all change! infections, injecting drug use and harm reduction. vivian hope idu team, hiv & sti...
TRANSCRIPT

All Change! Infections, injecting drug use and harm reduction.
Vivian HopeIDU Team, HIV & STI Department, Health Protection Services – Colindale
Dr Vivian HopeInjecting Drug Use Team, HIV & STI Department,Centre for Infectious Disease Surveillance and Control, Public Health England.&Honorary Senior Lecturer, Centre for Research on Drugs & Health Behaviour,London School of Hygiene & Tropical Medicine.

The 1990’s
HeroinCocaine powder
Amphetamine
0%
20%
40%
60%
80%
100%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Anti-HBc Anti-HCV
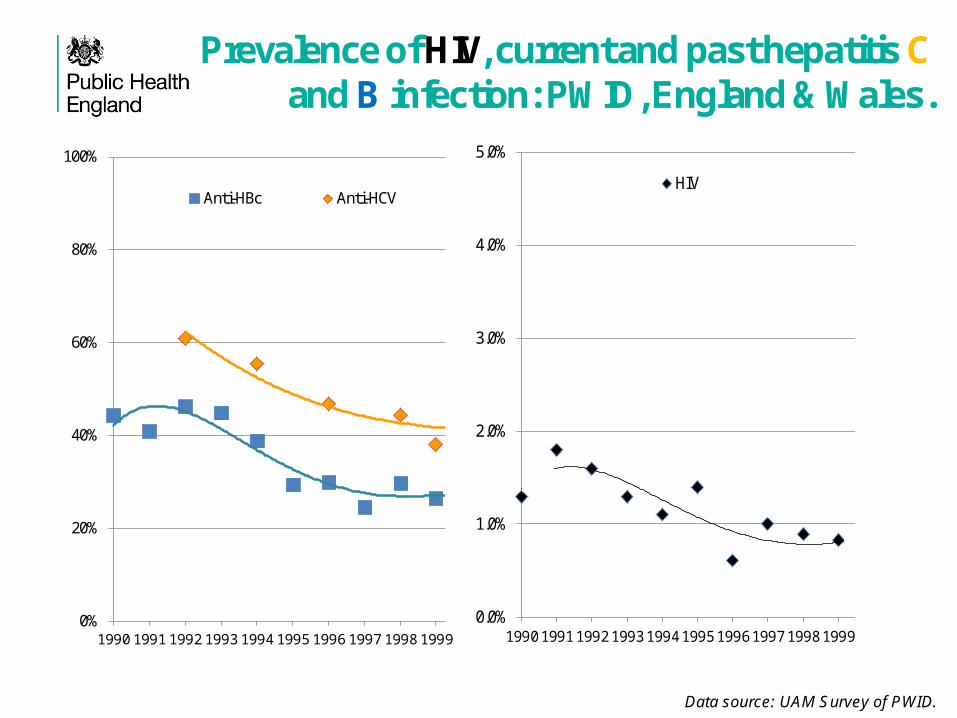
Prevalence of HIV, current and past hepatitis Cand B infection: PWID, England & Wales.
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
HIV
Data source: UAM Survey of PWID.

Risks and other infections in the 1990’s
Throughout the 1990’s just over half of PWID reported that they had ever been tested for HIV.
But, only a quarter of PWID had taken up the vaccine against hepatitis B.
General concerns about ‘hygiene’ related bacterial infections.
Two cases of tetanus between 1984-2000.
Reported needle and syringe sharing declined from 24% in 1991 to 17% in 1998, before rising again to 33% in 1999.
Data sources: UAM Survey of PWID.Shooting Up report 2010

The 2000’s
HeroinCocaine powder
Amphetamine
Crack-cocaine
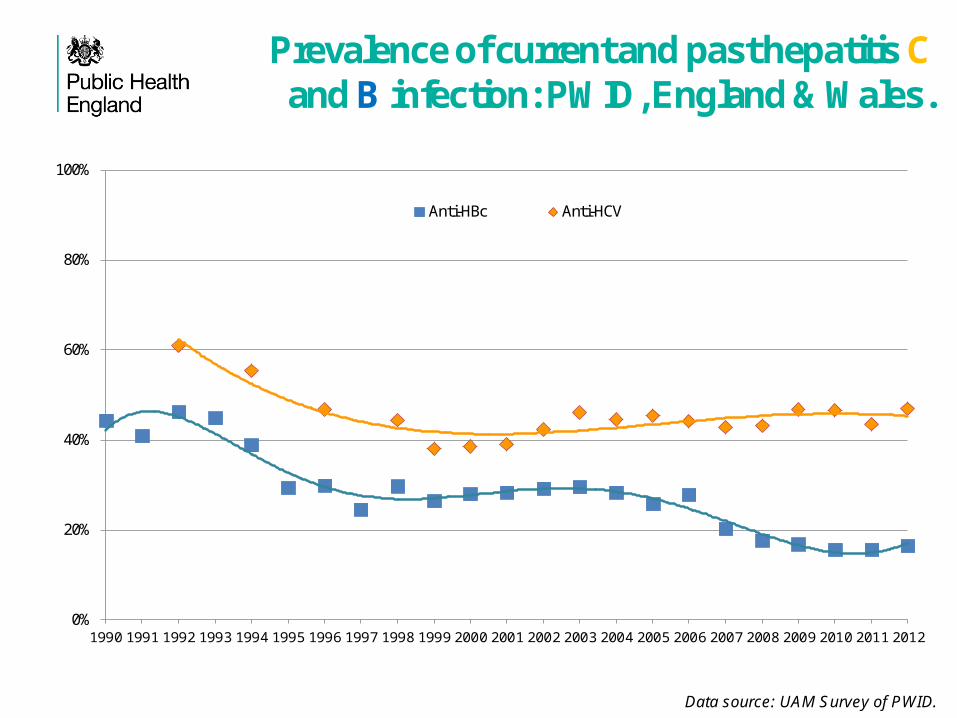
Prevalence of current and past hepatitis Cand B infection: PWID, England & Wales.
Data source: UAM Survey of PWID.
0%
20%
40%
60%
80%
100%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Anti-HBc Anti-HCV

HIV prevalence:PWID, England & Wales.
Data source: UAM Survey of PWID.
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
HIV prevalence in London is about four times higher than elsewhere.
In 2012, it was 3.7% in London; 0.8% elsewhere.

0.1
.2.3
.4.5
.6.7
HC
V
0.0
2.0
4.0
6.0
8H
IV
1980 1985 1990 1995 2000 2005 2010Year
1st year injecting
0.1
.2.3
.4.5
.6.7
HC
V
0.0
2.0
4.0
6.0
8H
IV1980 1985 1990 1995 2000 2005 2010
Year
7 years injectingLondon
0.1
.2.3
.4.5
HC
V
0.0
05.0
1.0
15.0
2.0
25H
IV
1980 1985 1990 1995 2000 2005 2010Year
1st year injecting
0.1
.2.3
.4.5
HC
V
0.0
05.0
1.0
15.0
2.0
25H
IV
1980 1985 1990 1995 2000 2005 2010Year
7 years injectingRest of E&W
Estimated HIV (& HCV) incidence among PWID, England & Wales.
Data source: UAM Survey of PWID.Incidence modelled in a Bayesian framework using prevalence by time since first injection, and modelling for HIV and hepatitis C together. Hope et al, EuroSurveilance in press.

Bacterial infections
Spore formers.•C. Noyvi outbreak in 2000.•Since 2000, on-going occurrence of wound botulism and tetanus cases – including clusters.•Since 2009 also issues with anthrax.•Related to spores contaminating heroin.
Also hygiene related bacteria infections.•Around one-third of PWID report an abscess, sore or open wound, all possible symptoms of an injecting-site infection, during the last year.
Spore forming bacterial infections among PWID: reported cases in the UK
Data source: Shooting Up report 2013.

2010’s and the future
HeroinMephedrone
Cocaine powder
AmphetamineMethamphetamine
Crack-cocaine

Injecting drug use has been ‘declining’
‘Drug’ treatment demand: Injecting status at presentation, new treatment journeys (Data Source: NTDMS).
Estimated number of opiates and/or crack-cocaine users who are injecting.
(Data Source: NTA Website)
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2007/08 2008/09 2009/10 2010/11 2011/12
Nu
mb
er
Prp
ort
ion
of
tota
l
Currently Injecting Previously Injected
Never Injected* Missing / Inconsistent
Currently Injecting Total inc. Missing / Inconsistent
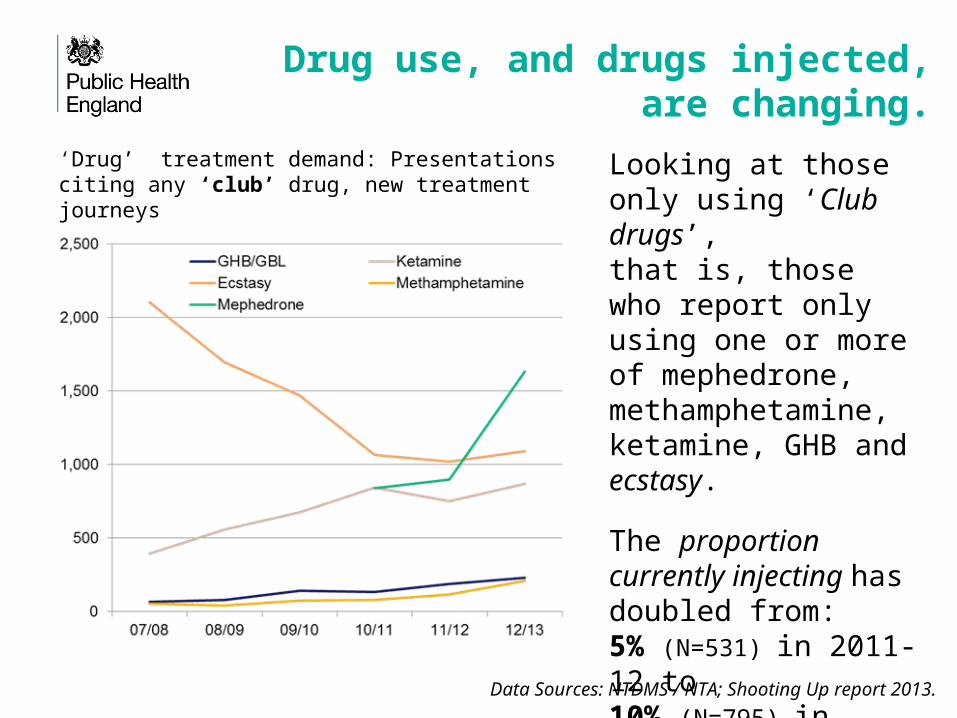
Drug use, and drugs injected, are changing.
‘Drug’ treatment demand: Presentations citing any ‘club’ drug, new treatment journeys
Looking at those only using ‘Club drugs’,that is, those who report only using one or more of mephedrone, methamphetamine, ketamine, GHB and ecstasy.
The proportion currently injecting has doubled from: 5% (N=531) in 2011-12 to 10% (N=795) in 2012-13.
Data Sources: NTDMS / NTA; Shooting Up report 2013.
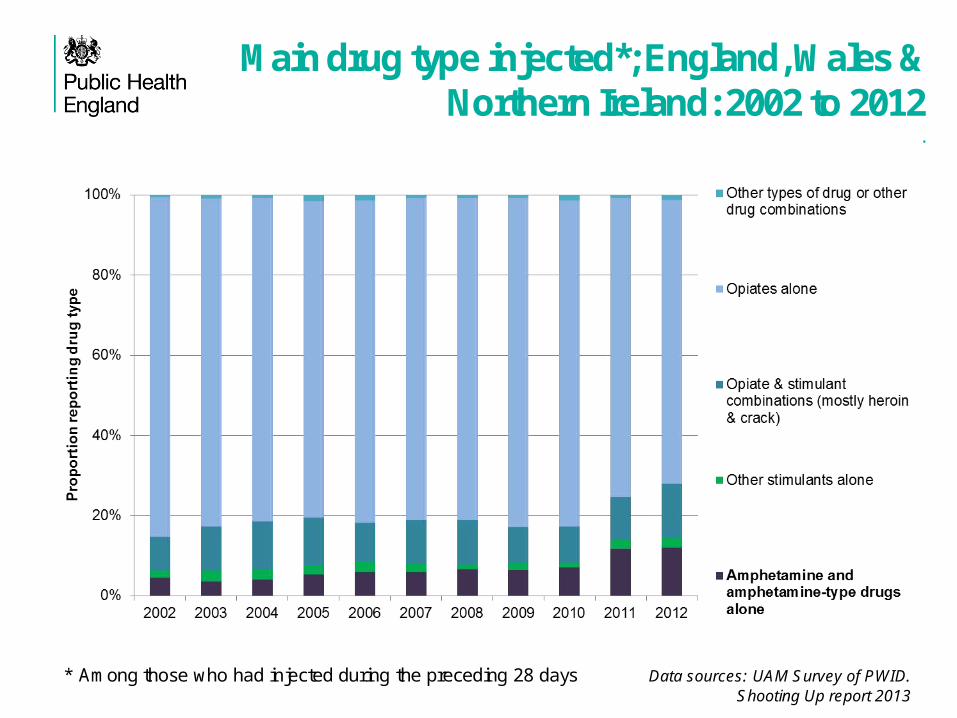
Main drug type injected*; England, Wales & Northern Ireland: 2002 to 2012
.
* Among those who had injected during the preceding 28 days Data sources: UAM Survey of PWID.Shooting Up report 2013
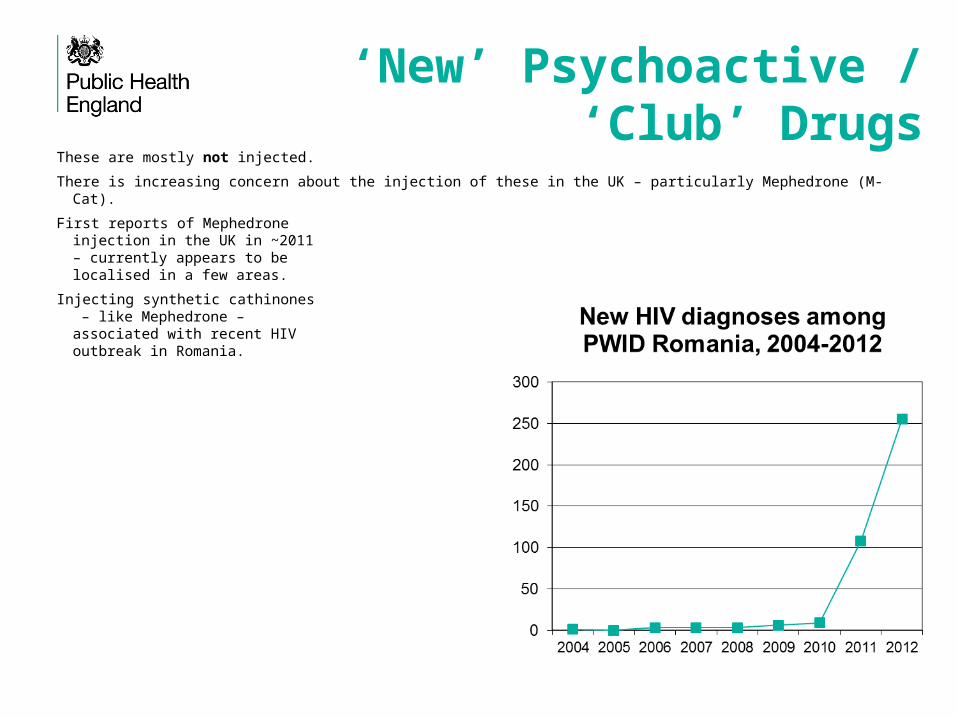
‘New’ Psychoactive / ‘Club’ Drugs
These are mostly not injected.
There is increasing concern about the injection of these in the UK – particularly Mephedrone (M-Cat).
First reports of Mephedrone injection in the UK in ~2011 – currently appears to be localised in a few areas.
Injecting synthetic cathinones – like Mephedrone – associated with recent HIVoutbreak in Romania.

Injecting drug use among MSM
There have recently been concerns about the changing patterns of drug use among some sub-groups of MSM.
Particularly the use of ‘new psychoactive drugs’ and increased use of methamphetamine.
Historically injecting drug use was relatively rare among gay and bisexual identified men.
There is evidence that a small number of MSM – mostly HIV positive gay identified men – are ‘slamming’ (injecting methamphetamine) often in the context of ‘sex parties’.
Low levels of condom use and high level of injecting equipment sharing.
Concerns about transmission of STIs and hepatitis C.

Image and performance
enhancing drugs (IPED)

‘All’ & ‘new’ clients attending agency based NSPs in Cheshire & Merseyside
(1991-2011).Data provided by Centre for Public Health at Liverpool JMU.
AS = Anabolic Steroid.
IPED use and risk
A wide range IPED are used and injected - Anabolic Steroids are the mostly commonly used and injected.
A recent study of 395 male IPED injectors:-
• Main IPEDs injected: Anabolic steroids (86%); Growth hormone (32%); hCG (16%); Insulin (6%); Melanotan I/II (9% ).
• Main IPED taken orally: Anabolic steroids (57%); Anti–oestrogens (23%); Clenbuterol (15%); Ephedrine (20%); Phosphodiesterase type 5 inhibitors (“Viagra /Cialis”, 7%).
•Overall, 9% had ever shared injecting equipment.
•High levels of sexual activity, condom use poor; 3% had sex with a man in the past year.
•High levels of non-injecting psychoactive drug use in past year: 46% cocaine, 12% amphetamine.
•Overall, 5% had ever injected a psychoactive drug.
Hope et al. BMJ Open 2013

IPED use and BBV infectionNote: Oral Fluid sample test sensitivity for anti-HBc is 75% and for anti-HCV is 92%.
Among the male injectors of psychoactive drugs taking part in the UAM Survey in 2011:
•45% (95%CI 43%-48%) had anti-HCV;
•16% (95%CI 14% -18%) had anti-HBc;
•1.4% (95% CI 0.88% -2.2%) had anti-HIV.
Hope et al. 2013 BMJ Open.Crampin et al. 1998 Epidemiology & Infection.
A study of IPED injectors in the 1990s (N=149) found no HIV and 2.7% had ever been infected with hepatitis B.

Implications

Implications service provision and harm
reduction “Traditional” focus of harm reduction services is on:• Heroin, and more recently heroin and crack, injection / use.
• Small number of people injecting stimulants (such as, amphetamine and cocaine), though in some areas, e.g. in parts of South Wales, the injection of these has been more common.
• An aging cohort.
Now (and the future?):• People who inject IPED.
• Wider range of psychoactive drugs being injected.
• Changes in demographics.
Issues:• ‘Different needs’;
• Sex & Drugs;
• ‘Health and fitness’;
• Different settings.
Implications for research:Harm reduction
What are the best ways to :-
1. Engage with IPED injectors/users so as to reduce harm?
2. Provide effective harm reduction services – particularly NSPs – to a wide range of people, using a wide range of drugs, who may have very different needs?
3. Address the harm related to drug use, including injecting, around sexual activity?
And to address these issues in a time of austerity.
Currently among people who inject psychoactive drugs
Hepatitis C stable around 45%. In 2012, 83% ever had a diagnostic test for hepatitis C; but only 54% of those infected are aware of their infection.
HIV prevalence probably stable at around 1.0% to 1.5%. Majority (>80%) of PWID living with HIV are aware of their infection.
Hepatitis B declining (17%) mainly due to vaccination: currently 75% report uptake of vaccine against hepatitis B compared with 58% in 2002.
Needle and Syringe sharing has been declining again, down from 34% in 2002 to 14% in 2012.
Proportion reporting a recent injection site ‘wound or abscess’ may be declining (29% in 2012, down from 38% in 2007).
Data source: UAM Survey of PWID.

In conclusion
Changing patterns of psychoactive drug use and injection – not a new issue (e.g. crack-cocaine a decade ago).• Could increase infection risks.
• Different population groups.
Changing ‘nature’ of injecting drug use – increased use of image and performance enhancing drugs.• Different population groups.
• ‘Health and fitness‘ – not ‘drug use’.
Need to be vigilant for emerging patterns of use and risk, and to respond to these quickly.

www.hpa.org.uk/Publications/InfectiousDiseases/BloodBorneInfections/ShootingUp/