aesthetic resto article
TRANSCRIPT
15Dentistry www.dentistry.co.uk 24 April 2014
clinical
It can be confusing attempting to identify occlusal factors that may be contributing to failure of the dentition, or that may precipitate premature failure of restorative/aesthetic dentistry if not corrected.
It is useful to consider the ideal occlusion and how the dentition you are assessing deviates from this. This involves static and dynamic examination of the teeth with the patient performing functional movements of the mandible and examining the teeth for possible indicators of occlusal damage.
By doing so a risk assessment of the likely stability of the dentition or predictability of any restorative/aesthetic treatment can be made.
If the occlusion is not ideal it may be of no consequence as most patients function satisfactorily with imperfect occlusions. However, there is a difference between accepting a less than ideal occlusion and failing to identify it.
A few of the features of the ideal occlusion that are particularly relevant to
restorative/aesthetic dentistry include:• A stable and reproducible pathwayinto the intercuspal position (ICP)• Simultaneous and even cusp fossacontact in ICP- No vertical or horizontal slides• Posterior disclusion on mandibularprotrusion- Smooth guidance by the palatalsurfaces of the upper anterior teeth• Canineguidanceonlateralmandibularmovements- Canines acting as ramps separating and protecting the anterior and posterior teeth• AclassIincisorrelationship- No excessive overbite• Absenceofcrossbites.
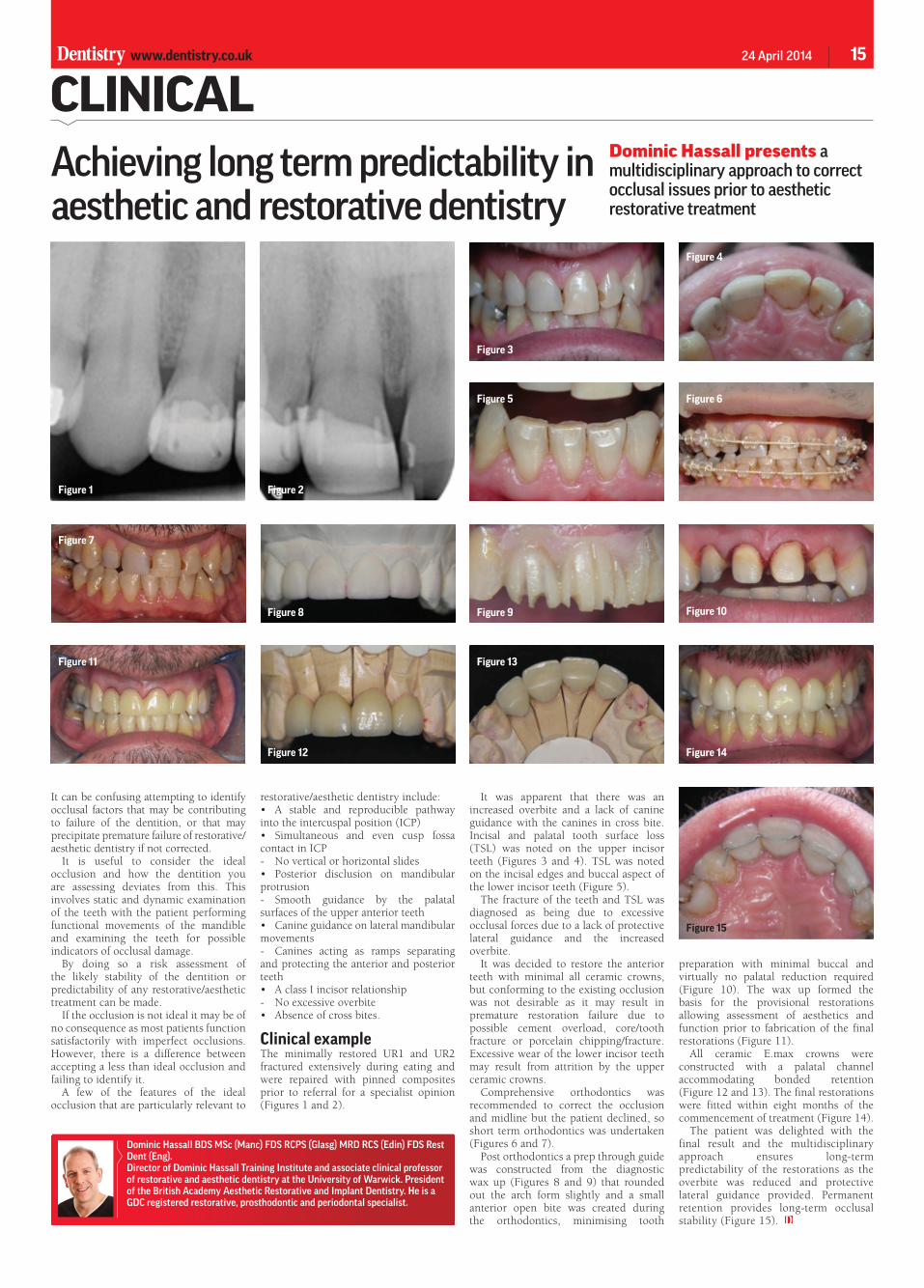
Clinical exampleThe minimally restored UR1 and UR2 fractured extensively during eating and were repaired with pinned composites prior to referral for a specialist opinion (Figures 1 and 2).
It was apparent that there was an increased overbite and a lack of canine guidance with the canines in cross bite. Incisal and palatal tooth surface loss (TSL) was noted on the upper incisorteeth (Figures 3 and 4). TSL was notedon the incisal edges and buccal aspect of the lower incisor teeth (Figure 5).
ThefractureoftheteethandTSLwasdiagnosed as being due to excessive occlusal forces due to a lack of protective lateral guidance and the increased overbite.
It was decided to restore the anterior teeth with minimal all ceramic crowns, but conforming to the existing occlusion was not desirable as it may result in premature restoration failure due to possible cement overload, core/tooth fracture or porcelain chipping/fracture. Excessive wear of the lower incisor teeth may result from attrition by the upper ceramic crowns.
Comprehensive orthodontics was recommended to correct the occlusion and midline but the patient declined, so short term orthodontics was undertaken (Figures 6 and 7).
Post orthodontics a prep through guide was constructed from the diagnostic wax up (Figures 8 and 9) that rounded out the arch form slightly and a small anterior open bite was created during the orthodontics, minimising tooth
Figure 1 Figure 2
Achieving long term predictability in aesthetic and restorative dentistry
Dominic Hassall presents a multidisciplinary approach to correct occlusal issues prior to aesthetic restorative treatment
Dominic Hassall BDS MSc (Manc) FDS RCPS (Glasg) MRD RCS (Edin) FDS Rest Dent (Eng).Director of Dominic Hassall Training Institute and associate clinical professor of restorative and aesthetic dentistry at the University of Warwick. President of the British Academy Aesthetic Restorative and Implant Dentistry. He is a GDC registered restorative, prosthodontic and periodontal specialist.
Figure 3
Figure 4
Figure 5 Figure 6
Figure 7
Figure 11
Figure 9
Figure 13
Figure 8
Figure 12
Figure 10
Figure 14
preparation with minimal buccal and virtually no palatal reduction required (Figure 10). The wax up formed the basis for the provisional restorations allowing assessment of aesthetics and function prior to fabrication of the final restorations (Figure 11).
All ceramic E.max crowns were constructed with a palatal channel accommodating bonded retention (Figure 12 and 13). The final restorations were fitted within eight months of the commencement of treatment (Figure 14).
The patient was delighted with the final result and the multidisciplinary approach ensures long-term predictability of the restorations as the overbite was reduced and protective lateral guidance provided. Permanent retention provides long-term occlusal stability (Figure 15).
Figure 15