditions including: psoriatic arthritis, ankylosingspondylitis, fibromyalgia, carpal tunnel syndrome,colles fracture, hemophilia and in patientsundergoing joint replacement surgery. A 1-pagesummary of results has been developed for use inclinical practice.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-administered and relatively easy to
complete.
Training. None required.
Time to administer/complete. AIMS 15 minutes,Shortened AIMS 6–8 minutes, AIMS2 20–30minutes, AIMS2-SF 10 minutes.
Equipment needed. None.
Availability/cost. Available with user manualfrom Dr. Meenan (contact information above). Alsoavailable at http://www.qolid.org. (Click on freeaccess/disease-specific measures/rheumatology/AIMS2/public domain access/copy of original
Alison Carr, MSc, PhD: University of Nottingham, UnitedKingdom.
Address correspondence to Alison Carr, MSc, PhD, Spe-cial Lecturer in Musculoskeletal Epidemiology, Universityof Nottingham, Academic Rheumatology Clinical SciencesBuilding, City Hospital, Nottingham, NG5 1PB, UK. E-mail:[email protected].
Submitted for publication June 9, 2003; accepted June 19,2003.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 49, No. 5S, October 15, 2003, pp S113–S133DOI 10.1002/art.11414© 2003, American College of Rheumatology
MEASURES OF QUALITY OF LIFE
S113

AIMS2 question/copy of the user’s manual. Dutchand Italian translations available at same website.
ScoringResponses. Scale. Guttman.
Score range. Range is 0–10 for each section.Total health score 0–60.
Interpretation of scores. Zero represents goodhealth status, 10 and 60 represent poor healthstatus.
Method of scoring. Each section contains aGuttman Scale (a series of questions/statementsthat are graded so that endorsement of one level ofdisability automatically indicates disability on alllevels below it). In AIMS the number of responseoptions within the Guttman scales varies acrosssections. In AIMS2, the response format has beenstandardised across sections to 5-point scales. Forscoring, the Guttman scaling is ignored and eachitem is scored separately without weights. Higherscores indicate greater disability. The score foreach section is standardized to a 0–10 scale usinga standardization formula. The total health score iscalculated by summing the standardized scores formobility, physical and household activities,dexterity, pain, and depression.
Time to score. Scoring by hand takes around 10minutes. Computerized scoring can be completedin seconds.
Training to score. Minimal training is requiredfor scoring. Users’ guides are available.
Training to interpret. No specific training isrequired for interpretation of scores but familiaritywith the range and direction of scoring is helpful.
Norms available. None.
Psychometric InformationReliability. AIMS. Guttman scale coefficients for
scalability �0.6. Guttman scale coefficients forreproducibility �0.9. Internal consistency viaCronbach’s alpha �0.60 for each of the 9 sections.Test-retest correlations between 2 administrationsover a 2-week period in several studies �0.80.
Shortened AIMS. Internal consistency and test-retest reliability similar to the original AIMS.
AIMS2. Internal consistency via Cronbach’salpha over the 9 sections range from 0.72 to 0.91.
Test-retest intraclass correlation coefficients rangefrom 0.65 to 0.90 over a 10-day period, and from0.78 to 0.94 over a 3-week period.
AIMS2-S. Test-retest intraclass correlationcoefficients �0.70 over a 1-week period.
Validity. AIMS content validity. Items in AIMSare based on the content of the Rand HealthSurvey Questionnaires, the Quality of Well-BeingScale, and Katz’s Index of Activities of DailyLiving. Items on dexterity and pain were added.Factor analysis identified 3 factors (physicalfunction, psychological, and pain), which havebeen replicated in subsequent studies.
AIMS construct. Relevant subscales of AIMScorrelate strongly with other measures of theconstruct (e.g., physical activity AIMS scale withHealth Assessment Questionnaire (HAQ), AIMSpain scale with HAQ pain scale, AIMS andFunctional Status Questionnaire). Physicalfunctioning AIMS scales correlate more stronglywith measures of disease activity than AIMSpsychological or social scales. All scales correlatewith increasing age (i.e., reduced function withincreasing age).
AIMS2 content. Derived from AIMS butexpanded to include arm function, social support,and work giving a 5-factor structure (lowerextremity function, upper extremity function,affect, pain, and social interaction).
AIMS2 criterion. Moderate correlations withgeneral health status measures: NHP, SIP and ShortForm-36 (SF-36).
AIMS2 construct. Moderate, expectedcorrelations with disease activity (swollen jointcount, pain visual analog scale (VAS) anderythrocyte sedimentation rate).
AIMS2-SF content. Derived from AIMS2 usingDelphi and nominal group techniques. Principalcomponents factor analysis confirmed the same5-factor structure as AIMS2.
AIMS2-SF criterion. Comparison between AIMS2and AIMS2-SF using the Bland and Altmanmethod for measuring agreement found almostcomplete agreement. Moderate correlations withother general health status measures (MHAQ, SF-36, SIP) were very similar to the correlationsbetween these measures and AIMS2.
S114 Carr

AIMS2-SF construct. Correlations with clinicaland disease factors were moderate and as expected.
Responsiveness/sensitivity to change.Responsiveness of AIMS is better than most othergeneric and disease-specific measures (SIP, QWB,HAQ, Functional Status Index, MacMaster HealthIndex). AIMS2, and AIMS2-SF have similarresponsiveness. Standardized response means forchanges in AIMS2-SF scores over 3 months rangefrom 0.36 (small) to 0.8 (high).
Comments and CritiqueThe AIMS is a widely used disease-specific
measure that has a broad scope, measuring manyaspects of health status. It is more responsive inpatients with arthritis than any of the genericmeasures. The revised version, AIMS2 has goodpsychometric properties and the advantage ofincluding measures of satisfaction with health andpatients’ priorities for improvement. The full-length versions are quite time consuming tocomplete, and the short-form (AIMS2-SF) that hassimilar psychometric properties to the full-lengthversions, may be more appropriate for postalsurveys, studies where patients are required tocomplete several questionnaires, and in clinicalpractice.
References1. (Original) Meenan RF, Gertman PM, Mason JH.
Measuring health status in arthritis: the ArthritisImpact Measurement Scales. Arthritis Rheum 1980;23:146–52.
Additional ReferencesMeenan RF, Mason JH, Anderson JJ, Guccione AA, Kazis
LE. AIMS2: the content and properties of a revisedand expanded Arthritis Impact Measurement Scaleshealth status questionnaire. Arthritis Rheum 1992;35:1–10
Guillemin F, Coste J, Pouchot J, Ghezail M, Bregeon C,Sany J, and the French Quality of Life inRheumatology Group. The AIMS2-SF: a short formof the Arthritis Impact Measurement Scales 2.Arthritis Rheum 1997;40:1267–74.
Kazis LE, Anderson JJ, Meenan RF. Health statusinformation in clinical practice: the developmentand testing of patient profile reports. J Rheumatol1988;15:338–44.
Liang MH, Fossel AH, Larson MG. Comparisons of fivehealth status instruments for orthopaedicevaluation. Med Care 1990;28:632–42.
DISEASE REPERCUSSION PROFILE(DRP)General Description
Purpose. An individualized measure ofperceived disadvantage resulting from illness.Designed specifically for use in routine clinicalpractice in arthritis (1).
Content. Perceived disadvantage is measured in6 domains: physical activity, social activity,socioeconomic status, relationships, emotions, andbody image. In each domain, patients are asked tospecify the problem or problems they are currentlyexperiencing and to rate the degree of importancethat those problems have for them. The domainsare standardized but the specific problems withindomains are unique to each individual completingthe questionnaire.
Developer/contact information. Developed byAlison Carr, Department of AcademicRheumatology, University of Nottingham, ClinicalSciences Building, City Hospital, Nottingham NG52PR, UK.
Versions. One version, and adaptations toscoring (1997).
Number of items in scale. There are 6 items.
Subscales. A profile measure with 6 domainslisted above.
Populations. Developmental/target. Developedfor use in routine clinical practice with patientswith rheumatoid arthritis (RA), to identify specificproblems that might be amenable to interventionand to assess the effectiveness of care.
Other uses. Adapted for use in osteoarthritis,low back pain, upper limb problems, osteoporosis,and patients undergoing joint replacement surgery.Used in evaluative studies as a measure ofoutcome. It has also been used in clinical practiceas the basis for goal-setting for patients with RA.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-administered. Easy to complete for
all age groups and severity of disease.
Training. None required.
Adult Quality of Life S115

Time to administer/complete. Time is 2–15minutes depending on the number of problemspatients are experiencing. Problems are specifiedusing free text.
Equipment needed. None.
Availability/cost. Available from Dr. Carr at theabove address. No charge for research/clinical use.Also available at the Arthritis Care & ResearchWeb site at http://www.interscience.wiley.com/jpages/0004-3591:1/suppmat/index.html.
ScoringResponses. Scale. Ordinal.
Score range. Range is 0–10 for each domain.
Interpretation of scores. Produces a profile ofdisadvantage across the 6 domains. The profile ispresented as a bar chart. Zero represents noproblems or no perceived disadvantage resultingfrom problems, and 10 represents severedisadvantage.
Method of scoring. Each domain has a screeningquestion asking whether any problems arecurrently experienced in this area. If yes, patientsare asked to specify the problem and itsconsequences using free text. They are then askedto rate the importance of the consequences.Screening questions are coded 0 for no problem, 1for yes. Domain scores are calculated bymultiplying the screening question by theimportance rating. These are plotted on a bar chart.The qualitative information is not scored but isused as the basis for setting treatment goals.
Time to score. Scoring by hand takes around 1minute.
Training to score. Minimal.
Training to interpret. Minimal. The bar chartprofile enables problem areas to be identified at aglance. The questionnaire can then be reviewed toidentify the specific problems experienced by thepatient.
Norms available. None.
Psychometric InformationReliability. Internal consistency. Assessment of
internal consistency is not appropriate in this sortof profile measure where each domain is distinct
and items within the domain are individuallyspecified by patients.
Test-retest. Good reliability over a 1-weekperiod. No differences in profile scores.
Validity. Content. The domains covered weredetermined by a 2-step process: qualitative in-depth interviews with patients, followed by alarge-scale postal survey of patients to confirm thecontent specified in the interviews.
Construct. Moderate correlations betweenindividual domains and other measures of thesame construct (e.g. functional activity with HAQdisability index and SF-36 physical function score;social activity with SF-36 social function score;relationships with Quality of Social Support Scale;emotions with Hospital Anxiety and DepressionScale; and body image with Body SatisfactionScale). Socioeconomic scores are higher inunemployed and invalid-retired than employed orretired patients. Weak correlations betweenmeasures of disease activity (C-reactive protein[CRP], early morning stiffness, Ritchie Index, pain)and most domains demonstrating the conceptualdifference between impairment and disadvantage.
Responsiveness/sensitivity to change. More dataneeded from clinical trials. As responsive tochange in clinical practice as other measures ofhealth status (HAQ and SF-36). A ceiling effect forsome domains reflects the design of the tool as anindividualized measure for use in clinical practice(i.e., a minority of patients report problems insome domains which may be important in clinicalpractice).
Comments and CritiqueThe DRP is different from most other general
health status measures, being individualized ratherthan standardized and designed specifically for usein clinical practice. This means it may need to beassessed using methods that differ slightly fromtraditional psychometric methods. This problem iscommon to other individualized measures such asthe Patient Generated Index and the Schedule forthe Evaluation of Individualized Quality of Life(SEIQoL) and may account for some problems inassessing the construct validity of individualizedmeasures. It has been successfully used as thebasis for a goal-setting approach to diseasemanagement in RA, and its main strength remainsits use in routine clinical practice, although it hasalso been used as an outcome measure inevaluative studies.
S116 Carr
References1. (Original) Carr AJ. A patient-centered approach to
evaluation and treatment in rheumatoid arthritis: thedevelopment of a clinical tool to measure patient-perceived handicap. Br J Rheumatol 1996;35:921–32.
Additional ReferencesSharpe L, Sensky T, Brewin CR, Allard S. Characteristics
of handicap for patients with recent onsetrheumatoid arthritis: the validity of the DiseaseRepercussion Profile. Rheumatology 2001;40:1169–74.
Carr AJ. Beyond disability: measuring the social andpersonal consequences of osteoarthritis.Osteoarthritis Cartilage 1999;7:230–8.
EUROQOL/EQ-5DGeneral Description
Purpose. Generic measure of health-relatedquality of life designed for use in evaluativestudies to allow comparison across patient groups.It is also a utility measure that can assess patients’preferences for health states for use in economicanalyses (1).
Content. In its simplest form for use in clinicalresearch, it assesses quality of life in 5 dimensions:mobility, self-care, usual activity, pain/discomfort,and anxiety/depression. It also includes an overallassessment of patients’ perception of their healthstate.
Developer/contact information. The EuroQol(EQ-5D) was developed by the EuroQol Group in1990. The Group is an international network ofresearchers from different disciplines. Itsadministrative office is in Rotterdam: Frank deCharro, Centre for Health Policy and Law, ErasmusUniversity, PO Box 1738, 3000 DR Rotterdam, theNetherlands. E-mail: [email protected].
Versions. The EQ-5D was developedsimultaneously in English, Dutch, Finnish,Norwegian, and Swedish. It has also beentranslated into 20 other languages including mostEuropean languages.
Number of items in scale. There are 5 items plusthe 0–100 graphic rating scale for overall healthstatus.
Subscales. Each of the 5 items and the generalhealth status scale can act as subscales.
Populations. Developmental/target. Developedfor use in evaluative studies in all patients.
Other uses. Health economic studies, populationsurveys, healthcare audit, needs assessmentstudies.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-completed. Suitable for postal
surveys. Very quick and easy to complete.
Training. None required.
Time to administer/complete. 2–5 minutes.
Equipment needed. None required.
Availability/cost. Available from: Frank deCharro at Erasmus University (address above) orProfessor Paul Kind: Centre for Health Economics,University of York, York YO1 5DD UK. E-mail:[email protected]. Also available through:http://www.euroqol.org. There is no charge for itsuse in clinical research. Users are encouraged toregister and share their results with the EuroQoLGroup.
ScoringResponses. Scale. Ratio.
Score range. Index score 0–1, general healthstatus score 0–100.
Interpretation of scores. For the index score, 0represents full health and 1, death. On the generalhealth status scale, 0 represents the worst and 100the best imaginable health state.
Method of scoring. EQ-5D can give 3 differentscores: a profile, a weighted health index, and thegeneral health status score. Each of the 5 items/dimensions is divided into 3 levels (no problem,some problem, and extreme problem).
To produce the profile score, the levels foreach item are simply represented as a 5-digitnumber, each digit representing the level ofdifficulty on one of the dimensions. To calculatethe weighted index across the 5 dimensions,population weights are assigned for each level ofdifficulty selected and are subtracted from 1. In theUK, the population weights were obtained from ahealth survey in 1993.
To obtain a general health status score,patients are asked to place a horizontal line acrossthe point on a 100-point graphic rating scale that
Adult Quality of Life S117
corresponds to their current health state and thescore is read directly from the scale.
Time to score. The profile and general healthstate scoring can be done by hand and takes 1–2minutes. Computer software can be used tocalculate the weighted index.
Training to score. Minimal. User manualavailable.
Training to interpret. Minimal.
Norms available. In the UK, norms are availableby age group, sex and socioeconomic class.
Psychometric InformationReliability. Test-retest. Intraclass correlations for
test-retest reliability over a 1 week period rangefrom 0.69 to 0.94.
Validity. Content. The questionnaire wasdevised by a group of experts, based on knowledgeof existing health status measures. The aim forcontent was brevity but with the most importantdimensions of quality of life represented. It istherefore not exhaustively comprehensive but isdesigned to be used in conjunction with otherquality of life measures.
Criterion. Correlates with SF-36 and the HealthUtilities Index.
Construct. Patterns of responses across recentusers of healthcare, age group, gender and socio-economic group are as expected. Correlations withspecific measures of individual domains (HAQ,Hospital Anxiety and Depression Questionnaire,pain VAS) are moderately strong.
Responsiveness/sensitivity to change.Responsiveness to change has been demonstrated,but the EQ-5D is less responsive than the SF-36,and in specific conditions (e.g., back pain), it isless responsive than disease-specific measures.There are also reports of a ceiling effect in thefunction dimension with 95% of respondents atthe ceiling for function.
Comments and CritiqueThe EQ-5D has become an increasingly
popular measure of health status. Its attractionsinclude its simplicity and length, which makes itquick and easy to complete, and the potential forits use as a utility measure in economic analyses.For these reasons it is widely used in clinical trials
of treatment interventions. Its brevity means thaton its own, it would probably not provide anadequate assessment of quality of life in a studywhere quality of life is a major outcome but it canbe and often is, used alongside more detailedquality of life questionnaires. It is probably alsomore appropriate in studies in which large healthchanges are expected.
Although some users in rheumatic diseasehave found the EQ-5D valid and responsive, othershave been critical of its inability to discriminatepatients with moderate morbidity, the restricteddistribution of scores and differences betweenpatient and societal utility tariffs. This last point isan increasingly recognised phenomenon: peoplewith chronic or severe diseases may value thequality of their lives in different ways from thehealthy population. This “disability paradox”explains the high quality of life ratings of severelydisabled or seriously ill patients and hasimplications for the appropriateness of societal-determined weights.
References1. (Original) EuroQol Group. EuroQol: a new facility for
the measurement of health-related quality of life.Health Policy 1990;16:199–208.
Additional ReferencesBrazier JE, Harper R, Munro J, Walters SJ, Snaith ML.
Generic and condition-specific outcome measuresfor people with osteoarthritis of the knee.Rheumatology 1999;38:870–7.
Johnson JA, Coons SJ, Ergo A, Szava-Kovats G. Valuationof EuroQol (EQ-5D) health states in an adult USsample. Pharmacoeconomics 1998;13:421–33.
Kind P, Dolan P, Gudex C, Williams A. Variations inpopulation health status: results from a UnitedKingdom national questionnaire survey. BMJ 1998;316:736–41.
Polsky D, Wilkie RJ, Scott K, Schulman KA, Glick HA. Acomparison of scoring weights for the EuroQolderived from patients and the general public.Health Econ 2001;10:27–37.
Wolfe F, Hawley DJ. Measurement of the quality of lifein rheumatic disorders using the EuroQol. Br JRheumatol 1997;36:786–93.
NOTTINGHAM HEALTH PROFILE (NHP)General Description
Purpose. Generic measure of general healthstatus designed for use in primary care settings (1).
Content. It measures functional ability, pain,sleep, energy, emotional problems, andparticipation (work and social activities).
S118 Carr
Developer/contact information. Sonja Hunt,Galen Research, Enterprise House, ManchesterScience Park, Lloyd St, North, Manchester M156SE, UK.
Versions. There is an original and a revisedversion and it has been translated into mostEuropean languages and Arabic.
Number of items in scale. There are 38 items (inPart 1).
Subscales. The questionnaire is in 2 parts. Part 1has 6 subscales: physical activities (8 items); pain(8 items); sleep (5 items); social isolation (5 items);emotional reactions (9 items); and energy level (3items). Part 2 is optional and assesses handicap in7 items (occupation, household tasks, personalrelationships, sex life, social life, holidays, andhobbies).
Populations. Developmental/target. Developedin patients with acute and chronic illness.Designed for use in primary care settings.
Other uses. The NHP has been widely used inclinical trials in secondary care settings and inpopulation surveys.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-administered. The yes/no response
options have the apparent advantage of simplicity,but there are reports that some patients find itfrustrating to be limited to these options and maymake arbitrary responses as a result.
Training. None required.
Time to administer/complete. 10–15 minutes.
Equipment needed. None required.
Availability/cost. Available from Galen Research,Enterprise House, Manchester Science Park, LloydSt. North, Manchester M15 6SE, UK. Users must beregistered with Galen research and there is a smallcharge for its use. Instrument may be viewed athttp://www.medal.org/adocs/docs_ch1/doc_ch1.07.html.
ScoringResponses. Scale. Interval. Each item has
dichotomous yes/no responses.
Score range. The range is 0–100 for eachsection. The overall score is 0–1.
Interpretation of scores. For the section scores: 0represents no problems, 100 means all the itemswithin the section have been selected (i.e.,maximum impact of condition on health status).For the overall score the meaning is reversed: 0represents a poor health status score, and 1 meansgood health status.
Method of scoring. The questionnaire consists ofa series of statements about current health status.Patients answer yes or no to each statement withina section. In part 1, each item has a preassignedweight and the weights of the positive responseswithin each section are summed to give a score outof 100.
The overall score for part 1 can be generatedin several different ways. The simplest of these isto calculate what proportion of the 36 items havepositive responses and then subtract this from 1.This gives an unweighted overall score butcomparison with methods that generated weightedoverall scores found little difference between them.Items in part 2 are unweighted, and it is scored bythe number of positive responses.
Time to score. Scoring by hand can take up to10 minutes. If data are entered onto a computer,use of scoring algorithms makes scoring quick andeasy.
Training to score. Some training required if thequestionnaire is to be scored by hand. Minimal ifcomputer scoring is used.
Training to interpret. None required. 0–100scores make intuitive sense. The handicap score ismore difficult to interpret and requires guidance orfamiliarity.
Norms available. For healthy people by agegroup, social class, and sex and for some patientgroups. Norms should be used with cautionbecause of concerns about the lack of smoothtrends in health status across expected groups.
Psychometric InformationReliability. Test-retest correlation coefficients for
repeated administrations over a 4-week periodwere reported as 0.75–0.88 for Part 1 and 0.44–0.86 for Part 2. In patients with musculoskeletaldisease, the intraclass correlation coefficient was0.95.
Adult Quality of Life S119

Validity. Content. The questionnaire is based onpatients’ values and descriptions of the impact ofdisease on their quality of life rather thanprofessional views, ensuring good content validity.
Criterion validity. The NHP shows moderatecorrelations with other measures of general healthstatus (SF-36, SIP, Dartmouth COOP charts, andAIMS) and is less good than those measures atdetecting minor disability, indicating a floor effect.
Construct. Moderate to strong correlations withclinical and disease measures (McGill PainQuestionnaire, physician ratings, Ritchie index,pain VAS) in expected directions. Discriminatesbetween patients before and after total hipreplacement surgery; between those patients andtheir well spouses; between patients with physicaland mental handicaps; between stroke patients andhealthy controls; and between different severitiesof the same disease. However, it was unable todiscriminate differences in the severity andfrequency of angina.
Responsiveness/sensitivity to change. Data onthe responsiveness of NHP are mixed. It does notseem to be responsive to small changes in health(probably because of the dichotomous responsescaling), and the score distribution in patients withCOPD was skewed (�50% of patients had the bestscore). This and the floor effects (46% of people ina community survey reported no problems on theNHP) probably mean it is best avoided in healthsurveys, studies of mild disability/disease severity,or where treatment effects are expected to be small.
Comments and CritiqueBefore the development of the SF-36, the NHP
was one of the most widely-used health statusmeasures in Europe. It was an innovative measureat the time of its development, capturing thepatient’s perception of their health status.Although it is still a valuable tool in somesituations, it should be used with caution inhealthy populations (or those with mild disability)because of the floor effects, and there have beensuggestions that it is not suitable for use in healthsurveys because the range of disability covered byeach item is uneven. Its system of weighting andscoring has also been criticized, particularly inpeople whose disabilities limit their roles. Thenorms are considered of limited value as standardsbecause there are no smooth trends in health statusacross expected groups.
References1. (Original) Hunt SM, McEwen J. The development of a
subjective health indicator. Sociol Health Illness1980;2:231–46
Additional ReferencesDonovan JL, Frankel SJ, Eyles JD. Assessing the need for
health status measures. J Epidemiol CommunityHealth 1993;47:158–62
Jenkinson C. Why are we weighting? A criticalexamination of the use of item weights in a healthstatus measure. Soc Sci Med 1991;32:1413–6.
Kind P, Carr-Hill R. The Nottingham Health Profile: auseful tool for epidemiologists? Soc Sci Med 1987:25:905–10.
PATIENT GENERATED INDEX (PGI)
General DescriptionPurpose. Generic, individualized measure of
quality of life (1).
Content. Based on Calman’s definition of health-related quality of life as the gap betweenexpectations and reality. It asks patients to list the5 most important areas/activities in their life thatare affected by their condition and assesses theseverity of impact of their condition on theseareas/activities.
Developer/contact information. Developed byDr. Danny A. Ruta, Department of Epidemiologyand Public Health, Ninewells Hospital and MedicalSchool, Ninewells Road, Dundee, DD1 9SY, UK.
Versions. Interviewer and self-completedversions.
Number of items in scale. There are 5 items.
Subscales. Profile measure where eacharea/activity reported constitutes a scale.
Populations. Developmental/target. Designed toassess quality of life in evaluative studies across allconditions.
Other uses. It has been used in populationhealth surveys.
WHO ICF Components. Not applicable.
AdministrationMethod. Interviewer-administered and self-
completed. The self-completed version uses aprompt list to encourage patients to specify their 5
S120 Carr

areas/activities. Generally easy to completealthough some patients have difficulty with thevaluation exercise in which they are asked toallocate 60 points between their 5 areas on thebasis of which is most important. Difficulties inself-completion have been reported among elderlyand disabled patients.
Training. Minimal training required forinterviewer-administered version.
Time to administer/complete. 10–20 minutes.
Equipment needed. None.
Availability/cost. Available at no charge from DrRuta at the above address. It is also in the publicdomain, (reference 1).
ScoringResponses. Scale. Interval.
Score range. Range is 0–100 for each of 5domains, 0–100 for the overall quality of lifeindex.
Interpretation of scores. The scores representthe extent to which reality falls short ofexpectations. Zero represents a situation that is theworst imaginable, 100 represents a situation that isas good as the patient wants it to be.
Method of scoring. Having specified the 5 areas/activities affected by their condition that are ofmost importance to them, patients then rate thedegree of impact of their condition in each of these5 areas on a 0–100 scale. They are then asked todistribute 60 points between the 5 areas to reflecttheir relative importance. The overall index iscalculated by multiplying the rating for each areaby the points allocated to that area and summingthe 5 areas.
Time to score. Hand scoring is relatively quickand easy and takes a few minutes.
Training to score. Minimal.
Training to interpret. Scores of 0–100 arereadily interpreted.
Norms available. None.
Psychometric InformationReliability. Internal consistency. As with the
DRP, the nature and structure of the scale makeassessment of internal consistency inappropriate.
Test-retest. The original evaluation reportedPearson correlations of 0.7 over a 2-week period.More recent evaluation suggests some elderlypatients incorrectly interpret scoring instructions,reducing assessments of reliability (intraclasscorrelation coefficient [ICC] � 0.55). Reliabilitywas still good in patients who had interpreted theinstructions correctly (ICC � 0.67).
Validity. Content. Content is specified by eachindividual patient, thereby ensuring validity foreach patient.
Construct. Discriminates between patients withmild, moderate and severe arthritis, between usersand non-users of health services and betweenprimary care and specialist-referred patients withthe same condition. Correlates with general healthstatus measures (SF-36 and AIMS) and withsymptom severity.
Responsiveness/sensitivity to change. Data onresponsiveness is mixed. It is more responsive toclinical change in back pain than disease-specificinstruments and more responsive to changefollowing therapy in patients with sleep apneathan the EQ-5D or SF-36. However, it was unableto detect changes in health in a study of 1,027patients with arthritis.
Comments and CritiqueThe PGI is an innovative measure, one of a
handful that attempt to capture the individualnature of quality of life. Unlike many standardizedquality of life measures, it is based on anunderlying theory of what constitutes quality oflife. Its main drawback is the difficulty somepatients have with the evaluation exercise. Wherequality of life is to be measured in elderly ordisabled patients, it may be worth using theinterviewer-administered form to overcome theseproblems. Disease-specific trigger lists for the PGIare being developed for use in some rheumaticconditions (for example, ankylosing spondylitis) inan attempt to increase responsiveness and reduceproblems with completion. These versions are stillunder evaluation.
References1. (Original) Ruta DA, Garratt AM, Leng M, Russell IT,
MacDonald LM. A new approach to measurement ofquality of life: The Patient Generated Index. Med Care1994;32:1109–26.
Additional ReferencesMacDuff C, Russell E. The problem of measuring change
in individual health-related quality of life by postal
Adult Quality of Life S121
questionnaire: use of the patient generated index ina disabled population. Qual Life Res 1998;7:761–9.
Ruta DA, Garratt AM, Russell IT. Patient centredassessment of quality of life for patients with fourcommon conditions. Qual Health Care 1999;8:22–9.
Tully M, Cantrill J. The test-retest reliability of themodified Patient Generated Index. J Health ServRes Policy 2002;7:81–9.
Tully MP, Cantrill J. The validity of the modified patientgenerated index: a quantitative and qualitativeapproach. Qual Life Res 2000:9:509–20.
QUALITY OF WELL-BEING SCALE(QWB)General Description
Purpose. Generic measure of general healthstatus that places individuals on a continuum ofwellness from death to full asymptomatic function.It combines this index with an assessment ofprognosis and mortality to estimate qualityadjusted life years (QALYs). It was designed as ameasure of outcome for evaluative studies and inneeds assessment exercises (1).
Content. Symptoms and problems and currentstatus in terms of mobility, physical activity, andsocial activity.
Developer/contact information. Developed byJ. W. Bush and R. M. Kaplan. Contact R. M. Kaplan,PhD, Professor and Chief, Division of Health CareSciences 0622, School of Medicine, University ofCalifornia, San Diego, La Jolla, CA 92093-0622.
Versions. Original (interviewer-administered)with several modifications (most recent versionfrom 1994), a self-completed version, a childversion, and a version with simplified scoring(Functional Status Index).
Number of items in scale. There are 30 items.
Subscales. Quality of life index has 3 items;Symptom/problem complexes have 27 items.
Populations. Developmental/target. Patientswith all types of disease. Designed to enablecomparison between effectiveness of treatmentacross different disease groups.
Other uses. Evaluative studies (clinical trials).
WHO ICF Components. Not applicable.
AdministrationMethod. Interviewer administered. Self-
completion of the original version was associated
with poorer ability to detect disabilities. The newerself-completed version is still being assessed.
Training. Two weeks training for theinterviewer-administered version.
Time to administer/complete. 30 minutes.
Equipment needed. None.
Availability/cost. Interview schedule andmanual available at cost from Dr. Kaplan ataddress above. Also see http://medicine.ucsd.edu/fpm/hoap/instruments.html.
ScoringResponses. Scale. Ratio.
Score range. Quality of well-being index 0–1.
Interpretation of scores. Zero represents death,1 represents full, asymptomatic functioning.
Method of scoring. Each of the 3 items in thefunctional status section of the questionnaire hasseveral levels reflecting the severity of impact ofdisease on functioning (i.e., mobility [3 levels],physical activity [3 levels], social activity [5levels]). Each level has a pre-assigned weightrepresenting the social undesirability of that healthstate. Patients are categorized by level of severitywithin each section. The presence of any of the 27symptoms/problems is recorded (whether or not itaffects functional ability). As with the levels offunctional status, each symptom/problem complexhas a pre-assigned weight. Where there aremultiple symptoms, only the most undesirable isscored.
The QWB is calculated from the followingformula: W (QWB) � 1 – (mobility level �mobility weight) – (physical activity level �physical activity weight) – social activity level �social activity weight) – (symptom � symptomweight).
QALYs associated with the QWB score arecalculated by multiplying the QWB score by theamount of time spent in that state. Where severalmeasurements are available over time, thiscalculation is repeated for each change in healthstate and the results summed to give QALYs.Where there are data available on the probabilitiesof transition to a better or worse level offunctioning for the specific disease/treatment beingassessed, the QWB score is adjusted to reflect thisprognosis.
S122 Carr
Time to score. Scoring by hand is timeconsuming. Scoring by computer algorithm isquick and easy.
Training to score. Training is necessary forscoring by hand. For computerized scoring, littletraining is necessary beyond writing the computeralgorithm.
Training to interpret. Some training necessary tointerpret the scores. Interpretation requires afamiliarity with indices and QALYs.
Norms available. Norms are available for the USpopulation and for some disease groups (such asrheumatoid arthritis).
Psychometric InformationReliability. Interrater reliability of weights for
the functional status scale is high (0.90). Test-retestis assessed by comparing scores on day 1 with themean of daily scores on 8 subsequent days.Correlation between day 1 and subsequent scores�0.93.
Validity. Content. The scale has a broad scopebut does not specifically include any assessment ofpsychosocial functioning in the physicalfunctioning index (although the symptom/problemlist does include psychological symptoms).
Criterion. Moderate correlations with SIP, SF-36and AIMS.
Construct. Moderate correlations with clinicaltests in cystic fibrosis (forced expiratory volume(FEV1), peak oxygen consumption (VO2 max), andchronic obstructive pulmonary disease (exercisetolerance treadmill test). Moderate correlationswith Jette’s Functional Status Index. Strongcorrelations with the number of reportedsymptoms and chronic health problems. Moderatecorrelations with the number of recent physiciancontacts.
Responsiveness/sensitivity to change. QWB scalehas demonstrated significant treatment effects in anumber of conditions and treatments including:Chronic obstructive pulmonary disease, diabetes,AIDS, and rheumatoid arthritis (RA). In the RAtrial, the QWB scale was more responsive thanAIMS.
Comments and CritiqueThe QWB scale is a well-established measure
that is based on a clear conceptual background. Its
advantage is that it is able to produce utilities forhealth economic evaluations with more detaileddata than the EQ-5D, and the inclusion of asymptom/ problem list is likely to make it moresensitive to minor morbidity than some othergeneric measures. One of its major drawbacks inthe interviewer-administered form is that it is timeconsuming and appears relatively complex toscore. The development of a self-administeredversion that is as accurate as the interviewer-administered version and the use of computerizedscoring may significantly reduce these problems.Another major criticism has been the exclusion ofpsychological or emotional functioning from thescale, although the symptom list does includepsychological symptoms and the QWB score hasshown weak-moderate correlations with the Centerfor Epidemiologic Studies Depression Scale andthe AIMS psychological score.
References1. (Original) Kaplan RM, Bush JW, Berry CC. Health
status: types of validity and the Index of Well-Being.Health Serv Res 1976;11:478–507.
Additional ReferencesAnderson JP, Bush JW, Berry CC. Classifying function for
health outcome and quality of life evaluation: selfversus interviewer modes. Med Care 1986;24:454–69.
Andresen EM, Rothenberg BM, Kaplan RM. Performanceof a self-administered mailed version of the qualityof well-being (QWB-SA) questionnaire among olderadults. Med Care 1998;36:1349–60.
Kaplan RM, Ganiats TG, Sieber WJ, Anderson JP. Thequality of well-being scale: critical similarities anddifferences with SF-36. Int J Qual Health Care 1998;10:509–20.
RAQOLGeneral Description
Purpose. Disease-specific quality of life measurefor use in patients with rheumatoid arthritis (RA)(1).
Content. Assesses the impact of RA on activitiesof daily living, social interaction, emotional well-being, and relationships.
Developer/contact information. Developed by Dvan der Heijde, D Whalley, SP McKenna, and Z deJong in 1997 Galen Research, Enterprise House,Manchester Science Park, Lloyd St. North,Manchester M15 6SE, UK.
Adult Quality of Life S123

Versions. The original version was developedsimultaneously in English and Dutch. It has sincebeen translated into other languages includingSwedish, Canadian French, and Danish.
Number of items in scale. There are 30 items.
Subscales. None.
Populations. Developmental/target. Patientswith RA in the context of evaluative, economicand cohort studies, to determine the burden ofillness, and in clinical practice.
Other uses. None.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-administered.
Training. None required.
Time to administer/complete. Around 6 minutes,although it can be considerably longer in somepatients.
Equipment needed. None required.
Availability/cost. Available from Galen Research.Users are required to register. Items may be viewedat http://rheumatology.oupjournals.org/cgi/reprint/36/8/878.pdf (in appendix).
ScoringResponses. Scale. Ordinal. Dichotomous (yes/
no) responses to items.
Score range. The range is 0–30.
Interpretation of scores. A higher scorerepresents a poor quality of life.
Method of scoring. The questionnaire consists of30 statements that have a yes/no response. Itemsare scored 1 for yes and 0 for no. Scores for eachitem are summed to give an overall quality of lifescore.
Time to score. The questionnaire can be scoredby hand in a few minutes.
Training to score. Minimal.
Training to interpret. Minimal but someguidance/familiarity about what scores represent isnecessary.
Norms available. None.
Psychometric InformationReliability. Internal consistency via Cronbach’s
alpha is 0.90. Test-retest via Spearman rankcorrelations between first and secondadministrations 14 days apart is 0.90–0.94.
Validity. Content. Content of the questionnaireis based on qualitative interviews with RApatients, ensuring content validity. Simultaneousdevelopment in the Netherlands and the UKensures content validity across 2 cultural settings.
Criterion. Moderate correlations withNottingham Health Profile.
Construct. Discriminates between differentseverities of disease; and between active andinactive disease.
Responsiveness/sensitivity to change.Responsiveness currently under evaluation in arandomized controlled trial. Preliminary resultssuggest moderate responsiveness, similar to theNottingham Health Profile.
Comments and CritiqueThe RAQoL is quick and easy to use and has
the advantage of being specifically designed for usein RA. It is a new tool and needs furtherassessment in different research settings toevaluate its performance. It also needs to beevaluated in clinical practice and itsresponsiveness in individual patients should beestablished. The dichotomous response optionsmay make it susceptible to similar problems interms of responsiveness and questionnairecompletion as those suffered by the NottinghamHealth Profile. In addition, its superiority overother generic measures of health status/quality oflife should be established for it to have asignificant role in clinical research.
References1. (Original) De Jong Z, van der Heijde D, McKenna SP,
Whalley D. The reliability and construct validity ofthe RAQoL: a rheumatoid arthritis-specific quality oflife instrument. Br J Rheumatol 1997;36:878–83.
S124 Carr
Additional ReferenceWells G, Boers M, Shea B, Tugwell P, Westhovens R,
Suarez-Almazor M, et al, and the OMERACT/ILARTask Force on Generic Quality of Life, the LifeOutcome Measures in Rheumatology, InternationalLeague of Associations For Rheumatology.Sensitivity to change of generic quality of lifeinstruments in patients with rheumatoid arthritis:preliminary findings in the generic healthOMERACT study. J Rheumatol 1999;26:217–21.
SHORT FORM-36 (SF-36)General Description
Purpose. A generic measure of general healthstatus (health related quality of life) designed foruse in population surveys (1,2).
Content. The questionnaire assesses 8dimensions of health status: physical functioning,role limitations due to physical problems, bodilypain, social functioning, mental health, rolelimitations due to emotional problems, vitality andoverall/general health. It aims to measure positiveas well as negative health status.
Developer/contact information. Developed bythe Rand Corporation and John E. Ware. SF-36Health Survey, The Health Institute, New EnglandMedical Center Hospitals, Box 345, 750Washington Street, Boston, MA, 02111.
Versions. The SF-36 has been altered slightly onat least 2 occasions since the original version wasdeveloped. SF-36v2 is a revised and improvedversion of the original questionnaire that is nowrecommended in place of the SF-36v1.Improvements include changes to the questionsand responses that increases compatibility betweencultural settings; changes to question andinstruction wording and to the layout thatsimplifies and clarifies the questionnaire andreduces the number of missing responses;increased sensitivity of the role functioning scalesby changing the dichotomous responses to 5-itemresponses; and simplification of the mental healthand vitality scales by reducing the responses from6-level to 5-level.
SF-36 has been translated and adapted for usein a number of other languages including French,German, Dutch, Danish, Swedish, Spanish, Italian,and Japanese and has also been adapted for use inthe UK. The translated/adapted versions may bebased on different original versions of thequestionnaire. For example, the UK version wasadapted from the first version, before the two morerecent revisions were made.
There is an alternative form available thatmeasures change over shorter time periods (overthe last week) to enable assessment in acute healthconditions. Some disease-specific versions havealso been developed to improve responsiveness.For example, there is a version designedspecifically to measure health status in patientsundergoing knee replacement surgery.
Two shorter versions of the SF-36 areavailable: SF-12 and SF-8. These are based on theSF-36 and designed to reduce responder burden inlarge-scale population surveys.
Number of items in scale. SF-36 has 36 items,SF-12 has 12 items, SF-8 has 8 items.
Subscales. All of the SF versions have the same8 dimensions/subscales: Physical functioning (SF-36 has 10 items), Social functioning (SF-36 has 2items), Bodily pain (SF-36 has 2 items), Energy/vitality (SF-36 has 4 items), Mental health (SF-36has 5 items), Role limitations due to physicalproblems (SF-36 has 4 items), Role limitations dueto emotional problems (SF-36 has 3 items), Generalhealth (SF-36 has 5 items). The SF-12 and SF-36share 12 items with identical wording andresponse options, and the SF-8 and SF-36 share 1item.
Populations. Developmental/target. The SF-36 isa shortened version of the questionnaires designedfor use in the Rand Corporation’s Health InsuranceStudy. The target population was adults aged 14–61 years with a full spectrum of medicalconditions.
Other uses. It has been used in older patients(�61 years) and in many evaluative studiesincluding pharmaceutical trials.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Questionnaires that can be self-
completed or interviewer administered (atinterview or by telephone). Generally easy toadminister although there are reports that somepatient groups (for example, the elderly) mayexperience some difficulty in completion, resultingin missing data. There is also an internet versionavailable that enables patients to complete thequestionnaire on line on repeated occasions.Physicians can then access their patients’ datathrough the internet and monitor their progressover time.
Adult Quality of Life S125

Training. None required.
Time to administer/complete. SF-36 takesapproximately 10 minutes for most patient groups,15–20 minutes for some elderly patients. The SF-12 takes 5 minutes, and the SF-8 takes 2 minutes.
Equipment needed. None required.
Availability/cost. All SF-36 survey instruments,scoring manuals and licences for use are availablefrom QualityMetric at www.qualitymetric.com.There is a charge for the manual and use of thequestionnaires. Different charges are levied foracademic and commercial use. The internetversion is available from QualityMetric and islisted under Small Group Patient Tracking. Thereis a $99 set-up fee and then each surveytransaction is charged at $0.50 (with a minimumpurchase of 500 transactions).
Computerized scoring systems are availablefrom Response Technologies, Inc., 3399 SouthCountry Trail, East Greenwich, Rhode Island,02818. Items may be viewed at: http://www.medal.org/adocs/docs_ch1/doc_ch1.08.html#A01.08.01(SF-36), http://www.medal.org/adocs/docs_ch1/doc_ch1.08.html#A01.08.03 (SF-12).
ScoringResponses. Scale. Ordinal. There is a mixture of
3-, 5-, and 6-point scales for different items. In SF-36v2, dichotomous responses and 6-point scaleshave been changed to 5-point scales. All versions(SF-36v1, SF-36v2, SF-12v2, and SF-8) produce aprofile of 8 QoL scores. Two summary scores canalso be calculated from the profile scores: physicalhealth (physical functioning, role-physical, bodilypain, general health), and mental health (vitality,social functioning, role-emotional, mental health).
Score range. Range is 0–100 for each of the 8dimensions in SF-36v1. SF-36v2, SF-12v2, and SF-8 use norm-based scoring (mean 50, SD 10).
Interpretation of scores. Zero indicates poorhealth status, 100 indicates very good health status(i.e., no impact of condition on general healthstatus). For norm-based scores, any score above orbelow 50 can be considered above or below thepopulation average health status for that dimensionand each point on the scale is 1/10 of the standarddeviation.
Method of scoring. Computerized scoringrecommended. Responses on each item are enteredinto the computer using the codes given on the
questionnaire. Ten of the items are then recoded.Raw scores for each dimension are computed bysumming across the items in the samescale/dimension. Raw scores are transformed togive scores 0–100 for each dimension for SF-36v1.Norm-based scores are calculated for SF-36v2, SF-12v2, and SF-8 by including population norms inthe scoring algorithms.
Time to score. Once questionnaire data areentered on the computer, scoring takes a fewseconds. Computer software for analysis of SF-36is available from a number of sources. Scanningprograms that enable the completed questionnairesto be optically scanned into the database are alsoavailable. Computerized scoring recommended forversions that use norm-based scoring.
Training to score. Minimal if computer softwareis used.
Training to interpret. Minimal. The 0–100scores produced are easy to understand. Whatconstitutes a meaningful change in score is lessclear. Norm-based scoring makes interpretationeasier in relation to the general population andmakes change within populations more accurateand meaningful. It also allows direct comparisonbetween scores of each of the versions of the SFsurvey (SF-36v2, SF-12v2, SF-8) and comparisonbetween scores on each of the individualdimensions within the questionnaires.
Norms available. Population norms available forUS and UK. In the US, these are given for 7 agegroups and by sex. In the UK, they are given bysex, age, socioeconomic class, and for chronichealth conditions.
Psychometric InformationSF-36 is the version that has been most
extensively used and evaluated. SF-12 has beenevaluated in some studies and further evaluation ofit and SF-8 is being undertaken in large-scalepopulation surveys and clinical trials.
Reliability. Internal consistency. MedianCronbach’s alpha across several reliability studies�0.80 for all dimensions except social function(0.76). Studies suggest all dimensions reliable forcomparisons between groups of patients and thatthe physical function dimension may be reliablefor comparison within individuals.
Test-retest. Correlation coefficients for test-retestover a 2-week period �0.80 across all dimensions.
S126 Carr

Agreement between scores was high, differencesbetween measurements did not exceed 1 point onthe 100-point scales.
Validity. Face and content validity.Questionnaire was derived from pre-existingquestionnaires used in large population studies.
Criterion validity. Many studies have shownassociations between SF-36 and other generalhealth status measures such as NHP, EuroQoL,QWB, and SIP, indicating criterion validity.Criterion validity for individual dimensions hasbeen established by association with ability towork and pain ratings. SF-12 and SF-8 weredeveloped from the content of the SF-36. Theitems in SF-12 are identical to 12 of the items inSF-36. One of the items in SF-8 is identical to anitem in SF-36 and the others were developed fromevaluation of the SF-36 in population studies anddifferent cultural settings.
Construct validity. Distinguishes between knowngroups (ill and healthy, severe disease and milddisease, and chronic medical condition frommedical condition combined with psychologicalproblem).
Responsiveness/sensitivity to change. Mixedresults from studies assessing responsiveness.Appears responsive in some chronic conditions(e.g., in patients with soft tissue injuries). Somestudies have identified floor and ceiling effectswith specific patient groups (e.g. floor effects of therole dimensions in people on hemodialysis),although floor and ceiling effects should bereduced with version 2. In other studies,responsiveness was superior to other health statusmeasures (e.g., SF-36 identifies minor impacts onhealth status that cannot be identified using theNHP).
Comments and CritiqueThe SF-36 is the most widely used health
status measure worldwide. This means that,theoretically, the data in cross-cultural studies canbe aggregated or directly compared. It is a well-designed measure that has undergone exhaustivetesting in a number of situations. Some sensitivityand comprehensiveness have inevitably beensacrificed in the interests of brevity andstandardization, and users should evaluate theirresults in the context of what has actually beenmeasured. This consideration is even morepertinent for SF-12 and SF-8. Although mostpatients find it easy to use, there have been some
criticisms that elderly patients find thequestionnaire difficult to complete, often becausethe questions do not have significance for them,and it should be used with caution in patients �60years old, possibly in an interviewer-administeredform. This concern would be relevant to manypopulations of people with rheumatic disease.
The SF-36 has been used in many studies inrheumatology to document the relative healthstatus of different rheumatic conditions, assess theeffectiveness of interventions, or to assess thevalidity of new disease-specific questionnaires. Theshortened versions may be of use in populationsurveys of rheumatic disease where respondentburden is a concern. A computerized version of theSF-36 has been successfully used to collect healthstatus data in routine clinical practice inrheumatology.
One of the strongest arguments for using ageneric measure is the ability to makecomparisons, not only between patients with thesame condition in different settings or studies, butalso across patients groups but this should beundertaken with caution. Studies of differentpatient groups have found anomalies in the waysin which patients rate their quality of life, withmany chronically and seriously ill patients ratingtheir quality of life higher than patients with acute,mild disease. These differences may also existbetween different cultural settings. This disabilityparadox undermines the use of generic measures inmaking global comparisons.
References1. (Original) Ware JR, Sherbourne C. The MOS-36 item
short form health survey 1: conceptual framework anditem selection. Med Care 1992;30:473–83.
2. Ware JR, Kosinski M, Keller SD. A 12-item Short-Form Health Survey: construction of scales andpreliminary tests of reliability and validity. Med Care1996;4:220–33.
Additional ReferencesAnderson JJ, Ruwe M, Miller DR, Kazis L, Felson DT,
Prashker M. Relative costs and effectiveness ofspecialist and general internist ambulatory care forpatients with 2 musculoskeletal conditions.J Rheumatol 2002;29:1488–95.
Angst F, Aeschlimann A, Steiner W, Stucki G.Responsiveness of the WOMAC osteoarthritis indexas compared with the SF-36 in patients withosteoarthritis of the legs undergoing acomprehensive rehabilitation intervention. AnnRheum Dis 2001;60:834–40.
McHorney CA, Haley SM, Ware JE Jr. Evaluation of theMOS SF-36 Physical Functioning Scale (PF-10): II.Comparison of relative precision using Likert and
Adult Quality of Life S127
Rasch scoring methods. J Clin Epidemiol 1997;50:451–61.
Stucki G, Daltroy L, Katz JN, Johannesson M, Liang MH.Interpretation of change scores in ordinal clinicalscales and health status measures: the whole maynot equal the sum of the parts. J Clin Epidemiol1996;49:711–7.
Wilson AS, Kitas GD, Carruthers DM, Reay C, Skan J,Harris S, et al. Computerized information-gatheringin specialist rheumatology clinics: an initialevaluation of an electronic version of the ShortForm-36. Rheumatology (Oxford) 2002;41:268–73.
SICKNESS IMPACT PROFILE (SIP)General Description
Purpose. Generic measure of general healthstatus designed for use in population surveys,evaluative studies of the outcomes of care and inclinical practice to monitor patients. It measureschanges in behavior and daily activities due tosickness (1).
Content. The SIP assesses performance ofactivities in 12 categories: sleep and rest; eating;work; home management; recreation and pastimes;ambulation; mobility; body care and movement;social interaction; alertness behavior; emotionalbehavior; and communication.
Developer/contact information. Developed byMarilyn Bergner, Health Policy and Management,School of Hygiene and Public Health, JohnsHopkins University, 624 Broadway, Baltimore MD21205.
Versions. The SIP has been adapted for use inthe UK (known as the Functional LimitationsProfile) and has been translated into manylanguages including Swedish, Spanish, French,and Dutch. There are also shorter, disease- orsituation-specific versions for use in rheumatoidarthritis (SIP-RA), back pain, and nursing homes.
Number of items in scale. There are 136 items.
Subscales. There are 12 category scales (listed inContent section) that can be aggregated into 2subscales: physical (ambulation, mobility, bodycare and movement) and psychosocial (socialinteraction, alertness behavior, emotional behavior,and communication).
Populations. Developmental/target. Patientswith a range of medical conditions.
Other uses. Specific disease groups includingRA, head injury, back pain, and the elderly.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Interviewer-administered or self-
completed.
Training. Minimal. User manuals available.
Time to administer/complete. Approximately20–30 minutes.
Equipment needed. None needed.
Availability/cost. Available from Health Policyand Management, School of Hygiene and PublicHealth, Johns Hopkins University, 624 Broadway,Baltimore MD 21205. Also available from theMedical Outcomes Trust, PO Box 1917, Boston,MA, 02205 or through their Website:www.outcomes-trust.org.
ScoringResponses. Scale. Interval.
Score range. Each of the 12 categories is scoredfrom 0 to 100. The overall score ranges from 0 to100.
Interpretation of scores. Zero represents goodhealth status or no change of behavior resultingfrom sickness. 100 represents poor health status orlarge impact of sickness on behavior.
Method of scoring. The questionnaire consists ofa series of statements. Respondents check thoseitems that most relate to them. Each item isindividually weighted to indicate the severity ofimpact. The overall score is calculated by summingthe weighted values of the items selected, dividingthem by the scale values for all items andmultiplying the result by 100.
Time to score. 10 minutes.
Training to score. Minimal.
Training to interpret. Minimal. The 0–100scores have intuitive meaning.
Norms available. No.
Psychometric InformationReliability. Cronbach’s alpha values from several
studies for internal consistency range from 0.91 to0.95 for overall score, 0.84–0.93 for the 2
S128 Carr
subscales, and 0.60–0.90 for the 12 categories. Thetest-retest correlations between the 2administrations range from 0.88 to 0.92 for theoverall score. Test-retest correlation forinterviewer-administered version was 0.97 and was0.87 for the self-completed version. The interraterreliability (between raters Kappa) was 0.87.
Validity. Content. Face and content validityensured by the way in which questionnaire itemswere generated. Items were derived from aliterature review and interviews with professionals,patients and a healthy population.
Criterion. Concurrent validity established bycomparison with patients’ self assessments offunctional and sickness limitations and clinicians’assessments of functional and sickness limitation.There are strong correlations between SIP andAIMS (0.83) and AIMS2 (0.73).
Construct. Individual items and subscalescorrelated with other measures (e.g., Katz’s Indexof Activities of Daily Living, the Barthel Index,Carroll Rating Scale for Depression, and theGeriatric Depression Scale.) Correlations withmeasures of disease activity and severity areweaker (e.g., in RA, SIP scores correlate weakly[0.17–0.26] with disease duration, early morningstiffness, erythrocyte sedimentation rate andanatomic stage).
Responsiveness/sensitivity to change. Data onthe responsiveness of SIP are mixed. One study inRA patients suggested good responsiveness. Othershave found the SIP less responsive in patients withmusculoskeletal disease than other health statusmeasures.
Comments and CritiqueBefore the advent of the SF-36, the SIP was
considered the gold standard measure of generalhealth status. It is very comprehensive and hasbeen used over many years. It has been used inrheumatology to quantify health status and toassess the effectiveness of interventions/health caredelivery in RA. Limitations to its use inrheumatology relate to general problems in scoringand completion. Problems with responsivenessmay be worse if overall scores are used instead ofcategory scores because the same overall score canbe achieved through many different combinationsof item scores. This may obscure change in specificitems of importance to certain patient groups ortypes of treatment. An alternative method ofscoring has been proposed based on the highest
category score but this requires further evaluation.Its main disadvantage is that it is time-consumingto complete and score. This may limit itsusefulness in clinical practice and in studies wherepatients are required to complete severalquestionnaires. A shortened, disease-specificversion for rheumatoid arthritis (SIP-RA) has beendeveloped to overcome some of these problems.
References1. (Original) Bergner M, Bobbitt RA, Kressel S, Pollard
WE, Gilson BS, Morris JR. The sickness impactprofile: conceptual formulation and methodology for adevelopment of a health status measure. Int J HealthServ 1976;6:393–415.
Additional ReferencesAhlmen M, Sullivan M, Bjelle A. Team versus non-team
outpatient care in rheumatoid arthritis: acomprehensive outcome evaluation including anoverall health measure. Arthritis Rheum 1988;31:471–9.
Bergner M, Bobbitt RA, Carter WB, Gilson BS. TheSickness Impact Profile: development and finalrevision of a health status measure. Med Care 1981;19:787–805.
Pollard B, Johnston M. Problems with the sicknessimpact profile: a theoretically based analysis and aproposal for a new method of implementation andscoring. Soc Sci Med 2001;52:921–34.
Sullivan M, Ahlmen M, Bjelle A, Karlssm J. Healthstatus assessment in rheumatoid arthritis. II.Evaluation of a modified Shorter Sickness ImpactProfile. J Rheumatol 1993;20:1500–7.
SIP-RAGeneral Description
Purpose. Shortened version of the SIP developedto measure health status in patients withrheumatoid arthritis (RA) in clinical practice (1).
Content. SIP-RA measures performance in 10 ofthe original 12 SIP categories: body care andmanagement; mobility; emotional behavior; socialinteraction; alertness behavior; communication;sleep and rest; home management; recreation andpastimes; and eating.
Developer/contact information. MarianneSullivan, Professor of Psychology, Health CareResearch Unit, Sahlgrenska University Hospital,S-413 45 Gothenburg, Sweden.
Versions. Original, adapted from SIP.
Number of items in scale. There are 64 items.
Adult Quality of Life S129

Subscales. Physical: body care and movement(14 items), mobility (6 items); Psychosocial:Emotional behavior (7 items), social interaction (9items), alertness behavior (6 items),communication (2 items); and Free-standingcategories: sleep and rest (4 items), homemanagement (10 items), recreation and pastimes (5items), eating (1 item).
Populations. Developmental/target. Developedin women with RA. Target population, all patientswith RA.
Other uses. None to date.
WHO ICF Components. Activity limitation,Participation restriction.
AdministrationMethod. Self-administered and interviewer-
administered. Relatively easy to complete. Requirespatients to indicate which statements relate to theircurrent health status.
Training. Minimal.
Time to administer/complete. Time is 10–15minutes.
Equipment needed. None.
Availability/cost. Available from the developer.
ScoringResponses. Scale. Interval.
Score range. Each of the 10 categories is scoredfrom 0 to 100. The overall score ranges from 0–100.
Interpretation of scores. Zero represents goodhealth status or no change of behavior resultingfrom sickness, and 100 represents poor healthstatus or large impact of sickness on behavior.
Method of scoring. The questionnaire consists ofa series of statements. Respondents check thoseitems that most relate to them. Each item isindividually weighted to indicate the severity ofimpact. The overall score is calculated by summingthe weighted values of the items selected, dividingthem by the scale values for all items andmultiplying the result by 100.
Time to score. Time is 8–10 minutes.
Training to score. Minimal.
Training to interpret. None required.
Norms available. No.
Psychometric InformationReliability. Internal consistency. Cronbach’s
alpha values 0.59–0.86.
Test-retest. No published data available.
Validity. Content. Derived from the SIP. Itemreduction was performed in a 3-step process basedon the dependent variables: physical discomfort,bodily pain scale, overall mood (mood adjectivechecklist), and joint function (Keitel Index).
Criterion. High correlations between SIP-RA andthe original SIP. Some correlation would beexpected because SIP-RA is the same instrument.No data available for Bland and Altman’s methodfor measuring agreement, which removes this bias.
Construct. Discriminates between known groupson basis of American Rheumatism Associationfunctional class. Weaker correlations withmeasures of disease activity/severity (pain scale,Keitel Index, Ritchie Index, Lansbury Articularindex, C-reactive protein), similar to correlationsbetween the original SIP and disease measures.
Responsiveness/sensitivity to change.Responsiveness assessed by correlating change inSIP-RA with changes in measures of diseaseactivity over a 1-year period. The results showweak but statistically significant correlations,similar to correlations between the original versionof SIP and changes in measures of disease activity.No specific measures of responsiveness (effect sizeor standardized response means) published whichmakes the responsiveness of SIP-RA difficult toassess.
Comments and CritiqueThis disease-specific shorter form of the SIP
has some potential for use in rheumatology. It isbased on a well-established measure and thereduction in length will make it much easier andmore practical to use and score. One possiblecriticism is that the adaptation was based on dataonly from women with RA, which may limit itsgeneralizability to men with RA. The publisheddata do not indicate that it has any significantadvantages over the original version of SIP interms of responsiveness but this needs further
S130 Carr
investigation in clinical trials and statisticalindicators of responsiveness should be published.
References1. (Original) Sullivan M, Ahlmen M, Bjelle A, Karlssm
J. Health status assessment in rheumatoid arthritis. II.Evaluation of a modified Shorter Sickness ImpactProfile. J Rheumatol 1993;20:1500–7.
WORLD HEALTH ORGANIZATION’SQUALITY OF LIFE INSTRUMENTS:WHOQoL, WHOQoL-100, WHOQoL-BrefGeneral Description
Purpose. Multidimensional, multilingual profiledesigned for the cross-cultural assessment ofquality of life (1).
Content. Based on the WHO definitions ofhealth, it measures the positive as well as thenegative effects of ill health. It assessesindividuals’ perceptions of their position in life inrelation to their goals and expectations and withinthe context of their culture and value systems.
WHOQoL covers 30 facets of QoL: pain anddiscomfort; energy and fatigue; sexual activity;sleep and rest; sensory functions; positive feelings;thinking, learning, memory and concentration; self-esteem; body image and appearance; negativefeelings; mobility; activities of daily living;dependence on medication or treatment;dependence on non-medicinal substances;communication capacity; working capacity;personal relationships; practical social support;activities as provider; supporter; physical safetyand security; home environment; work satisfaction;financial resources; health and social care;opportunities for acquiring new skills;participation (recreation and leisure); physicalenvironments; transport; spirituality. There is alsoa section for overall perceptions of health andquality of life.
WHOQoL-100 covers the same areas butexclude sensory functions; dependence on non-medicinal substances; activities as supporter/provider; and work satisfaction.
WHOQoL-Bref has the same content asWHOQoL-100 but with fewer items.
Developer/contact information. The WHOQoLinstruments were developed by the WHOQoLgroup, a collaboration of international experts atWHOQOL Group Program on Mental Health,World Health Organization, CH-1211, Geneva 27,Switzerland. Further information about theWHOQoL instruments can be obtained from the
WHO Website: http://www.who.int/evidence/assessment-instruments/qol/index.html.
Versions. The original version, a shortenedversion (WHOQoL-100) and a brief version of theWHOQoL-100 (WHOQoL-Bref). WHOQoLinstruments were developed simultaneously inmany countries and are available in more than 40different languages worldwide.
Number of items in scale. WHOQoL: 281,WHOQoL-100:100, WHOQoL-Bref: 25.
Subscales. WHOQoL and WHOQoL-100 have 6domains containing different facets of QoL (eachfacet has several items): Physical (WHOQoL: 5facets, WHOQoL-100: 4 facets); Psychological (5facets); Activities (WHOQoL: 6 facets, WHOQoL-100: 4 facets); Social relationships (3 facets);Environment (WHOQoL: 9 facets, WHOQoL-100: 8facets), Spirituality (1 facet). WHOQoL-Bref has 4domains: Physical health (7 facets); Psychological(6 facets); Social Relationships (3 facets);Environment (8 facets).
Populations. Developmental/target.Measurement of quality of life in all well and illpopulations cross-culturally.
Other uses. None.
WHO ICF Components. Impairment, Activitylimitation, Participation restriction, Environmentalfactors.
AdministrationMethod. Self-completed. Even the longest
version (WHOQoL) is easy to complete for mostpopulations.
Training. None required.
Time to administer/complete. The longestversion (WHOQoL) takes 20 minutes for a wellpopulation to complete but can take up to 1.5hours for severely ill people to complete.Completion of WHOQoL-100 and WHOQ-L-Bref ismuch quicker.
Equipment needed. None.
Availability/cost. Available for use withpermission from the WHOQoL group at the addressabove. Manuals and syntax files for scoring are alsoavailable from the WHOQOL group. Thequestionnaires can be viewed on the WHO
Adult Quality of Life S131

Website: http://www.who.int/evidence/assessment-instruments/qol/index.html.
ScoringResponse. Scale. Ordinal.
Score range. Profiles of scores given for eachdomain. For WHOQoL-Bref, domain scores are 4–20.
Interpretation of scores. High scores indicate abetter quality of life.
Method of scoring. Individual items are scoredon one of 5 different 5-point rating scales. Domainscores for WHOQoL-100 are calculated bymultiplying the mean of all facet scores within thedomain by 4. Domain scores for WHOQoL-Bref arecalculated by multiplying the mean of all itemsincluded in the domain by 4.
Time to score. Minimal if computerized methodsused.
Training to score. Minimal.
Training to interpret. Minimal but someguidance about the meaning of scores necessary.
Norms available. None yet.
Psychometric InformationReliability. Internal consistency. Cronbach alpha
values for the domain scores range from 0.66 to0.97.
Validity. Content. The unique method ofdevelopment (simultaneous developmentworldwide with the ability to ensure conceptualequivalence in content) ensured the contentvalidity of the WHOQoL instruments. The contentis very comprehensive, covering all aspects of lifeand assessing the positive as well as negativeeffects of health on quality of life.
Construct. All instruments discriminate betweenwell and ill groups and between inpatients andoutpatients. Quality of life scores for all domainsexcept spirituality correlate with self-rated generalhealth (higher quality of life scores are associatedwith positively rated health and with SF-36
scores). The pain and discomfort facets correlatewith the McGill Pain questionnaire.
Responsiveness/sensitivity to change. Limitedresponsiveness data available to date. WHOQoL-100 and WHOQoL-Bref are responsive to changepost liver transplantation, after a pain managementprogram in chronic pain and to improvement indepression following antidepressant therapy.
Comments and CritiqueThe WHOQoL instruments are a unique
development in the measurement of quality of life.Their conceptual underpinning, the methods usedin their development and the comprehensivenessof the data they provide are very different from anyof the other available health status measures. Theyare still under psychometric evaluation but theresults to date have been very promising. Theavailability of a short form instrument (WHOQoL-Bref) makes its use in postal surveys and clinicalpractice more achievable, although using the short-form necessarily involves sacrificing some of thecomprehensiveness of the measure. For this reason,it has been recommended that if measurement ofsocial interactions/relationships is of primaryimportance, the more detailed WHOQoL-100 or theoriginal instrument should be used. To date, theWHOQoL instruments have only achieved limiteduse in rheumatology in patients with RA. However,its unique cross-cultural validity, ease ofcompletion, and comprehensive content make it apotentially valuable tool for clinical practice andresearch in rheumatology and in particular forinternational studies.
References1. (Original) The WHOQOL Group. The World Health
Organization Quality of Life assessment (theWHOQOL) position paper from the World HealthOrganization. Soc Sci Med 1995;41:1403–9.
Additional ReferencesSkevington SM. Measuring quality of life in Britain:
introducing the WHOQOL-100. J PsychosomResearch 1999;47:449–59.
The WHOQOL Group. Development of the World HealthOrganization WHOQOL-BREF Quality of LifeAssessment. Psychol Med 1998;2:551–8.
Wirnsberger RM, De Vries J, Jansen TL, Van Heck GL,Wouters EF, Drent M. Impairment of quality of life:rheumatoid arthritis versus sarcoidosis. Neth J Med1999;54:86–95.
S132 Carr
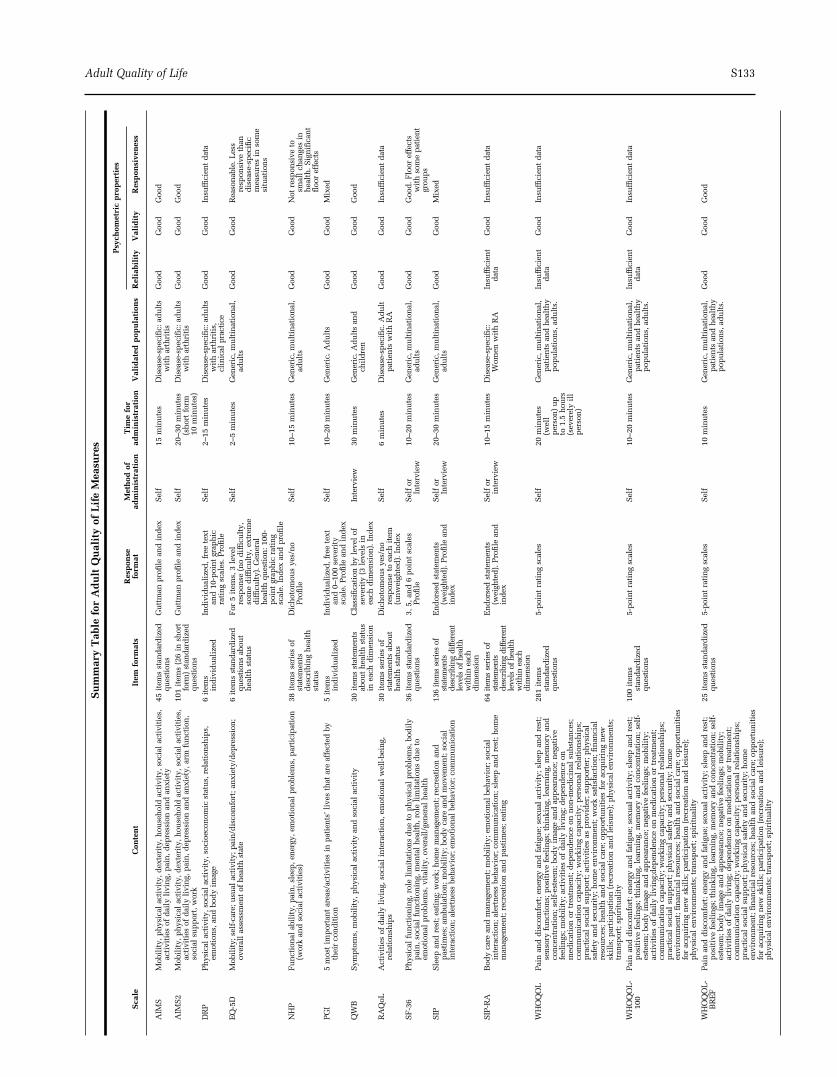
Su
mm
ary
Tab
lefo
rA
du
ltQ
ual
ity
ofL
ife
Mea
sure
s
Sca
leC
onte
nt
Item
form
ats
Res
pon
sefo
rmat
Met
hod
ofad
min
istr
atio
nT
ime
for
adm
inis
trat
ion
Val
idat
edp
opu
lati
ons
Psy
chom
etri
cp
rop
erti
es
Rel
iabi
lity
Val
idit
yR
esp
onsi
ven
ess
AIM
SM
obil
ity,
ph
ysic
alac
tivi
ty,d
exte
rity
,hou
seh
old
acti
vity
,soc
ial
acti
viti
es,
acti
viti
esof
dai
lyli
vin
g,p
ain
,dep
ress
ion
and
anxi
ety
45it
ems
stan
dar
diz
edqu
esti
ons
Gu
ttm
anp
rofi
lean
din
dex
Sel
f15
min
ute
sD
isea
se-s
pec
ific:
adu
lts
wit
har
thri
tis
Goo
dG
ood
Goo
d
AIM
S2
Mob
ilit
y,p
hys
ical
acti
vity
,dex
teri
ty,h
ouse
hol
dac
tivi
ty,s
ocia
lac
tivi
ties
,ac
tivi
ties
ofd
aily
livi
ng,
pai
n,d
epre
ssio
nan
dan
xiet
y,ar
mfu
nct
ion
,so
cial
sup
por
t,w
ork
101
item
s(2
6in
shor
tfo
rm)
stan
dar
diz
edqu
esti
ons
Gu
ttm
anp
rofi
lean
din
dex
Sel
f20
–30
min
ute
s(s
hor
tfo
rm10
min
ute
s)
Dis
ease
-sp
ecifi
c:ad
ult
sw
ith
arth
riti
sG
ood
Goo
dG
ood
DR
PP
hys
ical
acti
vity
,soc
ial
acti
vity
,soc
ioec
onom
icst
atu
s,re
lati
onsh
ips,
emot
ion
s,an
dbo
dy
imag
e6
item
sin
div
idu
aliz
edIn
div
idu
aliz
ed,f
ree
text
and
10-p
oin
tgr
aph
icra
tin
gsc
ales
.Pro
file
Sel
f2–
15m
inu
tes
Dis
ease
-sp
ecifi
c:ad
ult
sw
ith
arth
riti
s,cl
inic
alp
ract
ice
Goo
dG
ood
Insu
ffici
ent
dat
a
EQ
-5D
Mob
ilit
y;se
lf-c
are;
usu
alac
tivi
ty;p
ain
/dis
com
fort
;an
xiet
y/d
epre
ssio
n;
over
all
asse
ssm
ent
ofh
ealt
hst
ate
6it
ems
stan
dar
diz
edqu
esti
ons
abou
th
ealt
hst
atu
s
For
5it
ems,
3le
vel
resp
onse
(no
dif
ficu
lty,
som
ed
iffi
cult
y,ex
trem
ed
iffi
cult
y).G
ener
alh
ealt
hqu
esti
on:1
00-
poi
nt
grap
hic
rati
ng
scal
e.In
dex
and
pro
file
Sel
f2–
5m
inu
tes
Gen
eric
,mu
ltin
atio
nal
,ad
ult
sG
ood
Goo
dR
easo
nab
le.L
ess
resp
onsi
veth
and
isea
se-s
pec
ific
mea
sure
sin
som
esi
tuat
ion
s
NH
PF
un
ctio
nal
abil
ity,
pai
n,s
leep
,en
ergy
,em
otio
nal
pro
blem
s,p
arti
cip
atio
n(w
ork
and
soci
alac
tivi
ties
)38
item
sse
ries
ofst
atem
ents
des
crib
ing
hea
lth
stat
us
Dic
hot
omou
sye
s/n
oP
rofi
leS
elf
10–1
5m
inu
tes
Gen
eric
,mu
ltin
atio
nal
,ad
ult
sG
ood
Goo
dN
otre
spon
sive
tosm
all
chan
ges
inh
ealt
h.S
ign
ifica
nt
floo
ref
fect
sP
GI
5m
ost
imp
orta
nt
area
s/ac
tivi
ties
inp
atie
nts
’liv
esth
atar
eaf
fect
edby
thei
rco
nd
itio
n5
item
sin
div
idu
aliz
edIn
div
idu
aliz
ed,f
ree
text
and
0–10
0se
veri
tysc
ale.
Pro
file
and
ind
ex
Sel
f10
–20
min
ute
sG
ener
ic.A
du
lts
Goo
dG
ood
Mix
ed
QW
BS
ymp
tom
s,m
obil
ity,
ph
ysic
alac
tivi
tyan
dso
cial
acti
vity
30it
ems
stat
emen
tsab
out
hea
lth
stat
us
inea
chd
imen
sion
Cla
ssifi
cati
onby
leve
lof
seve
rity
(3le
vels
inea
chd
imen
sion
).In
dex
Inte
rvie
w30
min
ute
sG
ener
ic.A
du
lts
and
chil
dre
nG
ood
Goo
dG
ood
RA
QoL
Act
ivit
ies
ofd
aily
livi
ng,
soci
alin
tera
ctio
n,e
mot
ion
alw
ell-
bein
g,re
lati
onsh
ips
30it
ems
seri
esof
stat
emen
tsab
out
hea
lth
stat
us
Dic
hot
omou
sye
s/n
ore
spon
seto
each
item
(un
wei
ghte
d).
Ind
ex
Sel
f6
min
ute
sD
isea
se-s
pec
ific.
Ad
ult
pat
ien
tsw
ith
RA
Goo
dG
ood
Insu
ffici
ent
dat
a
SF
-36
Ph
ysic
alfu
nct
ion
ing,
role
lim
itat
ion
sd
ue
top
hys
ical
pro
blem
s,bo
dil
yp
ain
,soc
ial
fun
ctio
nin
g,m
enta
lh
ealt
h,r
ole
lim
itat
ion
sd
ue
toem
otio
nal
pro
blem
s,vi
tali
ty,o
vera
ll/g
ener
alh
ealt
h
36it
ems
stan
dar
diz
edqu
esti
ons
3,5,
and
6p
oin
tsc
ales
Pro
file
Sel
for
Inte
rvie
w10
–20
min
ute
sG
ener
ic,m
ult
inat
ion
al,
adu
lts
Goo
dG
ood
Goo
d.F
loor
effe
cts
wit
hso
me
pat
ien
tgr
oup
sS
IPS
leep
and
rest
;eat
ing;
wor
k;h
ome
man
agem
ent;
recr
eati
onan
dp
asti
mes
;am
bula
tion
;mob
ilit
y;bo
dy
care
and
mov
emen
t;so
cial
inte
ract
ion
;ale
rtn
ess
beh
avio
r;em
otio
nal
beh
avio
r;co
mm
un
icat
ion
136
item
sse
ries
ofst
atem
ents
desc
ribi
ngdi
ffere
ntle
vels
ofhe
alth
with
inea
chdi
men
sion
En
dor
sed
stat
emen
ts(w
eigh
ted
).P
rofi
lean
din
dex
Sel
for
Inte
rvie
w20
–30
min
ute
sG
ener
ic,m
ult
inat
ion
al,
adu
lts
Goo
dG
ood
Mix
ed
SIP
-RA
Bod
yca
rean
dm
anag
emen
t;m
obil
ity;
emot
ion
albe
hav
ior;
soci
alin
tera
ctio
n;a
lert
nes
sbe
hav
ior;
com
mu
nic
atio
n;s
leep
and
rest
;hom
em
anag
emen
t;re
crea
tion
and
pas
tim
es;e
atin
g
64ite
ms
seri
esof
stat
emen
tsde
scri
bing
diffe
rent
leve
lsof
heal
thw
ithin
each
dim
ensi
on
En
dor
sed
stat
emen
ts(w
eigh
ted
).P
rofi
lean
din
dex
Sel
for
inte
rvie
w10
–15
min
ute
sD
isea
se-s
pec
ific:
Wom
enw
ith
RA
Insu
ffici
ent
dat
aG
ood
Insu
ffici
ent
dat
a
WH
OQ
OL
Pai
nan
dd
isco
mfo
rt;e
ner
gyan
dfa
tigu
e;se
xual
acti
vity
;sle
epan
dre
st;
sen
sory
fun
ctio
ns;
pos
itiv
efe
elin
gs;t
hin
kin
g,le
arn
ing,
mem
ory
and
con
cen
trat
ion
;sel
f-es
teem
;bod
yim
age
and
app
eara
nce
;neg
ativ
efe
elin
gs;m
obil
ity;
acti
viti
esof
dai
lyli
vin
g;d
epen
den
ceon
med
icat
ion
ortr
eatm
ent;
dep
end
ence
onn
on-m
edic
inal
subs
tan
ces;
com
mu
nic
atio
nca
pac
ity;
wor
kin
gca
pac
ity;
per
son
alre
lati
onsh
ips;
pra
ctic
also
cial
sup
por
t;ac
tivi
ties
asp
rovi
der
;su
pp
orte
r;p
hys
ical
safe
tyan
dse
curi
ty;h
ome
envi
ron
men
t;w
ork
sati
sfac
tion
;fin
anci
alre
sou
rces
;hea
lth
and
soci
alca
re;o
pp
ortu
nit
ies
for
acqu
irin
gn
ewsk
ills
;par
tici
pat
ion
(rec
reat
ion
and
leis
ure
);p
hys
ical
envi
ron
men
ts;
tran
spor
t;sp
irit
ual
ity
281
item
sst
and
ard
ized
ques
tion
s
5-p
oin
tra
tin
gsc
ales
Sel
f20
min
ute
s(w
ell
per
son
)u
pto
1.5
hou
rs(s
ever
ely
ill
per
son
)
Gen
eric
,mu
ltin
atio
nal
,p
atie
nts
and
hea
lth
yp
opu
lati
ons,
adu
lts.
Insu
ffici
ent
dat
aG
ood
Insu
ffici
ent
dat
a
WH
OQ
OL
-10
0P
ain
and
dis
com
fort
;en
ergy
and
fati
gue;
sexu
alac
tivi
ty;s
leep
and
rest
;p
osit
ive
feel
ings
;th
inki
ng,
lear
nin
g,m
emor
yan
dco
nce
ntr
atio
n;s
elf-
este
em;b
ody
imag
ean
dap
pea
ran
ce;n
egat
ive
feel
ings
;mob
ilit
y;ac
tivi
ties
ofd
aily
livi
ng;
dep
end
ence
onm
edic
atio
nor
trea
tmen
t;co
mm
un
icat
ion
cap
acit
y;w
orki
ng
cap
acit
y;p
erso
nal
rela
tion
ship
s;p
ract
ical
soci
alsu
pp
ort;
ph
ysic
alsa
fety
and
secu
rity
;hom
een
viro
nm
ent;
fin
anci
alre
sou
rces
;hea
lth
and
soci
alca
re;o
pp
ortu
nit
ies
for
acqu
irin
gn
ewsk
ills
;par
tici
pat
ion
(rec
reat
ion
and
leis
ure
);p
hys
ical
envi
ron
men
ts;t
ran
spor
t;sp
irit
ual
ity
100
item
sst
and
ard
ized
ques
tion
s
5-p
oin
tra
tin
gsc
ales
Sel
f10
–20
min
ute
sG
ener
ic,m
ult
inat
ion
al,
pat
ien
tsan
dh
ealt
hy
pop
ula
tion
s,ad
ult
s.
Insu
ffici
ent
dat
aG
ood
Insu
ffici
ent
dat
a
WH
OQ
OL
-B
RE
FP
ain
and
dis
com
fort
;en
ergy
and
fati
gue;
sexu
alac
tivi
ty;s
leep
and
rest
;p
osit
ive
feel
ings
;th
inki
ng,
lear
nin
g,m
emor
yan
dco
nce
ntr
atio
n;s
elf-
este
em;b
ody
imag
ean
dap
pea
ran
ce;n
egat
ive
feel
ings
;mob
ilit
y;ac
tivi
ties
ofd
aily
livi
ng;
dep
end
ence
onm
edic
atio
nor
trea
tmen
t;co
mm
un
icat
ion
cap
acit
y;w
orki
ng
cap
acit
y;p
erso
nal
rela
tion
ship
s;p
ract
ical
soci
alsu
pp
ort;
ph
ysic
alsa
fety
and
secu
rity
;hom
een
viro
nm
ent;
fin
anci
alre
sou
rces
;hea
lth
and
soci
alca
re;o
pp
ortu
nit
ies
for
acqu
irin
gn
ewsk
ills
;par
tici
pat
ion
(rec
reat
ion
and
leis
ure
);p
hys
ical
envi
ron
men
ts;t
ran
spor
t;sp
irit
ual
ity
25it
ems
stan
dar
diz
edqu
esti
ons
5-p
oin
tra
tin
gsc
ales
Sel
f10
min
ute
sG
ener
ic,m
ult
inat
ion
al,
pat
ien
tsan
dh
ealt
hy
pop
ula
tion
s,ad
ult
s.
Goo
dG
ood
Goo
d
Adult Quality of Life S133