"align-tegrating" medication care for seniors
TRANSCRIPT



I have had no support, funding or honoraria from any drug company.
But I do own and operate a pharmacy
I am a senior myself so I have a bias
I take drugs too!

Quantity versus quality
Therapeutic benefit versus potential harm
Is life expectancy shorter than the time needed to benefit from the medication prescribed?
Can medications be reduced or stopped?

Is there evidence the medication is effective, needed or clearly indicated?
If not, can the medication be tapered, withdrawn, stopped or dose reduced?
Is there evidence the medication is causing harm (low blood pressure and low blood sugars can be harmful!)
What is the risk of stopping the medication?

Home Number of Residents
Male Female Age 90 or greater
AM 62 17 45 24
CO 76 18 58 25
PP 75 27 48 33
KC 74 5 69 29
Total 287 67 (23%) 220 (77%) 111 (39%)

Average weight: Male
Average weight: Female
74 Kg 57 Kg

AVERAGE AGE OF ALL 287 RESIDENTS IS 88.2 YEARS
AVERAGE MEDICATION USE IN CARE HOMES IS BETWEEN 6 AND 8 REGULAR MEDICATIONS PER RESIDENTS
RANGE IS 0 TO 20
11 RESIDENTS ARE 99 OR OLDER AND AVE FOR THESE IS 5!! (RANGE 0 TO 8)

Intensive control of blood pressure and blood sugars does not necessarily improve outcomes. In fact, studies have shown the opposite. Frail elderly do better with higher blood pressures and higher blood sugars than previously thought.
BUT! How high can we go? What is safe?

TARGET SYSTOLIC BLOOD PRESSURE 140 mm Hg
(SBP less than 140 mm does not improve outcomes and results in more side effects)
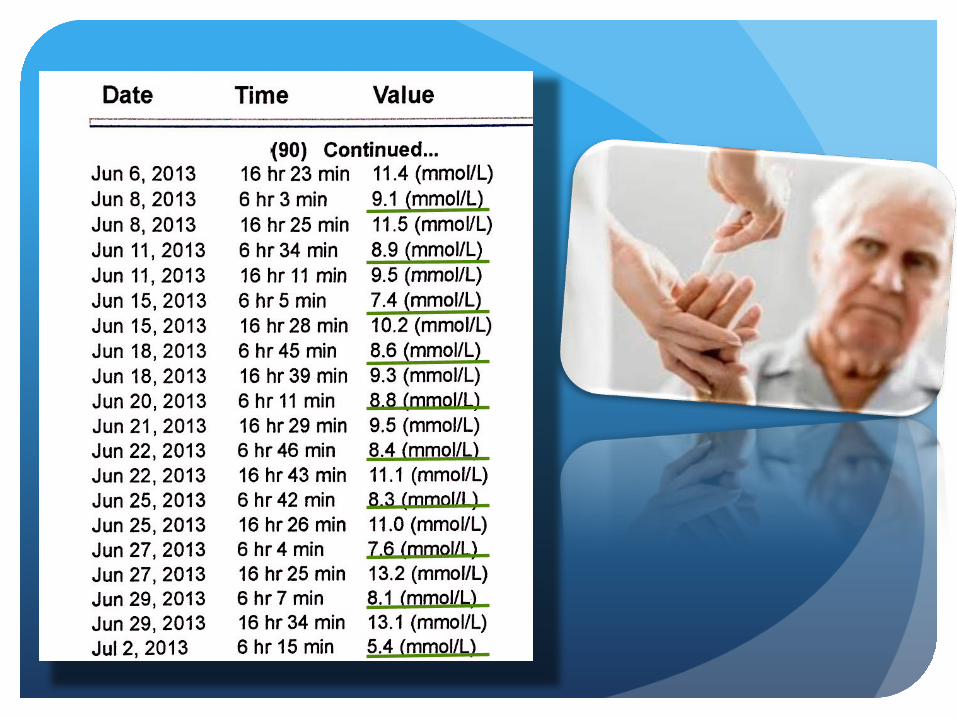
TARGET FASTING GLUCOSE 5.0 TO 12 mmol/L and HgA1c VALUES LESS THAN 8.5%
(Prevention of hypoglycemia should be a priority)

DO NOT CONSIDER STARTING TREATMENT UNLESS SBP IS GREATER THAN 160 mm Hg
IF SBP IS LESS THAN 140 mm Hg MEDICATIONS CAN BE TAPERED AND DISCONTINUED
IN THE VERY FRAIL WITH SHORT LIFE EXPECTANCY TARGET SBP IS 160 TO 190 mm Hg
DO NOT USE MORE THAN 2 ANTI-HYPERTENSIVES



BP FEB 2013 122/76
BP MAR 2013 115/78
BP APR 2013 131/79
AMLODIPINE 10 MG DAILY D/C MAY 6/2013
BP AUG 2013 144/54
BP SEP 2013 122/68


BP 122/66 MAY 7/13
BP 140/71 MAY 12/13
BP 116/76 JUN 1/13
AMLODIPINE 7.5 MG DAILY STOPPED JUN 19/13
BP 146/74 SEP 2013
BP 139/77 OCT 2013
BP 127/66 NOV 2013
















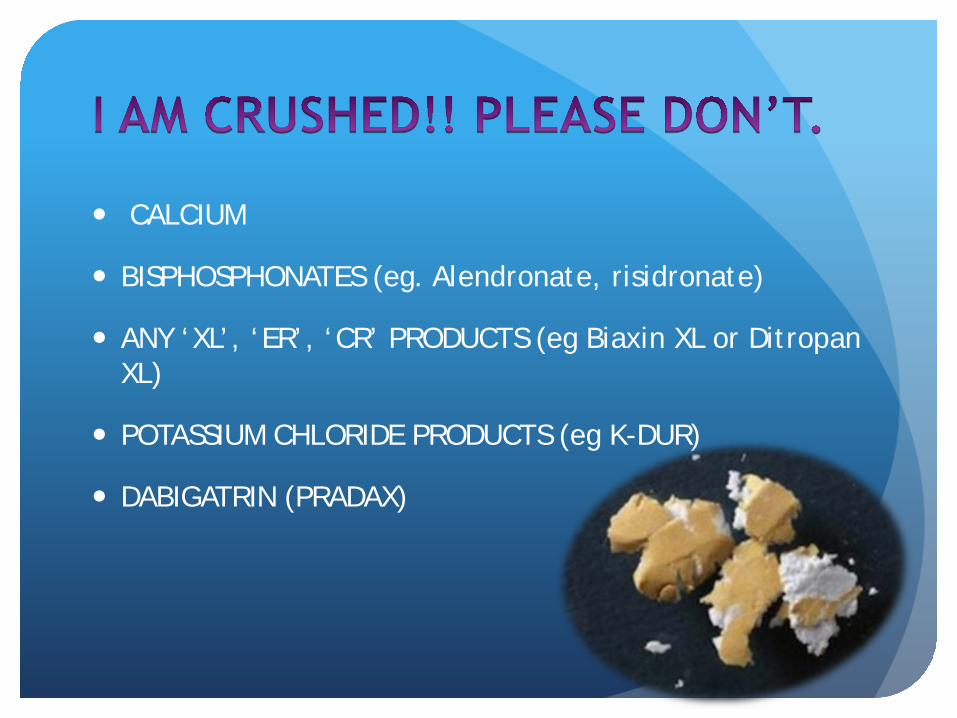
CALCIUM
BISPHOSPHONATES (eg. Alendronate, risidronate)
ANY ‘XL’, ‘ER’, ‘CR’ PRODUCTS (eg Biaxin XL or Ditropan XL)
POTASSIUM CHLORIDE PRODUCTS (eg K-DUR)
DABIGATRIN (PRADAX)

Primary Prevention (No history of stroke or ischemic heart disease)
Do not start or continue statins
Secondary Prevention (Prior history of stroke or ischemic heart disease)
Probably not necessary to start or continue satins There may be extenuating circumstances that shift the risk/benefit ratio

