ajpp_april june 2011
DESCRIPTION
AJPP_April June 2011TRANSCRIPT


From the desk oF group editor-in-chieF
Do not Give Prophylactic Paracetamol to Reduce Vaccine Reactions .................................................4
KK Aggarwal
original article
Urinary Iodine Excretion in Urine Samples Among Children in Dahod District, Gujarat ........5
JR Damor, NG Padhiyar, GL Ninama
case report
Collodion Baby .....................................................10
Seema Sharma
Holt-Oram Syndrome ...........................................12
Sunil Mhaske, Sandeep Mhaske
practice guidelines
AAP Reports on Use of Probiotics and Prebiotics in Children ..........................................15
Contents
Asian Journal of
Pediatric PracticeAn IJCP Group Publication
Advisory BodiesHeart Care Foundation of India
Non-Resident Indians Chamber of Commerce & Industry World Fellowship of Religions
Dr Sanjiv Chopra Prof. of Medicine & Faculty Dean
Harvard Medical SchoolGroup Consultant Editor
Dr Deepak ChopraChief Editorial Advisor
Dr KK AggarwalCMD, Publisher and Group Editor-in-Chief
Dr Veena AggarwalJoint MD and Group Executive Editor
Anand Gopal Bhatnagar Editorial Anchor
AJPP Speciality BoardChief Editor
Dr (Mrs.) Swati Y BhaveEditorial Board International (Group)
Dr Adenike Grange (Lagos Nigeria)
Dr Alberto Bissot (Panama)Dr Anagha (New Zealand)
Dr Andreas Constantopoulos (Greece)Dr Dilip Patel (USA)
Dr Donald E Greydanus (USA)Dr Ellis D Avner (USA)
Dr Giorgio Tamburlini (Italy)Dr Helen Pratt (USA)Dr James Tumwne (Kampala, Uganda)
Dr Jesson Unni (Kerala)Prof. Jose Boix Ochoa (Barcelona)
Dr Manuel Katz (Israel)Dr Manuel Moya (Spain)
Dr MC Rahimy (West Africa)Dr Murat Yurdakok (Turkey)
Dr Najwa Khuri-Bulos (Jordan)Dr Sergio Augusto Cabral (Brazil)
Dr Shiv Aggarwal (Florida)Dr VB Sanghi (Michigan)
Dr Yoshikatsu Eto (Japan)Dr Zulfiqar Bhutta (Pakistan)
Dr Zulfi Bhutta (Pakistan)Anand S Vasudev (New Delhi)
IJCP Editorial BoardDr Alka Kriplani
Asian Journal of Obs & Gynae PracticeDr VP Sood
Asian Journal of Ear, Nose and ThroatDr Praveen Chandra
Asian Journal of Clinical CardiologyDr Swati Y Bhave
Asian Journal of Paediatric PracticeDr Vijay Viswanathan
The Asian Journal of DiabetologyDr KMK Masthan
Indian Journal of Multidisciplinary DentistryDr M Paul Anand, Dr SK Parashar
CardiologyDr CR Anand Moses, Dr Sidhartha Das,
Dr A Ramchandran, Dr Smith A Sethi Diabetology
Dr Ajay Kumar Gastroenterology
Dr Hasmukh J Shroff Dermatology
Dr Georgi Abraham Nephrology
Dr Sidharth Kumar Das RheumatologyDr V Nagarajan
NeurologyDr Thankam Verma, Dr Kamala Selvaraj
Obs and Gyne

EDITORIAl & BuSINESS OffICESDelhi Mumbai Kolkata Bangalore Chennai Hyderabad
Dr Veena Aggarwal09811036687
E - 219, Greater KailashPart - 1, N.D. - 110 048
Cont.: [email protected]@ijcp.com
Dinesh: 9891272006 [email protected]: 09831363901
Nilesh Aggarwal09818421222
Building No - D 10 Flat No - 43, 4th
Floor Asmita Co-operative
Housing Society Near Charkop Naka
Marvey Road Malad (W)
Mumbai 400 [email protected]
Sr. BMRitu Saigal
09831363901Flat 5E,
Merlin Estate Geetanjali
25/8 Diamond Harbour Road
Kolkata - 700 008 Cont.: 24452066 [email protected]
Sr. BMH Chandrashekar
09845232974Arora Business
Centre, 111/1 & 111/2 Dickenson Road
(Near Manipal Centre)Bangalore - 560 042
Cont.: 25586337 [email protected]
Sr. BMChitra Mohan09841213823
40A, Ganapathy-puram
Main Road Radhanagar Chromepet
Chennai - 600 044Cont.: 22650144 [email protected]
Sr. BMVenugopal
09849083558H. No.
16-2-751/A/70 First Floor
Karan Bagh Gaddiannaram Dil Sukh Nagar
Hyderabad - 500 059
Cont.: [email protected]
Sr.: Senior; BM: Business Manager
Contents
Asian Journal of
Pediatric Practice
research review
From the Journals ... ............................................17
emedinews section
From eMedinewS ... .............................................18
lighter reading
Lighter reading ....................................................19
Editorial policies
The purpose of IJCP Academy of CME is to serve the medical profession and provide print continuing medical education as a part of their social commitment. The information and opinions presented in IJCP group publications reflect the views of the authors, not those of the journal, unless so stated. Advertising is accepted only if judged to be in harmony with the purpose of the journal; however, IJCP group reserves the right to reject any advertising at its sole discretion. Neither acceptance nor rejection constitutes an endorsement by IJCP group of a particular policy, product or procedure. We believe that readers need to be aware of any affiliation or financial relationship (employment, consultancies, stock ownership, honoraria, etc.) between an author and any organization or entity that has a direct financial interest in the subject matter or materials the author is writing about. We inform the reader of any pertinent relationships disclosed. A disclosure statement, where appropriate, is published at the end of the relevant article.
NoteAsian Journal of Pediatric Practice, does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is
commercial in nature in this issue.
Published, Printed and Edited byDr KK Aggarwal, on behalf of
IJCP Publications Pvt. Ltd. and Published at
E - 219, Greater Kailash, Part - 1,New Delhi - 110 048
E-mail: [email protected]
Printed at IG Printers Pvt. Ltd. New Delhi
E-mail: [email protected]
© Copyright 2011 IJCP Publications Pvt. ltd All rights reserved.
The copyright for all the editorial material contained in this journal, in the form of layout, content including images and design, is held by IJCP Publications Pvt.
Ltd. No part of this publication may be published in any form what-soever without the prior written
permission of the publisher.Cover Photograph by Jeevan Vamsi

� Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Do Not Give Prophylactic Paracetamol to Reduce Vaccine Reactions
Dr KK AggarwalPadma Shri and Dr BC Roy National Awardee
Sr Physician and Cardiologist, Moolchand MedcityPresident, Heart Care Foundation of India
Group Editor-in-Chief, IJCP Group Editor-in-chief, eMedinewS
Chairman Ethical Committee, Delhi Medical CouncilDirector, IMA AKN Sinha Institute (08-09)
Hony. Finance Secretary, IMA (07-08)Chairman, IMA AMS (06-07)
President, Delhi Medical Association (05-06)[email protected]
http://twitter.com/DrKKAggarwalKrishan Kumar Aggarwal (Facebook)
The pain and fever that may occur after vaccination can be attenuated by administering paracetamol at the time of immunization.1-3 However, this practice may be associated
with decreased vaccine response.4
The effects of prophylactic paracetamol on fever and immunogenicity were evaluated in a multicenter, open-label trial in which 459 infants (aged 9-16 weeks at study entry) were randomly assigned to receive paracetamol at the time of vaccination and for the next 24 hours or no prophylaxis before primary and booster immunizations.4 Primary immunizations consisted of 10-valent pneumococcal conjugate vaccine, nontypeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV), and hexavalent diphtheria-tetanus-acellular-pertussis-hepatitis B-inactivated polio-H. influenzae type b vaccine (DTaP-HBV-IPV/Hib) at three, four, and five months, and oral rotavirus vaccine at three and four months. Booster immunizations consisted of PHiD-CV and DTaP-HBV-IPV/Hib at 12-15 months of age.
Fewer children who received paracetamol had fever >38°C (42 vs 66% and 36% vs 58% after primary and booster immunization, respectively). However, there was no difference between groups in occurrence of fever ≥39.5°C (<1-2%) or fever requiring medical attention.
The vaccines were highly immunogenic in both groups, with at least 96% of children achieving protective levels of antibody for all antigens. However, prophylactic paracetamol was associated with lower geometric mean antibody titers (GMT) to pneumococcus, Haemophilus influenzae, pertussis, diphtheria, and tetanus after the primary series and lower GMT to pneumococcus, Haemophilus, and tetanus after the booster doses.
referencesIpp MM, Gold R, Greenberg S, et al. Acetaminophen prophylaxis of adverse reactions following vaccination of infants with diphtheria-pertussis-tetanus toxoid-polio vaccine. Pediatr Infect Dis J 1987;6:721-5.Uhari M, Hietala J, Viljanen MK. Effect of prophylactic acetaminophen administration on reaction to DTP vaccination. Acta Paediatr Scand 1988;77:747-51.Long SS, Deforest A, Smith DG, et al. Longitudinal study of adverse reactions following diphtheria–tetanus–pertussis vaccine in infancy. Pediatrics 1990;85:294-302.Prymula R, Siegrist CA, Chlibek R, et al. Effect of prophylactic paracetamol administration at time of vaccination on febrile reactions and antibody responses in children: two open-label, randomised controlled trials. Lancet 2009;374:1339-50.
n n n
1.
2.
3.
4.
From the Desk oF Group eDitor-in-ChieF

�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
oriGinal artiCle
Urinary Iodine Excretion in Urine Samples Among Children in Dahod District, GujaratJR Damor*, NG Padhiyar**, Gl Ninama†
*Associate Professor **Assistant Professor Dept. of Community Medicine†Assistant Professor Dept. of Microbiology Medical College and SSG Hospital, VadodaraAddress for correspondenceDr JR DamorD-27, Akanksha DuplexOpposite Laxmikunj Society Laxmipura Road, GorwaVadodara - 390 016, GujaratE-mail: [email protected]
abstraCt
Aim: To measure urinary iodine excretion level and to assess the iodine level in salt sample. Study design: Cross-sectional study done in 30 randomly selected wards/villages of Dahod district. Materials and method: The IDD survey at the Dahod district was conducted by population proportionate to size (PPS) cluster sampling. A sample of 90 children (45 boys and 45 girls) of age group of 6-12 years from the school was taken. In each cluster, seven urine samples of boys and seven samples of girls were collected and sent to the public health laboratories. From each cluster, salt samples were collected from a minimum of 10 houses and tested with the use of spot salt testing kit for the presence of iodine. Results: The median urinary iodine level was 115 μg/dl. Age-wise distribution of urinary iodine showed that the proportion of children with urinary iodine excretion <100 μg/dl was lowest in the 6-year age group, whereas the highest proportion was in the 10-year age group. Out of 300 salt samples, 207 samples (69%) had >15 ppm (parts per million) iodine; four samples (1.3%) had <15 ppm iodine. This means that the use of iodized salt was 70.3%. Conclusion: The lowest urinary iodine excretion was seen in age group of six years whereas highest urinary iodine excretion was seen in age group of 10 years. In 69%, salt samples had >15 ppm iodine present and in 1.3%, samples had <15 ppm iodine present. Thirty percent of salt samples were noniodized.
Key words: Iodine deficiency disorders, salt samples, urinary iodine excretion
Iodine is an essential micronutrient with an average daily requirement of 100-150 µg for normal human growth and mental development. Inadequate
or poor intake of iodine can result in physical and mental retardation. It affects people of all ages, both sexes and of different socioeconomic backgrounds. The disorders caused due to deficiency of nutritional iodine in the food or diet are called iodine deficiency disorders (IDDs).1
According to Public Health Standards, an area is declared to be iodine deficient, if 5% or more of school-going children suffer from goitre (enlargement of the thyroid gland situated in the neck). From this point of view, several districts in the state of Gujarat have the problem of iodine deficiency.
Major activities of National Iodine Deficiency Disorders Control Programme (NIDDCP) are to conduct surveys to assess the magnitude of the IDDs, monitoring of iodized salt consumption, laboratory monitoring of iodized salt, urinary iodine salt concentration and health education and publicity.1
It is a well-established fact that with the exception of certain types of goitre, IDDs are permanent and incurable. But, these disorders can be easily prevented. The simplest method to prevent the broad-spectrum of IDDs is to consume iodized salt daily. This is the most effective and inexpensive mode to prevent these disorders. Iodized salt should ensure availability of not <150 µg of iodine per person per day. Since salt is consumed by all every day, the supply of iodized salt will ensure the availability of iodine for normal body function. The average consumption of iodized salt per person per day is about 10 grams. This consumption is in moderate amounts.
The Central Government had issued a notification banning the sale of noniodized salt for direct human consumption in the entire country with effect from 17th May, 2006 under the Prevention of Food Adulteration Act 1954. Starting with Bharuch district in 1982, the State Government brought the entire state under

� Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
oriGinal artiCle
IDD Control Programme in a phased manner by the year 1994. Surveys conducted by the Preventive and Social Medicine (PSM) Dept. of the Govt. Medical Colleges in the state show that IDDs continue to be a health problem in several districts of the state. The high prevalence rate was found in Dangs, Bharuch and Valsad districts.2 The geographical difference reflects the difference in iodine content in drinking water and to some extent in milk.3
aims and objectivesTo determine median urinary iodine excretion in samples of school children.To assess iodine level in salt samples in households and at retail shops.To assess the availability of iodized salt and information, education and communication (IEC) material at public distribution system shop.
materials and methodThe survey for IDDs at Dahod district was conducted by population proportionate to size (PPS) cluster sampling. Selection of villages/wards by PPS was done from list of villages/wards along with the population from the latest census. The data are available for all districts of the country on CD from Registrar General Office. A sample of 30 villages/wards had to be selected from the district. The method of sampling
used was PPS systematic sampling. A sample of 90 children (45 boys and 45 Girls) of age group of 6-12 years from the school and in each cluster, seven urine samples of boys and seven samples of girls were collected and sent to the public health laboratories. From each cluster, salt samples were collected from a minimum of 10 houses and tested with the use of spot salt testing kit for the presence of iodine.
Limitations: As it is a cross-sectional study, children who were not present in school at the time of study could not be examined.
results and review of literatureThe median urinary iodine level is 115 µg/dl. The proportion of samples with urinary iodine <50 µg/dl was found to be 15.6%, which is <20% (Table 1). Thus, this corresponds to the category of adequate iodine nutrition as per WHO guidelines for monitoring for IDDs.
The age-wise distribution of urinary iodine showed that the proportion of children with urinary iodine excretion <100 µg/dl was lowest in the 6-year age group, whereas the highest proportion was found in the 10-year age group (Table 2). The gender-wise distribution of urinary iodine excretion showed that the proportion of children with urinary iodine excretion >100 µg/dl was almost similar
figure 1. Age-wise distribution of urinary iodine.
>100 µg/dl<100 µg/dl
Age (years)
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Per
cent
age
6 7 8 9 10 11 12 Total
63.2
36.8
55.9
44.1
53.4
46.6
56.7
43.3
52.5
47.5 39.7
60.3 57.6 57.1
42.942.4
�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
oriGinal artiCle
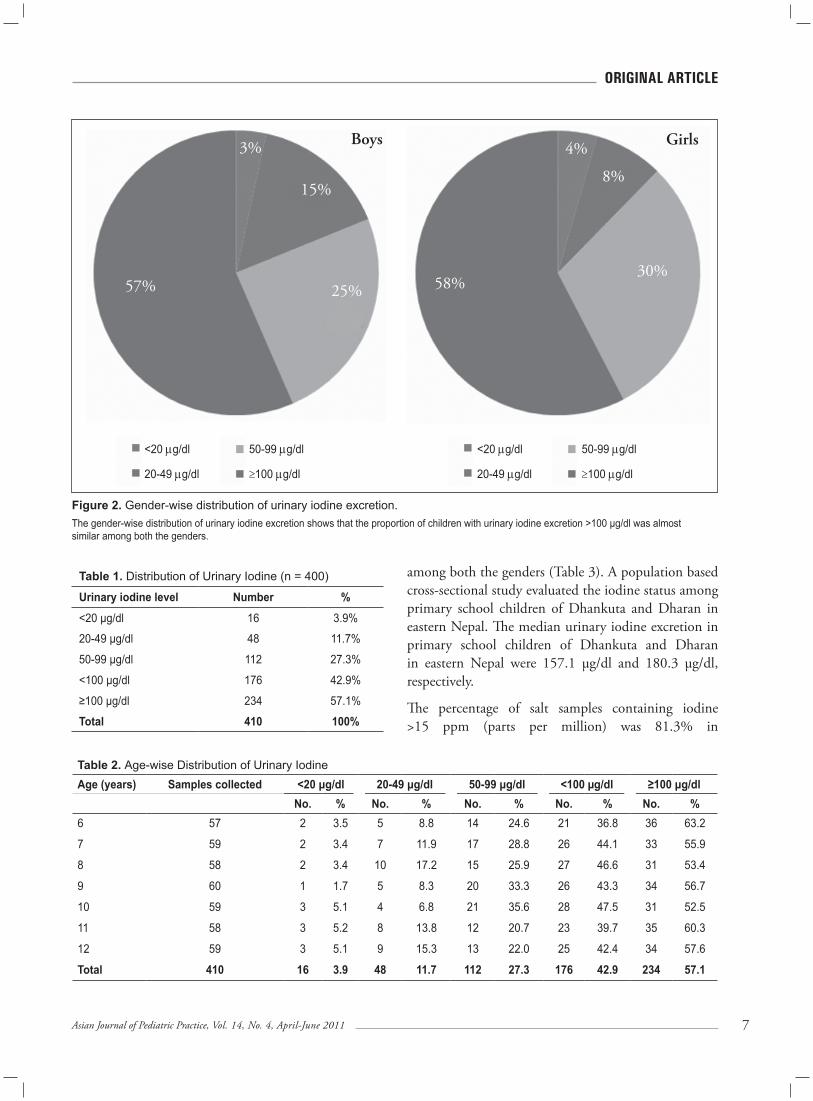
figure 2. Gender-wise distribution of urinary iodine excretion. The gender-wise distribution of urinary iodine excretion shows that the proportion of children with urinary iodine excretion >100 μg/dl was almost similar among both the genders.
<20 µg/dl
20-49 µg/dl
Boys
57%
3%
15%
25%
Girls4%
8%
58%30%
50-99 µg/dl
≥100 µg/dl
<20 µg/dl
20-49 µg/dl
50-99 µg/dl
≥100 µg/dl
Table 1. Distribution of Urinary Iodine (n = 400)
urinary iodine level Number %
<20 μg/dl 16 3.9%
20-49 μg/dl 48 11.7%
50-99 μg/dl 112 27.3%
<100 μg/dl 176 42.9%
≥100 μg/dl 234 57.1%
Total 410 100%
Table 2. Age-wise Distribution of Urinary IodineAge (years) Samples collected <20 μg/dl 20-49 μg/dl 50-99 μg/dl <100 µg/dl ≥100 μg/dl No. % No. % No. % No. % No. %6 57 2 3.5 5 8.8 14 24.6 21 36.8 36 63.2
7 59 2 3.4 7 11.9 17 28.8 26 44.1 33 55.9
8 58 2 3.4 10 17.2 15 25.9 27 46.6 31 53.4
9 60 1 1.7 5 8.3 20 33.3 26 43.3 34 56.7
10 59 3 5.1 4 6.8 21 35.6 28 47.5 31 52.5
11 58 3 5.2 8 13.8 12 20.7 23 39.7 35 60.3
12 59 3 5.1 9 15.3 13 22.0 25 42.4 34 57.6
Total 410 16 3.9 48 11.7 112 27.3 176 42.9 234 57.1
among both the genders (Table 3). A population based cross-sectional study evaluated the iodine status among primary school children of Dhankuta and Dharan in eastern Nepal. The median urinary iodine excretion in primary school children of Dhankuta and Dharan in eastern Nepal were 157.1 µg/dl and 180.3 µg/dl, respectively.
The percentage of salt samples containing iodine >15 ppm (parts per million) was 81.3% in
� Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
oriGinal artiCle
Dhankuta and 89.6% in Dharan.4 Horton et al observed that median urinary iodine excretion was significantly and positively related to household availability of iodized salt for developing countries.5
In a study of more than 2000 school children aged 6-12 years from Rajkot district, India, the median urinary iodine excretion was 110 µg/dl. Iodine level >15 ppm was found in 81% of salt samples tested at household level.6
Urinary iodine excretion level was <100 µg/dl in 42.9% talukas and >100 µg/dl in 57.1% talukas (Table 4). Out of 300 salt samples, 207 samples (69%) had >15 ppm iodine present (Table 5). Iodized salt was available in majority of private shops (88.8%) in the villages (Table 6).
conclusionThe proportion of samples with urinary iodine <50 µg/dl was found to be 15.6%, which is <20%. Thus this corresponds to the category of adequate iodine nutrition as per WHO guidelines
Table 4. Taluka-wise Urinary Iodine ExcretionTaluka Total samples
takenMedian urinary iodine
excretion (20 μg/dl)<20 μg/dl 20-49 μg/dl 50-99 μg/dl ≥100 μg/dl
No. % No. % No. % No. %Dahod 83 195 0 0 2 2.4 9 10.8 72 86.7
Devgadhbaria 48 150 1 2.1 2 4.2 12 25 33 68.8
Dhanpur 28 70 1 3.6 5 17.9 18 64.3 4 14.3
Fatehpura 55 95 3 5.5 8 14.5 22 40 22 40
Garbada 42 222.5 0 0 0 0 4 9.5 38 90.5
Jhalod 84 85 2 2.4 17 20.2 32 38.1 33 39.3
Limkheda 70 75 9 12.9 14 20 15 21.4 32 45.7
Total 410 115 16 3.9 48 11.7 112 27.3 234 57.1The median urinary iodine excretion is <100 μg/dl for Dhanpur, Jhalod, Fatehpura and Limkheda and it is >100 μg/dl for the rest of the Talukas.
Table 3. Gender-wise Distribution of Urinary Iodine ExcretionGender Samples collected <20 μg/dl 20-49 μg/dl 50-99 μg/dl <100 μg/dl ≥100 μg/dl No. % No. % No. % No. % No. %Male 207 7 3.4 32 15.5 51 24.6 90 43.5 117 56.5
Female 203 9 4.4 16 7.9 61 30 86 42.3 117 57.6
Total 410 16 3.9 48 11.7 112 27.3 176 42.9 234 57.1
for monitoring for IDDs. The age-wise distribution of urinary iodine showed that the proportion of children with urinary iodine excretion <100 µg/dl was lowest in the 6-year age group, whereas the highest proportion was found in the 10-year age group.
Sixty-nine percent contained >15 ppm iodine; 30% of the salt samples were noniodized. There was no gender-wise difference in urinary iodine excretion. More than 50% talukas had urinary iodine excretion levels >100 µg/dl.
recommendationsIn Dahod district, Gujarat, 30% salt samples were found to be noniodized hence, there is a need to create awareness among community people and school children about iodized salt by using IEC materials. To make available iodized salt in all public distribution shops.10% of private shops had noniodized salts, so there should be a strict implementation of ban on selling of noniodized salt.

�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
oriGinal artiCle
Out of 300 salt samples, 207 samples (69%) contained >15 ppm iodine.
Table 5. Use of Iodized Salt at Household LevelCluster No.
0 ppm <15 ppm ≥15 ppm Total samples
1 2 0 8 102 4 0 6 103 3 0 7 104 8 0 2 105 9 1 0 106 3 0 7 107 10 0 0 108 4 0 6 109 0 0 10 1010 10 0 0 1011 4 0 6 1012 5 0 5 1013 0 0 10 1014 0 0 10 1015 6 1 3 1016 0 0 10 1017 2 0 8 1018 0 1 9 1019 5 0 5 1020 0 1 9 1021 0 0 10 1022 0 0 10 1023 3 0 7 1024 2 0 8 1025 0 0 10 1026 0 0 10 1027 4 0 6 1028 0 0 10 1029 3 0 7 1030 2 0 8 10Total 89 (29.7%) 4 (1.3%) 207 (69%) 300
Table 6. Distribution of Private Shop with Respect to Salt Iodization StatusName of Taluka Salt Total
Iodized NoniodizedFatehpura 1 0 1Jhalod 1 0 1Limkheda 0 1 1Dahod 3 0 3Devgadhbaria 1 0 1Dhanpur 1 0 1Garbada 1 0 1Total 8 1 9
Iodized salt was available in majority of private shops (88.8%) in the villages.
suggested readingRevised Policy Guidelines on National Iodine Deficiency Disorders Control Programme. National Rural Health Mission IDD & Nutrition Cell, Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India New Delhi, Revised Edition, October 2006.
State Nutrition cell, Government of Gujarat Document on Iodine deficiency Disorders Control Programme: Gujarat, 2008.
1.
2.
Pedersen KM, Laurberg P, Nohr S, Jorgensen A, Anderson S. Iodine in drinking water varies by more than 100-fold in Denmark. Importance for iodine content of infant formulas. Eur J Endocrinol 1999;140(5): 400-3.
Gelal B, Chaudhri RK, Nepal AK, Sah GS, Lamsal M, Brodie DA, et al. Iodine deficiency disorders among primary school children in eastern Nepal. Indian J Pediatr 2011;78(1):45-8.
Horton S, Miloff A. Iodine status and availability of iodized salt: an across-country analysis. Food Nutr Bull 2010;31(2):214-20.
Chudasama RK, Verma PB, Mahajan RG. Iodine- nutritional status and goiter prevalence in 6-12 years primary school children of Saurashtra region, India. World J Pediatr 2010;6(3):233-7.
Chudasama R, Patel UV, Patel RR, Verma PH. Iodine deficiency disorders in 6-12 years - old rural primary school children in Kutch District, Gujarat. Indian Pediatr 2010 Nov 30. pii: S097475590900853-1. [Epub ahead of print].
Misra S, Kantharia SL, Damor JR. Prevalence of goitre in 6 -12 years school-going children of Panchmahal district in Gujarat, India. Indian J Med Res 2007;126(5):475-9.
Biswas AB, Chakraborty I, Das DK, Biswas S, Nandy S, Mitra J. Iodine deficiency disorders among school children of Malda, West Bengal, India. J Health Popul Nutr 2002;20(2):180-3.
Kapil U, Sharma TD, Singh P. Iodine status and goiter prevalence after 40 years of salt iodisation in the Kangra District, India. Indian J Pediatr 2007;74(2):135-7.
3.
4.
5.
6.
7.
8.
9.
10.

10 Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Case report
Collodion Baby
Seema Sharma
Assistant Professor Dr Rajendra Prasad Government Medical College and Hospital, Kangra, TandaAddress for correspondenceDr Seema Sharma 23, Block-B, Type V, DRPGMC Campus Kangra, Tanda, Himachal Pradesh - 176 001E-mail: [email protected]
abstraCt
Collodion baby is a rare congenital autosomal recessive disorder that resembles Harlequin fetus but is milder in degree. Treatment of this condition poses a considerable challenge. Supportive care is important to prevent mortality. We present herein a case of 4-day-old baby boy who presented with complaint of membrane over the whole body. The baby recovered well with treatment and was discharged with advice for regular emollient application and follow-up.
Key words: Collodion membrane, autosomal recessive, icthyosis
case reportA 4-day-old baby boy presented with complaint of membrane over the whole body, which started breaking on the second day (Fig. 1). The baby was the third issue born by normal delivery at full term to a consanguineous couple. There was history of similar complaint in the second issue who died at the age of 10 days. The baby’s weight was 2.3 kg and head circumference was 33 cm. On examination, the whole body was covered with parchment-like membrane resembling collodion and was peeling off on the chest and abdomen. The associated findings included ectropion (Fig. 2), flattening of nose and ears (Fig. 3), claw-like hands and limitation of joint movements. There were no other congenital anomalies. Hair and nails were normal. Sepsis screen turned out to be positive. Baby was treated in humidified environment with intravenous fluids and antibiotics. Emollient was applied to the whole body and systemic retinoids were given for two weeks. Baby recovered well and was discharged with advice for regular emollient application and follow-up (Fig. 4).
discussion Collodion baby is a rare congenital disorder resem-bling Harlequin fetus but milder in degree.1 Often
it is a manifestation of congenital ichthyosiform erythroderma or lamellar icthyosis. Incidence of this condition is one in 3,00,000 live births.2 Affected babies are born in a collodion membrane, a shiny waxy tight inelastic outer layer to the skin, resembling an oiled parchment or dried collodion (sausage skin), which is subsequently shed within 10-14 days after birth and infrequently, has normal skin after the membrane is shed. This condition is an autosomal
figure 1.
figure 2.

11Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Case report
figure 3. figure 4.
recessive genetic disorder.3 Ichthyosis lamellaris is associated with a deficiency of the enzyme keratinocyte transglutaminase. Genes involved include TGM1, ABCA12 and CYP4F22.4
There is presence of ectropion, flattening of ears and nose and fixation of lips in an O-shaped configuration. The hair may be absent or may perforate the horny covering. The collodion membrane is composed of greatly thickened stratum corneum that has been saturated with water. The presence of collodion membrane does not necessarily predict that the baby will develop ichthyosis and spontaneous healing may occur. Skin biopsy of collodion membrane is usually not diagnostic. Most collodion babies do have a form of ichthyosis and majority of them develop features of lamellar ichthyosis, bullous ichthyosis, X-linked ichthyosis, Netherton’s syndrome or Gaucher’s disease.
Collodion baby represents a difficult treatment challenge. The complications include cutaneous infections, aspiration pneumonia, hypothermia or hypernatremic dehydration (from excess transcutaneous fluid loss as a result of increased skin permeability).2 Therefore, supportive care is most important to prevent mortality. Treatment initially consists of high fluid intake to avoid dehydration and transepidermal fluid loss and use of heated humidified incubator and emulsifying ointment and retinoids. Refresh tears are used to prevent the eyes from becoming dried out. There is no need to operate immediately for ectropion as it can be corrected by local application of clobetasol in older children.5 The ear canal should
be cleaned very gently under an operating microscope. Life expectancy and difficulties that the collodion baby faces depend upon the particular underlying condition. With increasing age, the scaling tends to be concentrated around joints in areas such as the groin, the armpits, the inside of the elbow and the neck. The scales often tile the skin and may resemble fish scales. There is also an increased risk of skin infection and mechanical compression, leading to problems like limb ischemia. The affected child usually has deformed auricle-Pinna, narrow external auditory canal filled with keratin debris. There is no associated inner ear nerve hearing loss.
Newer therapies that have resulted in clinical improvement are topical N-acetylcysteine which has an antiproliferative effect,6 tazarotene topical 0.05%, a receptor selective retinoid7 and calcipotriol, a synthetic derivative of vitamin D. Gene therapy seems to be a novel therapeutic approach to lamellar icthyosis.8
references Nancy BE, Lawrence MS. Congenital and hereditary disorders of the skin. In: Schaffers Diseases of Newborn. 6th edition, (Taeusch, Ballard, Avery [Eds.]), WB Saunders: USA 1991:973-84. Shwayder T, Ott F. All about ichthyosis. Pediatr Clin North Am 1991;38(4):835-57.Dermatology at the Millenium. Delwyn Dyall-Smith, Robin Marks, Informa Health Care 1999:586. William D James, Timothy Berger, Dirk Elston. Andrews’ Diseases of the Skin: Clinical Dermatology. 10th edition, Saunders 2005.Van Gysel D, Lijnen RL, Moekti SS, de Laat PC, Oranje AP. Collodion baby: a follow-up study of 17 cases. J Eur Acad Dermatol Venereol 2002;16(5):472-5. Redondo P, Bauzá A. Topical N-acetylcysteine for lamellar icthyosis. Lancet 1999;354(9193):1880. Stege H, Hofmann B, Ruzicka T, Lehmann P. Topical application of tazarotene in the treatment of nonerythrodermic and lamellar icthyosis. Arch Dermatol 1998;134(5):640. Akiyama M, Shimizu H. An update on molecular aspects of non-syndromic icthyosis. Exp Dermatol 2008;17(5):373-82.
n n n
1.
2.
3.
4.
5.
6.
7.
8.

12 Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Case report
Holt-Oram syndrome is rare congenital anomaly of the musculoskeletal and the cardiovascular systems. The prevalence of this
syndrome is 1/1,00,000 population. The commonest findings are absent thumb and radius, atrial septal defect.
Holt-Oram syndrome is also known as heart hand syndrome, cardiac limb syndrome, atrio-digital syndrome or ventriculo-radial syndrome. In this syndrome 75% of the cases have cardiovascular problem. The commonest cause of mortality and morbidity is cardiovascular malformation.
case summaryAn unbooked rural habitat multigravida of 31-32 weeks of gestational period was admitted to the labor room with pain in abdomen and bleeding per vaginum since three days. She was first treated by a private practitioner who referred her to the medical college for further management.
According to her last menstrual period, her gestational age was 32 weeks and seven days. She had no antenatal check-up during this period. She had received two doses of TT injection. She had family history of consanguineous marriages. She was G4P3L3. First three are living, full term normal deliveries. Out of three, two are female and one is male. These children don’t have congenital abnormality.
She had pain in abdomen which was colicky in nature associated with nausea and bleeding per vaginum. Bleeding was moderate, fresh blood, since three days. She also had one bout of unconsciousness.
On examination, she was average built with moderate pallor, tachycardia bilateral pedal edema, BP was 170/110 mmHg. Rest all her vitals are normal. She received tablet nifedipine (10 mg) t.d.s.
P/A - showed uterus of 32 weeks with good relaxation, and a fetus with cephalic presentation. Inspection of the vulva showed moderate bleeding. Per vaginum examination was not done due to excessive bleeding.
USG showed live fetus of 32 weeks, severe oligo-hydramnios, cephalic presentation, placenta lying anteriorly with Grade 2 maturity. FHS 140/min. Mother’s investigation revealed Hb 9 g, TLC - 5,400/mm3, ESR - 20 mm. Blood group Tridot negative. LFT and RFT were normal. Urine showed traces of albumin.
A male baby weighing 1.7 kg was delivered by lower segment cesarean section. Baby cried immediately after birth. His HR - 35/min, RR - 40/min. His color was pink, there was no cyanosis and reflexes were normal. Placenta and cord were normal.
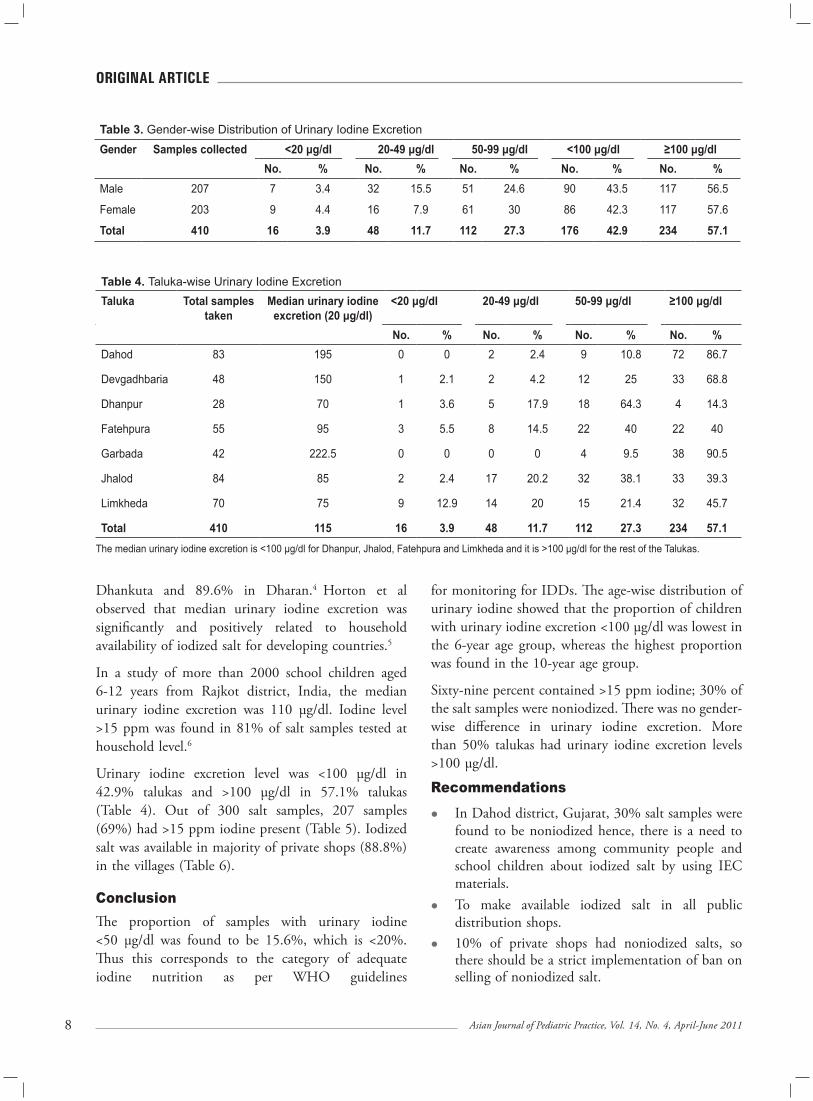
On inspection following abnormalities were found in the baby (Fig. 1):
Absence of thumb on both sidesWidely spaced eyesLow set earsHypoplastic receding mandibleSingle palmar creaseHigh arched palate.
*Professor and Head**Assistant Lecturer Dept. of Pediatrics Padma Shri Dr Vithalrao Vikhe Patil Memorial Hospital and Medical College, Ahmednagar, Maharashtra
abstraCt
Holt-Oram syndrome is a heart-upper limb malformation complex with an autosomal dominant inheritance and near-complete penetrance but variable expression.
Key words: Holt-Oram syndrome, atrial septal defect, radial hypoplasia
Holt-Oram Syndrome
Sunil Mhaske*, Sandeep Mhaske**
13Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Case report
figure 1. Inspection of the body revealed findings suggestive of Holt-Oram syndrome.
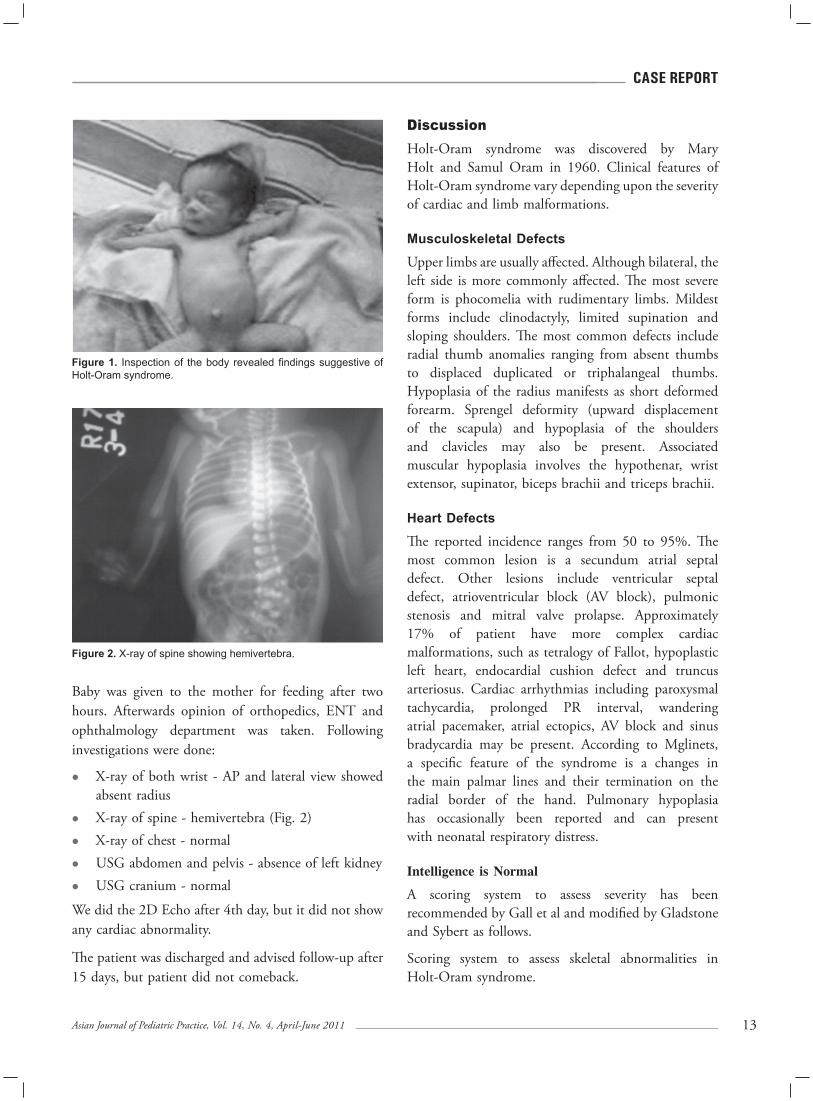
figure 2. X-ray of spine showing hemivertebra.
Baby was given to the mother for feeding after two hours. Afterwards opinion of orthopedics, ENT and ophthalmology department was taken. Following investigations were done:
X-ray of both wrist - AP and lateral view showed absent radiusX-ray of spine - hemivertebra (Fig. 2) X-ray of chest - normalUSG abdomen and pelvis - absence of left kidneyUSG cranium - normal
We did the 2D Echo after 4th day, but it did not show any cardiac abnormality.
The patient was discharged and advised follow-up after 15 days, but patient did not comeback.
discussionHolt-Oram syndrome was discovered by Mary Holt and Samul Oram in 1960. Clinical features of Holt-Oram syndrome vary depending upon the severity of cardiac and limb malformations.
Musculoskeletal Defects
Upper limbs are usually affected. Although bilateral, the left side is more commonly affected. The most severe form is phocomelia with rudimentary limbs. Mildest forms include clinodactyly, limited supination and sloping shoulders. The most common defects include radial thumb anomalies ranging from absent thumbs to displaced duplicated or triphalangeal thumbs. Hypoplasia of the radius manifests as short deformed forearm. Sprengel deformity (upward displacement of the scapula) and hypoplasia of the shoulders and clavicles may also be present. Associated muscular hypoplasia involves the hypothenar, wrist extensor, supinator, biceps brachii and triceps brachii.
Heart Defects
The reported incidence ranges from 50 to 95%. The most common lesion is a secundum atrial septal defect. Other lesions include ventricular septal defect, atrioventricular block (AV block), pulmonic stenosis and mitral valve prolapse. Approximately 17% of patient have more complex cardiac malformations, such as tetralogy of Fallot, hypoplastic left heart, endocardial cushion defect and truncus arteriosus. Cardiac arrhythmias including paroxysmal tachycardia, prolonged PR interval, wandering atrial pacemaker, atrial ectopics, AV block and sinus bradycardia may be present. According to Mglinets, a specific feature of the syndrome is a changes in the main palmar lines and their termination on the radial border of the hand. Pulmonary hypoplasia has occasionally been reported and can present with neonatal respiratory distress.
Intelligence is Normal
A scoring system to assess severity has been recommended by Gall et al and modified by Gladstone and Sybert as follows.
Scoring system to assess skeletal abnormalities in Holt-Oram syndrome.

1� Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
Case report
0. No abnormality on physical or radiological examination.
1. Minor abnormalities, including reduced thenar eminence, clinodactyly or hypoplasia of thumb.
2. Present arms and forearms, with one or more bones missing.
3. Phocomelia.A scoring system to assess cardiac abnormalities in Holt-Oram syndrome.
0. Asymptomatic, with no abnormal physical findings.
1. Conduction defect2. Structural heart abnormality that doesn’t require
surgery.3. Structural heart abnormality that requires surgery.4. Potentially lethal malformations.
Pathophysiology
Defective development of the embryonic radial ray (aplasia, hypoplasia, fusion) results in a wide-spectrum of phenotypes, including triphalangeal or absent thumb, foreshortened arms and phocomelia. The syndrome is associated with defective development of cardiac structures that results in atrial septal defect, most commonly, secundum type; heart block of varying degree or both.
The responsible gene has been mapped to band 12q 24.1, which encodes the human transcription factor TBX-5. One of the recently added loci is c.373 G > A, with results in the missense mutation p.Gly125 Arg, a novel mutation. A cardiomelic developmental field has also been postulated to relate the genetic heterogeneity of Holt-Oram syndrome, to a cascade of molecules, including the brachyury, sonic hedgehog homolog, bone morphogenetic protein,
retinoic acid receptor and transforming growth factor beta families.
suggested readingBasson CT, Bachinsky DR, Lin RC, Levi T, Elkin JA, Soults J, et al. Mutations in human TBX5 [corrected] cause limb and cardiac malformation in Holt-Oram syndrome. Nat Genet 1997;15(1):30-5.
Basson CT, Huang T, Lin RC, Bachinsky DR, Weremowicz, S, Vaglio A, et al. Different TBX5 interactions in heart and limb defined by Holt-Oram syndrome mutations. Proc Nat Acad Sci USA 1999;96(6):2919-24.
Borozdin W, Bravo-Ferrer Acosta AM, Seemanova E, Leipoldt M, Bamshad MJ, et al. Contiguous hemizygous deletion of TBX5, TBX3, and RBM19 resulting in a combined phenotype of Holt-Oram and ulnar- mammary syndromes. Am J Med Genet A 2006;140A(17):1880-6.
Braulke I, Herzog S, Thies U, Zoll B. Holt-Oram syndrome in four half-siblings with unaffected parents: brief clinical report. Clin Genet 1991;39(4):241-4.
Davies P. Obituary: S Oram, Brit Med J 1992;304:500.
Fryns JP, Bonnet D, De Smet L. Holt-Oram syndrome with associated postaxial and central polydactyly. Further evidence for genetic heterogeneity in the Holt-Oram syndrome. Genet Couns 1996;7(4):323-4.
Gruenauer-Kloevekorn C, Froster UG. Holt-Oram syndrome: a new mutation in the TBX5 gene in two unrelated families. Ann Genet 2003;46(1):19-23.
Hurst JA, Hall CM, Baraitser M. The Holt-Oram syndrome. J Med Genet 1991;28(6):406-10.
Kantaputra PN, Yamasaki K, Ishida T, Kishino T, Niikawa N. A dominantly inherited malformation syndrome with short stature, upper limb anomaly, minor craniofacial anomalies, and absence of TBX5 mutations: report of a Thai family. Am J Med Genet 2002;111(3):301-6.
n n n
1.
2.
3.
4.
5.
6.
7.
8.
9.

1�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
praCtiCe GuiDelines
AAP Reports on Use of Probiotics and Prebiotics in Children
Source: Adapted from Am Fam Physician. 2011;83(7):849-852.
In recent years there has been increased interest in adding probiotics and prebiotics to nutritional products to optimize intestinal microflora. However, as
with antibiotics, the use of these supplements should be supported by evidence-based medicine. The American Academy of Pediatrics (AAP) recently reviewed the medical uses of probiotics and prebiotics to help guide physicians in counseling parents about the use of these products as dietary supplements added to foods for children, including infant formula.
Infants have sterile gastrointestinal tracts at birth, but bacterial colonization occurs rapidly. Gestational age, mode of delivery, and diet seem to have significant effects on this process. Dysregulation of the intestinal mucosal defense system early in life is believed to be a factor in many chronic conditions, such as atopic diseases (e.g., asthma, eczema, allergic rhinitis) and autoimmune diseases (e.g., multiple sclerosis, type 1 diabetes mellitus, chronic inflammatory bowel disease). Because of their influence on intestinal microflora colonization and immune function, an infant’s early diet and intestinal microbial environment are thought to be pivotal factors in his or her overall health.
probioticsProbiotics are supplements containing organisms that change the microflora of the host. These organisms are typically Lactobacillus, Bifidobacterium, and Streptococcus species. They are able to predominate and prevail over potential pathogenic microorganisms in the human digestive tract, and are thought to produce metabolic byproducts that function as immune modulators.
As of December 2010, at least two infant formulas that contained probiotics were being sold in the United States. One contained Bifidobacterium lactis, and the other contained Lactobacillus rhamnosus GG (LGG). The addition of probiotics to powdered infant formula
has not been proven harmful to healthy term infants. However, there is no evidence of clinical effectiveness, and the routine use of these formulas is not recommended. No studies have compared the health benefits of using these formulas versus breastfeeding.
Probiotics should not be given to children who are seriously or chronically ill until the safety of these products has been established. The optimal duration of probiotic supplementation is not known, nor is the optimal dosage or species. The long-term effects on intestinal microflora in children also are not known.
Acute Infectious Diarrhea
The use of probiotics early in the course of diarrhea from acute viral gastroenteritis may reduce its duration by one day in otherwise healthy infants and young children. This benefit is strain-dependent; LGG is the most effective probiotic reported. However, the evidence does not support the routine use of probiotics to prevent infectious diarrhea unless there are special circumstances (e.g., in child care centers). The use of the new pentavalent rotavirus vaccine will likely be more effective than the use of probiotics in preventing the most common form of acute infectious diarrhea in infants.
Antibiotic-associated DiarrheaThere is some evidence to support the use of probiotics to prevent antibiotic-associated diarrhea, but there is no evidence that it is effective for treatment. LGG, B. lactis, Streptococcus thermophilus, and Saccharomyces boulardii were the most common probiotics used in randomized controlled trials (RCTs). There have been no RCTs examining the effects of probiotic use in children with Clostridium difficile antibiotic-associated diarrhea.
Atopic DiseasesThe intestinal bacterial flora of children with atopic disease has been proven to have more Clostridium and fewer Bifidobacterium organisms than that of children

1� Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
praCtiCe GuiDelines
without atopic disease. For this reason, it has been hypothesized that the administration of probiotics to infants at risk of atopic disease—particularly those who are formula fed—would be beneficial. There is some evidence supporting the prophylactic maternal use of probiotics during pregnancy and the continuation of therapy in the mother and infant during lactation, but further studies are needed. Probiotic use has not been proven effective in the treatment of eczema.
Necrotizing Enterocolitis
Preterm infants often have delayed and aberrant acquisition of normal digestive microflora, possibly because of restricted enteral feedings and frequent administration of antibiotics. These factors are thought to contribute to an increased risk of necrotizing enterocolitis in preterm infants. There is some evidence to support the use of probiotics in very low-birth-weight infants (birth weight of 1,000 to 1,500 g [2 lb, 4 oz to 3 lb, 5 oz]). However, the amount and specific type of probiotic are difficult to determine.
Chronic Inflammatory Bowel Disease
It is estimated that up to 70 percent of children and adults with chronic inflammatory bowel disease (i.e., Crohn disease or chronic ulcerative colitis) routinely use complementary and alternative medicine, including probiotics, as adjunctive or replacement therapy for prescribed medications. Theoretically, probiotics may be beneficial in the treatment of these conditions. However, the long-term benefit of using probiotics to treat Crohn disease requires further study and is not recommended in children. The results of RCTs in which probiotics were used to treat chronic ulcerative colitis are encouraging, but require further confirmation.
Other Conditions
The sustained or long-term benefit of using probiotics to treat disorders such as irritable bowel syndrome, constipation, and extraintestinal infections requires further study; currently, use is not recommended in children. There is some evidence that probiotics may be beneficial in treating children with Helicobacter pylori gastritis and infantile colic; however, further study is needed before recom-mendations can be made. Probiotics have not been proven beneficial in treating or preventing cancer. There are safety concerns with the use of probiotics in infants and children who are immunocompromised, chronically debilitated, or seriously ill and who have indwelling medical devices.
prebioticsPrebiotics are supplements containing a nondigestible ingredient—usually in the form of oligosaccharides—that selectively stimulates the favorable growth or activity of indigenous probiotic bacteria. Although prebiotics are indigestible, their presence in the digestive tract enhances the proliferation of probiotic bacteria in the colon, especially Bifidobacterium species.
Human milk contains substantial quantities of prebiotics and is preferred for infants up to six months of age. The addition of oligosaccharides as prebiotics to infant formula is not unreasonable, but lacks evidence showing clinical effectiveness. It is not known whether their use is cost-effective.
The use of prebiotics in preventing or treating diseases in children has not been tested extensively in RCTs, but the available evidence shows that there may be some long-term benefit for the prevention of atopic eczema and common infections in healthy infants. However, confirmatory studies, especially in children who are given formula that is not partially hydrolyzed, are needed before recommendations can be made.
n n n

1�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
casting vs. splinting for wrist Fractures in childrenBackground: Fracture of the distal radius is the most common fracture in children. These fractures are traditionally placed in a short arm cast for four to six weeks, but this can lead to poor hygiene and can cause additional damage if the cast fits poorly. Additionally, use of the cast saw can cause distress in children. Evidence from studies involving adults has shown splinting to be a safe alternative, but it has yet to be confirmed in children. Boutis and colleagues conducted a randomized controlled trial to determine if splinting was as effective as casting in the treatment of minimally angulated wrist fractures in children.
The Study: The authors enrolled children five to 12 years of age with minimally angulated (15 degrees or less) greenstick or transverse fractures of the distal radius. Of the 96 children who met inclusion criteria, 46 were placed in a splint and 50 were placed in a cast, each for four weeks. Children in splints were advised to remove the splint only for hygienic reasons. The angle of displacement of the bone was determined in the sagittal plane of the radiography. The authors defined 15 degrees or less as translation displacement of 5 mm or less on the frontal plane. Children with an injury that was older than five days; who had a buckle, open, or pathologic fracture; or whose fracture involved the growth plate were excluded from the study. Additionally, children with congenital wrist anomalies, coagulopathies, multisystem trauma, multiple injuries to the same limb, or developmental delay were excluded. Six weeks after the initial application of the immobilization
From the Journals ...
device, physiotherapists assessed the children’s physical function, using single-blinded methodology. Parents completed a weekly diary to record pain scores and compliance with treatment and were contacted three months after treatment to assess recovery.
Results: The authors found no significant differences between the groups based on each patient’s range of motion, grip strength, and ability to complete activities six weeks after initiation of treatment. There were also no significant differences between the immobilization devices in the irritation, itching, and discomfort reported. Six children had to wear their immobilization device for an additional two weeks because the angulation of their fracture had increased to 25 degrees by the fourth week; these children were evenly divided between the two groups. Based on parental reports, splint use became less frequent by the end of four weeks. The primary difference between the groups occurred at week 6 when 5 percent of parents and 12 percent of children in the splint group reported they would have preferred a cast, whereas 60 percent of parents and 68 percent of children in the cast group reported they would have preferred a splint. None of the children required surgical intervention during the follow-up period.
Conclusion: The authors conclude that splinting appears to be safe, effective, and preferred by patients and parents. However, care must be taken to correctly diagnose fracture type to determine whether splinting is an appropriate alternative to casting.
n n n
researCh review
Source: Adapted from Am Fam Physician. 2011;83(9):1103-1104.

18 Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
From eMedinewS ...
Dose-rounding Guidance for Pediatric Meds DevelopedResearchers have developed evidence-based and expert-validated dose-rounding recommendations for more than 100 medications commonly prescribed to children. The information can be used by existing and developing electronic prescribing systems to automatically calculate safe doses of these medications for young children, Kevin B. Johnson, MD, from Vanderbilt University School of Medicine, Nashville, Tennessee, and colleagues write in an article published online July 25 and in the August issue of Pediatrics. (Source: Medscape Medical News)
ADHD Kids Unlikely to Follow Crosswalk RulesAlthough children with attention–deficit/hyperactivity disorder, combined type (ADHD–C) behave largely the same as other children when crossing the street, they chose to cross in riskier situations, researchers found. The findings suggest that executive dysfunction might at least partly explain why kids with ADHD–C have a higher pedestrian injury risk than those with typical development, and those with other develop- mental disabilities, according to Despina Stavrinos, PhD, of the University of Alabama at Birmingham, and colleagues. (Source: Medpage Today)
Rapid TB Test Reliable in KidsA rapid automated test for tuberculosis –– already recommended by the World Health Organization for disease detection in adults –– proved more effective than smear microscopy for identifying Mycobacterium tuberculosis infection in children, a large prospective study found. Using two induced sputum samples from children whose median age was 19.4 months, the Xpert MTB/RIF test detected 75.9% (95% CI 64.5 to 87.2) of cases of tuberculosis, according to Mark P. Nicol, PhD, of the University of Cape Town in South Africa, and colleagues. In contrast, smear microscopy only detected 37.9% (95% CI 25.1 to 50.8), the researchers reported online in The Lancet. Diagnosis of tuberculosis –– particularly in the lower–income parts of the world where the disease flourishes –– typically has relied on smear microscopy. (Source: Medpage Today)
What is the Role of Liver Transplantation in Wilson’s Disease?Liver transplantation is the only effective option for those who present with acute liver failure in Wilson’s disease. It is also indicated for all patients of WD with decompensated liver disease who are unresponsive to medical therapy. Some individuals who undergo transplantation for decompensated cirrhosis have had psychiatric or neurologic symptoms, which improved after liver transplantation but liver transplantation primarily for neurological symptoms is not indicated.
—Dr. Neelam Mohan, Director Pediatric Gastroenterology, Hepatology and
Liver Transplantation, Medanta – The Medicity
Parents are the Key to Preventing Childhood Obesity: StudyA recent study conducted at Maastricht University in the Netherlands reported some new and interesting findings about childhood obesity. Their study, published in the International Journal of Obesity, found that treating parents of obese and overweight children was effective in helping kids to lose weight. The study did not treat kids – only parents – and the intervention was still effective. The study enrolled the parents of 98 overweight or obese children (aged from seven to 13) in training sessions aimed at helping their children lose weight. Parents were randomly assigned to either a treatment group or a waiting list (the control group). Training sessions occurred over the span of ten weeks. The study found that children’s weight decreased significantly in the treatment group. However, there was no change in weight in the waiting–list control group. Researchers followed up three months after the study and found that there was no weight gain or relapse in the children whose parents attended the treatment group. These novel study results show more evidence reinforcing the long standing idea that parents should be accountable for children’s weight. Now, researchers plan to replicate the study with a larger group, and these methods should be considered when planning treatment approaches for childhood obesity
—Rajat Bhatnagar, International Sports & Fitness Distribution, LLC,
http://www.isfdistribution.com
emedinews section

1�Asian Journal of Pediatric Practice, Vol. 14, No. 4, April-June 2011
liGhter reaDinG
an inspirational story
A little Mouse
A mouse looked through a crack in the wall to see the farmer and his wife opening a package. What food might it contain? He was aghast to discover that it was a mouse trap. Retreating to the farmyard the mouse proclaimed the warning: “There is a mouse trap in the house, a mouse trap in the house! “The chicken clucked and scratched, raised her head and said, “Excuse me, Mr. Mouse, I can tell this is a grave concern to you, but it is of no consequence to me. I cannot be bothered by it.” The mouse turned to the pig and told him, “There is a mouse trap in the house, a mouse trap in the house!” “I am so very sorry Mr. Mouse,” sympathized the pig, “but there is nothing I can do about it but pray. Be assured that you are in my prayers. “The mouse turned to the cow. She said, “You say, Mr. Mouse. A mouse trap? Like I am in grave danger....NOT!”
So the mouse returned to the house, head down and dejected, to face the farmer’s mouse trap alone. That very night a sound was heard throughout the house, like the sound of a mouse trap catching its prey. The farmer’s wife rushed to see what was caught. In the darkness, she did not see that it was a venomous snake whose tail the trap had caught. The snake bit the farmer’s wife. The farmer rushed her to the hospital. She returned home with a fever. Now everyone knows you treat a fever with fresh chicken soup, so the farmer took his hatchet to the farmyard for the soup’s main ingredient. His wife’s sickness continued so that friends and neighbors came to sit with her around the clock. To feed them, the farmer butchered the pig. The farmer’s wife did not get well and a few days later she passed away. So many people came for her funeral that the farmer had the cow slaughtered, to provide meat for all of them to eat. So the next time you hear that someone is facing a problem and think that it does not concern you, remember that when the least of us is threatened, we all may be at risk.
We are all one family on this planet Earth!
Lighter Reading
did You knowAvocados have the highest calories of any fruit at 167 calories per hundred grams.Strawberries are the only fruits whose seeds grow on the outside.
—Dr Uday Kakroo
mind teasertimertimer Answer: Two–timer
idiomsBack seat driver: People who criticize from the sidelines, much like someone giving unwanted advice from the back seat of a vehicle to the driver.Against the clock: Rushed and short on time.Add fuel to the fire: When something is done to make a bad situation even worse than it is.Actions speak louder than words: It’s better to actually do something than just talk about it.
laugh a whileThis is how our new generation may end up learning the alphabets:
A – AppleB – BlackberryC – ChattingD – DownloadE – EmailF – FacebookG – GoogleH – HotmailI – iTunesJ – JavaK – KasperskyL – LaptopM – Microsoft
N – NintendoO – OutlookP – PlaystationQ – Quicktime R – RapidShareS – SkypeT – TwitterU – USBV – VistaW – WikipediaX – XPY – YouTubeZ – Zorpia

Mail this coupon to : IJCP Publications Pvt. Ltd.Head Office: E - 219, Greater Kailash, Part - 1, New Delhi - 110 048Telefax: 40587513 Mob.: 9891272006Subscription Office: 5E, Merlin Estates, 25/8 Diamond Harbour Road, Kolkata - 700 008Tele No.: 033-24452066 Mob.: 9831363901, E-mail: [email protected], Website: www.ijcpgroup.com
Yes, I am interested in subscribing to the *Institutional Combo Package for one year (Institutional)Yes, I am interested in subscribing to the following journal(s) for one year (Institutional) (Individual)
ISSUES/YEAR INSTITUTIONAL ( Amount)` INDIVIDUAL ( Amount)`JOURNALS
12
4
4
12
4
Asian Journal of
Ear, NoseThroatEar, NoseThroat
4
12 3,500/- 1,650/-
550/-1,200/-
3,500/- 1,650/-
1,200/- 550/-
1,200/- 550/-
1,200/- 550/-
1,200/- 550/-
6 1,500/- 750/-
Payment Information: Total 14,500/- for 1 Year`
Name: ............................................................................................
Speciality: ......................................................................................
Address: ........................................................................................
........................................................................................
Country: ..................................... State: .......................................
Pincode: ....................................
Telephone: ............................... Mobile: ......................................
E-mail: ...........................................................................................
Pay Amount: ......................................................................................
Dated (dd/mm/yyyy): ..........................................................................
Cheque or DD No.: .............................................................................
Drawn on Bank: ................................................................................
Special Discounton Institutional
Packages` 1000/-
Save
Subscription Form (Jan-Dec 2011)
Cheques/DD should be drawn in favor of “M/s IJCP Publications Pvt. Ltd.”
We accept paymentsby Cheque/DD only,Payable at New Delhi.Do not pay Cash.
Subscribe to all JournalsYou Pay 13,500/-`