advances in understanding children with cerebral palsy: risk, resiliency, learning, and independence...
TRANSCRIPT

Advances in Understanding Children with Cerebral Palsy: Risk , Resiliency, Learning, and Independence
Michael E. Msall MDPartnering for ProgressReaching For the Stars
Rehabilitation Institute of Chicago
Saturday August 11, 2007

Neurodevelopmental Disorders(# Children 0-20 Years, POP 80 Million)
Condition Severe Communicative Disorders
Rate Per 1,000 5.0
# Children 400,000
Cognitive-Adaptive DD (IQ <50-55)
5.0 400,000
Cerebral Palsy 2.5 200,000 Autism 2.0 160,000 Hearing Loss (>50db) 2.0 160,000 Visual Loss (<20/200) 0.5 40,000 Technology Dependent 1.0 80,000 Any ND Disorder 20.0 1,600,000

Neurologic and Genetic Disorders(# Children 0-20 Years, POP 80 Million)
Condition Down Syndrome
Rate Per 1,000 1.2
# Children 96,000
Fragile X Syndrome 1.0 80,000 Fetal Alcohol Syndrome 1.0 80,000 Epilepsy 5.0 400,000 Childhood Stroke 0.5 40,000 Muscular Dystrophy 0.5 20,000 Congenital Heart Disease. 7.0 560,000 Any Congenital Disorder 30.0 2,400,000


ICF Model and Cerebral Palsy Health Condition
Cerebral Palsy
Body Function & Structure
Skeletal alignmentRange of motion
Muscle performanceFitness
ActivityMobility
Object manipulationCommunication
Self-carePlaying
ParticipationFamily
FriendshipsDay Care
Child CareRelatives
Environmental Factors
AccessibilityAccommodationPhysical support
Emotional support
Personal FactorsAge
GenderInterests
Self-regulation

Parental Concerns About Function
• Will my child be healthy? • Will my child walk?• Will my child talk?• Will my child learn self care?• Will my child learn at school?

Activities of Daily Living
Basic functions which occur daily
• Self-Care (Feed, dress, groom, bathe)
• Maintaining Continency
• Moving, Changing Positions
• Communication
• Learning
• Problem Solving/Social Interaction
• They have been used developmentally, educationally and in rehabilitation
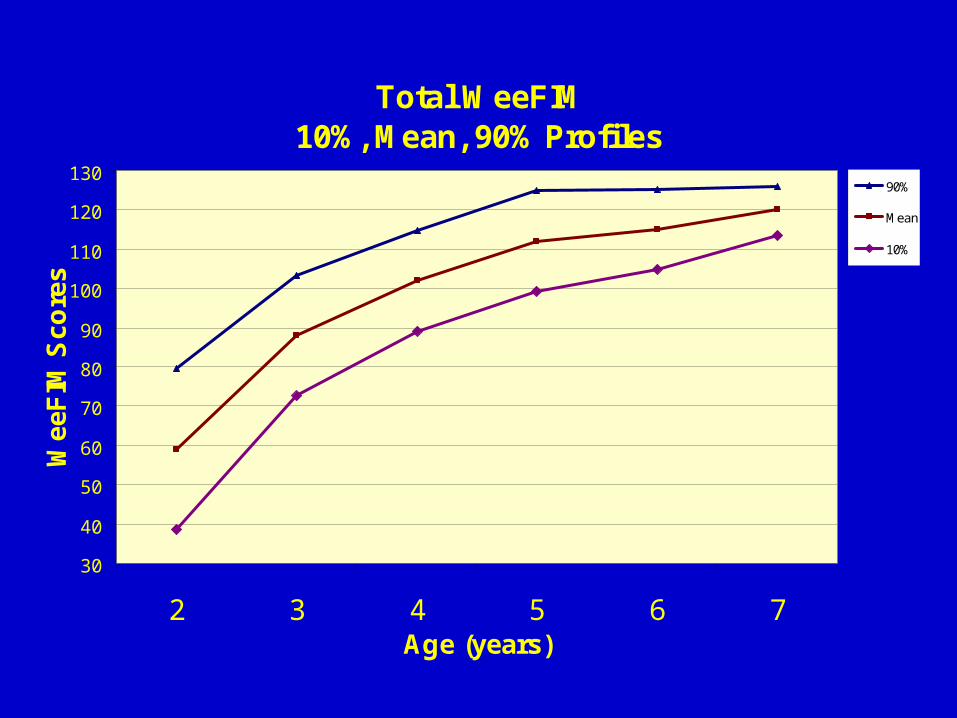
Total WeeFIM10%, Mean, 90% Profiles
30
40
50
60
70
80
90
100
110
120
130
2 3 4 5 6 7Age (years)
Wee
FIM
Sco
res
90%
Mean
10%



1983-86 RCT + Open InfasurfR
24-28 weeksn=194
50 Betamethasone
55 Neither
Kwong, et al. Pediatrics 1985; 76: 585-92 and 1986;78: 767-74
89Surfactant

Neurodevelopmental Impairments
79%
10%0%
1%10%
0%10%20%30%40%50%60%70%80%90%
None CP MR Blind Deaf
Neurodevelopmental morbidity among survivors (N=149). CP = cerebral palsy; MR = mental retardation

Functional Status at Kindergarten Entry
Msall et at. J Perinatology 1994; XIV: 41-47
Walks 150 Feet 97.3%
Talks in Sentences 96.6%
Toilets Self 95.9%
Self-Care/ADL 95.9%

Functional Outcomes and Neurodevelopmental Disability
Walks 150 Feet 87%
Talks in Sentences 84%
Toilets Self 81%
Self-Care/ADL 81%
Understands Request 94%
Msall et at. J Perinatology 1994; XIV: 41-47

Predictors of Functional Disability
• Parenchymal Brain Injury (IVH 3-4, PVL)
• Retinopathy of Prematurity
• Sepsis

Kindergarten Readiness Status
Requirements for special education resources among survivors of extreme prematurity (N=149)
None/At Risk
Some
Intensive41%50%
9%

Predictors of Special Education Resources at Kindergarten Entry
RR 95% CI
Poverty 7.3 2.5 - 21.4
Minority status 2.5 1.2 – 5.3
Male gender 2.4 1.1 – 5.0
Msall et al. AJDC 1992; 146:1371-1375
04/18/23

Spectrum of Gross Motor Function in ELBW
Children with Cerebral Palsy@18Months
Vohr BR, Msall ME, Wilson D, et al.
Pediatrics 2005;116:123-129
Spectrum of Gross Motor Function in ELBW
Children with Cerebral Palsy@18Months

Background and Subjects
• ELBW infants are at high risk of cerebral palsy and neurodevelopmental sequelae.
• Children with cerebral palsy vary in their gross motor performance
• 1860 ELBW infants born between 8/95 and 2/98 evaluated at 18 + 4 months CA.
Vohr, et al., 2005
Background and SubjectsBackground and Subjects

NICHD Network Sites
• Case Western• Wayne State• University of Miami• U of New Mexico• University of Cincinnati• Indiana University• Harvard University• University of Alabama
• Emory University• Univ. of Texas, Dallas• Emory University• U Tennessee, Memphis• Yale University• Stanford University• Brown University• Research Triangle NC
Vohr, et al., 2005

GMFCS @ 18 months
• Level 0: Walks 10 steps independently
• Level 1: Crawls, Pulls to stand, cruises
• Level 2: Sits tripod, creeps
• Level 3: Sits with support
• Level 4: Rolls, good head control
• Level 5: No head control

Cerebral Palsy Status at 18 months
• Cerebral Palsy in 15.2%
• Abnormal Neuro in 7.5%
• Diplegia in 39%
• Quad/Tri in 33%
• Hemi/Mono in 18%
• EPS-Hypotonic in 10%
• Cerebral Palsy in 15.2%
• Diplegia in 39%
• Quad/Tri in 33%
• Hemi/Mono in 18%
• EPS-Hypotonic in 10%

Risk Factors for CP
• Lower GA (p<.0001)
• IVH Grade 3-4 ((p<.001)
• PVL (p<.001)
• NEC (p<.005)
• CLD (p<.001)
• Postnatal steroids (p<.001)
• Outborn (p<.01)
Vohr, et al., 2005

Neurologic Status and GMC
GMC
Tri/Quad Di, hemi, mono
Abn Other
Normal
Normal 1% 11% 44% 96%
I 17% 62% 42% 4%
II 16% 16% 6% 0.3
Vohr, et al., 2005
Neurologic Status and GMC
GMC
Tri/Quad Di, hemi, mono
Abn Other
Normal
Normal 1% 11% 44% 96%
I 17% 62% 42% 4%
II 16% 16% 6% 0.3

Neurologic Status and GMC
GMC Tri/Quad Di, hemi, mono
Abn Other
Normal
III 15% 5% 3% 0.1%
IV 24% 3% 4% 0
V 27% 3% 2% 0
Vohr, et al., 2005

Multiple Disabilities(CP+Blind/DD/HI)
• Normal/Abnormal other 0%
• Monoplegia 64%
• Hemiplegia 55%
• Diplegia 83%
• Triplegia 88%
• Quadriplegia 100%
• EPS Hypotonic 89%

Neurologic Status & MDI (%)
MDI Tri/Quad Di, hemi, mono
Abn Other
Normal
85-115 8 20 19 47
70-84 5 17 28 31
50-69 20 4 32 18
<50 68 28 1 3
<50
Vohr, et al., 2000


Walking at 18 Months
• 99.7% of normals
• 85.9% of other abn neuro
• 73% of di, hemi, monoplegia
• 18% of tri, quadriplegia
Vohr, et al., 2005


04/18/23
Health Status, Functional Limitations, Family Supports and Health Related Quality of Life in
Children with Cerebral PalsyGiles Robinson, Michael E. Msall,
Michelle R. Tremont, Mary Fournier, and Maura Taylor
Brown University and University of Chicago
SDBP Chicago, IL March 17, 2006

Purpose
• To describe medical, developmental, functional and social factors associated with health related quality of life (HRQOL) in children with cerebral palsy

Hypotheses
• Higher levels of functional independence and family supports would be related to higher HRQOL ratings
• Children with more severe cerebral palsy would have lower ratings of health status, functional status, and HRQOL
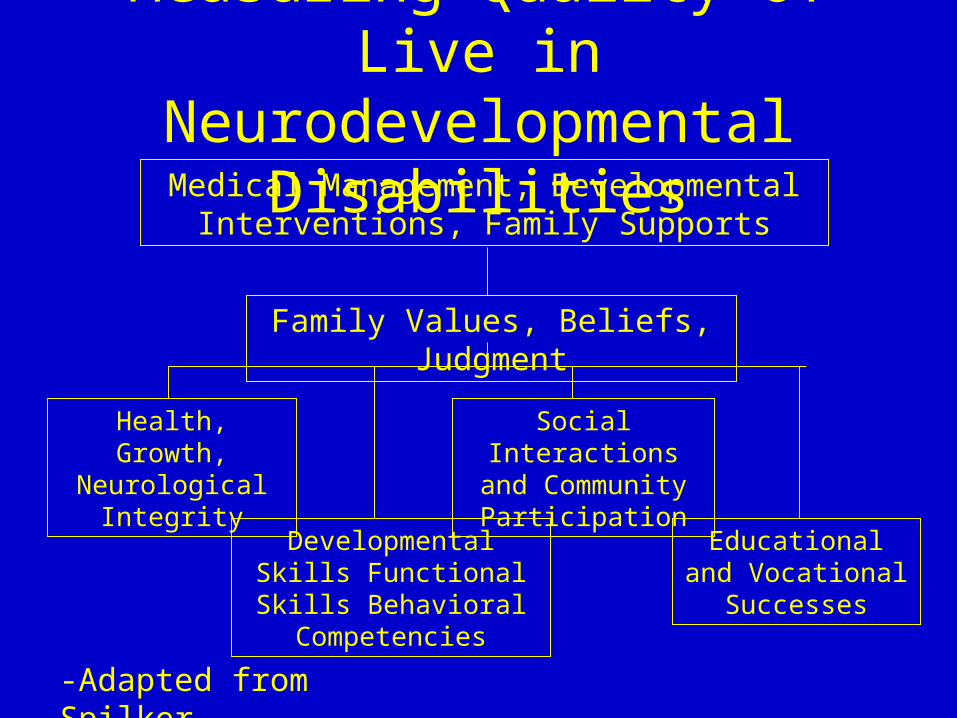
Measuring Quality of Live in Neurodevelopmental Disabilities
Medical Management, Developmental Interventions, Family Supports
Family Values, Beliefs, Judgment
Health, Growth, Neurological
Integrity
Developmental Skills Functional Skills
Behavioral Competencies
Social Interactions and Community
Participation
Educational and Vocational Successes
-Adapted from Spilker

Developmental Status and Support Status Assessments
• Pediatric Functional Independence Measure (WeeFIM)TM self-care, mobility, communication
• Functional Academic Resource Scale (FARS)• Family Support Scale• Support Function Scale• Health Utility Index - 2:
– Sensory, Mobility, Emotion, Cognitive, Self-care, Pain
• Feeling Thermometer

Functional Academic Resource Scale
Describe your child’s abilities in the following areas:Unsupervised play
Making friends with other children
Practical judgment
Following directions and completing chores
Running during a game
Participating in scouts, church, 4-H, band
(1=significantly behind, 3=about same, 5=considerably ahead)
*The higher the score, the greater the friendships, social maturity, and community participation

Quality of Life Rating
• Using hypothetical cases of varying degrees of health status, subject rates the cases and then self on a Feeling Thermometer
• Self rating then becomes the HUI-2 Quality of Life Rating
• Attributes– Sensory, Mobility, Emotion, Cognitive, Self-
care, Pain, Fertility

Hypothetical HUI-2 Cases• Adrian
– Can see, hear, and talk normally
– Can walk, bend, lift, jump, and run normally
– Happy and not worried most of the time
– Learns and does schoolwork normally without special help
– Can eat, bathe, dress, and is continent
– Free of pain
• Freida– Blind, deaf, unable to
talk– No purposeful
movement of arms or legs
– Frequently hospitalized to control anger and irritability
– Unable to learn and remember
– Completely dependent with all self-care tasks
– Frequent pain relieved by prescription narcotics
• Cynthya– Wears glasses but can hear
and speak normally– Walks, bends, and jumps
with limitations, more slowly than others
– Sometimes angry and fearful
– Learns schoolwork very slowly and needs special help
– Eats, bathes, dresses and uses the toilet independently with difficulty
– Free of pain

Feeling ThermometerMost Desirable=100
Least Desirable=0
Self Rating
Cynthya
Adrian
Freida

Pilot Cohort(n=26)
• 89% Caucasian
• 46% Male
• 50% Diplegia
• 31% Hemiplegia
• 19% Quadriplegia
• Mean age=7.9 years

Health Status (CHQ) and Functional Status (WeeFIM), HUI-2 and Severity of Cerebral Palsy
MeanCHQ (SD)
MeanWFQ (SD)
Mean HUI-2(SD)
Di/Hemi(N=21)
79 (13) 79% (19) 84.8(11.5)
Quad(N=5)
66 (12) 40% (24) 60.6(33.7)
p .049 .001 .185CHQ = Child Health Questionnaire Di/Hemi = Diplegia/HemiplegiaWFQ = WeeFIM Quotient Quad = QuadriplegiaHUI-2=Health Utilities Index-2

Family Supports, HUI-2 and Severity of Cerebral Palsy
Mean FSS(SD)
Mean SFS(SD)
Mean HUI-2(SD)
Di/Hemi(N=21)
71.5(15.7)
48.6(8.0)
84.8(11.5)
Quad(N=5)
61.1(1.1)
36.4(4.1)
60.6(33.7)
p .007 .003 .185FSS = Family Support Scale Di/Hemi = Diplegia/HemiplegiaSFS = Support Function Scale Quad = QuadriplegiaHUI-2= Health Utilities Index-2

HUI-2, Friendships and Community Participation (FARS)
0102030405060708090
100
FARS <14 FARS >14
HUI-2
HU
I-2
- F
eeli
ng T
herm
omet
er (
self
)
*P<.05
*
FARS = Functional Academic Resource Scale
N-13 N-11

Functional Status, Friendships, and Community Participation
0102030405060708090
100
FARS <14 FARS >14
WeeFIM Q
Wee
FIM
Tot
al Q
uot
ien
t
*P<.001
*
FARS = Functional Academic Resource Scale
N-13 N-11

Results• Children with higher self reported quality of life (HUI-2) had significantly
more friendships, community participation, and social maturity scores (FARS)
• Children with higher reported quality of life had significantly more family supports
• Children with higher functional status scores (WeeFIM) reported more friendships and social competencies and higher quality of life (HUI-2) ratings
• Children with more severe cerebral palsy have lower health and functional status rating
• No significant difference in HRQOL were found between children with diplegia/hemiplegia versus quadriplegia in this pilot study

Conclusion
• Functional status and community participation are key components of quality of life in children with cerebral palsy
• Explicit measurement strategies for a larger sample is required
• Future research measures should include child’s perception of quality of life

The Myths of Dyslexia
• Mirror writing is a symptom of dyslexia
• Eye training is a treatment for dyslexia
• More boys than girls are dyslexic
• Dyslexia can be outgrown
• Smart people cannot be dyslexic
Shaywitz, Scientific American, Nov. 1996

Clues to Dyslexia in School-Age Children• History
– Delayed language– Problems with the sounds of words– Expressive language difficulties– Difficulty naming– Difficulty learning to associate sounds with letters– History of reading and spelling difficulties in parents and siblings
• Reading– Difficulty decoding single words– Particular difficulty reading nonsense or unfamiliar words– Inaccurate and labored oral reading– Slow reading– Comprehension often superior to isolated decoding skills

Clues to Dyslexia in School-Age Children• Language
– Relatively poor performance on tests of word retrieval– Poor performance on tests of phonologic awareness – Relatively superior performance on tests of word recognition
• Clues most specific to young children at risk for dyslexia– Difficulty with tests assessing knowledge of the names of letters, the ability to
associate sounds with letters, and phonologic awareness
• Clues most specific to bright young adults with dyslexia– Childhood history of reading and spelling difficulties– Accurate but not automatic reading– Slow performance on timed reading tests– Penalized by multiple-choice tests

Lessons from Research
• RD is a language based disorder
• Phonological processing is the key core developmental process
• Reading single words from lists or text is the critical unit of analysis
Lyon GR, Chahabra. MRDD Research Rev 1996;2:2-9.

Phonological Awareness
• The phoneme is the smallest unit of functional sounds
• It can be measured in rhyming tasks*, rapid naming, digit and word span, memory tasks
*the ability of children “to hear” the ‘at’ sound in ‘hat’ and ‘cat’

Significance of Phonology Awareness Difficulties
• Phonological awareness difficulties co-occur with reading disorders and impede the acquisition of reading skills
• Limitations in phonological awareness lead to slow, labored, and inaccurate decoding of words
• Inaccurate decoding leads to poor reading comprehension
• The key to reading intervention is not context or memory, but skills in decoding single words

Intervention
• Phonological deficits can be identified in kindergarten
• Reading is the product of decoding and comprehension
• The fundamental problem is the accurate and fluent identification of words
Gough 1996

Preventive Intervention in Reading Disorders
(N=180)
• Children selected by phonological awareness scores in kindergarten
• Scores predict bottom 10% of children by second grade
• Children had VIQ >75
• Random assignment to 4 curricula

Intervention• Phonological awareness at oral/motor level
plus synthetic phonics (PA+) • Implicit phonological awareness training plus
phonics instruction of reading and spelling (Phonics)
• Regular classroom support groups receiving individual instruction to support classroom reading (Resource)
• No treatment control group (Control)

Intervention (cont.)
• Each instructional group received 20 minutes (4 times) per week one to one supplemental instruction in reading
• Over 2.5 years, 88 hours of supplemental instruction occurred
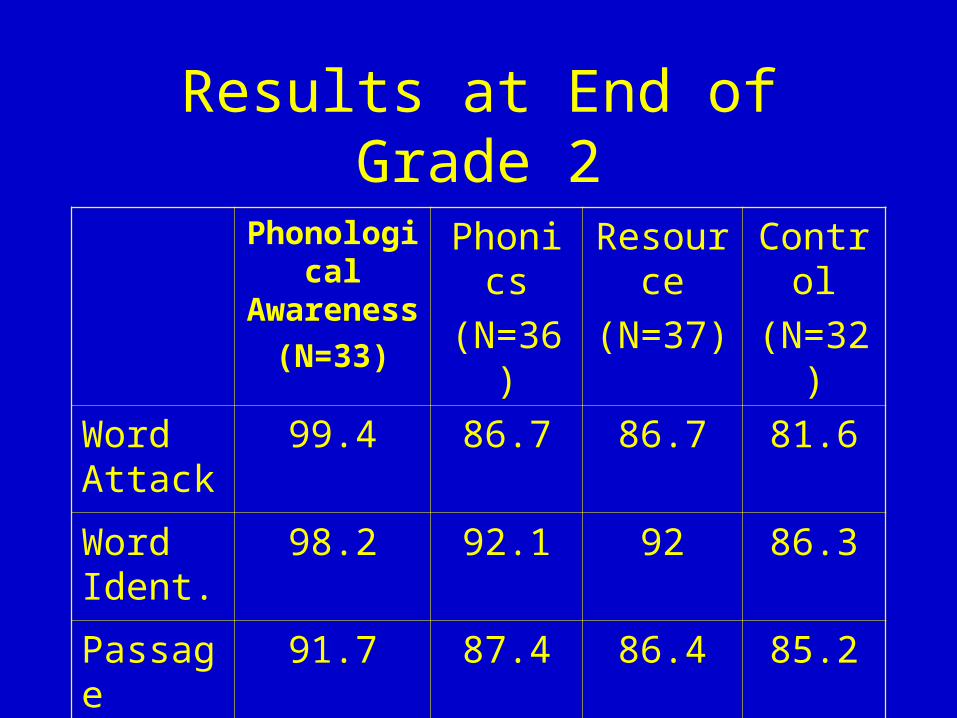
Results at End of Grade 2
Phonological Awareness
(N=33)
Phonics
(N=36)
Resource
(N=37)
Control
(N=32)
Word Attack
99.4 86.7 86.7 81.6
Word Ident.
98.2 92.1 92 86.3
Passage Comp.
91.7 87.4 86.4 85.2

Results at End of Grade 2
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
PA Phonics Resource Control
Grade Retention
Reading Disability and ADHD
• 40% co-morbidity in referred samples
• 15% co-morbidity in non-referred samples
• The impact of ADHD on higher cognitive function is variable with primary impact on rote verbal learning and memory
• ADHD exacerbates the cognitive morbidity of RD

Conclusion
• Common sense holism
• Be careful about grade repetition
• Time on task matters
• Promote prevention, resiliency, and community participation
Section 504 of Rehabilitation Act and IDEA 1997 (PL 105-17)
• School must provide reasonable accommodations and necessary related services and special education supports. Helpful tools include– Peer tutoring– Cooperative learning– Graphic organizers– Study guides– Organizational routines– Learning strategies instruction
Lerner & Yasutaki, pg 476.

Principals of Accommodation
• Recognize individual differences in pacing and cognitive style and promote full inclusion
• ADHD is not an excuse for threatening, noxious, or counterproductive behavior in school or employment
Hinchlaw in Accardo & Whitman, 2000. Pg XV

WWW Resources
• IDEA• Rehab Act 504• Chad.org• Allkindsofminds.org• AACPDM.org
• Nichy.org• Dbppeds.org• Pediatrics.org• Eparent.com• Pathways.org

What We Should Do
Connect the dots: examine the relationship among risk, structural
difference, motor control, and developmental functioning
Evaluate interventions: systematic assessments coupled with safe imaging
and quality habilitative and family supports.
Use the best science to understand potential pathways that would decrease
the functional severity of CP.
Understand the pathways of risk and protection among specific cohorts of
children with one of the CP Syndromes.

Key Points
• All children with cerebral palsy are children first, not a disease
• All children with cerebral palsy learn
• Most important preschool skills are curiosity, communication, hand skills and self-mobility
• Adults with cerebral palsy rank communication, self-care, and education as the most important areas for long term success

04/18/23
Translational Research Opportunities
Critically important to understand biological markers that increase
communicative, behavioral and learning impairments in vulnerable populations
Develop networks and mechanisms for tracking community outcomes for
children receiving neonatal, cardiac, oncological, neurological and genetic
interventions with respect to pathways of risk and resiliency
Optimizing outcomes among children with brain injury whether developmental
or acquired requires quality family, neurodevelopmental and educational
supports that promote functioning and social participation.
Current studies are underway examining transition to adulthood for teenagers
with chronic illness and disability in order to better understand health,
educational, vocational, and independent living outcomes.


Acknowledgments
Supported by 1U01HD37614 entitled “NICHD Family
and Child Well Being Network: Child Disability”.
Irving Harris, Herb Abelson, Paula Jaudes, and Nancy
Schwartz provided support of a shared vision and
commitment to vulnerable populations.
Larry Gray, Peter Smith, Tom Blondis, Shelly Field,
Melissa Gray, Rupa Nimmagada, Dilek Bishku, Jill
Glick, Todd Schuble, Cybele Raver, and Diana Ryan
provided critical feedback.