alcohol and substance abuse medical & psychosocial aspects of disability 11/18/06
TRANSCRIPT

Alcohol and Substance Abuse
Medical & Psychosocial Aspects of Disability11/18/06

Substance Use StatisticsAccording to the 2005 National Household Survey on Drug Abuse, an estimated 19.7 million Americans aged 12 or older were current (past month) illicit drug users, meaning they had used an illicit drug during the month prior to the survey interview. This estimate represents 8.1 percent of the population aged 12 years old or older.
The overall rate of current illicit drug use among persons aged 12 or older in 2005 (8.1 percent) was similar to the rate in 2004 (7.9 percent), 2003 (8.2 percent), and 2002 (8.3 percent).
Marijuana was the most commonly used illicit drug (14.6 million past month users). In 2005, it was used by 74.2 percent of current illicit drug users. Among current illicit drug users, 54.5 percent used only marijuana, 19.6 percent used marijuana and another illicit drug, and the remaining 25.8 percent used only an illicit drug other than marijuana in the past month
Changes in use in past month ratio of persons 12 and over were noted for:
2002 2005Marijuana 6.2% to 6.0%Cocaine 0.9% to 1.0%Pain Relievers 2.6% to 2.6%Tranquilizers 0.8% to 0.7%

More Substance Use Stats
In 2005 an estimated 2.4 million (1%) Americans age 12 or older were current cocaine users and 682,000 (0.3%) were current (used at least once in past month) crack users1.1 million (0.4%) currently used hallucinogens 502,000 used Ecstasy 334,000 used
Oxycontin non-medically Current Heroin use was reported to be 136,000 (0.1%)

Demographics
Men are more likely to report drug use than women (10.3 vs. 5.7%)Rates and patterns of drug use vary by age, peaking among 18-20year oldsDrug use is correlated with education. Rate for H.S graduates is 8.6% vs. 5.0 percent for four year college graduates, even though college graduates were more likely to have tried drugs.

Substance use & race/ethnicity
In 2005, current substance use: White – 7.9% Black/African American – 9.5% Native American – 11.9% Native Hawaiian/Pacific Islander –
8.0% Asian – 3.1% Multi-racial – 12.6% Hispanic or Latino – 7.3%

Alcohol
In 2005, 51.8% of Americans age 12 or older report being current drinkers Over one fifth (22.7%) reported bingeing at least once in last 30 days6.6% reported heavy drinking

Alcohol
Age: highest prevalence of alcohol use is between 21 (69.4%) and 25 (67%). Rate gradually drops between 25 (63.7%) and 60 (50.8%).Men are slightly more likely to drink than women.likelihood of drinking alcohol increases with education, however, binge drinking and heavy drinking were least prevalent among college graduates

Employment
Unemployment is highly correlated with drug and alcohol use however,
8.2% of illicit drug users are full-time employed10.4% of drug users are part-time employedMost binge and heavy drinkers were employed in 2005. Among the 52.6 million adult binge drinkers, 42.1 million (80%) are full-time or part-time employees.12.5 million (80.8%) of the heavy drinkers are also employed.8.4% of full-time employed adults (18+) reported heavy use of alcohol versus 10.4% of unemployed adults (SAMHSA, 2005)

Substance abuse & work
Drug abuse problems in the workplace are estimated to cost employers $60 billion annually in violent crimes, fire accidents, health care costs, lost productivity, and accidents on the job (Backer, 1988; Stude, 1990). Substance abuse also is known to significantly compromise work performance resulting in high rates of absenteeism, accidents, time off for illness, and Workers’ Compensation claims (Cardoso et al., 1999).

Substance Abuse as a Disability
1990 Americans with Disabilities Act ADA statues and guidelines recognize
substance abuse as a disability People with a substance abuse problem are
protected at work, unless they are currently engaging in the illegal use of drugs.
A person with a coexisting disability can be legally discharged from a job if illegally abusing substances.

Substance Abuse as a Disability
Diagnostic and Statistical Manual of Mental Disorders, 4th Ed. Substance USE Disorders
Abuse: Maladaptive pattern of substance use leading to a clinically significant impairment or distress as manifested by one or more of the following in a 12 month period:
Recurrent substance use resulting in a failure to fulfill a major role obligation at work, school or home
Recurrent substance use in situations in which it is physically hazardous
Recurrent substance-related legal problems Continued substance use despite having persistent or
recurrent social or interpersonal problems caused or exacerbated by the effects of the substance

DSM-IV – Substance Use Disorders
Dependence is defined by the occurrence of withdrawal following the abrupt reduction of dosage of the drug or the administration of a drug antagoist. 3 or more of the following must occur within a 12 moth period:
Need for increased amounts of substance to achieve a desired effect (or markedly diminished effect with continued use of same amount)
Characteristic withdrawal syndrome for that substance or the same substance is taken to relieve or avoid withdrawal.
A substance is often taken in larger amounts for longer periods of time than was intended.
Persistent desire for a drug or unsuccessful efforts to cut down or control substance use.
A great deal of time is spent in activities to obtain a substance, use a substance or recover from its effects
Important social, occupational, or recreational activities are given up or reduced because of substance use
Substance use is continued despite knowledge of having a persistent or recurrent physical or psychological problem.


Addiction is a brain disorder
Addiction is an independent disorder distinguished from drinking that is merely heavy, problematic, ill advised or socially unacceptable
Abuse - intentional overuse in cases of Abuse - intentional overuse in cases of celebration, anxiety, despair, self-celebration, anxiety, despair, self-medication, other mental health disorders medication, other mental health disorders or ignorance. Tends to decline with or ignorance. Tends to decline with consequences or adequate treatment of consequences or adequate treatment of other mental health disorder.other mental health disorder.

Functional Imaging
SPECT – single photon emission computed tomography
PET – positron emission tomography
fMRI – functional magnetic resonance imaging



Dopamine Pathways – Pleasure pathways
nucleusaccumbens
hippocampus
striatum
frontalcortex
substantianigra/VTA
cocaineheroinnicotineamphetaminesopiatesTHCPCPketamine
heroinalcoholbenzodiazepinsbarbiturates
alcohol

enzymesreceptorsresponses
malfunction MFB
Inherited genes oraltered expression
The explanation for why people respond differently!
Early exposure to drugs
abnormal proteins

Brain of the addicted is fundamentally different:
Gene expression (Liu, Nickolendko 1994; Daunais & McGinty 1995)
Glucose metabolism (Volkow, Gillespie, 1996)
Responsiveness to environmental cues (O’Brien, Childress, 1993; Kilgus & Pumariega, 1994)

What’s inherited???
TemperamentInitial sensitivity to rewarding or aversive qualities (like or dislike of the drug)ToleranceRates and routes of metabolismTaste preferencesResponse to memories related to use
Developing brain
Individuals who begin drinking before age 15 are 4 times more likely to develop alcohol dependence during their lifetimes than those who begin drinking at age 21. (Grant & Dawson 1997; Journal of Substance Abuse 9:103-110)
Earlier drinking more likely to result in alcohol dependence independent of family history (Grant, 1998)
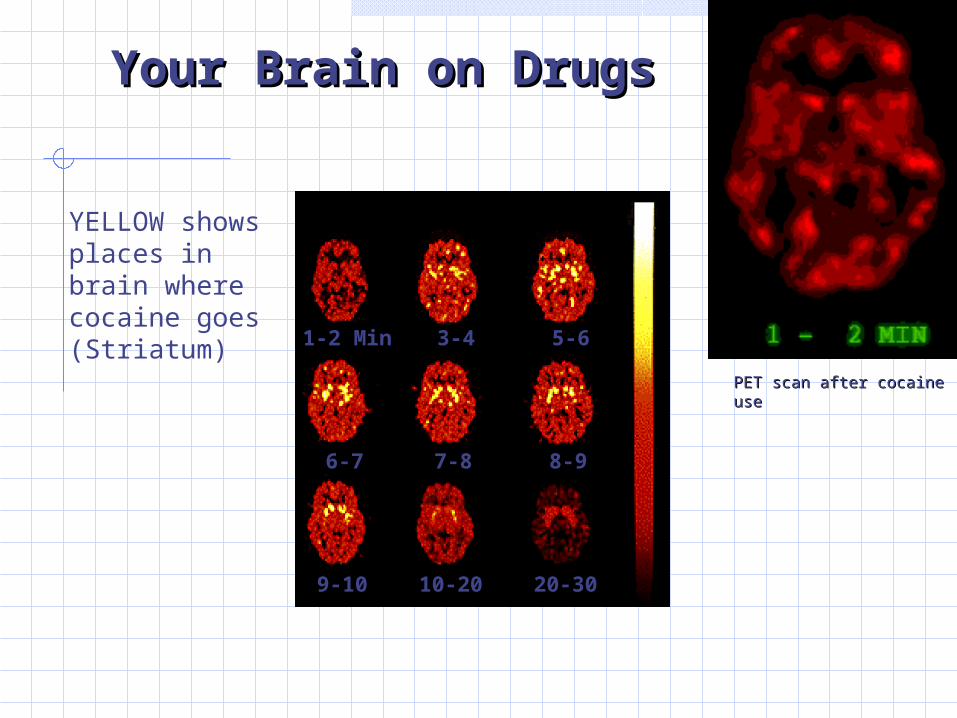
Your Brain on DrugsYour Brain on Drugs
1-2 Min 3-4 5-6
6-7 7-8 8-9
9-10 10-20 20-30
YELLOW shows places in brain where cocaine goes (Striatum)
PET scan after cocaine PET scan after cocaine useuse

Alcohol 25 yrsAlcohol 25 yrs Cocaine 2 yrsCocaine 2 yrs Marijuana 12 Marijuana 12 yrsyrs
NormalNormal
SPECT
(blood flow)

Assessment and Diagnosis
Bio-psycho-social-spiritual Assessment DSM-IVR:Seven Criteria
Two dimensions- Obsession and Compulsion.

Job is last to go!Job is last to go!

AbuseAddiction
Usually self-limitedProgressive course
Likely to stop as consequences progress
Unable to stop because of consequences – loss of control
May have significant consequences
Significant consequences
Frequent character or personality pathology
No specific personality
Normal brain chemistryAbnormal brain chemistry
Bad judgment, poor morals, self will
Cravings, preoccupation

Key Concepts
Motivation: the probability that a person will enter into, continue and adhere to a specific change strategy.Resistance: the result of interacting with one’s environment- not a characteristic.Ambivalence: the heart of the problem, not pathological.

Other Substance Abuse Disorders
Substance Induced Disorders E.g.: Intoxication, delirium, dementia, mood
disorders, sleep disorders – all with the precondition that the disorder is a result of substance use
Polysubstance Related Disorders Refers to disorders resulting from the use of
at least 3 groups of substances over a 12 month period with no single substance as predominating.

Impact of Substance Abuse and Disability
Basic living skills homelessness, lack of income, repeated legal problems
Health Poor or deteriorating health often results from years of abuse &
neglect of health
Education Substance abuse can lead to significant deficits in academic
development and basic learning skills
Employment Early onset and lengthy periods of substance abuse often result in
difficulty in obtaining & retaining meaningful employment
Relationships Interpersonal & socialization skills may be poor because
relationships were often based on the acquisition and use of drugs. The ability to communicate outside of the drug community is frequently impaired.

Continuum of Use, Abuse & Dependency
ExperimentationRecreational/social useUseDependenceAddiction

Commonly Abused Substances
Drugs are psychoactive chemicals that bring about changes in biological, psychological, social and/or spiritual functioning. This includes legal drugs (e.g., alcohol, over the counter meds, tobacco, caffeine) and illegal drugs such as marijuana, heroin and cocaine. Stimulants: produce increased awareness, attention
or excitement levels followed by depressed levels: eg: cocaine, amphetamines
Depressants: produce the opposite effects – decreased tension levels followed by an increase in tension: eg: alcohol, heroin, barbiturates, and pain relief meds.

Substance Abuse and other Disabilities
Alcohol and Marijuana Use in a Community-Based Sample of Persons with SCI (Young, Rintala, Rossi, Hart, & Fuhrer, 1995)
Alcohol use = 59% No relationship to impairment, disability, handicap, medical
complications, health ratings, health maintenance behaviors, pain, depression, life satisfaction, perceived stress, or social support
Men more likely to drink History of alcohol abuse = 21%
No significant gender difference Alcohol abusers were more likely to rate overall health as worse, say
they didn’t get enough rest, more depressed and more stressed Not related to impairment, disability, handicap, medical complications
Marijuana use = 16% No gender difference Those who used marijuana were younger and younger at injury and had
lower educational level Users more depressed and stressed

Substance Abuse and other Disabilities
Heinemann (1986) cited studies reporting intoxication at the time of spinal cord injury to be as high as 68% and suggested that impaired judgment because of substance abuse is related to an increase in risk-taking behavior and injury. Alcohol and other drug use are also a major contributing factor to traumatic brain injuries, with an incidence of intoxication at injury of approximately 50% (Heinemann, 1993).Bogner et al (2001) found that approximately 80% of persons with TBIs from violence-related causes had a history of substance abuse. Substance abuse was considered to be a strong predictor of long-term rehabilitation outcomes including satisfaction with life and productivity.

Substance Abuse and other Disabilities
Alcohol and drug abuse also limit rehabilitation outcomes by contributing to functional limitations (Greer, 1986; Greer, Roberts, May, & Jenkins, 1988; NIDRR, 1990). Indirect and direct self-destructive behaviors associated with alcohol and drug abuse, such as refusal of essential treatment and other forms of self-neglect, may continue after the onset of disability and adversely affect the potential for rehabilitation (Ingraham et al., 1992).

Substance Abuse and other Disabilities
Early identification of persons with disabilities who abuse or are addicted to substances should minimize the incidence of secondary complications of disabilities, decrease the cost of rehabilitation, and improve rehabilitation outcomes. Heinemann (1986) indicated that rehabilitation health professionals including psychologists lack sophistication concerning the dual problems of substance abuse and disability. He argued that rehabilitation and health care professionals must be trained to recognize substance abuse problems and to intervene in a timely and effective manner.

Defense mechanisms
Denial I can stop using anytime I want
Projection The boss is on my back all the time. I think
I’m doing a great job. I just have a drink to calm my nerves. She’s making me sick!
Displacement My counselor makes me angry. She just
doesn’t get it that I’m trying. She’s on my back. She just wants to have a good client who does what she wants.
Theoretical Models of Substance Abuse
Moral model People who use substances and alcohol are weak –
places blame on the individual for the abuse and suggests that the person makes a conscious choice not to abuse substances
Spiritual model People who use substance and alcohol have lost
touch with a higher power and as a result have lost his or her way – return to a spiritual source will result in changing one’s abusive ways.
Disease model Substance abuse is illness – places importance on
biological factors.

Theoretical Models of Substance Abuse
Psychological Model Similar to disease model – focuses on maladaptation/poor
adustment at the emotional &/or cognitive level – substance abuse is seen as a compulsion
Social Model Based on the recognition of impact of negative life
experiences eg: societal attitudes, family relationships, finances, work pressures etc – maladaptive patterns of coping are possible causative agents for substance abuse
Bio-psycho-social model Sees substance abuse in a broad manner including biological,
psychological and social factors. The Bio-psycho-social-spiritual model adds the spiritual component. These are holistic models that place emphasis on all areas essential to personal well-being and integration.

Identification of Substance Abuse
Warning signs/symptoms Biological - loss of weight, liver disease, GI
conditions, loss of tooth enamel. Psychological - increase in anger, irritability,
lethargy, confusion Social – socializing with drug users, isolated from
non-using friends, lack of family relationships, loss of job, arrests
Spiritual – loss of values, denial of morality Medical detection – urinalysis can detect presence
of certain drug-related electrolytes and metabolites in the urine. Breathalyzer, hair samples

Identification of Substance Abuse
Screening through written materials CAGE: acronym for four questions asked
by the counselor to the individual – only used for ETOH screening)
MAST – Michigan Alcoholism Screening Test – only used for ETOH screening.
SASSI-2 SARDI Symptoms Checklist
Self-Reporting

CAGE
C- have you ever felt you ought to CUT down your drinking?A- have people ANNOYED you by criticizing your drinking?G- have you ever felt GUILTY about your drinking?E- have you ever had a drink first thing in the morning (EYE OPENER) to steady you nerves or get rid of a hangover.

Brief MAST Questions
Do you feel you are a normal drinkerDo friends or relatives think you are a normal drinkerHave you ever attended a meeting of AA?Have you ever lost friends or girlfriends/boyfriends because of drinking?Have you ever gotten into trouble at work because of drinking? Have you ever neglected your obligations, your family, or your work for 2 or more days in a row because you were drinking?
Have you ever had delirium tremens (DTs) severe shaking, heard voices, or seen things that weren’t there after heavy drinking?Have you ever gone to anyone for help about your drinking?Have you ever been hospitalized because of drinking?Have you ever been arrested for driving drunk?

Treatment
Medical detoxMethadone MaintenanceDrug-free Outpatient TreatmentChemical Dependency (28 days – Minnesota Model – Hazeldon type)Therapeutic CommunitiesSelf-help groups
Stages of Change: A model for understanding addictive behavior change
5 Stages: Precontemplation
Unawareness or denial of the problem Contemplation
Considering change Preparation
Increasing commitment and taking initial steps Action
The actual changing of behaviors Maintenance
Sustaining new behaviors

Spiral of changeFrom Prochaska, DiClemente & Norcross, 1992, p. 1104
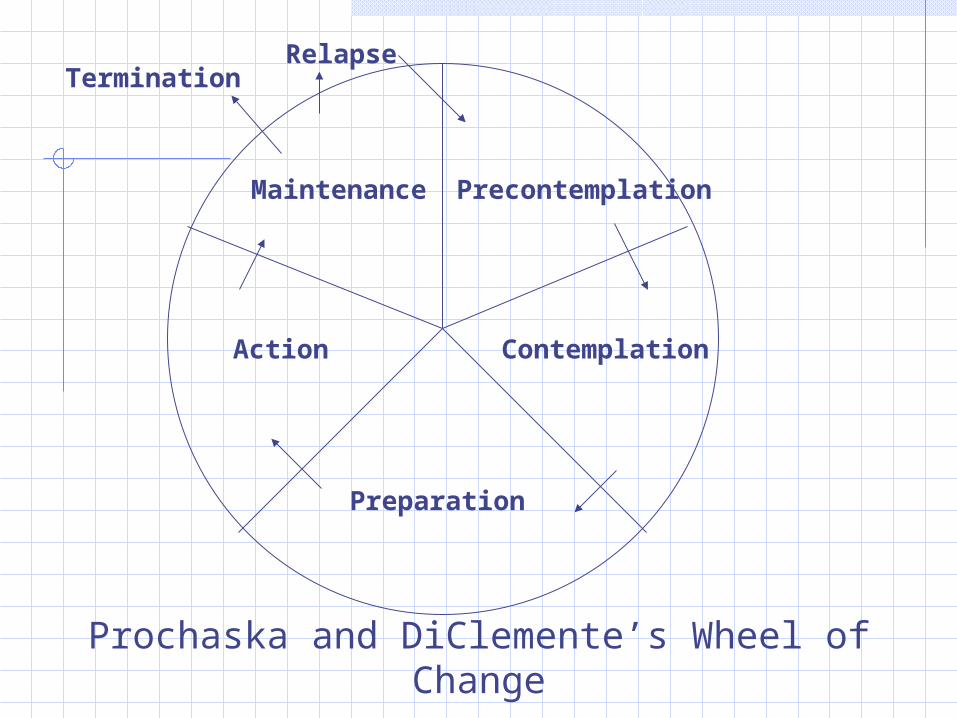
Maintenance
ContemplationAction
Preparation
Termination
Precontemplation
Prochaska and DiClemente’s Wheel of Change
Relapse

10 Common Types of Change Processes
These are coping methods or strategies utilized by people when trying to implement change
Each change process is a category of coping activities which entails numerous techniques or interventions

Processes of Change
Cognitive-Affective Consciousness
raising Self-evaluation Dramatic relief Environmental re-
evaluation Social liberation
Behavioral Counter-
conditioning Stimulus control Reinforcement
management Helping
relationships Self liberation
Stages of Change Model
Clients can be categorized into different stages based on their readiness or motivation to change Interventions should be tailored accordingly
Not a linear process People can cycle through certain stages
before they master the behaviors they want to change

Predictors of Change
Self-efficacy Confidence in the ability to perform certain
tasks Usually lowest during precontemplation stage
and highest during maintenance
Decisional balance Evaluation of pros and cons pertaining to the
performance of specific tasks

Facilitate Change – Motivational Enhancement Therapy
Key Factors for Change for the Counselor:StyleStyleStyle
Miller & Rollnick (2002)

SOC Interventions
Interventions should be designed to build self-efficacy and positive decisional balance through specific coping strategies & skills training for movement through specific stages of changeSOC has been applied to many types of behavior changes: Smoking and other addictive behaviors Weight control Risky health behaviors Understanding change in general psychotherapy,
counseling and case management

Substance Abuse as a Disability recap
ChronicityDeficits in Basic FunctioningDenialEffects all elements of lifeExists on a continuumImpacts self-esteem, self-concept and self-imageNeeds an individualized rehabilitation programExacerbation and RemissionPerson-specific

Links
Substance Abuse & Mental Health Services Administration: http://www.samhsa.gov/ http://www.drugabusestatistics.samhsa.gov/
nsduh/2k5nsduh/2k5Results.pdf
National Institute on Drug Abuse: http://www.nida.nih.gov/National Institute on Alcohol Abuse and Alcoholism: http://www.niaaa.nih.gov/