albany medical center hospital pps pac meeting · consumer and community affairs meeting schedule -...
TRANSCRIPT
Albany Medical Center Hospital PPS PAC Meeting
September 15, 2016

Meeting Attendance
Please email confirmation of your participation in today’s meeting to
Name and Organization is required within 24 hours
2

Agenda
• PMO Updates
• NYSDOH CBO Planning Grant Update
• Committee Updates
• Performance Reporting (IDS_E7)
• Project Updates
• Questions
3

PMO Updates
• Welcome Michael Ardieta
• September Contract Deliverable Trainings
• 9/30 Deliverables on track for submission on October 28th
• Patient Registries Due 9/15
4

September Training Webinars • AMCH PPS Compliance Training
– Friday August 19, 9-10
• AMCH PPS Information Technology Onboarding and Training
– Friday September 9, 9-10:30
• Workforce Reporting Webinar
– Friday September 16, 2-3:30
• CBO & Provider Networking Webinar
– Monday September 19, 1:30-3
• AMCH PPS Partner Reporting
– Tuesday September 20, 1-2:30
• AMCH PPS Cultural Competency Training
– Thursday September 29, 10-11:30
5
NYSDOH Community Based Organization Planning Grant Update
6

.
Please join us for the Bridges to Health and Healthcare Symposium
Wednesday, October 5, 2016 4 - 7:30 p.m.
CDPHP Patroon Cafe
500 Patroon Creek Blvd., Albany, NY
Opening remarks by Dr. John D. Bennett President and CEO of CDPHP
You are invited to join CDPHP, key stakeholders, and other health care professionals as we explore ways to improve public health outcomes with internationally-acclaimed author Dr. Ruby Payne and co-author Terie Dreussi-Smith, based on their groundbreaking book Bridges to Health and Healthcare: New solutions for improving access and services.
Enjoy dinner and learn effective strategies for engaging patients across the economic spectrum, communicating complex information, and reducing costs while achieving more successful patient outcomes.
Register for the symposium today! More details available here.
Please RSVP by Wednesday, September 21.
Seating is limited!
Questions? Contact Kathy Leyden at (518) 641-3298.
This email was sent by: Capital District Physicians' Health Plan, Inc.
500 Patroon Creek Blvd. Albany, NY 12206.
If you prefer not to receive emails from CDPHP, unsubscribe here.
© 2016 All rights reserved. Privacy policy
Upcoming Event
PPS partners are encouraged to attend this exciting
symposium sponsored by CDPHP on October 5, 2016.
Registration is free and dinner is provided.
Click on the link below to register by September 21st-
seating is limited!
Register
Contact [email protected] if you need more information.

Audit and Compliance MANDATORY TRAINING REMINDER
• Compliance Training is a required deliverable in your phase I contract.
• Initial training for all of your affected employees must be completed by 9/30/16.
• You must submit your completed Sign-in sheet and Attestation by 10/15/16 to receive your incentive payment and to remain an active partner in any DSRIP initiative.
• Starting 10/1/16 all new affected persons hired must receive DSRIP compliance training within the current DSRIP quarter they are hired into.
• All Compliance trainings must be reported in the DSRIP quarter they were completed to receive credit.
• The training video and attestation form are located on website: albanymedpps.org - committees tab - additional documents.
• PPS Audit and Compliance contact:
Todd Faubel
518-264-4967
8

Consumer and Community Affairs
Meeting Schedule - Every other month • Remaining 2016 meetings:
– Tuesday, October 11th-Location TBD – Tuesday, December 13th-Location TBD
• Collaboration & Networking – CBO Networking Webinar-9/19 – Northern Hub-CBO’s and Saratoga Hospital – Southern Hub-CBO’s and Columbia Memorial Hospital
• Consumer Listening Sessions being held through October 31st – Alliance for Positive Health – Alvarado-Little Consulting – Promesa Inc. – NY Statewide Senior Action Council
Kendal Pompey: [email protected]
9
Cultural Competency & Health Literacy • First CC/HL Training
– Introductory to CCHL: Thursday, September 29th at 10-11:30am
• Conducted by Wilma Alvarado-Little
• Learning objectives include: – Discuss health literacy and cultural and linguistic barriers to accessing healthcare
– Develop an awareness of federal, state and local mandates
– Provide resources regarding the provision of quality culturally and linguistically appropriate services (CLAS) to address barriers contributing to health disparities within our communities
– Invited attendees
• Primary Contacts, CCHL Champions, Clinical Contacts
– This training webinar will fulfill metric IDS_E2 for “Cultural Competency Training”
– RSVP by Monday, September 26th to receive pre-training assessment
• CCHL Champion Meeting – Fulfills metric IDS_E9 for “Cultural Competency and Health Literacy Webinar” –
Extended completion date (10/31/16)
• Questions? Please email Mingie Kang ([email protected])
10
Finance
• Reporting Webinar - 9/20/2016 1:00-2:30pm
• Review Partner Reporting Guide
• Review Partner Reporting Template
• Budget Subcommittee – meeting weekly in September
• Budget Reforecast (in progress)
• Contract Status
• Contracted Partners
• Outstanding Contracts
11

Finance – Contracted Partners as of 9/13/2016
12
1 820 RIVER ST., INC. 30 GREENE COUNTY PUBLIC HEALTH DEPARTMENT
2 ADDICTIONS CARE CENTER OF ALBANY 31 HCDI
3 ALBANY COUNTY DEPARTMENT FOR CHILDREN YOUTH AND FAMILIES 32 HARMONY MILLS PEDIATRICS
4 ALBANY COUNTY DEPT OF HEALTH 33 HUDSON MOHAWK AHEC
5 ALBANY COUNTY NURSING HOME 34 INDEPENDENT LIVING CENTER OF THE HUDSON VALLEY, INC.
6 ALBANY MEDICAL CENTER HOSPITAL 35 IN OUR OWN VOICES
7 ALBANY MEDICAL CENTER PRACTICE 36 KOINONIA PRIMARY CARE, INC.
8 ALL METRO HEALTH CARE 37 LIGHTHOUSE GUILD, JGB FACILITIES
9 ALLIANCE FOR POSITIVE HEALTH 38 MENTAL HEALTH ASSOCIATION OF COLUMBIA-GREENE COUNTIES, INC.
10 ANY-TIME HOME CARE, INC. 39 MENTAL HEALTH EMPOWERMENT PROJECT
11 ARC OF ULSTER-GREENE 40 NORTHERN RIVERS FAMILY OF SERVICES
12 BELVEDERE HEALTH SERVICES 41 NEW YORK STATEWIDE SENIOR ACTION COUNCIL, INC.
13 CAPITAL CARE MEDICAL GROUP 42 NYSARC, COLUMBIA COUNTY CHAPTER
14 CAPITAL DISTRICT PSYCHIATRIC CENTER -OMH 43 PLANNED PARENTHOOD MOHAWK HUDSON
15 CATHOLIC CHARITIES 44 PROMESA, INC.
16 CENTER FOR DISABILITY SERVICES 45 REHABILITATION SUPPORT SERVICES, INC.
17 COLUMBIA COUNTY COMMUNITY HEALTHCARE CONSORTIUM, INC. 46 SARATOGA HOSPITAL
18 COLUMBIA COUNTY DEPT. OF HEALTH 47 SENIOR HOPE COUNSELING, INC.
19 COLUMBIA COUNTY DEPT. OF HUMAN SERVICES 48 SHAKER PEDIATRICS
20 COLUMBIA MEMORIAL HEALTH 49 SHELTERS OF SARATOGA
21 COMMUNITY CARE PHYSICIANS 50 ST. CATHERINE'S CENTER FOR CHILDREN
22 COMMUNITY CAREGIVERS, INC. 51 THE ALTAMONT PROGRAM, INC.
23 COMMUNITY HEALTH CENTER 52 TRANSITIONAL SERVICES ASSOC., INC.
24 CONIFER PARK 53 TRINITY
25 DAUGHTERS OF SARAH NURSING CENTER 54 TWIN COUNTY RECOVERY SERVICES, INC.
26 DEPAUL HOUSING 55 UPPER HUDSON PLANNED PARENTHOOD
27
ENS HEALTH CARE MANAGEMENT, LLC D/B/A INTERIM HEALTHCARE OF
THE CAPITAL REGION 56 VNA HOME HEALTH
28 EQUINOX 57 WHITNEY M. YOUNG, JR. HEALTH CENTER
29 GREENE COUNTY MENTAL HEALTH CENTER 58 WILDWOOD PROGRAMS
EXECUTED AGREEMENTS AS OF 9.13.2016
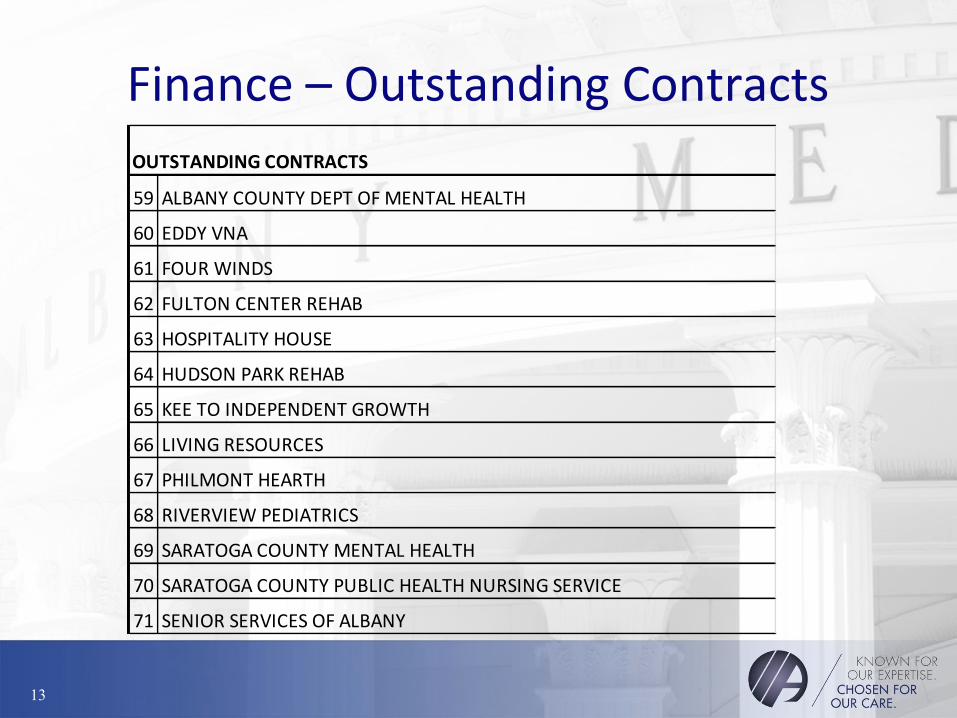
Finance – Outstanding Contracts
13
OUTSTANDING CONTRACTS
59 ALBANY COUNTY DEPT OF MENTAL HEALTH
60 EDDY VNA
61 FOUR WINDS
62 FULTON CENTER REHAB
63 HOSPITALITY HOUSE
64 HUDSON PARK REHAB
65 KEE TO INDEPENDENT GROWTH
66 LIVING RESOURCES
67 PHILMONT HEARTH
68 RIVERVIEW PEDIATRICS
69 SARATOGA COUNTY MENTAL HEALTH
70 SARATOGA COUNTY PUBLIC HEALTH NURSING SERVICE
71 SENIOR SERVICES OF ALBANY
Finance – IA Onsite Audit The DSRIP Independent Assessor (IA) will be conducting onsite audits in the upcoming months and is beginning the process of coordinating a schedule. A member of the IA team will contact you before the end of this week regarding the date of your onsite. This audit will encompass DSRIP year one (DY1) activities as well as Mid-Point Assessment topics. The IA will use the onsite audit to facilitate discussion and to assess the PPS’ overall progress toward meeting DSRIP goals. The intent is not to burden the PPS with any additional documentation requirements. We recognize that each PPS is unique. As such, the IA will review the documentation developed by your PPS that best supports your progress towards meeting the items below. Specific areas the IA Team expects to cover and discuss with each PPS include: a) Governance: PPS should be prepared to discuss the ongoing activities of the DSRIP governance structure, including monitoring of governance effectiveness, the role of sub-committees under your governance structure, and the process for capturing feedback from your partners and community. b) Cultural Competency & Health Literacy: PPS should be able to speak to your efforts for implementing your Cultural Competency training plan across your PPS network partners. c) Performance Reporting: PPS will be asked to provide supporting documentation for DY1 PPS Quarterly Report submissions for Actively Engaged and Funds Flow. The IA will provide the PPS with a formal documentation request approximately two weeks prior to the onsite. d) Financial Sustainability: PPS should be prepared to discuss your plans for assessing the financial stability of your network partners and monitoring those partners that are identified as financially fragile. The PPS should also be prepared to discuss your plans for supporting your partners in moving towards Value Based Purchasing. e) Expanding Access to Primary Care: PPS should be prepared to discuss your efforts to assess primary care network activities, including your assessment of network partners’ current PCMH status, your plans to support the move of your PCMH eligible partners to the DSRIP PCMH goals, and for monitoring the progress of network partners towards the PCMH goal. Other areas of focus may be added depending on individual PPS progress through your DY1, Q4 Quarterly Report.
14

Technology & Data Management/ EHR Sub-Committee
• Next TDMC meeting 9/21/16
• EHR Subcommittee: Co-Chaired by Dr. Manjunath and Azmat Ahmad;
met on 9/17/16. Agenda items included a DSRIP overview and an in-depth discussion of the Asthma project EHR requirements. Our next meeting will be held on 9/19/16. If your organization is interested in participating please email [email protected].
• IT Onboarding and Training WebEx for all contracted partners was held on 9/9/16 • Over 100 participants attended
• The training component of this WebEx satisfied three contract deliverables (IDS_E5, IDS_E6 and IDSR2)
• The presentation was recorded and distributed to all contracted partners
15

Performance Reporting
The Performance Reporting Workstream is charged with establishing and implementing a reporting structure and associated training strategy around dissemination and evaluation of performance measures.
• With completion of the milestone deliverables, the workstream’s effort is shifting and will include – Training of partners on our Performance Reporting
Strategy
– Communication of PPS Performance on various measures
– Contribution to rapid cycle evaluation
16

Performance Reporting cont.
Two Deliverables approved: • AMCH PPS Performance Reporting Strategy • AMCH PPS Performance Reporting Training
Strategy
• Review of Quarterly Reporting Specific to patient data
• Review of Available Dashboards and performance measures
• Review of Training Needs
17

Performance Reporting cont.
AMCH PPS’s Performance Reporting Strategy includes: • Data Collection and Information Sharing
– Patient Engagement Templates – Patient Registry Templates – Data Security and Confidentiality
• Hierarchical Reporting Structure – PPS Governance Structure – Partnering Organizations Reporting Role and PPS Role
• Reporting and Communication of Clinical Quality and Performance Measures
• Rapid Cycle Evaluation • Program Evaluation
18

Performance Reporting cont.
Dashboards • Dashboards have been developed to communicate quarterly
reporting deliverables and their relation to the target. Most frequently utilized, is the patient engagement dashboard and performance measure dashboards.
• Shared monthly or quarterly as updates occur to the PAC, PAC Leadership, and the Executive Steering Committee. Also shared with committees and sub-committee meetings as needed.
19

Performance Measure Dashboards DRAFT
20

Performance Measure Dashboards DRAFT
21
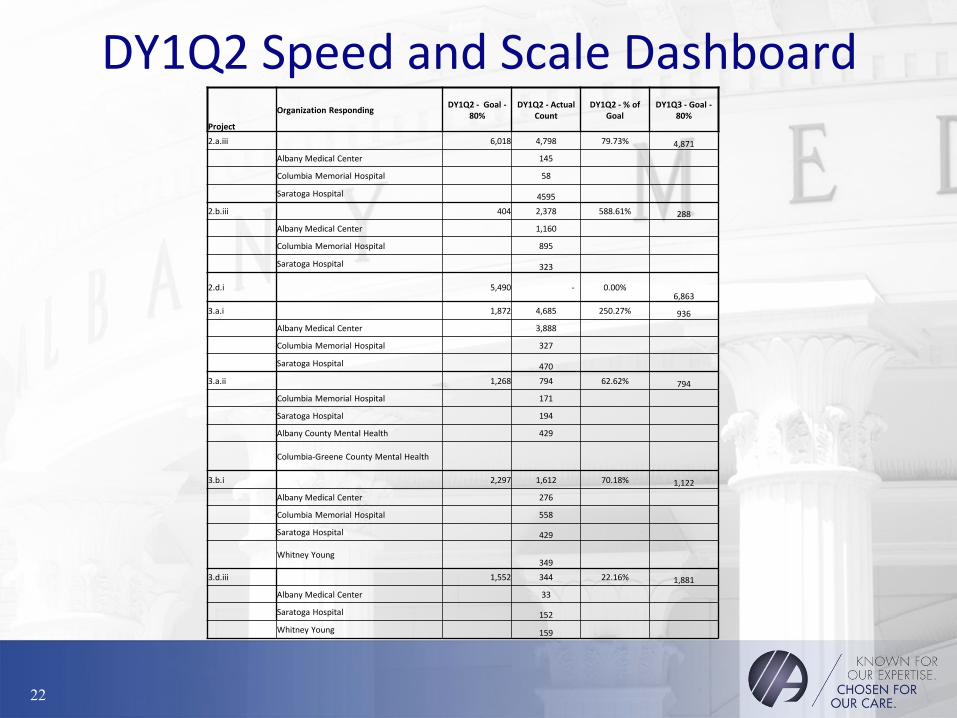
DY1Q2 Speed and Scale Dashboard Project
Organization Responding DY1Q2 - Goal -
80% DY1Q2 - Actual
Count DY1Q2 - % of
Goal DY1Q3 - Goal -
80%
2.a.iii 6,018 4,798 79.73% 4,871
Albany Medical Center 145
Columbia Memorial Hospital 58
Saratoga Hospital 4595
2.b.iii 404 2,378 588.61% 288
Albany Medical Center 1,160
Columbia Memorial Hospital 895
Saratoga Hospital 323
2.d.i 5,490 - 0.00% 6,863
3.a.i 1,872 4,685 250.27% 936
Albany Medical Center 3,888
Columbia Memorial Hospital 327
Saratoga Hospital 470
3.a.ii 1,268 794 62.62% 794
Columbia Memorial Hospital 171
Saratoga Hospital 194
Albany County Mental Health 429
Columbia-Greene County Mental Health
3.b.i 2,297 1,612 70.18% 1,122
Albany Medical Center 276
Columbia Memorial Hospital 558
Saratoga Hospital 429
Whitney Young 349
3.d.iii 1,552 344 22.16% 1,881
Albany Medical Center 33
Saratoga Hospital 152
Whitney Young 159
22

DY1Q3 Speed and Scale Dashboard Organization Responding DY1Q3 - Goal - 100%
DY1Q3 - Goal -
80%
DY1Q3 - Actual
CountTotal
2.a.iii 6,089 4,871 5,448
Columbia Memorial Hospital 21
Albany County DMH 654
2.a.v 0 - -
2.b.iii 360 288 3,620
Albany Medical Center 586
Saratoga Hospital 63
Columbia Memorial Hospital 595
2.d.i 8,579 6,863 -
3.a.i 1,170 936 8,080
Albany Medical Center 2164
Saratoga Hospital 113
Columbia Memorial Hospital 410
RSS 41
Albany County DMH 729
MHA Columbia-Greene County 38
3.a.ii 992 794 966
RSS 13
Albany County DMH 159
MHA Columbia-Greene County **291
3.b.i 1,403 1,122 2,276
Albany Medical Center 244
Columbia Memorial Hospital 492
RSS 253
3.d.iii 2,351 1,881 554
Albany Medical Center 38
Saratoga Hospital 102
Columbia Memorial Hospital 58
Harmony Mills 11*291 aggregate data collected but not reportable this quarter
23

DY1Q4 Speed and Scale Dashboard Project Organization Reporting Unduplicate Patients Reported Project Goal (80%) Reported to date
2aiii 11402 5589
Albany Medical Center 111
Columbia Memorial Hospital 30
2av - 0 80 0
2biii 686 4589
Albany Medical Center 477
Columbia Memorial Hospital 491
Saratoga Hospital 1
2di 9066 4835
Albany Medical Center 1012
Catholic Charities 611
Columbia Memorial Hospital 376
Community Health Center 2
Saratoga Hospital 2835
3ai 2434 10333
Albany Medical Center 1043
Capital Care 573
Center For Disability Services 13
Columbia Memorial Hospital 519
Philmont 8
Saratoga Hospital 97
3aii 1506 1757
Albany County Department for Children
Youth & Families 15
MH Association of Columbia & Greene
County 580
Northern Rivers 193
Philmont 3
3bi 4020 3316
Albany Medical Center 951
Columbia Memorial Hospital 481
Philmont 8
3diii 2156 672
Albany Medical Center 4
CoARC 4
Columbia Memorial Hospital 32
Philmont 2
Saratoga Hospital 76
24

DY2Q1 Speed and Scale Dashboard Project Organization Reporting Unduplicate Patients Reported Project Goal (80%) Reported to date
2aiii 7582 5645
Albany Medical Center 11
Center for Disability Services 8
Columbia Memorial Hospital 31
Saratoga Hospital 6
2av - 0 96 0
2biii 1050 6011
Albany Medical Center 457
Columbia Memorial Hospital 567
Saratoga Hospital 398
3ai 4259 13096
Albany Medical Center 637
Capital Care 568
Center For Disability Services 50
Columbia Memorial Hospital 679
Harmony Mills 19
Hudson River Healthcare 65
Koinonia Primary Care 353
Saratoga Hospital 411
3aii 1665 2524
Alb Cty Dept. for Children Youth &
Families 13
Alb Cty Dept. of Mental Health 32
Capital District Psychiatric Center 74
MH Assn of Columbia & Greene Cty 470
Northern Rivers 158
Rehabilitation Support Services 19
Wildwood Programs, Inc. 1
3bi 4882 3558
Albany Medical Center 145
Center for Disability Services 33
Hudson River Healthcare 64
3diii 3105 825
Albany Medical Center 5
Capital Care 4
Columbia Memorial Hospital 29
Saratoga Hospital 111
VNA 4
25

DY2Q1 Speed and Scale Dashboard
2di 12240 10319
Albany Family Medicine/ CCP 1
Albany Medical Center 737
AMC Faculty Group Practice 939
Catholic Charities 514
Columbia Memorial Hospital 524
Community Caregivers 29
Greene County Family Planning 54
Healthy Capital District Initiative 21
Ind. Living Center of the Hudson Valley 1
Koinonia Primary Care 197
Planned Parenthood Mohawk Hudson 280
Saratoga Hospital 2187
26
Performance Reporting cont.
Performance Reporting Training Strategy includes:
• Assessment of Training Necessity by Focus Provider Type
• Detailed Training Programs
• Workforce Communication and Engagement for Training needs
• Expected Outcomes towards DSRIP Goal Achievement
• Training and Tracking Systems
27

Performance Reporting cont.
• Assessment of training necessity by Provider Type – Close collaboration with WCC to complete
assessment of needs across the PPS
– Utilize a variety of training modalities including LMS, in person, webinar, or any combination of these
– Understanding training needs vary by provider type
– Specific trainings necessary for PCPs, BH/SU, PCMH, Care Coordination, Clinical Integration, IT-Infrastructure, patient navigation, CCHLC, and others
28
Performance Reporting cont. Sample Training Program Outline: • DSRIP
– DSRIP 101 • At the conclusion, participants should be able to define and explain key terms in DSRIP, key projects, workforce
development, and overall DSRIP goals
– AMCH PPS Governance Structure • At the conclusion, participants should understand the structure of the AMCH PPS to include 7 standing committees, the
PAC, voting membership of the PAC Executive Committee, the PPS Board, and the basic role of workgroups and subcommittees where appropriate
– Project-specific objectives and implementation plans • At the conclusion, participants will understand key concepts associated with the approved project the AMCH PPS will
implement, project domains, milestones, tasks, as well as the actively engaged definitions. Given that there are 11 projects, there will be 11 different courses.
– Performance Measures & Achievement Values (AVs) • Utilizing DOH provided documentation and Webinars, at the conclusion, participants will understand performance
measure requirements directly associated to the AMCH PPS projects, Achievement Values (AV) and payments tied to these measures, P4R vs. P4P, gap to goal, and high performance goals
• Performance Measure overview to include the specification source of measures and data elements such as 3M, AHRQ, CAHPS, and HEDIS
– Funds flow, Value Based Payments (VBP) and Financial Sustainability • Utilizing VBP Bootcamp documentation provided by DOH, at the conclusion, participants will be able to define Value
Based Purchasing, understand how VBP can improve quality and reduce costs. The module will also discuss how VBP will impact how care is delivered.
• A detailed presentation will be provided on the AMCH PPS funds flow process, highlighting deliverables, expectations, project addenda requirements, and funding associated with each of these
– Patient Satisfaction Feedback
29

Performance Reporting cont. Sample Training Program Outline:
• Patient Centered Medical Home (PCMH)
– Principles for PCMH
– Team-Based Care/Care Team Roles
– Planned Visit & Post-visit care
• Care coordination/Care Management (see below)
• PCMH sustainability
• Meaningful Use
• Care Coordination
– A detailed training conducted through Accenture will be utilized and uploaded for viewing purposes. At the conclusion, participants will understand the Care Coordination Model Framework, elements, processes, functions, and protocols. A deep dive into ED process flows as well as Transitions of Care (ToC) in Community Settings. Tools and Templates will also be reviewed
– Role of care coordinators/navigators/community health workers
– Identification of patients appropriate for care coordination
– Tracking patients receiving Care Coordination
– Referral Tracking
• Care Management
– Overview of care management and care plans
– Ways to integrate care plans into patient workflows
– Role of Health Homes in care management and care coordination
• Clinical Integration
– A detailed training conducted through Accenture will be utilized and uploaded for viewing purposes, at the conclusion, participants will understand the Care Coordination Model Framework, elements, processes, functions, and protocols. A deep diver into ED process flows as well as ToC in Community Settings. Tools and Templates will also be reviewed
– Evidence Based Guidelines and Protocols: Adoption, Implementation and Integration
– IT-facing Clinical Integration Solutions
30

Performance Reporting cont. Sample Training Program Outline:
• Information Technology
– Effective use of Electronic Health Records (EHRs) to support DSRIP initiatives
• Participants will receive training on the AMCH PPS Change Management Process that will involve change within an EHR system to maintain success. This process outlines data reporting requirements necessary for project implementation and how an organization will change their system in order to achieve success
– Utility of HIXNY/SHIN-NY, NY Data exchange, Encounter Notification Systems
• Per DOH recommendation, AMCH PPS will work with Hixny to provide appropriate training for users of Hixny to ensure data exchange is effective and appropriate based on provider type
– Use of technology for population health management
• When appropriate, population health registry training will be available. Training will be both provider and project specific to ensure patients are tracked and reported appropriately across the AMCH PPS
– HIPPA Compliance
• Participants will have an understanding of which entities are covered by HIPPA, which health transactions are covered, safeguards required by HIPPA to ensure security and integrity of electronic health information, utilization of unique employer identifiers under HIPPA, distinguish between uses and disclosures of health information that are and are not allowed under the HIPPA Privacy Rule, and identify changes to HIPPA as they impact security and privacy rules, penalties, and enforcement
31

Performance Reporting cont. Sample Training Program Outline:
• Patient Engagement
– Patient Activation Measure (PAM)
– Coaching for Activation (CfA)
– Self-management Support
– Motivational Interviewing
– Shared Decision Making
– Stanford Chronic Disease Self-Management Program (CDSMP)
– Cultural Competency/Health Literacy
• Participants will receive a review and background of Cultural Competency and Health Literacy, a description of clinical outcomes associated with cultural competence, overview of laws and recommendations around cultural competence, and learn to identify typical characteristics of several cultural groups specific to the AMCH PPS geographic area.
• Population Health Management
– Social Determinants of Health Care
– Panel Management & Registry Use
– Predictive Analytics and Risk Stratification
– IHI Triple Aim
• Performance Improvement
• The PDSA (Plan Do Study Act) Cycle
• Process vs. Outcome Measures
• Continuous Quality Improvement (CQI)
• Continuing Education (CE) Activities
32

Workforce Coordinating Council
• DY2Q2 Deliverables – Gap Analysis (BDO)
– Workforce Transition Roadmap (BDO)
– Training Strategy (PMO, WCC)
– Impact Analysis Projections (PMO)
– Impact Analysis Actuals (Partners)
• Reporting Webinar Friday 9/16 2pm-3:30pm
• Next WCC meeting- Today! 9/15 1pm-3pm
• Training Assessment Survey due 9/30
33

Albany Medical Center Hospital
Community Caregivers Koinonia Primary Care
Albany County Department of
Health Community Health Care
Mental Health Empowerment
Project
Alliance for Positive Health Greene County Family
Planning Northern Rivers
Amida Care Harmony Mills Pediatrics Planned Parenthood
Mohawk Hudson
Black Nurses Coalition HCDI Saratoga Hospital
Catholic Charities Healthcare Consortium Shelters of Saratoga
Columbia County Mental Health
Center
Hudson River Health
Care
St. Catherine’s Center for
Children
Columbia Memorial Hospital
Independent Living
Center of the Hudson
Valley
Trinity Alliance
Project 2.d.i
Implementation of Patient Activation Activities to Engage, Educate and Integrate the Uninsured and Low and Non-utilizing Medicaid Populations into Community-based Care
Total PAM® trained individuals as of 09/12/16 = 200+.
Total number of Patient Activation Measures completed as of 09/12/16 = 12,977.
The project team continues to roll out the “train the trainer” model across the five counties of the PPS.
The next 2.d.i project work group meeting is scheduled for October 27, 2016.

Project 2.d.i- Patient Activation
0
500
1000
1500
2000
2500
3000
Jan '16 Feb '16 Mar '16 Apr '16 May '16 Jun '16 Jul '16 Aug '16 Sept '16
495 463 576
419
960 936
407
1174
1669
1179
718
596
410
401
71 91
63
830
482
351
261
157
118
24
PAM DASHBOARD AMCH PPS / 2di Project
PAMs by Hub @09/12/'16 (n=12,977)
Southern Region
Northern Region
Capital Region

Questions???
DSRIP Project Management Office
**Please be sure to email us your name and your organization at the email above to get credit for your participation in today’s meeting**
Please also notify us of any changes to your organization’s contact list or committee membership
For additional information, please visit our website:
www.albanymedpps.org
36

Thank you!

AMCH PPS
Clinical & Quality Affairs Committee
September 15, 2016
AMCH PPS: Clinical & Quality Affairs (CQA) Committee
Presentation Objectives:
• Project Implementation Updates:
– BH Projects
– ED Care Triage
– Asthma & Telemedicine
– Health Home at Risk
– Cardiovascular Disease
• AMCH PPS CAHPS Survey Report

AMCH PPS
Project updates

3.a.i – Integration of Primary Care and Behavioral Health Services
Project Objective:
Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
• Co-Chairs: Keith Stack, The Addictions Care Center of Albany, Inc. & Brendon Smith, PhD, AMCH PPS
Key updates:
• Model-specific workgroups continue to support ongoing and planned service integration.
• Presentations on Pay For Performance BH measures and incentives; Partners identifying interventions for Pay For Performance progress.
• Current State Assessment was sent out 8/16/16. Due back on 9/30/16.
• Progress integrating primary care and behavioral health services was one of six key elements in the Primary Care Plan, submitted to the DOH on 8/30 as Mid-Point Assessment deliverable.
Next Steps:
• Continue to support implementation through presentations, workgroup meetings, individual partner meetings, and analysis of Current State Assessment results.
• AMC Pediatrics to present on integrated behavioral health model.
• Proposed presentations on metabolic screenings in integrated care settings.
• DY2 Q4 deliverables, including Sub-committee/Workgroups to develop collaborative evidence-based standards of care.

3.a.ii – Behavioral Health Community Crisis Stabilization Services
Project Objective:
To provide readily accessible behavioral health crisis stabilization services, that allow access to appropriate levels of care and support rapid de-escalation of the crisis.
• Co-Chairs: Tyleia Harrell, LCSW-R, Albany County Department of Mental Health & Brendon Smith, PhD, AMCH PPS
Key updates:
• Sub-Committee reconvened to support ongoing and planned service integration.
• New partners join, as a result of Phase 1 Contracting efforts.
• Presentations on Pay For Performance BH measures and incentives; Focus on high-performance measures; Partners identifying interventions for Pay For Performance progress.
Next Steps:
• Support implementation through presentations, sub-committee meetings, and individual partner meetings.
• Focus on supporting regional implementation of BHCS project.
• Presentation on Parson’s Child and Family Center’s proposed BH Crisis Stabilization Center.
• DY2 Q4 deliverables, including Sub-Committee drafting treatment protocols for review by CQAC and PPS dissemination.

2.b.iii – ED Care Triage • Project Objective:
– To develop a care coordination/care transition program that will assist patients to link with a PCP
– To provide supportive assistance to transitioning members to the least restrictive environment
• Key Updates:
– ED Care Triage Subcommittee meeting held on September 7th
– Asthma Pathway presentation from Dr. Dick
– Discussion about access to primary care
– Discussion on processes/steps for patient navigators
• Next Steps:
– Continue to support the implementation of patient navigator resources within ED setting
– Enhance PC and BH participation in ED subcommittee deliberations
• Next Meeting: Monday, October 3rd at 10am

3.d.iii: Implementation of Evidence Based Medicine Guidelines for Asthma Management
• Project Objective:
Ensure access for all patients with asthma to care consistent with evidence-based
medicine guidelines for asthma management.
• Key updates:
•Update on Project-Related IT Requirements
• Review of 3.d.iii Deliverables & Data Sources
• Review of Co-Management Agreement Template
• Training materials sent out week of 9/4 for PCPs and applicable clinical staff
•Next steps:
– Focus on completing all milestones by 9/30/2016
–Discuss and Identify opportunities to improve Pay for Performance measures
• Next Meeting: October 14, 2016, 12-1 PM

2.a.iii – Health Home At-Risk Intervention
• Project Objective:
Expanded access to community primary care services (PCMH 2011 Level III certified sites)
and develop integrated care teams to meet the individual needs of higher risk patients
who do not currently qualify for NYS Health Home services.
• Key updates:
– Development of a pilot project in Columbia and Greene Counties in collaboration
with CMH and our Health Home downstream providers in those counties.
• Next steps:
– Begin pilot project implementation October 2016
– Continue to focus on strengthening PCMH involvement
– Focus on Pay for Performance measures
• Next meeting: October 10th, 2016 at 8 AM

3.b.i: Evidence-Based Strategies for Disease Management in High Risk/Affected Populations (Adults Only) – “CVD Project”
• Project Objective:
To support implementation of evidence-based best practices for disease management in medical practice for adults with cardiovascular conditions.
• Key updates:
– ACDOH Community Health worker program overview
– Project progress review for 9/30 deliverables • Implementation of walk-in BP screening policy and procedure
• Adoption of tools to document self-management goals
• Web-based training on providing support for self-management
• Next steps:
– Discuss and Identify opportunities to improve Pay for Performance measures
– Review and approve cholesterol management guidelines for adoption.
• Next Meeting: Friday, October 7, 2016, 8-9am. Rm: South Clinical Campus Conference Room/WebEx

AMCH PPS Performance Measures:
MY 1 CAHPS Survey Report

C&G CAHPS & H-CAHPS Survey
• Background
• Potential Incentives – GNYHA Analysis – July 2016
• Project Distribution
• Medicaid Members - July 2016 CQI Report – Summary
• Survey administration for uninsured individuals – project 2.d.i

C&G CAHPS & H-CAHPS Survey - Overview
• The CAHPS survey assesses patients' experiences with health care providers,
hospitals and staff in doctors' offices. Survey results can be used to:
• Improve care provided by individual providers, sites of care, medical
groups, or provider networks.
• Equip consumers with information they can use to choose physicians and
other health care providers, physician practices, or medical groups.
• CAHPS Survey: NYS DOH will be required to collect and report these
performance measures as appropriate.
• Incentives are linked to PPS performance on measures as compared to
identified DOH goals.
Ref: AHRQ & NYSDOH

C&G CAHPS & H-CAHPS Survey - Overview
• Questions address domains of patient experience and service delivery in the following areas;
– getting timely appointments,
– care and information – tobacco cessation and Aspirin use,
– communication with doctors,
– overall satisfaction with the provider,
– care coordination and care transitions,
– health promotion - Flu vaccine,
– health literacy.
• MY 1 Survey Period (DOH)– September 14, 2015 through December , 2015
• For our PPS – 1,500 surveys sent to adults, 453 responses (31.8% response rate)
• Total incentives at stake – Approx. $ 14,033,041 (nearly 25% of P4P incentive)
C&G CAHPS & H-CAHPS Survey – Project Distribution
DOH reported survey:
• System Transformation Domain - 2.a.i, 2.aiii, 2.a.v, 2.b.iii
• Clinical Improvement Domain – 3.b.i (CVD Project)
PPS reported survey:
• 2.d.i project – Patient Engagement Project (PAM project)

Edit the text with your own short phrases.
The animation is already done for you; just copy and paste the slide into your existing presentation.
MY 1
MY 3
MY 2 2.d.i
survey

Domain 2 – Performance Measures – (“Non-MAPP”) AMCH PPS Performance Measures – Domain 2 (minus 2.d.i) February 2016
1
Measure Name AV DOH/PPS
DY 2 and 3
DY 4 and 5
Percent of total Medicaid provider reimbursement received through sub-capitation or other forms of non-FFS reimbursement
1 DOH P4R P4R
Percent of eligible providers meeting Meaningful Use Criteria, who have participating agreements with qualified entities (RHIOs) and are able to participate in bi-directional exchange
1 DOH P4R P4R
Percent of PCP Providers meeting PCMH (NCQA or Advance Primary Care (SHIP) Standards
1 DOH P4R P4R
Primary Care- Usual Source of Care-Q2 0.5 DOH P4R P4P Primary Care- Length Relationship-Q3 0.5 DOH P4R P4P
Getting Timely Appointments, Care and information (Q6, 8, and 10)
1 DOH P4R P4P
Medicaid Spending on ER and Inpatient Services 1 DOH P4R P4R
Medicaid Spending on Primary Care and community based behavioral health care
1 DOH P4R P4R
H-CAHPS-Care Transition Metrics (Q23, 24, and 25) 1 DOH P4R P4P Care Coordination (Q13, 17 and 20) 1 DOH P4R P4P

Domain 2 Performance Measures (minus 2.d.i) – C&G CAHPS
Measure Name Specs.
Version
Numerator Description Denominator
Description
MY 1
Results
MY 2
Targets
Performance Goal
*High Perf. eligible
#Statewide measure
Achievement Value Report
DOH/
PPS
Pmt.
DY 2
Pmt.
DY 3, 4 and
5
Primary Care-
Usual Source of
Care-Q2
(AV = 0.5)
1351a_C&G
CAHPS Adult
Primary
Care
(Version
3.0)
Percent of Reponses ‘Yes’ All responses
79.3%
80.6%
92.5%
#SW measure
0.5 if annual improvement
target or performance goal
met or exceeded
NYS
DOH
P4R P4P
Primary Care-
Length
Relationship-Q3
(AV = 0.5)
As above
Percent of Responses at least
‘1 year’ or longer
All responses
79.8%
80.5%
86.5%
#SW measure
0.5 if annual improvement
target or performance goal
met or exceeded
NYS
DOH
P4R P4P
Getting Timely
Appointments,
Care and
information (Q6,
8, and 10)
(AV = 1)
As above
Number responses ‘Usually’
and ‘Always’ got appt for
urgent care or routine care as
soon as needed, and got
answers the same day if
called during the day
Number who
answered they
called for
appointments or
called for
information
87.1%
87.7%
92.5%
#SW measure
1 if annual improvement
target or performance goal
met or exceeded
NYS
DOH
P4R P4P
Care Coordination
(Q13, 17 and 20)
(AV = 1)
As above
Number responses ‘Usually’
or ‘Always’ that provider
seemed to know important
history, follow up to give
results from tests, and talked
about all prescription
medicines
All responses
94
94.3
97
89.9%
90.1%
91.9%
#SW measure
1 if annual improvement
target or performance goal
met or exceeded
NYS
DOH
P4R P4P
H-CAHPS-Care
Transition
Metrics (Q23, 24,
and 25)
V9.0 Average of hospital specific
results for the Care
Transition composite using
‘Strongly Agree’ and ‘Agree’
responses
Hospitals with H-
CAHPS
participating in
the PPS network
94% 94.3% 97% 1 if annual improvement
target or performance goal
met or exceeded
NYS
DOH
P4R P4P

C&G CAHPS Survey - Primary Care: Usual Source of Care
Primary Care- Usual
Source of Care-Q2
(AV = 0.5)
Percent of Reponses ‘Yes’ (n=286)
All responses (n=361)
79.3 (n=286) 79.0 80.6 (n=291)
92.5 (n=334)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020

C&G CAHPS Survey - Primary Care: Length of Relationship
Primary Care- Length
of Relationship-Q3
(AV = 0.5)
Percent of Responses at
least ‘1 year’ or longer (n=342)
All responses (n=429)
79.8 (n=342)
74.00
80.5 (n=345)
86.5 (n=371)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020
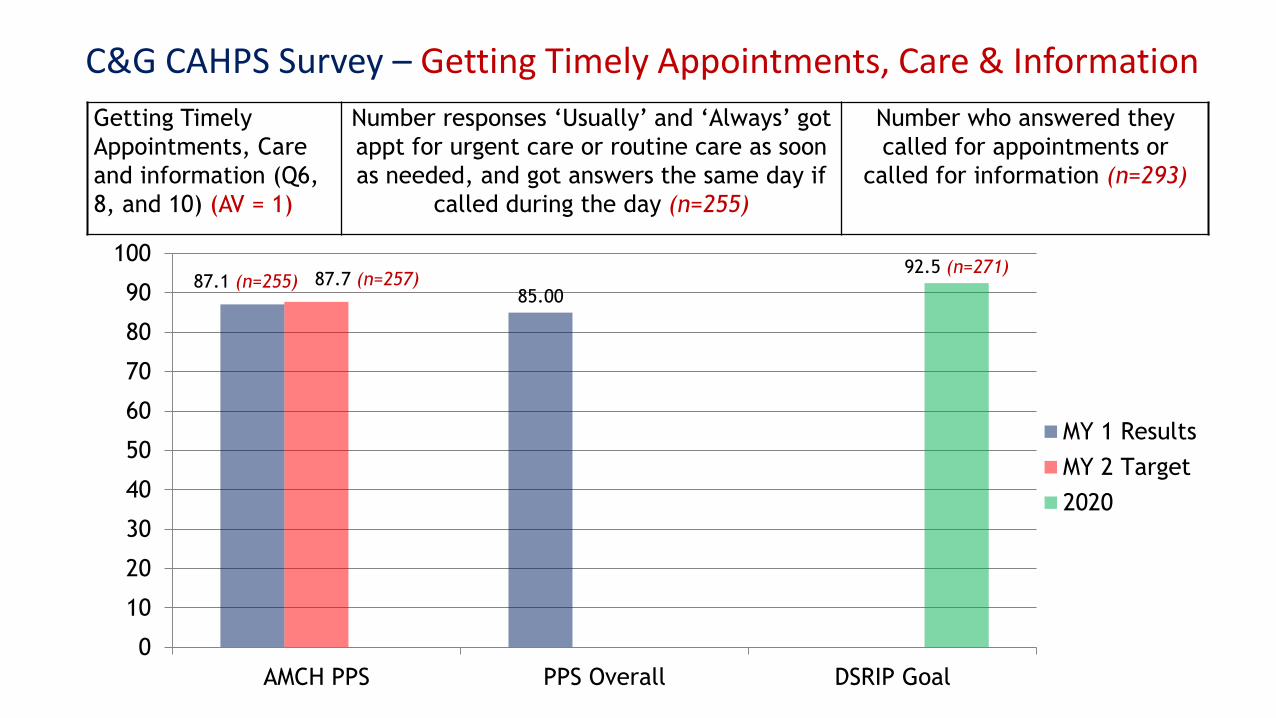
C&G CAHPS Survey – Getting Timely Appointments, Care & Information
Getting Timely
Appointments, Care
and information (Q6,
8, and 10) (AV = 1)
Number responses ‘Usually’ and ‘Always’ got
appt for urgent care or routine care as soon
as needed, and got answers the same day if
called during the day (n=255)
Number who answered they
called for appointments or
called for information (n=293)
87.1 (n=255) 85.00
87.7 (n=257) 92.5 (n=271)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020
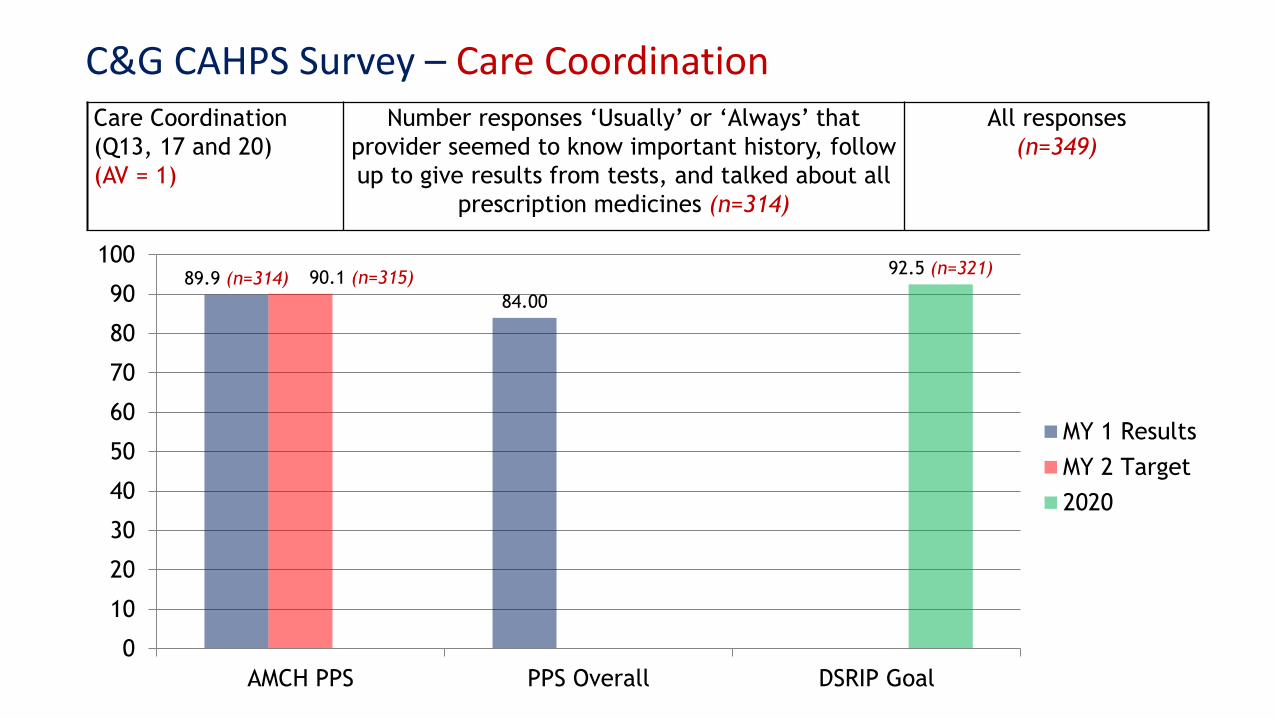
C&G CAHPS Survey – Care Coordination Care Coordination
(Q13, 17 and 20)
(AV = 1)
Number responses ‘Usually’ or ‘Always’ that
provider seemed to know important history, follow
up to give results from tests, and talked about all
prescription medicines (n=314)
All responses
(n=349)
89.9 (n=314)
84.00
90.1 (n=315) 92.5 (n=321)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020
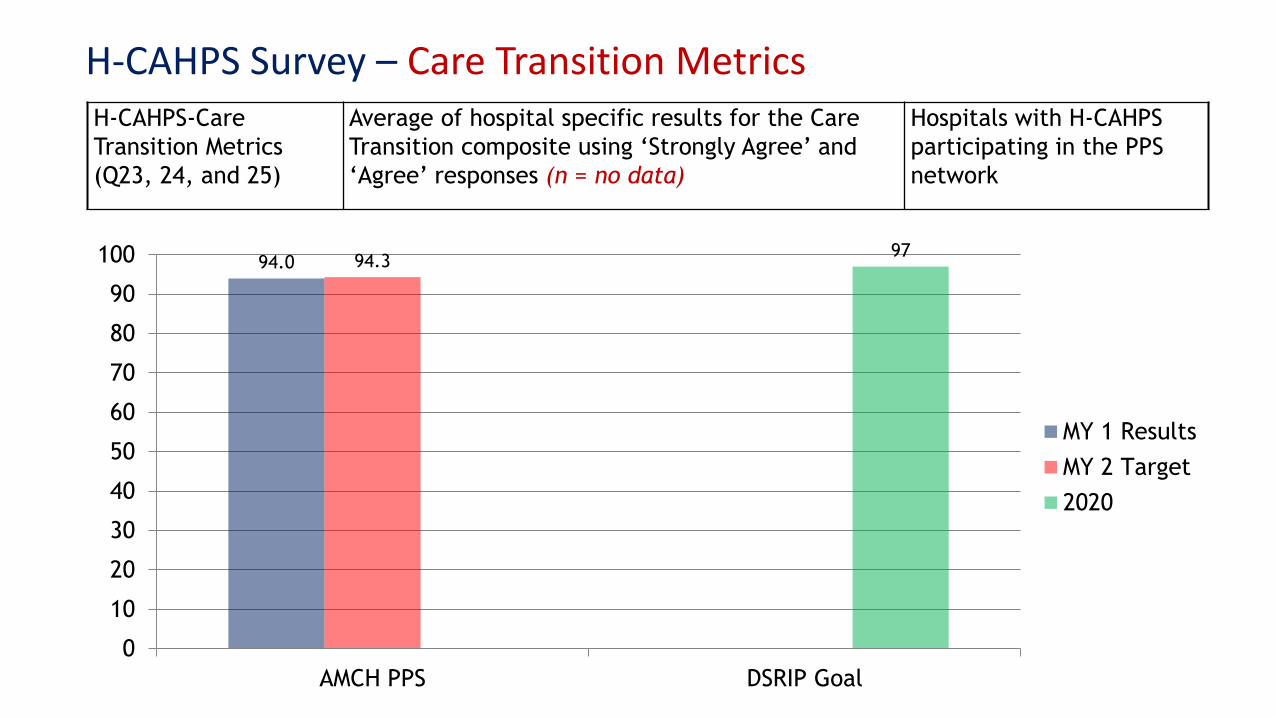
H-CAHPS Survey – Care Transition Metrics H-CAHPS-Care
Transition Metrics
(Q23, 24, and 25)
Average of hospital specific results for the Care
Transition composite using ‘Strongly Agree’ and
‘Agree’ responses (n = no data)
Hospitals with H-CAHPS
participating in the PPS
network
94.0 94.3 97
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS DSRIP Goal
MY 1 Results
MY 2 Target
2020
CVD Project – HEDIS CAHPS & C&G CAHPS Survey Measures
Four Measure Groups:
- Aspirin
- Flu shots
- Tobacco use cessation
- Health literacy

CVD Project – HEDIS CAHPS & C&G CAHPS Member Survey Measures
Measure Name Numerator Description
Aspirin Use (HEDIS CAHPS) % of respondents who are currently taking aspirin daily or
every other day
Discussion of Risks and Benefits of
Aspirin Use (HEDIS CAHPS)
% of respondents who discussed the risks and benefits of
using aspirin with a doctor or health provider
Medical Assistance with Smoking and
Tobacco Use Cessation – Advised to
Quit (HEDIS CAHPS)
% of respondents who were advised to quit
Medical Assistance with Smoking and
Tobacco Use Cessation – Discussed
Cessation Medication (HEDIS CAHPS)
% of respondents who discussed or were recommended
cessation medications
Medical Assistance with Smoking and
Tobacco Use Cessation – Provided
Cessation Methods or Strategies (HEDIS
CAHPS)
% of respondents who discussed or were provided cessation
methods or strategies

CVD Project – HEDIS CAHPS & C&G CAHPS Member Survey Measures
Measure Name Numerator Description
Flu Shots for Adults Ages 18 – 64
(HEDIS)
% of respondents who have had a flu shot
Health Literacy – Instructions Easy to
Understand (C&G CAHPS)
% of responses ‘Usually’ or ‘Always’ that instructions for
caring for condition were easy to understand,
Health Literacy – Describing How to
Follow Instructions (C&G CAHPS)
% of responses ‘Usually’ or ‘Always’ that provider asked
patient to describe how the instruction would be followed
Health Literacy – Explained What to
do if Illness Got Worse (C&G CAHPS)
% of responses ‘Usually’ or ‘Always’ that provider explained
what to do if illness/condition got worse or came back
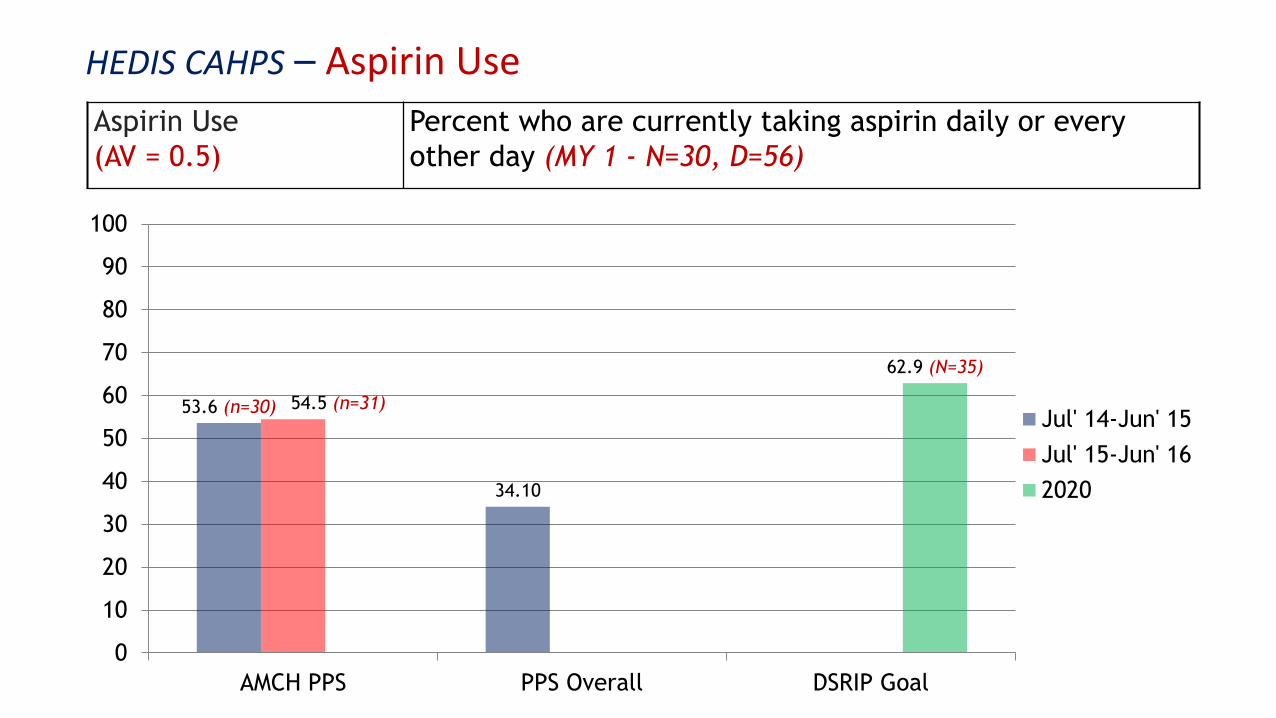
HEDIS CAHPS – Aspirin Use
Aspirin Use
(AV = 0.5)
Percent who are currently taking aspirin daily or every
other day (MY 1 - N=30, D=56)
53.6 (n=30)
34.10
54.5 (n=31)
62.9 (N=35)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
2020

HEDIS CAHPS – Discussion of Aspirin Use
Discussion of Aspirin
Use (AV = 0.5)
Percent who discussed the risks and benefits of using aspirin
with a doctor or health provider (MY 1 - N=62, D=106)
58.5 (n=62)
47.8
59.4 (n=63)
67.3 (n=71)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
2020

HEDIS CAHPS – Flu shots for adults 18-64
Flu shots (AV = 1.0) Percent who had flu shots since Jan 1, 2015 (MY 1 - N=114,
D=416)
27.4 (n=114) 31.2 31 (n=129)
63.4 (n=264)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
2020

HEDIS CAHPS Survey – Medical Assistance with Smoking and Tobacco Use Cessation – Advised to Quit
Tobacco Use Cessation
Advised to Quit (AV = 0.33)
Percent of respondents who were advised to quit
(MY 1 - N=132, D=146)
90.4 (n=132) 89.2 90.9 (n=133) 95.6 (n=140)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
2020

HEDIS CAHPS – Medical Assistance with Smoking and Tobacco Use Cessation – Discussed Cessation Medication
Tobacco Use Cessation
Discussed Cessation Medication
(AV = 0.33)
Percent of respondents who discussed or were
recommended cessation medications
(MY 1 - N=102, D=146)
69.9 (n=102) 70.9 71.3 (n=104)
83.9 (n=122)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
2020

HEDIS CAHPS – Medical Assistance with Smoking and Tobacco Use Cessation – Cessation Methods or Strategies
Tobacco Use Cessation
Methods or strategies
(AV = 0.33)
Percent of respondents who discussed or were provided
with cessation methods or strategies
(MY 1 - N=95, D=146)
65 (n=95) 62
66 (n=96) 67 (n=98)
75 (n=110)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
Jul' 14-Jun' 15
Jul' 15-Jun' 16
HP Goal
2020

C&G CAHPS – Health Literacy – Instructions Easy to Understand
Instructions Easy to
Understand(AV = 0.33)
Number responses ‘Usually’ or ‘Always’ that instructions for caring
for condition were easy to understand (MY 1 - N=231, D=238)
97.0 (n=231) 95.90 97.2 (n=231) 98.8 (n=235)
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020

C&G CAHPS – Health Literacy – Describing How to Follow Instructions
Describing How to Follow
Instructions (AV = 0.33)
Number responses ‘Usually’ or ‘Always’ that provider asked
patient to describe how the instruction would be followed (MY
1 - N=188, D=237)
79.3 (n=188) 79.40 80.4(n=191)
89.7
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020
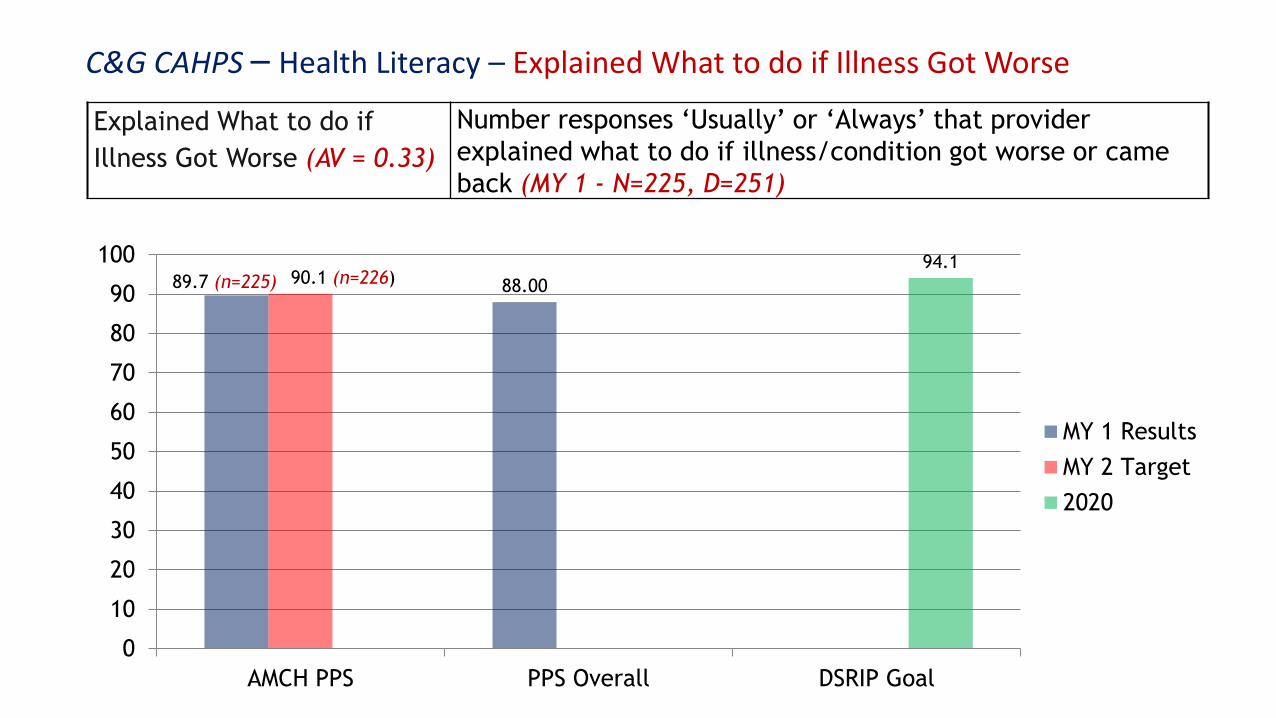
C&G CAHPS – Health Literacy – Explained What to do if Illness Got Worse
Explained What to do if
Illness Got Worse (AV = 0.33)
Number responses ‘Usually’ or ‘Always’ that provider
explained what to do if illness/condition got worse or came
back (MY 1 - N=225, D=251)
89.7 (n=225) 88.00 90.1 (n=226) 94.1
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS Overall DSRIP Goal
MY 1 Results
MY 2 Target
2020
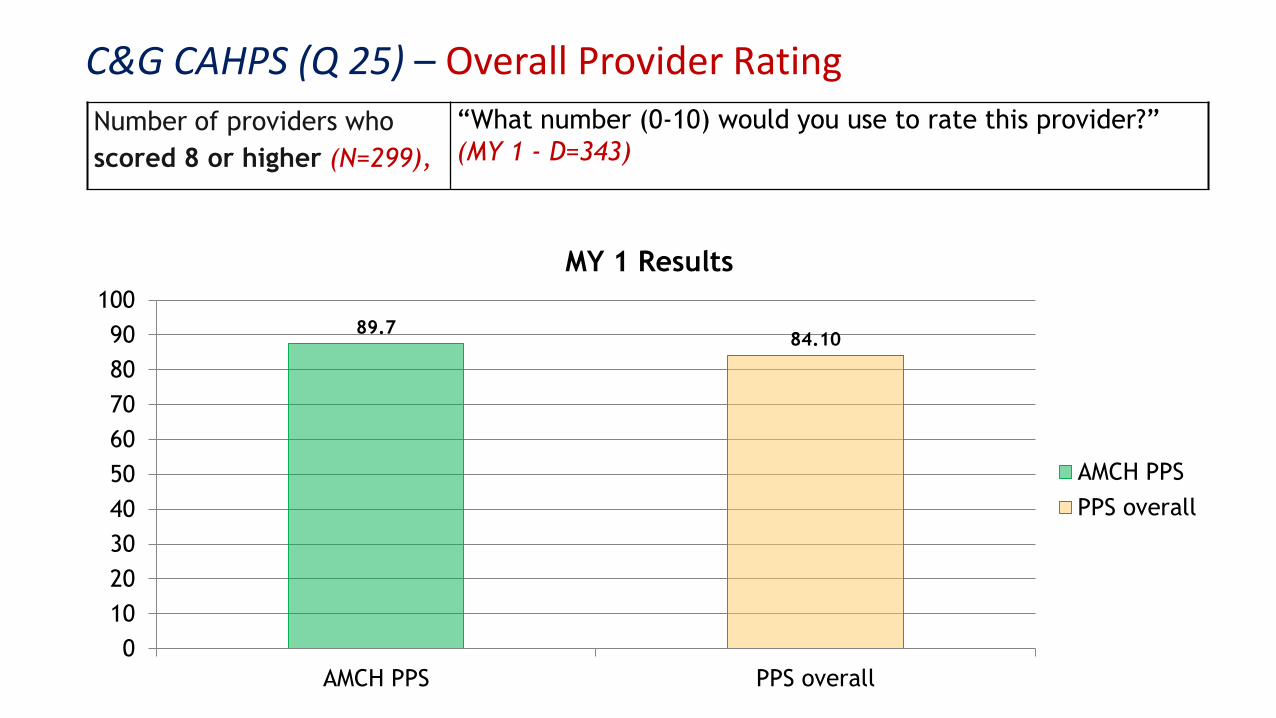
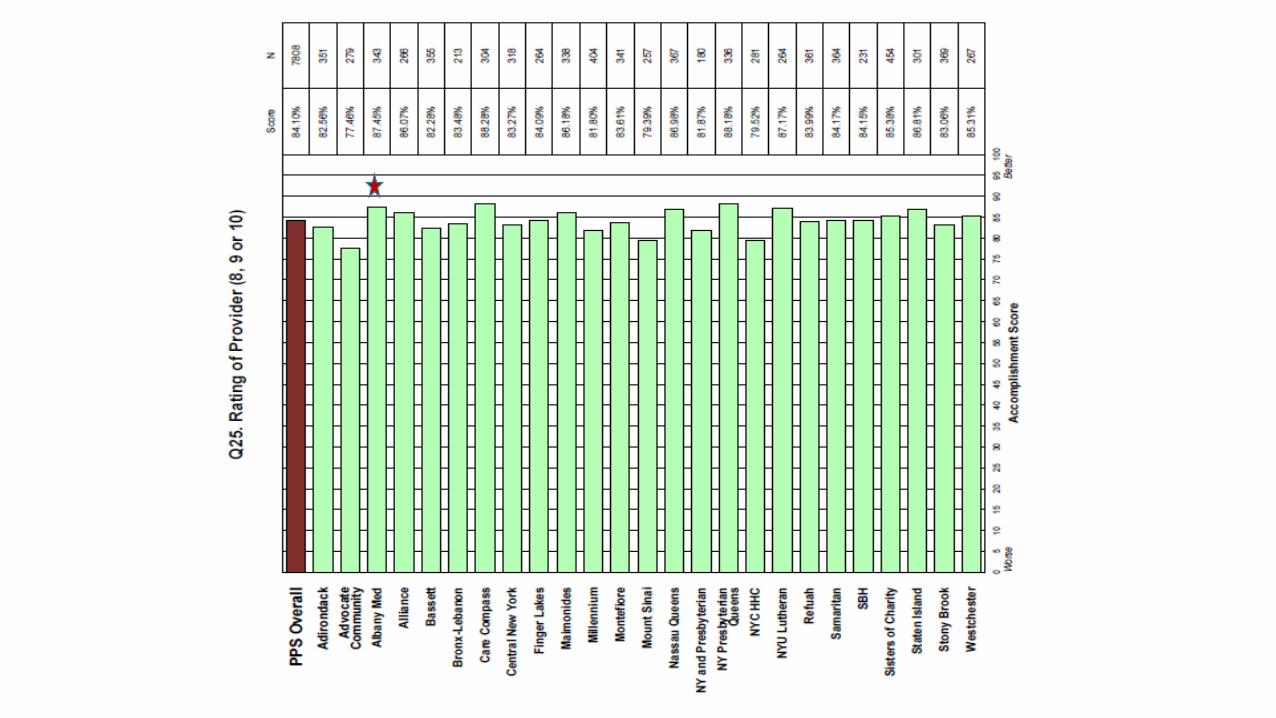
C&G CAHPS (Q 25) – Overall Provider Rating
Number of providers who
scored 8 or higher (N=299),
“What number (0-10) would you use to rate this provider?”
(MY 1 - D=343)
89.7 84.10
0
10
20
30
40
50
60
70
80
90
100
AMCH PPS PPS overall
MY 1 Results
AMCH PPS
PPS overall
Edit the text with your own short phrases.
The animation is already done for you; just copy and paste the slide into your existing presentation.

• To gain an understanding of uninsured individuals’ experiences during the
course of their care by PPS, the CG-CAHPS Survey will be a required tool for
all performing provider systems (PPSs) participating in Project 2.d.i.
• All PPSs are advised to use the entire 31-question CG-CAHPS Survey
(version 3.0) when completing this measure.
• Achievement values for this measure will be based on the ability to have
the required volume of completed surveys.
• Performance reports will contain the PPS results for four composite
measures, comprised of only ten individual questions taken from the CG-
CAHPS Survey 3.0.2
• First survey due by 12/15/2016
CG-CAHPS for The Uninsured (2.d.i) – DOH Guidelines

C&G CAHPS Survey – Improvement Strategies (AHRQ 2015)
http://www.ahrq.gov/cahps/quality-improvement/improvement-guide/improvement-guide.html

Questions?
Kallanna Manjunath, MD- Medical Director
Tara Foster, MS, RN- Nurse Manager
Simone Brooks, MBA