all ed unit performance for gwh - modern mindset - opr oct board.… · 1.0 emergency performance...
TRANSCRIPT
1.0 Emergency Performance
1.1 Four Hour Stay Performance
This section summarises the work currently undertaken as part of the 4 Hour Recovery Plan.
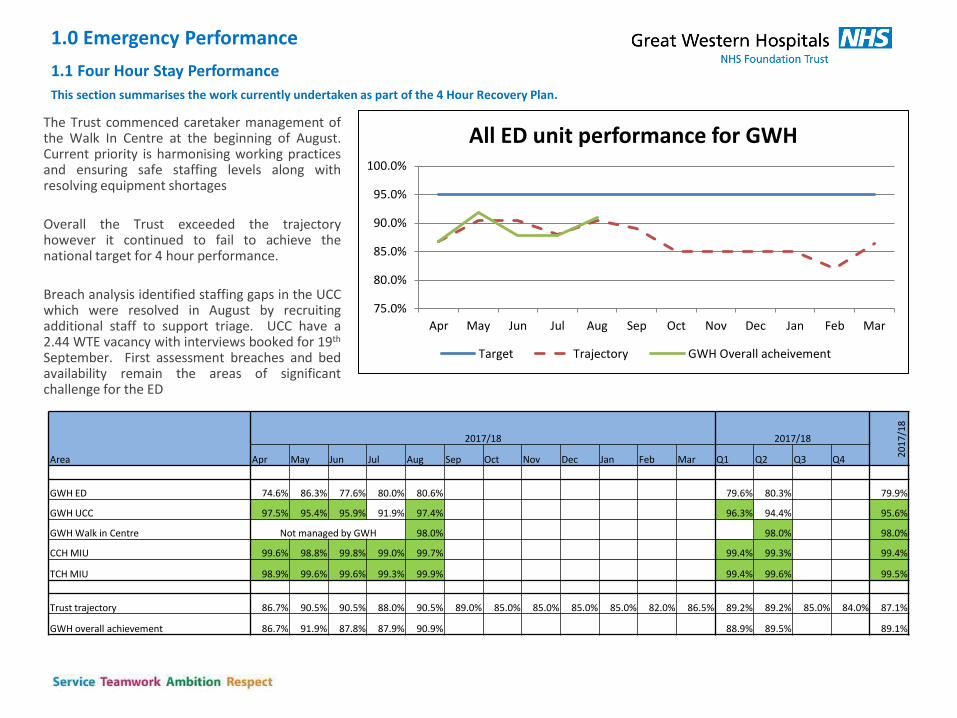
The Trust commenced caretaker management of the Walk In Centre at the beginning of August. Current priority is harmonising working practices and ensuring safe staffing levels along with resolving equipment shortages
Overall the Trust exceeded the trajectory however it continued to fail to achieve the national target for 4 hour performance.
Breach analysis identified staffing gaps in the UCC which were resolved in August by recruiting additional staff to support triage. UCC have a 2.44 WTE vacancy with interviews booked for 19th September. First assessment breaches and bed availability remain the areas of significant challenge for the ED
Area
2017/18 2017/18
20
17
/18
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Q1 Q2 Q3 Q4
GWH ED 74.6% 86.3% 77.6% 80.0% 80.6% 79.6% 80.3% 79.9%
GWH UCC 97.5% 95.4% 95.9% 91.9% 97.4% 96.3% 94.4% 95.6%
GWH Walk in Centre Not managed by GWH 98.0% 98.0% 98.0%
CCH MIU 99.6% 98.8% 99.8% 99.0% 99.7% 99.4% 99.3% 99.4%
TCH MIU 98.9% 99.6% 99.6% 99.3% 99.9% 99.4% 99.6% 99.5%
Trust trajectory 86.7% 90.5% 90.5% 88.0% 90.5% 89.0% 85.0% 85.0% 85.0% 85.0% 82.0% 86.5% 89.2% 89.2% 85.0% 84.0% 87.1%
GWH overall achievement 86.7% 91.9% 87.8% 87.9% 90.9% 88.9% 89.5% 89.1%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
All ED unit performance for GWH
Target Trajectory GWH Overall acheivement
1.2: Update from Daily ED Breach Analysis: Actions & Themes
A new 3 tier breach analysis process has been implemented in the Division.
Tier 1 – Daily review of breaches in the department, picking up key themes and issues
Tier 2 – weekly review of action plans within the Division, incorporating a weekend wash-up meeting
Tier 3 – Formal reporting of key themes using this Operational Performance Report
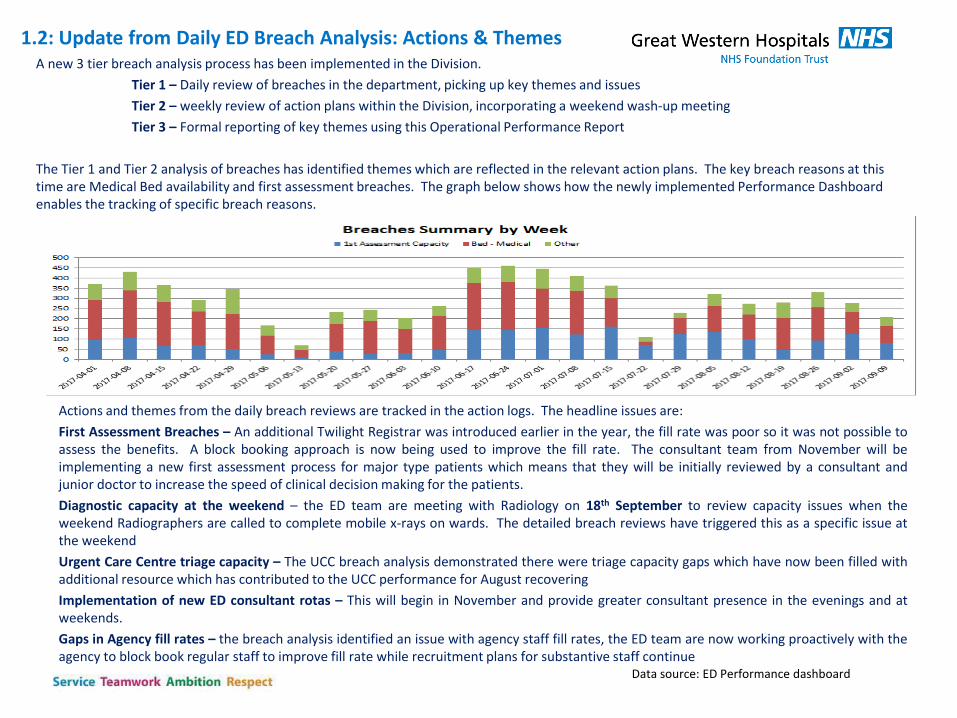
The Tier 1 and Tier 2 analysis of breaches has identified themes which are reflected in the relevant action plans. The key breach reasons at this time are Medical Bed availability and first assessment breaches. The graph below shows how the newly implemented Performance Dashboard enables the tracking of specific breach reasons.
Data source: ED Performance dashboard
Actions and themes from the daily breach reviews are tracked in the action logs. The headline issues are:
First Assessment Breaches – An additional Twilight Registrar was introduced earlier in the year, the fill rate was poor so it was not possible to assess the benefits. A block booking approach is now being used to improve the fill rate. The consultant team from November will be implementing a new first assessment process for major type patients which means that they will be initially reviewed by a consultant and junior doctor to increase the speed of clinical decision making for the patients.
Diagnostic capacity at the weekend – the ED team are meeting with Radiology on 18th September to review capacity issues when the weekend Radiographers are called to complete mobile x-rays on wards. The detailed breach reviews have triggered this as a specific issue at the weekend
Urgent Care Centre triage capacity – The UCC breach analysis demonstrated there were triage capacity gaps which have now been filled with additional resource which has contributed to the UCC performance for August recovering
Implementation of new ED consultant rotas – This will begin in November and provide greater consultant presence in the evenings and at weekends.
Gaps in Agency fill rates – the breach analysis identified an issue with agency staff fill rates, the ED team are now working proactively with the agency to block book regular staff to improve fill rate while recruitment plans for substantive staff continue
1.3 Learning from 12 hour DTA & 12 hour department stay
performance in August = 0 DTA reported
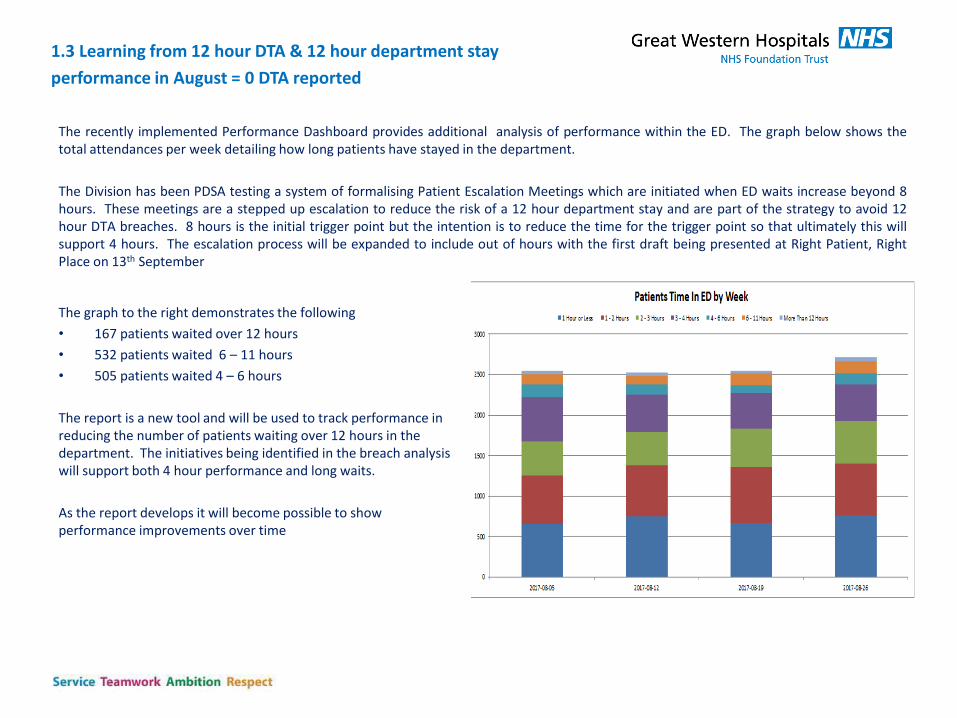
The recently implemented Performance Dashboard provides additional analysis of performance within the ED. The graph below shows the total attendances per week detailing how long patients have stayed in the department.
The Division has been PDSA testing a system of formalising Patient Escalation Meetings which are initiated when ED waits increase beyond 8 hours. These meetings are a stepped up escalation to reduce the risk of a 12 hour department stay and are part of the strategy to avoid 12 hour DTA breaches. 8 hours is the initial trigger point but the intention is to reduce the time for the trigger point so that ultimately this will support 4 hours. The escalation process will be expanded to include out of hours with the first draft being presented at Right Patient, Right Place on 13th September
The graph to the right demonstrates the following
• 167 patients waited over 12 hours
• 532 patients waited 6 – 11 hours
• 505 patients waited 4 – 6 hours
The report is a new tool and will be used to track performance in reducing the number of patients waiting over 12 hours in the department. The initiatives being identified in the breach analysis will support both 4 hour performance and long waits.
As the report develops it will become possible to show performance improvements over time
1.4: Emergency Activity
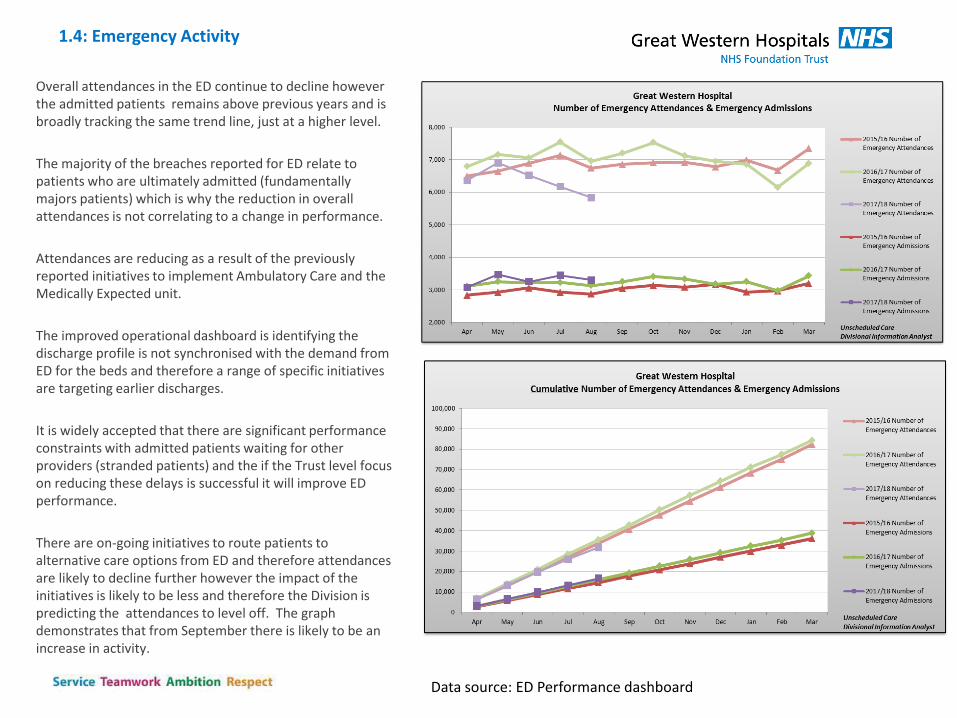
Overall attendances in the ED continue to decline however the admitted patients remains above previous years and is broadly tracking the same trend line, just at a higher level.
The majority of the breaches reported for ED relate to patients who are ultimately admitted (fundamentally majors patients) which is why the reduction in overall attendances is not correlating to a change in performance.
Attendances are reducing as a result of the previously reported initiatives to implement Ambulatory Care and the Medically Expected unit.
The improved operational dashboard is identifying the discharge profile is not synchronised with the demand from ED for the beds and therefore a range of specific initiatives are targeting earlier discharges.
It is widely accepted that there are significant performance constraints with admitted patients waiting for other providers (stranded patients) and the if the Trust level focus on reducing these delays is successful it will improve ED performance.
There are on-going initiatives to route patients to alternative care options from ED and therefore attendances are likely to decline further however the impact of the initiatives is likely to be less and therefore the Division is predicting the attendances to level off. The graph demonstrates that from September there is likely to be an increase in activity.
Data source: ED Performance dashboard
1.5: Streaming update
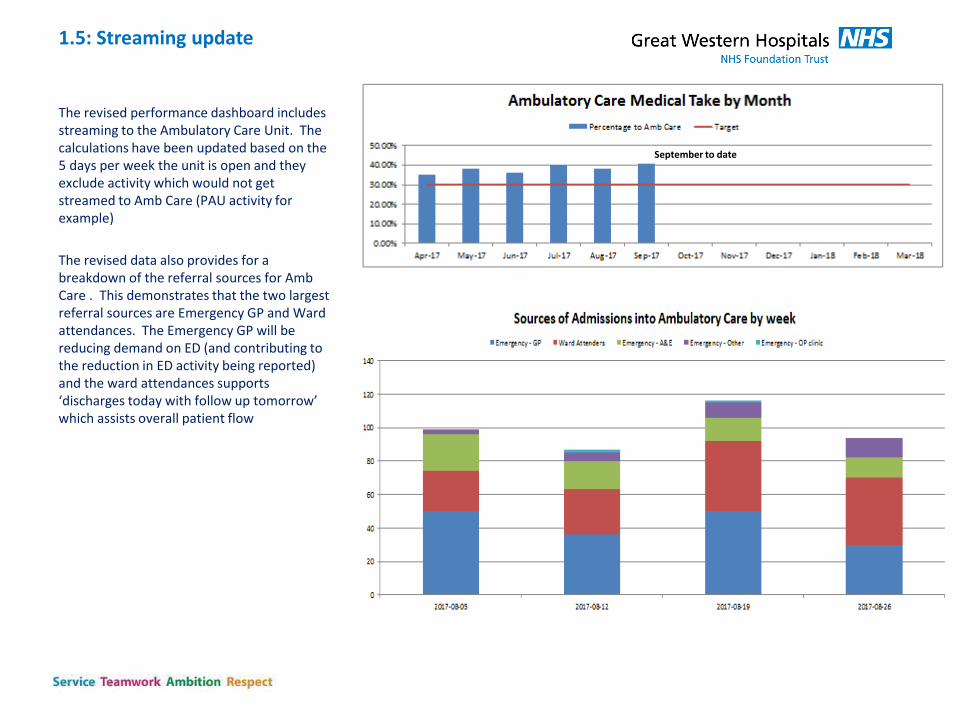
The revised performance dashboard includes streaming to the Ambulatory Care Unit. The calculations have been updated based on the 5 days per week the unit is open and they exclude activity which would not get streamed to Amb Care (PAU activity for example)
The revised data also provides for a breakdown of the referral sources for Amb Care . This demonstrates that the two largest referral sources are Emergency GP and Ward attendances. The Emergency GP will be reducing demand on ED (and contributing to the reduction in ED activity being reported) and the ward attendances supports ‘discharges today with follow up tomorrow’ which assists overall patient flow
September to date
1.6: Ambulance Arrivals - Thirty Minute Handover Performance
Area
2017/18 2017/18
20
17
/18
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Q1 Q2 Q3 Q4
Handovers within 30 minutes (UNVALIDATED) 95.1% 97.0% 96.5% 96.5% 97.9% 96.2% 97.0% 96.6%
Breaches between 30 and 60 minutes 77 50 62 59 37 189 96 258
Breaches greater than 60 minutes 14 7 4 8 4 25 12 37
Total Ambulance Arrivals 1839 1900 1875 1926 1961 5614 3887 9501
0
500
1000
1500
2000
2500
93.5%
94.0%
94.5%
95.0%
95.5%
96.0%
96.5%
97.0%
97.5%
98.0%
98.5%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Handover performance
30 to 60 minute breachers Breaches greater than 60 minutes
Handovers within target Target
Handovers in 30 minutes
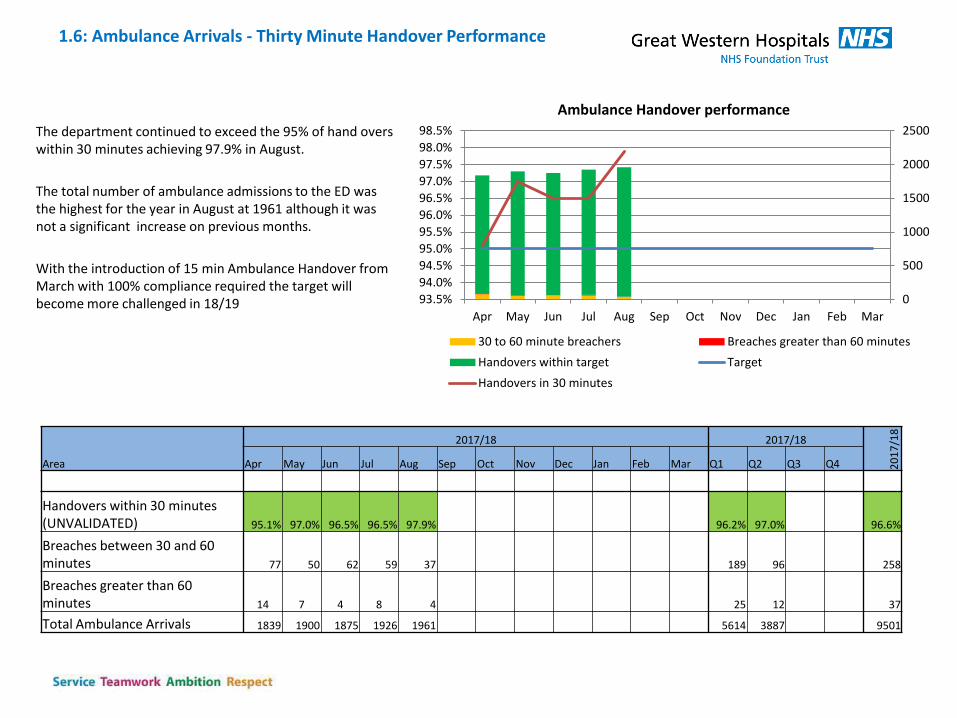
The department continued to exceed the 95% of hand overs within 30 minutes achieving 97.9% in August.
The total number of ambulance admissions to the ED was the highest for the year in August at 1961 although it was not a significant increase on previous months.
With the introduction of 15 min Ambulance Handover from March with 100% compliance required the target will become more challenged in 18/19
Section 2: Right Patient Right Place
2.1 Overview
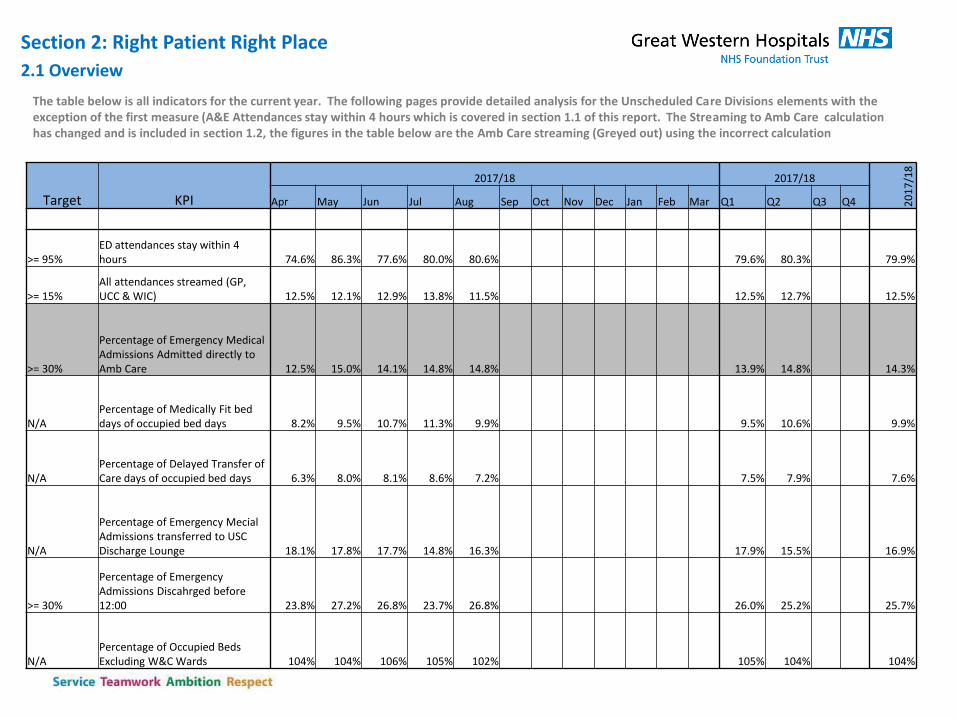
The table below is all indicators for the current year. The following pages provide detailed analysis for the Unscheduled Care Divisions elements with the exception of the first measure (A&E Attendances stay within 4 hours which is covered in section 1.1 of this report. The Streaming to Amb Care calculation has changed and is included in section 1.2, the figures in the table below are the Amb Care streaming (Greyed out) using the incorrect calculation
Target KPI
2017/18 2017/18
20
17
/18
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Q1 Q2 Q3 Q4
>= 95% ED attendances stay within 4 hours 74.6% 86.3% 77.6% 80.0% 80.6% 79.6% 80.3% 79.9%
>= 15% All attendances streamed (GP, UCC & WIC) 12.5% 12.1% 12.9% 13.8% 11.5% 12.5% 12.7% 12.5%
>= 30%
Percentage of Emergency Medical Admissions Admitted directly to Amb Care 12.5% 15.0% 14.1% 14.8% 14.8% 13.9% 14.8% 14.3%
N/A Percentage of Medically Fit bed days of occupied bed days 8.2% 9.5% 10.7% 11.3% 9.9% 9.5% 10.6% 9.9%
N/A Percentage of Delayed Transfer of Care days of occupied bed days 6.3% 8.0% 8.1% 8.6% 7.2% 7.5% 7.9% 7.6%
N/A
Percentage of Emergency Mecial Admissions transferred to USC Discharge Lounge 18.1% 17.8% 17.7% 14.8% 16.3% 17.9% 15.5% 16.9%
>= 30%
Percentage of Emergency Admissions Discahrged before 12:00 23.8% 27.2% 26.8% 23.7% 26.8% 26.0% 25.2% 25.7%
N/A Percentage of Occupied Beds Excluding W&C Wards 104% 104% 106% 105% 102% 105% 104% 104%
2.2 – Emergency Attendances Streamed
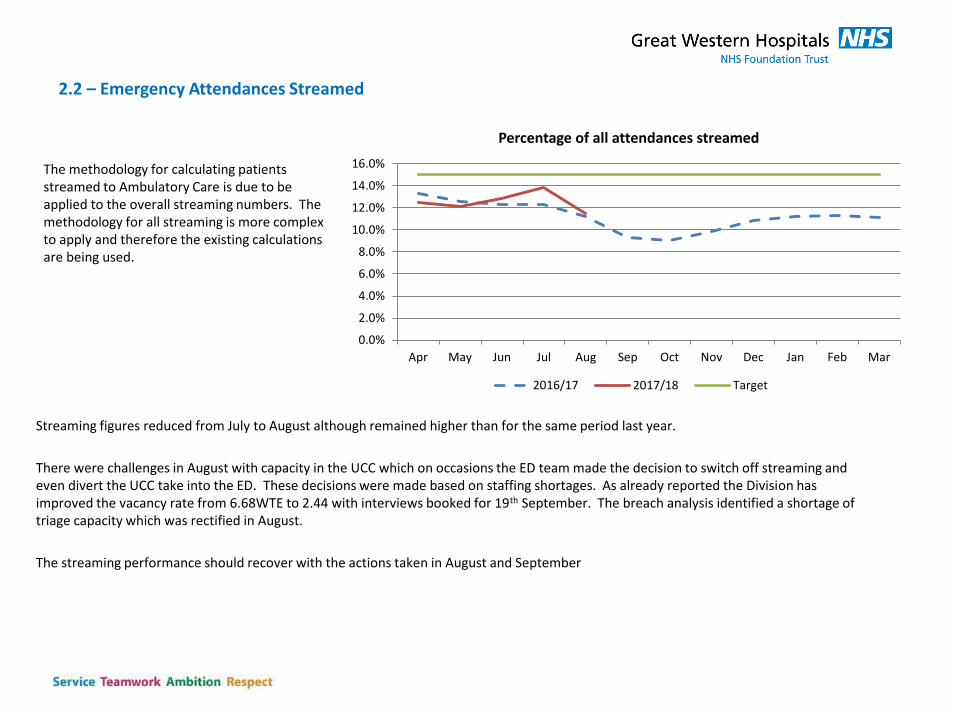
The methodology for calculating patients streamed to Ambulatory Care is due to be applied to the overall streaming numbers. The methodology for all streaming is more complex to apply and therefore the existing calculations are being used.
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage of all attendances streamed
2016/17 2017/18 Target
Streaming figures reduced from July to August although remained higher than for the same period last year.
There were challenges in August with capacity in the UCC which on occasions the ED team made the decision to switch off streaming and even divert the UCC take into the ED. These decisions were made based on staffing shortages. As already reported the Division has improved the vacancy rate from 6.68WTE to 2.44 with interviews booked for 19th September. The breach analysis identified a shortage of triage capacity which was rectified in August.
The streaming performance should recover with the actions taken in August and September
2.3: % of Medical Admissions transferred to the USC Discharge Lounge
Data source: ED Performance dashboard
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of admissions to the Discharge Lounge
2016/17 2017/18
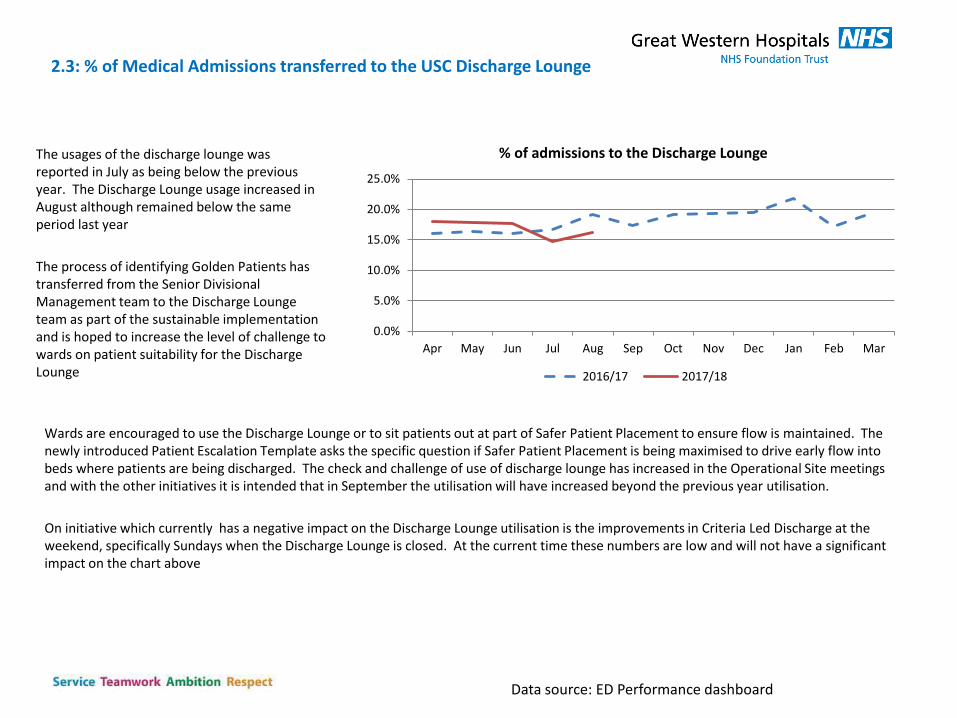
The usages of the discharge lounge was reported in July as being below the previous year. The Discharge Lounge usage increased in August although remained below the same period last year
The process of identifying Golden Patients has transferred from the Senior Divisional Management team to the Discharge Lounge team as part of the sustainable implementation and is hoped to increase the level of challenge to wards on patient suitability for the Discharge Lounge
Wards are encouraged to use the Discharge Lounge or to sit patients out at part of Safer Patient Placement to ensure flow is maintained. The newly introduced Patient Escalation Template asks the specific question if Safer Patient Placement is being maximised to drive early flow into beds where patients are being discharged. The check and challenge of use of discharge lounge has increased in the Operational Site meetings and with the other initiatives it is intended that in September the utilisation will have increased beyond the previous year utilisation.
On initiative which currently has a negative impact on the Discharge Lounge utilisation is the improvements in Criteria Led Discharge at the weekend, specifically Sundays when the Discharge Lounge is closed. At the current time these numbers are low and will not have a significant impact on the chart above
2.4: % of Medical Admissions discharged before midday
Data source: ED Performance dashboard
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of discahrges before midday
2016/17 2017/18 Target
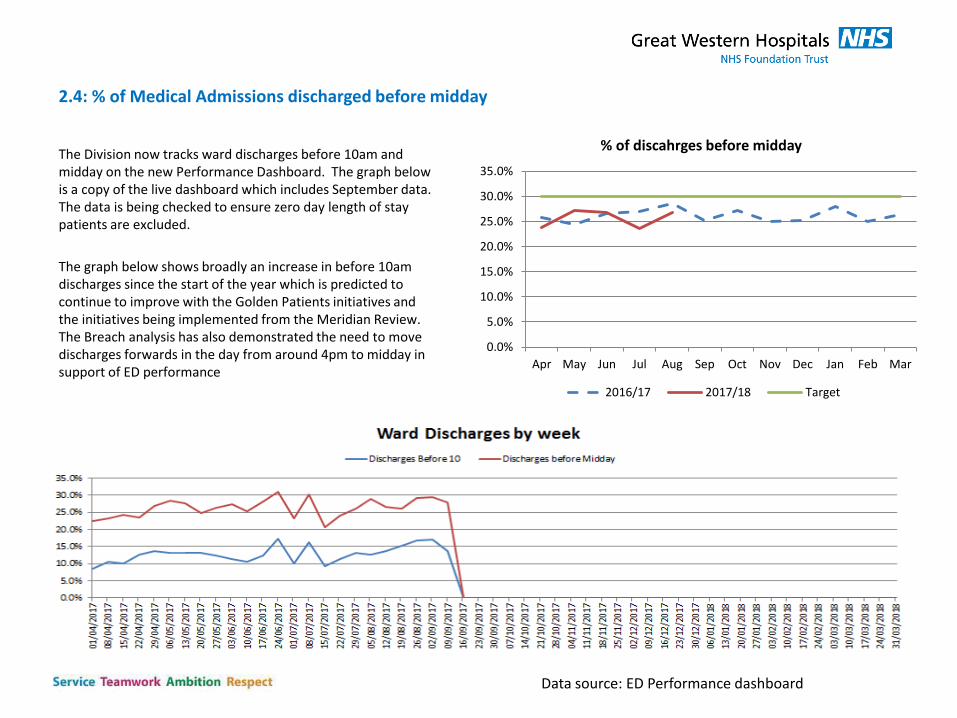
The Division now tracks ward discharges before 10am and midday on the new Performance Dashboard. The graph below is a copy of the live dashboard which includes September data. The data is being checked to ensure zero day length of stay patients are excluded.
The graph below shows broadly an increase in before 10am discharges since the start of the year which is predicted to continue to improve with the Golden Patients initiatives and the initiatives being implemented from the Meridian Review. The Breach analysis has also demonstrated the need to move discharges forwards in the day from around 4pm to midday in support of ED performance
2.5: Length of stay
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
NoN Elective LoS (CIVICA)
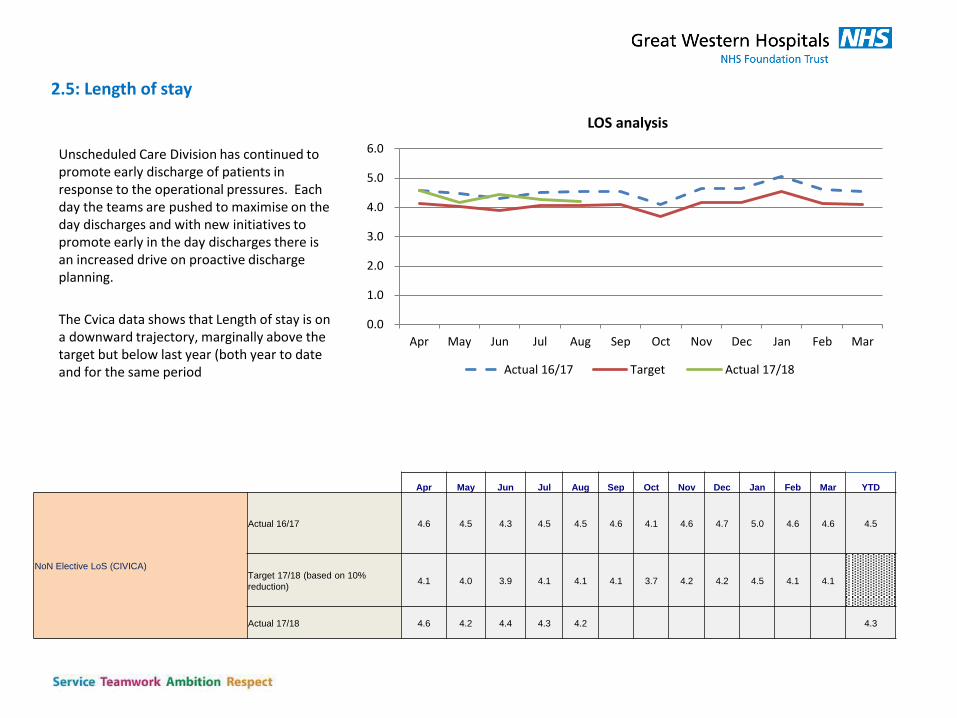
Actual 16/17 4.6 4.5 4.3 4.5 4.5 4.6 4.1 4.6 4.7 5.0 4.6 4.6 4.5
Target 17/18 (based on 10%
reduction) 4.1 4.0 3.9 4.1 4.1 4.1 3.7 4.2 4.2 4.5 4.1 4.1
Actual 17/18 4.6 4.2 4.4 4.3 4.2 4.3
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
LOS analysis
Actual 16/17 Target Actual 17/18
Unscheduled Care Division has continued to promote early discharge of patients in response to the operational pressures. Each day the teams are pushed to maximise on the day discharges and with new initiatives to promote early in the day discharges there is an increased drive on proactive discharge planning.
The Cvica data shows that Length of stay is on a downward trajectory, marginally above the target but below last year (both year to date and for the same period
2.6 Clinically owned targets / refresh of IPS
• IPS position agreed – Sign off Divisional Consultant Meeting (15th September) prior to RPRP
• Examples of the IPS agreed in principle
• Beds on Base Wards filled by 20:00
• Patients must be seen by a Doctor/practitioner within 1 hour of arrival within the ED
• Decision to refer/admit/discharge should have been made within 2.5 hours within the ED
• All patients to have left the department within 4 hours
• EDS by 15:00 prior day
• TTA by 17:00 for next day
• Definite discharge transferred to Discharge Lounge or sat out within 1 hour
• Maximum LOS on the Acute Medical Unit will be 24 hours
• Proforma for Clinical Criteria for Discharge completed on the Friday
• IPS measures have been assessed if a KPI can be system generated or if an audit is required for assurance.
• System generated KPI’s will be added to the operational performance dashboard
• Audit generated KPI’s will be produced by a range of teams, capitalising on existing audits where possible
• The IPS cut across a range of existing monitoring tools. Individual departments will have access to their own performance however a summary dashboard will be developed to provide clear oversight
9
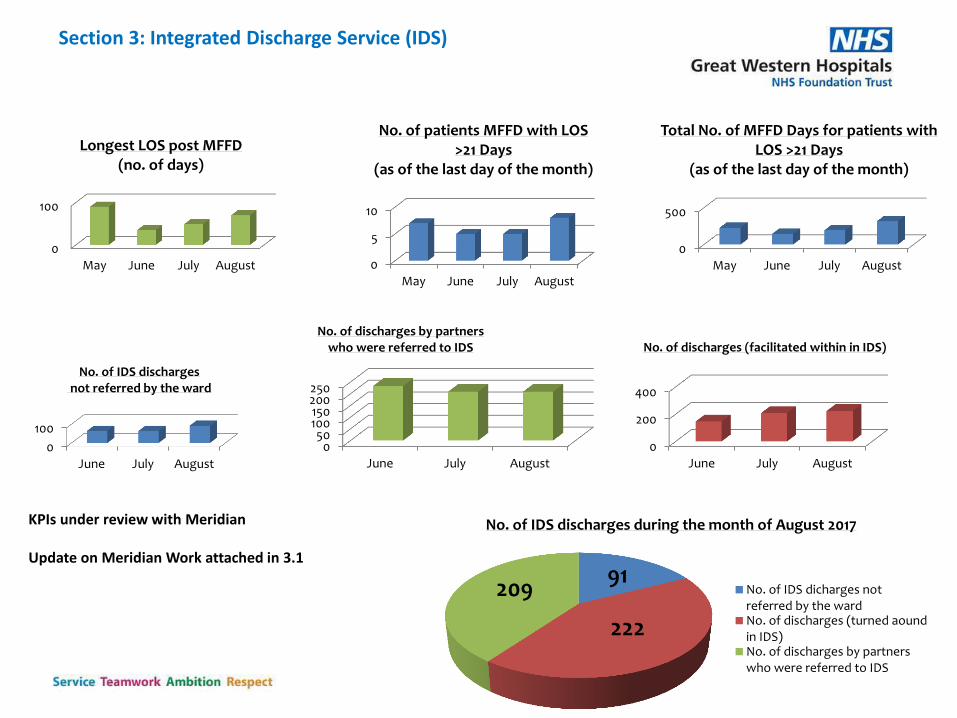
Section 3: Integrated Discharge Service (IDS)
KPIs under review with Meridian Update on Meridian Work attached in 3.1
No. of IDS discharges during the month of August 2017
No. of IDS dicharges notreferred by the wardNo. of discharges (turned aoundin IDS)No. of discharges by partnerswho were referred to IDS
91
222
209
0
500
May June July August
Total No. of MFFD Days for patients with LOS >21 Days
(as of the last day of the month)
0
200
400
June July August
No. of discharges (facilitated within in IDS)
0
100
June July August
No. of IDS discharges not referred by the ward
050
100150200250
June July August
No. of discharges by partners who were referred to IDS
0
5
10
May June July August
No. of patients MFFD with LOS >21 Days
(as of the last day of the month)
0
100
May June July August
Longest LOS post MFFD (no. of days)
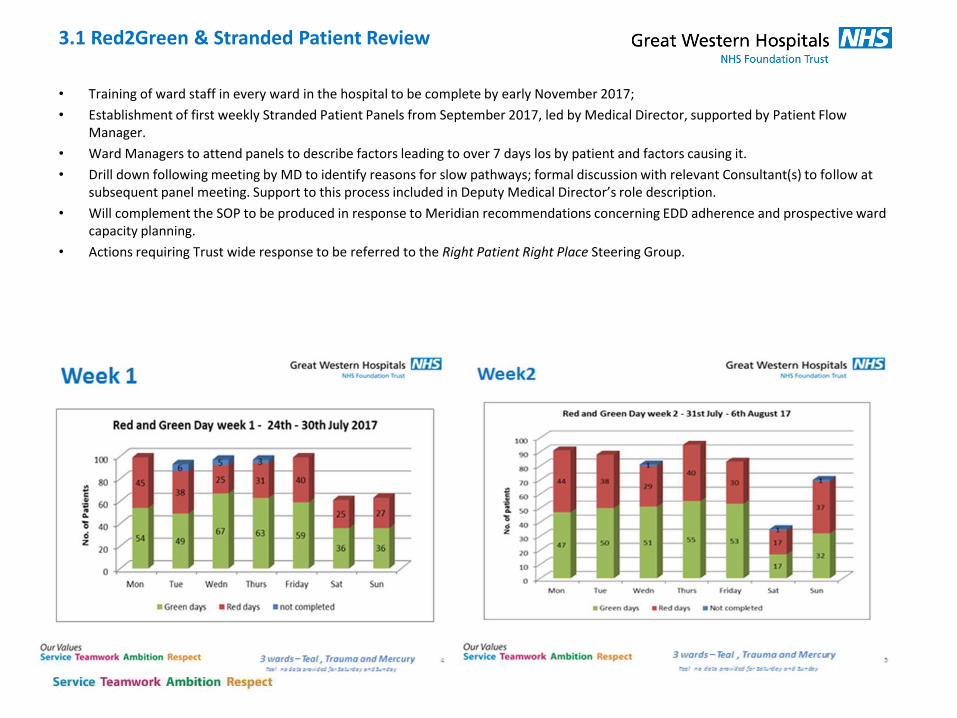
• Training of ward staff in every ward in the hospital to be complete by early November 2017;
• Establishment of first weekly Stranded Patient Panels from September 2017, led by Medical Director, supported by Patient Flow Manager.
• Ward Managers to attend panels to describe factors leading to over 7 days los by patient and factors causing it.
• Drill down following meeting by MD to identify reasons for slow pathways; formal discussion with relevant Consultant(s) to follow at subsequent panel meeting. Support to this process included in Deputy Medical Director’s role description.
• Will complement the SOP to be produced in response to Meridian recommendations concerning EDD adherence and prospective ward capacity planning.
• Actions requiring Trust wide response to be referred to the Right Patient Right Place Steering Group.
3.1 Red2Green & Stranded Patient Review
12
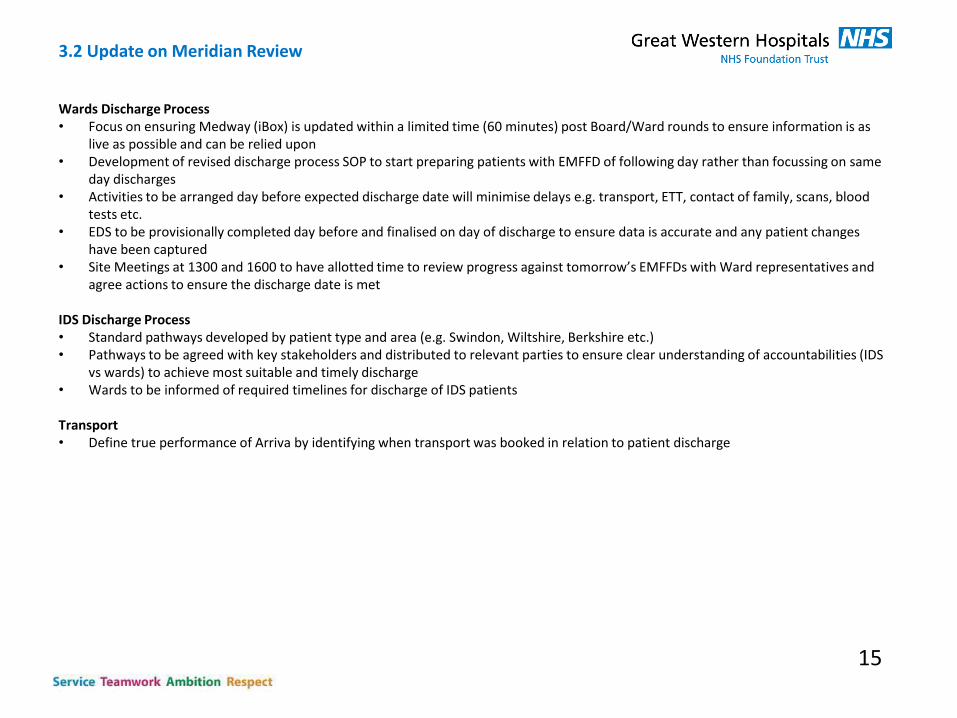
3.2 Update on Meridian Review
Wards Discharge Process • Focus on ensuring Medway (iBox) is updated within a limited time (60 minutes) post Board/Ward rounds to ensure information is as
live as possible and can be relied upon • Development of revised discharge process SOP to start preparing patients with EMFFD of following day rather than focussing on same
day discharges • Activities to be arranged day before expected discharge date will minimise delays e.g. transport, ETT, contact of family, scans, blood
tests etc. • EDS to be provisionally completed day before and finalised on day of discharge to ensure data is accurate and any patient changes
have been captured • Site Meetings at 1300 and 1600 to have allotted time to review progress against tomorrow’s EMFFDs with Ward representatives and
agree actions to ensure the discharge date is met
IDS Discharge Process • Standard pathways developed by patient type and area (e.g. Swindon, Wiltshire, Berkshire etc.) • Pathways to be agreed with key stakeholders and distributed to relevant parties to ensure clear understanding of accountabilities (IDS
vs wards) to achieve most suitable and timely discharge • Wards to be informed of required timelines for discharge of IDS patients
Transport • Define true performance of Arriva by identifying when transport was booked in relation to patient discharge
15
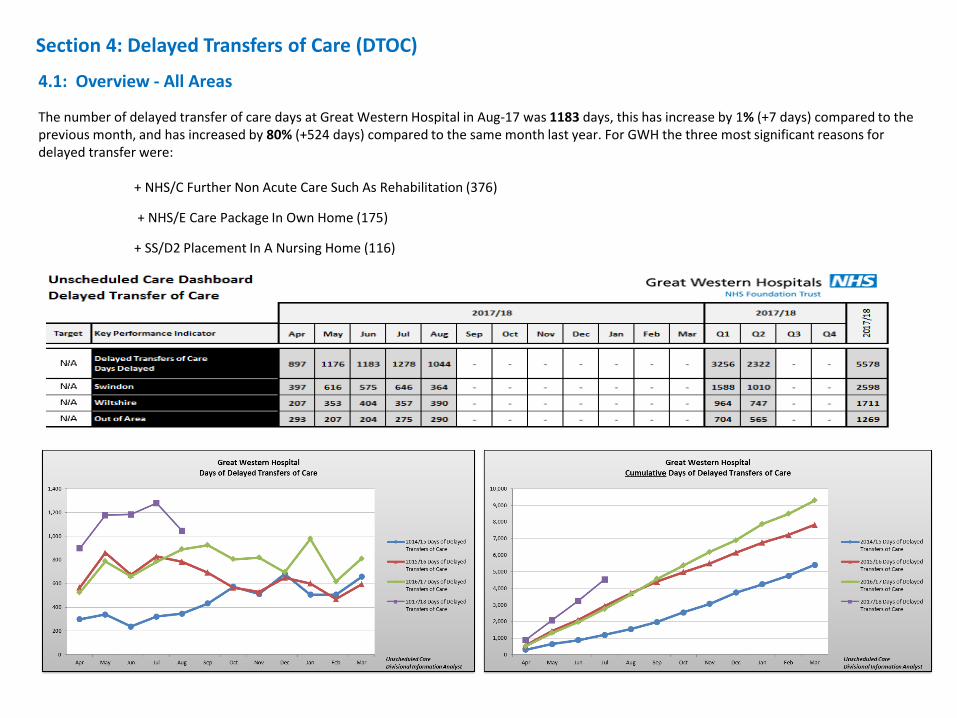
Section 4: Delayed Transfers of Care (DTOC)
4.1: Overview - All Areas
The number of delayed transfer of care days at Great Western Hospital in Aug-17 was 1183 days, this has increase by 1% (+7 days) compared to the previous month, and has increased by 80% (+524 days) compared to the same month last year. For GWH the three most significant reasons for delayed transfer were: + NHS/C Further Non Acute Care Such As Rehabilitation (376)
+ NHS/E Care Package In Own Home (175)
+ SS/D2 Placement In A Nursing Home (116)
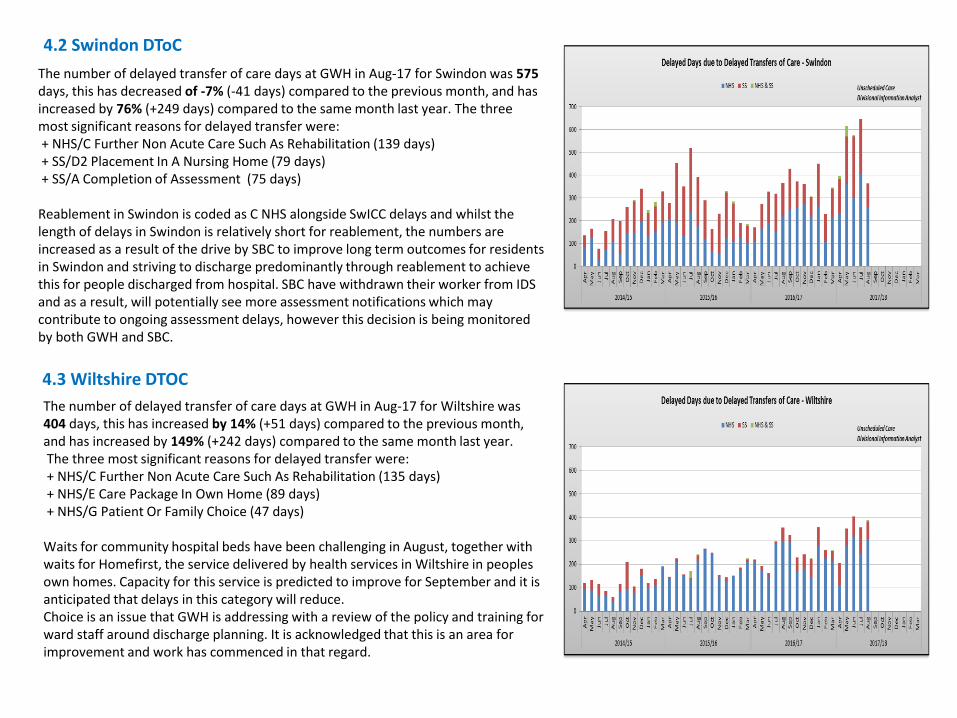
4.2 Swindon DToC
The number of delayed transfer of care days at GWH in Aug-17 for Swindon was 575 days, this has decreased of -7% (-41 days) compared to the previous month, and has increased by 76% (+249 days) compared to the same month last year. The three most significant reasons for delayed transfer were: + NHS/C Further Non Acute Care Such As Rehabilitation (139 days) + SS/D2 Placement In A Nursing Home (79 days) + SS/A Completion of Assessment (75 days) Reablement in Swindon is coded as C NHS alongside SwICC delays and whilst the length of delays in Swindon is relatively short for reablement, the numbers are increased as a result of the drive by SBC to improve long term outcomes for residents in Swindon and striving to discharge predominantly through reablement to achieve this for people discharged from hospital. SBC have withdrawn their worker from IDS and as a result, will potentially see more assessment notifications which may contribute to ongoing assessment delays, however this decision is being monitored by both GWH and SBC.
4.3 Wiltshire DTOC
The number of delayed transfer of care days at GWH in Aug-17 for Wiltshire was 404 days, this has increased by 14% (+51 days) compared to the previous month, and has increased by 149% (+242 days) compared to the same month last year. The three most significant reasons for delayed transfer were: + NHS/C Further Non Acute Care Such As Rehabilitation (135 days) + NHS/E Care Package In Own Home (89 days) + NHS/G Patient Or Family Choice (47 days) Waits for community hospital beds have been challenging in August, together with waits for Homefirst, the service delivered by health services in Wiltshire in peoples own homes. Capacity for this service is predicted to improve for September and it is anticipated that delays in this category will reduce. Choice is an issue that GWH is addressing with a review of the policy and training for ward staff around discharge planning. It is acknowledged that this is an area for improvement and work has commenced in that regard.
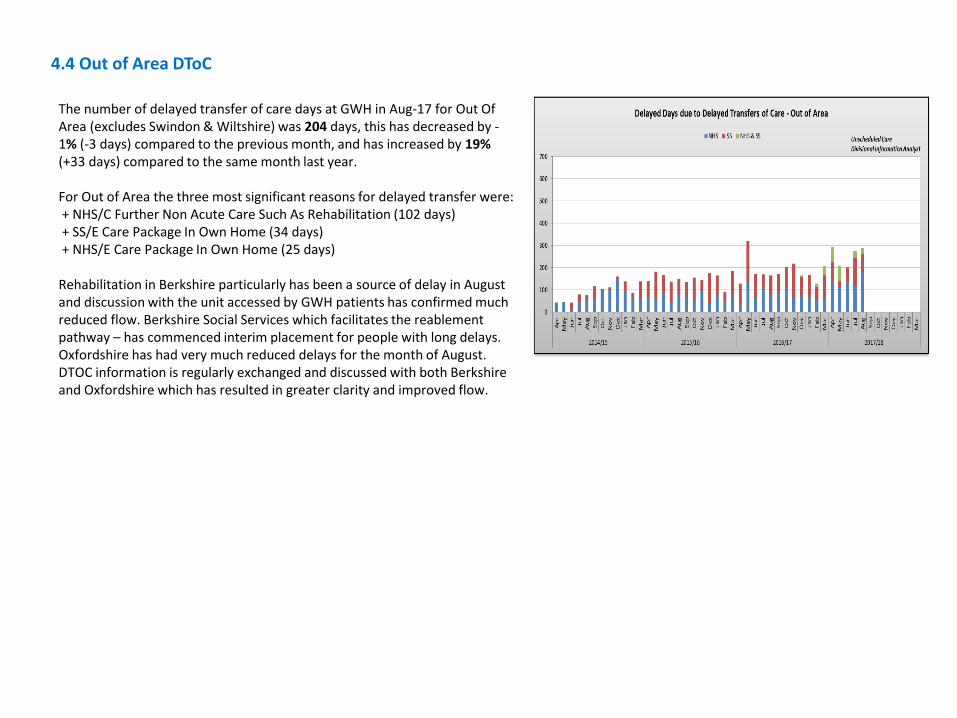
4.4 Out of Area DToC
The number of delayed transfer of care days at GWH in Aug-17 for Out Of Area (excludes Swindon & Wiltshire) was 204 days, this has decreased by -1% (-3 days) compared to the previous month, and has increased by 19% (+33 days) compared to the same month last year. For Out of Area the three most significant reasons for delayed transfer were: + NHS/C Further Non Acute Care Such As Rehabilitation (102 days) + SS/E Care Package In Own Home (34 days) + NHS/E Care Package In Own Home (25 days) Rehabilitation in Berkshire particularly has been a source of delay in August and discussion with the unit accessed by GWH patients has confirmed much reduced flow. Berkshire Social Services which facilitates the reablement pathway – has commenced interim placement for people with long delays. Oxfordshire has had very much reduced delays for the month of August. DTOC information is regularly exchanged and discussed with both Berkshire and Oxfordshire which has resulted in greater clarity and improved flow.
Section 5 : Night Moves
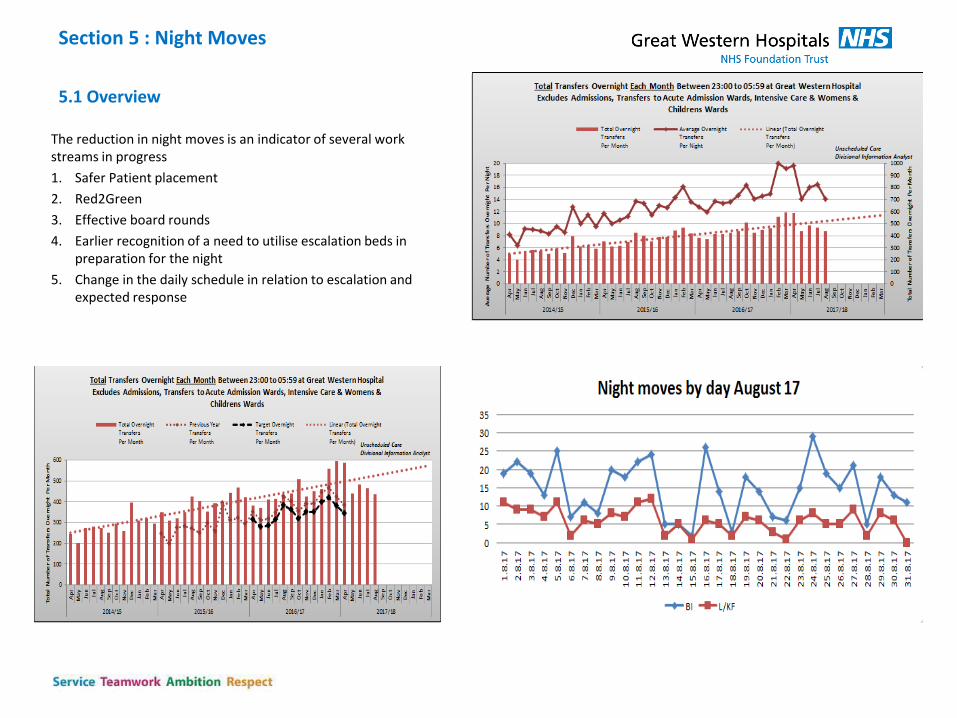
5.1 Overview
The reduction in night moves is an indicator of several work streams in progress
1. Safer Patient placement
2. Red2Green
3. Effective board rounds
4. Earlier recognition of a need to utilise escalation beds in preparation for the night
5. Change in the daily schedule in relation to escalation and expected response
5.2 Night Moves Themes and Trends
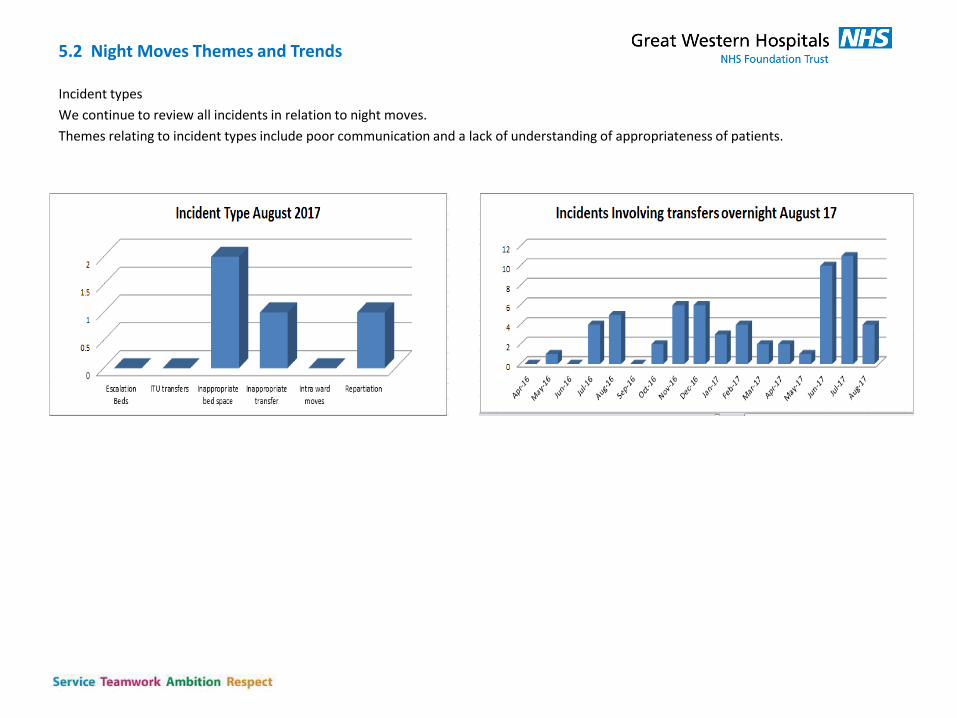
Incident types
We continue to review all incidents in relation to night moves.
Themes relating to incident types include poor communication and a lack of understanding of appropriateness of patients.
Data up to end of August 2017
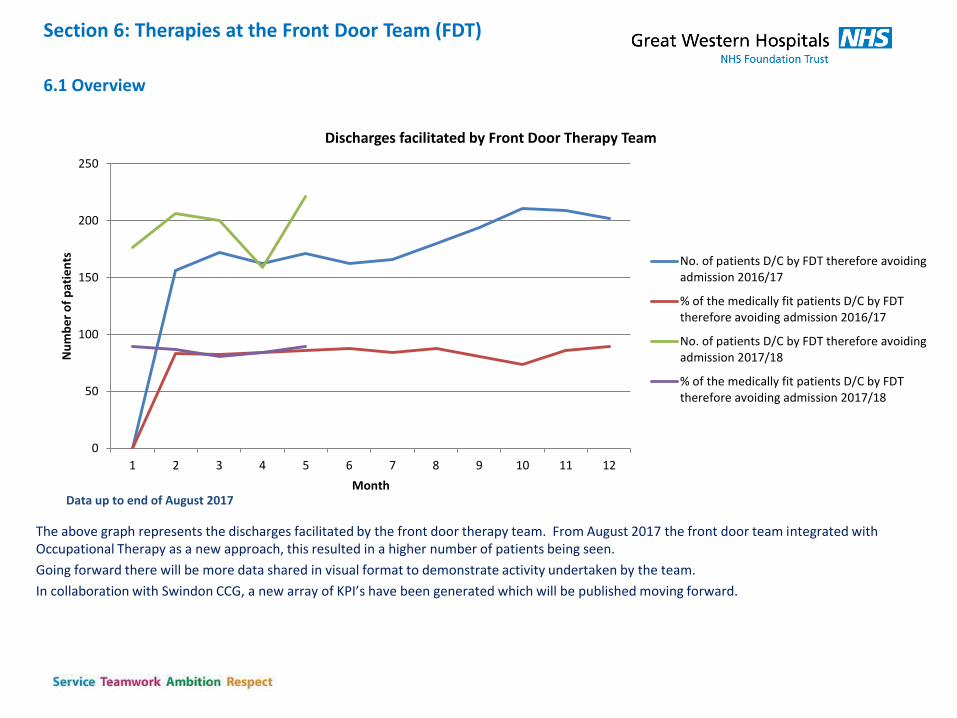
The above graph represents the discharges facilitated by the front door therapy team. From August 2017 the front door team integrated with Occupational Therapy as a new approach, this resulted in a higher number of patients being seen.
Going forward there will be more data shared in visual format to demonstrate activity undertaken by the team.
In collaboration with Swindon CCG, a new array of KPI’s have been generated which will be published moving forward.
0
50
100
150
200
250
1 2 3 4 5 6 7 8 9 10 11 12
Nu
mb
er
of
pat
ien
ts
Month
Discharges facilitated by Front Door Therapy Team
No. of patients D/C by FDT therefore avoidingadmission 2016/17
% of the medically fit patients D/C by FDTtherefore avoiding admission 2016/17
No. of patients D/C by FDT therefore avoidingadmission 2017/18
% of the medically fit patients D/C by FDTtherefore avoiding admission 2017/18
Section 6: Therapies at the Front Door Team (FDT)
6.1 Overview
The KPI’s have now been streamlined with Swindon CCG colleagues and sign up from Wiltshire CCG is progressing. The new KPI’s focus on outcomes measured for discharge and the barriers to the discharge happening (this will follow in September as the data set had to change in order to capture this).
The revised KPI’s are below -
Addition of WTE working per day to indicate productivity and contact per clinician per day (data in September 17)
Addition of length of time taken to be assessment and discharged by FDT. (data in September 17)
Admissions avoided at front door due to intervention – in the previous slide
KPI’s August
85% of Medically fit patients are discharged by FDT August = 89% - 221 patients discharged
Outcomes:
88% discharged to usual place of residence,
6% SWICC, 5% Community hospital, 1% Out of area Community
The admissions due to reduced capacity of services will be reported in Sept 17
Additional Information to accompany KPI’s
Reasons for medically fit patients being admitted and the reason why
Staffing
As of September 2017 there will be the vacancy factor from a Physio perspective filled – this is the 0.5 which has been highlighted for many months.
6.2: Therapies at the Front Door (FDT) - KPIs
Section 7: Stroke Performance
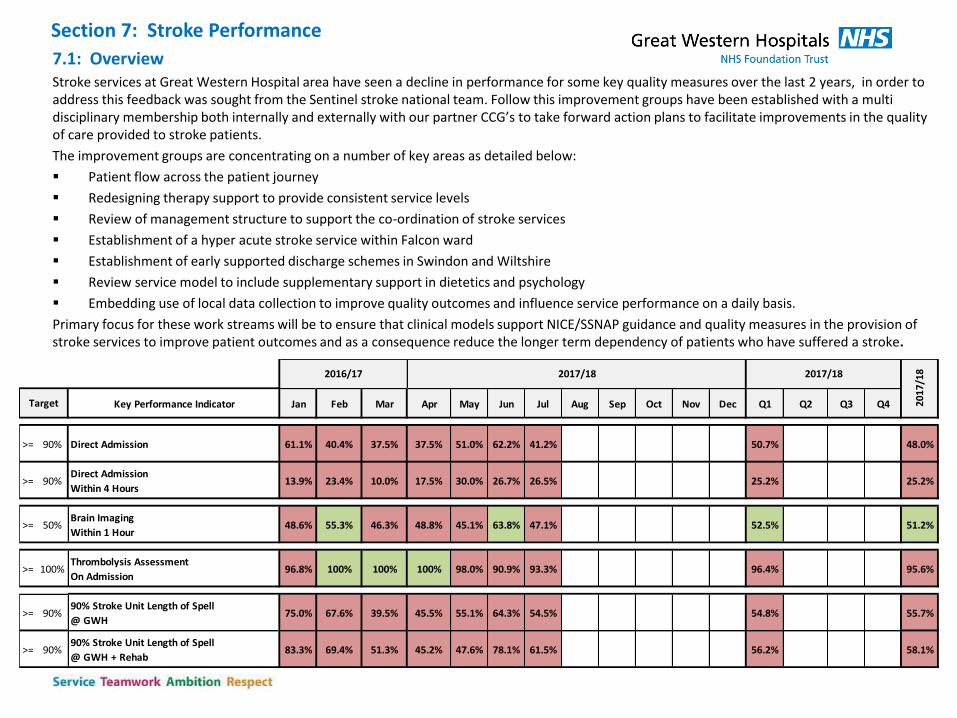
7.1: Overview Stroke services at Great Western Hospital area have seen a decline in performance for some key quality measures over the last 2 years, in order to address this feedback was sought from the Sentinel stroke national team. Follow this improvement groups have been established with a multi disciplinary membership both internally and externally with our partner CCG’s to take forward action plans to facilitate improvements in the quality of care provided to stroke patients.
The improvement groups are concentrating on a number of key areas as detailed below:
Patient flow across the patient journey
Redesigning therapy support to provide consistent service levels
Review of management structure to support the co-ordination of stroke services
Establishment of a hyper acute stroke service within Falcon ward
Establishment of early supported discharge schemes in Swindon and Wiltshire
Review service model to include supplementary support in dietetics and psychology
Embedding use of local data collection to improve quality outcomes and influence service performance on a daily basis.
Primary focus for these work streams will be to ensure that clinical models support NICE/SSNAP guidance and quality measures in the provision of stroke services to improve patient outcomes and as a consequence reduce the longer term dependency of patients who have suffered a stroke.
Key Performance Indicator Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Q1 Q2 Q3 Q4
>= 90% Direct Admission 61.1% 40.4% 37.5% 37.5% 51.0% 62.2% 41.2% 50.7% 48.0%
>= 90%Direct Admission
Within 4 Hours13.9% 23.4% 10.0% 17.5% 30.0% 26.7% 26.5% 25.2% 25.2%
>= 50%Brain Imaging
Within 1 Hour48.6% 55.3% 46.3% 48.8% 45.1% 63.8% 47.1% 52.5% 51.2%
>= 100%Thrombolysis Assessment
On Admission96.8% 100% 100% 100% 98.0% 90.9% 93.3% 96.4% 95.6%
>= 90%90% Stroke Unit Length of Spell
@ GWH75.0% 67.6% 39.5% 45.5% 55.1% 64.3% 54.5% 54.8% 55.7%
>= 90%90% Stroke Unit Length of Spell
@ GWH + Rehab83.3% 69.4% 51.3% 45.2% 47.6% 78.1% 61.5% 56.2% 58.1%
2017/18
2017
/18
Target
2016/17 2017/18
7.2 Stroke KPI – Brain Imaging
30%
40%
50%
60%
70%
80%
90%
100%
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
Dec
-16
Pe
rce
nta
ge
Admission Month
Brain Imaging for Stroke, Within 1 Hour & Within 12 Hours
Target = 50% Brain ImagingWithin 1 Hour
Linear (Brain ImagingWithin 1 Hour)
Key Performance Indicator Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Q1 Q2 Q3 Q4
>= 50%B rain Imaging
Within 1 H o ur48.6% 55.3% 46.3% 48.8% 45.1% 63.8% 47.1% 52.5% 51.2%
2017/18
20
17
/18
Target
2016/17 2017/18
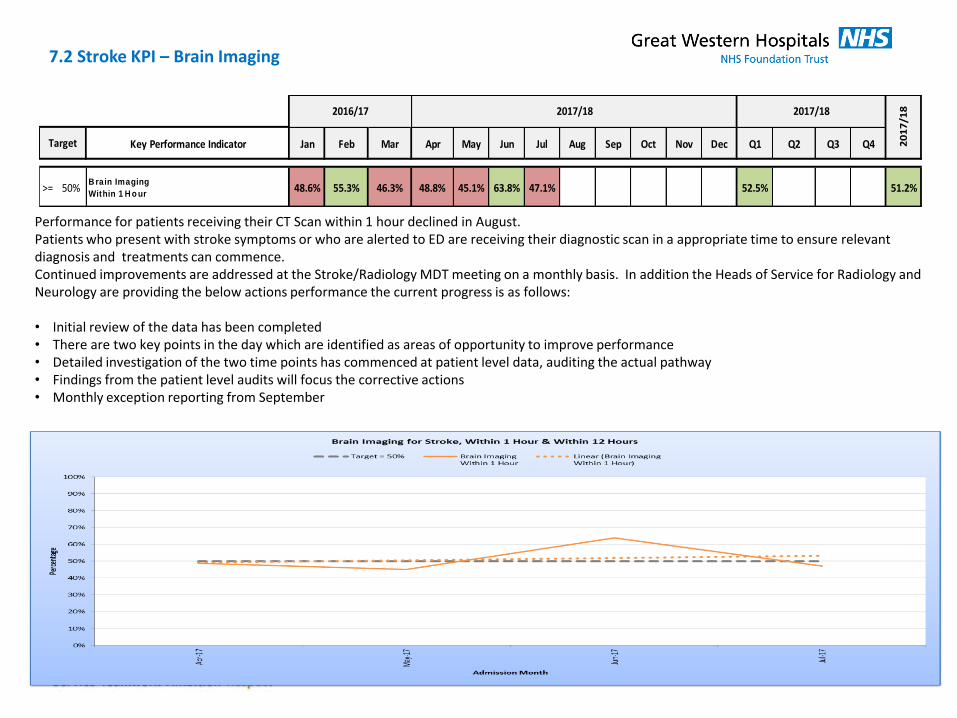
Performance for patients receiving their CT Scan within 1 hour declined in August. Patients who present with stroke symptoms or who are alerted to ED are receiving their diagnostic scan in a appropriate time to ensure relevant diagnosis and treatments can commence. Continued improvements are addressed at the Stroke/Radiology MDT meeting on a monthly basis. In addition the Heads of Service for Radiology and Neurology are providing the below actions performance the current progress is as follows: • Initial review of the data has been completed • There are two key points in the day which are identified as areas of opportunity to improve performance • Detailed investigation of the two time points has commenced at patient level data, auditing the actual pathway • Findings from the patient level audits will focus the corrective actions • Monthly exception reporting from September
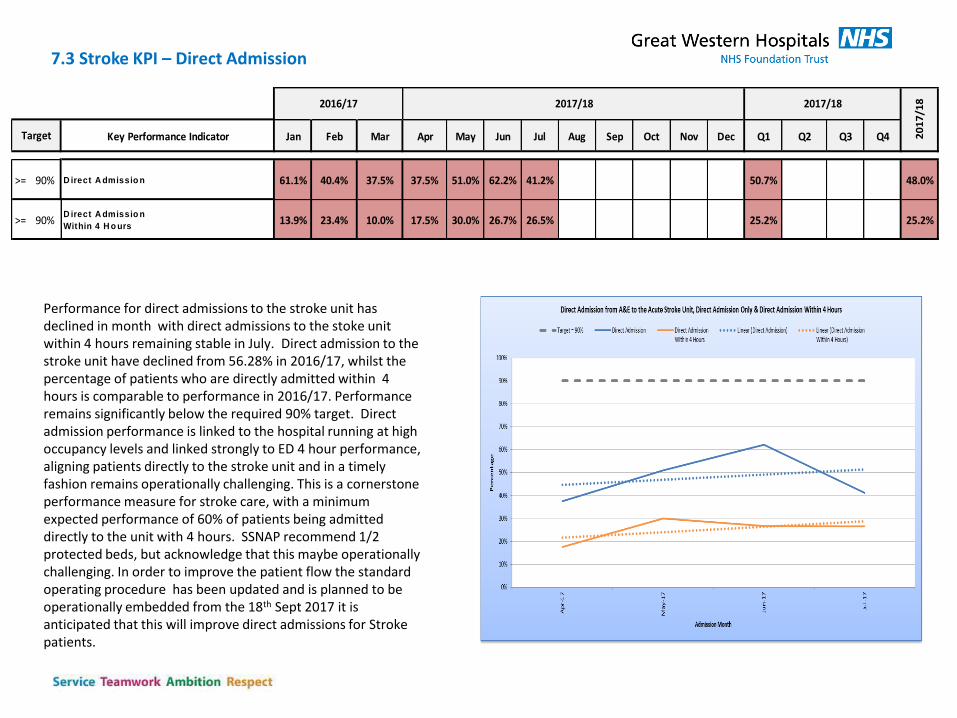
Performance for direct admissions to the stroke unit has declined in month with direct admissions to the stoke unit within 4 hours remaining stable in July. Direct admission to the stroke unit have declined from 56.28% in 2016/17, whilst the percentage of patients who are directly admitted within 4 hours is comparable to performance in 2016/17. Performance remains significantly below the required 90% target. Direct admission performance is linked to the hospital running at high occupancy levels and linked strongly to ED 4 hour performance, aligning patients directly to the stroke unit and in a timely fashion remains operationally challenging. This is a cornerstone performance measure for stroke care, with a minimum expected performance of 60% of patients being admitted directly to the unit with 4 hours. SSNAP recommend 1/2 protected beds, but acknowledge that this maybe operationally challenging. In order to improve the patient flow the standard operating procedure has been updated and is planned to be operationally embedded from the 18th Sept 2017 it is anticipated that this will improve direct admissions for Stroke patients.
7.3 Stroke KPI – Direct Admission
Key Performance Indicator Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Q1 Q2 Q3 Q4
>= 90% D irect A dmissio n 61.1% 40.4% 37.5% 37.5% 51.0% 62.2% 41.2% 50.7% 48.0%
>= 90%D irect A dmissio n
Within 4 H o urs13.9% 23.4% 10.0% 17.5% 30.0% 26.7% 26.5% 25.2% 25.2%
2017/18
20
17
/18
Target
2016/17 2017/18
7.4 Stroke KPI – Length of Stay on the Stroke Unit
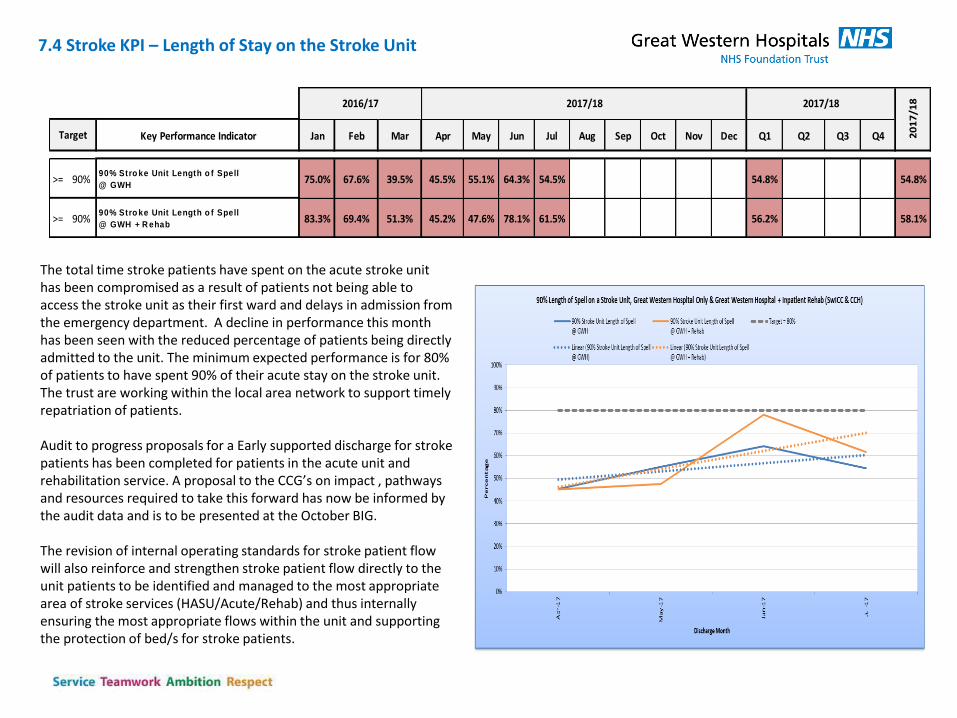
The total time stroke patients have spent on the acute stroke unit has been compromised as a result of patients not being able to access the stroke unit as their first ward and delays in admission from the emergency department. A decline in performance this month has been seen with the reduced percentage of patients being directly admitted to the unit. The minimum expected performance is for 80% of patients to have spent 90% of their acute stay on the stroke unit. The trust are working within the local area network to support timely repatriation of patients. Audit to progress proposals for a Early supported discharge for stroke patients has been completed for patients in the acute unit and rehabilitation service. A proposal to the CCG’s on impact , pathways and resources required to take this forward has now be informed by the audit data and is to be presented at the October BIG. The revision of internal operating standards for stroke patient flow will also reinforce and strengthen stroke patient flow directly to the unit patients to be identified and managed to the most appropriate area of stroke services (HASU/Acute/Rehab) and thus internally ensuring the most appropriate flows within the unit and supporting the protection of bed/s for stroke patients.
Key Performance Indicator Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Q1 Q2 Q3 Q4
>= 90%90% Stro ke Unit Length o f Spell
@ GWH75.0% 67.6% 39.5% 45.5% 55.1% 64.3% 54.5% 54.8% 54.8%
>= 90%90% Stro ke Unit Length o f Spell
@ GWH + R ehab83.3% 69.4% 51.3% 45.2% 47.6% 78.1% 61.5% 56.2% 58.1%
2016/17 2017/18 2017/18
20
17
/18
Target
Section 8: RTT
8.1: RTT
8.2: 52 Week Breaches
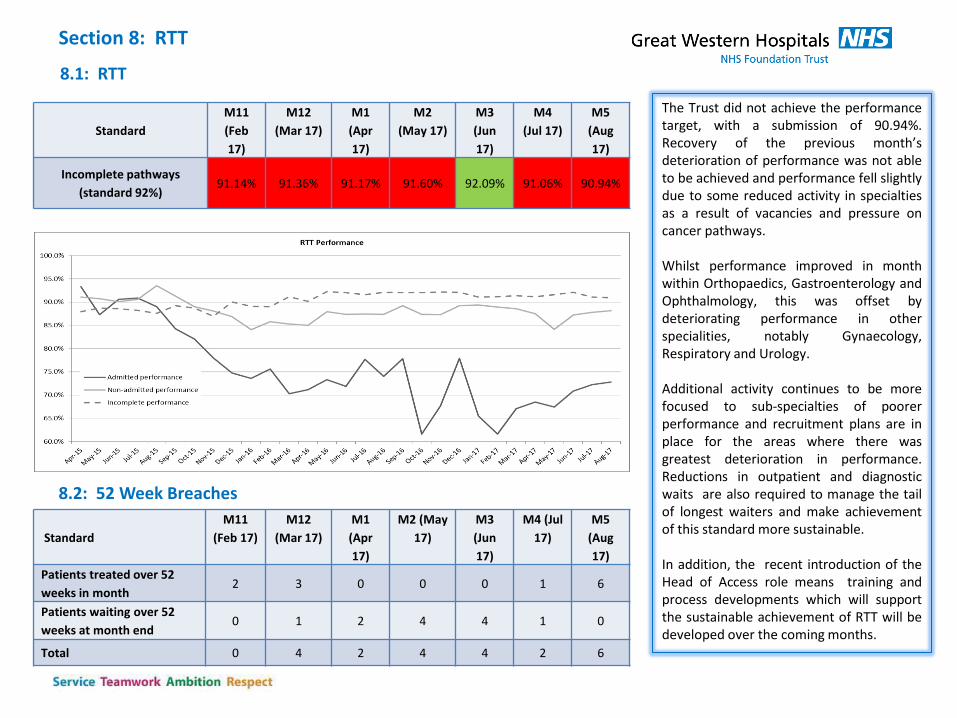
The Trust did not achieve the performance target, with a submission of 90.94%. Recovery of the previous month’s deterioration of performance was not able to be achieved and performance fell slightly due to some reduced activity in specialties as a result of vacancies and pressure on cancer pathways. Whilst performance improved in month within Orthopaedics, Gastroenterology and Ophthalmology, this was offset by deteriorating performance in other specialities, notably Gynaecology, Respiratory and Urology. Additional activity continues to be more focused to sub-specialties of poorer performance and recruitment plans are in place for the areas where there was greatest deterioration in performance. Reductions in outpatient and diagnostic waits are also required to manage the tail of longest waiters and make achievement of this standard more sustainable. In addition, the recent introduction of the Head of Access role means training and process developments which will support the sustainable achievement of RTT will be developed over the coming months.
Standard
M11
(Feb
17)
M12
(Mar 17)
M1
(Apr
17)
M2
(May 17)
M3
(Jun
17)
M4
(Jul 17)
M5
(Aug
17)
Incomplete pathways
(standard 92%) 91.14% 91.36% 91.17% 91.60% 92.09% 91.06% 90.94%
Standard
M11
(Feb 17)
M12
(Mar 17)
M1
(Apr
17)
M2 (May
17)
M3
(Jun
17)
M4 (Jul
17)
M5
(Aug
17)
Patients treated over 52
weeks in month 2 3 0 0 0 1 6
Patients waiting over 52
weeks at month end 0 1 2 4 4 1 0
Total 0 4 2 4 4 2 6
8.3: Longest waiting RTT patients
• There were no 52 week breaching patient submitted in the August incomplete submission. • The previously reported issue with General Surgery patients who had been incorrectly discharged when booked for an endoscopy procedure,
which has led to a number of 52 week breaches, is in the final stage of investigation. A cohort of 1788 patients who could have been affected by the issue have now been administratively validated. It was predicted that this would result in around 15-20 patients waiting longer than 52 weeks, however initial validation has demonstrated that the impact will be lower than anticipated. Clinical validation of the remaining patients who could be affected is now taking place which will confirm the number of long waiting patients who should still be on a live pathway. Plans for any long waiting patients will be put in place rapidly over the next month.
• Although patients within other specialities have not been identified as having waited over 52 weeks as a result of this issue, it is recommended that this validation exercise is rolled out to all specialties with an endoscopy pathway. The risk of this uncovering long waiting patients who should still be on a live pathway is felt to be lower than in General Surgery however is a possibility. The scale of this piece of work is currently being quantified in order to provide realistic timeframes for completion.
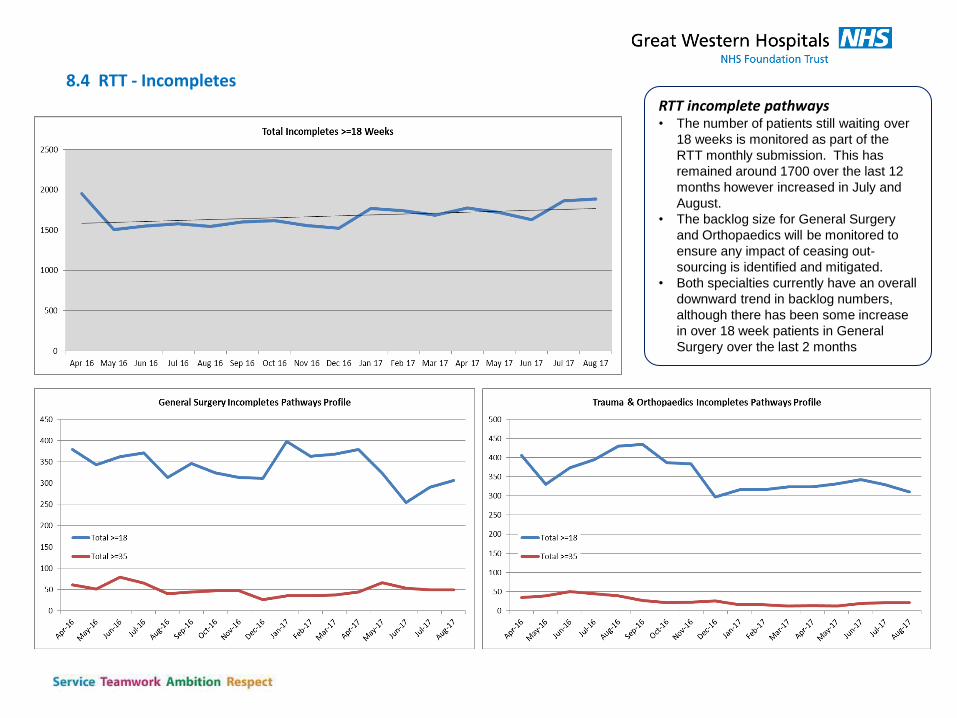
8.4 RTT - Incompletes
RTT incomplete pathways • The number of patients still waiting over
18 weeks is monitored as part of the
RTT monthly submission. This has
remained around 1700 over the last 12
months however increased in July and
August.
• The backlog size for General Surgery
and Orthopaedics will be monitored to
ensure any impact of ceasing out-
sourcing is identified and mitigated.
• Both specialties currently have an overall
downward trend in backlog numbers,
although there has been some increase
in over 18 week patients in General
Surgery over the last 2 months
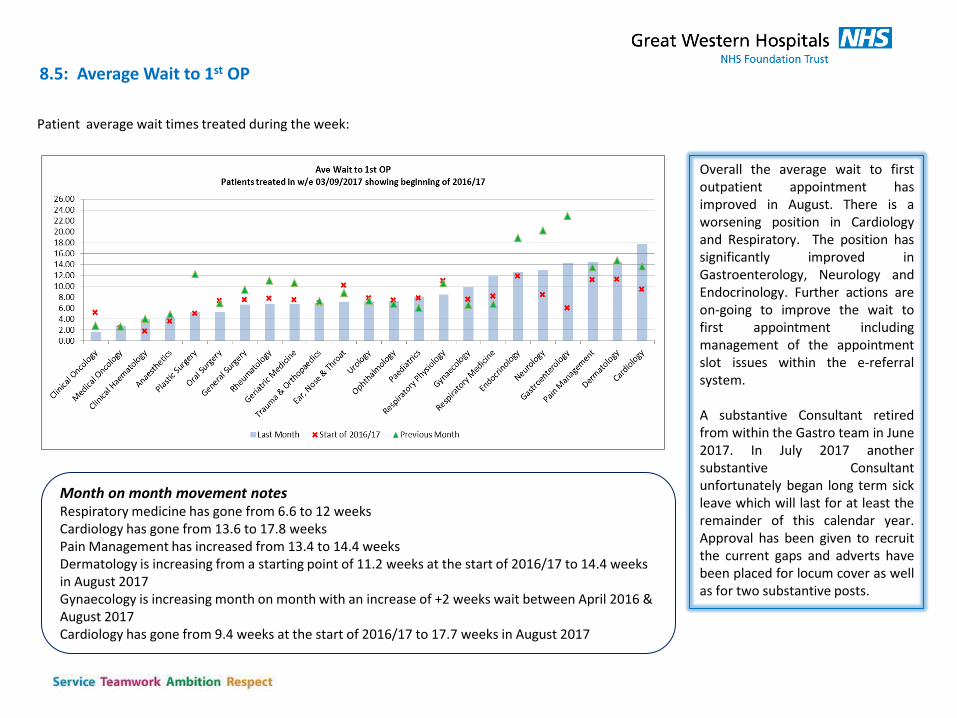
8.5: Average Wait to 1st OP
Patient average wait times treated during the week:
Overall the average wait to first outpatient appointment has improved in August. There is a worsening position in Cardiology and Respiratory. The position has significantly improved in Gastroenterology, Neurology and Endocrinology. Further actions are on-going to improve the wait to first appointment including management of the appointment slot issues within the e-referral system. A substantive Consultant retired from within the Gastro team in June 2017. In July 2017 another substantive Consultant unfortunately began long term sick leave which will last for at least the remainder of this calendar year. Approval has been given to recruit the current gaps and adverts have been placed for locum cover as well as for two substantive posts.
Month on month movement notes Respiratory medicine has gone from 6.6 to 12 weeks Cardiology has gone from 13.6 to 17.8 weeks Pain Management has increased from 13.4 to 14.4 weeks Dermatology is increasing from a starting point of 11.2 weeks at the start of 2016/17 to 14.4 weeks in August 2017 Gynaecology is increasing month on month with an increase of +2 weeks wait between April 2016 & August 2017 Cardiology has gone from 9.4 weeks at the start of 2016/17 to 17.7 weeks in August 2017
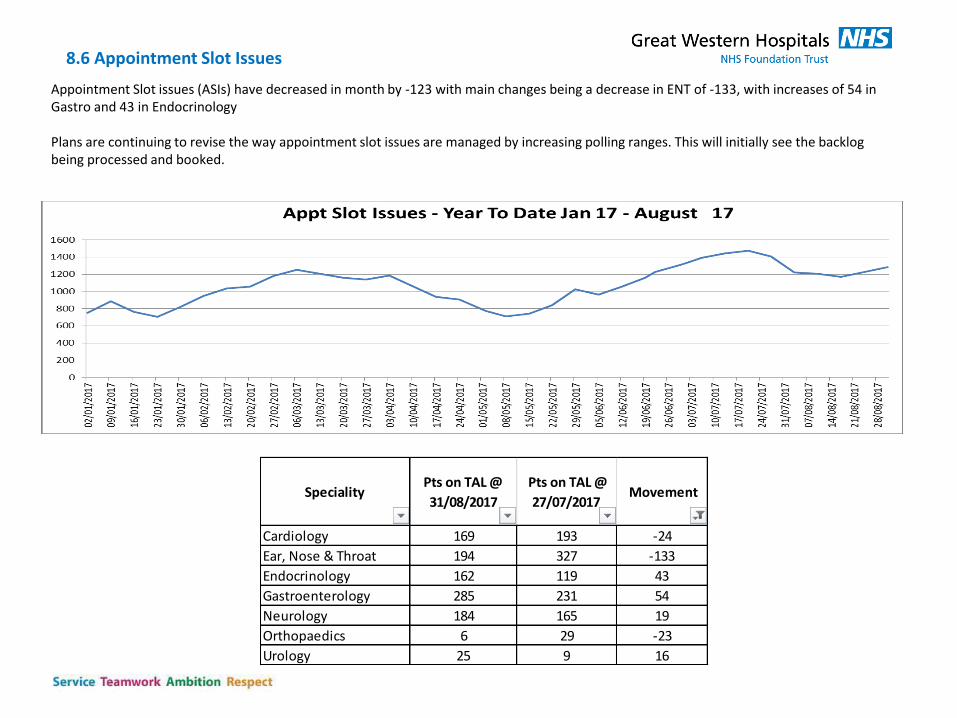
Appointment Slot issues (ASIs) have decreased in month by -123 with main changes being a decrease in ENT of -133, with increases of 54 in Gastro and 43 in Endocrinology Plans are continuing to revise the way appointment slot issues are managed by increasing polling ranges. This will initially see the backlog being processed and booked.
8.6 Appointment Slot Issues
SpecialityPts on TAL @
31/08/2017
Pts on TAL @
27/07/2017 Movement
Cardiology 169 193 -24
Ear, Nose & Throat 194 327 -133
Endocrinology 162 119 43
Gastroenterology 285 231 54
Neurology 184 165 19
Orthopaedics 6 29 -23
Urology 25 9 16
Section 9: Theatres
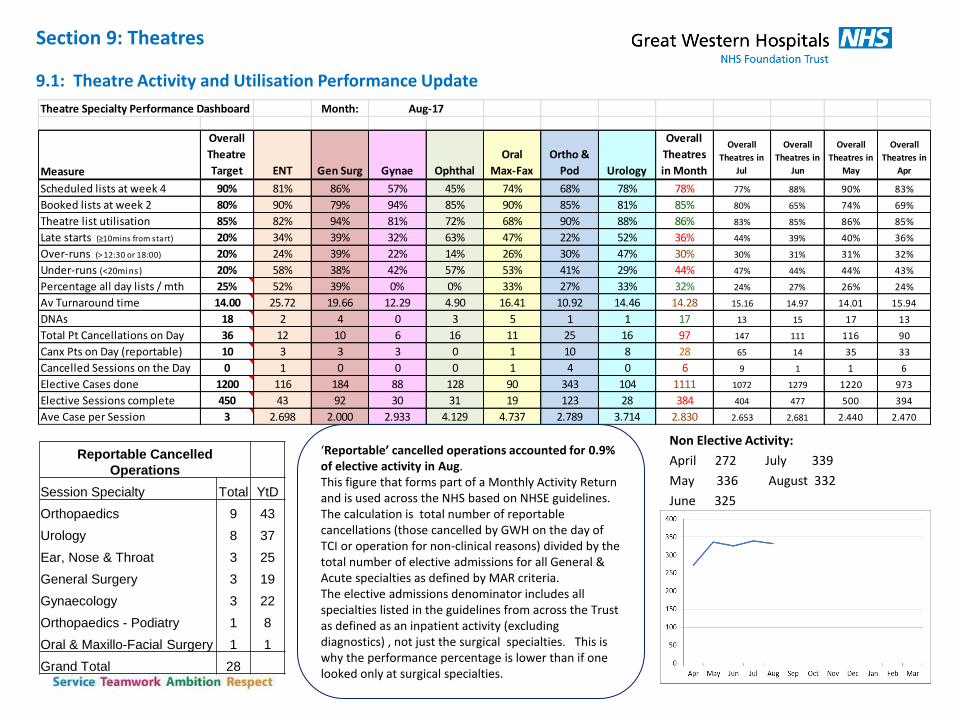
9.1: Theatre Activity and Utilisation Performance Update
Non Elective Activity:
April 272 July 339
May 336 August 332
June 325
Theatre Specialty Performance Dashboard Month:
Measure
Overall
Theatre
Target ENT Gen Surg Gynae Ophthal
Oral
Max-Fax
Ortho &
Pod Urology
Overall
Theatres
in Month
Overall
Theatres in
Jul
Overall
Theatres in
Jun
Overall
Theatres in
May
Overall
Theatres in
Apr
Scheduled lists at week 4 90% 81% 86% 57% 45% 74% 68% 78% 78% 77% 88% 90% 83%
Booked lists at week 2 80% 90% 79% 94% 85% 90% 85% 81% 85% 80% 65% 74% 69%
Theatre list utilisation 85% 82% 94% 81% 72% 68% 90% 88% 86% 83% 85% 86% 85%
Late starts (≥10mins from start) 20% 34% 39% 32% 63% 47% 22% 52% 36% 44% 39% 40% 36%
Over-runs (> 12:30 or 18:00) 20% 24% 39% 22% 14% 26% 30% 47% 30% 30% 31% 31% 32%
Under-runs (<20mins) 20% 58% 38% 42% 57% 53% 41% 29% 44% 47% 44% 44% 43%
Percentage all day lists / mth 25% 52% 39% 0% 0% 33% 27% 33% 32% 24% 27% 26% 24%
Av Turnaround time 14.00 25.72 19.66 12.29 4.90 16.41 10.92 14.46 14.28 15.16 14.97 14.01 15.94
DNAs 18 2 4 0 3 5 1 1 17 13 15 17 13
Total Pt Cancellations on Day 36 12 10 6 16 11 25 16 97 147 111 116 90
Canx Pts on Day (reportable) 10 3 3 3 0 1 10 8 28 65 14 35 33
Cancelled Sessions on the Day 0 1 0 0 0 1 4 0 6 9 1 1 6
Elective Cases done 1200 116 184 88 128 90 343 104 1111 1072 1279 1220 973
Elective Sessions complete 450 43 92 30 31 19 123 28 384 404 477 500 394
Ave Case per Session 3 2.698 2.000 2.933 4.129 4.737 2.789 3.714 2.830 2.653 2.681 2.440 2.470
Aug-17
Reportable Cancelled
Operations
Session Specialty Total YtD
Orthopaedics 9 43
Urology 8 37
Ear, Nose & Throat 3 25
General Surgery 3 19
Gynaecology 3 22
Orthopaedics - Podiatry 1 8
Oral & Maxillo-Facial Surgery 1 1
Grand Total 28
‘Reportable’ cancelled operations accounted for 0.9% of elective activity in Aug. This figure that forms part of a Monthly Activity Return and is used across the NHS based on NHSE guidelines. The calculation is total number of reportable cancellations (those cancelled by GWH on the day of TCI or operation for non-clinical reasons) divided by the total number of elective admissions for all General & Acute specialties as defined by MAR criteria. The elective admissions denominator includes all specialties listed in the guidelines from across the Trust as defined as an inpatient activity (excluding diagnostics) , not just the surgical specialties. This is why the performance percentage is lower than if one looked only at surgical specialties.
9.2: Theatre Performance Headlines, Improvement Opportunities and Actions:
• Utilisation – utilisation continues to be maintained close to target. Scheduled sessions dropped significantly in month with 120 sessions not taken up due to surgeon leave/unavailability. A further 44 sessions lost to planned Treatment Centre theatre closures for redecoration, which is now completed.
• Late starts, over-runs, under-runs and turnaround times – 36% lists started late which is an improvement on 44% the month before as a result of the trial of the use of recovery further work is on-going to improve this further. Turnaround times are higher for specialties with all day lists due to the flexible lunch, but there is a marked improvement in General Surgery in month.
• Cancellations – 36 reportable patients cancelled on the day (currently unvalidated), giving a performance of 1.1% against the 0.8% target. This was driving by sickness on the day (6 sessions also lost due to surgeon and anaesthetist sickness) as well as flow issues resulting in surgeons running out of time. DNA performance continues on target and significantly lower than 2016/17 & 2015/16.
• Average case per session – improvement towards target continues despite running fewer sessions in month. Number of sessions used and cases undertaken slighter lower than same period last year, although average case per session on a par.
• Actions: • Prompt starts: TU programme manager exploring actions taken by other Trusts to start lists earlier and promptly. • NCEPOD. Roll out emergency theatre booking card to reduce delays and improve list planning • List approval. Set up surgeon sign-off of planned lists to reduce on day delays due to list reordering by surgical team
(Urology/Ophthalmology) • Patient flow. Revisit audit of delays from Recovery to DSU/ICU/Ward to identify opportunities for improvement as insufficient data
from first audit; review trial of allocating TSWs to Theatre and Recovery to ascertain impact on patient transfers in/out of department; conduct process map of TAL first patient admissions to understand flow constraints.
• Outsourcing repatriation. 4-joint orthopaedic lists commence in September – review trial to understand barriers and constraints, successes and failures.
9.3 Specialty level performance trends and actions:
Using the monthly specialty-level dashboard we are able to identify trends or areas of focus across surgical specialties. Some fluctuations are directly related to in-month issues, like high annual leave; others represent a longer term performance barrier and the Theatre Utilisation project team are working with specialty leads to understand the causes, constraints and potential solutions. Main specialties with trending off-target performance:
ENT – under-running lists and turnaround times
• Service reviewing actual procedure times vs planned to see if any trends by surgeon or procedure. Reporting to TU Board October
General Surgery – scheduling and booking, overall use of theatre time, average case per session
• Service reviewing use of lists for complex patients and accuracy of procedure times. Improvements to Fast Track booking using underbooked lists required to avoid wasted time or reliance on WLIs. Reporting to TU Board September
Gynaecology - late starts and scheduling
• Service manager highlighted late starts at July clinician’s meeting, resulting in improvement in August performance.
• Scheduling down in August due to high surgeon’s leave and unable to recycle sessions as limited Registrar resource
Ophthalmology – scheduling and overall utilisation
• Scheduling affected in recent months by annual leave and job plan changes. This is now rectified and anticipating better scheduling of theatre lists in September.
• New interim HOS in post and reviewing theatre usage data. Creating a plan for a stepped increase to 7 cataracts per designated theatre list over for rest of 2017/18.
Oral Surgery – overall utilisation, late starts and under-runs
• Service experiences high DNAs or on day patient cancellations. Exploring options to over-book where there are trends, and explore use of theatre time and booking criteria. Reporting to TU Board October.
Orthopaedics – scheduling
• Scheduling impacted in month by closure of Treatment Centre theatres throughout August as part of planned redecoration programme.
• Trialling 4-joint orthopaedic lists to increase case per session to meet outsourcing repatriation targets.
Urology – late starts and under-runs
• Use of emergency slots of ward patients impacts utilisation and under-runs. Also high number of list changes on the day.
• Service setting up a surgeon review/sign-off of theatre list booking order 2wks in advance to reduce on the day changes and delays. Reporting to TU Board September.
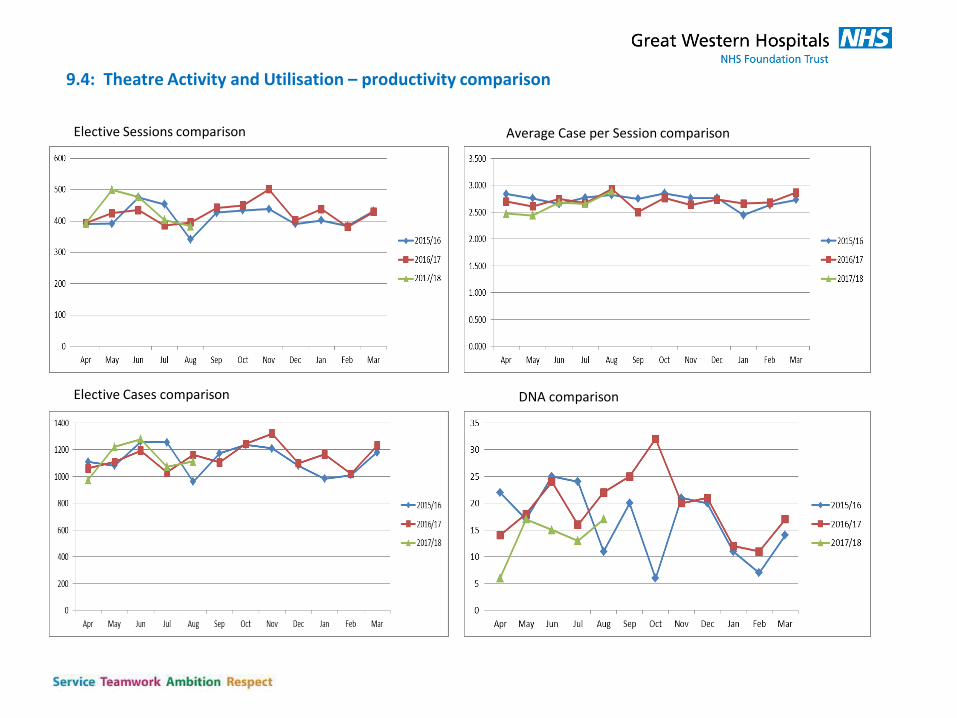
9.4: Theatre Activity and Utilisation – productivity comparison
Elective Sessions comparison
Elective Cases comparison
Average Case per Session comparison
DNA comparison
9.5: DSU IP Overnight Bed Occupancy
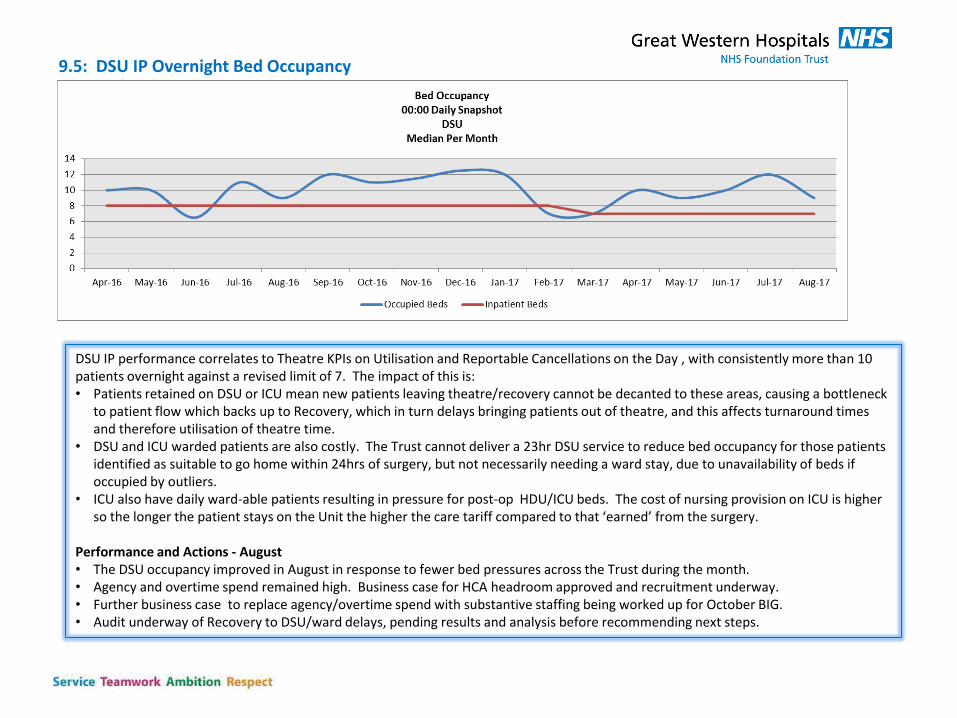
DSU IP performance correlates to Theatre KPIs on Utilisation and Reportable Cancellations on the Day , with consistently more than 10 patients overnight against a revised limit of 7. The impact of this is: • Patients retained on DSU or ICU mean new patients leaving theatre/recovery cannot be decanted to these areas, causing a bottleneck
to patient flow which backs up to Recovery, which in turn delays bringing patients out of theatre, and this affects turnaround times and therefore utilisation of theatre time.
• DSU and ICU warded patients are also costly. The Trust cannot deliver a 23hr DSU service to reduce bed occupancy for those patients identified as suitable to go home within 24hrs of surgery, but not necessarily needing a ward stay, due to unavailability of beds if occupied by outliers.
• ICU also have daily ward-able patients resulting in pressure for post-op HDU/ICU beds. The cost of nursing provision on ICU is higher so the longer the patient stays on the Unit the higher the care tariff compared to that ‘earned’ from the surgery.
Performance and Actions - August • The DSU occupancy improved in August in response to fewer bed pressures across the Trust during the month. • Agency and overtime spend remained high. Business case for HCA headroom approved and recruitment underway. • Further business case to replace agency/overtime spend with substantive staffing being worked up for October BIG. • Audit underway of Recovery to DSU/ward delays, pending results and analysis before recommending next steps.
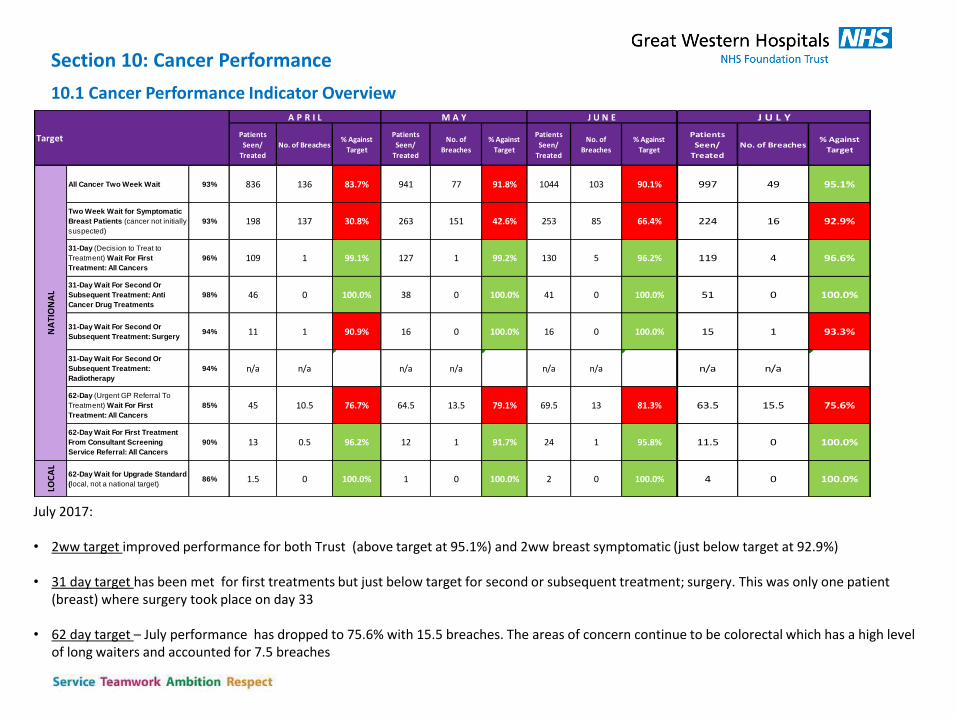
July 2017: • 2ww target improved performance for both Trust (above target at 95.1%) and 2ww breast symptomatic (just below target at 92.9%)
• 31 day target has been met for first treatments but just below target for second or subsequent treatment; surgery. This was only one patient
(breast) where surgery took place on day 33
• 62 day target – July performance has dropped to 75.6% with 15.5 breaches. The areas of concern continue to be colorectal which has a high level of long waiters and accounted for 7.5 breaches
Section 10: Cancer Performance
10.1 Cancer Performance Indicator Overview
Patients
Seen/
Treated
No. of Breaches% Against
Target
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
All Cancer Two Week Wait 93% 836 136 83.7% 941 77 91.8% 1044 103 90.1%
Two Week Wait for Symptomatic
Breast Patients (cancer not initially
suspected)
93% 198 137 30.8% 263 151 42.6% 253 85 66.4%
31-Day (Decision to Treat to
Treatment) Wait For First
Treatment: All Cancers
96% 109 1 99.1% 127 1 99.2% 130 5 96.2%
31-Day Wait For Second Or
Subsequent Treatment: Anti
Cancer Drug Treatments
98% 46 0 100.0% 38 0 100.0% 41 0 100.0%
31-Day Wait For Second Or
Subsequent Treatment: Surgery 94% 11 1 90.9% 16 0 100.0% 16 0 100.0%
31-Day Wait For Second Or
Subsequent Treatment:
Radiotherapy
94% n/a n/a #VALUE! n/a n/a #VALUE! n/a n/a #VALUE!
62-Day (Urgent GP Referral To
Treatment) Wait For First
Treatment: All Cancers
85% 45 10.5 76.7% 64.5 13.5 79.1% 69.5 13 81.3%
62-Day Wait For First Treatment
From Consultant Screening
Service Referral: All Cancers
90% 13 0.5 96.2% 12 1 91.7% 24 1 95.8%
LOC
AL
62-Day Wait for Upgrade Standard
(local, not a national target)86% 1.5 0 100.0% 1 0 100.0% 2 0 100.0%
NA
TIO
NA
L
Target
A P R I L M A Y J U N E
Patients
Seen/
Treated
No. of Breaches% Against
Target
997 49 95.1%
224 16 92.9%
119 4 96.6%
51 0 100.0%
15 1 93.3%
n/a n/a #VALUE!
63.5 15.5 75.6%
11.5 0 100.0%
4 0 100.0%
J U L Y
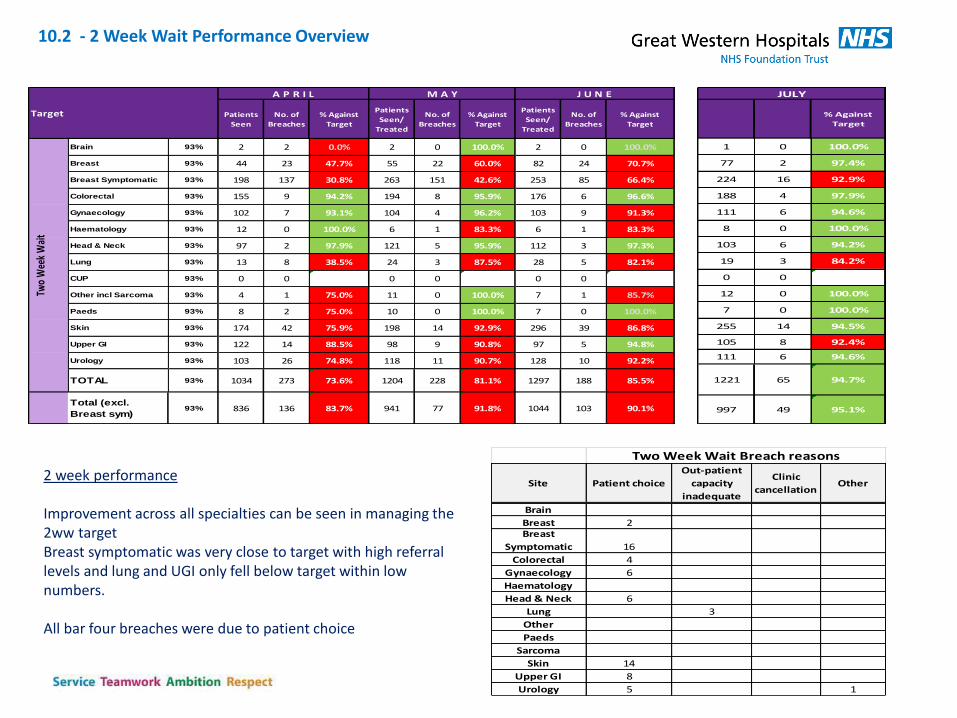
2 week performance Improvement across all specialties can be seen in managing the 2ww target Breast symptomatic was very close to target with high referral levels and lung and UGI only fell below target within low numbers. All bar four breaches were due to patient choice
Site Patient choice
Out-patient
capacity
inadequate
Clinic
cancellationOther
Brain
Breast 2Breast
Symptomatic 16
Colorectal 4
Gynaecology 6
Haematology
Head & Neck 6
Lung 3
Other
Paeds
Sarcoma
Skin 14
Upper GI 8
Urology 5 1
Two Week Wait Breach reasons
Patients
Seen
No. of
Breaches
% Against
Target
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Brain 93% 2 2 0.0% 2 0 100.0% 2 0 100.0%
Breast 93% 44 23 47.7% 55 22 60.0% 82 24 70.7%
Breast Symptomatic 93% 198 137 30.8% 263 151 42.6% 253 85 66.4%
Colorectal 93% 155 9 94.2% 194 8 95.9% 176 6 96.6%
Gynaecology 93% 102 7 93.1% 104 4 96.2% 103 9 91.3%
Haematology 93% 12 0 100.0% 6 1 83.3% 6 1 83.3%
Head & Neck 93% 97 2 97.9% 121 5 95.9% 112 3 97.3%
Lung 93% 13 8 38.5% 24 3 87.5% 28 5 82.1%
CUP 93% 0 0 #DIV/0! 0 0 #DIV/0! 0 0 #DIV/0!
Other incl Sarcoma 93% 4 1 75.0% 11 0 100.0% 7 1 85.7%
Paeds 93% 8 2 75.0% 10 0 100.0% 7 0 100.0%
Skin 93% 174 42 75.9% 198 14 92.9% 296 39 86.8%
Upper GI 93% 122 14 88.5% 98 9 90.8% 97 5 94.8%
Urology 93% 103 26 74.8% 118 11 90.7% 128 10 92.2%
TOTAL 93% 1034 273 73.6% 1204 228 81.1% 1297 188 85.5%
Total (excl.
Breast sym)93% 836 136 83.7% 941 77 91.8% 1044 103 90.1%
Target
A P R I L M A Y J U N E
Two
Wee
k W
ait
% Against
Target
1 0 100.0%
77 2 97.4%
224 16 92.9%
188 4 97.9%
111 6 94.6%
8 0 100.0%
103 6 94.2%
19 3 84.2%
0 0 #DIV/0!
12 0 100.0%
7 0 100.0%
255 14 94.5%
105 8 92.4%
111 6 94.6%
1221 65 94.7%
997 49 95.1%
JULY
10.2 - 2 Week Wait Performance Overview
10.3 – 62 day Performance for month (July) – 75.6% ( Standard 85%)
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Over 104
days
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Over 104
days
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Over 104
days
Brain 85% 0 0 #DIV/0! 0 0 #DIV/0! 0 0 #DIV/0!
Breast 85% 4 0 100.0% 4 1 75.0% 4 1 75.0%
Breast Symptomatic 85% 13 1 92.3% 8 2 75.0% 11 0 100.0%
Colorectal 85% 10 6 40.0% 0.5 6 2 66.7% 1 9.5 6.5 31.6% 1.5
Gynaecology 85% 1.5 0.5 66.7% 7 5 28.6% 3 2 33.3% 1
Haematology 85% 2 1 50.0% 6 1 83.3% 6 0 100.0%
Head & Neck 85% 2 0 100.0% 2.5 2 20.0% 0.5 1 0.5 50.0%
Lung 85% 6.5 0 100.0% 5 0 100.0% 7 1 85.7%
CUP 85% 0 0 #DIV/0! 0 0 #DIV/0! 0 0 #DIV/0!
Other incl Sarcoma 85% 0.5 0 100.0% 1 1 0.0% 2.5 0.5 80.0%
Skin 85% 8 0 100.0% 20.5 0 100.0% 17.5 0 100.0%
Upper GI 85% 2 1 50.0% 1 4 0 100.0% 6 0.5 91.7% 0.5
Urology 85% 8.5 2 76.5% 8.5 1.5 82.4% 13 1 92.3%
TOTAL 85% 58 11.5 80.2% 1.5 72.5 15.5 78.6% 1.5 80.5 13 83.9% 3
Total (excl.
Breast sym)85% 45 10.5 76.7% 1.5 64.5 13.5 79.1% 1.5 69.5 13 81.3% 3
Target
A P R I L M A Y J U N E
62-D
ay (
Urg
ent
GP
Ref
erra
l To
Tre
atm
ent)
Wai
t Fo
r Fi
rst
Trea
tmen
t: A
ll C
ance
rs
Patients
Seen/
Treated
No. of
Breaches
% Against
Target
Over 104
days
0 0 #DIV/0!
8 0 100.0%
6 0 100.0%
12.5 7.5 40.0% 2
0 0 #DIV/0!
2 0 100.0%
1 0 100.0%
6 1 83.3%
0.5 0.5 0.0%
10.5 0 100.0%
8 4.5 43.8% 1.5
1 0 100.0%
14 2 85.7% 1
69.5 15.5 77.7% 4.5
63.5 15.5 75.6% 4.5
JULY
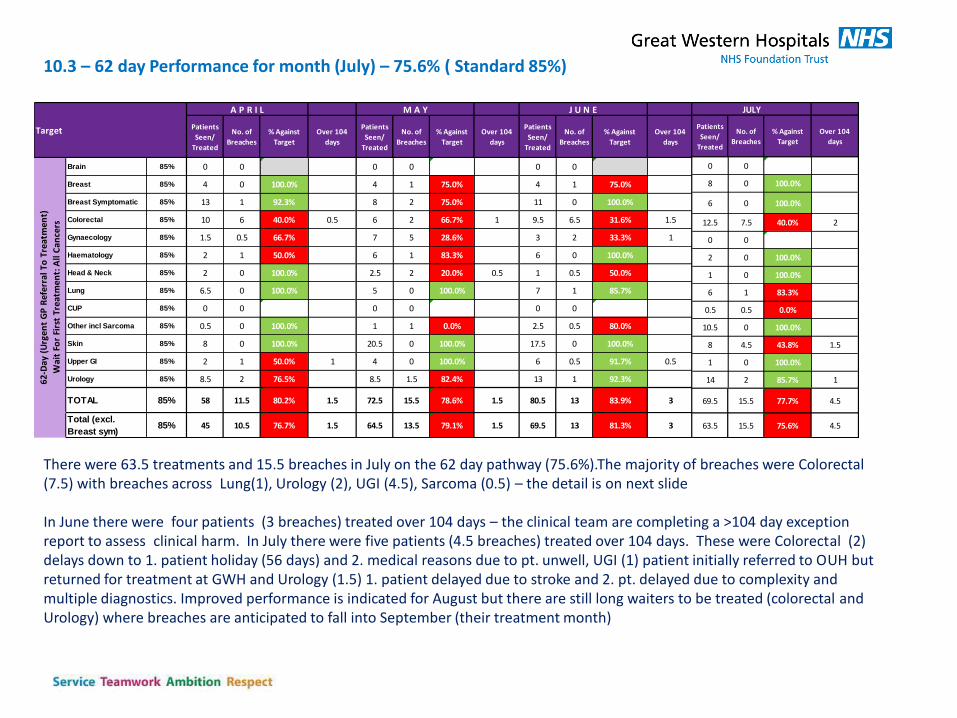
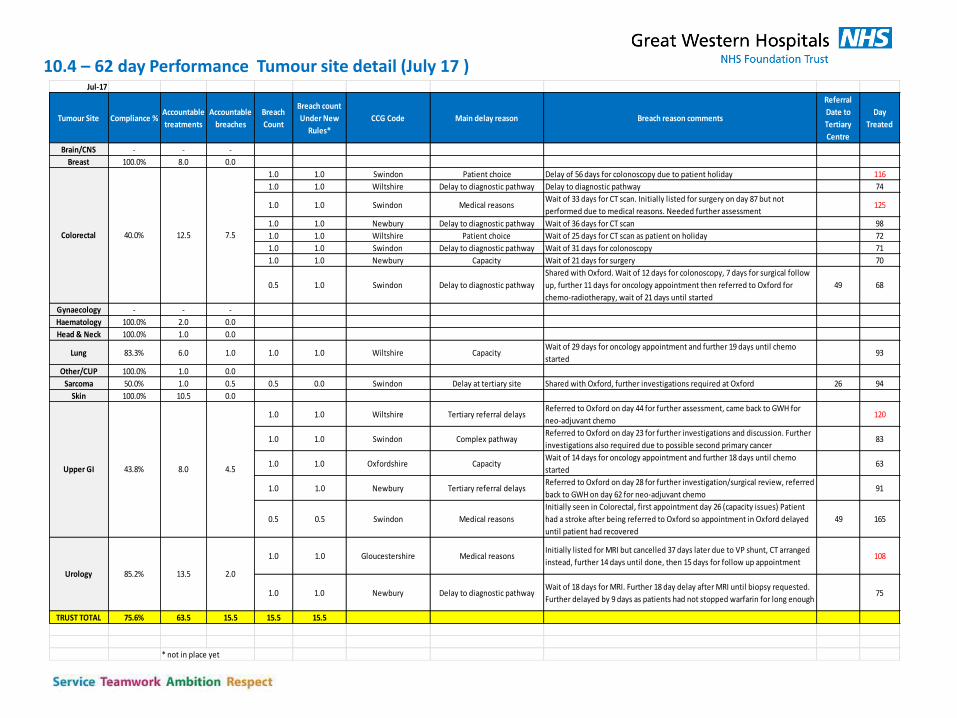
There were 63.5 treatments and 15.5 breaches in July on the 62 day pathway (75.6%).The majority of breaches were Colorectal (7.5) with breaches across Lung(1), Urology (2), UGI (4.5), Sarcoma (0.5) – the detail is on next slide In June there were four patients (3 breaches) treated over 104 days – the clinical team are completing a >104 day exception report to assess clinical harm. In July there were five patients (4.5 breaches) treated over 104 days. These were Colorectal (2) delays down to 1. patient holiday (56 days) and 2. medical reasons due to pt. unwell, UGI (1) patient initially referred to OUH but returned for treatment at GWH and Urology (1.5) 1. patient delayed due to stroke and 2. pt. delayed due to complexity and multiple diagnostics. Improved performance is indicated for August but there are still long waiters to be treated (colorectal and Urology) where breaches are anticipated to fall into September (their treatment month)
10.4 – 62 day Performance Tumour site detail (July 17 ) Jul-17
Tumour Site Compliance %Accountable
treatments
Accountable
breaches
Breach
Count
Breach count
Under New
Rules*
CCG Code Main delay reason Breach reason comments
Referral
Date to
Tertiary
Centre
Day
Treated
Brain/CNS - - -
Breast 100.0% 8.0 0.0
1.0 1.0 Swindon Patient choice Delay of 56 days for colonoscopy due to patient holiday 116
1.0 1.0 Wiltshire Delay to diagnostic pathway Delay to diagnostic pathway 74
1.0 1.0 Swindon Medical reasonsWait of 33 days for CT scan. Initially listed for surgery on day 87 but not
performed due to medical reasons. Needed further assessment125
1.0 1.0 Newbury Delay to diagnostic pathway Wait of 36 days for CT scan 98
1.0 1.0 Wiltshire Patient choice Wait of 25 days for CT scan as patient on holiday 72
1.0 1.0 Swindon Delay to diagnostic pathway Wait of 31 days for colonoscopy 71
1.0 1.0 Newbury Capacity Wait of 21 days for surgery 70
0.5 1.0 Swindon Delay to diagnostic pathway
Shared with Oxford. Wait of 12 days for colonoscopy, 7 days for surgical follow
up, further 11 days for oncology appointment then referred to Oxford for
chemo-radiotherapy, wait of 21 days until started
49 68
Gynaecology - - -
Haematology 100.0% 2.0 0.0
Head & Neck 100.0% 1.0 0.0
Lung 83.3% 6.0 1.0 1.0 1.0 Wiltshire CapacityWait of 29 days for oncology appointment and further 19 days until chemo
started93
Other/CUP 100.0% 1.0 0.0
Sarcoma 50.0% 1.0 0.5 0.5 0.0 Swindon Delay at tertiary site Shared with Oxford, further investigations required at Oxford 26 94
Skin 100.0% 10.5 0.0
1.0 1.0 Wiltshire Tertiary referral delaysReferred to Oxford on day 44 for further assessment, came back to GWH for
neo-adjuvant chemo120
1.0 1.0 Swindon Complex pathwayReferred to Oxford on day 23 for further investigations and discussion. Further
investigations also required due to possible second primary cancer83
1.0 1.0 Oxfordshire CapacityWait of 14 days for oncology appointment and further 18 days until chemo
started 63
1.0 1.0 Newbury Tertiary referral delaysReferred to Oxford on day 28 for further investigation/surgical review, referred
back to GWH on day 62 for neo-adjuvant chemo 91
0.5 0.5 Swindon Medical reasons
Initially seen in Colorectal, first appointment day 26 (capacity issues) Patient
had a stroke after being referred to Oxford so appointment in Oxford delayed
until patient had recovered
49 165
1.0 1.0 Gloucestershire Medical reasonsInitially listed for MRI but cancelled 37 days later due to VP shunt, CT arranged
instead, further 14 days until done, then 15 days for follow up appointment108
1.0 1.0 Newbury Delay to diagnostic pathwayWait of 18 days for MRI. Further 18 day delay after MRI until biopsy requested.
Further delayed by 9 days as patients had not stopped warfarin for long enough75
TRUST TOTAL 75.6% 63.5 15.5 15.5 15.5
* not in place yet
13.5 2.085.2%Urology
Colorectal 40.0% 12.5 7.5
Upper GI 8.0 4.543.8%
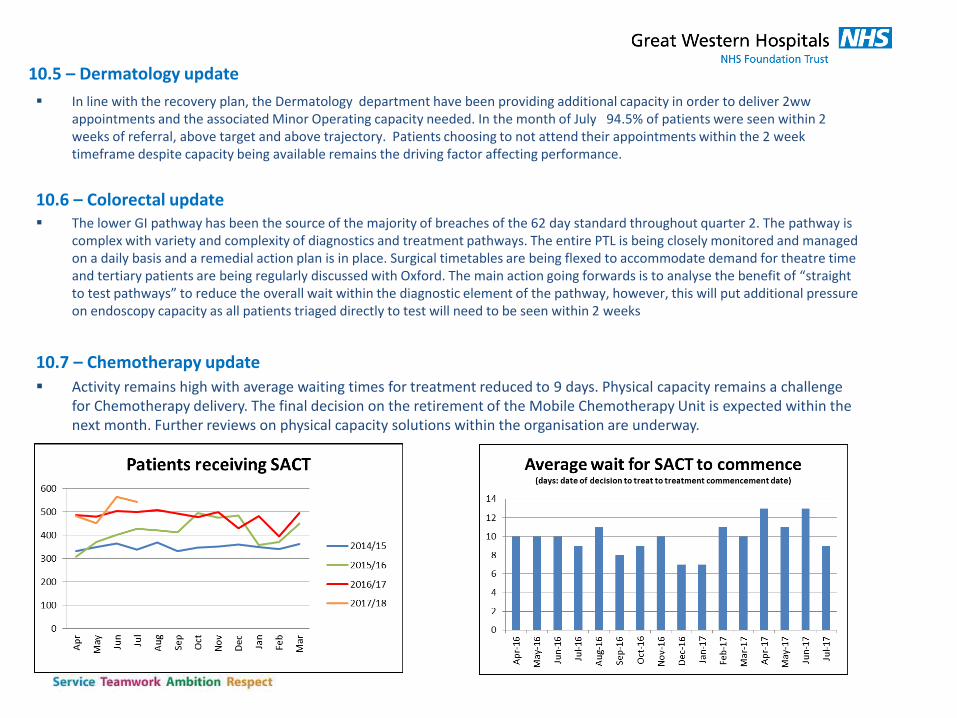
In line with the recovery plan, the Dermatology department have been providing additional capacity in order to deliver 2ww appointments and the associated Minor Operating capacity needed. In the month of July 94.5% of patients were seen within 2 weeks of referral, above target and above trajectory. Patients choosing to not attend their appointments within the 2 week timeframe despite capacity being available remains the driving factor affecting performance.
10.6 – Colorectal update The lower GI pathway has been the source of the majority of breaches of the 62 day standard throughout quarter 2. The pathway is
complex with variety and complexity of diagnostics and treatment pathways. The entire PTL is being closely monitored and managed on a daily basis and a remedial action plan is in place. Surgical timetables are being flexed to accommodate demand for theatre time and tertiary patients are being regularly discussed with Oxford. The main action going forwards is to analyse the benefit of “straight to test pathways” to reduce the overall wait within the diagnostic element of the pathway, however, this will put additional pressure on endoscopy capacity as all patients triaged directly to test will need to be seen within 2 weeks
10.7 – Chemotherapy update
Activity remains high with average waiting times for treatment reduced to 9 days. Physical capacity remains a challenge for Chemotherapy delivery. The final decision on the retirement of the Mobile Chemotherapy Unit is expected within the next month. Further reviews on physical capacity solutions within the organisation are underway.
10.5 – Dermatology update
Section 11: Diagnostics - Reported performance against national indicators (DM01)
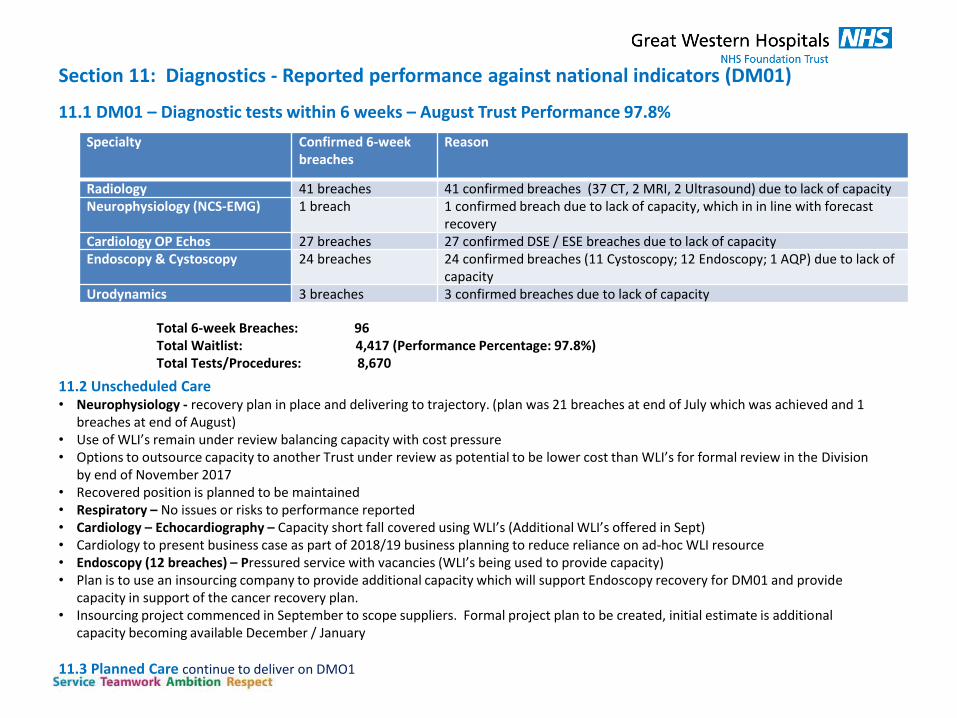
11.1 DM01 – Diagnostic tests within 6 weeks – August Trust Performance 97.8%
11.2 Unscheduled Care • Neurophysiology - recovery plan in place and delivering to trajectory. (plan was 21 breaches at end of July which was achieved and 1
breaches at end of August) • Use of WLI’s remain under review balancing capacity with cost pressure • Options to outsource capacity to another Trust under review as potential to be lower cost than WLI’s for formal review in the Division
by end of November 2017 • Recovered position is planned to be maintained • Respiratory – No issues or risks to performance reported • Cardiology – Echocardiography – Capacity short fall covered using WLI’s (Additional WLI’s offered in Sept) • Cardiology to present business case as part of 2018/19 business planning to reduce reliance on ad-hoc WLI resource • Endoscopy (12 breaches) – Pressured service with vacancies (WLI’s being used to provide capacity) • Plan is to use an insourcing company to provide additional capacity which will support Endoscopy recovery for DM01 and provide
capacity in support of the cancer recovery plan. • Insourcing project commenced in September to scope suppliers. Formal project plan to be created, initial estimate is additional
capacity becoming available December / January
11.3 Planned Care continue to deliver on DMO1
Specialty Confirmed 6-week breaches
Reason
Radiology 41 breaches 41 confirmed breaches (37 CT, 2 MRI, 2 Ultrasound) due to lack of capacity Neurophysiology (NCS-EMG) 1 breach 1 confirmed breach due to lack of capacity, which in in line with forecast
recovery Cardiology OP Echos 27 breaches 27 confirmed DSE / ESE breaches due to lack of capacity Endoscopy & Cystoscopy 24 breaches 24 confirmed breaches (11 Cystoscopy; 12 Endoscopy; 1 AQP) due to lack of
capacity Urodynamics 3 breaches 3 confirmed breaches due to lack of capacity
Total 6-week Breaches: 96 Total Waitlist: 4,417 (Performance Percentage: 97.8%) Total Tests/Procedures: 8,670
11.4: D&O
Against the current trajectory there continues to be anxiety around delivery due to capacity within CT scanning. CT bookings are now at 6 weeks, with particular difficulties in booking CT cardiac exams and CT Colons. Additional sessions are being provided where workforce allows. A case to enhance CT capacity has been 50% approved and procurement of 6 days per month CT mobile van is in progress but unlikely to be in place before September. US has improved due to agency use, however the radiology department has been unsuccessful to date in finding a replacement agency worker, or in recruiting new sonographers. This was expected to impact from July, a mitigation plan is currently in place, with one new agency sonographer in place 2 days per week for MSK, a second is being sought for routine work. Following recent interviews, although an increase in suitable applications only 1 candidate was interviewed and has accepted a position. The department continues to advertise. The department has been approached by an experienced Radiographer who wishes to return to practice and will commence her retraining in January.
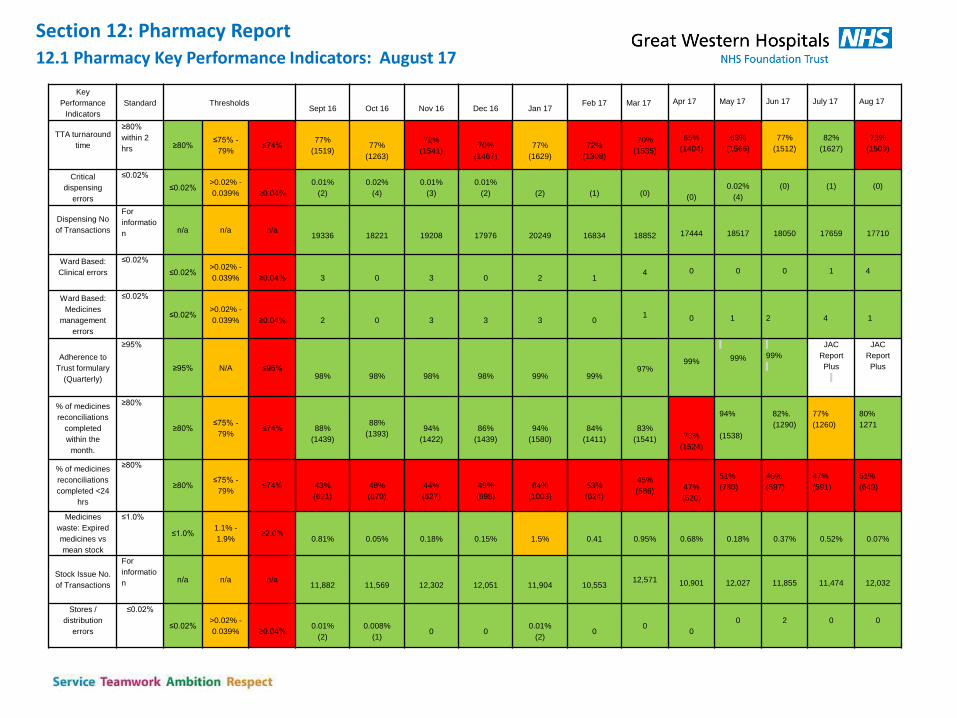
Section 12: Pharmacy Report 12.1 Pharmacy Key Performance Indicators: August 17
Key
Performance
Indicators
Standard Thresholds
Sept 16
Oct 16
Nov 16
Dec 16
Jan 17
Feb 17
Mar 17
Apr 17
May 17
Jun 17
July 17
Aug 17
TTA turnaround
time
≥80%
within 2
hrs ≥80% ≤75% -
79% ≤74%
77%
(1519)
77%
(1263)
72%
(1541)
70%
(1467)
77%
(1629)
72%
(1308)
70%
(1535)
65%
(1404)
63%
(1566)
77%
(1512)
82%
(1627)
73%
(1509)
Critical
dispensing
errors
≤0.02%
≤0.02% >0.02% -
0.039%
≥0.04%
0.01%
(2)
0.02%
(4)
0.01%
(3)
0.01%
(2)
(2)
(1)
(0)
(0)
0.02%
(4)
(0)
(1)
(0)
Dispensing No
of Transactions
For
informatio
n
n/a n/a n/a
19336
18221
19208
17976
20249
16834
18852
17444
18517
18050
17659
17710
Ward Based:
Clinical errors
≤0.02%
≤0.02% >0.02% -
0.039%
≥0.04%
3
0
3
0
2
1 4
0
0
0
1
4
Ward Based:
Medicines
management
errors
≤0.02%
≤0.02% >0.02% -
0.039%
≥0.04%
2
0
3
3
3
0 1
0
1
2
4
1
Adherence to
Trust formulary
(Quarterly)
≥95%
≥95% N/A ≤95%
98%
98%
98%
98%
99%
99% 97%
99%
99%
99%
JAC
Report
Plus
JAC
Report
Plus
% of medicines
reconciliations
completed
within the
month.
≥80%
≥80% ≤75% -
79% ≤74%
88%
(1439)
88%
(1393)
94%
(1422)
86%
(1439)
94%
(1580)
84%
(1411)
83%
(1541)
73%
(1524)
94%
(1538)
82%.
(1290)
77%
(1260)
80%
1271
% of medicines
reconciliations
completed <24
hrs
≥80%
≥80% ≤75% -
79% ≤74%
43%
(621)
48%
(670)
44%
(627)
49%
(698)
64%
(1003)
53%
(624)
45%
(586)
47%
(520)
51%
(780)
46%
(597)
47%
(591)
51%
(649)
Medicines
waste: Expired
medicines vs
mean stock
≤1.0%
≤1.0% 1.1% -
1.9% ≥2.0%
0.81%
0.05%
0.18%
0.15%
1.5%
0.41
0.95%
0.68%
0.18%
0.37%
0.52%
0.07%
Stock Issue No.
of Transactions
For
informatio
n
n/a n/a n/a
11,882
11,569
12,302
12,051
11,904
10,553 12,571
10,901
12,027
11,855
11,474
12,032
Stores /
distribution
errors
≤0.02%
≤0.02% >0.02% -
0.039%
≥0.04%
0.01%
(2)
0.008%
(1)
0
0
0.01%
(2)
0 0
0
0
2
0
0
Section 12.2: Pharmacy Report
Narrative Dispensary August has been a challenging month trying to achieve TTA turnaround times, which is reflected in the performance figures. The department experienced problems with its prescription tracking software which although now resolved, has resulted in manual data collection which has an impact on efficiency. The staff profile within the dispensary has shifted significantly with a number of new staff members requiring training. 173 dossette boxes were dispensed in August, which equates to 11.5% of the TTA’s dispensed and will also have had an impact. However, this investment in training is likely to lead to sustained and improved TTA turnaround times future months ready for the winter pressures. Crucially, there were no critical dispensing errors despite the staff training. Clinical Training new junior Doctors has been a priority and focus for the department in August to ensure that there is familiarity with EPMA and good prescribing practices. This is reflected in the number of ward based clinical errors (4) which all relate to EPMA mis-selections at the point of prescribing. The nature of some of the errors occurred where a similar sounding product had been incorrectly selected and prescribed on EPMA. August has seen an improvement in the number of medicines reconciliations completed both in total, and the number completed within 24 hours. Although reaching the KPI target for 24 hours remains unachievable without 7 day working. It has not been possible to provide the metrics for adherence to the trust formulary again in August. This is due to problems with the IT infrastructure needed for this report. The IT department are currently investigating solutions.
Section 13: Maternity
13.1: Maternity Overview
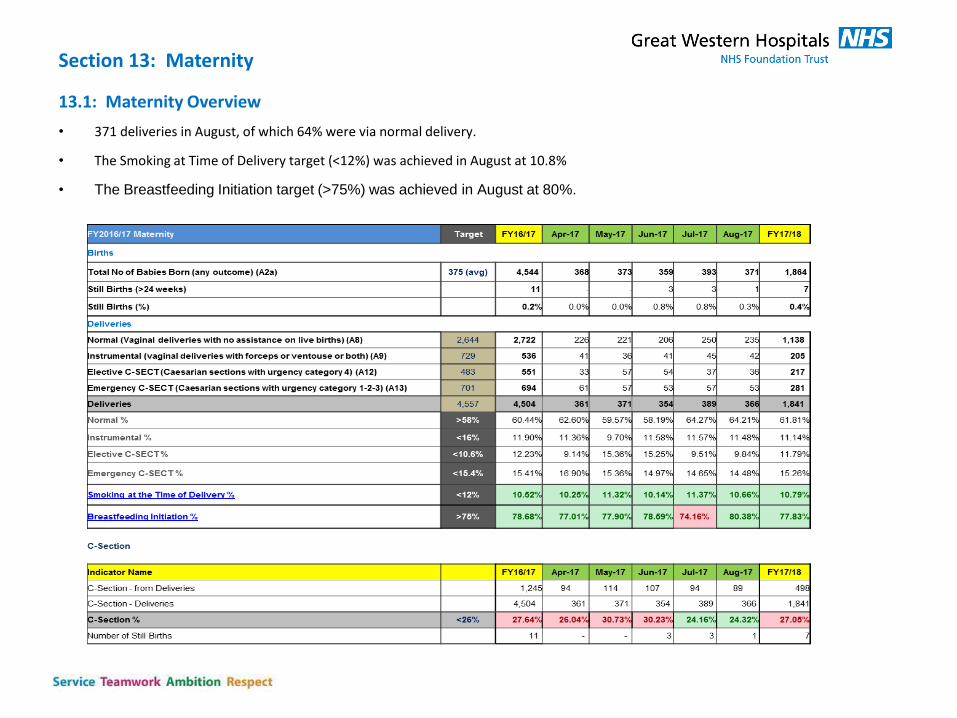
• 371 deliveries in August, of which 64% were via normal delivery.
• The Smoking at Time of Delivery target (<12%) was achieved in August at 10.8%
• The Breastfeeding Initiation target (>75%) was achieved in August at 80%.
13.2: Caesareans (Maternity)
The Maternity Unit’s elective and non elective combined caesarean rate in August is 24%, which is below the national benchmark of 26%.
Whilst the target was achieved in July the following actions are continued to be embedded in the service.
Measures aimed at reducing the Caesarean Section rates:
Obstetric Consultant presence in specialist antenatal clinic for women to discuss VBAC/birthing options now established.
Improved VBAC Care Pathway and associated patient information leaflet implemented.
Additional training pathway associated with new standardised guidelines related to use of Syntocinon for induction or augmentation of labour has been established and is being led by Consultant Obstetrician.
‘Normality Champions’ are to be allocated throughout the unit (initially in Delivery Suite) to support increased unit focus on Normality in 2017.
Frequency of the Caesarean Section Monitoring Group has been increased from quarterly to monthly. Meetings have been regularly scheduled for the second Monday of each month. Representative from Clinical Commissioning to attend.
In August In July
Elective C Section –9.8% (36 cases)
Emergency C Section – 14.5% (53 cases)
Total cases – 89
Elective C Section – 9.5% (37 cases)
Emergency C Section – 14.6% (27 cases)
Total cases – 94
13.3 Still Births
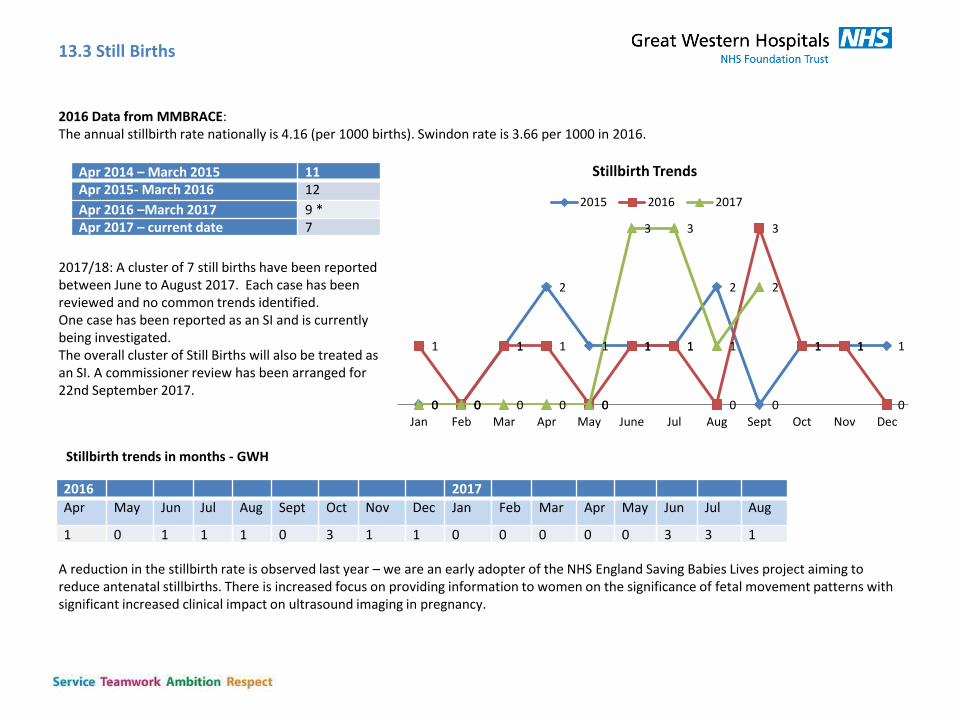
Apr 2014 – March 2015 11 Apr 2015- March 2016 12
Apr 2016 –March 2017 9 * Apr 2017 – current date 7
2016 2017
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug
1 0 1 1 1 0 3 1 1 0 0 0 0 0 3 3 1
2016 Data from MMBRACE: The annual stillbirth rate nationally is 4.16 (per 1000 births). Swindon rate is 3.66 per 1000 in 2016.
Stillbirth trends in months - GWH
0 0
1
2
1 1 1
2
0
1 1 1 1
0
1 1
0
1 1
0
3
1 1
0 0 0 0 0 0
3 3
1
2
Jan Feb Mar Apr May June Jul Aug Sept Oct Nov Dec
Stillbirth Trends
2015 2016 2017
A reduction in the stillbirth rate is observed last year – we are an early adopter of the NHS England Saving Babies Lives project aiming to reduce antenatal stillbirths. There is increased focus on providing information to women on the significance of fetal movement patterns with significant increased clinical impact on ultrasound imaging in pregnancy.
2017/18: A cluster of 7 still births have been reported between June to August 2017. Each case has been reviewed and no common trends identified. One case has been reported as an SI and is currently being investigated. The overall cluster of Still Births will also be treated as an SI. A commissioner review has been arranged for 22nd September 2017.
Section 14: Electronic Discharge Summaries
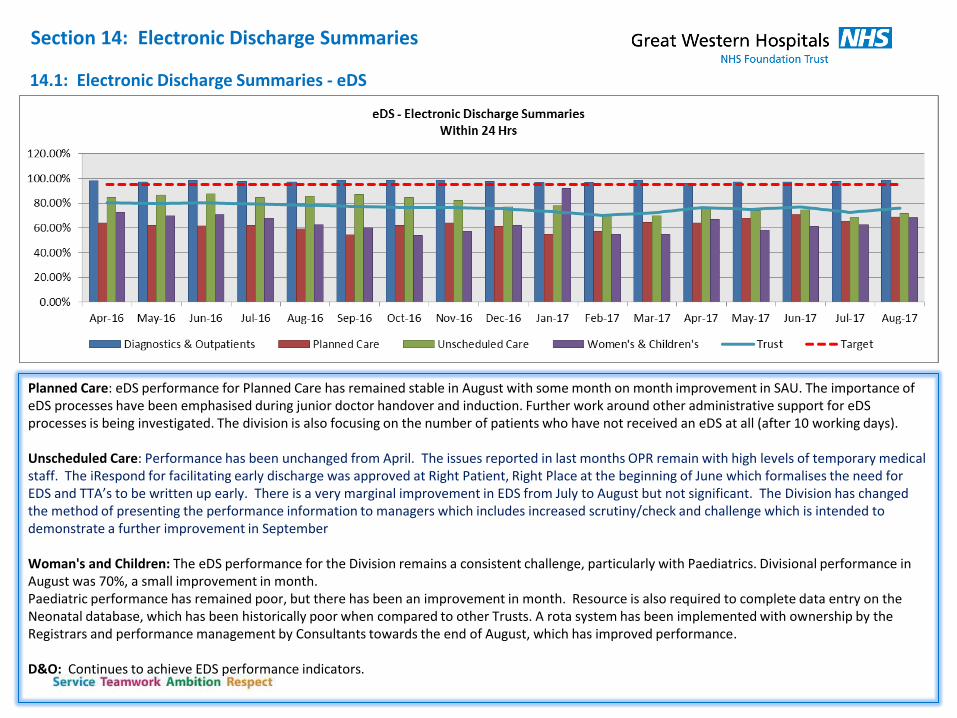
14.1: Electronic Discharge Summaries - eDS
Planned Care: eDS performance for Planned Care has remained stable in August with some month on month improvement in SAU. The importance of eDS processes have been emphasised during junior doctor handover and induction. Further work around other administrative support for eDS processes is being investigated. The division is also focusing on the number of patients who have not received an eDS at all (after 10 working days). Unscheduled Care: Performance has been unchanged from April. The issues reported in last months OPR remain with high levels of temporary medical staff. The iRespond for facilitating early discharge was approved at Right Patient, Right Place at the beginning of June which formalises the need for EDS and TTA’s to be written up early. There is a very marginal improvement in EDS from July to August but not significant. The Division has changed the method of presenting the performance information to managers which includes increased scrutiny/check and challenge which is intended to demonstrate a further improvement in September Woman's and Children: The eDS performance for the Division remains a consistent challenge, particularly with Paediatrics. Divisional performance in August was 70%, a small improvement in month. Paediatric performance has remained poor, but there has been an improvement in month. Resource is also required to complete data entry on the Neonatal database, which has been historically poor when compared to other Trusts. A rota system has been implemented with ownership by the Registrars and performance management by Consultants towards the end of August, which has improved performance. D&O: Continues to achieve EDS performance indicators.
Note: Planned Care & Trust level performance has been calculated manually from Jan 17 to include SAU which changed from eDS to Medway letters
Section 15. Clinical Correspondence – letters sent within 7 days of OP appointment
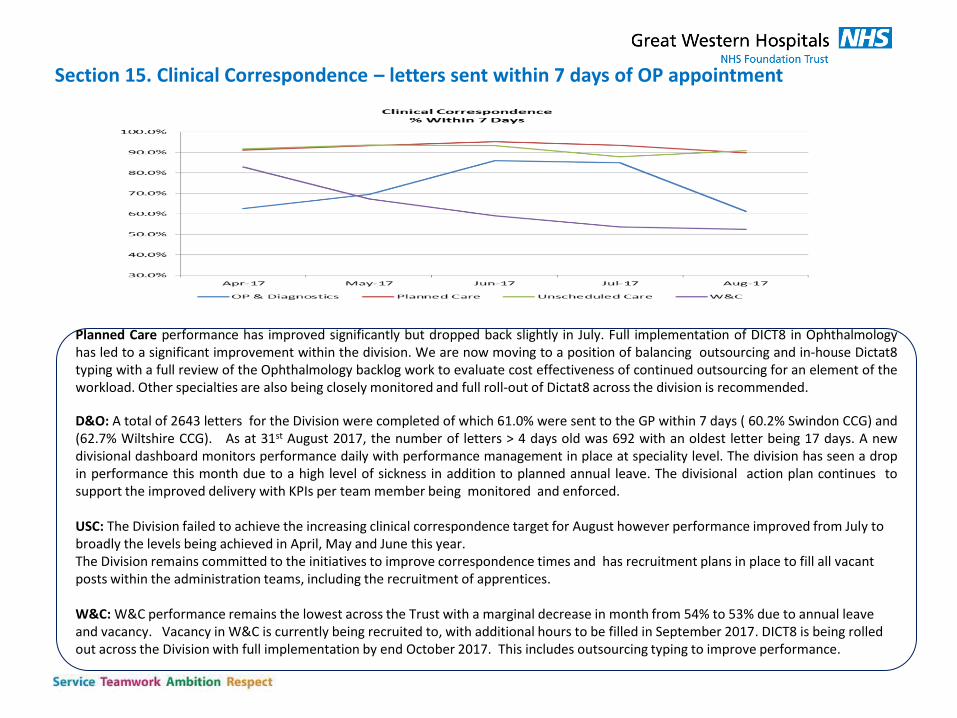
Planned Care performance has improved significantly but dropped back slightly in July. Full implementation of DICT8 in Ophthalmology has led to a significant improvement within the division. We are now moving to a position of balancing outsourcing and in-house Dictat8 typing with a full review of the Ophthalmology backlog work to evaluate cost effectiveness of continued outsourcing for an element of the workload. Other specialties are also being closely monitored and full roll-out of Dictat8 across the division is recommended.
D&O: A total of 2643 letters for the Division were completed of which 61.0% were sent to the GP within 7 days ( 60.2% Swindon CCG) and (62.7% Wiltshire CCG). As at 31st August 2017, the number of letters > 4 days old was 692 with an oldest letter being 17 days. A new divisional dashboard monitors performance daily with performance management in place at speciality level. The division has seen a drop in performance this month due to a high level of sickness in addition to planned annual leave. The divisional action plan continues to support the improved delivery with KPIs per team member being monitored and enforced. USC: The Division failed to achieve the increasing clinical correspondence target for August however performance improved from July to broadly the levels being achieved in April, May and June this year. The Division remains committed to the initiatives to improve correspondence times and has recruitment plans in place to fill all vacant posts within the administration teams, including the recruitment of apprentices. W&C: W&C performance remains the lowest across the Trust with a marginal decrease in month from 54% to 53% due to annual leave and vacancy. Vacancy in W&C is currently being recruited to, with additional hours to be filled in September 2017. DICT8 is being rolled out across the Division with full implementation by end October 2017. This includes outsourcing typing to improve performance.
Section 16 NHS Utilisation of Private Patients
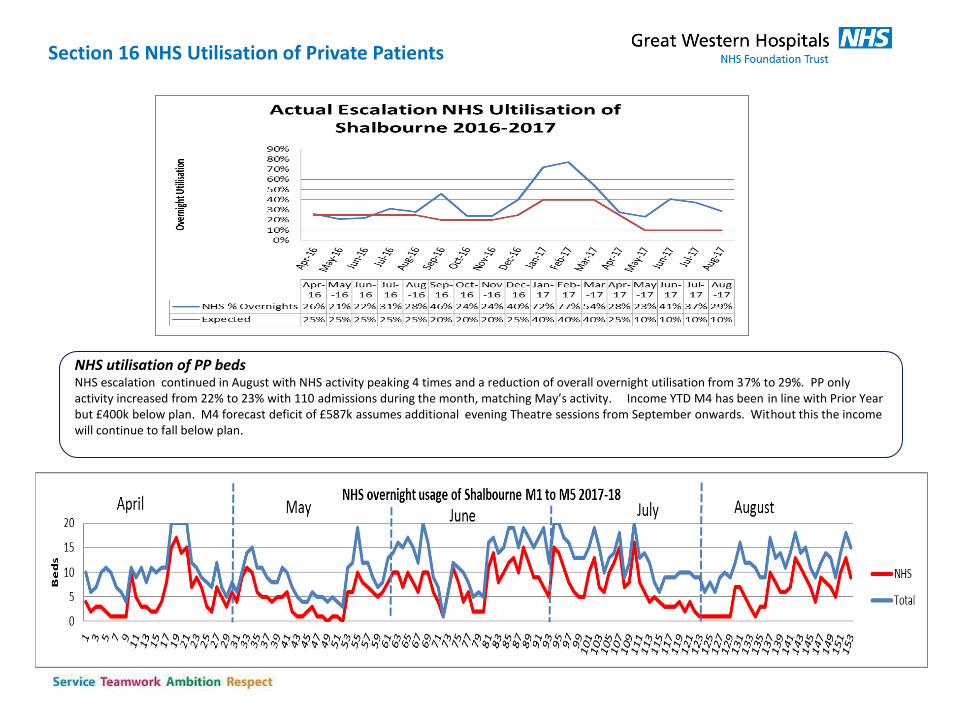
NHS utilisation of PP beds NHS escalation continued in August with NHS activity peaking 4 times and a reduction of overall overnight utilisation from 37% to 29%. PP only activity increased from 22% to 23% with 110 admissions during the month, matching May’s activity. Income YTD M4 has been in line with Prior Year but £400k below plan. M4 forecast deficit of £587k assumes additional evening Theatre sessions from September onwards. Without this the income will continue to fall below plan.
Swindon Community Health Services
Operational Performance Report: August 2017
1.1: Community Nursing Visits The SCHS Community Nursing uses SystmOne to track visits. Each day ,
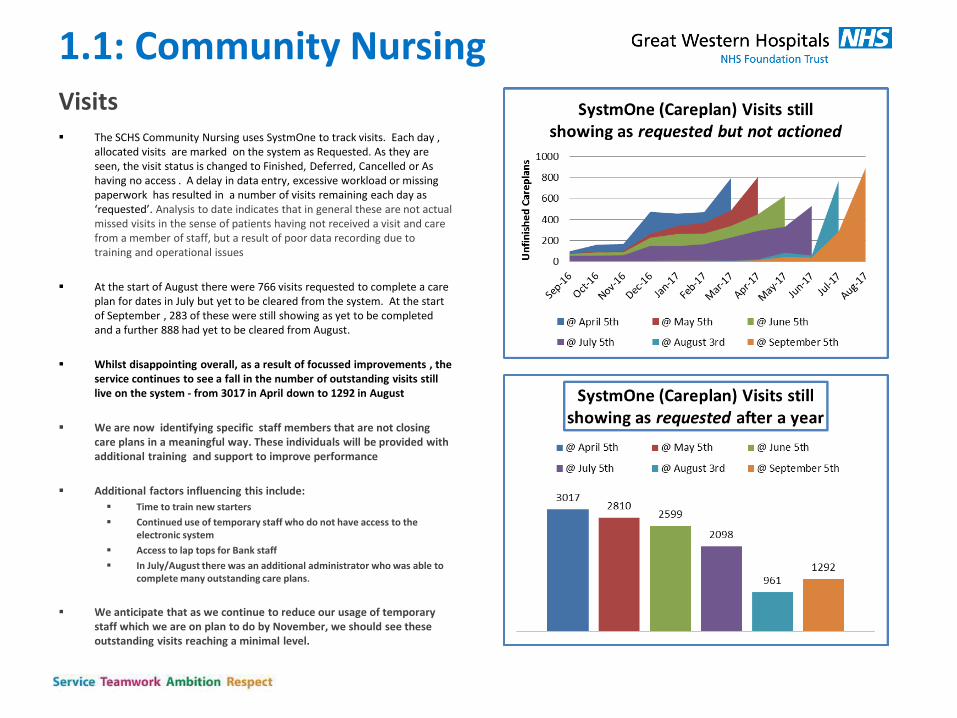
allocated visits are marked on the system as Requested. As they are seen, the visit status is changed to Finished, Deferred, Cancelled or As having no access . A delay in data entry, excessive workload or missing paperwork has resulted in a number of visits remaining each day as ‘requested’. Analysis to date indicates that in general these are not actual missed visits in the sense of patients having not received a visit and care from a member of staff, but a result of poor data recording due to training and operational issues
At the start of August there were 766 visits requested to complete a care plan for dates in July but yet to be cleared from the system. At the start of September , 283 of these were still showing as yet to be completed and a further 888 had yet to be cleared from August.
Whilst disappointing overall, as a result of focussed improvements , the service continues to see a fall in the number of outstanding visits still live on the system - from 3017 in April down to 1292 in August
We are now identifying specific staff members that are not closing care plans in a meaningful way. These individuals will be provided with additional training and support to improve performance
Additional factors influencing this include:
Time to train new starters
Continued use of temporary staff who do not have access to the electronic system
Access to lap tops for Bank staff
In July/August there was an additional administrator who was able to complete many outstanding care plans.
We anticipate that as we continue to reduce our usage of temporary staff which we are on plan to do by November, we should see these outstanding visits reaching a minimal level.
1.1: Community Nursing (cont) Visits Community Nursing Service Issues
Bank and Agency staff may finish their shifts late and
often do not drop off the care plans in a timely way or procedural way
Bank/Agency Staff who only work odd days at short notice, or who work weekend only, can be difficult to plan S1 training for. As it would not be cost effective to provide them with a lap top they are provided with paper care plans to complete.
Agency and bank staff are required to undertake patient care and visits as the priority and therefore arranging training for them adds pressure on the service.
In July/August there was an additional administrator who was able to complete many outstanding care plans.
Historic care plans are outdated and contain unnecessary instructions (e.g. wash your hands, open the dressing pack, lay out the towel, make the patient comfortable ) All of these actions have to be ‘completed’ on the paper care plan or on S1 in order to ‘perform’ and complete the care plan. If the nurse has not ticked on the paper care plan , or written a comment, the ward clerk, with no clinical knowledge, has to seek advice as to whether this action was performed causing a delay in ‘performing and completing’ a care plan
A number of IT issues have led to staff not being able to log onto the system. This is compounded by not having access to IT staff, to deal with these issues immediately.
There have been problems around scheduling SystmOne training for staff.
There is evidence of patients having duplicate care plans Staff complain of a lack of time and resource to
complete the paper care plans at a time of record caseload.
Community Nursing Service plans in place • 3 new Band 5 staff are currently being inducted • Band 6 due to start in 2/52 and the second band 6 waiting
for her DBS • Waiting for DBS on Band 3 and another Band 3 to start
within the next few days • 7 interviews taking place this coming Thursday for just over
5. WTE Band 5 nurses • Over 70 applicants for Band 3 post and 7 shortlisted –
interview date TBC • Expression of interest for Band 7 team leader post out to
advert internally for 6/12 secondment • Band 7 with substantive post as team leader due back on 1st
October • 2 bank Paramedics have completed S1 training and 1 will be
provided with a lap top as will be committing to regular weekly shifts
• 5 of our own staff have requested application forms to join the bank
• Increased staffing will reduce the number of visits the nurses have to a more manageable amount.
• A training schedule is in place to ensure all staff receive the relevant training in a timely manner
• Staff finishing late will have the procedure for dropping off paperwork explained clearly to them
• There will be a focus on supervision and caseload management gong forward .
• Increased timeliness of data input will lead to fewer inappropriate visits.
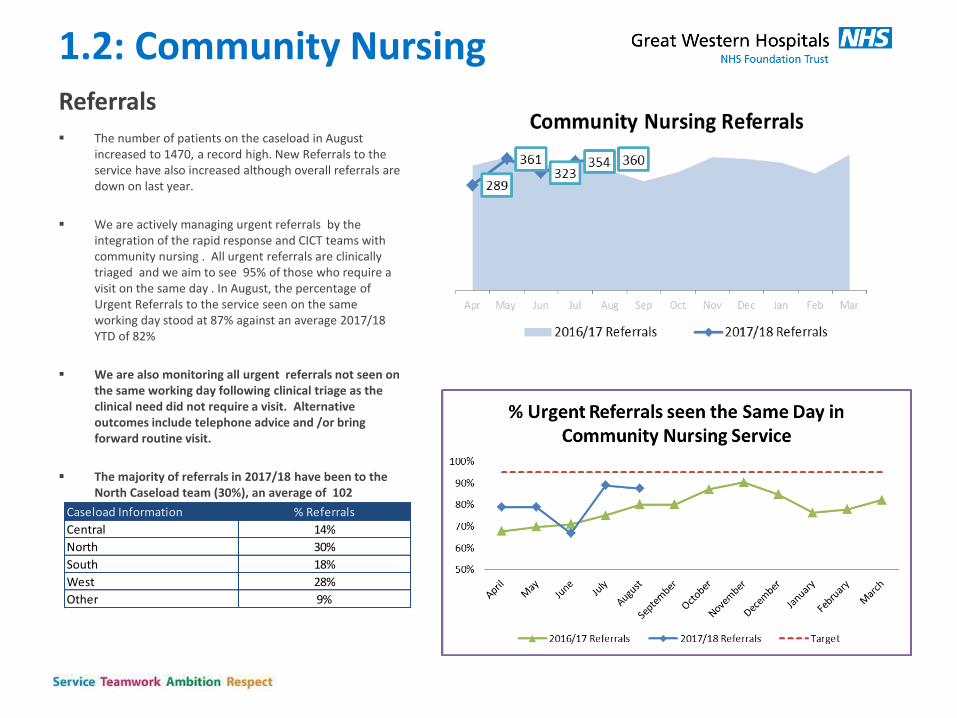
1.2: Community Nursing Referrals The number of patients on the caseload in August
increased to 1470, a record high. New Referrals to the service have also increased although overall referrals are down on last year.
We are actively managing urgent referrals by the integration of the rapid response and CICT teams with community nursing . All urgent referrals are clinically triaged and we aim to see 95% of those who require a visit on the same day . In August, the percentage of Urgent Referrals to the service seen on the same working day stood at 87% against an average 2017/18 YTD of 82%
We are also monitoring all urgent referrals not seen on the same working day following clinical triage as the clinical need did not require a visit. Alternative outcomes include telephone advice and /or bring forward routine visit.
The majority of referrals in 2017/18 have been to the North Caseload team (30%), an average of 102 referrals per month.
Caseload Information % Referrals
Central 14%
North 30%
South 18%
West 28%
Other 9%
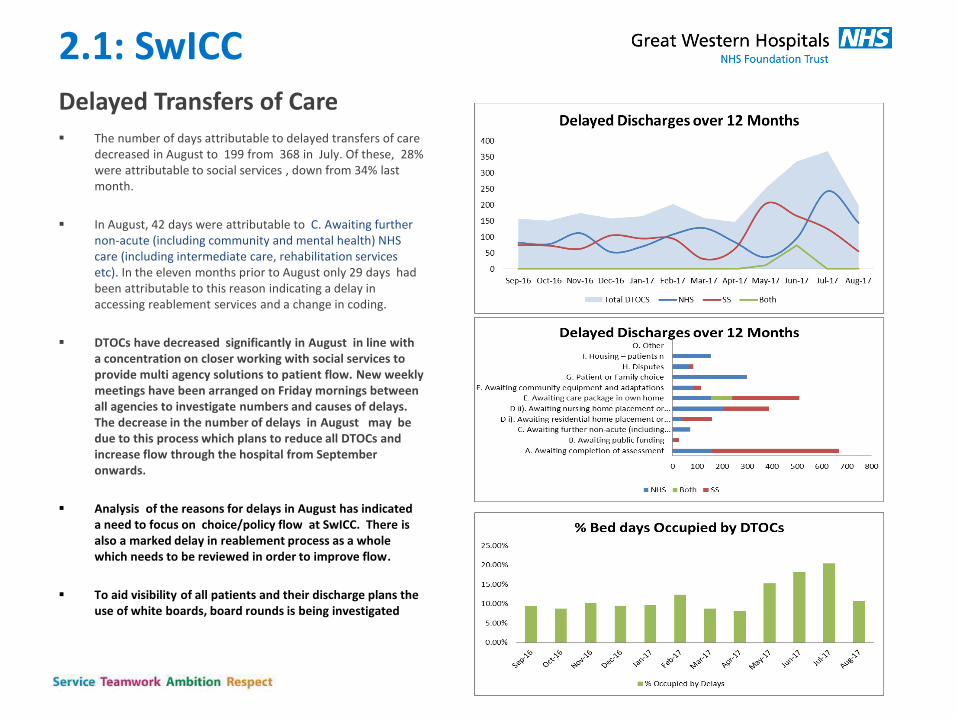
2.1: SwICC Delayed Transfers of Care The number of days attributable to delayed transfers of care
decreased in August to 199 from 368 in July. Of these, 28% were attributable to social services , down from 34% last month.
In August, 42 days were attributable to C. Awaiting further non-acute (including community and mental health) NHS care (including intermediate care, rehabilitation services etc). In the eleven months prior to August only 29 days had been attributable to this reason indicating a delay in accessing reablement services and a change in coding.
DTOCs have decreased significantly in August in line with a concentration on closer working with social services to provide multi agency solutions to patient flow. New weekly meetings have been arranged on Friday mornings between all agencies to investigate numbers and causes of delays. The decrease in the number of delays in August may be due to this process which plans to reduce all DTOCs and increase flow through the hospital from September onwards.
Analysis of the reasons for delays in August has indicated a need to focus on choice/policy flow at SwICC. There is also a marked delay in reablement process as a whole which needs to be reviewed in order to improve flow.
To aid visibility of all patients and their discharge plans the use of white boards, board rounds is being investigated
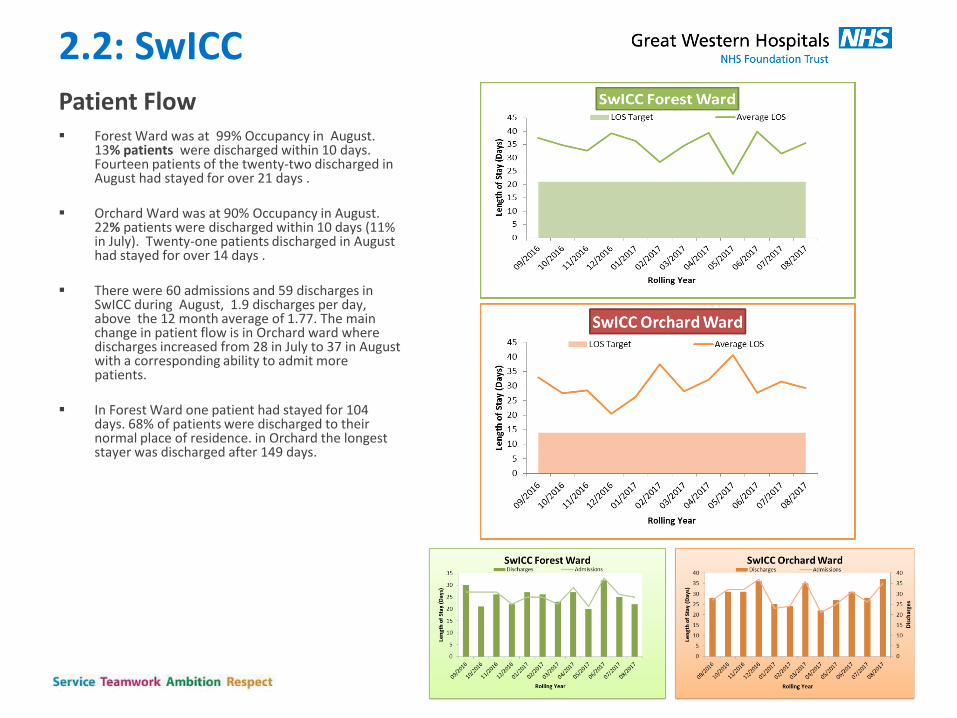
2.2: SwICC Patient Flow Forest Ward was at 99% Occupancy in August.
13% patients were discharged within 10 days. Fourteen patients of the twenty-two discharged in August had stayed for over 21 days .
Orchard Ward was at 90% Occupancy in August. 22% patients were discharged within 10 days (11% in July). Twenty-one patients discharged in August had stayed for over 14 days .
There were 60 admissions and 59 discharges in SwICC during August, 1.9 discharges per day, above the 12 month average of 1.77. The main change in patient flow is in Orchard ward where discharges increased from 28 in July to 37 in August with a corresponding ability to admit more patients.
In Forest Ward one patient had stayed for 104 days. 68% of patients were discharged to their normal place of residence. in Orchard the longest stayer was discharged after 149 days.
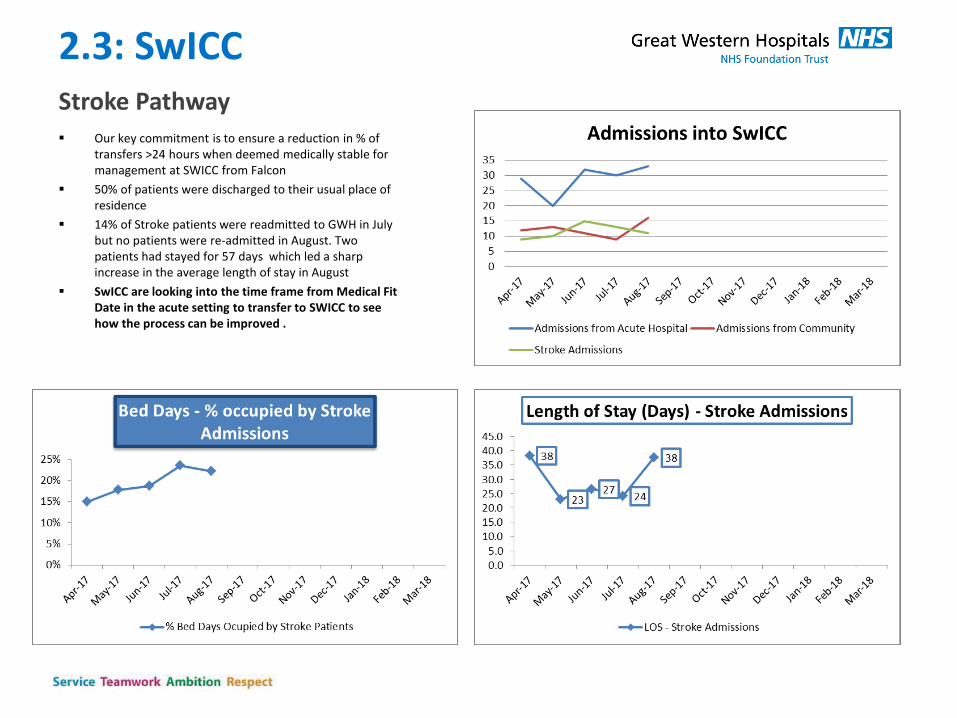
2.3: SwICC Stroke Pathway Our key commitment is to ensure a reduction in % of
transfers >24 hours when deemed medically stable for management at SWICC from Falcon
50% of patients were discharged to their usual place of residence
14% of Stroke patients were readmitted to GWH in July but no patients were re-admitted in August. Two patients had stayed for 57 days which led a sharp increase in the average length of stay in August
SwICC are looking into the time frame from Medical Fit Date in the acute setting to transfer to SWICC to see how the process can be improved .
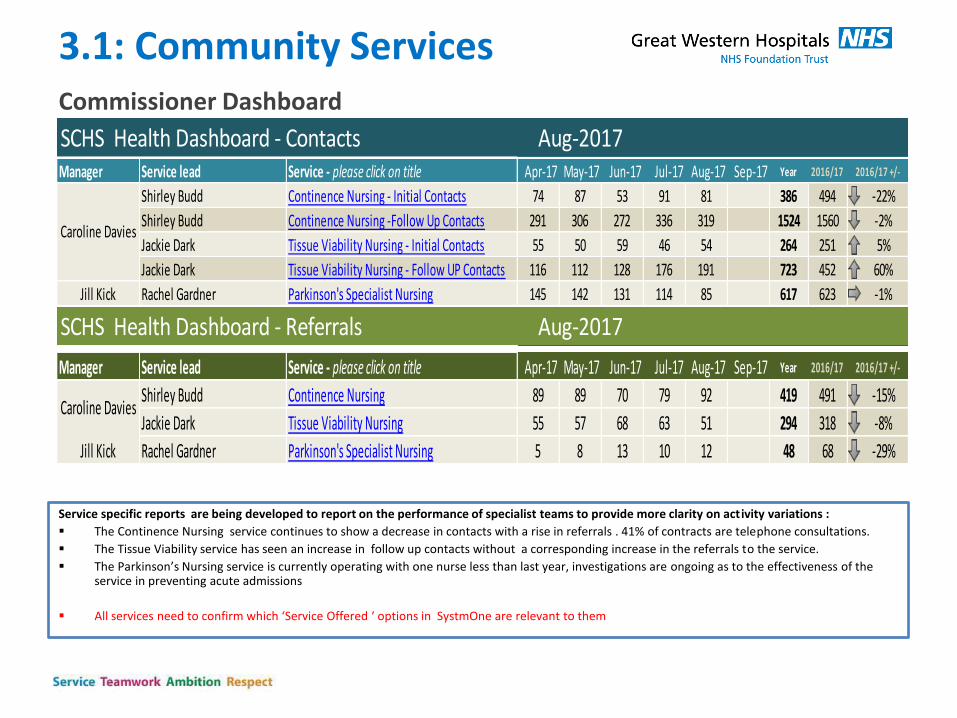
3.1: Community Services Commissioner Dashboard
Service specific reports are being developed to report on the performance of specialist teams to provide more clarity on activity variations :
The Continence Nursing service continues to show a decrease in contacts with a rise in referrals . 41% of contracts are telephone consultations.
The Tissue Viability service has seen an increase in follow up contacts without a corresponding increase in the referrals to the service.
The Parkinson’s Nursing service is currently operating with one nurse less than last year, investigations are ongoing as to the effectiveness of the service in preventing acute admissions
All services need to confirm which ‘Service Offered ‘ options in SystmOne are relevant to them
Aug-2017SCHS Health Dashboard - ContactsManager Service lead Service - please click on title Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Year 2016/17 2016/17 +/-
Shirley Budd Continence Nursing - Initial Contacts 74 87 53 91 81 386 494 -22%
Shirley Budd Continence Nursing -Follow Up Contacts 291 306 272 336 319 1524 1560 -2%
Jackie Dark Tissue Viability Nursing - Initial Contacts 55 50 59 46 54 264 251 5%
Jackie Dark Tissue Viability Nursing - Follow UP Contacts 116 112 128 176 191 723 452 60%
Jill Kick Rachel Gardner Parkinson's Specialist Nursing 145 142 131 114 85 617 623 -1%
Caroline Davies
SCHS Health Dashboard - Referrals Aug-2017
Manager Service lead Service - please click on title Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Year 2016/17 2016/17 +/-
Shirley Budd Continence Nursing 89 89 70 79 92 419 491 -15%
Jackie Dark Tissue Viability Nursing 55 57 68 63 51 294 318 -8%
Jill Kick Rachel Gardner Parkinson's Specialist Nursing 5 8 13 10 12 48 68 -29%
Caroline Davies
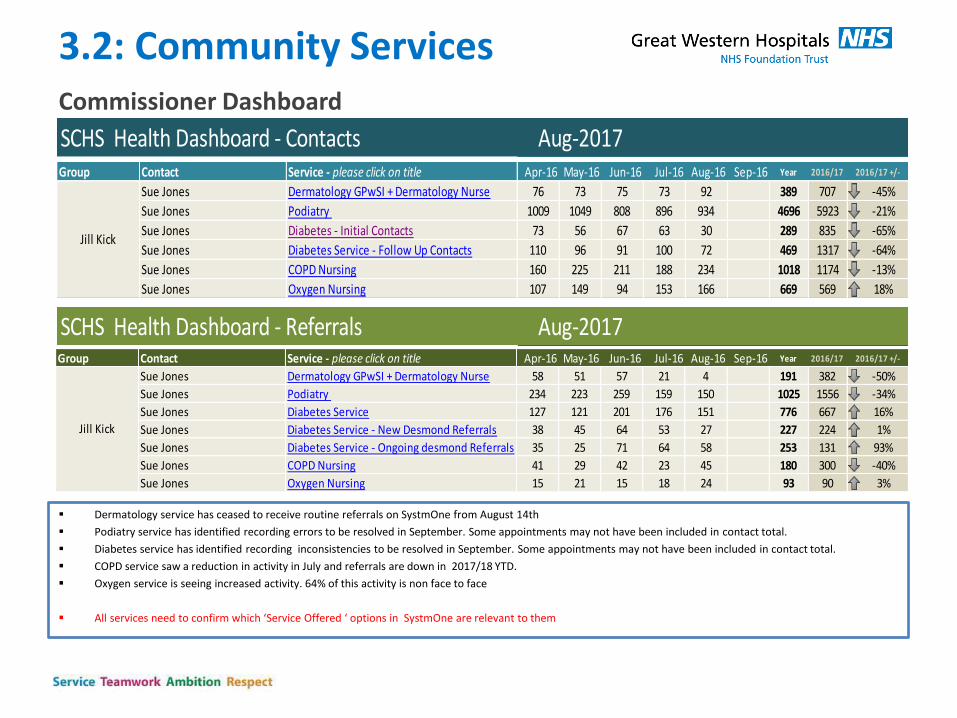
3.2: Community Services Commissioner Dashboard
Dermatology service has ceased to receive routine referrals on SystmOne from August 14th
Podiatry service has identified recording errors to be resolved in September. Some appointments may not have been included in contact total.
Diabetes service has identified recording inconsistencies to be resolved in September. Some appointments may not have been included in contact total.
COPD service saw a reduction in activity in July and referrals are down in 2017/18 YTD.
Oxygen service is seeing increased activity. 64% of this activity is non face to face
All services need to confirm which ‘Service Offered ‘ options in SystmOne are relevant to them
Aug-2017SCHS Health Dashboard - Contacts
SCHS Health Dashboard - Referrals Aug-2017
Group Contact Service - please click on title Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Year 2016/17 2016/17 +/-
Sue Jones Dermatology GPwSI + Dermatology Nurse 76 73 75 73 92 389 707 -45%
Sue Jones Podiatry 1009 1049 808 896 934 4696 5923 -21%
Sue Jones Diabetes - Initial Contacts 73 56 67 63 30 289 835 -65%
Sue Jones Diabetes Service - Follow Up Contacts 110 96 91 100 72 469 1317 -64%
Sue Jones COPD Nursing 160 225 211 188 234 1018 1174 -13%
Sue Jones Oxygen Nursing 107 149 94 153 166 669 569 18%
Jill Kick
Group Contact Service - please click on title Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Year 2016/17 2016/17 +/-
Sue Jones Dermatology GPwSI + Dermatology Nurse 58 51 57 21 4 191 382 -50%
Sue Jones Podiatry 234 223 259 159 150 1025 1556 -34%
Sue Jones Diabetes Service 127 121 201 176 151 776 667 16%
Sue Jones Diabetes Service - New Desmond Referrals 38 45 64 53 27 227 224 1%
Sue Jones Diabetes Service - Ongoing desmond Referrals 35 25 71 64 58 253 131 93%
Sue Jones COPD Nursing 41 29 42 23 45 180 300 -40%
Sue Jones Oxygen Nursing 15 21 15 18 24 93 90 3%
Jill Kick
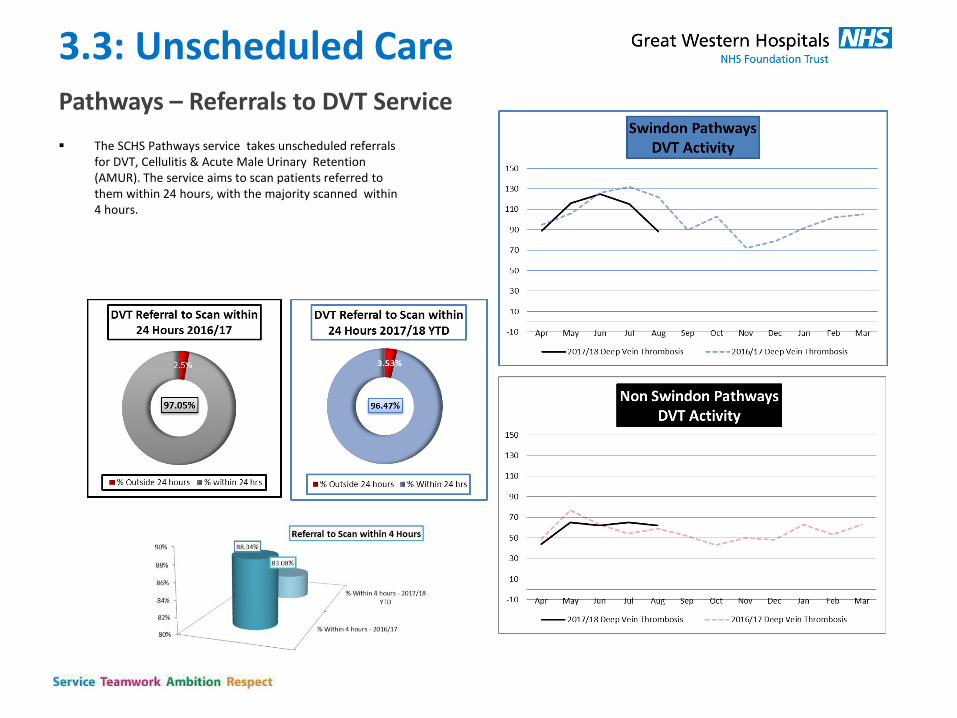
3.3: Unscheduled Care Pathways – Referrals to DVT Service
The SCHS Pathways service takes unscheduled referrals for DVT, Cellulitis & Acute Male Urinary Retention (AMUR). The service aims to scan patients referred to them within 24 hours, with the majority scanned within 4 hours.
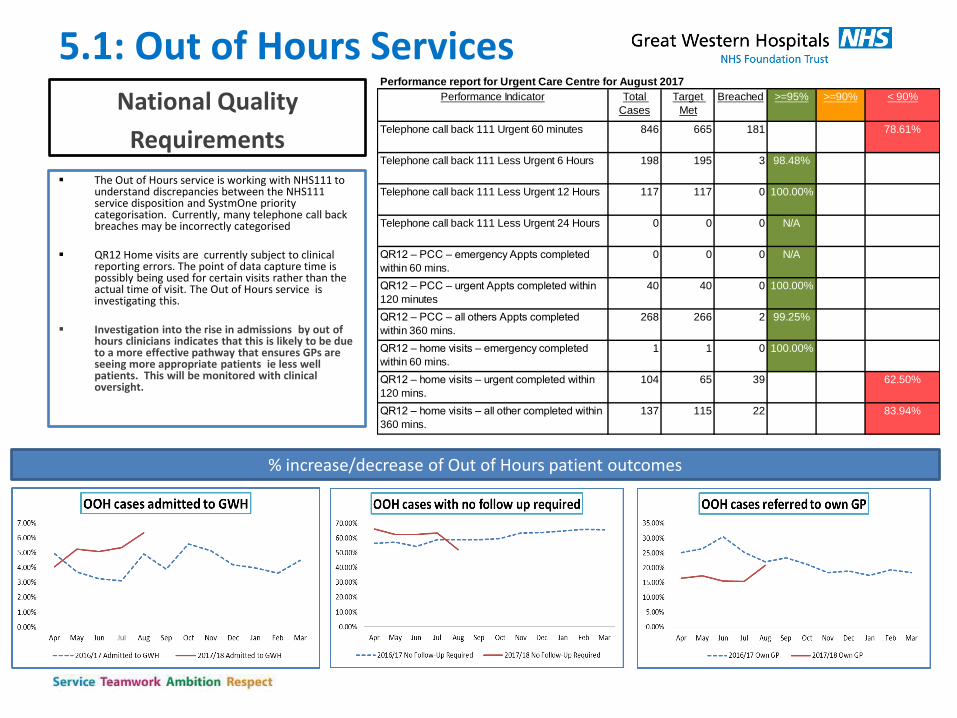
5.1: Out of Hours Services National Quality
Requirements
The Out of Hours service is working with NHS111 to understand discrepancies between the NHS111 service disposition and SystmOne priority categorisation. Currently, many telephone call back breaches may be incorrectly categorised
QR12 Home visits are currently subject to clinical reporting errors. The point of data capture time is possibly being used for certain visits rather than the actual time of visit. The Out of Hours service is investigating this.
Investigation into the rise in admissions by out of
hours clinicians indicates that this is likely to be due to a more effective pathway that ensures GPs are seeing more appropriate patients ie less well patients. This will be monitored with clinical oversight.
% increase/decrease of Out of Hours patient outcomes
Performance report for Urgent Care Centre for August 2017
Breached
846 665 181 78.61%
198 195 3 98.48%
117 117 0 100.00%
0 0 0 N/A
0 0 0 N/A
40 40 0 100.00%
268 266 2 99.25%
1 1 0 100.00%
104 65 39 62.50%
137 115 22 83.94%
QR12 – home visits – urgent completed within
120 mins.
QR12 – home visits – all other completed within
360 mins.
QR12 – PCC – urgent Appts completed within
120 minutes
QR12 – PCC – all others Appts completed
within 360 mins.
QR12 – home visits – emergency completed
within 60 mins.
QR12 – PCC – emergency Appts completed
within 60 mins.
Telephone call back 111 Urgent 60 minutes
Telephone call back 111 Less Urgent 6 Hours
Telephone call back 111 Less Urgent 12 Hours
Telephone call back 111 Less Urgent 24 Hours
< 90%>=90%Performance Indicator Total
Cases
Target
Met
>=95%
Emergency Department Quality & Safety Dashboard
ED Tri : Chris Bull - Matron, Dr Steve Haig - Clinical Lead & Emma White - Head of Service
Emergency Department Safety Dashboard Report Ran: By: Gary Crisp
Emergency Care Quality Dashboard Report Ran: By: Jessica Close
Month: Aug-17
Aim: To provide a summarised overview of Emergency Department quality and safety data
Performance Quality Audit Patient
Experience Workforce
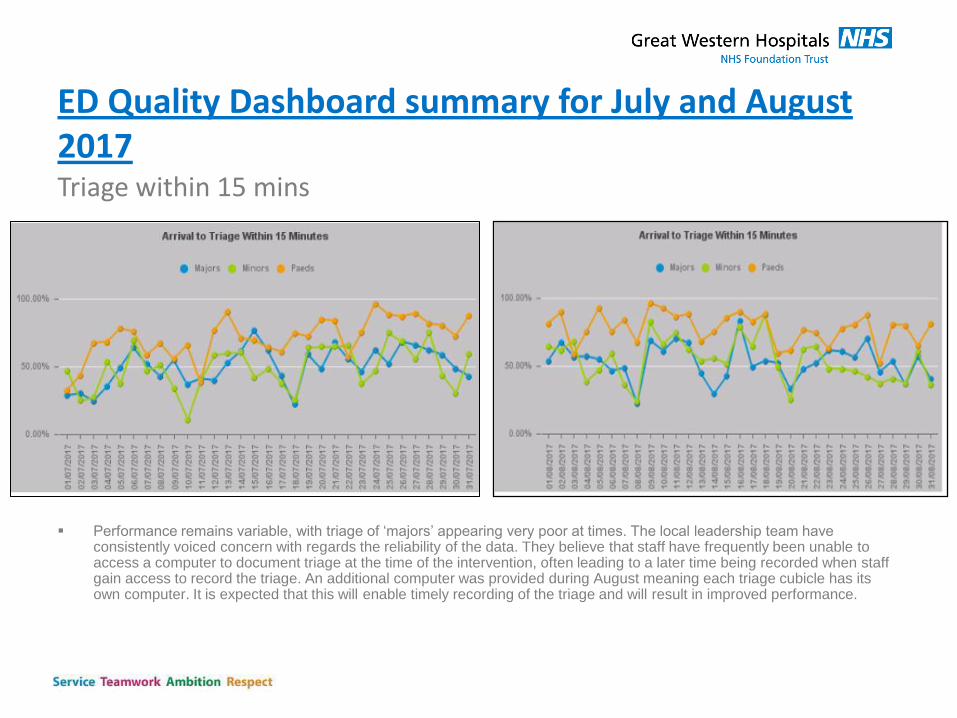
ED Quality Dashboard summary for July and August 2017 Triage within 15 mins
Performance remains variable, with triage of ‘majors’ appearing very poor at times. The local leadership team have
consistently voiced concern with regards the reliability of the data. They believe that staff have frequently been unable to access a computer to document triage at the time of the intervention, often leading to a later time being recorded when staff gain access to record the triage. An additional computer was provided during August meaning each triage cubicle has its own computer. It is expected that this will enable timely recording of the triage and will result in improved performance.
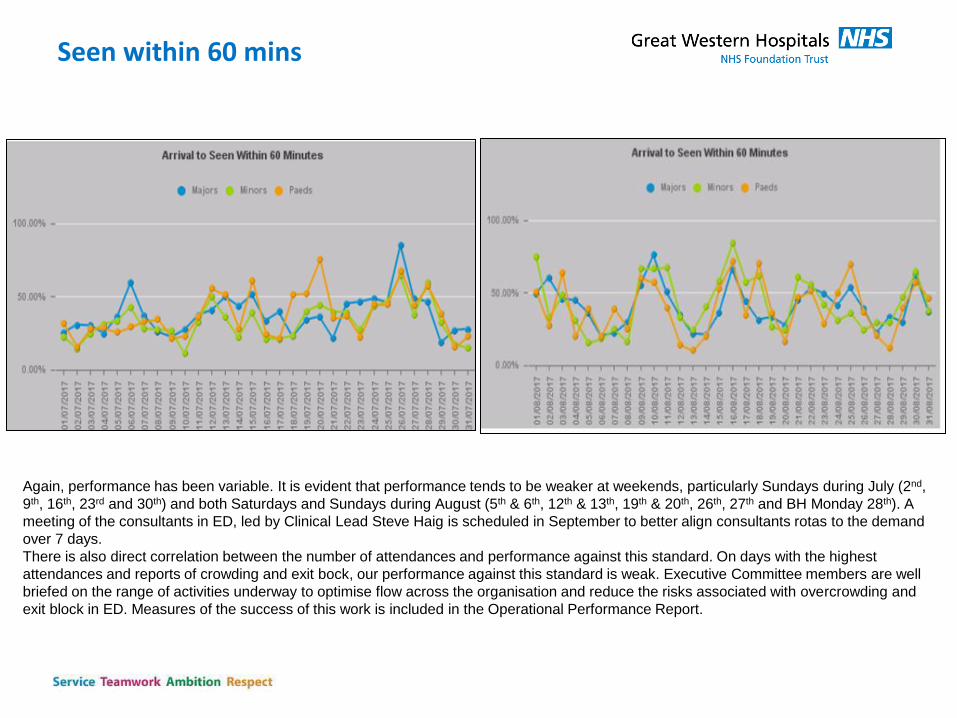
Seen within 60 mins
Again, performance has been variable. It is evident that performance tends to be weaker at weekends, particularly Sundays during July (2nd,
9th, 16th, 23rd and 30th) and both Saturdays and Sundays during August (5th & 6th, 12th & 13th, 19th & 20th, 26th, 27th and BH Monday 28th). A
meeting of the consultants in ED, led by Clinical Lead Steve Haig is scheduled in September to better align consultants rotas to the demand
over 7 days.
There is also direct correlation between the number of attendances and performance against this standard. On days with the highest
attendances and reports of crowding and exit bock, our performance against this standard is weak. Executive Committee members are well
briefed on the range of activities underway to optimise flow across the organisation and reduce the risks associated with overcrowding and
exit block in ED. Measures of the success of this work is included in the Operational Performance Report.
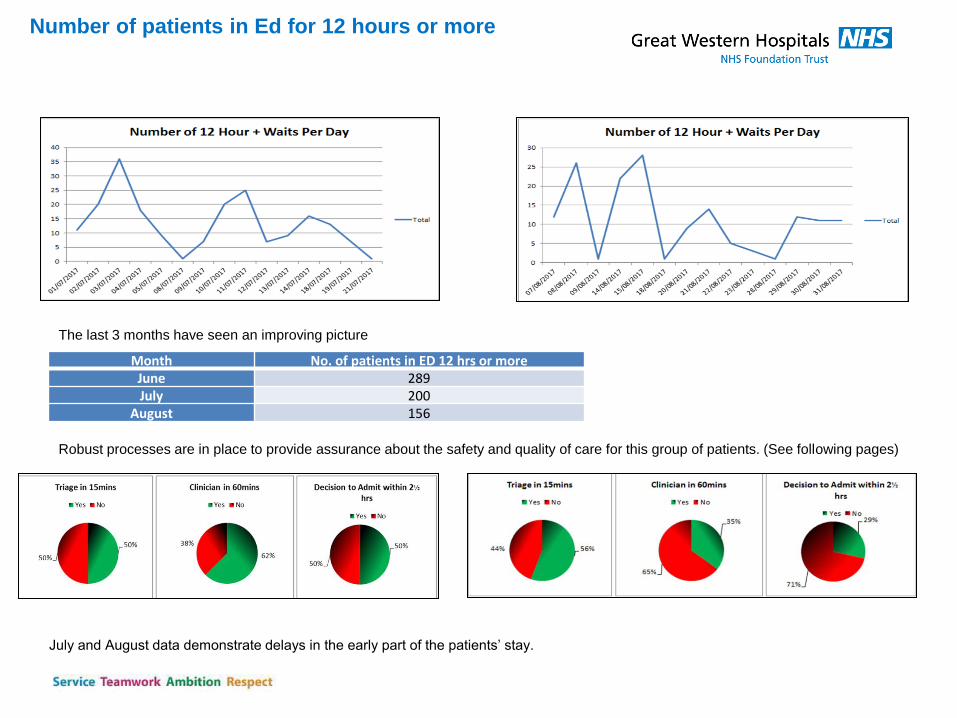
Number of patients in Ed for 12 hours or more
The last 3 months have seen an improving picture
Month No. of patients in ED 12 hrs or more
June 289
July 200
August 156
Robust processes are in place to provide assurance about the safety and quality of care for this group of patients. (See following pages)
July and August data demonstrate delays in the early part of the patients’ stay.
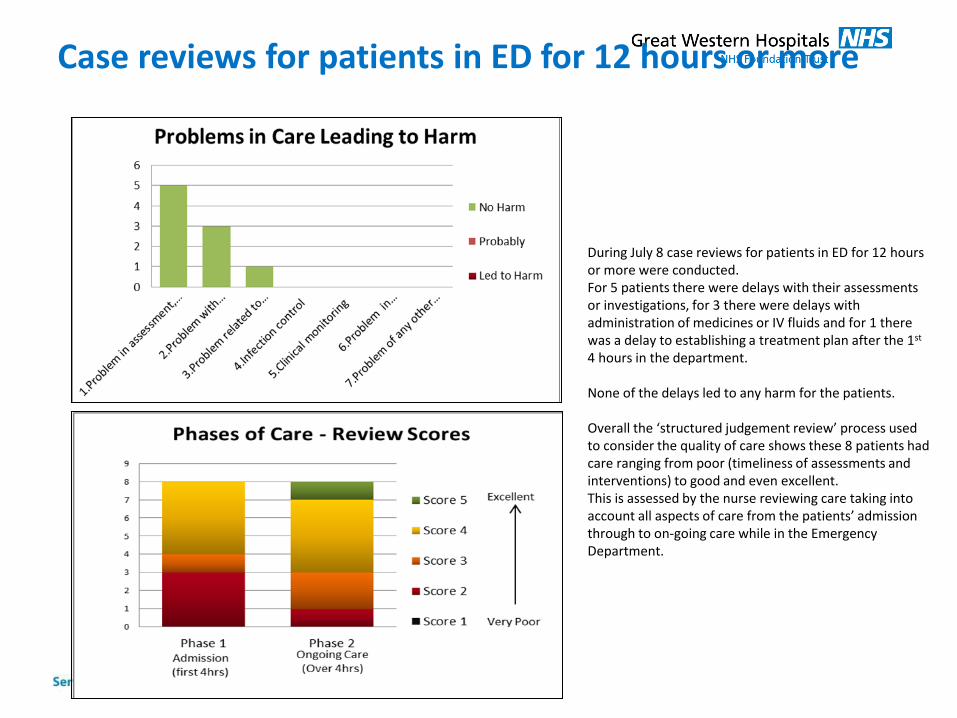
Case reviews for patients in ED for 12 hours or more
During July 8 case reviews for patients in ED for 12 hours or more were conducted. For 5 patients there were delays with their assessments or investigations, for 3 there were delays with administration of medicines or IV fluids and for 1 there was a delay to establishing a treatment plan after the 1st 4 hours in the department. None of the delays led to any harm for the patients. Overall the ‘structured judgement review’ process used to consider the quality of care shows these 8 patients had care ranging from poor (timeliness of assessments and interventions) to good and even excellent. This is assessed by the nurse reviewing care taking into account all aspects of care from the patients’ admission through to on-going care while in the Emergency Department.
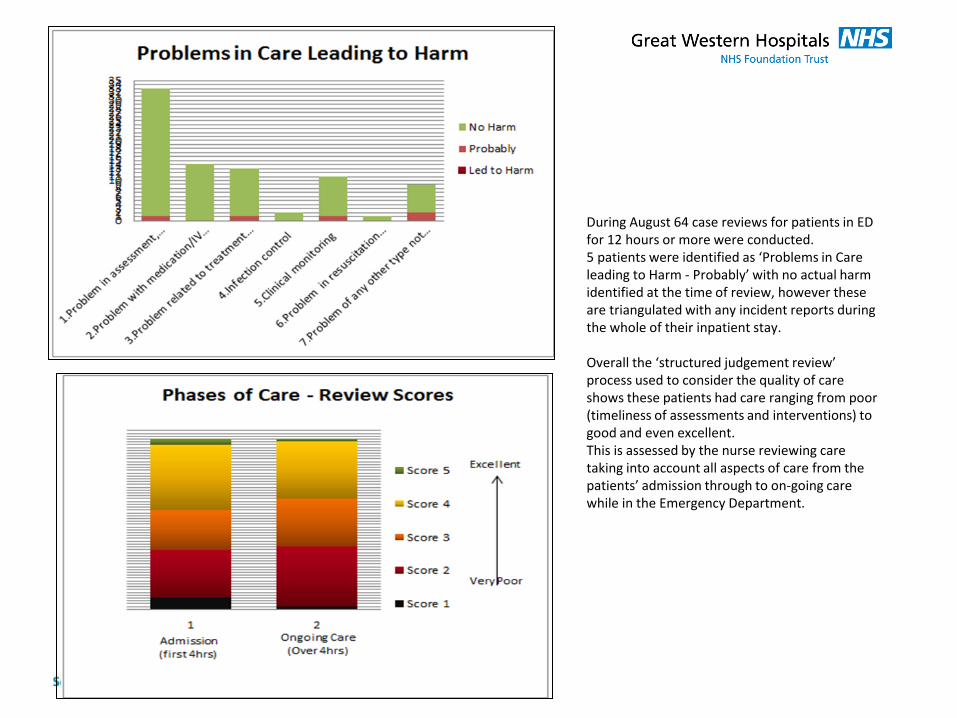
During August 64 case reviews for patients in ED for 12 hours or more were conducted. 5 patients were identified as ‘Problems in Care leading to Harm - Probably’ with no actual harm identified at the time of review, however these are triangulated with any incident reports during the whole of their inpatient stay. Overall the ‘structured judgement review’ process used to consider the quality of care shows these patients had care ranging from poor (timeliness of assessments and interventions) to good and even excellent. This is assessed by the nurse reviewing care taking into account all aspects of care from the patients’ admission through to on-going care while in the Emergency Department.
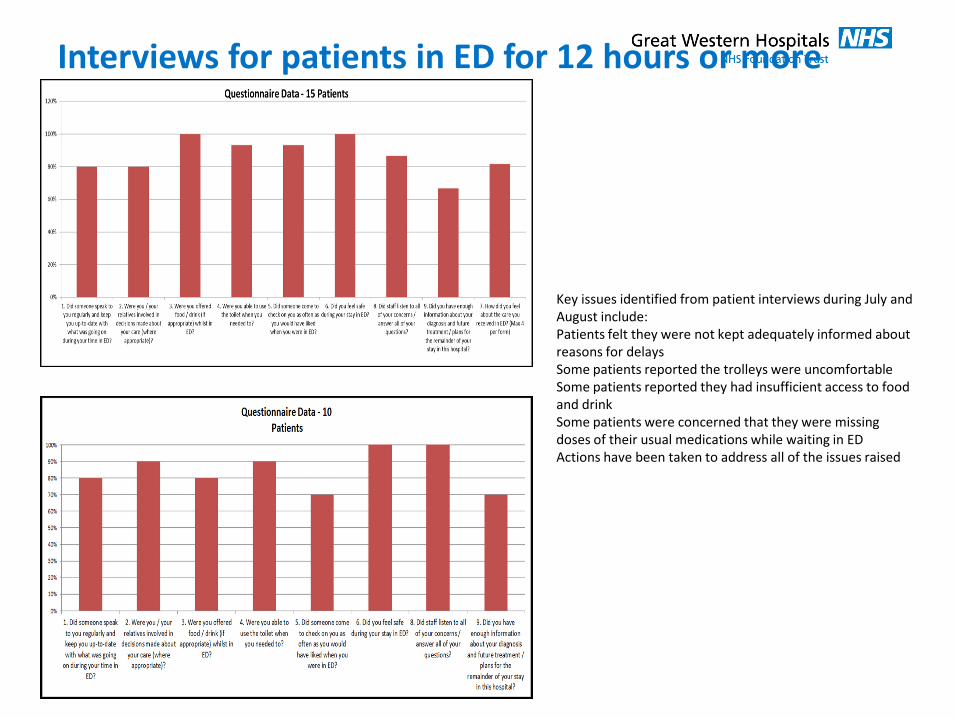
Interviews for patients in ED for 12 hours or more
Key issues identified from patient interviews during July and August include: Patients felt they were not kept adequately informed about reasons for delays Some patients reported the trolleys were uncomfortable Some patients reported they had insufficient access to food and drink Some patients were concerned that they were missing doses of their usual medications while waiting in ED Actions have been taken to address all of the issues raised
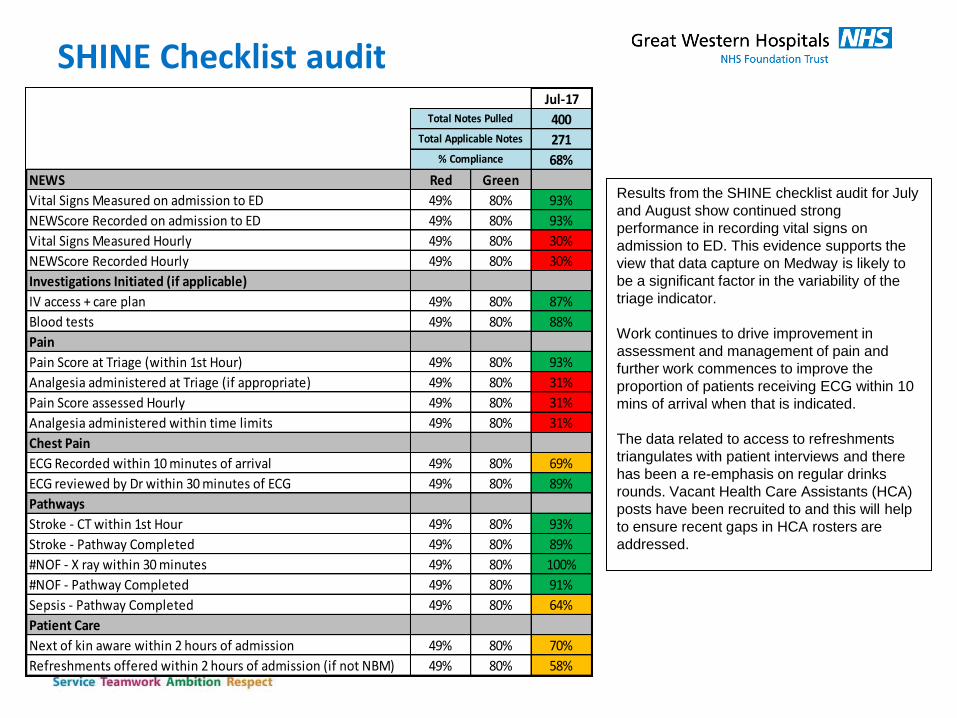
SHINE Checklist audit Jul-17
400
271
68%
NEWS Red Green
Vital Signs Measured on admission to ED 49% 80% 93%
NEWScore Recorded on admission to ED 49% 80% 93%
Vital Signs Measured Hourly 49% 80% 30%
NEWScore Recorded Hourly 49% 80% 30%
Investigations Initiated (if applicable)
IV access + care plan 49% 80% 87%
Blood tests 49% 80% 88%
Pain
Pain Score at Triage (within 1st Hour) 49% 80% 93%
Analgesia administered at Triage (if appropriate) 49% 80% 31%
Pain Score assessed Hourly 49% 80% 31%
Analgesia administered within time limits 49% 80% 31%
Chest Pain
ECG Recorded within 10 minutes of arrival 49% 80% 69%
ECG reviewed by Dr within 30 minutes of ECG 49% 80% 89%
Pathways
Stroke - CT within 1st Hour 49% 80% 93%
Stroke - Pathway Completed 49% 80% 89%
#NOF - X ray within 30 minutes 49% 80% 100%
#NOF - Pathway Completed 49% 80% 91%
Sepsis - Pathway Completed 49% 80% 64%
Patient Care
Next of kin aware within 2 hours of admission 49% 80% 70%
Refreshments offered within 2 hours of admission (if not NBM) 49% 80% 58%
Total Applicable Notes
Total Notes Pulled
% Compliance
Results from the SHINE checklist audit for July
and August show continued strong
performance in recording vital signs on
admission to ED. This evidence supports the
view that data capture on Medway is likely to
be a significant factor in the variability of the
triage indicator.
Work continues to drive improvement in
assessment and management of pain and
further work commences to improve the
proportion of patients receiving ECG within 10
mins of arrival when that is indicated.
The data related to access to refreshments
triangulates with patient interviews and there
has been a re-emphasis on regular drinks
rounds. Vacant Health Care Assistants (HCA)
posts have been recruited to and this will help
to ensure recent gaps in HCA rosters are
addressed.