albert health 2013 kss
TRANSCRIPT

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 1/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
SENTINEL LYMPH NODE BIOPSY IN HIGH RISK
CUTANEOUS SQUAMOUS CELL CARCINOMA
Effective Date: February 2013

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 2/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
BACKGROUND
Squamous cell carcinoma (SCC) is the second most common type of skin cancer. In Alberta, there were2,400 new cases of SCC diagnosed in 2004, with a total (direct and indirect) cost of nearly $40 million. 1 However, by 2031 the projected cost of SCC will rise to over $103 million, using a low annual percentagechange for the estimation. 1 Although most SCC is capable of cure, some lesions carry a higher risk ofrecurrence and metastases; high risk SCC typically includes lesions that are more than 2 cm in greatest
diameter and more than 4 mm in depth, as well as other factors such as histologic subtype (i.e., adenoid,adenosquamous, desmoplastic), and differentiation (e.g., moderate or poor versus well). 2-4 Whether ornot the lesion is a recurrence or in a site of prior radiotherapy or chronic inflammation, and whether thepatient is immunosuppressed, also influences how aggressive an SCC tumour will behavior (Table 1). 2-7
Table 1. Factors associated wit h an i ncreased risk of recurrence or metastases in cutaneous squamous cell carcinoma.
Factor Reported risk values References
Size >2 cm Metastases: OR 2.76 (95% CI 1.2-6.5; p=.02) for <2 cm vs. 2.1-3 cm vs. >3 cmRecurrence: HR 3.79 (95% CI 1.47-9.78; p=.006)
6,8,9
Depth >4 mm Local recurrence: HR 4.8 (95% CI2.22-10.36; p<.0001) for increased thicknessMetastases: HR 6.03 (2.71-13.43; p<.0001) for increased thickness
6,9
Desmoplastic, adenoid, adeno-squamous, spindle histologies
Local recurrence: HR 16.11 (95% CI 6.57-39.49; p<.0001) for desmoplasia 6
Site of a scarSite of a burnSite of prior radiotherapy
Recurrence: HR 3.12 (95% CI 1.36-7.20; p=.008)Recurrence: HR 2.95 (95% CI 0.88-9.84; p=.08)Metastases: strongly associated (p=.01)
889
Recurrent disease Recurrence: HR 1.68 (95% CI 0.58-4.90; p=.34) 8,9
Differentiation: poor Recurrence: HR 2.92 (95% CI 1.22-6.94; p=.016) for poor vs. moderate/well 8,9
Perineural invasion Metastases: strongly associated (p=.001) 9
Immunosuppression Metastases: HR 4.32 (95% CI 1.62-11.52; p=.0035) for immunosuppression 6

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 3/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
TARGET POPULATION
The target population for this guideline is patients with high risk, squamous cell carcinoma of the skin orlip. High risk patients include those with the following factors: (1) tumour size greater than two centimetersin greatest dimension; (2) tumour depth greater than four millimeters; (3) tumour histology of the subtypesdesmoplastic, adenoid, adenosquamous, spindle, or acantholytic; (4) undifferentiated tumour; (5) tumourwith perineural invasion; (6) tumour at the site of a scar, burn, or prior radiotherapy; (7) tumour in a patient
with clinical inflammation; (8) recurrent tumour; and (9) tumour in a patient with immunosuppression.
GUIDELINE QUESTIONS
1. Is SLNB appropriate for patients with high risk cutaneous squamous cell carcinoma (SCC)?
2. How should lymph node pathology in cutaneous SCC be reported?
3. How should patients with cutaneous SCC with histologically or radiographically proven lymph nodemetastases be managed?
Guidance on the following topics related to SLNB has been published elsewhere and will not be coveredin this guideline: (a) benefits and risks of SLNB; (b) appropriate surgeon training, organizational criteria,and resources for performing SLNB; and (c) appropriate techniques for performing SLNB. Forrecommendations related to these topics, please see the CancerControl Alberta guidelines Sentinel lymphnode biopsy and axillary node dissection in early stage breast cancer
14 and Regional node dissection inprimary cutaneous melanoma. 15
DEVELOPMENT PANEL
This guideline was reviewed and endorsed by the Alberta Cutaneous Tumour Team. Members of the Alberta Cutaneous Tumour Team include general surgeons, medical oncologists, radiation oncologists,
8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 4/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
from the College of American Pathologists (CAP) 20 and the American Joint Committee on Cancer (AJCC)21 staging definitions for squamous cell carcinoma were also included as reference documents.
RECOMMENDATIONS
Tumour Node Metastasis (TNM) staging for squamous cell carcinoma, according to the AJCC, 21 isprovided in Appendix A (page 10).
1. Nodal staging. Sentinel lymph node biopsy (SLNB) accurately identifies lymph node metastasis inpatients with high risk cutaneous squamous cell carcinoma (SCC); however, there is insufficient evidenceto suggest that the use of SLNB translates into any benefit, in terms of survival. Therefore, the use ofSLNB in this setting, as standard of care, has not yet been established.
• SLNB can be considered for staging in carefully selected patients (i.e., patients with tumours >2cmwith risk factors) with clinically node negative high risk SCC.
• SLNB should not be performed in patients with clinically or radiographically positive nodes. Patients
with palpable nodes should undergo preoperative fine needle aspiration (FNA) or core biopsy toconfirm the presence of nodal metastasis.
• Due to disruption of the lymphatic system, caution should be used if SLNB is to be performed inpatients with prior wide excision of the primary tumour with rotation flap, prior extensive surgery(e.g., dissection of the neck), or previous radiation to the head and the neck.
• Older age and obesity should not preclude patients from undergoing SLNB, but may preventsuccessful SLN mapping.
2. Therapeutic node dissection. Completion lymph node dissection (CLND) should be performed inpatients with evidence of nodal metastasis (i.e., positive SLNB, positive FNA or core biopsy, palpablenodes, positive imaging).

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 5/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
DISCUSSION
On the basis of data from small (i.e., fewer than 25 patients) prospective and retrospective cohorts, SLNBhas been shown to be an accurate lymph node staging procedure in patients with high risk cutaneoussquamous cell carcinoma (SCC). A systematic review of data from 82 patients with nonanogenital highrisk SCC who underwent SLNB prior to 2006 found an overall SLN positivity rate of 21% (17 of 82patients); of the patients with negative SLN who were available for follow-up, the rate of nodal metastasis
was 2% (1 of 48 patients) and the rate of distant metastasis was 3% (1 of 36 patients).22
A subsequentsystematic review of data from an additional 47 patients (n=130 total) with high risk SCC revealed nodepositivity rates of 14.1% overall, 10.1% for head/neck, and 18.6% for trunk/extremities; the correspondingfalse negative rates were 15.4%, 0%, and 22.2%, respectively. The negative predictive value was 98%overall. 23
Controversy exists around the benefit of SLNB in patients with high risk SCC because no randomizedcontrolled trials, comparing SLNB with CLND or with no nodal treatment, have been published. Therefore,a survival benefit cannot be determined. The systematic review by Kwon, et al. (2011)
23 is the largest
study to date, but of the 130 patients included, only eleven had a positive SLN and were available forfollow-up. Among these eleven patients, who received adjuvant lymph node dissection or radiotherapy orboth, there were two local recurrences (18%) and three distant metastases (27%), but no nodalrecurrences. Two nodal recurrences occurred in 89 SLN negative patients that were available for follow-up, giving a SLN failure rate of 2.2%.
Overall, the rate of metastasis to the SLN is low in patients with high risk SCC; six observational studiespublished in 2006 or later, including 82 patients, have reported SLN positivity rates ranging from 0% to
5%.23-28
The criteria used to define high risk SCC were similar among studies and typically includedtumour size (>2 cm), tumour depth (>4 mm) or Clark IV-V, poorly defined borders, moderate or poordifferentiation, perineural involvement, rapidly growing or recurrent lesion, and immunosuppression. A2003 cost analysis using data from a prospective cohort of Japanese patients with SCC of the head and

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 6/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
the CancerControl Alberta guidelines: Sentinel lymph node biopsy and axillary node dissection in earlystage breast cancer
14 and Regional node dissection in primary cutaneous melanoma. 15 A summary ofthe evidence used to develop the recommendations in this guideline can be found in Appendix B (page11).
GLOSSARY OF ABBREVIATIONS
Acronym Descript ion
AJCC American Joint Committee on Cancer
CAP Canadian Association of Pathologists
CLND completion lymph node dissection
FNA fine needle aspiration
SCC squamous cell carcinoma
SLNB sentinel lymph node biopsy
DISSEMINATION
• Present the guideline at the local and provincial tumour team meetings and weekly rounds.• Post the guideline on the Alberta Health Services website.• Send an electronic notification of the new guideline to all members of CancerControl Alberta
MAINTENANCE
A formal review of the guideline will be conducted at the Alberta Cutaneous Tumour Team AnnualMeeting in 2015. If critical new evidence is brought forward before that time, however, the guideline

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 7/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
REFERENCES
1 Canadian Partnership Against Cancer. The Economic Burden of Skin Cancer in Canada: Current and Projected.
2010 Feb; URL: http://www.partnershipagainstcancer.ca/wp-content/uploads/Economic-Burden-of-Skin-Cancer-in-Canada-Report-Final1.pdf
2 National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Basal Cell and
Squamous Cell Skin Cancers. V2.2012. URL: www.nccn.org
3 Jennings L and Schmults CD. Management of High-Risk Cutaneous Squamous Cell Carcinoma. J Clin Aesthet
Dermatol. 2010 April; 3(4): 39–48.
4 Motley RJ, Preston PW, Lawrence CM. Multi-professional guidelines for the management of the patient with primary
cutaneous squamous cell carcinoma. London (UK): British Association of Dermatology (BAD); 2009 Dec 11. 34 p.
5 Australian Cancer Network. Clinical practice guide: basal cell carcinoma, squamous cell carcinoma (and related
lesions) - a guide to clinical management in Australia. 2008 Nov. URL:http://www.cancer.org.au/content/pdf/HealthProfessionals/ClinicalGuidelines/Basal_cell_carcinoma_Squamous_cell_
carcinoma_Guide_Nov_2008-Final_with_Corrigendums.pdf 6 Brantsch KD, Meisner C, Schönfisch B, Trilling B, Wehner-Caroli J, Röcken M, Breuninger H. Analysis of risk factors
determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008 Aug;9(8):713-20.
7 Demir H, Isken T, Kus E, Ziya Tan Y, Isgoren S, Daglioz Gorur G, Oc A, Sen C, Cek D, Ercin C, Berk F. Sentinel
lymph node biopsy with a gamma probe in patients with high-risk cutaneous squamous cell carcinoma: follow-upresults of sentinel lymph node-negative patients. Nucl Med Commun. 2011 Dec;32(12):1216-22
8
Mullen JT, Feng L, Xing Y, Mansfield PF, Gershenwald JE, Lee JE, Ross MI, Cormier JN: Invasive squamous cellcarcinoma of the skin: defining a high-risk group. Ann Surg Oncol 2006, 13:902-909.
9 Cherpelis BS, Marcusen C, Lang PG. Prognostic factors for metastasis in squamous cell carcinoma of the skin.
Dermatol Surg 2002; 28:268 73

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 8/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
16 Essner R, Conforti A, Kelley MC, et al. Efficacy of lymphatic mapping, sentinel lymphadenectomy, and selective
complete lymph node dissection as a therapeutic procedure for early-stage melanoma. Ann Surg Oncol. 1999 Jul- Aug;6(5):442-9.
17 Morton DL, Cochran AJ, Thompson JF, et al; Multicenter Selective Lymphadenectomy Trial Group. Sentinel node
biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial. Ann Surg. 2005Sep;242(3):302-11; discussion 311-3.
18 Seigler HF. Axillary lymph node dissection versus the sentinel lymph node technique in breast cancer. Ann Surg.
2004;240:7–8.
19 Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection
(SLND) plus axillary lymph node dissection compared with SLND alone in the American College of SurgeonsOncology Group Trial Z0011. J Clin Oncol 2007; 25: 3657-63.
20 College of American Pathologists. Protocol for the examination of specimens from patients with squamous cell
carcinoma of the skin. 2012 Jun; v.3.1.0.1. URL:http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/SkinSquamousCell_12protocol.pdf
21 Cutaneous squamous cell carcinoma and other cutaneous carcinomas. In: Edge SB, Byrd DR, Compton CC, et al.eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 301–14.
22 Ross AS, Schmults CD. Sentinel lymph node biopsy in cutaneous squamous cell carcinoma: a systematic review of
the English literature. Dermatol Surg. 2006 Nov;32(11):1309-21.
23 Kwon S, Dong ZM, Wu PC. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: clinical
experience and review of literature. World J Surg Oncol. 2011 Jul 19;9:80.
24 Demir H, Isken T, Kus E, Ziya Tan Y, Isgoren S, Daglioz Gorur G, Oc A, Sen C, Cek D, Ercin C, Berk F. Sentinel
lymph node biopsy with a gamma probe in patients with high-risk cutaneous squamous cell carcinoma: follow-upresults of sentinel lymph node-negative patients. Nucl Med Commun. 2011 Dec;32(12):1216-22
25 Rastrelli M, Soteldo J, Zonta M, Trifirò G, Mazzarol G, Vitali GC, Mosconi M, Testori A. Sentinel node biopsy for

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 9/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
32 Cecchi R, Buralli L, de Gaudio C. Lymphatic mapping and sentinel lymphonodectomy in recurrent cutaneous
squamous cell carcinomas. Eur J Dermatol. 2005 Nov-Dec;15(6):478-9.
33 Motomura H, Ishii M. Lymphatic mapping and sentinel lymph node biopsy for malignant melanoma in Japanese.
Osaka City Med J. 2004 Jun;50(1):29-37.
34 Nouri K, Rivas MP, Pedroso F, Bhatia R, Civantos F. Sentinel lymph node biopsy for high-risk cutaneous squamous
cell carcinoma of the head and neck. Arch Dermatol. 2004 Oct;140(10):1284.
35 Wagner JD, Evdokimow DZ, Weisberger E, Moore D, Chuang TY, Wenck S, Coleman JJ 3rd. Sentinel node biopsy
for high-risk nonmelanoma cutaneous malignancy. Arch Dermatol. 2004 Jan;140(1):75-9.
36 Michl C, Starz H, Bachter D, Balda BR. Sentinel lymphonodectomy in nonmelanoma skin malignancies. Br J
Dermatol. 2003 Oct;149(4):763-9.
37 Reschly MJ, Messina JL, Zaulyanov LL, Cruse W, Fenske NA. Utility of sentinel lymphadenectomy in the
management of patients with high-risk cutaneous squamous cell carcinoma. Dermatol Surg. 2003 Feb;29(2):135-40.
38 Stoeckli SJ, Steinert H, Pfaltz M, Schmid S. Sentinel lymph node evaluation in squamous cell carcinoma of thehead and neck. Otolaryngol Head Neck Surg. 2001 Sep;125(3):221-6.
39 Alex JC, Sasaki CT, Krag DN, Wenig B, Pyle PB. Sentinel lymph node radiolocalization in head and neck
squamous cell carcinoma. Laryngoscope. 2000 Feb;110(2 Pt 1):198-203.
40 Fujisawa Y, Nakamura Y, Kawachi Y, Otsuka F. Indocyanine green fluorescence-navigated sentinel node biopsy
showed higher sensitivity than the radioisotope or blue dye method, which may help to reduce false-negative cases inskin cancer. J Surg Oncol. 2012 Jul 1;106(1):41-5. Epub 2012 Jan 17.
41 Fujisawa Y, Nakamura Y, Kawachi Y, Otsuka F. A custom made low cost intraoperative fluorescence navigationsystem with indocyanine green for sentinel lymph node biopsy in skin cancer. Dermatology. 2011;222(3):261-8. Epub2011 Apr 19.
42Stoffels I Poeppel T Boy C Mueller S Wichmann F Dissemond J Schadendorf D Rosenbaum Krumme S Klode
8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 10/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
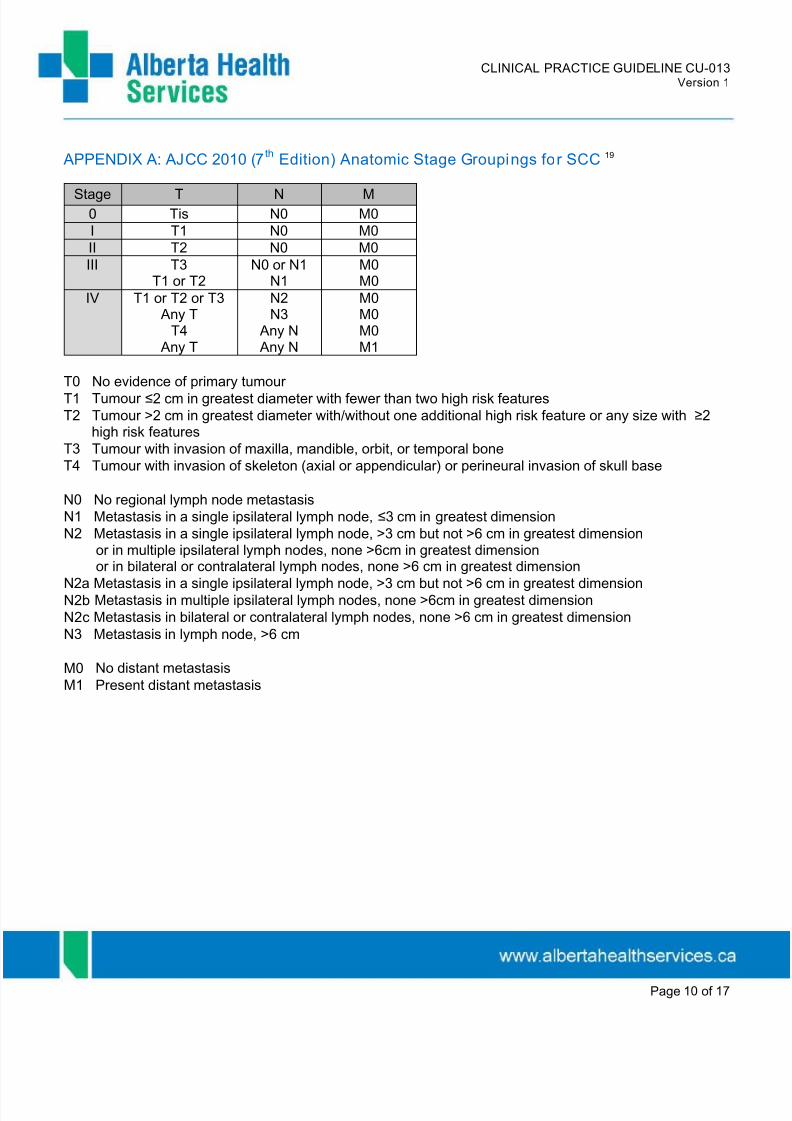
APPENDIX A: AJCC 2010 (7th
Edition) Anatomic Stage Groupings for SCC 19
Stage T N M
0 Tis N0 M0I T1 N0 M0II T2 N0 M0III T3
T1 or T2
N0 or N1
N1
M0
M0IV T1 or T2 or T3
Any TT4
Any T
N2N3
Any N Any N
M0M0M0M1
T0 No evidence of primary tumourT1 Tumour ≤2 cm in greatest diameter with fewer than two high risk features
T2 Tumour >2 cm in greatest diameter with/without one additional high risk feature or any size with ≥2 high risk features
T3 Tumour with invasion of maxilla, mandible, orbit, or temporal bone
T4 Tumour with invasion of skeleton (axial or appendicular) or perineural invasion of skull base
N0 No regional lymph node metastasisN1 Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension N2 Metastasis in a single ipsilateral lymph node, >3 cm but not >6 cm in greatest dimension
or in multiple ipsilateral lymph nodes, none >6cm in greatest dimensionor in bilateral or contralateral lymph nodes, none >6 cm in greatest dimensionN2a Metastasis in a single ipsilateral lymph node, >3 cm but not >6 cm in greatest dimensionN2b Metastasis in multiple ipsilateral lymph nodes, none >6cm in greatest dimension

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 11/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
APPENDIX B: EVIDENCE TABLES
Table 2: Recommendations from existing guidelines on the use of SLNB in SCCOrganization Definition of High Risk SCC Recommendation for Use of SLNB in High Risk SCC
NCCN, 2012 2 Location: head and neck, genitalia, mucosal surfaces, earsSize: >2cm
Poorly defined bordersRecurrent disease
Immunosuppression Site of prior RT or chronic inflammationPerineural involvementModerately, poorly, or undifferentiated
Rapidly growing tumourNeurologic symptoms
Adenoid, adenosquamous, desmoplastic SCC
For certain high-risk squamous cell lesions, sentinel lymph node mapping may be considered,although the benefit of this technique is yet to be proven.
Harvard UniversityDepartment ofDermatology2010 3
Location: ear, lip, anogenital, scars
Diameter: >2cm and depth: >4mm or beyond subcutaneous fat Perineural invasionPoorly differentiated tumorInfiltrative/desmoplastic growth pattern
History of local recurrenceImmunosuppressionOther: arsenic, psoralen UV-A, radiation exposure
SLN biopsy is a minimally invasive staging procedure that may be useful in identifying occult regionalLN disease in selected high-risk patients with CSCC.
Sensitivity can be increased with lymphoscintigraphy (plus blue dye) and step-sectioning techniques.
It is unknown whether early detection of LN metastasis will improve outcomes for patients with CSCC.
This awaits further study. Fortuitously, unlike melanoma, CSCC with nodal metastasis i s often curableso early detection of nodal spread has the potential to prevent distant metastasis and death.Prospective controlled trials are required to assess the utility of SLN biopsy in high-risk CSCC.
British Assoc.Dermatology,2008 4
Location: lip, ear, perineum, sacrum, sole of footSite of radiation, thermal scar, chornic ulcers, inflammationRecurrent SCC
Size: >2cm and invasion: >4cm (beyond dermis)Moderately or poorly differentiatedPerineural invasion
Acantholytic, spindle, or desmoplasticImmunosuppression
Elective prophylactic lymph node dissection has been proposed for SCC on the lip greater than 6 mmin depth and cutaneous SCC greater than 8 mm in depth, but evidence for this is weak. Elective lymphnode dissection is not routinely practised and there is no compelling evidence of benefit over morbidity.
There has been recent interest in the application of sentinel lymph node biopsy in the managementof high risk SCC. The procedure is technically feasible and may help avoid unnecessary lymph nodedissection. However, the overall benefit of the technique in patients with SCC has yet to be determined.
Australian CancerNetwork, 2008 5
Location: scalp, peri-ocular region, ears, lips, nose, genitaliaRecurrenceSite of previous treatmentRapidly growing
High grade, moderately or poorly differentiatedInvasion >4cm (beyond subcutaneous tissues)Immunosuppression
Clinically suspected lymph node metastases should be confirmed by fine needle aspiration cytology(under radiological or ultrasound guidance if required) if possible.
Open surgical biopsy should be avoided.
The treatment of metastatic disease to lymph nodes is primarily surgical.
Brantsch KD.2008 6
Prospective cohort (n=615) cutaneous SCC (med f/u: 43 months):Local recurrence (%): 20 pts (3%) and metastases (%): 26 pts (4%)
Mets - increased tumour thickness (HR 4.8 [2.22-10.36]; p<.0001)Multivariate analysis of key prognostic factors:
Mets - immunosuppression (HR 4.32 [1.62-11.52]; p=.0035)Mets - localisation at the ear (HR 3.61 [1.51-8.67]; p=.0040)Mets - increased horizontal size (HR 2.22 [1.18-4.15]; p=.0128)
Local Recur - increased thickness (HR 6.03 [2.71-13.43]; p<.0001)Local Recur - desmoplasia (HR 16.11 [6.57-39.49]; p<.0001)
n/a

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 12/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 12 of 17
Table 3: Clinical studies on the accuracy of SLNB in SCC
Author, year Methodolog y Patien ts Resul ts
ACCURACY of SLNB in SCC Node Pos iti vit y Recur renc e in SLNB- Other Inform atio n
Demir H. 20117 Prospective cohort:
SLNB with Tc-99m
nanocolloid
n=19high risk SCC clinical N0
high risk:
locations: ear, scalp, nose, temple, dorsum of hands, lipssize > 2cm and invasion > 4mm
poor differentiation, grade 2+perineural invasionrecurrent tumours
0% of LNs werepositive for mets
Local: 1/19 (5%)
Regional: 0/19 (0%)
Distant: 0/19 (0%)
Deaths(mean 41.1 mos f/u):
5 due to trauma or cardiac
Kwon S. 2011 23 Prospective cohort
SLNB
Literature review
SLNB
n=6high risk SCC clinical N0
high risk:
size ≥20 mm (trunk/extremeties) size ≥10 mm (head)
size ≥6 mm (face, genitalia, hand/feet) poorly defined borders
recurrent lesionimmunosuppression
moderate or poorly differentiated
rapidly growingperineural involvement
n=130high risk SCC
0% of SLNs werepositive for mets
14.1% all sites10.1% head/neck
18.6% trunk/extremities
Local: 1/6 (17%)
Distant: 1/6 (17%)
Nodal: 2/89 (2%)
Distant : 2/89 (2%)
-
False negative (%):15.4% all sites,0% head/neck,
22.2% trunk/extremeties
Neg. predict. value (%):
97.8% all sites100% head/neck
95.2% trunk/extremities
Rastrelli M. 2010 25 Retrospective cohort:
SNB followinglymphoscintigraphy andblue dye injection
n=20high risk SCC, N0 nonanogenital
high risk:
location: ear, scalp, nose, temple, dorsum hands, lipssize > 2 cm and depth of invasion > 4 mm
grade 2 differentiation or greater
perineural invasionrecurrent tumors
5% (1/20) of SLNs werepositive for mets
Regional: 2/20 (10%) Med f/u: 24 mosLocation: head/neck
(n=11), extremities (n=9)and trunk (n=1)
Deaths: 2 patients dieddue to SCC progressivedisease (1) or another
malignancy (1)
Cuccia G. 2008 26 Retrospective cohort: n=6 0% of SLNs were Local: none (0%) Med f/u: 10 mos

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 13/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 13 of 17
Author, year Methodolog y Patien ts Resul ts
ACCURACY of SLNB in SCC Node Pos iti vit y Recur renc e in SLNB- Other Inform atio nSLNB followinglymphoscintigraphy &vital dye injections
high risk SCC
high risk (Rowe’s criteria):
size >2 cm and clinical N0anatomic location
recurrent SCCClark and Breslow
histologic differentiation, stromal dysplasiaperineural or lymphatic invasion
positive for mets Regional: none (0%) False negative (%): 0%
Sanh RE. 2007 27 Retrospective cohort:
SLNB n=9
high risk SCC
high risk (physician assessment):
sites included: head/neck, thumb, trunk, leg
size included: >2 cmdepth included: all Clark V
differentiation included: anyrecurrence included: any (yes or no)
0% of SLNs werepositive for mets
none (0%) False-negative (%):possibly 1/9 (11%)
Deaths (med 9 mos f/u):4 patients (44%)
due to chronic kidney (1),distant SCC mets (2),unrelated cancer mets (1)
Renzi C. 2006 28 Retrospective cohort
SLNB
Retrospective cohort +
patients from previousstudies (lit review)
SLNB
n=22high risk SCC, N0
high risk:
size > 2 cm (14/22)infiltration to subcutis, bone or muscles (12/22)
depth >4 mm (10/22)sites: lip, ear (15/22)
poorly or moderately differentiaion (10/22)
perineural invasion (2/22)recurrent tumors (3/22)
immunosuppression (0/22)
n=83high risk SCC
4.5% (1/22) of SLNspositive for mets
12.5% to 44% of SLNspositive for mets
none (0%)
n/a
Med f/u: 17 mos
Recurrence after SLNB+:100% (1/1)
Odds of positive SLNB ifsize <2 cm vs. 2.1 to 3 cmvs. >3 cm: OR 2.76 (95%CI 1.2-6.5; p=.02)
Cecchi R. 200630
Retrospective cohort
SLNB
n=6high risk SCC
recurrent tumourssize >2 cm
deep invasion
17% (1/6) SLNspositive for mets
none 0% False-negative rate (%):0%
Ross AS. 2006 22 Systematic review:
SLNB
n=85high risk SCC
21% (17/82) of SLNspositive for mets
Local: 3/35 (9%) Nodal mets after SLNB-:2% (1/48)

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 14/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 14 of 17
Author, year Methodolog y Patien ts Resul ts
ACCURACY of SLNB in SCC Node Pos iti vit y Recur renc e in SLNB- Other Inform atio nnonanogenital
size > 2 cm (or 1cm lip, 1.5 cm hand)recurrent tumours
high risk histologies
False-neg. rate (%):5% (1/20), mostly prior to
radioisotope and dye
Distant mets: 3% (1/36)
Deaths from disease:3% (1/36)
Events: seroma,lymphatic fistula,
hematoma, infection,dehiscence
Civantos FJ. 2006 31 Prospective cohort:
SLNB with lymphatic
mapping and gammaprobe
n=11high risk cutaneous SCC T1-3
high risk:size >2 cm
deep invasion (estimated >8 mm) or Clark IVimmunosuppression
location: auricular, lip, nasal vestibular, cheek, neckhigh-grade pathologic features
vascular or lymphatic invasion, perineural invasion
single cell invasion pattern at the tumor–host interfacepoorly differentiated
rapid growth pattern documented
9% (1/11) SLNspositive for mets
(final pathology positive)
none 0% Mean f/u: 19 mos (12-30)
Events: rare; no
temporary or permanentdysfunction of facial or
spinal nerves
Cecchi R. 200532
Prospective cohort: SLNB
n=5high-risk cutaneous SCCs, N0
high risk:
recurrent tumours (all patients)Clark: IV to V
Breslow: 4 to 8.5 mm
20% (1/5) SLNspositive for mets
n/a False negative rate (%):0%
Motomura H. 200433
Prospective cohort: SLNB
n=4SCC
high risk:
T4
location: face, hand, leg
0% (0/4) SLNspositive for mets
none: 0% Med f/u: 22.5 mos (4-41)
Mets in SLNB-: none
Nouri K. 2004 34 Prospective cohort: SLNB, gamma probe–
guided
n=8highrisk SCC of head and neck
high risk:
12% (1/8) SLNspositive for mets
n/a False negative rate (%):0%

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 15/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 15 of 17
Author, year Methodolog y Patien ts Resul ts
ACCURACY of SLNB in SCC Node Pos iti vit y Recur renc e in SLNB- Other Inform atio nsize >2 cm, depth >8 mm or Clark IV
poorly differentiated, aggressive growth patternperineural, vascular, or lymphatic invasion
location: lower lip, ear, or over burn scarsrecurrent tumors
immunosuppression
Wagner JD. 2004 35 Prospective cohort: SLNB
using preop.
lymphoscintigraphy,
blue dye, intraop.
radiolocalization
n=17high risk SCC, anogenital or cutaneous
high risk:
size >4 cm or >2 cm in immunosuppressedinvation to deep connective, skeletal, or muscular
locally recurrent SCC
29% (5/17) SLNspositive for mets
none: (0%) Med f/u: 10 mos
False positive rate (%):17% (1/6), in a patient w/recurrent SCC of scalp
Sensitivity: 88%
Neg. predict value: 0.94
Michl C. 200336
Prospective cohort: lymphoscintigraphy
n=11high risk SCC, clinical N0
high risk features:
dedifferentiatedat least deep dermis invasion
size >8 mm
18% (2/11 SCC) SLNspositive for mets
Tumour disseminationafter SLNB-: none
Med f/u: 2.4 yrs
Deaths: none(1 SLNB+ patient alive
and disease free;1 SLNB+ patient alive
with mets)
Reschly MJ. 2003H. Lee Moffitt CancerCenter 37
Prospective cohort: sentinel
lymphadenectomy
n=9high risk cutaneous SCC, N0
44% (4/9) SLNspositive for mets
n/a Med f/u: 8 mos
Disease-related deaths:2/4 SLNB+ patients died
of metastatic diseasewithin 2 years; none of the
SLNB- patients died orexperienced recurrence
Kosuda S. 200329
Prospective cohort:
lymphoscintigraphy
using technetium Tc
99m tin colloid or
phytate
n=11SCC (N0) of head & neck
36% (4/11) SLNspositive for mets
n/a Cost savings(neck dissection vs SLNB,
billed costs, Japan):$1218 (US) per stage N0patient (41 pts needed)
Avoided surgical deathsper 1000 patients: 7
Sensitivity: 100% (11/11)
Stoeckli SJ. 2001 38 Prospective cohort:
lymphoscintigraphy
using technetium Tc
99m tin colloid
n=19SCC (N0) of head & neck
32% (6/19) SLNspositive for mets
n/a No mets were found in the13 SLN- pts

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 16/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 16 of 17
Author, year Methodolog y Patien ts Resul ts
ACCURACY of SLNB in SCC Node Pos iti vit y Recur renc e in SLNB- Other Inform atio n Alex JC. 2000
39 Prospective cohort:
lymphoscintigraphy
using technetium Tc
99m tin colloid
n=8SCC (N0) of head & neck
SLNB identification:100% (8/8 patients)
There was no instance inwhich sentinel node was
negative for micro-metastatic disease while
being positive in anonsentinel lymph node.
Table 4: Clinical studies on SLNB technique in SCC
Author, year Methodolog y Patien ts Resul ts
SLNB TECHNIQUE
Fujisawa Y. 201240
Fujisawa Y. 2011 41
Prospective study:
1. SLNB with RI
(99Tc-tin collo id)
2. SLNB with BD
(2% patent blue)
3. SLNB with ICG
(0.5% indocyanine)
charge-coupled devicecamera and light-emit-ting diodes
n=34SLNs in groin, axilla, neck
SLN detection (mean):ICG-Fi green: 2.18 SLNsRI detection: 1.76 SLNsBD detection: 1.73 SLNs
Per-basin detection (mean):ICG-FI: 1.64 SLNsRI: 1.50 SLNsBD: 1.51 SLNs
Detection in other basins (mean):ICG-FI: 1.32 SLNsRI: 1.18 SLNsBD: 1.15 SLNs
Stoffels I. 201242
Prospective study:
1. SLNB with preop.
lymphoscintigraphy +
preop . SPECT/CT
2. SLNB with i ntraop.
real time imaging
with γ-camera
n=60(19 high risk cutaneous SCC)
Visualization of preoperatively identified SLNs:γ-camera: 100% (126/126)lymphoscintigraphy: 91% (115/126)
Visualization of additional SLNs:γ-camera: 23 (15.4%) in 15 pts (2/23 were positive for mets)lymphoscintigraphy: none
Neves RI. 201143
Retrospective review:
SLNB with
1. lymphazurin (LZ)
2. methylene blue (MM)
n=93skin cancer patients
Amount of dye used (mean): 0.93 ml LZ vs. 1.24 ml MBComplication rate: 8.7% LZ va. 25.5% MB (p=.05)
skin graft complications: 6/12 MB vs. 0/15 LS (p<.003)
Fujiwara M. 2009 44 Prospective cohort: n=10 SLN and subcutaneous lymphatic detection: 100% of patients

8/10/2019 Albert Health 2013 KSS
http://slidepdf.com/reader/full/albert-health-2013-kss 17/17
CLINICAL PRACTICE GUIDELINE CU-013Version 1
Page 17 of 17
Author, year Methodolog y Patien ts Resul ts
SLNB TECHNIQUESLNB with indocyanine
green (ICG)
skin cancer(3 SCC)
Fluorescence from SLNs was detected for at least 3 hours after ICG injection.
Table 5: Clinical studies on the use of imaging for SLNB in SCC
Author, year Methodolog y Patien ts Resul ts
IMAGING for SLNB in SCC
Klode J. 2011 45 Retrospective cohort:
1. Preop. SPECT/CT
+ SLNB
2. No preop.SPECT/CT
+ SLNB
n=48cutaneous head & neck
(19 high risk SCC)
Postoperative aesthetic results (SPECT/CT vs. standard:submandibular vs. cheek standard (2 pts)dorsal site of sternocleidomastoid vs. fronto-cervical (3 pts)
superficial from parotid vs. in the gland (1 pt)superficial vs. deeo cervical (3 pts)Operating time: mean 44.2 min for SPECT/CT vs. 106 min for standard (p<.0001)Feasibility using local anaesthesia: good with SPECT/CT
Cost: €32.65/SLNE with local vs. €334.57/SLNE with general anaesthesia (p<.0001)
Cho SB. 2005 46 Prospective cohort:
Whole-body FDG PET
staging
n=12cutaneous SCC
(9 high risk)
Primary lesion detection: 83.3% (9 cases)all patients with high risk SCC (100%)
Involved lymph node detection: 25.0% (3 cases)all were high risk SCC
Involved distant. organ (lung) detection: 8.3% (1 case)all were high risk SCC