agenda finance committee meeting of the board … payor update joan kezic, vp payor relations...
TRANSCRIPT

A copy of the agenda for the Regular Committee Meeting will be posted and distributed at least seventy-two (72) hours prior to the
meeting. In observance of the Americans with Disabilities Act, please notify us at 650-988-7504 prior to the meeting so that we
may provide the agenda in alternative formats or make disability-related modifications and accommodations.
AGENDA Finance Committee Meeting of the Board
Monday, January 26, 2015, 6:30 p.m.
Conference Rooms A and B, Ground Floor
2500 Grant Road, Mountain View, California
Richard Juelis will participate via teleconference from 230 N. Admiral Byrd Road, Salt Lake City, UT MISSION: The purpose of the Finance Committee (“Committee”) is to provide oversight, information sharing and financial reviews
related to budgeting, capital budgeting, long-range financial planning and forecasting, and monthly financial reporting for El
Camino Hospital Board of Directors (“Board”). In carrying out its review, advisory and oversight responsibilities, the Committee
shall remain flexible in order to best define financial strategies that react to changing conditions.
AGENDA ITEM PRESENTED BY
1. CALL TO ORDER/ROLL CALL Dennis Chiu, Chair 6:30 p.m.
2. POTENTIAL CONFLICT OF INTEREST
DISCLOSURES
Dennis Chiu, Chair 6:31 – 6:32
3. PUBLIC COMMUNICATION Dennis Chiu, Chair 6:32 – 6:33
4. CONSENT CALENDAR ITEMS
Any Committee Member may remove an item for
discussion before a motion is made.
Dennis Chiu, Chair public
comment
Motion(s) for
recommendation
required
6:33 – 6:35
Approval:
a. September 29, 2014 Minutes
b. November 2014 Financials
Information: c. Finance Committee Charter
d. Articles of Interest
ATTACHMENT 4
5. REPORT ON BOARD ACTIONS Dennis Chiu, Chair Information
6:35 – 6:40
6. ICD 10 PLAN
ATTACHMENT 6
Frank Kuziel, Director HIMS Information
6:40 – 6:50
7. DECEMBER 2014 FINANCIALS
ATTACHMENT 7
Iftikhar Hussain, Chief
Financial Officer
public
comment
Motion for
recommendation
required
6:50 – 7:00
8. ADJOURN TO CLOSED SESSION 7:00
9. POTENTIAL CONFLICT OF INTEREST
DISCLOSURES
Dennis Chiu, Chair 7:00 – 7:01
10. CONSENT CALENDAR
Any committee member may remove an item for
discussion before a motion is made.
Dennis Chiu, Chair
Motion for
recommendation
required
7:01 – 7:05

Finance Committee Meeting El Camino Hospital Board January 26, 2015 Page 2
AGENDA ITEM PRESENTED BY
Approval: a. September 29, 2014 Closed Minutes. Gov’t
Code Section 54957.2. Information: Physician Contracts: b. Interventional Radiology On-Call Agreement,
Mountain View. Report involving health care facility trade secrets. Health and Safety Code Section 32106(b).
c. Interventional Radiology On-Call Agreement, Los Gatos. Report involving health care facility trade secrets. Health and Safety Code Section 32106(b).
Don Holmquest, Senior Medical Director, Physician Services
11. Health and Safety Code Section 32106(b) for a report involving health care facility trade secret.
- Behavioral Health – Addictions Services a. Addictions Business Plan b. Recruitment of Addiction Specialist
Michael Fitzgerald, Executive Director Behavioral Health Rich Katzman, Chief Strategy Officer
Information 7:05 – 7:20
12. Health and Safety Code Section 32106(b) for a report involving health care facility trade secret. - Capital Facilities Spending Report
Ken King, Chief Administrative Services Officer
Information 7:20 – 7:30
13. Health and Safety Code Section 32106(b) for a report involving health care facility trade secret. - Los Gatos Projects a. LG OR Room 4 Conversion b. LG NICU Expansion
Ken King, Chief Administrative Services Officer Rich Katzman, Chief Strategy Officer
Information 7:30 – 7:45
14. Health and Safety Code Section 32106(b) for a report involving health care facility trade secret. - North Parking Solar Panels
Ken King, Chief Administrative Services Officer
Information 7:45 – 7:55
15. Govt. Code Section 54956.8, conference with real estate negotiator Ken King regarding property.
- Property Planning Strategy
Ken King, Chief Administrative Services Officer
Motion for recommendation
required 7:55 – 8:05
16. Health and Safety Code Section 32106(b) for a report involving health care facility trade secret.
- Payor Update
Joan Kezic, VP Payor Relations
Information 8:05 – 8:20
17. RECONVENE OPEN SESSION 8:20 – 8:21 To report any required disclosures regarding permissible actions taken during Closed Session.
Dennis Chiu, Chair
18. PHYSICIAN CONTRACTS
a. Interventional Radiology On-Call Agreement, Mountain View b. Interventional Radiology On-Call Agreement, Los Gatos
Dennis Chiu, Chair public comment
Motion(s) for recommendation
required 8:21 – 8:22

Finance Committee Meeting El Camino Hospital Board January 26, 2015 Page 3
AGENDA ITEM PRESENTED BY
19. BEHAVIORAL HEALTH – ADDICTIONS SERVICES
a. Addictions Business Plan b. Recruitment of Addiction Specialist
Dennis Chiu, Chair public comment
Motion(s) for recommendation
required 8:22 – 8:23
20. LOS GATOS PROJECTS a. LG OR Room 4 Conversion b. LG NICU Expansion
Dennis Chiu, Chair public comment
Motion(s) for recommendation
required 8:23 – 8:24
21. NORTH PARKING SOLAR PANELS Dennis Chiu, Chair public
comment Motion for
recommendation required
8:24 – 8:25 22. ADJOURNMENT Dennis Chiu, Chair 8:25 p.m.
FY 2015 Finance Committee Meetings: - Wednesday, March 25, 2015 (Semi-Annual ECH Board and Advisory Committee Session) - Monday, March 30, 2015 - Tuesday, May 26, 2015

Separator Page
4a. 9-29-14 FC OPEN Minutes_10202014.docx
Minutes of the Open Session Meeting
Finance Committee of the Board of Directors
Of El Camino Hospital
Monday, Sepember 29, 2014
El Camino Hospital, 2500 Grant Road, Mountain View, California
Conference Room A
1. Call to Order/Roll Call. The Open Session meeting of the Finance Committee
of El Camino Hospital (the “Committee”) was called to order by Committee Chairman Dennis
Chiu at 5:31 pm.
Committee members present: Dennis Chiu, Richard Juelis, and John Zoglin.
Committee members absent: Bill Hobbs and Nandini Tandon.
2. Potential Conflict of Interests Disclosures. Chair Chiu asked if any committee
member or anyone in the audience believes that a committee member may have a conflict of
interest on any of the items on the agenda. No conflict of interest was reported.
3. Public Communication. Chair Chiu asked if there were any public
communications, there was none.
4. Consent Calendar. Chair Chiu asked if anyone would like to remove any items
from the Consent Calendar. Mr. Zoglin requested that the following items be removed: 4c)
FY2015; 4d) FY2015 Organizational Goals; and 4f) LG OR Room 4 Conversion, Final Funding
Request.
Motion: To approve Consent Calendar items 4a (July 28, 2014 meeting minutes), 4b (July 2014
Financials, and 4e (iCare Dashboard)
Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
There was a brief discussion regarding adjusted patient days worked hours versus patient days on the
Corporate Scorecard. Mick Zdeblick, Chief Operating Officer, explained that the Scorecard is more
robust and contains different metrics for different dimensions of operations. The Organizational
Goals is what drives the organizational component of metric of compensation for directors, managers
and senior managers. He further explained that every organizational goal is included in the corporate
scorecard and that the corporate scorecard aligns with the major bucket of organizational goals.
Motion: To approve Consent Calendar items 4c (FY2015 Corporate Scorecard) and 4d (FY2015
Corporate Goals)
Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin
DRAFT

Finance Committee of the Board
September 29, 2014
Page 2
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
Ken King, Chief Administrative Services Officer, was available via Webex to answer questions
regarding the Los Gatos OR Room 4 conversion final funding request. He explained that an ROI
was put together when this project was envisioned about two years ago and presented background
information about this project which was identified early on as a project that needed to be done. He
stated the ROI has been updated since the expenditures have become more expensive than originally
planned. Mr. Zoglin would like to understand what the value and benefits would be for the money
spent and stated he does not believe there is enough information currently to recommend approval
from the Board. Chair Chiu recommended that the item be referred to the Board without a motion
from the Committee but to include an adjusted ROI along with a summary that includes justification
of the expenditure and the value and benefits received.
5. Agenda Item 5 – August 2014 Financials. Iftikhar Hussain, Chief Financial
Officer presented the August 2014 financials stating that we had a very good start for the year
with volume increasing by 4%, and expenses are lower than budget. Mr. Juelis asked if this is
expected to continue as a trend. Mr. Hussain stated the goal is to flatten out the curve in the
growth of expenses as revenue increases slow. At a future meeting, Mr. Juelis requested that Mr.
Hussain track where we are with cost savings in regards to the $10M target. Michelle McGowen,
Senior Director of Business Analytics, reviewed slides (Worked Hours per Adjusted Patient Day;
Year to Date Variance; and Revenue and Expense per CMI Adjusted Discharge) included in the
Summary of Financial Operations presentation.
Motion: To recommend that the Board approve the FY 2014 August Financials. Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
6. Agenda Item 6 - Pacing Plan. Chair Chiu noted the following: 1) the November
Finance Committee meeting has been rescheduled to December 1 due to the Thanksgiving
Holiday; 2) the December 1 meeting will be a joint meeting with the Investment Committee; and
3) ICD-10 has been added onto the Pacing Plan based on the August 21, 2014 Compliance
Committee discussion.
7. Adjourn to Closed Session.
Motion: To adjourn to closed session at 5:59 pm.
Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin

Finance Committee of the Board
September 29, 2014
Page 3
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
8. Agenda Item 16 – Reconvene Open Session. Open session reconvened at 8:35
pm. Lily Wong, Executive Assistant, reported that the following was approved in closed
session: 1) July 28, Closed Session minutes; 2) FY2014 Summary of Physician Arrangements;
and 3) Mountain View Campus Development Plan. A motion was made to recommend approval
of the Property Planning Strategy with modification.
9. Agenda Item 17 – Physician Contracts.
Motion: To approve the following physician contracts provided that a policy be forwarded to
the Chair of the Board for discussion and to be agendized at the next meeting as to the
percentile by which physician contracts should be approved: 17a) Interventional Radiology
Renewal; 17b) OB Hospitalist; 17c) Utilization Management; 17d) Traditions Behavioral Health;
and 17e) Tele-psychiatry Contracting for ED.
Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
10. Agenda Item 18 – Long Term Financial Plan.
Motion: To approve the Long Term Financial Plan to use as guidance for the future.
Movant: Zoglin
Second: Juelis
Ayes: Chiu,, Juelis and Zoglin
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None
11. Agenda Item 19 – Recruiting New Committee Member.
Motion: To recommend that El Camino Hospital Board Director Dave Reeder and Mr. Hussain
make contact with candidate Kathy Cain.
Movant: Zoglin
Second: Juelis
Ayes: Chiu, Juelis and Zoglin
Noes: None
Abstentions: None
Absent: Hobbs and Tandon
Recused: None

Finance Committee of the Board
September 29, 2014
Page 4
14. Adjournment – There being no further business of the Finance Committee, the
meeting was adjourned at 8:39pm.
Minutes prepared by: Lily Wong, Executive Assistant
______________________________ ______________________________
Dennis Chiu Dennis Chiu
Chair, Finance Committee ECH Board Secretary

Separator Page
4b. Board and Finance Committee FY15 Period 5
Final.pptx

Summary of Financial Operations
Fiscal Year 2015 – Period 5
7/1/2014 to 11/30/2014
Date Issue: December 17, 2014

2 2 Hospital entity only, excludes controlled affiliates (1)

3 Hospital entity only, excludes controlled affiliates (1)
CMI Adjusted Discharges Gross revenues were 3.0% lower than budget for services delivered in the month of November, but 0.5% higher than budget year to date. Inpatient discharges were 1.2% above budget year to date but the case mix index was lower than current year budget and actual for same period last year. CMI adjusted discharges were 4.4% below budget for the month and -0.5% below budget for year to date. Operating Margin The loss in November brings the operating margin for the year $1.1 million behind budget. The loss is driven by lower revenues due to unfavorable payor mix and low volume. Expenses remain favorable compared to budget. Net Days in AR The AR plan is to get the 48.3 target by April 2015. AR dropped for three consecutive months ending in October but climbed in November primarily due to fewer processing days in November. November had 5 week-ends plus the thanksgiving holiday. December cash collection show that we remain on track to get to target by April.

4
ECH Operating Margin
Run rate is booked operating income adjusted for material non-recurring transactions
(1)
Hospital entity only, excludes controlled affiliates
(2) Run rate exclusions of cost report settlements, EPIC expenses, and pay for performance bonuses
(1)

5 5 Hospital entity only, excludes controlled affiliates (1)
6
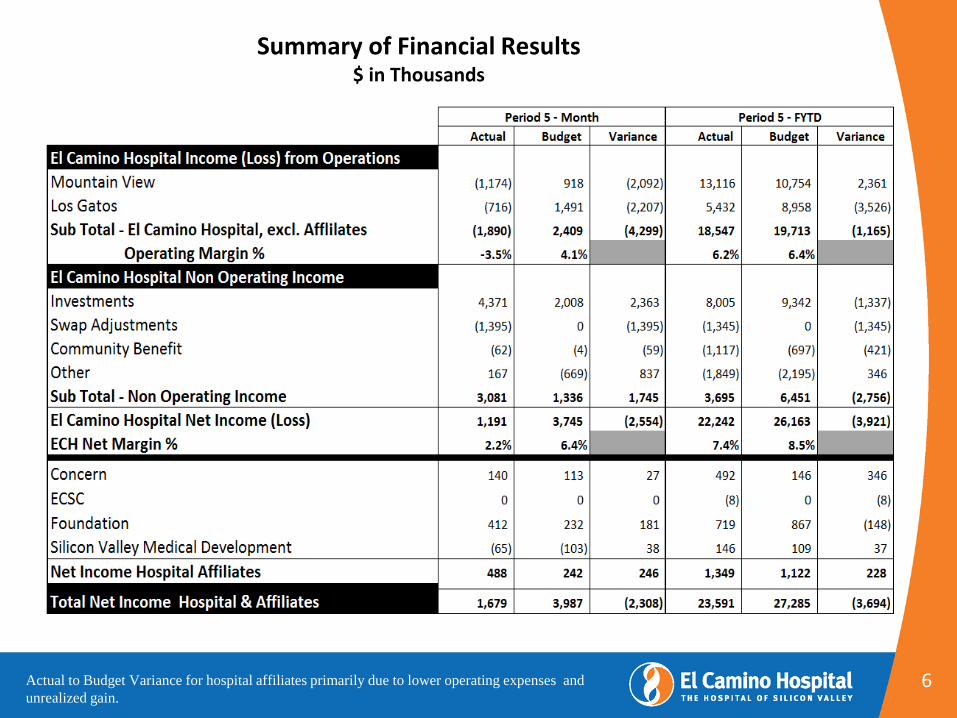
Summary of Financial Results $ in Thousands
Actual to Budget Variance for hospital affiliates primarily due to lower operating expenses and
unrealized gain.

7
Worked Hours per Adjusted Patient Day: Favorable to Budget

8
Year to date Labor Variance: $2,049,000 Favorable to Fixed Budget
- -
-3,000,000
-2,000,000
-1,000,000
0
1,000,000
2,000,000
3,000,000
4,000,000
Sitter variance – ($340,480) (58%)
RN variance - $1,519,541
All other wages – ($230,715)
Health insurance – $670,885
Incentive – ($1,806,000) - not budgeted
All other benefits – $1,330,516
Social Security-$904,974
* Positive number = Favorable to budget

9
Revenue per CMI adjusted discharge was lower than budget while Expense per CMI adjusted discharge was higher than budget
Hospital entity only, excludes controlled affiliates (1)

10
ECH Volume Statistics (1)
Hospital entity only, excludes controlled affiliates (1)
Excludes normal newborns, includes discharges from L&D (2)

11
El Camino Hospital Volume Trends
Prior and Current Fiscal Years

12 12
BAL _ SHEET
El Camino Hospital Financial Metrics Trend
Prof I t _ Loss
Operating EBITDA
lower than FYE 2014
(1)
Represents cash of $655
million
Hospital entity only, excludes controlled affiliates (1)

13
APPENDIX

14 14
YTD: 1.8% under budget YTD: 8.5% over budget
Supply Cost per CMI Adjusted Discharges
Mountain View Los Gatos
11
(1)
Hospital entity only, excludes controlled affiliates (1)

• Medicare: Due to DRG reimbursement, financial results usually improve with decreased LOS and increased CMI • Non-Medicare: Reimbursement varies; financial results usually improve when both LOS & CMI increase
15 15
Mountain View LOS & CMI Trend
(1)
Hospital entity only, excludes controlled affiliates (1)
All data excludes normal newborns (MS-DRG=795), Medicare data excludes Medicare HMOs and PPOs

• Medicare: Due to DRG reimbursement, financial results usually improve with decreased LOS and increased CMI • Non-Medicare: Reimbursement varies; financial results usually improve when both LOS & CMI increase
16 16
Los Gatos LOS & CMI Trend
(1)
Hospital entity only, excludes controlled affiliates (1)
All data excludes normal newborns (MS-DRG=795), Medicare data excludes Medicare HMOs and PPOs

El Camino Hospital Results from Operations vs. Prior Year
5 months ending 11/30/2014
17
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Mountain View Results from Operations vs. Prior Year
5 months ending 11/30/2014
18
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Los Gatos Results from Operations vs. Prior Year
5 months ending 11/30/2014
19
1(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital Results from Operations vs. Budget
5 months ending 11/30/2014
20
1
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Mountain View Results from Operations vs. Budget
5 months ending 11/30/2014
21
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Los Gatos Results from Operations vs. Budget
5 months ending 11/30/2014
22
(1)
Hospital entity only, excludes controlled affiliates (1)

23
El Camino Hospital Balance Sheet ($ Thousands)
1
(1)
Hospital entity only, excludes controlled affiliates (1)
24
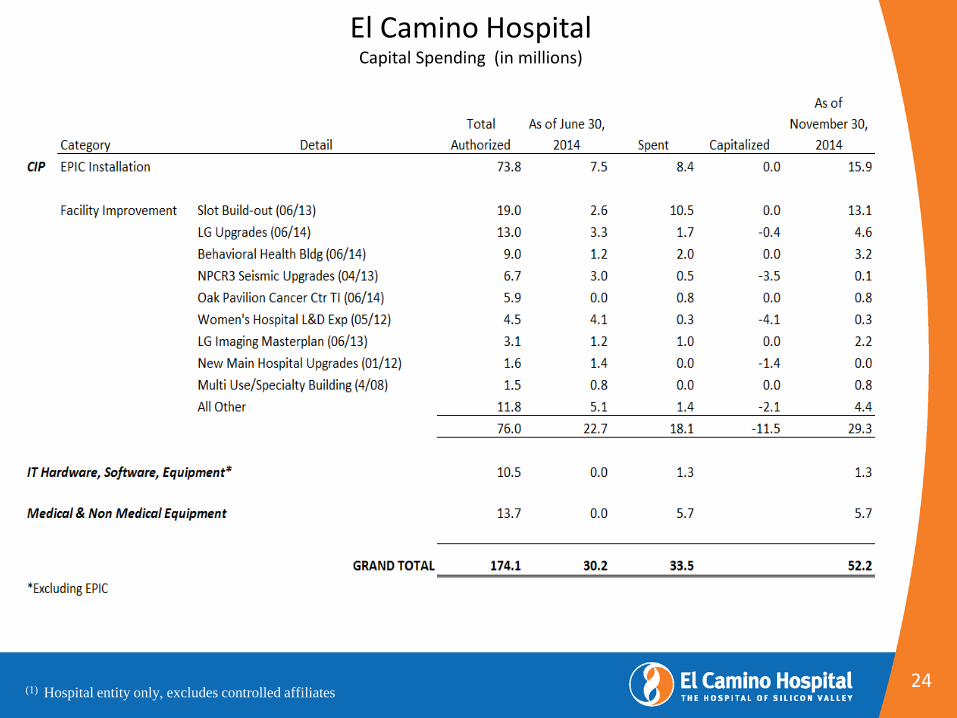
El Camino Hospital Capital Spending (in millions)
1
Hospital entity only, excludes controlled affiliates (1)

Separator Page
4c. Finance Committee Charter as Approved 11-12-
14.doc

Page 1 of 4
Finance Committee Charter
Purpose
The purpose of the Finance Committee (the “Committee”) is to provide oversight, information
sharing and financial reviews related to operating and capital budgeting, financial planning,
financial reporting, capital structure, banking relationships and certain contractual agreements for
El Camino Hospital (ECH) Board of Directors (“Board”). In carrying out its review, advisory
and oversight responsibilities, the Committee shall remain flexible in order to best define
financial strategies that react to changing conditions.
Authority
All governing authority for ECH resides with the Board and the Committee serves as an advisory
body only. The Committee will report to the Board at the next scheduled meeting any
recommendation made within the Committee’s authority. The Committee has the authority to
select, engage, and supervise any consultant it deems necessary to advise the Committee on
issues related to its responsibilities. In addition, the Committee, by resolution, may adopt a
temporary advisory committee (ad hoc) of less than a quorum of the members of the Committee.
The resolution shall state the total number of members, the number of board members to be
appointed, and the specific task or assignment to be considered by the advisory committee.
Voting members of the Committee shall include the directors assigned to the Committee and
external (non-director) members appointed to the Committee.
Membership
The Committee shall be comprised of two (2) or more Hospital Board members. The
Chair of the Committee shall be appointed by the Board Chair, subject to approval by the
Board. All members of the Committee shall be eligible to serve as Chair of the
Committee.
The Finance Committee may also include 2-3 external (non-Hospital Board member)
members with expertise which is relevant to the Committee’s areas of responsibility, such
as banking, financial management, planning and real estate development, etc.
All Committee members shall be appointed by the Board Chair, subject to approval by
the Board, for a term of one year expiring on June 30th
each year, renewable annually.
It shall be within the discretion of the Chair of the Committee to appoint a Vice-Chair
from among the members of the Committee. If the Chair of the Committee is not a
Hospital Board member, the Vice-Chair must be a Hospital Board member.

Page 2 of 4
Staff Support and Participation
The CFO shall serve as the primary staff support to the Committee and is responsible for drafting
the Committee meeting agenda for the Committee Chair’s consideration. Additional members of
the executive team may participate in the Committee meetings as deemed necessary.
General Responsibilities
The Committee’s primary role is to provide oversight and to advise the management team and
the Board on matters brought to this Committee. With input from the Committee, the
management team shall develop dashboard metrics that will be used to measure and track
financial performance for the Committee’s review. It is the management team’s responsibility to
develop and provide the Committee with reports, plans, assessments, and other pertinent
materials to inform, educate, and update the Committee, thereby allowing Committee members
to engage in meaningful, data-driven discussions. Upon careful review and discussion and with
input from management, the Committee shall then make recommendations to the Board. The
Committee is responsible for ensuring that performance metrics which are not being met to the
Board’s expectations are reported to the Board.
Specific Duties
The specific duties of the Committee are:
A. Budgeting
Review the annual operating and capital budgets for alignment with the mission
and vision of ECH and make recommendations to the Board.
Review any financial requests in excess of the CEO’s signing authority and make
recommendations to the Board.
Review ECH’s long-range forecasts and financial plans and make
recommendations to management regarding steps advisable to improve ECH’s
financial strength.
B. Financial Reporting
Review each accounting period’s financial statements and ensure the Board is
advised of any necessary corrective actions.
Obtain a clear understanding of ECH’s financial reporting process by reviewing
the hospital’s dashboard items and periodic financial reports and advise
management on how to improve its financial reporting in order to improve
accountability and ease of reading and understanding.
C. Financial Planning and Forecasting
Annually, review and evaluate ECH’s payor contracts that generate net revenues
in excess of $30m and make recommendations to management regarding

Page 3 of 4
contracting strategy. The Committee shall review management’s assessment of
expected results as well as potential risks related to the payor contracts.
Evaluate the financial implications of emerging payment processes and provide
advice to management regarding associated risk management concerns.
Evaluate financial planning and forecasting to help ensure it remains in alignment
with the mission and strategic direction of ECH.
Evaluate and make recommendations to the Board regarding any proposed
changes in corporate structure.
D. Treasury, Pension Plans & Contracting Concerns
Review and make recommendations to the Board regarding all new debt issuances
and derivative instruments in excess of $1m.
Monitor compliance with debt covenants and evaluate ECH’s capital structure.
Review and make recommendations to the Board regarding changes in banking
relationships, including, without limitation, depository accounts, investment
accounts and major credit facilities. The term “major credit facilities” does not
include management-approved trade credit facilities offered in the ordinary course
of business by vendors to the hospital. The Committee may recommend
delegation of approval authority for specified changes to the CFO, but must
maintain reporting and oversight of any such changes.
Review and make recommendations to the Board regarding proposed changes to
employee retirement plans, excluding changes to investments within those plans.
Review and make recommendations to the Board regarding contractual
agreements with persons considered to be “insiders” under IRS regulations, and
those which are in excess of the CEO’s signing authority.
E. Capital and Program Analysis
Review and make recommendations to the Board with respect to the business
plans of all capital items or proposed business ventures in excess of the CEO’s
signing authority, and all variances to budget in excess of the CEO’s signing
authority on projects in process.
Review retrospective analyses of all strategic business ventures and all strategic
capital expenditures in excess of $1 million, as presented by management or as
per the review schedule set forth by the Committee, to assess the reasonableness
of business plans that were developed at the time of original approval and to
promote learning as a result of any identified issues or concerns.

Page 4 of 4
Review and approve the acquisition or disposition of any real property which is in
excess of the CEO’s signing authority.
F. Financial Policies
Review and recommend approval of any Board-level financial policies, excluding
any financial policies for which responsibility has been specifically assigned to
another Board Committee.
G. Ongoing Education
Endorse and encourage Committee education and dialog relative to emerging
healthcare issues that will impact the viability and strategic direction of ECH.
H. Management Partnership
Work in partnership with the CFO and other hospital executives to assist in the
development of financial policies which will help ensure organizational success.
Provide ongoing counsel to the CFO regarding areas of opportunity for either
personal or organizational improvement, and annually provide a written
evaluation of the committee’s perceptions of the CFO’s performance to the CEO.
Committee Effectiveness
The Committee is responsible for establishing its annual goals, objectives and workplan in
alignment with the Board and ECH’s strategic goals. The Committee strives for continuous
improvement with regard to its processes, procedures, materials, and meetings, and other
functions to enhance its contribution to the Board.
Meetings and Minutes
The Committee shall meet at least once per quarter. The Committee Chair shall determine the
frequency of meetings based on the Committee’s annual goals and work plan and the operational
requirements of the organization. Minutes shall be kept by the assigned staff and shall be
delivered to all members of the Committee when the agenda for the subsequent meeting is
delivered. The approved minutes shall be forwarded to the Board for review and approval.
Meetings and actions of the advisory committees of the Board shall be governed by, and held
and taken in accordance with, the provisions of Article VI of the Bylaws. Special meetings of
the committees may also be called by resolution of the Board or the Committee Chair. Notice of
special meetings of the advisory committees shall also be given to any and all alternate members,
who shall have the right to attend all meetings of the Committee. Notice of any special meetings
of the Committee requires a 24 hour notice.
Approved as Revised: November 12, 2014

Separator Page
4d. ARTICLES OF INTEREST.pdf

11/18/14, 4:31 PM
Page 1 of 5http://www.modernhealthcare.com/article/20140917/NEWS/309179965?template=print
Advertisement
Safari Power SaverClick to Start Flash Plug-in
Advertisement
Advertisement
Safari Power SaverClick to Start Flash Plug-in
This copy is for your personal, noncommercial use only. You can order presentation-ready copies for distribution to your colleagues, clients or customers here or use the"Reprints" link that appears next to any article. Visit modernhealthcare.com/reprints foradditional information.
Reform Update: Anthem's Vivity alliance with
seven L.A. systems aims at Kaiser
By Melanie Evans | September 17, 2014GruberNews of anunusualjointventurebetweenAnthemBlue Crossand sevenLosAngeleshealthsystemssignalednew
competition for Kaiser Permanente, theintegrated health system with one ofCalifornia's largest insurers. It alsounderscores the eagerness across theindustry to broker novel and riskier dealsin an increasingly competitivemarketplace.

11/18/14, 4:31 PM
Page 2 of 5http://www.modernhealthcare.com/article/20140917/NEWS/309179965?template=print
Safari Power SaverClick to Start Flash Plug-in
The new company—called Vivity—willseek to replicate some of KaiserPermanente's success managing the useand cost of healthcare, but without theownership Kaiser has over its healthplans and health system. To do so,participants in the joint venture agreed toshare equally in profits and losses.
The venture will market a new healthplan to employers with no deductible andpremiums 10% below competitors,according to Anthem Blue Cross, adivision of publicly traded insurerWellPoint. Patients who select the healthplan will be limited to a select network ofproviders, which includes 6,000 doctorsand 14 hospitals. The California PublicEmployees' Retirement System agreed toinclude the Vivity network in its HMOplan.
Related Content
New California CCO Vivity willlook to Anthem for data sharing,analytics
(http://www.modernhealthcare.com/article/20140917/NEWS/309179945/new-california-cco-vivity-will-look-to-anthem-for-data-sharing)
With Kaiser in sight, Anthem creates new plan with major Californiahospitals(http://www.modernhealthcare.com/article/20140917/NEWS/309179938/with-kaiser-in-sight-anthem-creates-new-plan-with-major-california)
New Anthem network makes business case for HMO-ACO hybrid(http://www.modernhealthcare.com/article/20140917/NEWS/309179964)
Health economist Jonathan Gruber described the move as an overdue reaction toKaiser's integrated model. “When it comes to healthcare cost control, if the marketis going to solve our problems, it has to be through competing systems,” said

11/18/14, 4:31 PM
Page 3 of 5http://www.modernhealthcare.com/article/20140917/NEWS/309179965?template=print
Gruber, a professor at the Massachusetts Institute of Technology.
“For years, the question has been why hasn't this happened?” Gruber said.Hospitals and health plans lacked the incentive to more closely coordinate, he said,but the more expensive healthcare grows, the more price-sensitive consumersbecome. The move by Anthem and health systems to compete with KaiserPermanente suggests that rising healthcare prices have “reached the breakingpoint,” Gruber said.
The Patient Protection and Affordable Care Act's new insurance markets andpublicly reported premium prices have also made consumers more aware of price,giving plans and providers more incentive to find new ways to compete on cost, hesaid.
The network of seven health systems joining hands with Anthem—Cedars-SinaiHealth System, Good Samaritan Hospital and UCLA Health, all in Los Angeles;Huntington Memorial Hospital, Pasadena; Memorial Medical Center, Torrance;MemorialCare Health System, Fountain Valley; and PIH Health, Whittier—will work tocoordinate medical care for patients and manage medical costs.
Click to enlarge.But success will require clear communication and tightcoordination of medical care across sevenindependent health systems, something with whichsingle health systems struggle. Kaiser Permanente'sadvantage here is clear. “There are seven differentways of doing things,” said Steve Valentine, presidentof the Camden Group, a consulting firm based in LosAngeles.
Kaiser officials touted their organization's integrationas an advantage after Wednesday's announcement. “The fact that our system is notjust stitched together from existing parts, but has actually been built with thisintegration as the goal, will be difficult for others to copy," said Peter Andrade,senior vice president of California sales and account management for Kaiser.
Anthem and its partner health systems risk losses unless all members perform well.Profits and losses will be shared equally among the members, said Anthem's PamKehaly.
The participants' shared earnings or losses on the venture will depend on whatremains of the premium revenue after medical and administrative expenses. Theplan will be marketed to fully insured employer groups starting Oct. 1 and may

11/18/14, 4:31 PM
Page 4 of 5http://www.modernhealthcare.com/article/20140917/NEWS/309179965?template=print
expand into California's health insurance exchange--but not before the partnersgain experience.
“We want to be purposefully small,” she said. “We don't want it to fail right off thebat.” Anthem may eventually expand the approach to other markets.
The model is similar to accountable care contracts that have emerged in the privateinsurance market and in Medicare under the Affordable Care Act. Accountable careties financial incentives to targets for reduced health spending and quality. ACOsunder Medicare have struggled to slow spending(http://www.modernhealthcare.com/article/20140916/NEWS/309169938/medicare-acos-improve-quality-have-mixed-results-on-slowing-spending) enough to earn incentivepayouts.
“That is a pretty bold play,” said Leemore Dafny, former deputy director forhealthcare and antitrust with the Federal Trade Commission and professor withNorthwestern University's Kellogg School of Management. “It's not obvious howthey're going to reduce hospital occupancy and come out on top.”
Click to enlarge.The partners' willingness to enter into such a riskyagreement reflects the mounting pressure faced byhealth insurers, hospitals and doctors to blunt risingmedical costs. The Patient Protection and AffordableCare Act, too, has created new incentives, increasedprice transparency and created a new market for thenewly insured.
“The current market is in such turmoil that people arewilling to agree to a lot of things,” said Mark Pauly, a
professor of health management at the University of Pennsylvania. “They don'tknow where history is going to end up, but they want to end up on the right side ofhistory. It's made hospitals a lot more willing to agree to things that they mighthave rejected out of hand.”
That turmoil is apparent in joint ventures, mergers and acquisitions across theindustry. Recent deals have created new regional mega-systems, such as theproposed merger of Advocate Health Care and NorthShore University HealthSystem (http://www.modernhealthcare.com/article/20140913/MAGAZINE/309139964) in theChicago suburbs. Others have united rivals under new joint ventures to operatehealth systems, health insurers or post-acute care, as has been the case with astring of recent agreements secured by Ascension Health. One, for example, willunite Michigan hospitals owned by Ascension Health and CHE Trinity Health to

11/18/14, 4:31 PM
Page 5 of 5http://www.modernhealthcare.com/article/20140917/NEWS/309179965?template=print
jointly contract(http://www.modernhealthcare.com/article/20140726/MAGAZINE/307269952/ascensions-anthony-tersigni-on-accountability-integrity) across the entire state.
Accountable care: More results, little change
The CMS released the latest look at Medicare accountable care this week(http://www.modernhealthcare.com/article/20140916/NEWS/309169938) , with a report ofACOs performance on savings and quality targets. The report captured update andnew results for ACOs through the end of 2013. The mixed performance is similar touneven results for Medicare ACOs reported in January. Of the roughly 250 MedicareACOs, one-quarter earned bonuses based on performance. The bonuses totaled$445 million. Medicare saved another $372 million. Scores for quality improved formany measures. Pioneer ACOs, a small group that Medicare's Innovation Centerrecruited to test accountable care, saw an average increase in performance scoresof about 15% across 33 measures. ACOs in the larger Medicare Shared SavingsProgram improved performance on 30 of 33 quality measures, though CMS did notrelease additional details.
Follow Melanie Evans on Twitter: @MHmevans
Tags: Accountable Care Organizations, Acquisitions, Antitrust, Costs, Deals,Healthcare Reform, Medicare, Mergers
Advertisement
Copyright © 1996-2014 Crain Communications, Inc. (http://www.crain.com/)

Separator Page
4d2. Kaiser Permanente's Q1 profits soar 44 percent, to
$1.1 billion - San Francisco Business Times.pdf

11/18/14, 4:26 PMKaiser Permanente's Q1 profits soar 44 percent, to $1.1 billion - San Francisco Business Times
Page 1 of 2http://www.bizjournals.com/sanfrancisco/blog/2014/05/kaiser-permanente-q1-profits-kathy-lancaster.html?s=print
From the San Francisco Business Times:http://www.bizjournals.com/sanfrancisco/blog/2014/05/kaiser-permanente-q1-profits-kathy-lancaster.html
Kaiser Permanente's Q1 profits soar 44percent, to $1.1 billionMay 9, 2014, 1:04pm PDT Updated: May 9, 2014, 3:43pm PDT
Chris RauberReporter- San Francisco Business TimesEmail | Twitter | LinkedIn
Kaiser Permanente is sitting on a pile of first-quarter profits, up nearly 44 percent from a yearago at $1.1 billion.
Its Kaiser Foundation Hospitals, Kaiser Foundation Health Plan Inc. and subsidiaries reportedbig positives on all fronts May 9 for the year's first quarter, ending March 31.
Like other big health care systems locally and nationally, Kaiser is chanting the mantra ofaffordability and cost-reduction, as it moves to take advantage of and adjust to the opportunitiesand demands of health reform under President Barack Obama's Affordable Care Act.
Other major data points announced by Kaiser Friday:
Operating revenue climbed 6 percent, from a restated $13.1 billion last year to $13.9 billionin 2014's first quarter. (Last spring, Kaiser said it posted $13.3 billion in operating revenue in2013's first quarter.)Operating profits soared 49 percent, to $822 million from $551 million in 2013.Non-operating income jumped 44 percent, to $324 million from $219 million.Enrollment jumped 243,000 to 9.3 million systemwide, with three-quarters of those newenrollees coming through Covered California and other Obamacare exchanges.
Kathy Lancaster, the Oakland-based nonprofit system's CFO and executive vice president, said theQ1 results show that Kaiser is becoming more efficient without hurting quality.
"Reducing our cost trends allows us to be more affordable to our members (enrollees) andcustomers (employers)," Lancaster noted.

11/18/14, 4:26 PMKaiser Permanente's Q1 profits soar 44 percent, to $1.1 billion - San Francisco Business Times
Page 2 of 2http://www.bizjournals.com/sanfrancisco/blog/2014/05/kaiser-permanente-q1-profits-kathy-lancaster.html?s=print
Kaiser spent $827 million on capital projects in the quarter, compared to $779 million a year ago,as it nears completion on three huge Northern California hospital construction projects, in Oakland,Redwood City and San Leandro, and another new hospital in Harbor City down south.
Tom Meier, Kaiser's treasurer and senior vice president, said those projects will bring all of thesystem's California hospitals into full compliance with the state's seismic safety requirements foracute-care facilities.
Down the road, however, Kaiser will continue to spend large sums on new outpatient sites and onhealth information technology, so overall capital spending is not expected to decline significantly incoming years, Meier told the Business Times. "You're not going to see a significant change," hesaid. "It will come down, but it's not going to be dramatic."
For example, Meier said, eight new medical office buildings came online during the first quarter,including five in California (in Oakland, Tustin Ranch, Oceanside, Pasadena and Victorville).
Chairman and CEO Bernard Tyson noted that the system's performance so far this year "gives meadded confidence that we will deliver more affordable pricing and greater value in 2015 andbeyond."
In mid-February, the California-based giant reported posting $2.7 billion in 2013 profits, on $53.1billion in operating revenue.
Chris covers health care, insurance, nonprofits and the wine industry.

Separator Page
6. ICD-10 Presentation 012615.ppt

ICD-10 Implementation
January 26, 2015 Frank Kuziel, RHIA Director Health Information Management

2
ICD-10 Steering Committee Chart
Contracts Patient
Financial
Services
Clinical
Documentation
Improvement
Information
Services
Health
Information
Management
Patient
Access/
Registration
Medical
Staff
Administration
(Admin champion)
ECH
Education
Coding
ICD-10 Physician
Education Sub-
committee

3
ICD-10 Awareness
Detailed organization plan initiated
Assessment of ECH ICD-10 preparations
Continued physician and HIM coder education
Final assessment of areas of ICD-10 risk and risk mitigation
Final preparation before go-live
Go-live across the U.S.
Post go-live
2012-13
2013
Spring 2014
Fall 2014
Spring 2015
Summer 2015
2016
El Camino ICD-10 Preparedness
A high level
presentation
of ICD-10,
explaining
the need and
the general
description
Due to
government
announced
postponement
of ICD-10 go-
live, ECH
ICD-10
preparedness
reassessed
for readiness
Continued
monitoring of
ICD-10
education for
medical staff
and HIM coding
staff.
Completion of
software
upgrades to
HIM coding, 3M
360 Computer
Assisted Coding
Comparative
data retrieved
from dual
coding
identifying
areas of risk
with physician
documentation.
Contracts dept.
to use data for
contract
renegotiation
with major
payers.
Intensive
physician
preparation
for ICD-10
readiness,
recheck of
software and
workflow
processes in
HIM and
PFS. ICD-10
training for
hospital
employees
Coding and
Billing
activated in
ICD-10.
Additional
coding staff
on standby
to address
any coding
slowdown
Assessment of
physician
specificity in
documentation,
to include further
educational
sessions as
needed,
monitoring of
claims, denials
and system
effectiveness
ICD-10 Steering
Committee
implemented to
assess
systems,
hardware,
overall risk and
identification of
key
stakeholders
involved and to
prepare for
implementation
Impact Assessment
Implementation Preparation
Go-Live Preparation
Post Go-Live
ICD-10
on
Hold
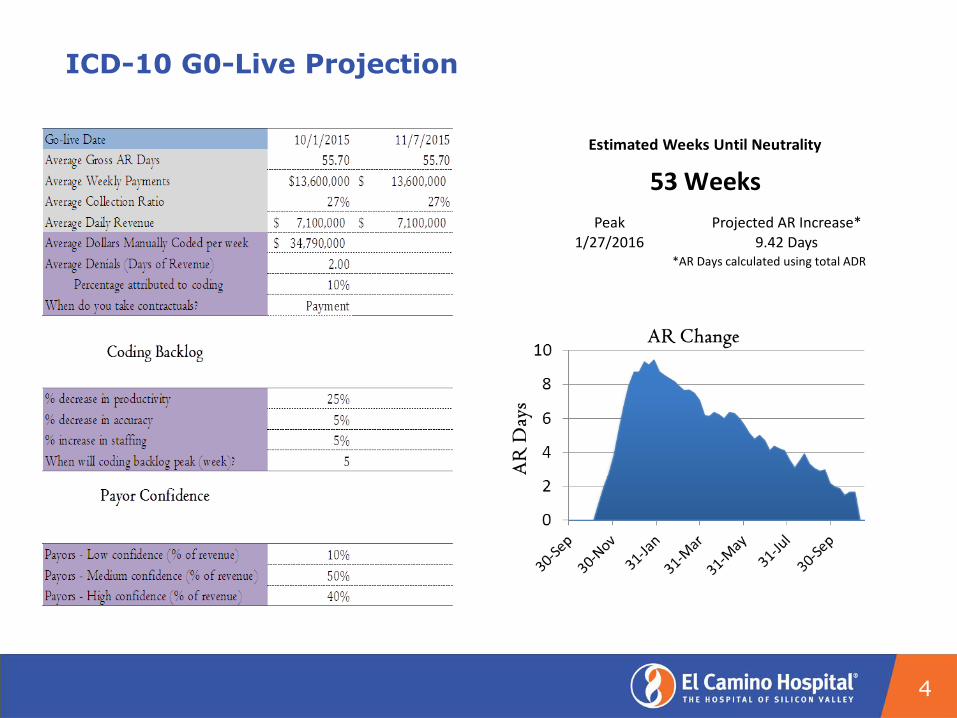
ICD-10 G0-Live Projection
4
Peak Projected AR Increase* 1/27/2016 9.42 Days
*AR Days calculated using total ADR
Estimated Weeks Until Neutrality
53 Weeks
ICD-10 Completed Objectives:
• 76% providers have completed training at ECH or at another facility
• HIM coding staff are fully trained in ICD-10
• 3M 360 computer assisted coding operational
• 3M ICD-10 upgrade for dual coding, in-progress to begin March 2015
• Contracts department preparing to negotiate with health plans to
neutralize any decrease in net revenue ensuring payment the same
amount as negotiated before ICD-10 implementation
• PFS prepared for monitoring of denials, rejected claims and payments
due to ICD-10
• Physician training to continue in ICD-10 with individualized courses in
Healthstream Precyse training modules, small group and 1:1 training
sessions. HIM clinical documentation/coder staff available for physician
1:1 and department assistance to begin in late March
• Individual provider documentation to be audited by HIM to ensure
documentation is adequate for ICD-10 coding/billing needs
5

Questions?
6

Separator Page
7. Board and Finance Committee FY15 Period 6.pptx
Summary of Financial Operations
Fiscal Year 2015 – Period 6
7/1/2014 to 12/31/2014
Date Issue: January 20, 2014

2 2 Hospital entity only, excludes controlled affiliates (1)

3 Hospital entity only, excludes controlled affiliates (1)
Volume – Discharges recovered from the November low; MV deliveries were very strong. For the year, discharges were 3.8% above prior and deliveries are 1.8% higher. Operating Margin December operating margin was at budget with the exception of $5 million IGT payment that was delayed to January. For the year, excluding IGT, operating margin is $500,000 below budget. The loss is driven by lower revenues due to unfavorable payor mix . Expenses remain favorable compared to budget. Net Days in AR The AR plan is to get the 48.3 target by April 2015. In December, receivables decreased by $4.5 million and net days in A/R decreased by 3 days to 51.7

4
ECH Operating Margin
Run rate is booked operating income adjusted for material non-recurring transactions
(1)
Hospital entity only, excludes controlled affiliates
(2) Run rate exclusions of cost report settlements, EPIC expenses, and pay for performance bonuses
(1)

5 5 Hospital entity only, excludes controlled affiliates (1)

6
Summary of Financial Results $ in Thousands
Actual to Budget Variance for hospital affiliates primarily due to lower operating expenses and
unrealized gain.

7
Worked Hours per Adjusted Patient Day: Favorable to Budget

8
Year to date Labor Variance: $3,581,000 Favorable to Fixed Budget
- -
-3,000,000
-2,000,000
-1,000,000
0
1,000,000
2,000,000
3,000,000
4,000,000
Sitter variance – ($360,486) (51%)
RN variance - $1,868,522
All other wages – $555,400
Health insurance – $659,564
Incentive – ($1,884,741) - not budgeted
All other benefits – $1,488,157
Social Security-$1,254,972
* Positive number = Favorable to budget

9
Revenue per CMI adjusted discharge was lower than budget while expense per CMI adjusted discharge is favorable
Hospital entity only, excludes controlled affiliates (1)

10
ECH Volume Statistics (1)
Hospital entity only, excludes controlled affiliates (1)
Excludes normal newborns, includes discharges from L&D (2)

11
El Camino Hospital Volume Trends
Prior and Current Fiscal Years

12 12
BAL _ SHEET
El Camino Hospital Financial Metrics Trend
Prof I t _ Loss
Operating EBITDA
lower than FYE 2014
(1)
Represents cash of $673
million
Hospital entity only, excludes controlled affiliates (1)
13
APPENDIX

14 14
YTD: 0.3% under budget YTD: 7.7% over budget
Supply Cost per CMI Adjusted Discharges
Mountain View Los Gatos
11
(1)
Hospital entity only, excludes controlled affiliates (1)

• Medicare: Due to DRG reimbursement, financial results usually improve with decreased LOS and increased CMI • Non-Medicare: Reimbursement varies; financial results usually improve when both LOS & CMI increase
15 15
Mountain View LOS & CMI Trend
(1)
Hospital entity only, excludes controlled affiliates (1)
All data excludes normal newborns (MS-DRG=795), Medicare data excludes Medicare HMOs and PPOs

• Medicare: Due to DRG reimbursement, financial results usually improve with decreased LOS and increased CMI • Non-Medicare: Reimbursement varies; financial results usually improve when both LOS & CMI increase
16 16
Los Gatos LOS & CMI Trend
(1)
Hospital entity only, excludes controlled affiliates (1)
All data excludes normal newborns (MS-DRG=795), Medicare data excludes Medicare HMOs and PPOs

El Camino Hospital Results from Operations vs. Prior Year
6 months ending 12/31/2014
17
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Mountain View Results from Operations vs. Prior Year
6 months ending 12/31/2014
18
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Los Gatos Results from Operations vs. Prior Year
6 months ending 12/31/2014
19
1(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital Results from Operations vs. Budget
6 months ending 12/31/2014
20
1
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Mountain View Results from Operations vs. Budget
6 months ending 12/31/2014
21
(1)
Hospital entity only, excludes controlled affiliates (1)

El Camino Hospital – Los Gatos Results from Operations vs. Budget
6 months ending 12/31/2014
22
(1)
Hospital entity only, excludes controlled affiliates (1)

23
El Camino Hospital Balance Sheet ($ Thousands)
1
(1)
Hospital entity only, excludes controlled affiliates (1)

24
El Camino Hospital Capital Spending (in millions)
1
Hospital entity only, excludes controlled affiliates (1)