alien vs terminator? by stephan windecker, md pcr 2014. resolute all comers 5-year tlf ... arroyo...
TRANSCRIPT
11/30/2016
1
Absorb vs Synergy
Clinical Efficacy -Review of Absorb 3 and
Evolve 2 Trials
Dr. Marc Litt
Director Cardiac Cath Lab Baptist Medical Center
Jacksonville,Flordia
SYNERGY™
Everolimus-Eluting Platinum Chromium Stent System with Abluminal Bioresorbable PLGA Polymer
ABSORB BVS GT 1 Bioresorable PLLA scaffold with a Bioresorable PLLA
Polymer with Everolimmus
VS
Alien vs Terminator?
11/30/2016
2
Why develop bioresorable stents or polymers?
5
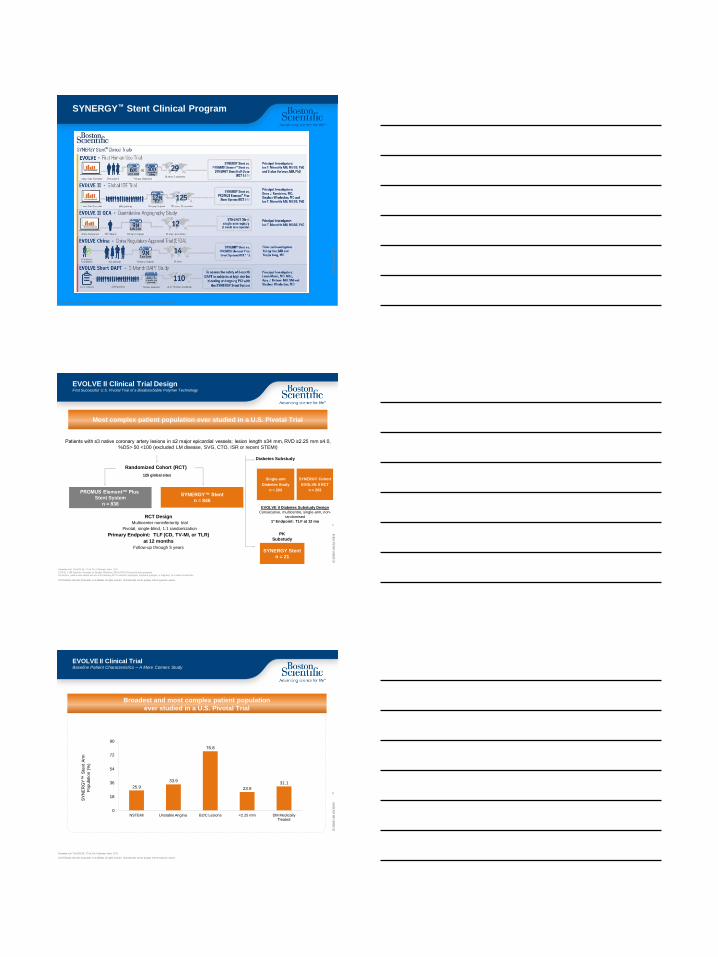
Event rates persist beyond 1 year with current PERMANENT Polymer DES
Presented by Stephan Windecker, MD PCR 2014.
Resolute All Comers 5-year TLF
TLF (target Lesion Failure) is defined as cardiac death, TVMI, of clinically driven TLR.
Why develop bioresorable
stents or polymers?
• Lower late event rates - late TLF ,late ST
• Improve vasomotion
• Reduce need for prolonged DAPT
• Reduce delayed healing/incomplete endothelial coverage
• Reduce inflammation,foreign body giant cell reaction
• Reduce risk negative vessel remodeling
• Reduce late stent malapposition
• Reduce neoatherosclerosis i
11/30/2016
3
Circulation. 2016;134:168–182. DOI: 10.1161/CIRCULATIONAHA.116.021539
DES stent platforms
Stent Xience Resolute Synergy BVS
Structure CoCr/EES CoNi/ZES PtCr/EES PLLA/EES
Strut
Thickness
81 um
91um
74um
150um
Polymer BVDF Biolink PLGA PDLLA
Distribution/
Thickness
conformal/7
-8 um
conformal/6
um
abluminal/4
um
conformal/
7 um
9
Ultrathin Abluminal Coating
Bioabsorbable Polymer Coating (PLGA) • Abluminal • 4µm thick • 85:15 ratio • <4 month absorption time
Everolimus-Eluting • 100μg/cm2
• 3 month release time
Platinum Chromium Platform • 74μm (0.0029in) strut thickness Visibility Strength Flexibility Conformability Recoil
SYNERGY Stent Technology Design
11/30/2016
4
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
10
SYNERGY™ Stent Clinical Program
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
Randomized Cohort (RCT)
SYNERGY™ Stent
n = 846
PROMUS Element™ Plus
Stent System
n = 838
RCT Design
Multicenter noninferiority trial
Pivotal, single-blind, 1:1 randomization
Primary Endpoint: TLF (CD, TV-MI, or TLR)
at 12 months
Follow-up through 5 years
Patients with ≤3 native coronary artery lesions in ≤2 major epicardial vessels; lesion length ≤34 mm, RVD ≥2.25 mm ≤4.0,
%DS> 50 <100 (excluded LM disease, SVG, CTO, ISR or recent STEMI)
SYNERGY Stent
n = 21
Diabetes Substudy
PK
Substudy
125 global sites Single-arm
Diabetes Study
n = 203
SYNERGY Cohort
EVOLVE II RCT
n = 263
EVOLVE II Diabetes Substudy Design
Consecutive, multicentre, single-arm, non-
randomised
1° Endpoint: TLF at 12 mo
Kereiakes et al. The EVOLVE II T rial. Circ Cardiovasc Interv. 2015.
EVOLVE II DM Substudy. Presented by Stephan Windecker, MD at PCR 2015.wing the index procedure.
Per protocol, patients were treated with one of the following P2Y12 inhibitors (clopidogrel, ticlopidine, prasugrel, or ticagrelor) for at least 6 months follo
Most complex patient population ever studied in a U.S. Pivotal Trial
11
EVOLVE II Clinical Trial Design First Successful U.S. Pivotal Trial of a Bioabsorbable Polymer Technology
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
Kereiakes et al. The EVOLVE II T rial. Circ Cardiovasc Interv. 2015.
SY
NE
RG
Y™
Ste
nt
Arm
Po
pu
latio
n (
%)
25.9
33.9
76.8
23.9
31.1
0
18
36
54
72
90
NSTEMI Unstable Angina B2/C Lesions <2.25 mm DM Medically Treated
Broadest and most complex patient population
ever studied in a U.S. Pivotal Trial
12
EVOLVE II Clinical Trial Baseline Patient Characteristics – A More Comers Study

11/30/2016
5
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
EVOLVE II Clinical Trial 2-Year Results
8.5
1.5
5.4
3.1
6.2
9.4
1.0
5.5
4.3
6.7
0
4
8
12
16
20
TLF Cardiac Death TV-MI TLR TVR
Incid
en
ce
Ra
te (
%)
SYNERGY™ Stent System Promus Element™ Plus
Stent System (PP-DES)
Components of TLF
SYNERGY™ Stent System
BP-DES (n=816)
Presented by D. Kereiakes, MD at ACC 2016
ITT Population; Patients who did not receive a study stent were censored at 1 year; KM Event Rates; Per protocol spontaneous MI is defined as rise and/or fall of cardiac biomarkers with ≥1 value >99th percentile of the URL + evidence of myocardial ischemia.
1. TLF: ischemia-driven TLR, MI related to the target vessel, or any cardiac death. The study primary endpoint was the rate of 12-month TLF by both intent-to-treat and per-protocol analyses.
2. Peri-PCI MI is defined as ≥1 of the following: i) biomarker elevations within 48 hours of PCI (based on CK-MB >3X URL), ii) new pathological Q waves, or iii) autopsy evidence of acute MI
P=0.57 P=0.35 P=0.89 P=0.17
Primary Endpoint of Target Lesion Failure (TLF) Met
TLF Cardiac Death Target Vessel MI2 TLR
P=0.57
PROMUS Element™ Plus Stent System
PP-DES (n=796)
13
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
ST Landmark Analysis Definite/Probable ST after 24 hours to 2-Years
Presented by D. Kereiakes, MD at ACC 2016
‡Day 715 – Definite ST: Patient was not compliant to aspirin and was not taking at P2Y12 inhibitor at time of presentation
ST occurring between 0 and 1 years have been previously reported in Kereiakes et al. Circ Cardiovasc Interv 2015
ITT; Patients who did not receive a study stent were censored at 1 year; KM Event Rate; log-rank P values
NNumerically lower ARC Definite/Probable ST with the SYNERGY BP-DES compared to
the PROMUS Element PP-DES
SYNERGY™ Stent System
BP-DES
PROMUS Element™ Plus Stent System
PP-DES
14
P=0.056
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
PROMUS Element Plus
SYNERGY
Subacute (2-30 days) Late (30 days – 1 year)
0.8%
(N=6)
0.4%
(N=3)
P=0.31
Acute (≤1 day)
N=1 (Prob)
N=5 (2 Definite/3 Probable)
N=2 (Definite)
Very Late (1 year – 2 years)
N=1 (Def)
ZERO Definite ST in the SYNERGY arm after 24 hours
Presented by D. Kereiakes, MD at ACC 2016
PROMUS
Element Plus™
Stent System
PP-DES
SYNERGY™
Stent System
BP-DES
EVOLVE II Clinical Trial Exceptionally Low Stent Thrombosis
15

11/30/2016
6
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
SWEET
Registry
Fribourg
Experience
Belfast
Experience
EVOLVE II
Trial
EVOLVE
Trial
EVOLVE
China
EVOLVE II
QCA Study
SCAAR
Registry
N: 820 671 100 846 94 205 100 7880
Acute 1.5% 0.3% 0% 0.2% 0% 0% 0%
Sub-
acute 0.1% 0.3% 0% 0% 0% 0% 0%
Late 0.1% 0.1% 0% 0% 0% 0% 0% 0.1%*
Acute: ≤ 1 day
Subacute: 2 – 30 days
Late: 30 days – 1 year
*Cumulative adjusted ARC def ST
SWEET Registry: Cook TCT 2015., Fribourg Experience: Arroyo CRT 2016. Belfast Experience: Noad TCT 2015., EVOLVE II: Kereiakes, et al. Circ Cardiovasc Interv. 2015;8:e002372.DOI:10.1161/CIRCINTERVENTIONS.114.002372.,EVOLVE FHU:
Meredith et al. J Am Coll Cardiol. 2012; 59 (15):1362., EVOLVE II QCA: Meredith ACC 2015., SCAAR Registry: James TCT 2015.
0.2%*
16
ARC ST (Def) Rates for the
SYNERGY™ Stent at 1-Year
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
Arterial Wall
Promus PREMIER™ Stent Conformal Permanent Polymer
SYNERGY Stent Abluminal PLGA
Bioabsorbable Polymer
17
*Strut thickness for small vessel model is 74μm, Workhorse model is 79μm and large vessel is 81μm. Boston Scientific data on file.
78 µm* Strut + Polymer
97 µm Strut + Polymer
SYNERGY™ Stent Abluminal Coating
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.
IC-3
38
00
1-A
H J
UL
Y2
01
6
96.9
98.3
90.
100.
PROMUS Element™ Plus Stent System
SYNERGY Stent System
Series 1
Kereiakes et al. The EVOLVE II T rial. Circ Cardiovasc Interv. 2015.
1 Technical Success is defined as successful delivery and deployment of the study stent to the target vessel, without balloon rupture or stent embolization, and post-procedure diameter stenosis of <30% in 2 near-orthogonal projections with T IMI 3 flow in the target lesion, as visually assessed by
the physician. Summarized per lesion
(n = 838) (n = 846)
P = 0.04
Te
ch
nic
al S
ucce
ss (
%)
SYNERGY Stent displayed greater technical success1 with delivery and deployment
18
EVOLVE II Clinical Trial SYNERGY™ Stent System Technical Success

11/30/2016
7
19
Summary
• Positive clinical performance of SYNERGY supported by:
• 2-year EVOLVE II Trial data proving non-inferiority to the Promus Element Plus Stent for TLF in a diverse population (>60% ACS, >25% MI, 31% diabetes, smaller vessels, longer lesions, ≥75% AHA/ACC B2/C lesion morphology)
• 2-year EVOLVE II Trial data with no definite ST after 24 hours
• Bioabsorbable polymer-coated DES may enhance healing and improve late outcomes (ST, TLR).
Everolimus/PDLLA (1:1) matrix coating
• 7 µm
• Conformal coating
• Controlled drug release similar to Xience CoCr-EES
PLLA Backbone
• Semi-crystalline
• Circumferential sinusoidal rings connected by linear links
• Strut thickness 150 µm
• Platinum markers in each end ring
Fully
Bioresorbable
Absorb BVS
The current available technology: The reabsorption process
Hydrolysis occurs via random chain scission of the ester bond
1 3 6 24
Support
Mass Loss
Tie
chains Initially, hydrolysis preferentially cleaves amorphous tie
chains, leading to a decrease in molecular weight without
altering radial strength
When enough tie chains are broken, the device
begins losing radial strength
Molecular Weight
12 18
� �
� �
�
� �
�
� � �
�
36 Months
Abbott Vascular.

11/30/2016
8
See Important Safety Information referenced within. ©2016 Abbott. All rights reserved. AP2942359-US Rev. A 22
ABSORB IS BUILT ON PROVEN XIENCE TECHNOLOGY
INDICATIONS: The XIENCE Family of Everolimus Eluting Coronary Stent Systems are indicated for improving coronary luminal diameter in patients, including those with diabetes mellitus, with symptomatic heart disease due to de novo native coronary artery lesions for XIENCE V (length ≤ 28 mm), XIENCE Prime, XIENCE Xpedition and XIENCE Alpine (lengths ≤ 32 mm) with reference vessel diameters of ≥2.25 mm to ≤ 4.25 mm. Additionally, the entire XIENCE Family is indicated for treating de novo chronic total coronary occlusions.
ABSORB: Extensive Clinical Program Real World and Complex Patient Populations
GABI-R Design: All-comers registry
N=~5000 1˚: Safety & efficacy
ABSORB FIRST Design: Prospective, multi-center, global registry
N= ~1800
1˚: ST, CD, MI, revascularization, MACE, TLF, & TVF
BVS EXPAND* Design: All-comers registry
N=~300 1˚: 1-year MACE
GHOST EU Design: All-comers registry N=continuous enrollment
1˚: TVF
FRANCE ABSORB Feasibility: De novo lesions
N=~2000 1˚: 1-year MACE
AIDA Design: RCT vs. XIENCE
N=~1850 1˚: 2-year TVF
REPARA Design: All-comers registry
N=~1500 1˚: 1-year MACE
EVERBIO II Design: Non-inferiority
RCT EES vs. BES vs. BVS
N=~240
1˚: Late lumen loss at 9 months
ASSURE Design: All-comers registry
N=180 1˚: Safety & efficacy
ALL-COMERS
POLAR-ACS Design: ACS registry
N=94 1˚: Safety, clinical device, procedure, success & in-
hospital MACE
TROFI II Design: STEMI vs. XIENCE
N=190 1˚: 6-months,
neo-intimal healing score
PRAGUE 19 Design: STEMI (STEMI Killip I/II)
N=79 1˚: Clinical outcomes
ISAR ABSORB MI Design: Non-inferiority vs. EES
N=260 1˚: % diameter stenosis at 6-8 months
ABSORB CTO Feasibility: CTO
N=35 1˚: Safety & performance
PABLOS Feasibility: Bifurcations
N=30 1˚: Device, procedural, main & side branches
IT-DISAPPEARS Design: MVD and Long Lesion Registry
N=~1000 1˚: Safety & efficacy
ABSORB II Design: Randomized 2:1 Absorb BVS:XIENCE
N=501
1˚: Vasomotion & lumen diameter
after the index procedure & at 3 years
SIMPLE TO MODERATELY COMPLEX POPULATIONS
ABSORB EXTEND Design: Prospective, single-arm, open-label
clinical study
N=812
1˚: ID-MACE
ABSORB COHORT B Design: Allocated (non-randomized)
N=101
1˚: Safety & performance
ABSORB III Design: RCT. N= ~2250
1˚: TLF at 1 year
ADDITIONAL LARGE RCTs
ABSORB JAPAN Design: RCT. N= ~400
1˚: TLF at 1 year
ABSORB CHINA Design: RCT. N= ~440
1˚: In-segment late loss at 1 year
ABSORB IV Design: RCT. N= ~3000
1˚: Angina within 1 year
COMPLEX POPULATIONS
*Excludes STEMI patients. ACS, acute coronary syndrome; MVD, multi -vessel disease; CTO, chronic total occlusion; MI, myocardial infarction RCT, randomized controlled trial; OMT, optimal medical therapy; EES, everolimus-eluting stents; BVS, bioresorbable vascular
scaffold; STEMI, ST-segment–elevation myocardial infarction; MACE, major adverse cardiac events; ID-MACE, ischemia-driven major adverse cardiac events; TLF, target lesion failure; IVUS MLA, intravascular ultrasound minimal lumen area; TVF, target vessel failure; LAD,
left anterior descending; FIM, first-in-man.
UK REGISTRY Design: Prospective, single-arm, multi center,
observational registry N= 1005
1˚: RDS < 50% at procedure conclusion, MACE
FEAST Russia Registry Design: All-comers registry
N=2500
1˚: 1-year MACE, TVF, Revascularization, ST, Peri-procedural
MI, Angina
COMPARE ABSORB Design: High risk for ISR
N=~2100 1˚:TLF Kuwait Registry
Design: All-comers registry N=200
1˚: Safety & efficacy PROSPECT ABSORB Design: RCT BVS vs. OMT in unstable asymptomatic
pts N=900
1˚: 2-Yr IVUS MLA
BVS STEMI First Design: STEMI
N=151 1˚: Safety & performance
RAI Registry Design: All-comers registry
N=1505 1˚: Safety & efficacy
Retrospective Multicentric/MICAT Registry Design: All-comers registry
N=1305 1˚: Safety & efficacy
UNDERDOGS Design: Long Lesions/Overlap
N=314 DOCE at 1 Year

11/30/2016
9
Primary Endpoint
Target Lesion Failure at 1 year (CD,TV-MI,ID-TLR), powered for non-inferiority in 2000 clinical follow-up subjects
Power Secondary Endpoints
1.Angina at 1 year for superiority test of Absorb to Xience
2.ID-TVR at 1 year for superiority test
3.All Revascularization at 1 year for superiority test
Treatment Up to 2 de novo lesions in different epicardial vessels. No planned overlap; RVD (site) 2.5-3.75mm; LL ≤ 24mm
25
30 d 6 mo 12 mo 24 mo 36 mo 48 mo 60 mo
Clinical Follow-up
Prospective, multicenter, single blind, randomized 2:1
Absorb vs. Xience, in ~2000 patients
ABSORB III Study Design
Randomized 2:1
N=2008 (ITT)
ABSORB
N=1322
ABSORB
N=1312
Xience
N=677
99.2% Complete 98.7% Complete
N=4 lost to follow-up
N=6 withdrew consent
N=6 lost to follow-up
N=3 withdrew consent
Xience
N=686
12-month Follow-up
Study Flow and Follow-up
11/30/2016
10
11/30/2016
11
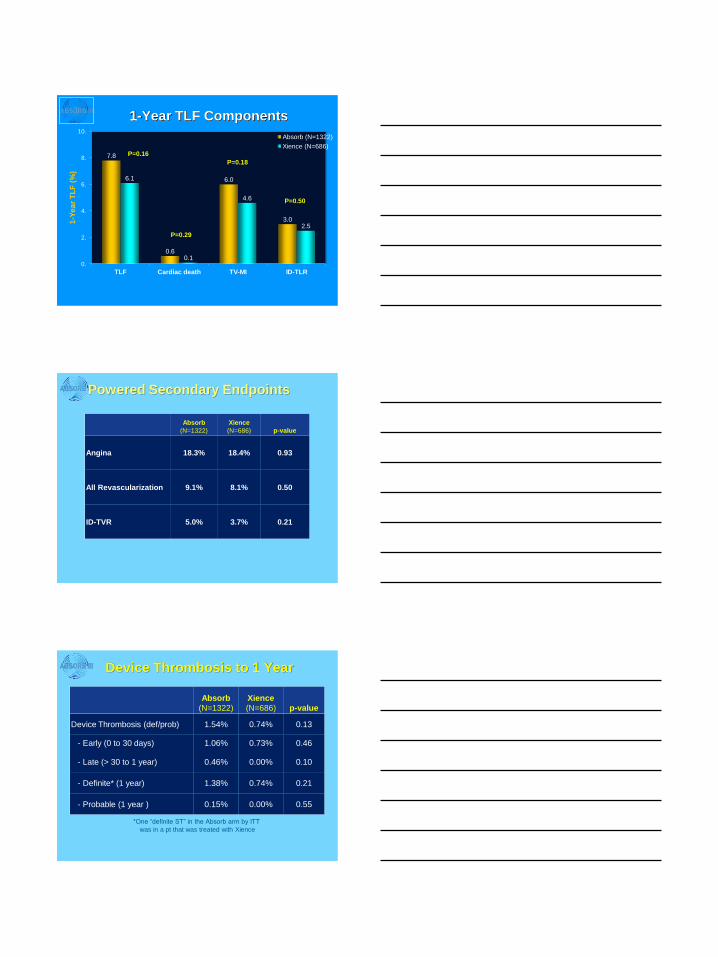
1-Year TLF Components
7.8
0.6
6.0
3.0
6.1
0.1
4.6
2.5
0.
2.
4.
6.
8.
10.
TLF Cardiac death TV-MI ID-TLR
1-Y
ea
r T
LF
(%
)
Absorb (N=1322)
Xience (N=686) P=0.16
P=0.29
P=0.18
P=0.50
Absorb
(N=1322)
Xience
(N=686) p-value
Angina 18.3% 18.4% 0.93
All Revascularization 9.1% 8.1% 0.50
ID-TVR 5.0% 3.7% 0.21
Powered Secondary Endpoints
Absorb
(N=1322)
Xience
(N=686) p-value
Device Thrombosis (def/prob) 1.54% 0.74% 0.13
- Early (0 to 30 days) 1.06% 0.73% 0.46
- Late (> 30 to 1 year) 0.46% 0.00% 0.10
- Definite* (1 year) 1.38% 0.74% 0.21
- Probable (1 year ) 0.15% 0.00% 0.55
*One “definite ST” in the Absorb arm by ITT
was in a pt that was treated with Xience
Device Thrombosis to 1 Year
11/30/2016
12
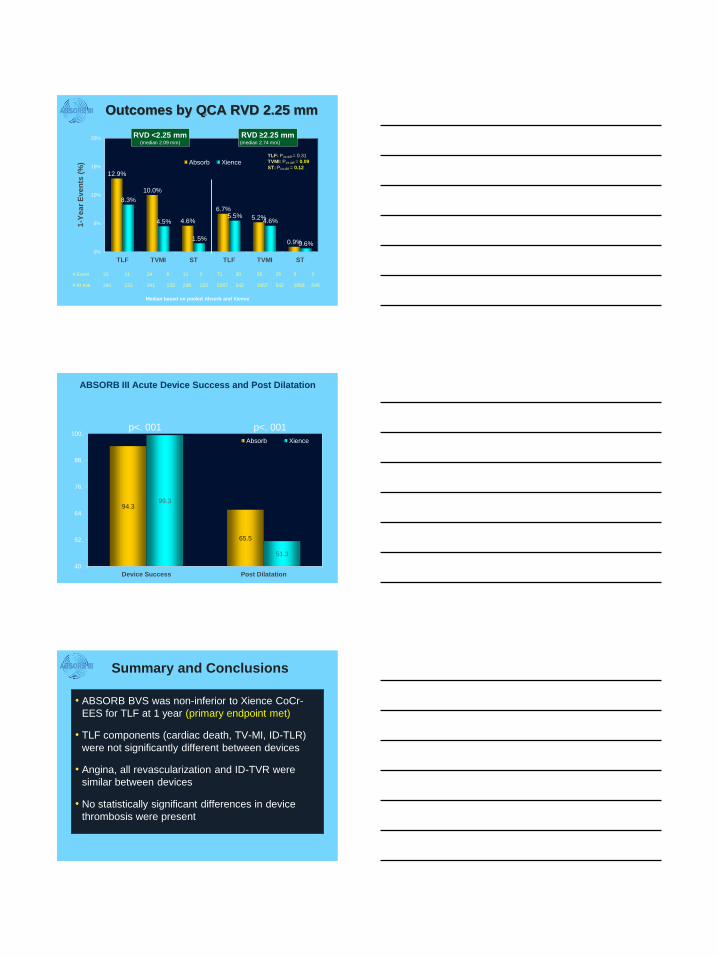
12.9%
10.0%
4.6%
6.7%
5.2%
0.9%
8.3%
4.5%
1.5%
5.5% 4.6%
0.6% 0%
5%
10%
15%
20%
TLF TVMI ST TLF TVMI ST
Absorb Xience
RVD <2.25 mm (median 2.09 mm)
1-Y
ea
r E
ve
nts
(%
)
Median based on pooled Absorb and Xience
RVD ≥2.25 mm (median 2.74 mm)
Outcomes by QCA RVD 2.25 mm
TLF: Pint diff = 0.31
TVMI: Pint diff = 0.09
ST: Pint diff = 0.12
# Event 31 11 24 6 11 2 71 30 55 25 9 3
# At risk 241 133 241 133 238 133 1067 542 1067 542 1058 540
ABSORB III Acute Device Success and Post Dilatation
p<. 001
94.3
65.5
99.3
51.3
40.
52.
64.
76.
88.
100.
Device Success Post Dilatation
Absorb Xience
p<. 001
• ABSORB BVS was non-inferior to Xience CoCr-
EES for TLF at 1 year (primary endpoint met)
• TLF components (cardiac death, TV-MI, ID-TLR)
were not significantly different between devices
• Angina, all revascularization and ID-TVR were
similar between devices
• No statistically significant differences in device
thrombosis were present
Summary and Conclusions

11/30/2016
13
• The ABSORB III trial has demonstrated safety and
efficacy of Absorb BVS at 1 year in patients with
stable CAD and stabilized ACS
• Longer term evaluation is ongoing to determine if
ABSORB improves late outcomes compared to
Xience
Summary and Conclusions
Absorb Meta-analysis 1 year

11/30/2016
14
Absorb II
Absorb China
Absorb Japan
Absorb III
Summary
20/331
8/238
11/265
102/1313
141/2147
1-Year DoCE (TLF): Cardiac Death,TV-MI or ID-TLR
DoCE = Device-oriented composite endpoint
0.1 0.5 5.0 10.0 1.0
Absorb BVS Better
Xience CoCr-EES Better
Test for heterogeneity: I2=0%; P=0.78
Test for overall effect: Z=1.36; P=0.18
7/165
10/237
5/133
41/677
63/1212
1.42 [0.61, 3.30]
0.80 [0.32, 1.98]
1.10 [0.39, 3.11]
1.28 [0.90, 1.82]
1.22 [0.91, 1.64]
Study Absorb BVS
XIENCE CoCr-EES
RR [95% CI] RR [95% CI]
ABSORB 1-Year Meta-analysis
5.7
1.3
4.
0.5
0.
2.
4.
6.
8.
10.
MI ST
1-Y
ear
TLF (
%)
Absorb Xience
P<.08 P<.08
1 Year Absorb Meta-analysis
ABSORB II: Three-year Clinical Outcomes from a
Prospective, Randomized Trial of an Everolimus-
Eluting Bioresorbable Vascular Scaffold vs. an
Everolimus-Eluting Metallic Stent in Patients with
Coronary Artery Disease
PW Serruys, B Chevalier, D Dudek, et al.
A bioresorbable everolimus-eluting scaffold versus a metallic everolimus-eluting stent for ischaemic heart disease caused by de-novo native coronary artery lesions (ABSORB II): an interim 1
Lancet, 385 (2015), pp. 43–54
11/30/2016
15
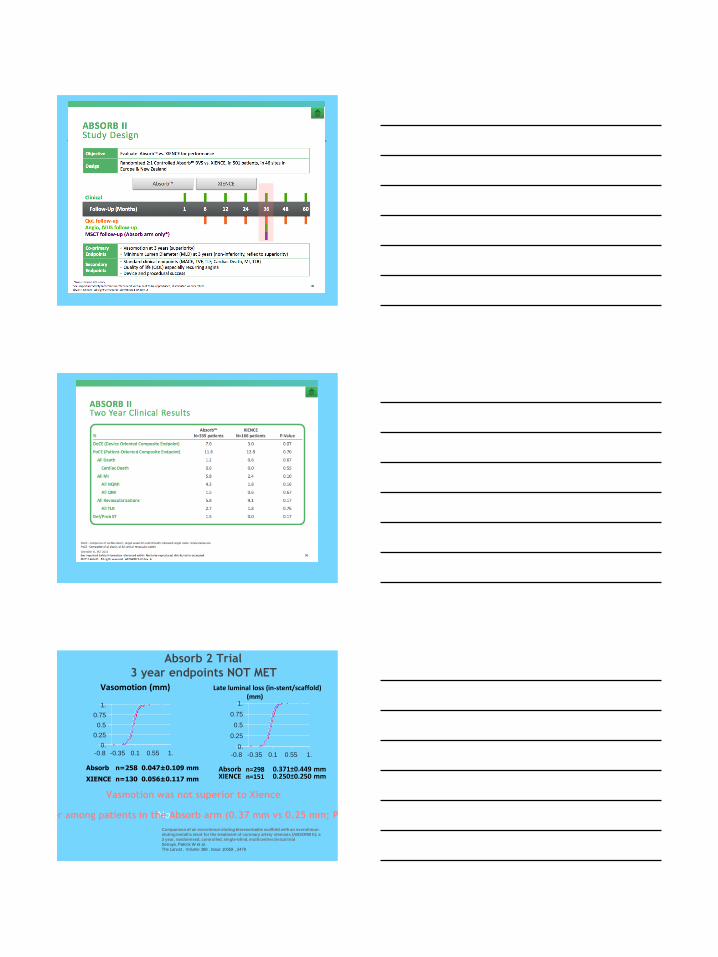
Absorb n=258 0.047±0.109 mm
XIENCE n=130 0.056±0.117 mm
Absorb n=298 0.371±0.449 mm XIENCE n=151 0.250±0.250 mm
0.
0.25
0.5
0.75
1.
-0.8 -0.35 0.1 0.55 1. 0.
0.25
0.5
0.75
1.
-0.8 -0.35 0.1 0.55 1.
Late luminal loss (in-stent/scaffold) (mm)
Vasomotion (mm)
Absorb 2 Trial
3 year endpoints NOT MET
No Late lumen loss was larger among patients in the Absorb arm (0.37 mm vs 0.25 mm; P = 0.78 for noninferiority
Vasmotion was not superior to Xience
Comparison of an everolimus-eluting bioresorbable scaffold with an everolimus-
eluting metallic stent for the treatment of coronary artery stenosis (ABSORB II): a
3 year, randomised, controlled, single-blind, multicentre clinical trial
Serruys, Patrick W et al.
The Lancet , Volume 388 , Issue 10059 , 2479

11/30/2016
16
Composite secondary endpoints
Cardiac death,TV-MI,TVR !0% Absorb 5% Xience P<.04
Absorb 2 -three year results
PW Serruys, B Chevalier, D Dudek, et al.
A bioresorbable everolimus-eluting scaffold versus a metallic everolimus-eluting stent for ischaemic heart disease caused by de-novo native coronary artery lesions (ABSORB II): an interim 1
Lancet, 385 (2015), pp. 43–54
Stent Thombosis Definite Scaffold or stent thrombosis
8/320 (3%) Absorb 0/159 (0) Xience P<.06
6 in Absorb group very late ST >365 days !
Intraluminal scaffold dismantling (ILSD)- the
protrusion of sections of the scaffold into the
lumen due to segmental bulk erosion, which may
occur when little neointimal tissue is present to
otherwise restrain the scaffold struts
J Am Coll Cardiol Intv. 2015;8(13):1768-1769. doi:10.1016/j.jcin.2015.06.026

11/30/2016
17
Perfect Stent Material ??
polymimetic alloy
Or one that dissolves
The Future of Bioresorbable Vascular Scaffolds (BVS):
James C Blankenship MD MHCM MACC M-SCAI
Director, Cardiology and Cardiac Cath Labs
Geisinger Medical Center, Danville PA
No Conflicts of Interest Relevant to this Topic
Principle Investigator at Geisinger
Medical Center for multi-center trials
funded by
Astra-
Zeneca
Boston
Scientific
Abbott
Vascular
Medinal
Stentys Inc
St Jude Medical
Regado
Biosciences
Medinal LTD
GlaxoSMithKline
Takeda
Pharmaceuticals

11/30/2016
18
Problems with First Generation BVS
Strut Absorption Time Radial (Hoop) Strength
Strut Thickness and Width Strut Fracture Resistance
Visibility
Strut Absorption Time
Radial (Hoop) Strength Strut Thickness and Width Strut Fracture Resistance
Visibility
Problems with First Generation BVS
Kereiakes DJ, Onuma Y, Serruys PW, Stone GW. Bioresorbable vascular scaffolds for coronary revascularization.
Circulation. 2016 Jul 12;134(2):168-82.
Supportive
Role of BVS is
Short-Lived
BVS Struts Persist
Long After They Are
Functional

11/30/2016
19
Poly-Lacti
des
Decompos
e at
Different
Rates
Biodegradable magnesium alloy
and polymer
Maintains mechanical integrity for 6
months, totally degrades by 12
months.
Slide
courtes
y of
Chaud

11/30/2016
20
Strut Absorption Time
Radial (Hoop) Strength
Strut Thickness and Width Strut Fracture Resistance
Visibility
Problems with First Generation BVS
Polymer (PLLA) stents have poor radial (hoop) strength
--Therefore lesion preparation is essential
Metal stents have much better radial strength (Mg, Fe)
“Self-Correction”: some stents (e.g., DESolve) expand
.3 mm in the days after implantation
Strut Absorption Time Radial (Hoop) Strength
Strut Thickness and Width
Strut Fracture Resistance Visibility
Problems with First Generation BVS
11/30/2016
21
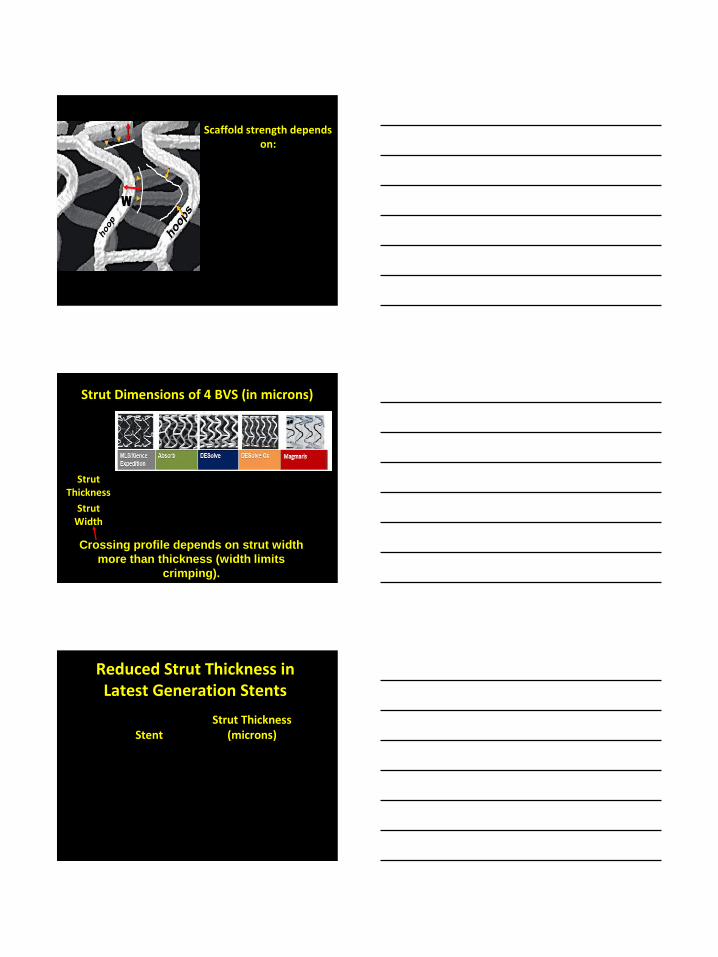
Scaffold strength depends on:
Strut width (exponentially)
Strut thickness (directly)
Shape of hoops, and
# hoops per unit length,
Strut Thickness
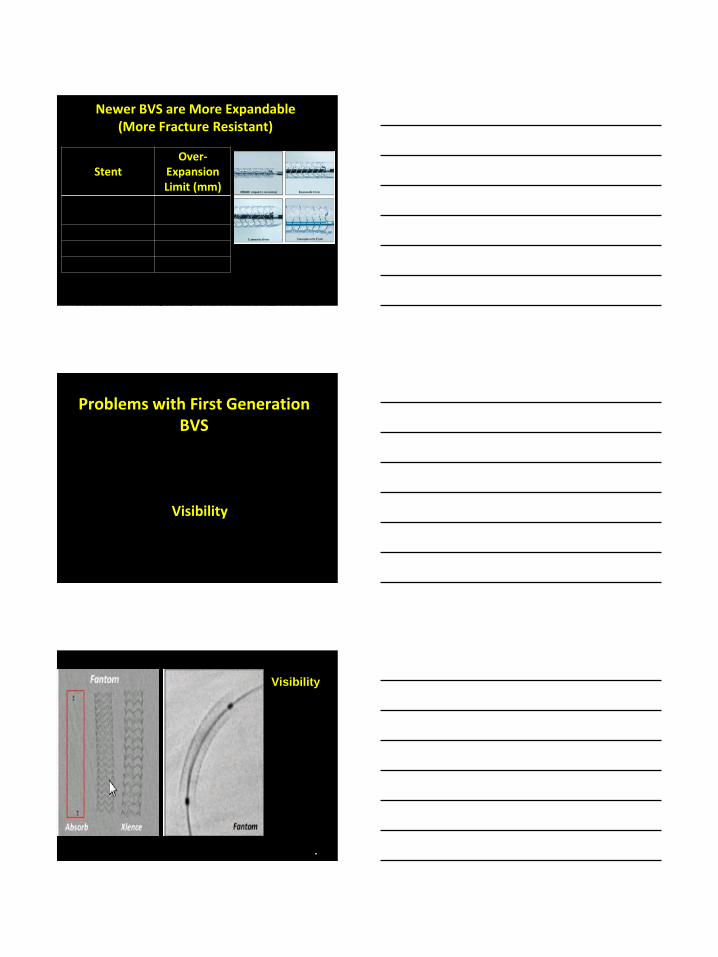
89 157 150 120 150
Strut Width
89-112 191 165 30 20
Strut Dimensions of 4 BVS (in microns)
Crossing profile depends on strut width
more than thickness (width limits
crimping).
Stent
Strut Thickness (microns)
FANTOM/ReZolve 125
DeSolve CX 120
DREAMS 2G/Magmaris
120
ReZolve 2 100
MeRES 100
Absorb next 100
Reduced Strut Thickness in Latest Generation Stents

11/30/2016
22
Strut Absorption Time Radial (Hoop) Strength
Strut Thickness and Width
Strut Fracture Resistance Visibility
Problems with First Generation BVS
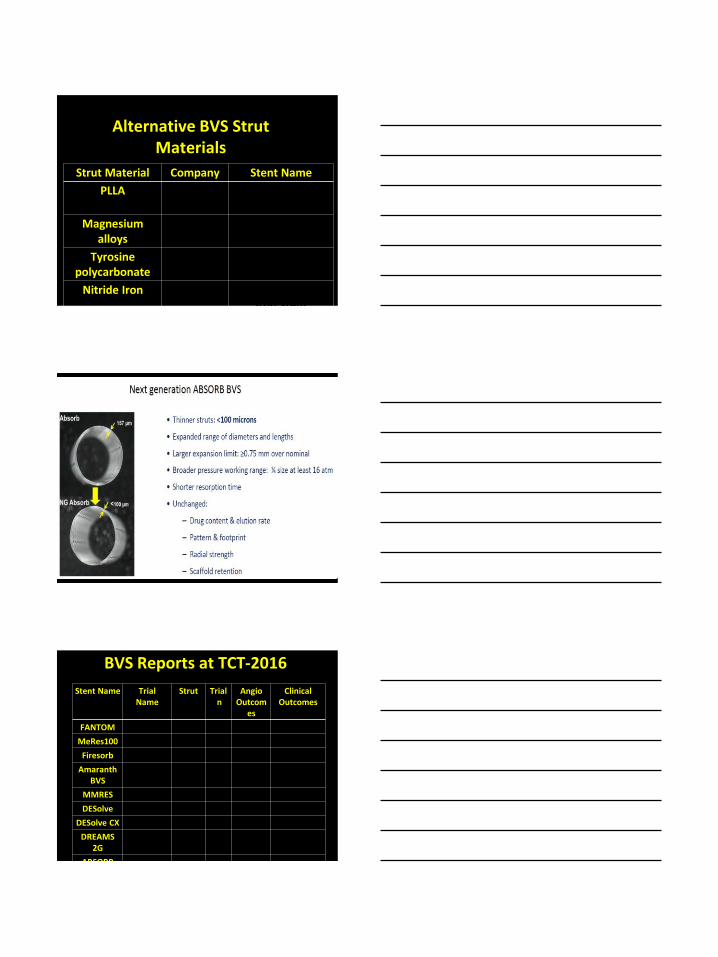
Expansion
Limits
Stent
Over-Expansion Limit (mm)
Absorb next generation
.75
FANTOM 1.0
DESolve 1.5
Newer BVS are More Expandable (More Fracture Resistant)
11/30/2016
23
Stent
Over-Expansion Limit (mm)
Absorb next generation
.75
FANTOM 1.0
DESolve 1.5
DREAMS 2.3
https://www.researchgate.net/figure/261254372_fig8_Fig-8-
Post-dilatation-capability-of-a-30-mm-DREAMS-2nd-
generation-The-device-is
Newer BVS are More Expandable (More Fracture Resistant)
Strut Absorption Time Radial (Hoop) Strength
Strut Thickness and Width Strut Fracture Resistance
Visibility
Problems with First Generation BVS
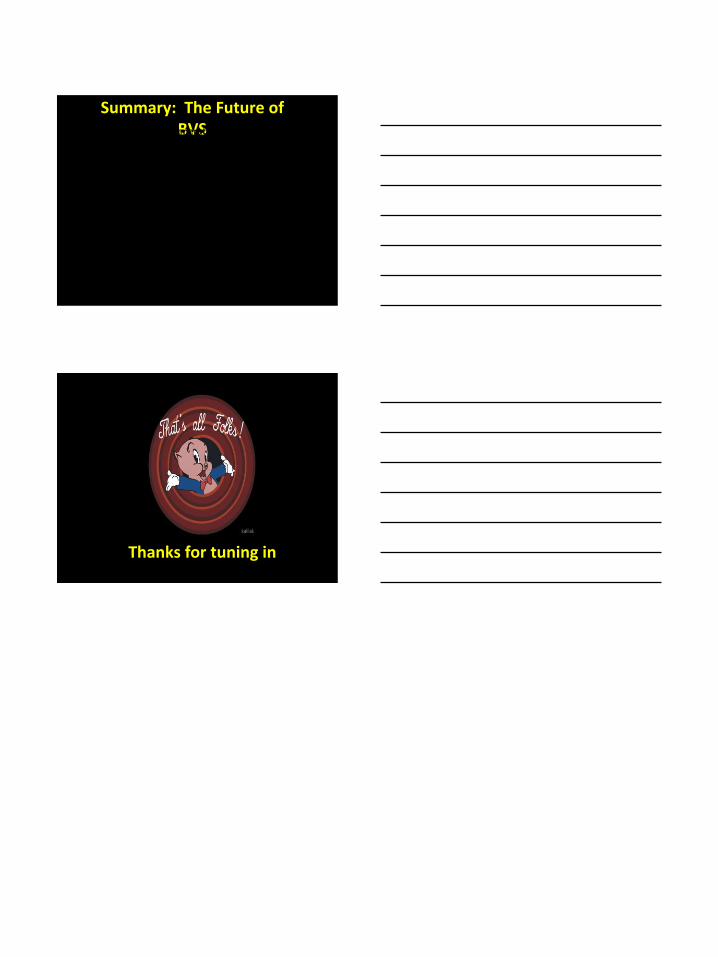
Visibility
Abizaid A, Ribamar Costa J.
The unmet needs: How future
technologies will address
current limitations of
bioresorbable scaffold
technology. Catheterization
and Cardiovascular
Interventions. 2016 Nov
1;88(S1):54-9.
Polyester
carbonate
scaffold with
iodinated
tyrosine
molecules.
Iodine gives it
radiovisibility

11/30/2016
24
Next-Generation BVS
Faster Strut Absorption Better Radial Strength
Thinner Struts More expandable, Fracture-
Resistant Better Angiographic Visibility
Kereiakes DJ, Onuma Y, Serruys PW, Stone
GW. Bioresorbable vascular scaffolds for
coronary revascularization. Circulation. 2016
Jul 12;134(2):168-82.
The Race to Create the
Better Bioabsorbable
Vascular Scaffold
19 companies
23 stents
The Race to Create the
Better Bioresorbable
Vascular Scaffold
Euro Heart J. 2014;35:765-
11/30/2016
25
Strut Material Company Stent Name
PLLA Abbott Vascular
Absorb
Magnesium alloys
Biotronik DREAMS/Magmaris
Tyrosine polycarbonate
Reva Fantom/ReZolve
Nitride Iron Lifetech Lifetech Nitride Iron Stent
Alternative BVS Strut Materials
Stent Name Trial Name
Strut Trial n
Angio Outcom
es
Clinical Outcomes
FANTOM FANTOM II PLLA 240 good good
MeRes100 MeRes 1 PLLA 108 good good
Firesorb FUTURE1 PLLA 45 good good
Amaranth BVS
FORTITUDE PLLA 63 good good
MMRES MIRAGE PLLA 60 good good
DESolve DESolve PLLA 120 good good
DESolve CX DESolve CX PLLA 25 good good
DREAMS 2G
BIOSOLVE II
Mg 123 good good
ABSORB Absorb- PLLA 467 good good
BVS Reports at TCT-2016
11/30/2016
26
Summary: The Future of BVS Efficacy of 1st-generation BVS is uncertain
2nd-generation BVS are addressing problems of 1st-gen BVS
All versions are drug-eluting, made of polymer or metal
19 companies are competing
Uncertain if BVS can rival current DES short-term
outcomes
Long-term benefits of BVS are attractive but unproven
Thanks for tuning in