ahead of the game: keeping up with sports concussion matthew s. reeves, do, caqsm scott schroeder,...
TRANSCRIPT
Ahead of the Game:Keeping Up with Sports Concussion
Matthew S. Reeves, DO, CAQSMScott Schroeder, MSPT, LAT, ATC
August 13, 2013

Ahead of the Game: Keeping Up with Sports Concussion
Matthew S. Reeves, DO, CAQSM
Scott Schroeder, MSPT, LAT, ATC
August 13, 2013
Housekeeping
• Thank you for being here!
• DisclosureTonight’s speakers have no financial or other conflicts of interest to disclose in regards to the topic presented today
Remember these three words (but do not write down!!)

Speaker Background
Matthew S. Reeves, DO, CAQSM
• Board Certified and Licensed Primary Care Physician
• Fellowship trained in Sports Medicine
• 20+ years experience working with sports-related concussion and other sports related injuries and illnesses
Scott Schroeder, MSPT, LAT, ATC
• Certified and Licensed Athletic Trainer
• Licensed Physical Therapist
• 20+ years experience working with sports-related concussion and other sports related injuries and illnesses
Objectives• Differentiate between fundamental concussion related
fact and fiction
• Discuss the current Indiana state law related to sports concussion and its proposed amendments
• Discuss the process for diagnosing a concussion
• Discuss the most up to date treatment options for concussion
• Explain the currently accepted best practice process for return to school, sports and/or work after concussion
• Answer questions related to concussion
• Get audience feedback related to community understanding of sports related concussion its management

Introduction

“I’m a big football fan, but I have to tell you, if I had a son, I’d have to think long and hard before I let him play football.”
Barack Obama President of the United
States Interview with New
Republic January 27, 2013

“Interesting. I do have boys and I’m thinking long and hard about them getting near politics. No problem them playing football.” Tony Boselli
Former NFL PlayerTwitterJanuary 28, 2013
Concussion vs. Head Injury
• Square vs. Rectangle
• Concussion is one of many types of head injury
• Head injuries– Lacerations, fractures, bleeds,
aneurysm, etc.

What is a concussion?
• A brain injury caused by a traumatic force
• May be caused by a blow to the head, face, neck, or elsewhere on the body with force transmitted to head
• May also be a result of hitting a hard surface, player collisions or being hit by equipment

What is a concussion?
Getting “dinged” or having your “bell rung”
IS
a concussion!

“Common Knowledge”
• Many misconceptions about concussion– Examples from 2003 study:
•42% of respondents believed that sometimes a second blow to the head can help a person remember things that were forgotten
•66% of respondents believed that the only sure way to tell if someone has suffered brain damage from a head injury is by an x-ray of the brain
•28% of respondents believed that a concussion is harmless and never results in long term problems or brain damage
Concussions Facts
• ALL concussions are serious
• Often occur without loss of consciousness (<10% of cases) or obvious signs
• Can occur in ANY sport
• Can occur in game, practice or outside of sports
• Can occur in athletes of any age

Concussions Facts
• Athletes can get a concussion even when wearing proper equipment (including a helmet)
• Athletes often don’t report symptoms due to sense of responsibility to their team, peer pressure or fear of losing playing time
• Identification and proper, early response can help prevent additional injury or even death (second impact syndrome)

Second Impact Syndrome
• Results from a “second blow” when athlete is still recovering from initial concussion
• Often times is NOT a hard impact
• Causes rapid onset of brain swelling, increased intracranial pressure, ischemia (oxygen loss) and permanent brain injury
• Can lead to death or permanent
disability
• Most common in immature brain– High School age and younger
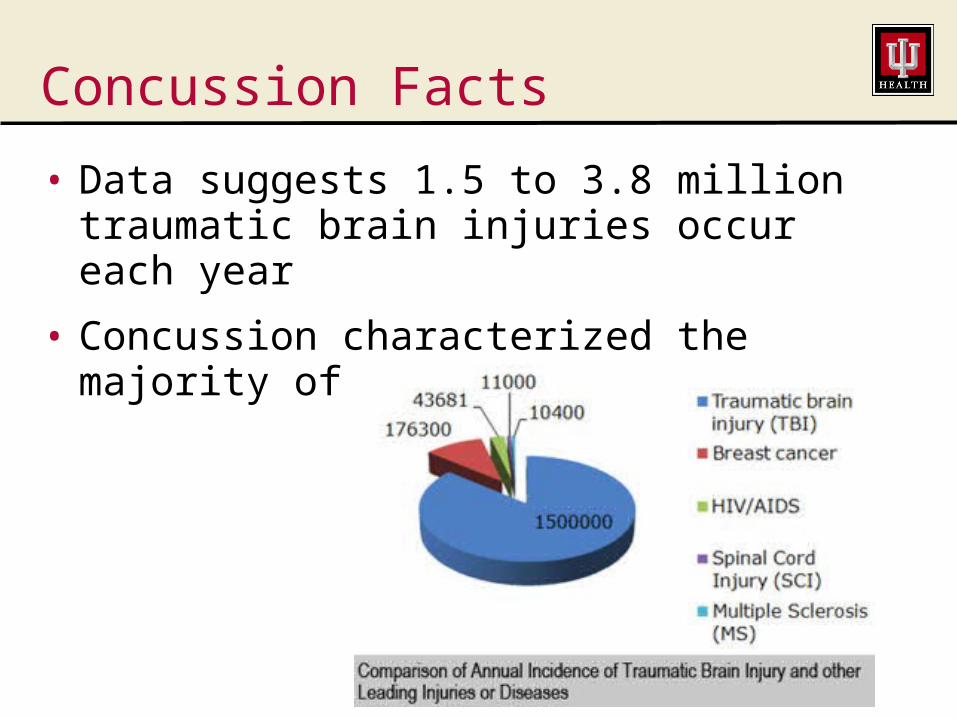
Concussion Facts
• Data suggests 1.5 to 3.8 million traumatic brain injuries occur each year
• Concussion characterized the majority of these – about 75%

Concussion Facts
• The pediatric (18 and younger) brain vs. the adult brain– More vulnerable to concussions– Longer recovery from concussion– More vulnerable to repeated
concussions– More susceptible to second impact
syndrome
Concussion Facts
• At risk populations– Female gender– Pediatric (age 18 and younger)– Mood Disordered– Learning Disorders– Migraine Sufferers– Family History– Fatigue– Apolipoprotein E Promoter Gene (G-219T
TT subtype)– Those Recovering from Recent Concussion

Concussion Facts
• Risk factors for prolonged recovery– ADD/ADHD– Learning disabilities– Anxiety disorder– Depression– Emotional/behavioral/conduct disorders– Seizure disorders– Previous concussion– History of headaches (migraines
especially)

Recognizing a Concussion
• Watch for these things
– A forceful blow to the head or body leading to rapid movement of the head
– Any change in the student-athlete’s behavior, thinking or physical function

Signs observed by others
• Dazed/confused appearance
• Clumsy movement or balance problems
• Slurred speech/slow response
• Loss of consciousness (even brief)
• Memory loss• Behavior/personality
change

Symptoms reported by Athlete
• Headache
• Nausea/vomiting
• Dizziness/balance problems
• Vision problems
• Light/noise sensitivity
• Concentration/memory problems
• Confusion
• Feel foggy/groggy/hazy/sluggish
• Doesn’t “feel right”

Preparation/Prevention** Can’t absolutely prevent concussion – can minimize risk
• What you can do– Know concussion signs and symptoms– Recognize potential for harm specific to the
activity– Use the proper protective equipment, check
for proper fit of equipment, understand safe sports technique
– Know and follow the process for return to activity• Don’t return too early!
• Safety First– Athletes should use safe-play techniques and
follow the rules– Athlete should immediately report symptoms
of concussion either in themselves or a teammate

Avalanche of State Legislation
• Since 2009, 44 states and the District of Columbia have passed legislation designed to reduce the overall impact of concussion/traumatic brain injuries in young athletes
• Most revolve around 3 core elements– Annual education for athletes and parents– Mandatory removal from play if
concussion suspected– Clearance by a designated health
professional before able to return to play
Zack Lystedt• In large part because of his case, the first
concussion law was passed in the state of Washington– 2006 suffered a concussion playing football– Returned pre-maturely to play– Collapsed after the game and had
emergency surgery– Suffered numerous strokes, spent 7 days on
ventilator and 3 months in a coma; then spent 4 weeks in a nursing home followed by 2 months in children’s rehab hospital

Zack Lystedt
• Life changed irrevocably– 13 months before he moved an arm or
leg– Spent 20 months on a feeding tube– Nearly 3 years before Zack would stand
(with assistance) on his own 2 feet

Indiana’s Law
• IC 20-34-7– Athletes and parents/guardians must be
provided with concussion information then sign and return a form acknowledging receipt of the information
– Athletes will be removed from play (practice or game) if suspected of having a concussion
– To return to play, require written clearance from a licensed healthcare provider trained in the management of concussions and head injuries
– Addresses high school age athletes

Indiana’s Law
• Proposed Amendments– Expand to include all athletes less than
20 years of age– Mandate annual coach education– Organizing entity defined as any school
that sponsors athletic activity or any non-profit or for-profit entity that uses school property for an athletic activity

Knowing What We Don’t Know
• There are many things we still don’t know
• Some questions answered, but many new questions have been identified
• The practice of concussion care continues to evolve
• In the absence of definitive evidence, we use the best evidence available and err on the side of conservative care (especially in young athletes)

Concussion Publications by Decade:1970s to Current
826
113323323
248
195195
60605577
13023
12
Modified from: Philip Schatz PhD, St. Joseph’s University
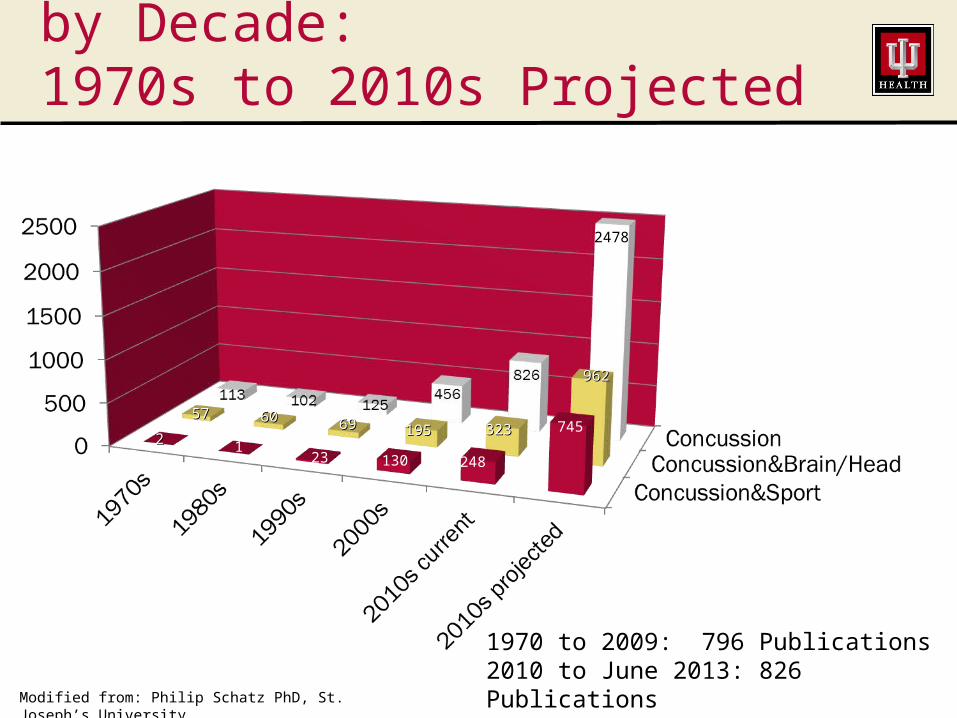
Concussion Publications by Decade:1970s to 2010s Projected
2478
195195
130
323323
248
6969
23
6060
1
5757
22
962962
745
1970 to 2009: 796 Publications2010 to June 2013: 826 Publications2010 to 2019 projected: 2478 Publications
Modified from: Philip Schatz PhD, St. Joseph’s University
Preparation, Identificationand
Medical Management
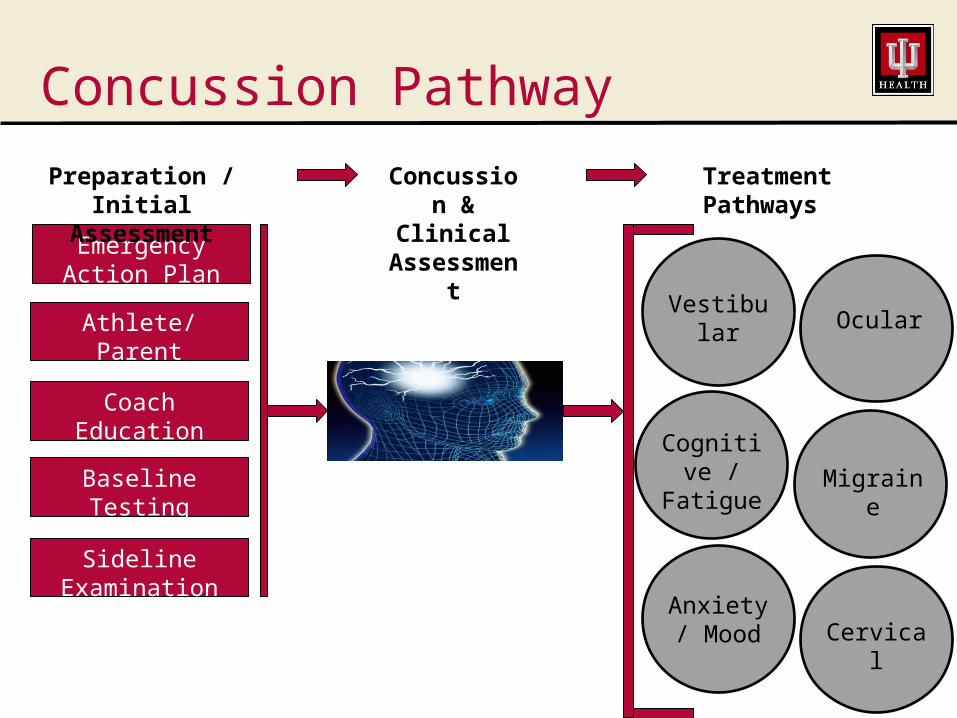
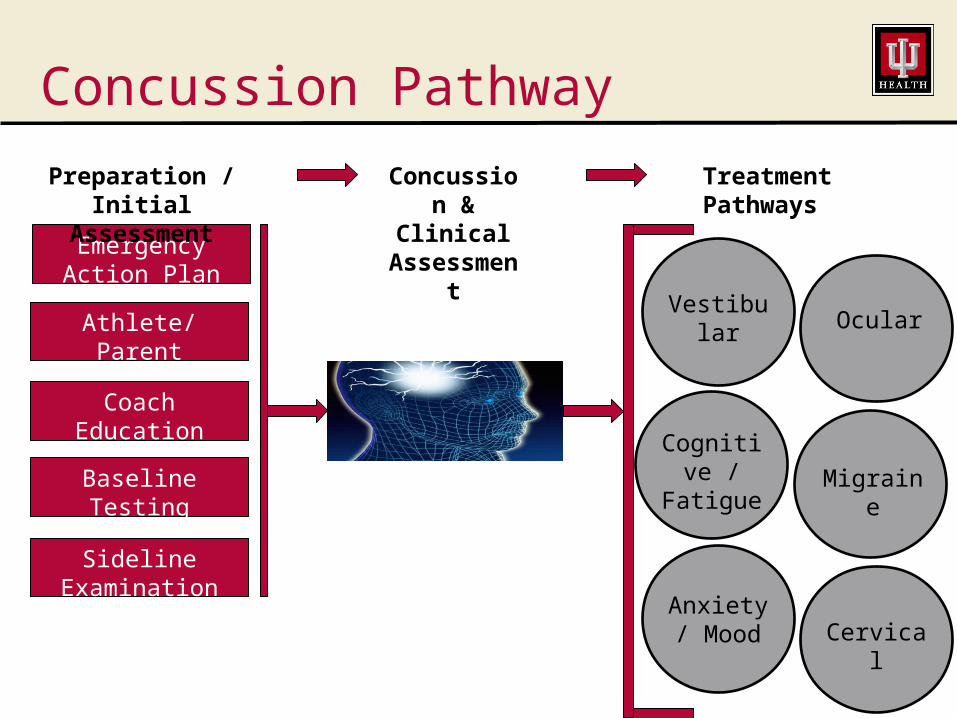
Concussion Pathway
Athlete/ParentEducation
Coach Education
Baseline Testing
Emergency Action Plan
Sideline Examination
Preparation / Initial
Assessment
Concussion &
Clinical Assessme
nt
Treatment Pathways
Vestibular Ocular
CervicalAnxiety /
Mood
Cognitive /
FatigueMigraine

Emergency Action Plan (EAP)
• A written blueprint for how to handle emergency situations
• Establishes a situation based plan, identifies who carries out duties
• Helps to ensure efficient and appropriate care is delivered

Athlete/Parent Education
• Helps parties understand what concussions are and what the course of care might be

Coach Education
• Helps coaches understand what to look for, especially when no medical personnel are available
• Clarifies the standards for removal from and return to play

Baseline Testing
• Used to determine pre-injury status; can be compared with testing after injury to determine severity of injury and track progress
• Components include:– Pre-participation screen– Symptom checklist– Neurocognitive testing– Balance testing

Baseline Testing:Pre-Participation Screen
• Commonly called “physicals”
• Not as involved or thorough as a true “physical” and should not be used as a replacement for one
• Identifies medical conditions that may indicate increased risk of concussion
• History of previous concussions
• List of current medications

Baseline Testing:Symptom Type and Severity Measure
• To determine the type and nature of pre-injury symptoms if present
• Included in neurocognitive testing as well as pencil and paper test
Baseline Testing:Neurocognitive Testing• We use ImPACT™ Test
– Computer based– This is currently done for contact
intensive sports; parents can request baseline testing for other sports
– Re-test if concussion occurs– Measures symptoms and scores
severity– Measures attention, memory,
processing speed and reaction time.
– Assists healthcare providers with return to play decisions (not the only factor in determining when to return to full activity)
– Automatically compares to “norms” and individual “baseline”

Baseline Testing:Balance
• Recent research has indicated that this an important component to consider with baseline testing
• Working to add this component to what we are doing with baseline testing
• Multiple ways to assess; we are working on finding the best test for the circumstances

Sideline Examination
• Goal: To identify signs or symptoms that indicate the possibility of concussion or more serious injury
• Multiple standardized examination forms available– ACE, SCAT2, SCAT3, SAC, MACE
• Should consider physical, cognitive and emotional symptoms and impairments
If a concussion is suspected:
• Remove from activity– “When in doubt, sit them out”
• Educate on immediate concussion management– Take home sheet
• Early evaluation by licensed healthcare professional with training in the identification and management of head injuries– Rule out other serious head injuries
Who are the “appropriate health care professionals”?
Appropriate healthcare professionals are those with specialized backgrounds in the management of sports injury/concussion
•Sports medicine physicians
•Licensed athletic trainers
•Healthcare providers (Physicians, physician assistants, nurse practitioners, etc.) with concussion management training

Clinical Examination
• Symptoms
• Cranial nerve function
• General musculoskeletal examination
• Neurocognitive performance (ImPACT™ test)
• Balance
• Vestibular/Ocular function
• Imaging tests?
Symptoms
• First thing addressed in clinical examination
• Typically are divided in to 4 categories– Physical Symptoms– Cognitive Symptoms– Emotional Symptoms (frontal impact
concussions)– Sleep

Physical Symptoms
• Headache
• Dizziness
• Nausea
• Impaired Balance
• Tinnitus
• Fatigue
• Light Sensitivity
• Blurred or Double Vision
Emotional Symptoms and SleepDysfunction
• Depression or Anxiety
• Mood Changes (degree and speed)
• Irritability
• Sadness
• Nervousness
• Sleep Pattern Changes
Cognitive Symptoms
• Amnesia
• Disorientation
• Confusion
• Impaired Concentration
• Impaired Reasoning
• Impaired memory

Cranial Nerve Function
• Tests motor functions throughout the body and gives us a window to see what is going on in the brain
• Helps to rule out other significant injuries
• Tests might include -
General Musculoskeletal Examination
• Screen for associated injuries, initially unrecognized due to focus on head
• Neck – headache and pain may be from here, not concussion
• Other brain injuries may affect musculoskeletal function throughout the body
Neurocognitive Function
• Compare to baseline or normative data if available
• ImPACT™
• Used to assess memory, reaction time, processing of information, judgment
• Tests might include: serial 7, months in reverse
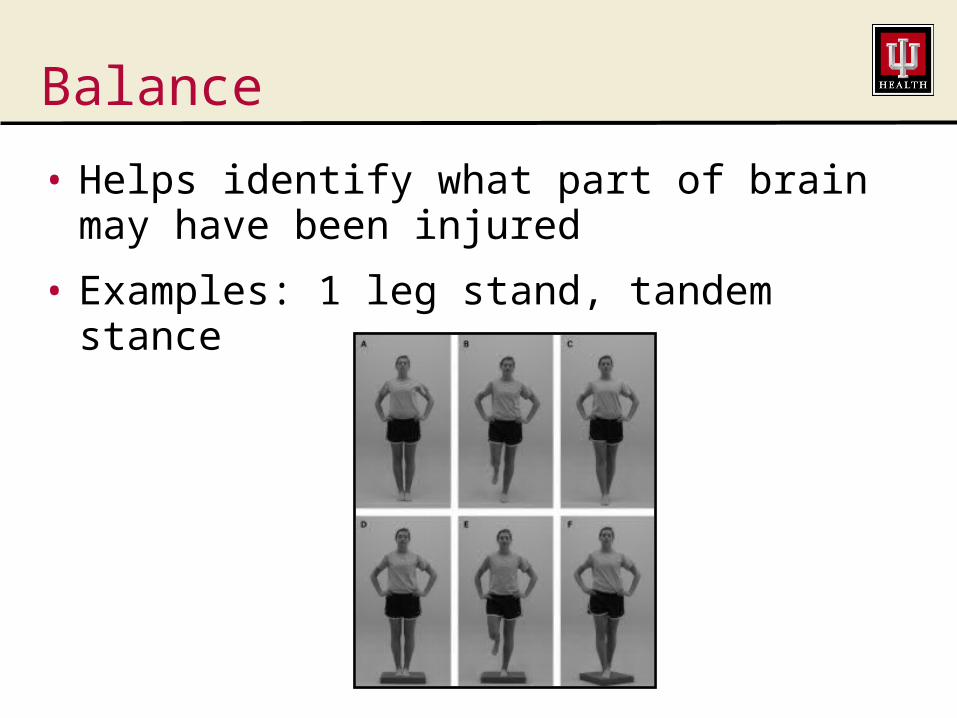
Balance
• Helps identify what part of brain may have been injured
• Examples: 1 leg stand, tandem stance

Vestibular/Ocular Function
• Helps more clearly define the nature of the deficit or lesion
• Helps to clarify the course of treatment
Imaging Tests
• Used to rule out certain life threating or other severe injuries
• Identify structural lesions
• Structural vs metabolic injury
• If you are told you don’t have a concussion because the your standard CT, CAT scan or MRI is normal …

Immediate Medical Treatment
• Cognitive rest
• Reduced school work
• Physical rest
• Limit TV, computer, video games, texting, phone
• Confer when safe to drive, ride bike
• Tylenol ONLY – Not ibuprofen type drugs
• NO alcohol
• NO narcotics, blood thinners, drugs that cause drowsiness

School Considerations
• May need to be excused from school initially or until symptoms are very mild
• Consider postponing exams
• Consider a reduced school day
• Allowances for reduced/no homework
• Ask teachers to notify parent if athlete can’t reasonably focus in class or has change in behavior or reported symptoms
Post Concussive Syndrome
• Ill-defined term
• Ambiguity leads to imprecision and variability in study
• Characterized by persistence of symptoms longer than would be expected– Typically defined as symptoms greater
than 3 months after injury– In athletes or very active may consider
the threshold of 3-6 weeks

Medication Interventions
• Used for prolonged or severe symptoms (usually begin 3-6 weeks after injury)
• Based on categorization of symptoms– Physical: Lexapro, Zoloft, Amytriptyline– Emotional: Lexapro, Zoloft– Cognitive: Amantadine, Methylphenidate– Sleep: Melatonin, Trazodone
• Recommend being off medications prior to return to activity

When OK to return to sports/activity?
• Return to baseline symptoms at rest AND
• Physical examination is normal AND
• Satisfactory results of brain function with neurocognitive testing (ImPACT™ test) AND
• Successfully completes structured exertion reintegration program AND
• When cleared by a licensed healthcare professional trained in the evaluation and management of concussion

Rehabilitation
Concussion Pathway
Athlete/ParentEducation
Coach Education
Baseline Testing
Emergency Action Plan
Sideline Examination
Preparation / Initial
Assessment
Concussion &
Clinical Assessme
nt
Treatment Pathways
Vestibular Ocular
CervicalAnxiety /
Mood
Cognitive /
FatigueMigraine
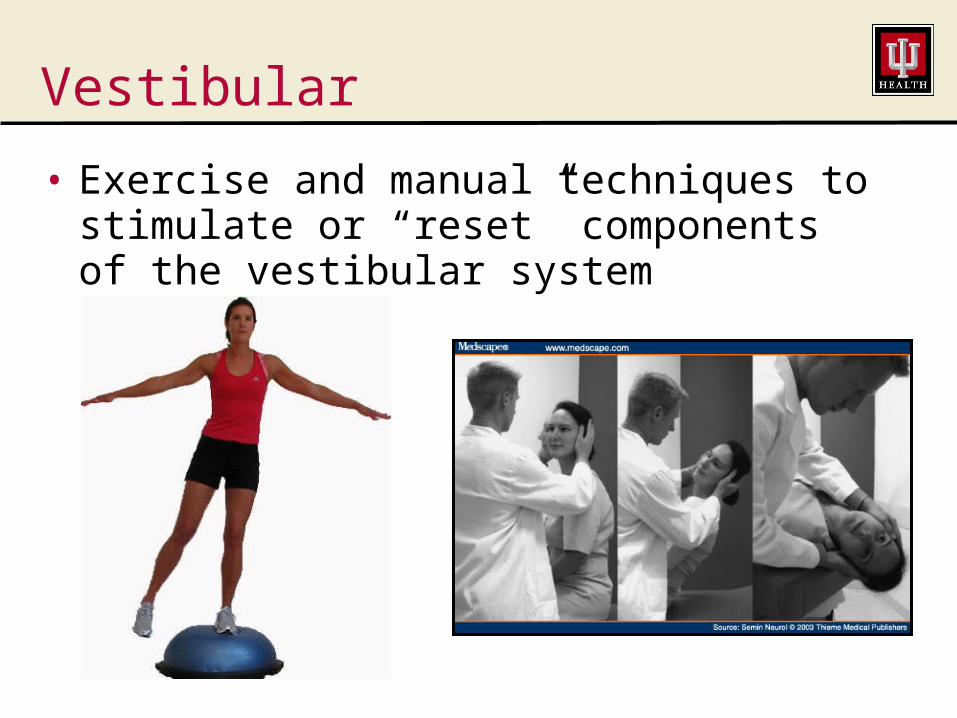
Vestibular
• Exercise and manual techniques to stimulate or “reset” components of the vestibular system

Ocular
• Exercises to aid with resolution of identified deficits
• Incorporate functional activities
• If not responding consider referral to optometrist or ophthalmologist

Cognitive
• Tasks to stimulate cognitive function with:– Attention/concentration, memory,
organizational skills, reasoning, problem solving, decision making, executive stills
• Goal is to incorporate with relevant functional activities
Headaches and Migraine
• Identify the “trigger(s)”
• Treat the appropriate triggers as well as the symptoms
• Often treated in conjunction with the neck
• Relaxation, soft tissue mobilization, joint mobilization, relaxation, cranio-sacral therapy

Cervical
• Rule out significant cervical issues (fractures, etc.)
• Identify involved structure(s)
• Soft tissue mobilization, joint mobilization, stretching, strengthening
Reintegration of ExertionReturn to Activity Guidelines
• Step 1: Physical and Cognitive Rest
• Step 2: Light Aerobic Based Activity
• Step 3: Higher Intensity / Function Specific Activities
• Step 4: Non-contact Training Activities
• Step 5: Full-contact Activities
• Step 6: Return to Full Participation
• May alter this slightly based on nature of dysfunction

When OK to return to sports/activity?
• Return to baseline symptoms at rest AND
• Physical examination is normal AND
• Satisfactory results of brain function with neurocognitive testing (ImPACT™ test) AND
• Successfully completes structured exertion reintegration program AND
• When cleared by a licensed healthcare professional trained in the evaluation and management of concussion
Summary

The Plan – Step by Step
• Evaluation/re-evaluation
• Very limited daily activities until return to baseline symptoms at rest
• When returned to baseline symptoms at rest, begin re-integration of exertional activity– Sport specific drills– Non-contact drills– Full-contact drills

Take Home Points
• Education is a key facor!
• Early recognition and start of and appropriate treatment plan is essential
• EARLY REST - physical and cognitive is the hallmark of initial treatment
• Return to activity in a graduated fashion and not before symptoms have returned to baseline levels
• Multiple criteria must be met prior to unrestricted return to activity

What Does the Future Bring?
• More research
• Improved imaging tests for diagnosis of concussion
• Improved equipment to help minimize the risk of concussion
• Improved techniques for the treatment of concussion
Important to Remember
• Many people play a role in ensuring the health and safety of athletes; all need to communicate and act as a team– Concussion sufferer– Family (parent, spouse, etc.)– Coach– Teachers– Employers– Athletic Trainer– Physician/PA/NP– Nurse– Friends/teammates/co-workers
??QUESTIONS????QUESTIONS??
Anyone, AnyoneAnyone, Anyone

THANK THANK YOU!YOU!