advancing care models for children with complex medical ... · advancing care models for children...
TRANSCRIPT
On the vanguard of thought. On the front lines of ac�on.
W H I T E P A P E R
Five Keys to Success: Advancing Care Models for Children with Complex Medical Needs
Authors: James Karpook and Mark Werner, MD

Page i
Table of Contents
The Challenge of Delivering and Managing Care ...................................................... 1
Children’s Hospitals Leading the Way ...................................................................... 2
New Models for Coordinating and Delivering Care: The Complex Care Team ................. 3
Addressing the Full Spectrum of Patient and Family Needs ........................................ 5
Key Requirements for Success .............................................................................. 8
Meeting the Challenge .........................................................................................10
For More Information ..........................................................................................11

Advancing Care Models for Children with Complex Medical Needs
Page 1
In the United States, approximately one in 25 children is considered “medically complex,” challenged with multi ple, chronic, severe health conditi ons and requiring substanti al medical and psychosocial support. The number of children with complex medical needs is expected to double in the next decade – increasing from three to six million – as advances in medicine and technology reduce mortality rates.1 These children typically require ongoing care provided by numerous pediatric specialists, many found only in pediatric centers of excellence, as well as access to services and providers found outside the healthcare system. Families oft en travel long distances for specialized diagnosti c and treatment services, and assume much of the responsibility for care coordinati on and communicati on among and between providers, without the benefi t of a comprehensive care plan. The stress, strain and cost of navigati ng, managing and coordinati ng their child’s care within a fragmented health delivery and fi nancing system is a signifi cant part of the total burden of care to the family and the healthcare system.
The number of children with complex medical needs is expected to double in the next decade.
The cost of providing care to children with medical complexity is esti mated to be as much as 10 ti mes the costs for other children.2 Approximately two-thirds of these children are covered by Medicaid, and esti mates suggest this populati on accounts for more than 40% of Medicaid’s total spending on children. The highest area of medical expense is associated with inpati ent care, which accounts for as much as 80% of the total healthcare cost. While only 4% of the total pediatric populati on, these children represent approximately 10% of admissions to children’s hospitals, 25% of pati ent days and 40% to 50% of hospital charges.3 The fi nancial impact on families is also signifi cant; a nati onal survey reported that more than half of the families of children with special healthcare needs experience fi nancial hardship or had a family member stop working to care for their child.4
As the focal point for care, leading children’s hospitals are launching new clinical, operati ng and care management models designed to support bett er coordinati on and delivery of care across the conti nuum of inpati ent, outpati ent and community-based services. These models promote engagement and alignment of primary and specialty care physicians, other clinicians, pati ents and their families around a comprehensive plan of care with clearly defi ned outcomes and accountabiliti es that addresses medical and social needs and resource requirements to achieve opti mal health status and quality of life. Importantly, they address the full spectrum of pati ent and family needs, defi ning the approaches to managing these children from the ti me they are on-boarded into the program, through transiti on to adulthood. This paper will explore the power of a comprehensive program for children with medically complex needs, and share the experiences and lessons learned from several leading children’s hospitals in designing and implementi ng these targeted programs to advance the care and support of pati ents and their families.
The Challenge of Delivering and Managing Care Pati ents with multi ple acute and chronic illnesses and comorbiditi es require extraordinary levels of coordinati on among primary care physicians (PCPs) and specialists, including hospitalists who oft en manage the inpati ent care. Primary care practi ces are organized to address preventi on and wellness and manage acute needs of generally healthy children. Primary care physicians may face challenges with inadequate ti me and reimbursement for children with greater needs, and most practi ces do not have suffi cient care coordinati on support to help pati ents and their families navigate the myriad of specialty care services required. Oft en, PCPs will quickly refer more complex cases to specialists, where

Advancing Care Models for Children with Complex Medical Needs
Page 2
they consume a large percentage of those physicians’ capacity and challenge their ability to meet the ambulatory and inpati ent needs of the broader pediatric populati on. Children’s hospitals oft en face challenges managing the emergent medical needs and inpati ent care delivery of this populati on, including ensuring the opti mal service assignment, communicati ng and coordinati ng care among services, and providing comprehensive post-discharge planning and educati on. Many hospital and practi ce-based care coordinati on services do not have suffi cient knowledge of community-based resources that can provide additi onal support and improve the quality of life for pati ents and their families.
Oft en, there is no comprehensive plan of care to provide caregivers with an overall picture of the pati ents’ full spectrum of health issues, or to support pati ents and families in health maintenance and anti cipati on of future healthcare needs. Even when a plan of care is in place, communicati ng to the numerous care team members and sharing informati on across practi ces and inpati ent setti ngs can be an enormous challenge. Further, the nature of these pati ents’ clinical conditi ons makes care planning complicated and ti me consuming, and oft en results in plans of care that can be diffi cult to understand or navigate. In their desire to bett er meet the needs of pati ents, providers will oft en look to familiar resources to address perceived gaps in care and reduce the burden on pati ents and their families. At ti mes, this leads to ineffi cient and unnecessary deployment of high cost resources to address perceived needs. For example, physicians may refer pati ents to home care services to monitor the pati ents’ clinical conditi on or to address basic needs and acti viti es of daily living which could be supported by less expensive technology or community-based resources.
Children’s Hospitals Leading the WayAcross the country, leading children’s hospitals have developed new specialized programs and approaches to bett er serve children with complex medical needs and reduce the burden on pati ents and their families. The success of these programs is founded on greater engagement and alignment of families and interdisciplinary care teams in developing comprehensive plans of care that address current and anti cipated future medical needs, as well as the personal and social factors that aff ect quality of life. Central to these plans is the defi niti on of broad-based clinical and non-clinical outcome goals, including achieving opti mal health status while maintaining independence in the least restricti ve environment possible. To achieve these goals, programs are designed to support greater integrati on and collaborati on among health, educati on and other social systems that together enable children with medical complexity to achieve physical well-being, meaningful social interacti ons, individualized educati on and training, and opti mal quality of life.
Evidence shows that many of these programs have achieved material improvements in both clinical quality and cost through bett er care planning and coordinati on as well as more proacti ve preventi ve care. A review of 12 leading studies esti mated that bett er care coordinati on and the creati on of specialty medical homes for children with complex medical needs could reduce uti lizati on of inpati ent and emergency department use by 40% and 20% respecti vely.5 Another recent study compared outcomes for high-risk children with chronic illness who were treated at a comprehensive care clinic at the University of Texas, Houston, to those treated at private offi ces or faculty-supervised clinics. The study showed a decrease of 55% in the number of children with a serious illness for those treated at the high risk clinic, as compared to “usual care,” and a reducti on of total hospital and clinic costs from approximately $27,000 to roughly $17,000 per year.6 Similar results have been achieved at a number of other children’s hospitals aft er the opening of comprehensive care clinics for medically complex kids. Arkansas Children’s saw a decrease in the monthly Medicaid costs per pati ent from approximately $4,700 to a litt le over $3,500 in just one year following the pati ent’s fi rst visit to the comprehensive care clinic, driven by reducti ons in uti lizati on of inpati ent and emergency services.7 At Primary Children’s Medical Center, the comprehensive outpati ent program for children with medical and psychosocial

Advancing Care Models for Children with Complex Medical Needs
Page 3
complexity, fragility and technology dependence delivered improvements in pati ent and family sati sfacti on as well as health outcomes and cost: over 85% of parents expressed agreement with the statement, “I receive exactly what I want and need, exactly when and how I want and need it.”8
Increasingly, children’s hospitals are being asked to demonstrate their ability to improve outcomes, manage clinical variati on, and reduce total cost of care for medically complex pati ents as a criti cal value propositi on to their communiti es. This value propositi on is being put to the test by new narrow networks and ACO products which require children’s hospitals to demonstrate diff erenti ati ng levels of value, or be excluded. Many children’s hospitals have approached the management of children with medical complexity as an opportunity to advance their journey to value by focusing on a populati on with signifi cant opportunity for quality and cost improvement. A number of programs and pilots have been launched in partnership with state Medicaid programs and commercial payors who recognize the opportunity to collaborate with children’s hospitals to reduce total cost of care and improve outcomes. As the payment environment conti nues to shift from fee-for-service to more value-based models, children’s hospitals have also found that the experience of managing this populati on can help build new organizati onal capacity and capabiliti es that support broader populati on health management goals.
New Models for Coordinati ng and Delivering Care: The Complex Care TeamLeading children’s hospitals are developing new models to address the unique clinical and social needs of this populati on. These models diff er in terms of clinical scope and size of the populati on served, with some designed to manage large populati ons of Medicaid pati ents using a broad clinical defi niti on of medical complexity (e.g., using all pati ents with CRG 5b through 9), and others focused on the most expensive and highest uti lizers of services. Some programs exclude pati ents who are supported by other multi -specialty care management programs, for example transplant and cancer. A few programs include siblings of pati ents with complex medical needs as a means of providing additi onal support to families. Despite diff erences, these programs share a common goal of enhancing support to care teams, pati ents and families in care planning and delivery, communicati on and transiti on management across providers and setti ngs, and access to community-based services.
Most programs have a dedicated Complex Care Team that includes physicians, nurses, case managers, social workers and non-licensed workers who play an acti ve role in non-clinical aspects of care coordinati on, including liaising with community resources, scheduling appointments and arranging transportati on. Some programs include mental health professionals, pharmacists, nutriti onists and palliati ve care specialists. One key diff erence among programs is the relati onship between the Complex Care Team and the pati ents’ primary care physician or medical home. In some cases, PCPs retain their relati onships with their pati ents, providing a full-range of preventi on and wellness services, as well as coordinati ng specialty and complex care needs. In other cases, the Complex Care Team becomes the medical home, assuming responsibility for comprehensive management of clinical needs across the conti nuum. Some programs use a hybrid approach. The three diff erent models are illustrated below:

Advancing Care Models for Children with Complex Medical Needs
Page 4
• Some patients retain their primary care physician as their medical home while others utilize the Complex Care Team as their medical home
• Where PCP relationship is retained, Complex Care Team operates as in Consultative Model
• As in the Consultative Model, the Complex Care Team consults with PCPs and specialists to support care planning, and rounds on inpatients
• Some patients retain
2
Care Team Model and Care Management Approach
• Patients retain relationship with their primary care physician as the medical home
• The PCP-based medical home provides all essential routine and well-care services and supports the coordination of care for specialty and chronic care needs
• Complex Care Team consults with the PCPs to support care planning, coordinate complex medical needs and support transitions across care settings
• Complex Care Team rounds on patients when admitted to the hospital to support coordination of care and communication among specialists and PCPs
1• Complex Care Team becomes the medical home providing the
full range of services including prevention and well-care, and coordination of care for all chronic and complex needs
• Complex Care Team provides care in both the ambulatory and inpatient settings on either a rotational basis or using separate teams
• Complex Care Team works closely with specialists in care planning and coordination
• Patients requiring hospitalization may be admitted to a dedicated complex care unit or a specialty care unit; Complex Care Team rounds on inpatients
Medical Home Model
Consultative Model
3
Hybrid Model

Advancing Care Models for Children with Complex Medical Needs
Page 5
Diff erences in approach are oft en driven by the relati onship of the children’s hospital to the primary care physicians; organizati ons with a largely independent primary care base typically develop programs with a “consultati ve model,” while organizati ons with a largely employed primary care base more oft en use the “medical home model.” The approach may also refl ect the primary care physicians’ capacity and comfort with management of this populati on. Reimbursement challenges, the need for longer visit ti mes, challenges in care planning and signifi cant care coordinati on needs with limited resources someti mes results in primary care physicians transiti oning the relati onship with pati ents and families to the Complex Care Team.
Regardless of the approach and model selected, programs must carefully defi ne the roles for the primary care physicians and Complex Care Team. Families should understand these roles and have clarity around the point of contact for routi ne pediatric primary care, urgent and emergent care, and general medical questi ons related to health maintenance or exacerbati on of underlying medical conditi ons. Families should also understand the role of the Complex Care Team in supporti ng access to services outside the healthcare system. Parti cularly in the hybrid model, the Complex Care Team must have clarity around their relati onship with each pati ent, and ensure that they are managing the full conti nuum of needs of those children for whom they are the medical home, while coordinati ng with and supporti ng PCPs for care of the other children.
For hospitals who have or are engaged in developing a clinically integrated network (CIN), the approach used for managing medically complex kids must be aligned with the CIN’s clinical operati ng model and approach to care management. Specifi cally, the roles and responsibiliti es of the Complex Care Team should be synergisti c with the CIN’s approach to care management, transiti ons in care management, use of community health workers and social workers as examples. The assignment of accountability as a pediatric medical home for these children has implicati ons for providers’ roles in achieving quality and cost improvement consistent with the general pediatric and specialty measures established by the CIN. Developing consensus among physicians and creati ng a shared understanding of the requirements for demonstrati ng value can be complicated with the shift in relati onships and accountability inherent in a new model for managing the care for these children.
Addressing the Full Spectrum of Pati ent and Family NeedsRegardless of the model selected, successful care management should be organized to address the full spectrum of pati ents’ and families’ needs – both medical and non-medical – across the conti nuum from pati ent onboarding through the transiti on to adulthood. Clearly arti culated processes will need to be defi ned for how the program and the Complex Care Team will engage with pati ents, families and caregivers, and support the connecti on to services outside the health system. While many programs begin with a focus on bett er coordinati on of medical needs and clinical care, more mature programs have recognized the importance of supporti ng families in connecti ng with social services, school systems, fi nancial resources, legal resources and other community-based services. This holisti c view that extends beyond clinical measures to include improvements to quality of life and reduced burden of care is a hallmark of high-performing programs.
Regardless of the model selected, successful care management should be organized to address the full spectrum of patients’ and families’ needs – both medical and non-medical - across the continuum from patient onboarding through the transition to adulthood.

Advancing Care Models for Children with Complex Medical Needs
Page 6
A framework for developing the core components of an eff ecti ve care management model for children with complex medical needs is illustrated and described below:
F or children’s hospitals considering developing a program, key elements include:
Aligning around Program Goals and Scope of Service: Pati ents and families of children with complex medical needs have goals that extend beyond narrow clinical outcomes; while they are looking to achieve opti mal health, they also have aspirati ons for independence and a meaningful family and community life. Organizati ons will need to align around a comprehensive set of goals and expectati ons for performance that include clinical outcomes, uti lizati on, cost of receiving and providing care, quality of life, burden of care on families, provider sati sfacti on and other measures. There must be clarity around program scope and size, and well-defi ned clinical criteria for pati ent eligibility (e.g., three or more chronic conditi ons, three or more inpati ent admissions or ED visits within the past 12 months), as well as a process to assist those pati ents who do not meet criteria for the program. In additi on, there will need to be a process for pati ent recruitment and referral management, and communicati on to primary care physicians, specialists and case managers regarding the program, goals and
Program Vision and Goals
Patient and Family Needs
Post-Acute
Care
Self
Care
Specialty
Care
Urgent/
Emergent
Care
Inpatient
Care
Primary
Care C
OM
MU
NIT
Y SERVICES FINANCIAL SERVIC
ES SOC
IAL SERVICES EDUCATIO
NAL SE
RV
ICES
Patient and Family Engagement, Education and Activation
Better Outcomes | Better Pat ient and Fami ly Exper ience | Lower Cost of Care
O p t i m a l Ca re
Patient and Family Onboarding Transition to Adulthood
Advancing Care Models for Children with Complex Medical Needs
Page 7
eligibility. Some programs have also involved payors in the identi fi cati on of high cost, high uti lizati on target populati ons.
Pati ent and Family On-Boarding and Care Plan Development. As pati ents and families are referred into the program, a criti cal initi al area of focus is the development of a comprehensive plan of care. Acti ve engagement of pati ents and their families in defi ning outcomes, along with input from the enti re care team, is essenti al. The plan should support the pati ent, family and care team in understanding the requirements for maintaining opti mal health status and in anti cipati ng and addressing potenti al future healthcare needs. Care planning may include a visit to the pati ent’s home to understand the environment and support the family in interacti ng and connecti ng with their child on a daily basis, and to identi fy ways to maximize the child’s ability to maintain independence. The plan of care should also defi ne the criti cal points of access to services outside the health system including the school system and other social and community-based services. Front-end fi nancial counseling is an important element as there may be resources available to families to help off set the signifi cant fi nancial burden of an intensive healthcare regimen that may include physician, hospital, home health, technology, pharmaceuti cals, therapy and other care.
Care Delivery and Transiti on Management: The care management model should defi ne how the Complex Care Team will support pati ents and their families in achieving opti mum health status and in accessing care and interacti ng with caregivers in all setti ngs. In additi on, the model should acti vely facilitate engagement, coordinati on and communicati on among providers and across setti ngs.
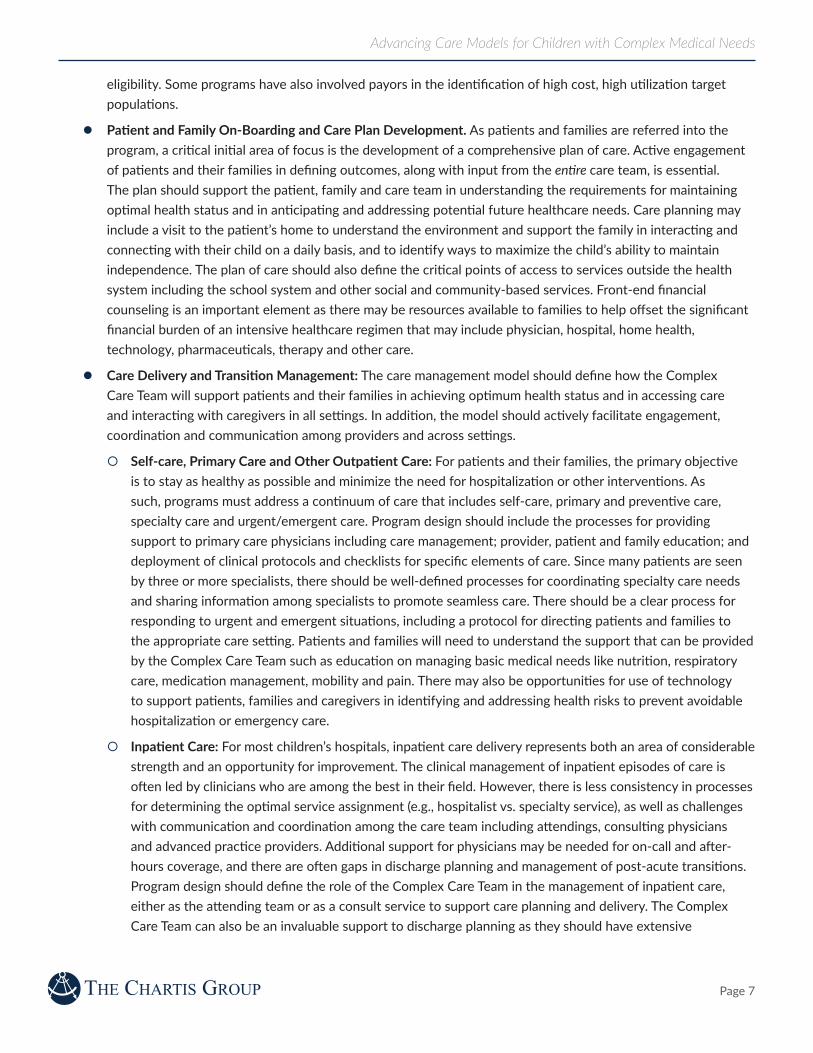
Self-care, Primary Care and Other Outpati ent Care: For pati ents and their families, the primary objecti ve is to stay as healthy as possible and minimize the need for hospitalizati on or other interventi ons. As such, programs must address a conti nuum of care that includes self-care, primary and preventi ve care, specialty care and urgent/emergent care. Program design should include the processes for providing support to primary care physicians including care management; provider, pati ent and family educati on; and deployment of clinical protocols and checklists for specifi c elements of care. Since many pati ents are seen by three or more specialists, there should be well-defi ned processes for coordinati ng specialty care needs and sharing informati on among specialists to promote seamless care. There should be a clear process for responding to urgent and emergent situati ons, including a protocol for directi ng pati ents and families to the appropriate care setti ng. Pati ents and families will need to understand the support that can be provided by the Complex Care Team such as educati on on managing basic medical needs like nutriti on, respiratory care, medicati on management, mobility and pain. There may also be opportuniti es for use of technology to support pati ents, families and caregivers in identi fying and addressing health risks to prevent avoidable hospitalizati on or emergency care.
Inpati ent Care: For most children’s hospitals, inpati ent care delivery represents both an area of considerable strength and an opportunity for improvement. The clinical management of inpati ent episodes of care is oft en led by clinicians who are among the best in their fi eld. However, there is less consistency in processes for determining the opti mal service assignment (e.g., hospitalist vs. specialty service), as well as challenges with communicati on and coordinati on among the care team including att endings, consulti ng physicians and advanced practi ce providers. Additi onal support for physicians may be needed for on-call and aft er-hours coverage, and there are oft en gaps in discharge planning and management of post-acute transiti ons. Program design should defi ne the role of the Complex Care Team in the management of inpati ent care, either as the att ending team or as a consult service to support care planning and delivery. The Complex Care Team can also be an invaluable support to discharge planning as they should have extensive

Advancing Care Models for Children with Complex Medical Needs
Page 8
knowledge of the pati ent, family, available resources and community services. The team can also support communicati on to primary care physicians and post-discharge follow-up with specialists as needed.
Integrati on with Services outside the Health System. A key feature of more comprehensive programs is the support provided to pati ents and families in accessing services that are outside the health system and essenti al to promoti ng independence, opti mizing social interacti ons, achieving maximum independence, and transiti oning to adulthood. Families oft en benefi t from support groups for parents and siblings, and assistance with health insurance or obtaining additi onal fi nancial support through grants and waiver programs. Program design should include processes and resources focused on creati ng awareness of, and access to, developmental and early interventi on programs, educati onal services, recreati onal opportuniti es, specialized vacati on camps, and other community-based services. Parents may also benefi t from help in advocati ng for their children, for example in the creati on of an Individualized Educati on Program (IEP) that defi nes the child’s learning needs, the services the school will provide and how progress will be measured.
Transiti on to Adulthood: As pati ents transiti on to adulthood, they may face physical and cogniti ve barriers, and families oft en lack the informati on needed to navigate the transiti on successfully. For hospitals, the transiti on from pediatric to adult care can have considerable challenges, including acti vati on of pati ents in understanding and assuming responsibility for self-care and fi nding adult providers who are comfortable managing their care. Some programs have no upper age limit, allowing the pati ents’ pediatric primary care physicians and the Complex Care Team to conti nue managing their care through adulthood. Others begin transiti on planning several years prior to pati ents reaching adulthood. Some programs off er a team of transiti on-care providers who are available 24/7 for consultati on to adult providers. Program design should carefully consider alternati ve models, including the implicati ons on program size and capacity, if ongoing clinical management is retained into adulthood. Further, it is important that the transiti on model addresses support for important enablers of adult independence and quality of life including higher educati on, employment, home life, and social interacti on.
Key Requirements for Success A well-organized and thoughtf ully implemented program can have a material impact on health outcomes, quality of life and total cost of care. In our experience, there are fi ve key requirements for success:
1. Leadership alignment around the goals for the program and the requirements for success. While the opportunity for reducing uti lizati on and cost of care may be signifi cant, program design should place primary emphasis on addressing the comprehensive needs of pati ents and their families, with a clear commitment to improving care delivery, outcomes and quality of life. Doing so will require addressing services within and outside the health system. Agreement on program scope and the size of the populati on to be enrolled is criti cal. Many leading programs have started small, focusing on the highest-cost cohort within the populati on and explicit caps on membership. Other programs have focused on broader populati ons, e.g., Medicaid pati ents, with explicit goals for cost reducti on and shared savings arrangements. Leadership must be aligned around the vision for the hospital’s and its physicians’ role in the management of this populati on, and how that role relates to primary care and specialty physicians. Finally, there should be a shared understanding of the degree to which the hospital will assume accountability and risk for the delivery of value, including total cost of care. For hospitals and physicians who are part of a CIN, program design should support alignment with strategic objecti ves, performance requirements and accountability for outcomes.

Advancing Care Models for Children with Complex Medical Needs
Page 9
2. Agreement on specifi c, measurable performance requirements for the program that support the quanti fi cati on of value to pati ents, providers and payors. Expectati ons should be defi ned for improvement across multi ple dimensions of performance including clinical quality, pati ent and family experience, provider sati sfacti on, uti lizati on and cost. Providers must have an understanding of the current baseline, and agreement around the required future performance. If payors parti cipate in the program, or if the program receives other external funding (e.g., grants), there may be explicit performance targets established jointly with funding partners. Programs must be able to assess current and improved performance related to clinical variati on, development and implementati on of consensus-based standards of care, avoidance of redundant and unhelpful care, and the resultant impact on total cost of care. The value propositi on to children, families, employers, communiti es, and payors must be demonstrable improvements in clinical outcomes, quality of life, pati ent and family sati sfacti on and total medical expense. Building programs with these value propositi ons tangibly in place can facilitate migrati on to diff erent payment models and collaborati on across payment sources to help address funding requirements.
3. Acti ve engagement of payors as partners. Many successful programs have been pursued in partnership with Medicaid and/or commercial insurers who have helped fund program investment and implemented shared savings programs to reward providers for management of total cost of care. In some cases, payors have also parti cipated in establishing guidelines for enrollment and recruiti ng the target populati on. Engaging payors at the outset is an important strategy for success, and may require risk-sharing by providers and hospitals. Absent payor involvement, some hospitals in markets where there is considerable fee-for-service volume have found the economics of these programs to be challenging or infeasible, as signifi cant investment in staffi ng and other resources (e.g., space, informati on technology) combined with a reducti on in uti lizati on of hospital services has resulted in a negati ve impact on overall fi nancial performance. Sti ll, other organizati ons that have waited to approach payors unti l aft er programs have been launched have found it diffi cult to generate interest from the payors who are less likely to reward performance that has already been achieved. Ulti mately, the successful migrati on toward value depends on the hospitals’ and providers’ ability to demonstrate diff erenti ated quality and cost to payors and employers. Superior performance will also strengthen the hospitals’ and providers’ positi on to parti cipate in narrow networks and ACOs.
4. Adequate support to the Complex Care Team. Providing and coordinati ng care for these pati ents is challenging, and organizati ons must carefully consider how support requirements diff er from what is required to support general primary care and specialty practi ces. Recruiti ng physicians and other clinicians who are passionate about this populati on is essenti al. Training for primary care physicians, pati ents and their families can reduce the demand on the Complex Care Team and lead to improved outcomes through more ti mely preventi ve health and greater awareness of potenti al medical issues. Supplementi ng the core Complex Care Team with additi onal support such as pharmacy, social work and behavioral health professionals should be considered. In additi on, it is important to understand the Complex Care Team’s capacity and determine reasonable inpati ent and clinic caseloads to avoid overburdening the team.
5. A roadmap and migrati on plan that is aligned with organizati onal capacity and permits suffi cient ti me for successful program implementati on. Building a comprehensive program is a signifi cant undertaking and must be implemented in a manner that supports the development of internal capacity and new competencies required to manage the populati on. There must be ti me allocated for collaborati on with both independent and employed physicians on development of new inpati ent and outpati ent care models, detailed design of operati ng models and tools, infrastructure build, and recruitment of leadership and key personnel. The roadmap must also refl ect
Advancing Care Models for Children with Complex Medical Needs
Page 10
the ti me requirements for pati ent enrollment and the development of personalized plans of care, which can vary signifi cantly based on the size and scope of the program. Parti cularly if the program is approached as a pilot (e.g., in collaborati on with a payor), there will also need to be structured milestones and points at which results can be measured and decisions made about ongoing collaborati on or the need for program changes.
Meeti ng the ChallengeA comprehensive program for children with complex medical needs off ers the promise of enabling these children to achieve their aspirati ons for health, quality of life and independence – and can greatly reduce the burden on pati ents and their families. Designing and launching these programs requires new, innovati ve models of care delivery and unprecedented levels of integrati on and coordinati on of health and community services that challenge the current organizati on and roles of children’s hospitals and pediatric physicians. Programs will need to achieve bett er quality and lower costs, and hospitals should look to secure funding from payors, grants or philanthropy to off set investments or potenti al reducti ons in fee-for-service revenue. When successful, these programs present an opportunity for children’s hospitals to demonstrate value and strengthen their positi on to successfully compete and maintain fi nancial viability under new reimbursement models. Importantly, these programs support children’s hospitals in fulfi lling their mission and commitment to improving the health and well-being of the pediatric populati on by closing the gap in care faced by the pediatric populati on with the most complex medical conditi ons.
(Endnotes)1 Vestal, C. “Improving Medicaid for ‘Medically Complex’ Kids.” The Pew Charitable Trusts. 8 Jan. 2015.2 “Opti mizing Care for Children with Medical Complexity.” Children’s Hospital Associati on. 20123 Ossman A. “Taking Steps, Children’s Hospitals Today.” Summer 2013; Simon TD et al. “Children with Complex Chronic Conditi ons in Inpati ent Hospital Setti ngs in the US.” Pediatrics. 2010: 126(4):647-655; Berry JG et al. “The Landscape of Medical Care for Children with Medical Complexity.” Children’s Hospital Associati on. June 2013; “Opti mizing Healthcare for Children with Medical Complexity.” Children’s Hospital Associati on. 2013.4 Dennis Z. Kuo, MD, MHS, Eyal Cohen, MD, MSc, Rishi Agrawal, MD, MPH, Jay G. Berry, MD, MPH,and Patrick H. Casey, MD. “A Nati onal Profi le of Caregiver Challenges of More-Complex Children with Special Health Care Needs.” JAMA Pediatrics. Nov. 2011: 165 (11)5 Dobson A, DaVanzo J, and Berger G. “Summary of Available Evidence and Methodology for Determining Potenti al Medicaid Savings from Improving Care Coordinati on for Medically Complex Children.” Submitt ed to Children’s Hospital Associati on. Oct. 2013.6 Mosquera, Ricardo et al. “Eff ect of an Enhanced Medical Home on Serious Illness and Cost of Care among High-Risk Children With Chronic Illness.” The Journal of the American Medical Associati on. 24/31 Dec. 2014: 312 (24)7 Casey, Patrick H et al. “Eff ect of Hospital-Based Comprehensive Care Clinic on Health Costs for Medicaid-Insured Medically Complex Children.” The Journal of the American Medical Associati on. 2 May2011: 165 (5)8 Murphy, Nancy A et al. “The Value of Intensive Outpati ent Care for Children with Complex Chronic Conditi ons.” htt ps://www.aacpdm.org/UserFiles/fi le/SP30_MurphyN_complexcare.pdf

Advancing Care Models for Children with Complex Medical Needs
Page 11
For More Informati on
James Karpook, Principal305.610.6542jkarpook@charti s.com
Mark Werner, MD, Nati onal Director, Clinical Consulti ng 540.520.4161mwerner@charti s.com

About The Charti s Group
The Charti s Group (Charti s) is a nati onal advisory services fi rm dedicated to the healthcare industry. Charti s provides strategic and economic planning, accountable care, clinical transformati on, and informati cs and technology consulti ng services and decision support tools to the country’s leading healthcare providers. Charti s has been privileged to work with over two-thirds of the academic medical centers on the U.S. News and World Report “Honor Roll of Best Hospitals,” seven of the 10 largest integrated health systems, four of the fi ve largest not-for-profi t health systems, nine of the top 10 children’s hospitals, emerging and leading accountable care organizati ons, hundreds of community-based health systems, and leading organizati ons in healthcare services. The fi rm is comprised of uniquely experienced senior healthcare professionals and consultants who apply a disti ncti ve knowledge of healthcare economics, markets, clinical models and technology to help clients achieve unequaled results. Charti s has offi ces in Boston, Chicago, Needham, New York, Portland and San Francisco. For more informati on, visit www.charti s.com.
Boston | New York | Chicago | San Francisco | Needham | Portland
© 2016 The Charti s Group, LLC. All rights reserved. This content draws on the research and experience of Charti s consultants and other sources. It is for general informati on purposes only and should not be used as a substi tute for consultati on with professional advisors.