advancing adjuvant her2- targeted therapyher2 testing in clinical practice: 2007 asco/cap algorithm...
TRANSCRIPT
1
Advancing Adjuvant HER2-Targeted Therapy
Debu Tripathy, MD
Professor of Medicine
University of Southern California
USC/Norris Comprehensive Cancer Center
Ongoing Controversies Regarding Adjuvant Therapy for HER2+ Breast Cancer
• Are anthracylines more effective for higher risk disease?
• Can shorter duration be as effective?
• Is longer duration optimal?
• Should trastuzumab be used for T1a or T1b N0 disease?
New Data from ESMO
• Can trastuzumab be given with single agent paclitaxel or hormonal therapy for low risk disease?
• Are there predictors for cardiac toxicity other than age, hypertension, use of anthracyclines?
• How to handle borderline subnormal and subclinical drops in cardiac ejection fraction
• Predictive factors of response?? (p95, PTEN-, PI3K mutations, MUC4, IGF-1R, HER-3, c-MET)
HER2 Oncogene: A Biological Target
• Increased A iHER2 gene amplification Aggressiveness
• Shortened Survival
• Hormonal Resistance
HER2 protein overexpression
HER2 gene amplification
2
HER1/EGFR
HER2 HER3
HER4
EGF
TGF
AR
HRGHRG
TK
TK
TK
X
HER Family Ligands and Signaling
PI3K/AKTRas/MEK/MAPK
(STAT)
TF
CoACoR
ProliferationMigrationDifferentiationApoptosis
PP
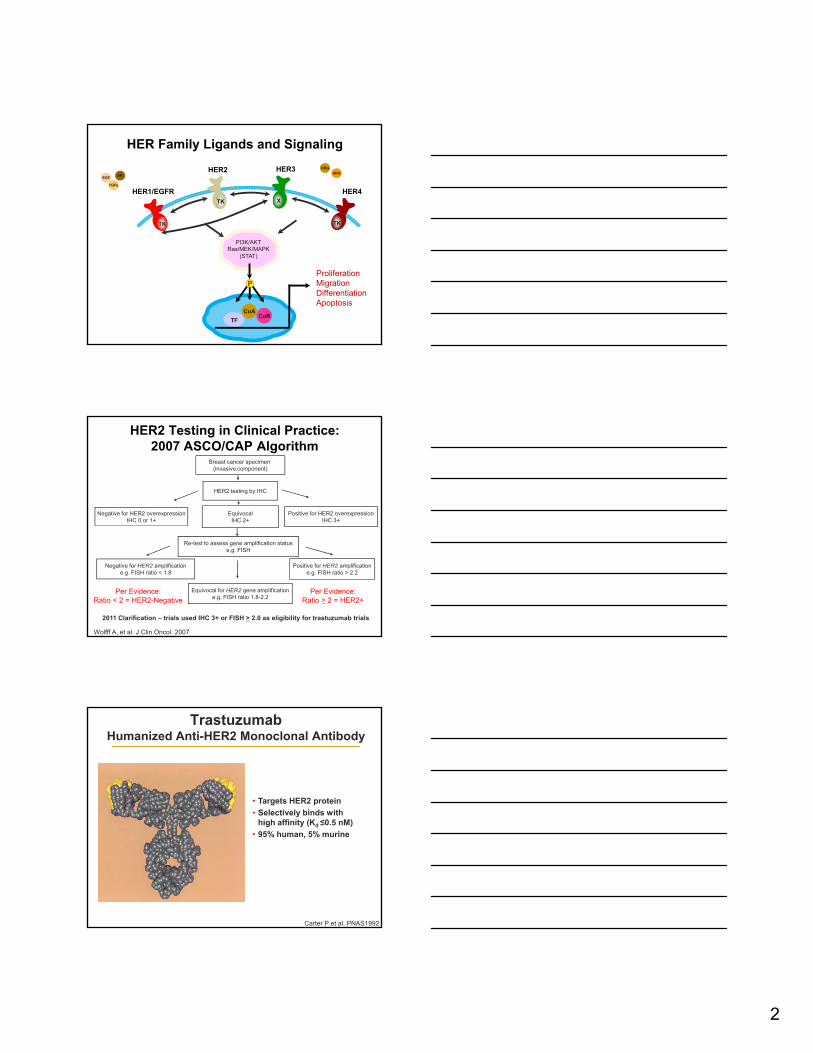
HER2 Testing in Clinical Practice: 2007 ASCO/CAP Algorithm
Breast cancer specimen (invasive component)
HER2 testing by IHC
EquivocalIHC 2+
Negative for HER2 overexpressionIHC 0 or 1+
Positive for HER2 overexpressionIHC 3+
Wolfff A, et al. J Clin Oncol. 2007
Re-test to assess gene amplification statuse.g. FISH
Negative for HER2 amplificatione.g. FISH ratio < 1.8
Positive for HER2 amplificatione.g. FISH ratio > 2.2
Equivocal for HER2 gene amplificatione.g. FISH ratio 1.8-2.2
Per Evidence:Ratio < 2 = HER2-Negative
Per Evidence:Ratio > 2 = HER2+
2011 Clarification – trials used IHC 3+ or FISH > 2.0 as eligibility for trastuzumab trials
TrastuzumabHumanized Anti-HER2 Monoclonal Antibody
• Targets HER2 protein
• Selectively binds with
Carter P et al. PNAS1992
high affinity (Kd ≤0.5 nM)
• 95% human, 5% murine
3
Adjuvant Trastuzumab Trial Designs
Summary of Trastuzumab AdjuvantTrial DFS Benefits
Study FU, yrs N
HERA1 3,387
2 3,401
NSABP B 31/ 2 3 351
HR
0.54
0.64
0.48NSABP B-31/NCCTG 9891
2 3,351
4 3,968
BCIRG 006 3 3,222
FinHer 3 231
PACS 04 4 528
0 1 2In favor of T In favor of Obs.
0.48
0.48
0.61
0.42
0.86
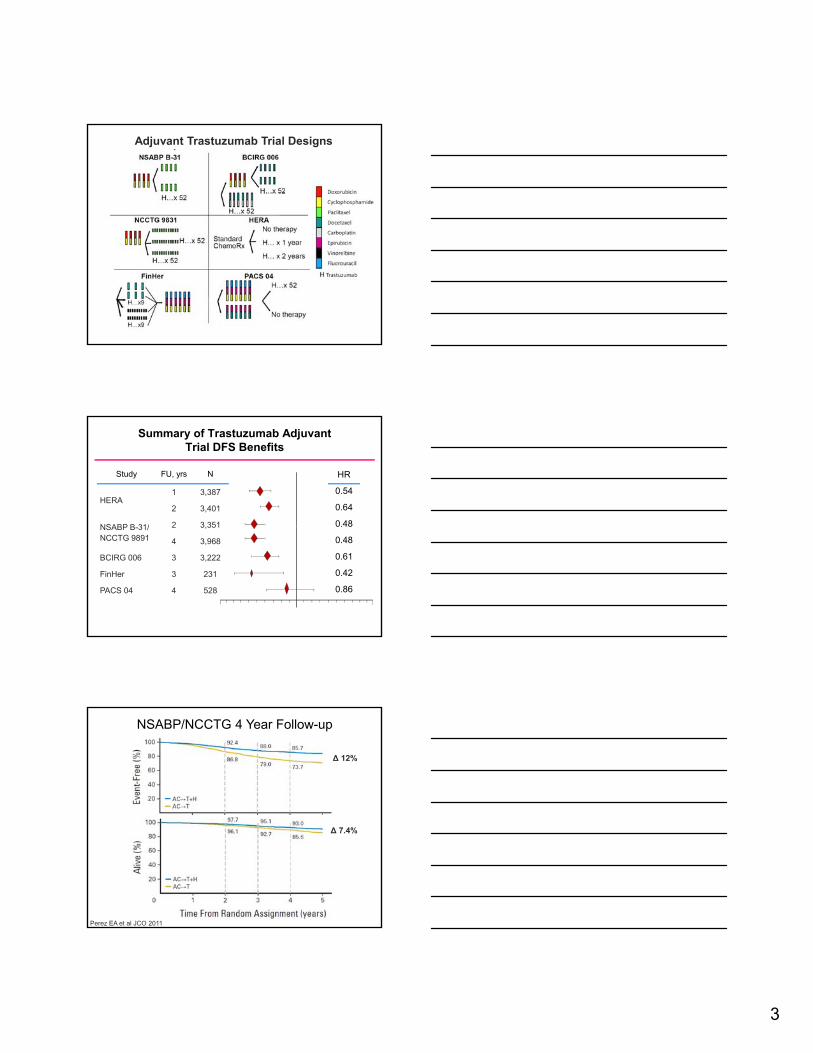
NSABP/NCCTG 4 Year Follow-up
Δ 12%
Δ 7.4%
Perez EA et al JCO 2011
4
Europe, Canada, SA, Australia, NZ (2438) 161 vs 235 0.66 (0.54, 0.81)Asia Pacific, Japan (405) 21 vs 37 0.53 (0.31, 0.90)Eastern Europe (369) 23 vs 36 0.54 (0.32, 0.91)
Region of the world
<35 years (253) 19 vs 31 0.57 (0.32, 1.01)35-49 years (1508) 89 vs 150 0.54 (0.42, 0.70)
Age at randomisation
No. eventsT vs obs
HR (95% CI)Subgroup (no. patients)
Central + South America (189) 13 vs 13 0.98 (0.45, 2.11)
Exploratory DFS Subgroup Analysis (ITT):1 year Trastuzumab vs Observation - HERA Trial
0.0 0.5 1.0 1.5
HR
50-59 years (1096) 71 vs 97 0.71 (0.52, 0.97)>60 years (544) 39 vs 43 0.91 (0.59, 1.41)
Premenopausal (491) 43 vs 49 0.80 (0.53, 1.21)Uncertain (1373) 70 vs 135 0.48 (0.36, 0.64)Postmenopausal (1535) 105 vs 137 0.75 (0.58, 0.97)
Neoadjuvant CT (372) 39 vs 50 0.66 (0.43, 1.00)Negative (1099) 34 vs 58 0.59 (0.39, 0.91)1-3 positive nodes (976) 50 vs 80 0.61 (0.43, 0.87)
Nodal status
Menopausal status at randomisation
>4 positive nodes (953) 95 vs 132 0.64 (0.49, 0.83)All patients (3401) 218 vs 321 0.64 (0.54, 0.76)
HROverall Result
Smith I, et al. Lancet 2007
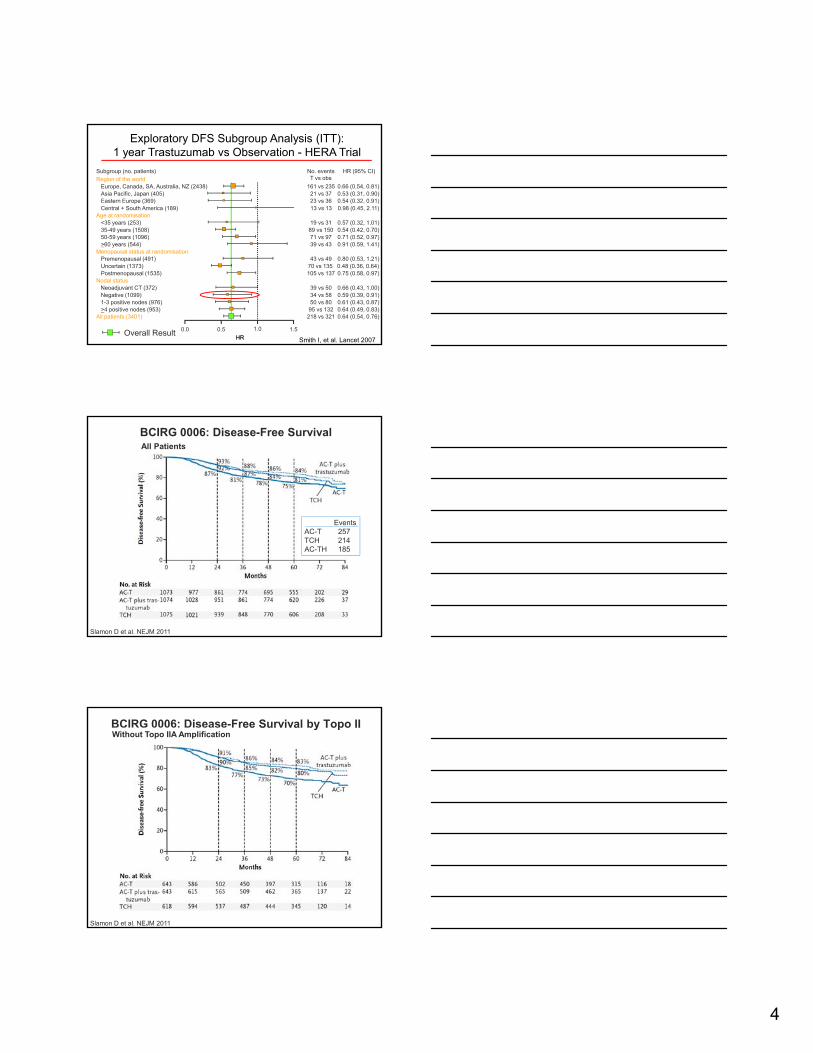
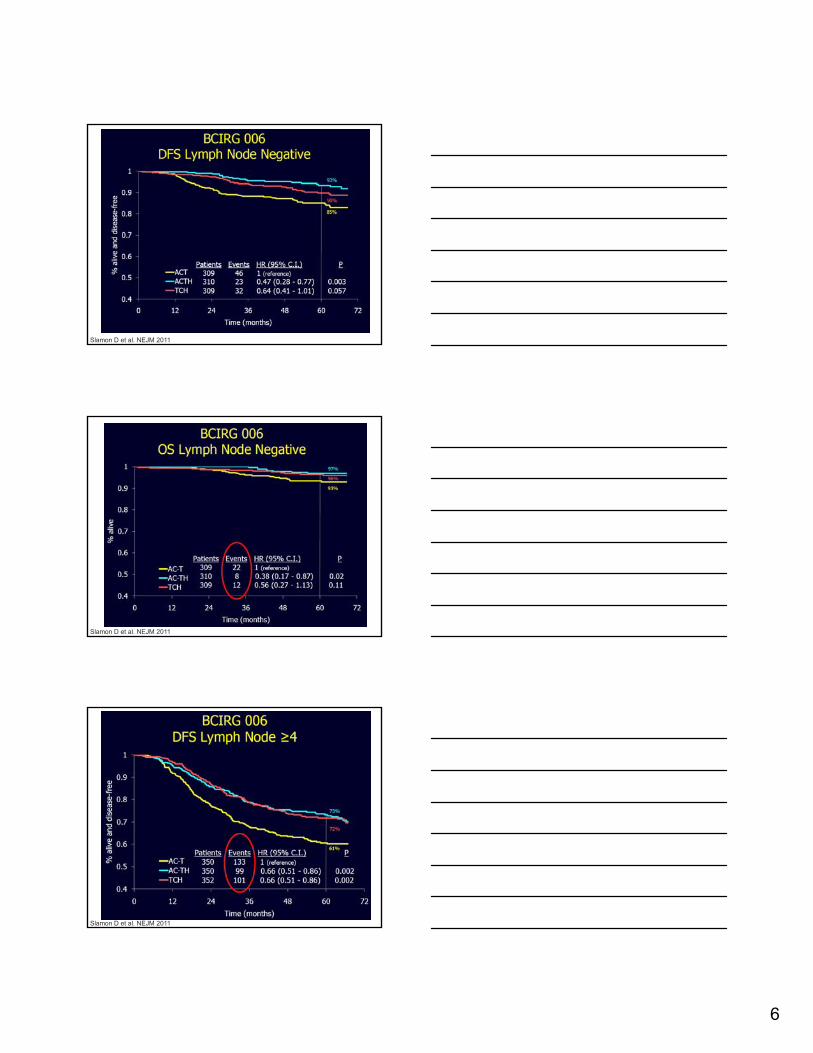
BCIRG 0006: Disease-Free Survival
Events
All Patients
Slamon D et al. NEJM 2011
AC-T 257TCH 214AC-TH 185
BCIRG 0006: Disease-Free Survival by Topo IIWithout Topo IIA Amplification
Slamon D et al. NEJM 2011
5
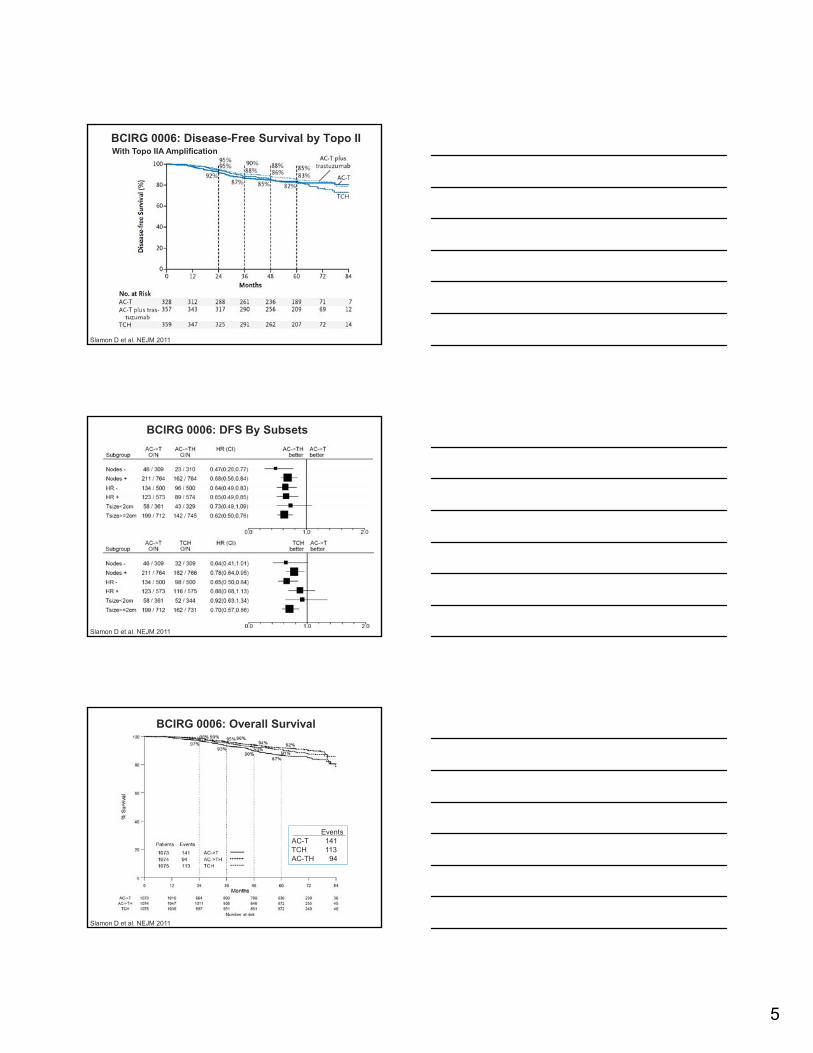
BCIRG 0006: Disease-Free Survival by Topo IIWith Topo IIA Amplification
Slamon D et al. NEJM 2011
BCIRG 0006: DFS By Subsets
Slamon D et al. NEJM 2011
BCIRG 0006: Overall Survival
Slamon D et al. NEJM 2011
EventsAC-T 141TCH 113AC-TH 94
6
Slamon D et al. NEJM 2011
Slamon D et al. NEJM 2011
Slamon D et al. NEJM 2011
7
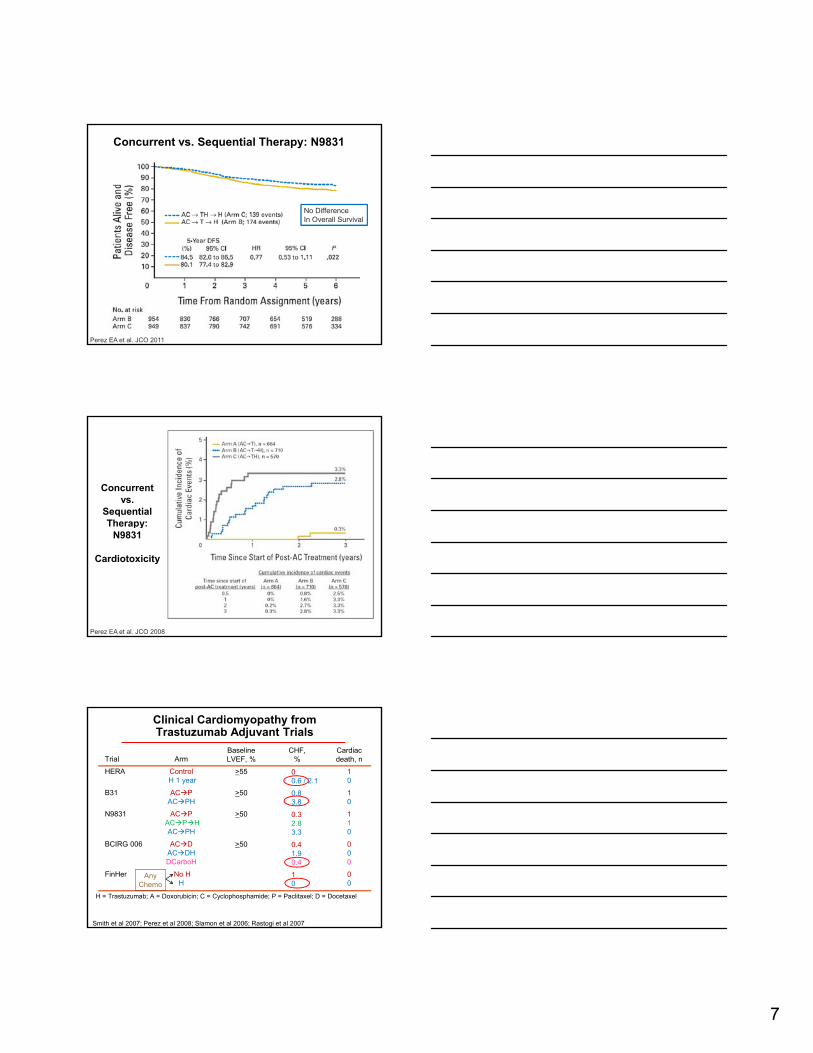
Concurrent vs. Sequential Therapy: N9831
No DifferenceIn Overall Survival
Perez EA et al. JCO 2011
Concurrent vs.
Sequential Therapy:Therapy:
N9831
Cardiotoxicity
Perez EA et al. JCO 2008
Trial
HERA
B31
N9831
Arm
ControlH 1 year
ACPACPH
ACP
BaselineLVEF, %
>55
>50
>50
CHF, %
Cardiacdeath, n
10
10
1
00.6 / 2.1
0.83.8
0.3
Clinical Cardiomyopathy fromTrastuzumab Adjuvant Trials
BCIRG 006
FinHer
ACPHACPH
ACDACDHDCarboH
No HH
>50
10
000
00
Smith et al 2007; Perez et al 2008; Slamon et al 2006; Rastogi et al 2007
2.83.3
0.41.90.4
10
H = Trastuzumab; A = Doxorubicin; C = Cyclophosphamide; P = Paclitaxel; D = Docetaxel
Any Chemo
8
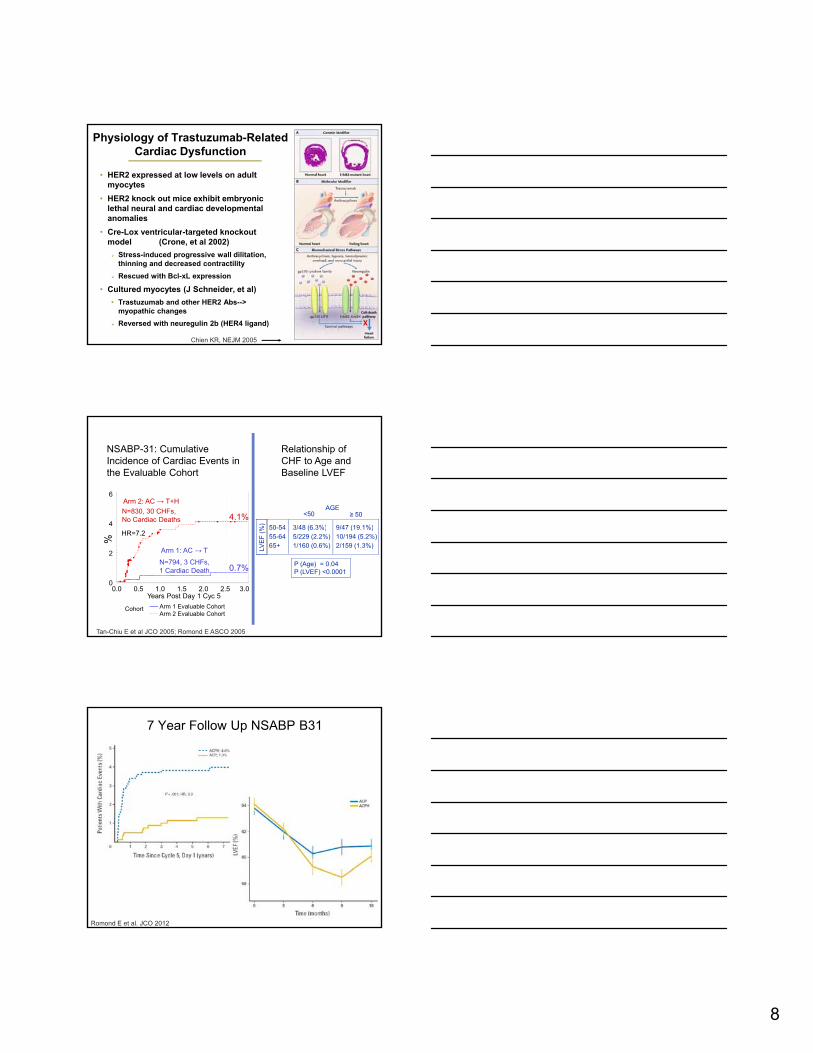
Physiology of Trastuzumab-RelatedCardiac Dysfunction
• HER2 expressed at low levels on adult myocytes
• HER2 knock out mice exhibit embryonic lethal neural and cardiac developmental anomalies
• Cre-Lox ventricular-targeted knockoutCre Lox ventricular targeted knockout model (Crone, et al 2002)
Stress-induced progressive wall dilitation, thinning and decreased contractility
Rescued with Bcl-xL expression
• Cultured myocytes (J Schneider, et al)
• Trastuzumab and other HER2 Abs--> myopathic changes
Reversed with neuregulin 2b (HER4 ligand)
Chien KR, NEJM 2005
4
6
N=830, 30 CHFs,No Cardiac Deaths
NSABP-31: Cumulative Incidence of Cardiac Events in the Evaluable Cohort
4.1%
Arm 2: AC → T+H
3/48 (6 3%) 9/47 (19 1%)
Relationship of CHF to Age and Baseline LVEF
50 54%)
AGE<50 ≥ 50
Tan-Chiu E et al JCO 2005; Romond E ASCO 2005
Cohort Arm 1 Evaluable CohortArm 2 Evaluable Cohort
%
0
2
Years Post Day 1 Cyc 50.0 0.5 1.0 1.5 2.0 2.5 3.0
Arm 1: AC → T
N=794, 3 CHFs, 1 Cardiac Death
HR=7.2
0.7%
3/48 (6.3%)5/229 (2.2%)1/160 (0.6%)
9/47 (19.1%)10/194 (5.2%)2/159 (1.3%)
50-5455-6465+LV
EF
(%
P (Age) = 0.04P (LVEF) <0.0001
7 Year Follow Up NSABP B31
Romond E et al. JCO 2012
9
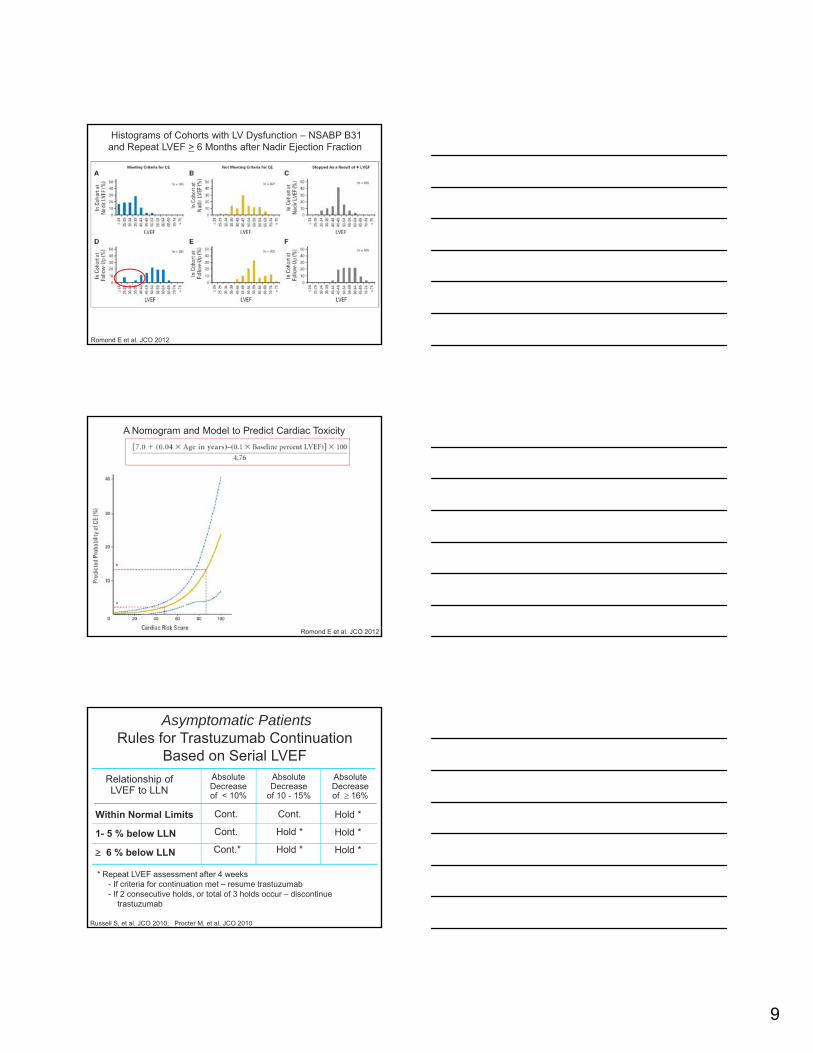
Histograms of Cohorts with LV Dysfunction – NSABP B31and Repeat LVEF > 6 Months after Nadir Ejection Fraction
Romond E et al. JCO 2012
A Nomogram and Model to Predict Cardiac Toxicity
Romond E et al. JCO 2012
Within Normal Limits Cont.
Relationship of LVEF to LLN
Absolute Decreaseof < 10%
Absolute Decrease
of 10 - 15%
Absolute Decrease of 16%
Hold *Cont.
Asymptomatic PatientsRules for Trastuzumab Continuation
Based on Serial LVEF
Within Normal Limits
1- 5 % below LLN
6 % below LLN
Hold *
Hold *
o d
Hold *
Hold *
Cont.
Cont.*
* Repeat LVEF assessment after 4 weeks - If criteria for continuation met – resume trastuzumab - If 2 consecutive holds, or total of 3 holds occur – discontinue
trastuzumab
Russell S, et al. JCO 2010; Procter M, et al. JCO 2010
10
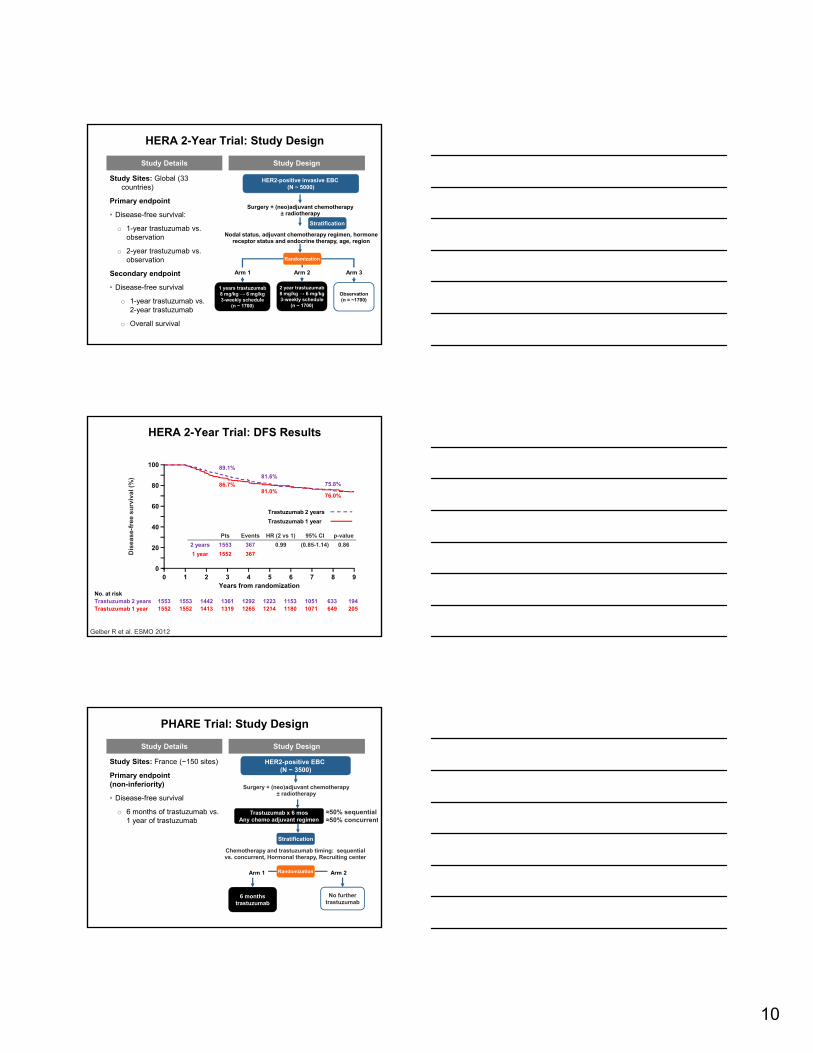
HERA 2-Year Trial: Study Design
Study Sites: Global (33 countries)
Primary endpoint
• Disease-free survival:
o 1-year trastuzumab vs. b ti
Study Details Study Design
Nodal status adjuvant chemotherapy regimen hormone
HER2-positive invasive EBC (N ~ 5000)
Stratification
Surgery + (neo)adjuvant chemotherapy ± radiotherapy
observation
o 2-year trastuzumab vs. observation
Secondary endpoint
• Disease-free survival
o 1-year trastuzumab vs. 2-year trastuzumab
o Overall survival
Nodal status, adjuvant chemotherapy regimen, hormone receptor status and endocrine therapy, age, region
Observation(n = ~1700)
Randomization
1 years trastuzumab8 mg/kg → 6 mg/kg3-weekly schedule
(n ~ 1700)
2 year trastuzumab8 mg/kg → 6 mg/kg3-weekly schedule
(n ~ 1700)
Arm 2Arm 1 Arm 3
fre
e s
urv
iva
l (%
)
89.1%
86.7%81.0%
81.6%75.8%
76.0%
100
80
60
40Trastuzumab 1 year
Trastuzumab 2 years
HERA 2-Year Trial: DFS Results
Dis
ea
se
-f
Years from randomization
40
20
00 1 2 3 4 5 6 7 8 9
No. at riskTrastuzumab 2 years 1553 1553 1442 1361 1292 1223 1153 1051 633 194Trastuzumab 1 year 1552 1552 1413 1319 1265 1214 1180 1071 649 205
Pts Events HR (2 vs 1) 95% CI p-value
2 years 1553 367 0.99 (0.85-1.14) 0.86
1 year 1552 367
Gelber R et al. ESMO 2012
PHARE Trial: Study Design
HER2-positive EBC (N ~ 3500)
Trastuzumab x 6 mosA h dj t i
Study Sites: France (~150 sites)
Primary endpoint (non-inferiority)
• Disease-free survival
o 6 months of trastuzumab vs. 1 f b
Surgery + (neo)adjuvant chemotherapy ± radiotherapy
Study Details Study Design
≈50% sequential50% tAny chemo adjuvant regimen
Chemotherapy and trastuzumab timing: sequential vs. concurrent, Hormonal therapy, Recruiting center
Stratification
Randomization
No further trastuzumab
6 months trastuzumab
1 year of trastuzumab
Arm 1 Arm 2
≈50% concurrent
11
0 25
0.50
0.75
1.00
Pro
bab
ility
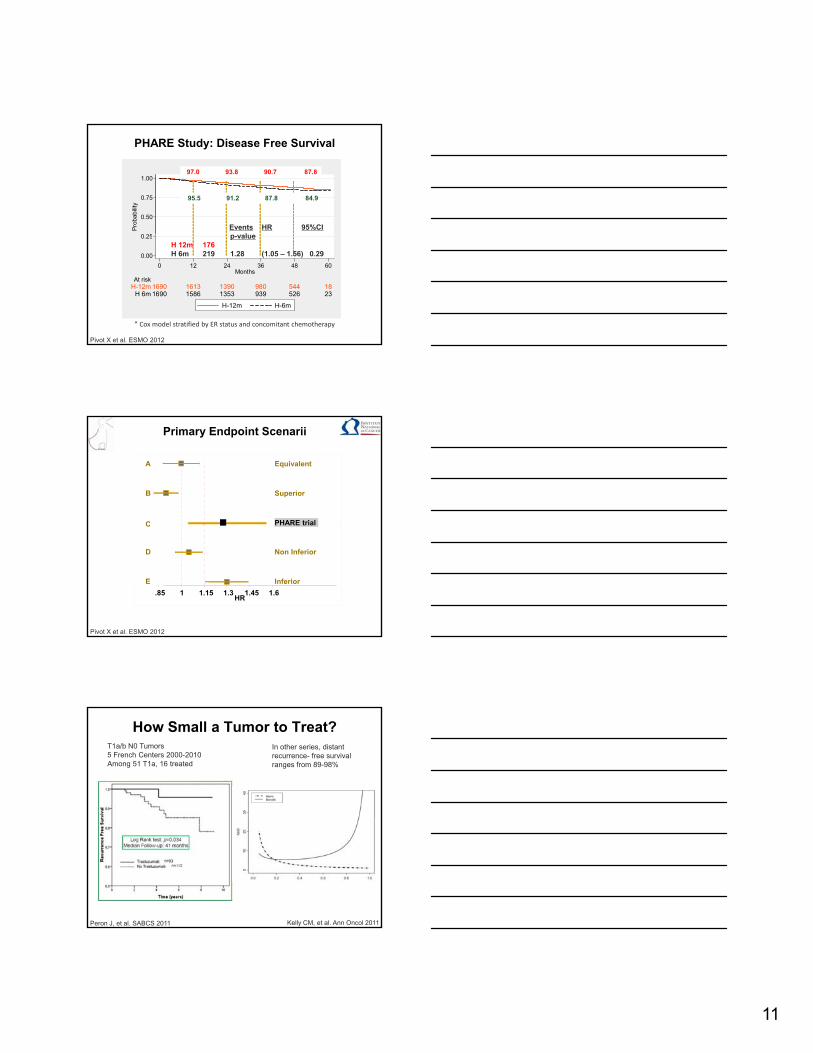
PHARE Study: Disease Free Survival
95.5 91.2 87.8 84.9
97.0 93.8 90.7 87.8
Events HR 95%CIl
0.00
0.25
1690 1586 1353 939 526 23H 6m1690 1613 1390 980 544 18H-12m
At risk
0 12 24 36 48 60Months
H-12m H-6m
* Cox model stratified by ER status and concomitant chemotherapy
p-valueH 12m 176H 6m 219 1.28 (1.05 – 1.56) 0.29
Pivot X et al. ESMO 2012
Equivalent
Superior
A
B
C
Primary Endpoint Scenarii
PHARE trial
Non Inferior
Inferior
C
D
E
.85 1 1.15 1.3 1.45 1.6HR
Pivot X et al. ESMO 2012
How Small a Tumor to Treat?T1a/b N0 Tumors5 French Centers 2000-2010Among 51 T1a, 16 treated
In other series, distant recurrence- free survival ranges from 89-98%
Peron J, et al. SABCS 2011 Kelly CM, et al. Ann Oncol 2011
12
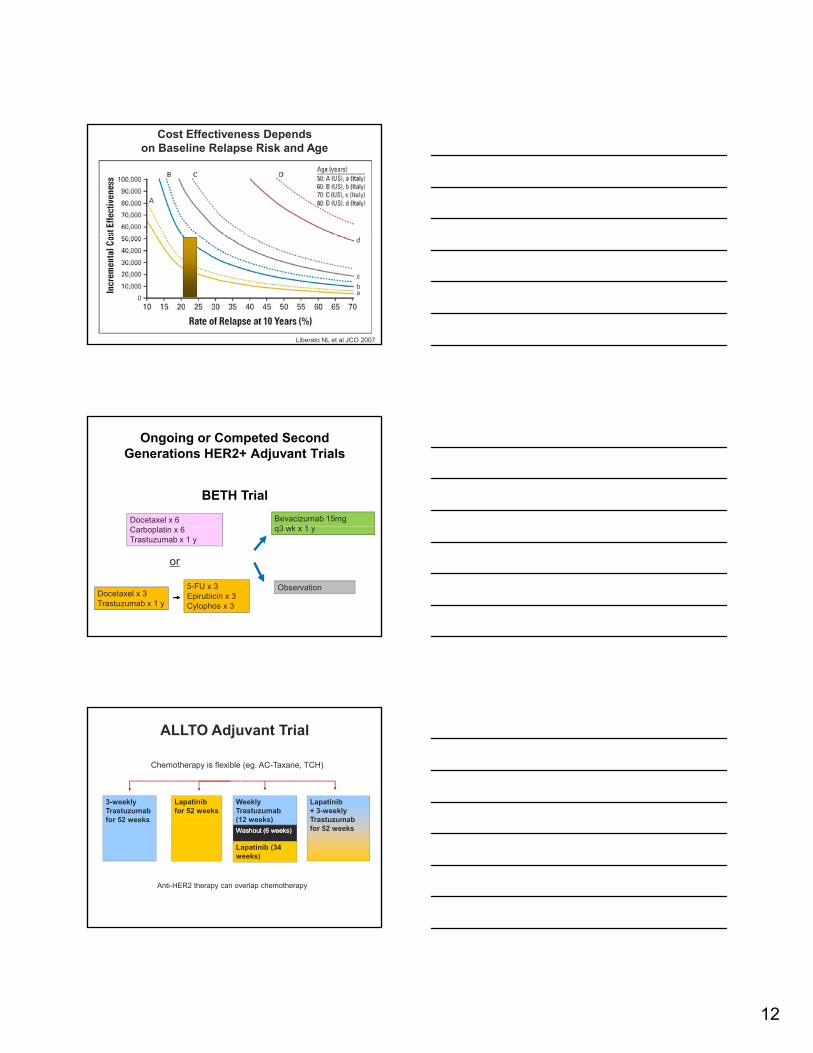
Cost Effectiveness Dependson Baseline Relapse Risk and Age
Liberato NL et al JCO 2007
Ongoing or Competed Second Generations HER2+ Adjuvant Trials
Docetaxel x 6 Bevacizumab 15mg 3 k 1
BETH Trial
Carboplatin x 6Trastuzumab x 1 y
Docetaxel x 3Trastuzumab x 1 y
5-FU x 3Epirubicin x 3Cylophos x 3
or
q3 wk x 1 y
Observation
ALLTO Adjuvant Trial
3-weeklyTrastuzumabf 52 k
Lapatinibfor 52 weeks
WeeklyTrastuzumab (12 k )
Lapatinib + 3-weeklyT t b
Chemotherapy is flexible (eg. AC-Taxane, TCH)
for 52 weeks (12 weeks) Trastuzumab for 52 weeksWashout (6 weeks)Washout (6 weeks)
Lapatinib (34 weeks)
Anti-HER2 therapy can overlap chemotherapyAnti-HER2 therapy can overlap chemotherapy
13
Aphinity Adjuvant Trial
6-8 cycles of Anthracycline or non-
th li th
Trastuzumab x 52 weeks
anthracyline therapy
Trastuzumab +Pertuzumab x 52 weeks
Even Further in the Future: T-DM1, mTOR inhibitors, PI3K inhibitors, HER2/3 bispecific antibodies, heat shock/chaperone inhibitors
Personalizing CombinatorialTherapy for HER+ Breast Cancer
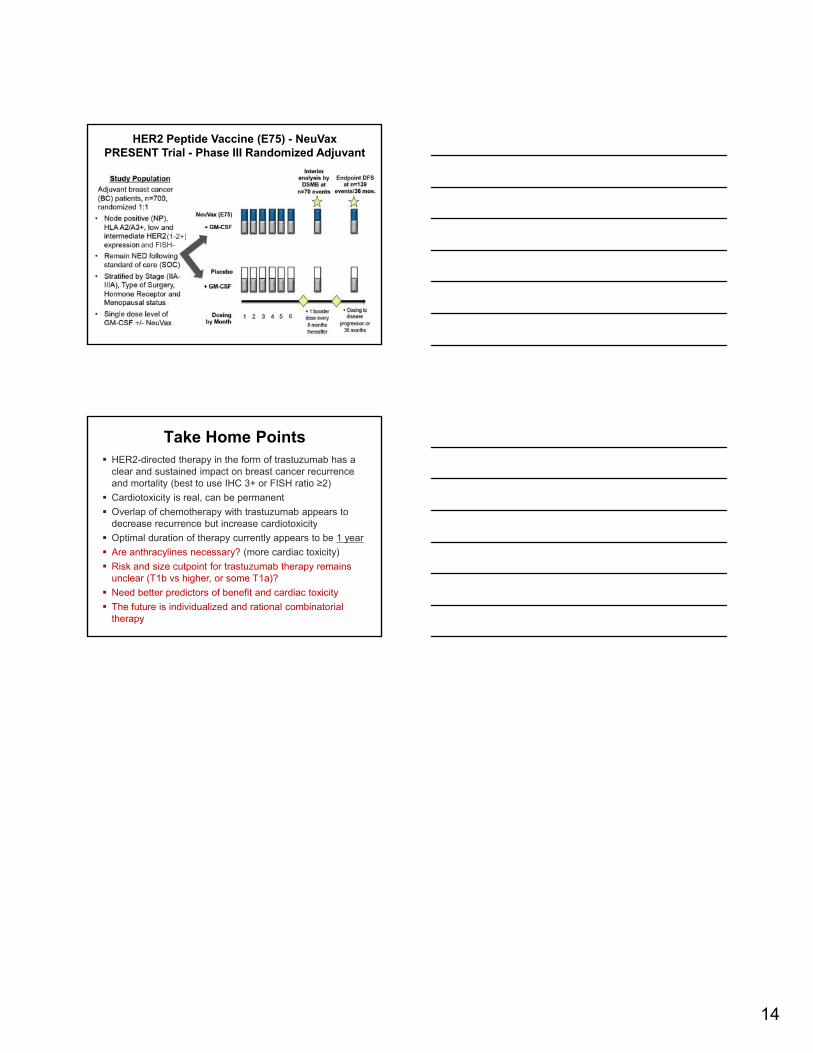
• E75 = immunogenic peptide (aa 369-377) of the HER2 protein
• 6 cycles monthly intradermal E75 with GM-CSF (250 mcg)
• Combined analysis of 2 trials• Trial 1: dose-escalation
trial of node+ pts with BC
HER2 Peptide Vaccine (E75)In Early Stage Breast Cancer – Non randomized
Mittendorf EA, Peoples GE et al. Cancer 2012
p• Trial 2: dose-optimization
trial of node- pts with BC)• Median F/U = 24 mo.• N = 186
• E75 vaccine = 106 (HLAA2/A3+)
• Controls = 76 (HLAA2/A3-)
• 26% HER2+
14
HER2 Peptide Vaccine (E75) - NeuVaxPRESENT Trial - Phase III Randomized Adjuvant
(1 2 )and FISH-
(1-2+)
Take Home Points HER2-directed therapy in the form of trastuzumab has a
clear and sustained impact on breast cancer recurrence and mortality (best to use IHC 3+ or FISH ratio ≥2)
Cardiotoxicity is real, can be permanent
Overlap of chemotherapy with trastuzumab appears to decrease recurrence but increase cardiotoxicitydecrease recurrence but increase cardiotoxicity
Optimal duration of therapy currently appears to be 1 year
Are anthracylines necessary? (more cardiac toxicity)
Risk and size cutpoint for trastuzumab therapy remains unclear (T1b vs higher, or some T1a)?
Need better predictors of benefit and cardiac toxicity
The future is individualized and rational combinatorial therapy