aesthetic surgery journal perioperative steroids for …€¦ · professor, dr. hollier is...
TRANSCRIPT

Rhinoplasty
Aesthetic Surgery Journal31(6) 648 –657© 2011 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X11416110www.aestheticsurgeryjournal.com
Rhinoplasty continues to be a challenging and popular operation, with the most recent American Society for Aesthetic Plastic Surgery statistics indicating that rhino-plasty was the sixth-most popular cosmetic surgical proce-dure performed in 2009.1 Because of the complex interplay among the different tissues and anatomical regions of the nose, rhinoplasty is difficult even in the best of hands. Achieving superior aesthetic results while limiting postop-erative sequelae remains every surgeon’s goal.2-4
Periorbital ecchymosis and edema are inconvenient sequelae after rhinoplasty. Although expected, prolonged cases of ecchymosis can discolor the skin and are concerning
Perioperative Steroids for Minimizing Edema and Ecchymosis After Rhinoplasty: A Meta-Analysis
Daniel A. Hatef, MD; Warren A. Ellsworth, MD; Jessica N. Allen, BS; Jamal M. Bullocks, MD; Larry H. Hollier Jr, MD; and Samuel Stal, MD
AbstractBackground: Minimizing complications after rhinoplasty is a priority for every surgeon performing the procedure. Perioperative steroid administration has been shown to decrease postoperative edema and ecchymosis in a number of prospective randomized trials.Objectives: In an effort to further elucidate the significance of the data and develop an evidence-based algorithm for steroid administration, the authors offer a meta-analysis of the existing literature.Methods: A systematic review of the literature was performed. All articles were reviewed for relevant data, which were extracted, pooled, and compared. Seven prospective randomized trials investigating perioperative steroid use in rhinoplasty have been conducted and reported. Four of these studies had the same method of patient edema and ecchymosis assessment, and their data were compared.Results: Based on results from the four relevant studies, perioperative steroid use significantly reduces postoperative edema and ecchymosis of the upper and lower eyelids at one day and seven days postoperatively (P < .0001). Preoperative steroid administration decreases postoperative upper and lower eyelid edema at one day preoperatively, when compared to postoperative administration (P < .05). Extended dosing is superior to one-time dosing (P < .05).Conclusions: Perioperative steroid use decreases postoperative edema and ecchymosis associated with rhinoplasty. Preoperative administration is superior to postoperative, and extended dosing is superior to singular. Based on these results, evidence-based guidelines for perioperative steroid administration can be given.
Level of Evidence: 2
Keywordsrhinoplasty, steroids, edema, ecchymosis
Accepted for publication April 14, 2011.
Dr. Hatef and Dr. Ellsworth are residents, Dr. Bullocks is Associate Professor, Dr. Hollier is Professor and Program Director, and Dr. Stal is Professor and Chairman in the Department of Plastic Surgery, Baylor College of Medicine/Texas Medical Center, Houston, Texas. Dr. Allen is a resident at the University of South Florida School of Medicine, Tampa, Florida.
Corresponding Author:Dr. Samuel Stal, Department of Plastic Surgery, Baylor College of Medicine/Texas Medical Center, 6701 Fannin Street, Houston, TX 77030 USA. E-mail: [email protected]
Review Article

Hatef et al 649
for patients and families. Severe edema can compromise healing, leading to suboptimal formation of scar tissue and significantly altering the intended morphologic result. Many surgeons have utilized steroids in an effort to decrease these postoperative morbidities. Goldman was the first to report their use in the English literature, in the early 1950s.5 Since that time, there have been a number of investigations into the efficacy of different steroids, along with their various doses and schedules.6-13
Griffies et al were the first to undertake a prospective randomized study to examine the use of steroids in rhino-plasty. Comparing the effects of dexamethasone versus control in edema after rhinoplasty, the authors demon-strated that a one-time bolus of dexamethasone yielded a statistically significant reduction in swelling over the root of the nose.6 Subsequently, Hoffmann et al demonstrated the superiority of one-time preoperative steroid adminis-tration in decreasing eyelid and paranasal edema in a prospective study of 49 patients undergoing rhinoplasty.7 In 1998, Berinstein et al utilized magnetic resonance imag-ing and showed that the perioperative administration of dexamethasone yielded a statistically significant increase in swelling over the root of the nose.8
The first prospective randomized trial investigating the efficacy of steroids in rhinoplasty patients was published by Kara et al in 1999. In 55 consecutive patients, preoperative and postoperative administration of dexamethasone led to decreased edema in the upper and lower eyelids for the first two days postoperatively when compared to control.9 Kargi et al examined dexamethasone and its effect on edema, ecchymosis, and intraoperative bleeding in rhinoplasty.10 These authors were the first to examine extended dosing of steroids beyond the operation. They studied groups of patients receiving single preoperative doses, preoperative doses with extended dosing for 48 hours postoperatively, postoperative doses with extended dosing for 48 hours post-operatively, and a control group receiving nothing. All groups receiving steroids before osteotomies demonstrated decreased edema in the early postoperative period when compared to controls and patients receiving the initial dose postoperatively. Extended dosing to 48 hours postopera-tively led to significantly decreased edema and ecchymosis on Postoperative Day (PD) 5 when compared to other groups. In 2006, Gurlek et al demonstrated no benefit in the reduction of edema and ecchymosis with perioperative dexamethasone or betamethasone in rhinoplasty patients.11 Their findings, along with the previously-mentioned results from Berinstein et al, confuse the picture surrounding the clinical efficacy of steroids in rhinoplasty.
Prospective randomized investigations have also assessed the efficacy of methylprednisone as compared to arnica and no treatment.12 In 48 consecutive patients, there was a statis-tically significant increase in the amount of edema immedi-ately postoperatively in the control group as compared to the patients who received arnica and those who received ster-oids. No difference was found between the methylprednisone group and the arnica group. Because of the controversy sur-rounding the efficacy of steroids in rhinoplasty patients, Gurlek et al undertook a prospective randomized investiga-
tion to compare high-dose methylprednisolone (500 mg) with 250-mg doses and control.13 The study demonstrated a statis-tically significant benefit to administering steroids versus control in terms of edema. There was no difference between the steroid dose groups.
Because these studies were prospective randomized trials, the collective data gathered through these efforts lend themselves to meta-analysis. In an effort to pool these data and make a stronger conclusion regarding the efficacy of steroids on edema reduction in rhinoplasty, a systematic literature review was designed. Subsequently, a meta-analysis of the relevant data was performed. Our goal was to gain a greater understanding of the role of steroids for the rhinoplasty patient and their potential to reduce ecchymosis and edema. We also wished to estab-lish evidence-based treatment guidelines for successful steroid administration.
MEthOdsLiterature ReviewA comprehensive literature search was performed. We searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials for articles discussing corti-costeroid use in rhinoplasty. These sources were searched from their inception (MEDLINE, 1966; EMBASE, 1974; Cochrane, 2005) through December 2008. The terms rhino-plasty, steroids, corticosteroids, edema, and ecchymosis were entered to find relevant articles that discussed the pertinent items in question. Only articles written in English were reviewed.
Article Selection
The selection of appropriate data from existing articles was organized in a two-step fashion. First, prospective randomized trials evaluating the efficacy of steroid treat-ment for minimization of postoperative edema and ecchymosis were identified. Second, the articles were thoroughly examined, and those whose authors utilized a comparable method of quantifying edema and ecchy-mosis of the upper and lower eyelids were included in the analysis so that the data could be accurately pooled and statistically compared.
Data Collection and Statistical Analysis
Relevant data were extracted from the chosen articles, including which intervention was given to which group, the total number of patients in each group, the upper and lower eyelid edema ratings, and the upper and lower eyelid ecchy-mosis ratings for each time point. Different categories of outcomes were examined: upper eyelid edema, lower eyelid edema, upper eyelid ecchymosis, lower eyelid ecchymosis, intraoperative bleeding, postoperative pain/discomfort, and analgesics. Categories of intervention were also assessed.

650 Aesthetic Surgery Journal 31(6)
Patients receiving steroids and patients receiving no steroids were both examined globally; steroids for patients receiving them were then broken down by type, timing of administra-tion, dosage, and length of treatment.
Upon review of the relevant data, three tests were devised: Test 1, a global examination of edema and ecchy-mosis seen in all groups receiving steroids of any sort versus all controls; Test 2, a comparison of edema and ecchymosis seen in groups receiving preoperative versus postoperative steroids; and Test 3, an examination of edema and ecchymosis seen in groups receiving one dose versus extended dosing. None of the articles provided patient-specific numbers; rather, the results were reported by group means. These means were extracted and multi-plied by their respective group total to provide a group sum. These sums were then added where relevant and divided by the total group number for that respective inter-vention, group, and so on.
Test 1: Steroid Versus Control Group Calculations
Mean edema and ecchymosis scores for all patient groups receiving steroids and all patient control groups were mul-tiplied by their respective group numbers to calculate total group scores. These were added and then divided by the respective total group number to calculate means and standard deviations for the groups—specifically, for upper eyelid edema scores, lower eyelid edema scores, upper eyelid ecchymosis scores, and lower eyelid ecchymosis scores on PD 1, 4, and 7. Statistical analysis was carried out on the pertinent data utilizing standard χ2 nonpara-metric comparisons.
Test 2: Preoperative Initial Dose Versus Postoperative Initial Dose Calculations
Mean edema and ecchymosis scores for all patient groups who received their first dose of steroids preoperatively or at induction and all patient groups who received their first dose of steroids postoperatively were multiplied by their respective group numbers to calculate total group scores. These were added and then divided by the total group number to calculate means and standard devia-tions for the respective groups—namely, for upper eyelid edema scores, lower eyelid edema scores, upper eyelid ecchymosis scores, and lower eyelid ecchymosis scores on PD 1 and 7. Statistical analysis was carried out on the pertinent data utilizing standard χ2 nonparametric comparisons.
Test 3: Single Dose Versus Extended Postoperative Dosing Calculations
Mean edema and ecchymosis scores for all patient groups who received one-dose steroids and all patient groups who
received extended steroid dosing were multiplied by their respective group numbers to calculate total group scores. These were added and then divided by the total group number to calculate means and standard deviations for the respective groups—again, for upper eyelid edema scores, lower eyelid edema scores, upper eyelid ecchymosis scores, and lower eyelid ecchymosis scores on PD 1 and 7. Statistical analysis was carried out on the pertinent data utilizing standard χ2 nonparametric comparisons.
REsuLts
The initial search revealed 29 articles of interest. Four were not written in English and did not meet inclusion crite-ria.14-17 Eleven were not included because their discussion of steroids was about the postoperative treatment of pol-lybeak or supratip deformity, complications of steroid use in rhinoplasty patients, global steroid administration in plastic surgical procedures, or the medical use of steroids in rhinoplasty.18-28 Six discussed steroid use in rhinoplasty, but their data were excluded either because the articles were reviews or because the study designs were not rand-omized and prospective.29-34 Eight were prospective rand-omized trials investigating postoperative edema and ecchymosis in rhinoplasty patients.6-13
Upon closer investigation of these eight studies, seven utilized the same methods of quantifying postoperative edema and ecchymosis in the upper and lower eyelids, whereby eyelid edema was graded 0 if there was no edema, 1 if the edema was minimal, 2 if the edema extended onto the iris, 3 if the edema covered the iris, and 4 if the edema caused the eyelids to be swollen shut. Ecchymosis was graded 1 if it was only medial, 2 if it extended to the iris, 3 if the ecchymosis was lateral to the pupil, and 4 if it extended to the lateral canthus.6-11,13 Three studies were not included in the meta-analysis because their scoring systems and outcomes evaluations were different and did not allow appropriate cross-evaluation.6,8,11 This resulted in four pro-spective randomized studies that were felt to have compa-rable data (Table 1).7,9-11
Test 1: Steroids Versus Control
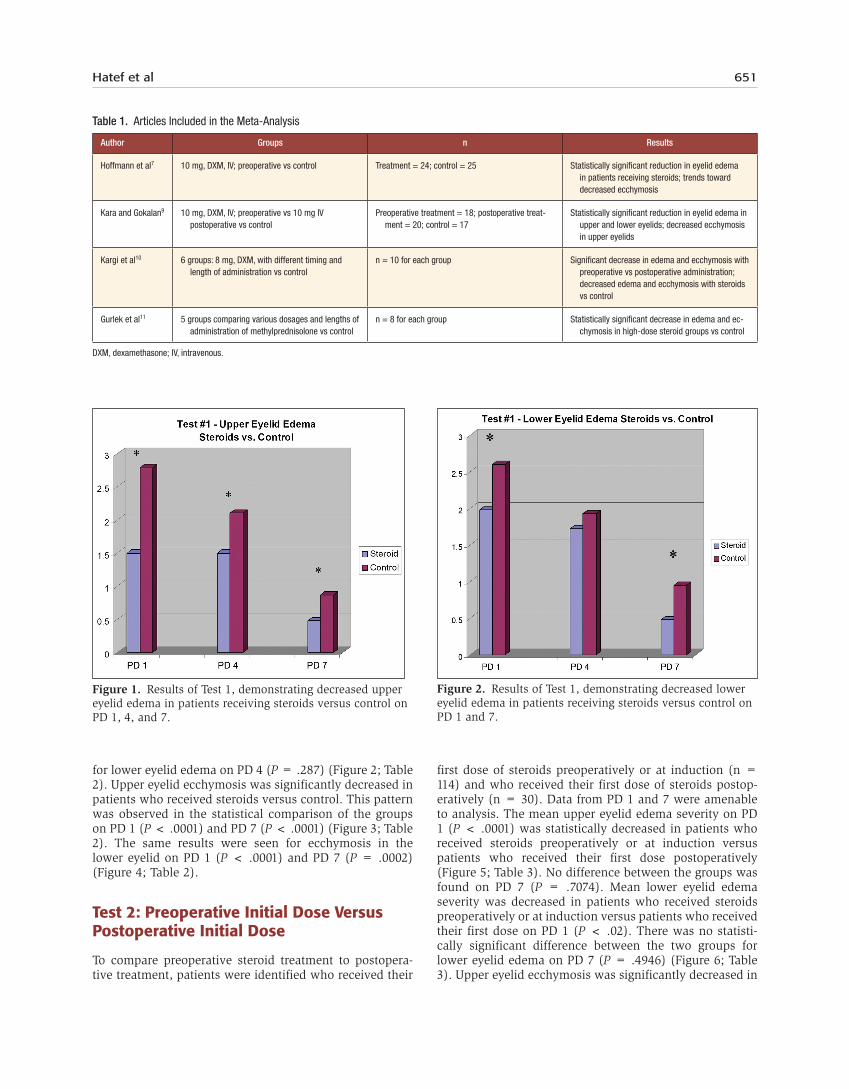
All groups from all four studies were included in the sta-tistical analysis. In sum, 144 patients who received ster-oids and 60 patients who did not receive steroids had data from PD 1 and 7 amenable to analysis; furthermore, 62 patients treated with steroids and 42 control patients had data for analysis of PD 4 numbers. The mean upper eyelid edema severity on PD 1 (P < .0001), PD 4 (P = .0001), and PD 7 (P = .0002) was statistically decreased in patients who received steroids versus control patients, who received no treatment (Figure 1; Table 2). Mean lower eyelid edema severity in patients receiving steroids was significantly decreased in comparison to control patients on PD 1 (P < .0001) and PD 7 (P = .0036). There was no statistically significant difference between the two groups
Hatef et al 651
for lower eyelid edema on PD 4 (P = .287) (Figure 2; Table 2). Upper eyelid ecchymosis was significantly decreased in patients who received steroids versus control. This pattern was observed in the statistical comparison of the groups on PD 1 (P < .0001) and PD 7 (P < .0001) (Figure 3; Table 2). The same results were seen for ecchymosis in the lower eyelid on PD 1 (P < .0001) and PD 7 (P = .0002) (Figure 4; Table 2).
Test 2: Preoperative Initial Dose Versus Postoperative Initial Dose
To compare preoperative steroid treatment to postopera-tive treatment, patients were identified who received their
first dose of steroids preoperatively or at induction (n = 114) and who received their first dose of steroids postop-eratively (n = 30). Data from PD 1 and 7 were amenable to analysis. The mean upper eyelid edema severity on PD 1 (P < .0001) was statistically decreased in patients who received steroids preoperatively or at induction versus patients who received their first dose postoperatively (Figure 5; Table 3). No difference between the groups was found on PD 7 (P = .7074). Mean lower eyelid edema severity was decreased in patients who received steroids preoperatively or at induction versus patients who received their first dose on PD 1 (P < .02). There was no statisti-cally significant difference between the two groups for lower eyelid edema on PD 7 (P = .4946) (Figure 6; Table 3). Upper eyelid ecchymosis was significantly decreased in
Table 1. Articles Included in the Meta-Analysis
Author Groups n Results
Hoffmann et al7 10 mg, DXM, IV; preoperative vs control Treatment = 24; control = 25 Statistically significant reduction in eyelid edema in patients receiving steroids; trends toward decreased ecchymosis
Kara and Gokalan9 10 mg, DXM, IV; preoperative vs 10 mg IV postoperative vs control
Preoperative treatment = 18; postoperative treat-ment = 20; control = 17
Statistically significant reduction in eyelid edema in upper and lower eyelids; decreased ecchymosis in upper eyelids
Kargi et al10 6 groups: 8 mg, DXM, with different timing and length of administration vs control
n = 10 for each group Significant decrease in edema and ecchymosis with preoperative vs postoperative administration; decreased edema and ecchymosis with steroids vs control
Gurlek et al11 5 groups comparing various dosages and lengths of administration of methylprednisolone vs control
n = 8 for each group Statistically significant decrease in edema and ec-chymosis in high-dose steroid groups vs control
DXM, dexamethasone; IV, intravenous.
Figure 1. Results of Test 1, demonstrating decreased upper eyelid edema in patients receiving steroids versus control on PD 1, 4, and 7.
Figure 2. Results of Test 1, demonstrating decreased lower eyelid edema in patients receiving steroids versus control on PD 1 and 7.

652 Aesthetic Surgery Journal 31(6)
patients who received preoperative or induction first-dose steroids versus postoperative first-dose steroids. This was seen on both PD 1 (P < .0001) and PD 7 (P < .012) (Figure 7; Table 3). No difference was found between the two groups when their lower eyelid ecchymosis was com-pared, on either PD 1 (P = .523) or PD 7 (P = .12) (Figure 8; Table 3).
Test 3: Single Dose Versus Extended Postoperative Dosing
Some groups from all four studies were included in the statistical analysis. Control groups were not included, as they did not receive steroids. Because of the statistically significant results from Test 2, results from groups of patients who received their first dose of steroids postop-eratively were not included, in an effort to maximize the reliability of the data. Fifty-four patients who received just one dose of steroids preoperatively and 60 patients who received extended dosing of steroids beyond their initial dose had data from PD 1 and 7 amenable to analysis. Mean upper eyelid edema severity on PD 1 (P < .0001) and PD 7 (P = .0017) was statistically decreased in patients who received extended dosing versus patients who received single doses (Figure 9; Table 4).
On PD 7 there was a statistically significant decrease in lower eyelid edema severity in patients who received extended dosing of steroids (P < .0001). This difference was not seen between the groups on PD 1 (P = .125) (Figure 10; Table 4). Upper eyelid ecchymosis was decreased in patients who received extended dosing of steroids versus those who received a single dose of
steroids. This was seen on both PD 1 (P < .002) and PD 7 (P < .0001) (Figure 11; Table 4). Comparison of lower eyelid ecchymosis on PD 1 (P < .0001) and PD 7 (P < .0001) demonstrated a statistically significant decrease in severity in patients receiving extended dosing of steroids (Figure 12; Table 4).
Table 2. Test 1: Steroids Versus Control—Mean Severity
ConditionPostoperative
Day Steroids Control P
Edema: upper eyelid
1 1.50 2.48 < .0001
4 1.50 2.01 .0001
7 0.41 0.61 .0002
Edema: lower eyelid
1 1.98 2.60 < .0001
4 1.72 1.93 .287
7 0.48 0.95 .0036
Ecchymosis: upper eyelid
1 1.80 2.79 < .0001
7 0.64 1.09 < .0001
Ecchymosis: lower eyelid
1 1.66 2.79 < .0001
7 0.48 0.87 .0002
Figure 3. Results of Test 1, demonstrating decreased upper eyelid ecchymosis in patients receiving steroids versus control on PD 1 and 7.
Figure 4. Results of Test 1, demonstrating decreased lower eyelid ecchymosis in patients receiving steroids versus control on PD 1 and 7.

Hatef et al 653
disCussiOnThe periorbital area is especially prone to postoperative edema and bruising that can be difficult for the patient to camouflage. Intraoperative rhinoplasty maneuvers often cause significant postoperative periorbital morbidity, includ-ing palpebral edema that can result in temporary obstruction of vision. Furthermore, periorbital bruising can be visually disturbing and frightening to patients and families and can lead to permanent pigmentation of surrounding skin.11 To
minimize these postoperative conditions, many surgeons have attempted different preventative measures. Some have suggested hypotensive general anesthesia as a way to address these issues,35 while others argue that this may actu-ally increase the amount of ecchymosis, as appropriate intra-operative hemostasis may not be obtained.36 Still others have evaluated intravenous administration of steroids and other agents.
Perioperative administration of corticosteroids has been shown to decrease both edema and ecchymosis in several
Figure 5. Results of Test 2, demonstrating decreased upper eyelid edema in patients receiving preoperative/induction steroids versus those receiving the first dose postoperatively on PD 1.
Table 3. Test 2: Steroids Preoperatively or at Induction Versus Postoperatively—Mean Severity
ConditionPostoperative
DayPreoperative /
Induction Postoperative P
Edema: upper eyelid
1 1.41 1.87 < .0001
7 0.40 0.43 .7074
Edema: lower eyelid
1 1.91 2.23 < .02
7 0.40 0.31 .4946
Ecchymosis: upper eyelid
1 1.75 2.17 < .0001
7 0.59 0.80 < .012
Ecchymosis: lower eyelid
1 2.07 2.03 .523
7 0.45 0.53 .12
Figure 6. Results of Test 2, demonstrating decreased lower eyelid edema in patients receiving preoperative/induction steroids versus those receiving the first dose postoperatively on PD 1.
Figure 7. Results of Test 2, demonstrating decreased upper eyelid ecchymosis in patients receiving preoperative/induction steroids versus those receiving the first dose postoperatively on PD 1 and 7.

654 Aesthetic Surgery Journal 31(6)
studies. Other studies have shown no benefit. In the present meta-analysis, four trials that met previously-described inclusion criteria were identified and studied for outcomes after perioperative steroid administration.
Many different steroid preparations and dosage schedules have been utilized in rhinoplasty patients. In addition, lack of standard evaluation of postoperative edema and bruising complicates comparison among groups in different studies. However, the studies reviewed here were consistent in their scale of postoperative evaluation. An overall analysis of
pooled data from four trials therefore supports these sugges-tions and yields greater evidence for treatment guidelines for steroid administration in rhinoplasty patients.
Our review confirms that there is decreased upper and lower eyelid ecchymosis and edema after perioperative administration of steroids when compared to no interven-tion. These results reached statistical significance at PD 1 and 7. Three of the four studies reviewed utilized between 8 and 10 mg of dexamethasone intravenously, while the final review studied methylprednisolone. We were unable to
Figure 8. Results of Test 2, demonstrating no difference in lower eyelid ecchymosis between patients receiving preoperative/induction steroids versus those receiving the first dose postoperatively on PD 1 and PD 7.
Figure 9. Results of Test 3, demonstrating decreased upper eyelid edema in patients receiving extended dosing versus single dosing on PD 1 and 7.
Table 4. Test 3: Single Dose Versus Extended Dosing of Steroids
ConditionPostoperative
Day Single DoseExtended Dosing P
Edema: upper eyelid
1 1.81 1.26 < .0001
7 0.53 0.28 .0017
Edema: lower eyelid
1 2.06 2.04 .125
7 0.87 0.33 < .0001
Ecchymosis: upper eyelid
1 1.86 1.56 .002
7 0.80 0.27 < .0001
Ecchymosis: lower eyelid
1 2.23 1.86 < .0001
7 0.61 0.29 < .0001 Figure 10. Results of Test 3, demonstrating decreased lower eyelid edema in patients receiving extended dosing versus single dosing on PD 7.

Hatef et al 655
determine a benefit of one particular steroid over another in the meta-analysis, but due to ease of dosing, dexametha-sone continues to be the steroid of choice.
The timing of steroid administration has also been a topic of concern for many rhinoplasty surgeons. Many believe that circulating steroids before osteotomy minimizes the degree of bruising and edema, when compared to administration in the recovery room. Our data would sup-port this common notion. This benefit was lost, however, in upper and lower eyelid edema as well as in lower eyelid ecchymosis by PD 7. Finally, this meta-analysis suggests that, in addition to a preoperative dose, patients have a significant reduction in swelling and bruising when steroids are continued for up to three days. In our clinic, most patients are treated with an initial preoperative intravenous dose followed by redosing on PD 1 and 2 or discharge with oral prednisone taper over two days. This method can offer the best possible outcome for the occasional patient who requires earlier reintroduction to work or society events. Most patients undergoing rhinoplasty at our institution are discharged home from the recovery room; thus, for ease of treatment, oral steroids are preferred if at-home postopera-tive steroid administration is to continue.
Steroid administration is not always harmless and should not be given (especially for a prolonged period) without serious consideration of patient-specific medical factors. Prolonged steroid treatment should therefore be undertaken only when necessary and with the appropriate patient, after risk-benefit analysis. Complications such as gastrointestinal ulcer formation are usually seen in patients treated over the long term.37 Consider, however, that meta-bolic changes and immunologic responses are altered in the postoperative period.38 Metabolism of carbohydrates, lipids, and proteins is altered in the face of steroid treatment,
especially affecting our diabetic patients.39 Furthermore, mood changes secondary to steroid administration are well documented and can vary from depression to eupho-ria.9 Of note, in the studies reviewed, there was a case of gastrointestinal bleeding in a patient treated with steroids for five days.7
There are studies that have found no benefit with preop-erative steroids in open rhinoplasty. Berinstein et al demon-strated that preoperative intravenous dexamethasone was associated with increased soft tissue edema, when evalu-ated by magnetic resonance imaging preoperatively and postoperatively.8 The measurement of soft tissue thickness over the nasal bone–maxillary junction proved thicker in the steroid treatment group. The significance of this study is unknown and it was not analyzed in our meta-analysis due to the inability to compare the authors’ postoperative definition of edema with our edema and ecchymosis scales. One of the studies included in this analysis demonstrated that betamethasone, dexamethasone, and methylpredniso-lone did not decrease postoperative edema.11 This shows the utility of combining data sets, where possible, to further elucidate the answers to ongoing debate.
Other methods of minimizing swelling and bruising after facial surgery have been described. These methods include less traditional “herbal” medicines, such as papaya extract40 and Melilotus extract,41 in postrhinoplasty patient manage-ment. Totonchi and Guyuron conducted a prospective rand-omized trial to evaluate the difference in efficacy between arnica and steroids for control of postoperative swelling and bleeding.12 They were found to be equally effective in reduc-ing swelling in the early postoperative period, but arnica did not reduce ecchymosis while steroid treatment did.
Unfortunately, we were unable to differentiate between closed and open rhinoplasty because the discussed studies
Figure 11. Results of Test 3, demonstrating decreased upper eyelid ecchymosis in patients receiving extended dosing versus single dosing on PD 1 and 7.
Figure 12. Results of Test 3, demonstrating decreased lower eyelid ecchymosis in patients receiving extended dosing versus single dosing on PD 1 and 7.

656 Aesthetic Surgery Journal 31(6)
did not allow comparison. A comparison of the postopera-tive nasal edema seen after open and closed rhinoplasty would be a worthy investigation. Furthermore, there is clearly some subjectivity involved in the point-scale evalu-ation of edema and ecchymosis, which is why only trials that included blinded evaluation of patient outcomes were chosen. The nature of these evaluations lends itself to lowered interrater reliability. Finally, note that there is an inherent subjectivity in analyzing results from plastic sur-gery. The aesthetic nature of our specialty means that every patient is truly different and every procedure pre-sents a unique challenge, which may lead to some decrease in reliability when data between patients and surgeons are compared.
COnCLusiOns
Based on our meta-analysis of existing randomized, pro-spective trials, patients who were given steroids had reduced edema and ecchymosis when compared with control patients who did not receive them. The overall data analysis confirms a statistically significant benefit when steroids are given in the preoperative period (either in preoperative holding or upon induction). Further, there is clearly a trend toward long-term reduction in edema and bruising if steroid treatment is continued in the post-operative period for three days. For this reason, patients who must return to work or social engagements in the early postoperative period (prior to Day 10) may ben-efit from continuing oral steroids at home to minimize postoperative edema and ecchymosis. Reinforced by these data-based guidelines, it is our practice to give 10 mg of dexamethasone in the preoperative area or upon induction. In a select group, we consider continuation of oral prednisone, 50 mg and 25 mg, on Postoperative Day 2 and Day 3, respectively. Ultimately, our review sug-gests that all patients have significant resolution of both edema and ecchymosis, regardless of treatment, by Day 10 postoperatively.
disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
REFEREnCEs
1. American Society for Aesthetic Plastic Surgery. 2010 statistics. http://www.surgery.org/sites/default/files/Stats 2010_1.pdf. Accessed July 15, 2011.
2. Guyuron B. Dynamics of rhinoplasty. Plast Reconstr Surg 1991;88:970.
3. Guyuron B, Daniel RK, Constantian MB, Gunter JP. Avoiding secondary rhinoplasty. Paper presented at the American Society of Aesthetic Plastic Surgeons annual meeting, April 2004, Vancouver, Canada.
4. Constantian MB. Four common anatomic variants that predispose to unfavorable rhinoplasty results: a study based on 150 consecutive secondary rhinoplasties. Plast Reconstr Surg 2000;105:316.
5. Goldman IB, Freeman J, Bloom S. The effect of cortogen in rhinoplasty. Eye Ear Nose Throat Mon 1952;31:548.
6. Griffies WS, Kennedy K, Gasser C, Fankhauser C, Taylor R. Steroids in rhinoplasty. Laryngoscope 1989;99:1161.
7. Hoffmann DF, Cook TA, Quatela VC, Wang TD, Brown-rigg PJ, Brummett RE. Steroids and rhinoplasty: a double-blind study. Arch Otolaryngol Head Neck Surg 1991;117:990.
8. Berinstein TH, Bane SM, Cupp CL, DeMarco JK, Hunsaker DH. Steroid use in rhinoplasty: an objective assessment of postoperative edema. Ear Nose Throat J 1998;77:40.
9. Kara CO, Gokalan I. Effects of single-dose steroid usage on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Plast Reconstr Surg 1999;104:2213.
10. Kargi E, Hosnuter M, Babuccu O, Altunkaya H, Altin-yazar C. Effect of steroids on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Ann Plast Surg 2003;51:570.
11. Gurlek A, Fariz A, Aydogan H, Ersoz-Ozturk A, Eren AT. Effects of different corticosteroids on edema and ecchymo-sis in open rhinoplasty. Aesthetic Plast Surg 2006;30:150.
12. Totonchi A, Guyuron B. A randomized, controlled com-parison between arnica and steroids in the management of postrhinoplasty ecchymosis and edema. Plast Reconstr Surg 2007;120:271.
13. Gurlek A, Fariz A, Aydogan H, Ersoz-Ozturk A, Evans GRD. Effects of high dose corticosteroids in open rhino-plasty. J Plast Reconstr Aesth Surg 2009;62:650-665.
14. Mahe E, Camblin J, Micheli Pelegrin V. Injections of tri-amcinolone acetonide in the treatment of parrot beak. Ann Otoalryngol Chir Cervicofac 1974;91:695.
15. Mahe E, Camblin J, Pelligrini VM. Treatment of postop-erative Corbin’s beak using repeated local triamcinolone acetonide injections. Ann Chir Plast 1975;20:79.
16. Labayle J, Vignaux, Dervaux JL. Alfathesin anesthesia: its use in otorhinolaryngology. Ann Otolaryngol Chir Cer-vicofac 1976;93:707.
17. Meites G, Protecazuax A, Pessey JJ. Importance of fluni-trazepam for the reduction of bleeding in rhinoplasty. Cah Anesthesiol. 1984;32:21.
18. Baker DC. Treatment of obstructing inferior turbi-nates with intranasal corticosteroids. Ann Plast Surg 1979;3:253.
19. Whiteman DW, Rosen DA, Pinkerton RM. Retinal and choroidal microvascular embolism after intranasal corti-costeroid injection. Am J Ophthalmol 1980;89:851.
20. Habal MB. Prevention of postoperative facial edema with steroids after facial surgery. Aesthetic Plast Surg 1985;9:69.
21. Milford CA, Mugliston T, Lund VJ. Medical rhinoplasty in nasal sarcoidosis. Rhinology 1990;28:137.

Hatef et al 657
22. Quatela VC, Sherris DA, Rounds MF. Esthetic refinements in forehead flap nasal reconstruction. Arch Otolaryngol Head Neck Surg 1995;121:1106.
23. Shafir R, Cohen M, Gur E. Blindness as a complication of subcutaneous nasal steroid injection. Plast Reconstr Surg 1999;104:1180.
24. Mabrie DC, Papel ID. An unexcpected occurrence of acute contact dermatitis during rhinoplasty. Arch Facial Plast Surg 1999;1:320.
25. Hanasono MM, Kridel RW, Pastorek NJ, Glasgold MJ, Koch RJ. Correction of the soft tissue pollybeak using tri-amcinolone injection. Arch Facial Plast Surg 2002;4:26.
26. Rajabian MH, Sodaify M, Aghaei S. Severe facial dermati-tis as a late complications of aesthetic rhionplasty: a case report. BMC Dermatol 2004;4:1.
27. Yavuzer R, Basterzi Y, Ozkose Z, Yucel Dmier H, Yilmaz M, Ceylan A. Tapia’s syndrome following septorhino-plasty. Aesthetic Plast Surg 2004;28:208.
28. Ozdel O, Kara CO, Kara IG, Sevinc D, Oguzhanoglu NK, Topuz B. Does corticosteroid usage in rhinoplasty cause mood changes? Adv Ther 2006;23:809.
29. Donald PJ. Postoperative care of the rhinoplasty patient. Otolaryngol Clin North Am 1975;8:797.
30. Kittel H, Masing H. Corticosteroid therapy in rhinoplasty. Rhinology 1976;14:163.
31. Mondolfi PE. Postrhinoplasty edema. Plast Reconstr Surg 1981;68:122.
32. Ofo E, Singh A, Marais J. Steroids in rhinoplasty: a survey of current UK otolaryngologists’ practice. J Laryngol Otol 2006;120:108.
33. Xu F, Zeng W, Mao X, Fan GK. The efficacy of melilotus extract in the management of postoperative ecchymosis and edema after simultaneous rhinoplasty and blepharo-plasty. Aesthetic Plast Surg 2008;32:599.
34. Cochran CS, Ducic Y, DeFatta RJ. Current concepts in the postoperative care of the rhinoplasty patient. South Med J 2008;101:935.
35. Dionyssiou D. A simple and effective combined method for the management of postrhinoplasty ecchymosis and edema. Plast Reconstr Surg 2008;121:2176.
36. Guyuron B. Reply: a simple and effective combined method for the management of postrhinoplasty ecchy-mosis and edema. Plast Reconstr Surg 2008;121:2176.
37. Hamby LS, Zweng TN, Strodel WE. Perforated gastric and duodenal ulcer: an analysis of prognostic factors. Am Surg 1993;59:319.
38. Fujita T, Imai T, Anazawa S. Influence of modest endo-toxemia on postoperative antithrombin deficiency and circulating secretory immunoglobulin A levels. Ann Surg 2003;238:258.
39. Ackerman NB. Metabolic consequences from conver-sion of jejunoileal bypass to gastric bypass. Ann Surg 1982;196:553.
40. Vallis CP, Lund MH. Effect of treatment with Carica papaya on resolution of edema and ecchymosis follow-ing rhinoplasty. Curr Ther Res Clin Exp 1969;11:356.
41. Xu F, Zeng W, Mao X, Fan GK. The efficacy of Melilotus extract in the management of postoperative ecchymosis and edema after simultaneous rhinoplasty and blepharo-plasty. Aesthetic Plast Surg 2008;32:599.