allergy and parasites
TRANSCRIPT

Allergy and Parasites
Journal of Parasitology Research
Guest Editors:Fabrizio Bruschi, Maria Ilma Araujo, William Harnett, and Elena Pinelli

Allergy and Parasites

Journal of Parasitology Research
Allergy and Parasites
Guest Editors: Fabrizio Bruschi, Maria Ilma Araujo,William Harnett, and Elena Pinelli

Copyright © 2013 Hindawi Publishing Corporation. All rights reserved.
This is a special issue published in “Journal of Parasitology Research.” All articles are open access articles distributed under the CreativeCommons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the originalwork is properly cited.

Editorial Board
Takeshi Agatsuma, JapanJeffrey Bethony, USAD. D. Chadee, USAKwang Poo Chang, USAWej Choochote, ThailandAlvin A. Gajadhar, CanadaC. Genchi, ItalyBoyko B. Georgiev, Bulgaria
Ana Maria Jansen, BrazilMaria V. Johansen, DenmarkNirbhay Kumar, USAD. S. Lindsay, USABernard Marchand, FranceRenato A. Mortara, BrazilDomenico Otranto, ItalyBarbara Papadopoulou, Canada
A. F. Petavy, FranceBenjamin M. Rosenthal, USAJoseph Schrevel, FranceJose F. Silveira, BrazilM. J. Stear, UKXin-zhuan Su, USAKazuyuki Tanabe, Japan

Contents
Allergy and Parasites, Fabrizio Bruschi, Maria Ilma Araujo, William Harnett, and Elena PinelliVolume 2013, Article ID 502562, 2 pages
Mast Cell Subsets and Their Functional Modulation by the Acanthocheilonema viteae Product ES-62,Dimity H. Ball, Hwee Kee Tay, Kara S. Bell, Michelle L. Coates, Lamyaa Al-Riyami, Justyna Rzepecka,William Harnett, and Margaret M. HarnettVolume 2013, Article ID 961268, 13 pages
Helminths: Immunoregulation and Inflammatory Diseases—Which Side Are Trichinella spp. andToxocara spp. on?, Carmen Aranzamendi, Ljiljana Sofronic-Milosavljevic, and Elena PinelliVolume 2013, Article ID 329438, 11 pages
Human Schistosome Infection and Allergic Sensitisation, Nadine Rujeni, David W. Taylor,and Francisca MutapiVolume 2012, Article ID 154743, 17 pages
Risk Factors for Asthma in a Helminth Endemic Area in Bahia, Brazil, Luciana S. Cardoso,Daniela M. Costa, Maria Cecılia F. Almeida, Robson P. Souza, Edgar M. Carvalho, Maria Ilma Araujo,and Ricardo R. OliveiraVolume 2012, Article ID 796820, 8 pages
The Effect of Antihelminthic Treatment on Subjects with Asthma from an Endemic Area ofSchistosomiasis: A Randomized, Double-Blinded, and Placebo-Controlled Trial,Maria Cecilia F. Almeida, Givaneide S. Lima, Luciana S. Cardoso, Robson P. de Souza, Regis A. Campos,Alvaro A. Cruz, Joanemile P. Figueiredo, Ricardo R. Oliveira, Edgar M. Carvalho, and Maria Ilma AraujoVolume 2012, Article ID 296856, 11 pages

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2013, Article ID 502562, 2 pageshttp://dx.doi.org/10.1155/2013/502562
EditorialAllergy and Parasites
Fabrizio Bruschi,1 Maria Ilma Araujo,2 William Harnett,3 and Elena Pinelli4
1 Department of Translational Research and New Technologies in Medicine and Surgery, University of Pisa, 56126 Pisa, Italy2 Serviço de Imunologia, Universidade Federal da Bahia (UFBA), 40110-160 Salvador, BA, Brazil3 Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow G4 0RE, UK4Centre for Infectious Disease Control Netherlands, National Institute of Public Health and the Environment (RIVM),Bilthoven 3720 BA, e Netherlands
Correspondence should be addressed to Fabrizio Bruschi; [email protected]
Received 12 December 2012; Accepted 12 December 2012
Copyright © 2013 Fabrizio Bruschi et al. is is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
It is estimated that at least one-��h of the world�s populationsuffers from allergic diseases (atopic asthma and allergicrhinitis are the most common). Different factors contributeto the development of allergies; a predisposing genetic back-ground is needed; however, environmental factors play animportant role, among them is the exposure to infectiousagents.
Allergy is increasing in the recent decades particularly inWestern industrialized countries, and according to the so-called hygiene hypothesis this might be ascribable to the lowerexposure to infectious agents, including parasitic helminths.e reasons for such a situation are several: small family size,stability of intestinal micro�ora, a�uent urban homes, highuse of antibiotics, good sanitation which means low oral-fecal pathogen burden, and �nally low or absent helminthinfections. On the other hand, the low prevalence of atopyin developing countries is generally associated with highexposure to parasites in these regions.
e hygiene hypothesis has been revisited pointing out,for example, the role of IL-10-producing Treg cells, which areinduced during chronic infections and play an essential rolein downregulating allergic responses.
To verify the above hypotheses, a number of publicationshave appeared, studying the effects of parasitic infections orof molecules derived from parasites on the well-establishedexperimental models of allergy, along with epidemiologicalstudies, which have tried to correlate these conditions.
is special issue on allergy and parasites is composed ofpapers, which address this topic.
A review by N. Rujeni et al. focuses on the relationshipbetween helminth parasites and allergic reactivity, takinginto account the new concept to explain why 2 immuneresponses have evolved.e2 response has been associatedwith host resistance to helminth infections and generallyconsidered a harmfully allergic response. e review dis-cusses these concepts and also the mechanisms underlyingthe interface between allergy and helminth infections and theevolutionary processes of the immune response associatedwith these conditions.
In the paper by D. Ball et al., the in�uence of ES-62,a glycoprotein produced by Acanthocheilonema viteae, onthe activity of mast cells of different sources (peritoneal,connective tissue, and bone marrow derived) was assayed,comparing surface phenotype, degranulation responses toLPS and Fc𝜀𝜀R1 cross-linking, and cytokine production inresponse to those stimuli. e authors show the activationpathways in mouse mast cells that may be altered by ES-62. ese results will advance our understanding of theimmunomodulatory activity directed against the allergyeffector cells by this parasite-derived glycoprotein.
C. Aranzamendi et al. observe that the associationbetween allergy and helminth infections is not always thesame. ese authors review the literature on some of thecell types that play an essential role in helminth-inducedimmunoregulation and the conse�uences for in�ammatorydiseases. In addition, epidemiological as well as experimen-tal studies indicating the contrasting effects of Toxocaraand Trichinella infection on allergic asthma are discussed.

2 Journal of Parasitology Research
According to the authors, this diversity might depend on thehelminth species, whether it is a chronic or acute infection,the different role played by the host in the various infections(natural or occasional), as well as on the different life cycles inwhich the parasite may affect the lung (in toxocarsis) or not(in trichinellosis), and on parasite burden.
Several epidemiological studies have consistently shownan inverse association between clinical asthma and Schisto-soma infections. M. C. F. Almeida et al. carried out an elegantintervention study using the appropriate method to assesswhether helminth infections are associated with asthmasymptoms. e method used was a prospective, double-blinded, placebo-controlled study evaluating the in�uence ofantihelminthic treatment on asthma severity, carried out inan endemic area for schistosomiasis. Findings on worseningof asthma severity aer repeated antihelminthic treatmentssupport the hypothesis on the protective effect of helminthinfections in in�ammatory diseases. Additional studies, suchas the one described by Almeida et al. which would includea larger number of participants and continue for a longerperiod of time, are necessary in order to elucidate furtherthe association between different helminth infections andin�ammatory diseases.
In the paper by L. S. Cardoso and colleagues, risk factorsfor asthma were investigated in an area of helminth transmis-sion in Bahia, Brazil, by the use of questionnaires. e effectof Schistosoma mansoni and also various gastrointestinalnematodes was investigated. Although the authors couldnot conclude that schistosomes offered a protective effect,the results indicated that Ascaris lumbricoides infection wasnegatively associated with asthma. is paper may thus beconsistent with the idea referred to earlier that parasitic wormspecies vary in their immunomodulatory effects, but it shouldalso be noted (as outlined above) that other studies showschistosome infection to be associatedwith protection againstallergy.
In conclusion, the editors hope to have stimulated, withthis special issue, the interest on the relationship betweenallergy andparasitic infections; envisaging new researchworkis needed not only to clarify many aspects which remainuncertain, but also to open the way to possible new strategiesto control allergic diseases.
Fabrizio BruschiMaria Ilma Araujo
William HarnettElena Pinelli

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2013, Article ID 961268, 13 pageshttp://dx.doi.org/10.1155/2013/961268
Research ArticleMast Cell Subsets and Their Functional Modulation by theAcanthocheilonema viteae Product ES-62
Dimity H. Ball,1 Hwee Kee Tay,1 Kara S. Bell,2 Michelle L. Coates,2 Lamyaa Al-Riyami,2
Justyna Rzepecka,2 William Harnett,2 and Margaret M. Harnett1
1 Centre for Immunobiology, Glasgow Biomedical Research Centre, Institute of Infection, Immunity and Inflammation,College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow G12 8TA, UK
2 Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow G4 0RE, UK
Correspondence should be addressed to Margaret M. Harnett; [email protected]
Received 3 September 2012; Accepted 16 October 2012
Academic Editor: Fabrizio Bruschi
Copyright © 2013 Dimity H. Ball et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ES-62, an immunomodulator secreted by filarial nematodes, exhibits therapeutic potential in mouse models of allergicinflammation, at least in part by inducing the desensitisation of Fc𝜀RI-mediated mast cell responses. However, in addition totheir pathogenic roles in allergic and autoimmune diseases, mast cells are important in fighting infection, wound healing, andresolving inflammation, reflecting that mast cells exhibit a phenotypic and functional plasticity. We have therefore characterisedthe differential functional responses to antigen (via Fc𝜀RI) and LPS and theirmodulation by ES-62 of themature peritoneal-derivedmast cells (PDMC; serosal) and those of the connective tissue-like mast cells (CTMC) and the mucosal-like mast cells derived frombone marrow progenitors (BMMC) as a first step to produce disease tissue-targeted therapeutics based on ES-62 action. All threemast cell populations were rendered hyporesponsive by ES-62 and whilst the mechanisms underlying such desensitisation have notbeen fully delineated, they reflect a downregulation of calcium and PKC𝛼 signalling. ES-62 also downregulated MyD88 and PKC𝛿in mucosal-type BMMC but not PDMC, the additional signals targeted in mucosal-type BMMC likely reflecting that these cellsrespond to antigen and LPS by degranulation and cytokine secretion whereas PDMC predominantly respond in a degranulation-based manner.
1. Introduction
Mast cells are increasingly recognised as playing an importantpathogenic role in a variety of allergic and autoimmunediseases [1–4]. However, there is also developing evidenceof their participation in tissue repair and resolution ofinflammation [5–7], as well as for their exhibiting pathogenicand protective roles in cancer [8, 9]. Such contradictoryevidence relating to mast cell function most likely reflectsthat mast cells, which are haematopoietic cells found inall vascularised organs [10–13], constitute a heterogeneouscell population [14] varying in morphology, function, andlocation with subpopulations being characterised by theirdifferential protease, eicosanoid, and proteoglycan content[10, 13–17]. Such heterogeneity arises because bone marrow-derived mast cell progenitors [18, 19] arrive in tissue beforethey are fully matured [20] allowing the different cytokines,
hormones, and reactive oxygen and/or nitrogen speciesproduced by various microenvironments to essentially create“custom-made” site-specific mast cells [12–14].
Moreover, the functional response of mast cells dependson the stimuli received [12]; for example, following classicalactivation via the IgE receptor, Fc𝜀R1, mast cells degranulaterapidly (within minutes) to exocytose prostaglandins andleukotrienes as well as preformed cytokines, tryptase, his-tamine, heparin, and platelet activating factor (PAF) whilstde novo synthesised cytokines exhibit a more delayed (hours)release [8, 21]. However, mast cells can also be activatedindependently of Fc𝜀RI and this can be initiated by cytokinesor other proinflammatory mediators [21] reflecting a directinteraction with triggering factors such as LPS, parasitemolecules, or allergic stimuli in the skin or the mucosa.Hence, mast cells are frequently the first cell type to respondduring inflammation [6], as evidenced by the important roles

2 Journal of Parasitology Research
played by mast cells in bacterial and parasitic infections[22–25]. However, mast cells are also able to influencedisease progress subsequently; both directly via the releaseof proinflammatorymediators, and indirectly via their effectson other immune cells, including dendritic cells (DC), T andB cells, and macrophages [6].
Isolation of in vivo differentiated mast cell subsets isdifficult due to their limited numbers in tissue [5, 26] andthis has led to the development of in vitro culture protocolsto generate human and mouse mast cells, as defined bytheir expression of CD117, Fc𝜀R1 and the IL-1 receptor familymember, ST2 (suppression of tumorigenicity 2), that can besubclassified as distinct phenotypes due to their differentialgranular phenotypic and functional responses [14]. Thus,although mast cells make up <5% of the peritoneal cellpopulation, they can be expanded by in vitro culture with SCFto create large numbers of homogenous peritoneal-derivedmast cells (PDMC) that are serosal-type mast cells andretainmost of themorphological, phenotypic, and functionalfeatures of mature mast cells [5, 14]. Such PDMC exhibitdifferential functional responses (generating less lipid medi-ators, chemokines, and cytokines but displaying strongerdegranulation responses) [5, 14] to bone marrow-derivedmast cells (BMMC), generated by culture in the presence ofIL-3 and SCF [27–29] and often used to represent mucosal-type mast cells (mucosal-type BMMC) [10, 14]. Phenotyp-ically, these BMMC, more closely resemble immature cellsand have no identifiable physiological equivalent in tissues[5, 12]. Nevertheless, such BMMC can repopulate both themucosal and serosalmast cell compartmentswhen adoptivelytransferred to mast cell-deficient mice, consistent with theproposal that these cells represent precursor cells that requireadditional site-specific signals to develop into mature tissuemast cells [12, 14]. By contrast, coculture of BMMC withfibroblasts [30, 31] generates connective tissue mast cells(CTMC) which have been used to represent serosal mastcells [10, 14]; more recently it has been shown that thesecan be differentiated from bone marrow precursors usingSCF and IL-4 [14, 32] and CTMC have been implicatedas being involved in both autoimmunity [33] and contacthypersensitivity [34].
The phosphorylcholine (PC)-containing excretory-secretory filarial nematode product, ES-62 exhibits broadanti-inflammatory properties including the desensitisation ofFc𝜀RI-mediated mast cell responses and displays therapeuticpotential in associated mucosal allergic inflammatorydisorders such as asthma [35, 36]. As ES-62 is also protectivein autoimmune and allergic connective tissue inflammatorypathologies such as arthritis and contact hypersensitivity,respectively [35, 36], we have therefore investigated its effectsonmature PDMC and also on both CTMC andmucosal-typeBMMC function in order to better understand mast cellbiology as a first step to producing disease tissue-targetedtherapeutics based on ES-62 action.
2. Materials and Methods
2.1. Mice and Reagents. BALB/c and C57BL/6mice were pur-chased from Harlan Olac and maintained at the Universities
of Glasgow and Strathclyde. All procedures were conductedin accordance with Home Office, U.K. animal guidelines andwith the approval of the local ethical committees. Unlessotherwise stated, all reagents were obtained from Sigma.
2.2. Peritoneal Derived Mast Cells (PDMC). PDMC wereexpanded as described previously [5]. Briefly, cells wereharvested following washing of the peritoneal cavity of 6–8 week-old mice with 5mL sterile, cold RPMI 1640 by cen-trifugation at 400 g for 5min and then resuspended in freshcomplete RPMI (RPMI with 10% FBS, 4mM L-glutamine,100U/mL penicillin, 100𝜇g/mL streptomycin, 1mM sodiumpyruvate, 100 𝜇M nonessential amino acids, and 50𝜇M 𝛽-mercaptoethanol; Invitrogen Life Technologies) before beingincubated at 5 × 106 cell/mL for 2 h at 37∘C in tissue culture-treated petri dishes (Corning) to remove adherent cells.The suspension cells were cultured at 0.3 × 106/mL incomplete RPMI supplemented with 10 ng/mL recombinantSCF (Pepro Tech) or 4% conditioned medium from the SCF-secreting cell line KLS-C. KLS-C is a CHO (Chinese HamsterOvary) cell line that produces SCF and was a kind giftfrom Dr Xiaoping Zhong, Duke University Medical Center.KLS-C cells were cultured at 37∘C in Minimum EssentialMedium alpha (MEM𝛼) without nucleosides (InvitrogenLife Technologies) and with 10% FBS, 100U/mL penicillin,100 𝜇g/mL streptomycin and 2.5𝜇M methotrexate. SCF-enriched supernatant was filtered to remove cell debris andthe concentration determined by ELISA and then adjustedwith PBS to 550 ng/mL to be used at a final concentration of22 ng/mL for PDMC.
2.3. Bone Marrow-Derived Mast Cells. Intact femurs andtibias were dissected from BALB/c or C57BL/6 mice and sin-gle cell suspensions were obtained by passing bone marrowcells through a 100𝜇M nylon monofilament gauze (CadischPrecision Meshes) and lysis of red blood cells for 1min at22∘C, followed by washing in PBS at 400 g.
Mucosal-type BMMC were derived by culture of bonemarrow progenitors [27–29] at 0.5 × 106/mL in RPMI with10% FBS, 2mML-glutamine, 100U/mL penicillin, 100 𝜇g/mLstreptomycin, 1mM sodium pyruvate, 10mM HEPES, and50𝜇M 𝛽-mercaptoethanol supplemented with conditionedmedium from KLS-C (1%; SCF) and TOP3 (3%; IL-3) celllines. TOP3 is a cell line that produces IL-3 and was a kindgift fromDrMassimoGadina, NIH. TOP3 cells were culturedat 37∘C in RPMI with 5% FBS, 2mM L-glutamine, 100U/mLpenicillin, 100 𝜇g/mL streptomycin, 1mM sodium pyruvate,and 50 𝜇M 𝛽-mercaptoethanol and 0.4mg/mL G418. IL-3-enriched supernatant was filtered to remove cell debrisand the concentration determined by ELISA, with the stockconcentration adjustedwith PBS to 1300 ng/mL to be used at afinal concentration of 39 ng/mL. Alternatively, mucosal-typeBMMC were derived using 10 ng/mL recombinant SCF and10 ng/mL recombinant IL-3 (Pepro Tech).
CTMC were derived by culture of bone marrow progen-itors [14, 32] at 0.8 × 106/mL in RPMI with 10% FBS, 4mML-glutamine, 100U/mL penicillin, 100𝜇g/mL streptomycin,1mM sodium pyruvate, 100 𝜇M nonessential amino acids

Journal of Parasitology Research 3
and 50 𝜇M 𝛽-mercaptoethanol supplemented with 1% KLS-C conditioned medium (or 10 ng/mL recombinant SCF) and1 ng/mL recombinant murine IL-4 (Pepro Tech).
PDMC, mucosal-type BMMC, and CTMC were culturedat 37∘C/5% CO
2in tissue culture-treated flasks (Greiner Bio-
one) for at least 28 days, with adherent cells being discarded.A purity of >95% mast cells was routinely obtained asevidenced by the surface expression of CD117, Fc𝜀R1 and ST2and viability was determined by Trypan Blue staining.
2.4. Mast Cell Stimulation. Unless otherwise stated, mastcells were sensitised with 0.5𝜇g/mL murine anti-DNP IgEfor 18 h prior to stimulation. In experiments investigat-ing immunomodulation by ES-62, mast cells were incu-bated with ES-62 (2𝜇g/mL) simultaneously with IgE duringthe sensitisation period. Cells were then stimulated (1 ×106 cells/mL except where indicated) by addition of medium,0.5 𝜇g/mL DNP-HSA to cross-link Fc𝜀R1, 0.5 𝜇g/mL LPS(Salmonella minnesota) or PMA (phorbol myristate acetate;1 𝜇M) plus ionomycin (1 𝜇M). Reactions were terminatedafter the desired culture period by centrifugation at 400 g andsupernatants aspirated for determination of mediator releasewhilst the cell pellets were stored at −20∘C until subjected toWestern Blot analysis.
2.5. Preparation of Endotoxin-Free ES-62. ES-62 was puri-fied to homogeneity from spent culture medium of adultAcanthocheilonema viteae using endotoxin-free reagents asdescribed previously [37]. The purity and identity of eachbatch were confirmed by SDS-PAGE and the level of endo-toxin in the ES-62 sample was determined using a LimulusAmebocyte Lysate (LAL) QCL-1000 kit (Lonza Biologics).ES-62 is used at a working concentration that has an endo-toxin reading of <0.003 endotoxin units/mL [37].
2.6. Mast Cell Phenotyping. To identify mast cells by positivestaining of heparin with Toluidine Blue, cells (0.01 × 106) werecytofuged using a Shandon Cytospin3 (Thermo Shandon) at500 rpm for 5min. Slides were air dried before staining with0.5% Toluidine Blue in 0.5MHCl for 10–15min. Images wereobtained using an Olympus BX41TF microscope.
Mast cells were also phenotyped by flow cytomet-ric analysis of lineage markers. Briefly, cells were pre-incubated with 50𝜇L Fc receptor (FcR) blocking buffer(anti-CD16/32, clone 2.4G2, hybridoma supernatant, 10%mouse serum, and 0.1% sodium azide) for 20min at 4∘Cprior to incubation with the appropriate flurochrome-conjugated or biotinylated antibodies (2 𝜇g/mL; suspendedin 50𝜇L Fc Block; CD117, eBioscience; Fc𝜀RI, eBioscience;ST2, MD Bioproducts; and TLR4/MD2, eBioscience) for30min, 4∘C. Following washing, for biotinylated primaryantibodies, flurochrome-conjugated streptavidin was addedfor a further 30min at 4∘C. After labelling, cells werewashed twice with 3mL FACS buffer (PBS containing 2%FBS and 2mM EDTA) at 1500 rpm for 6min, 4∘C andthen resuspended in FACS buffer. To enable exclusion ofdead cells from the analyses, cells were either stainedwith Live/Dead Viability/Cytotoxicity Kit (Invitrogen) before
commencement of staining or by the addition of 1 𝜇L 7-AAD (7-Amino Actinomycin D; eBioscience) immediatelyprior to data acquisition. Cellular fluorescence data wereacquired using a Becton Dickinson LSR II or FACSCaliburflow cytometer and analysed using FlowJo software (TreeStar Inc). Analysis was performed on a minimum of 10,000events.
2.7. Calcium Mobilisation. Cells were loaded with the fluo-rescent calcium-sensing dye Fura-2/AM (5 𝜇M; Invitrogen)in HBSS (145mM NaCl, 5mM KCl, 1mM MgSO
4, 1 mM
CaCl2, and 10mM HEPES) supplemented with 0.18% (w/v)
D-glucose and 0.2% (w/v) BSA for 30min at 37∘C in thedark. For measurement of intracellular calcium mobilisationin the absence of extracellular calcium, calcium-free HBSSsupplemented with 100𝜇MEGTA (ethylene glycol tetraaceticacid) to chelate any remaining free calcium, was used. Cells(106) were added to a stirred glass cuvette in a Hitachi F-700 fluorescence spectrophotometer at 37∘C and stimulatedas indicated at 𝑡 = 50 s and measurements acquired fora total of 180 s. Calcium levels were detected every 500msusing excitation-emission ratios of 340/380 nm. Followingeach experiment 𝑅max and 𝑅min values were determined bythe addition of 1% Triton-X100 and subsequent addition of20mM EGTA pH 7.4, respectively.
2.8. Cytokine and Prostaglandin D2(PGD2) Release. ELISAs
for IL-6, IL-13, MCP-1, and TNF𝛼 (limits of detection4 pg/mL, 4 pg/mL, 15 pg/mL, and 8 pg/mL resp.; eBioscience)and PGD2 (Cayman Chemicals) were performed on tripli-cate samples according to the suppliers’ recommendationsand developed using TMB substrate and absorbances weredetermined using a TECAN Sunrise Microplate Reader.
2.9. Mast Cell Degranulation. The level of degranulation wasdetermined using a modified colorimetric assay to assessthe release of 𝛽-hexosaminidase. Mast cells (0.2 × 106) weresuspended in 200𝜇L Tyrode’s buffer supplemented with 1%FCS and stimuli were added for 30min at 37∘C. Reactionswere terminated by centrifugation (400 g) and 50𝜇L aliquotsof supernatants assayed for release of 𝛽-hexosaminidase andnormalised to total cellular 𝛽-hexosaminidase following celllysis by the addition of 1% Triton-X 100 and by incubationwith 1mM p-nitrophenyl-N-acetyl-𝛽-d-glucosamine (NAG)in 200𝜇L 0.05Mcitrate buffer, pH4.5. After incubation in thedark at 37∘C for 1 h the reaction was quenched by the removalof 62.5 𝜇L of the reaction mix into a clean well and theaddition of 125𝜇L/well 0.1M sodium bicarbonate buffer andoptical density determined by a TECAN Sunrise MicroplateReader at 405 nm.
2.10. Western Blotting. Mast cells (2 × 106/mL) were stimu-lated as indicated and reactions terminated by the additionof ice-cold PBS and centrifugation at 400 g at 4∘C for5min. Lysis was performed by the addition of 50 𝜇L ice-cold, modified RIPA lysis buffer (50mM Tris buffer, pH7.4 containing 150mM sodium chloride, 2% (v/v) NP40,0.25% (w/v) sodium deoxycholate, 1mM EGTA, 10mM

4 Journal of Parasitology Research
sodium orthovanadate, 0.5mM phenylmethylsulfonylfluo-ride, chymostatin (10𝜇g/mL), leupeptin (10 𝜇g/mL), antipain(10 𝜇g/mL), and pepstatin A (10 𝜇g/mL)). After vortexing,the cells were incubated on ice for 30min before microcen-trifugation of lysates at 12000 rpm for 15min. The resultingsupernatants (cell lysates) were stored at −20∘C.
Equal protein loadings of cell lysates (30–40𝜇g pro-tein perlane), determined by BCA protein assay (bicin-choninic acid assay; Thermo Pierce), were resolved usingthe XCell SureLock Mini-Cell kit with NuPAGE Novexhigh-performance precast Bis-Tris gels and NuPAGE buffersand reagents (Invitrogen). Proteins were then transferred tonitrocellulose (Amersham) or PVDFmembranes and proteinloading was validated by Ponceau Red staining. Membraneswere washed in Tris-buffered saline (TBS) (0.5M NaCl and20mM Tris pH 7.5) with 0.1% (v/v) Tween-20 (TBS/Tween)and blocked for 1 h in TBS/Tween with 5% nonfat milk(Marvel). Membranes were then incubated overnight at4∘C with the appropriate primary detection antibody. Allantibodies were diluted in TBS/Tween with either 5% nonfatmilk or 5%BSA. Following incubationwith primary antibodythe membranes were washed with TBS/Tween and incubatedin the appropriate horseradish peroxidase (HRP)-conjugatedsecondary antibody for 2 h at room temperature beforevisualisation using the ECL detection system and KodakX-Ray film. Densitometry was performed using Image Jsoftware.
2.11. Statistical Analysis. All statistical analysis was per-formed using GraphPad Prism 5.0 (GraphPad Software Inc).Statistical analysis was by unpaired 𝑡-test or one-wayANOVAwith Tukey’s post-test and 𝑃 is significant at ∗𝑃 < 0.05,∗∗𝑃 < 0.01, ∗∗∗𝑃 < 0.001, and ∗∗∗∗𝑃 < 0.0001.
3. Results and Discussion
3.1. Phenotyping of PDMC, Mucosal-Type BMMC, and CTMCMast Cell Subsets. Following expansion of PDMC andderivation ofmucosal-type BMMCandCTMC for 4–6weeksin vitro, these mast cell populations were phenotyped formast cell lineage markers (CD117, Fc𝜀RI, and ST2) and alsofor TLR4 (toll-like receptor-4) and proteoglycan (heparin)expression (Figure 1). This analysis revealed all three mousesubsets to be of similar size, although the CTMC appearedrather less granular (Figure 1(a)), with each subset com-prising a homogeneous population of CD117+Fc𝜀RI+ mastcells (Figure 1(b)). Moreover, all 3 populations expressedTLR4 (Figure 1(c)) and ST2 (Figure 1(d)), with BMMC typ-ically expressing the highest levels of TLR4 and CTMCshowing most ST2 expression. Similarly, PDMC, mucosal-type BMMC, and CTMC all contained heparin-containinggranules as indicated by toluidine blue staining (Figure 1(e)),although there was some heterogeneity in the CTMC, and toa lesser extent, the mucosal-type BMMC populations, per-haps reflecting their differences in granularity (Figure 1(a)).Mucosal-type mast cells from mice have generally beenconsidered to express little or no heparin, but in agreementwith our results, it has been reported that heparin expression
can be upregulated in response to SCF in these cells [14]:this functional plasticity is consistent with the ability ofmouse BMMC to repopulate both serosal and mucosalcompartments of mast cells in vivo [14].
3.2. Differential Functional Responses of Mast Cell Subsets.It has previously been reported that serosal- and mucosal-type mast cells exhibit differential functional responses withPDMC displaying strong degranulation responses whilstBMMC preferentially produce chemokines and cytokines,and that these responses can be further “fine-tuned” selec-tively in response to inflammatory stimuli and microen-vironment [14]. We therefore characterised the differ-ential responses of PDMC, mucosal-type BMMC, andCTMC in response to Ag-mediated crosslinking of Fc𝜀RI,LPS/TLR4 signalling and also the pharmacological stimulusPMA plus ionomycin (P/I) in terms of degranulation (𝛽-hexosaminidase), eicosanoid (PGD2), chemokine (MCP-1), and cytokine (IL-6, IL-13 and TNF𝛼) release (Table 1).These data confirmed that PDMC were the subtype thatdegranulated most strongly in response to Fc𝜀RI and PMAplus ionomycin and demonstrated that all of these subtypesgenerated in vitro exhibited little or no degranulation inresponse to LPS. All of the mast cell populations consti-tutively secreted high levels of PGD2 (lowest in PDMC);however, whilst PDMC did not produce any more PGD2 inresponse to Fc𝜀RI crosslinking, both mucosal-type BMMCand CTMC responded further to this stimulus and also toLPS. Further differential responses were observed in termsof chemokine release as whilst LPS stimulated release ofMCP-1 in all subtypes, Fc𝜀RI crosslinking induced little orno release of MCP-1 over the basal levels in PDMC, yetstrongly stimulated release of this chemokine from mucosal-type BMMC and CTMC. Only PMA plus ionomycin wereable to induce substantial secretion of IL-6 and IL-13 byPDMC, and none of the stimuli were routinely able to triggerTNF𝛼 release by these cells. Similarly, whilst Fc𝜀RI- andLPS/TLR4-signalling induced little or no IL-13 or TNF𝛼production by CTMC, LPS, but not Fc𝜀RI crosslinking,triggered strong secretion of IL-6. By contrast, Fc𝜀RI andLPS/TLR4 signalling both induced the production of allthree cytokines (IL-6, IL-13 and TNF𝛼) by mucosal-typeBMMC. It has been reported that BMMC and freshly isolatedPDMC derived from C57BL/6 mice exhibited higher levelsof degranulation (𝛽-hexosaminidase) and generated lowerlevels of cytokine and prostaglandin production than thosederived from BALB/c mice [38] but we did not find this to bea significantly reproducible trend in this study (data are notshown).
3.3. ES-62 Inhibits Functional Responses in Both Serosal andMucosalMast Cell Subtypes. Given the differential functionalresponses of the mast cell subtypes, we next investigatedwhether the filarial nematode product showed selectivity inits desensitisation of mast cell responses, both in terms of themast cell subtype targeted and alsowith respect to their differ-ential responses to the individual proinflammatory stimuli.These studies showed that exposure to ES-62 significantly

Journal of Parasitology Research 5
0 200 400 600 800 10000
200
400
600
800
1000
FSC-H: FSC-height
SSC-
H: S
SC-h
eigh
t
0 200 400 600 800 10000
200
400
600
800
1000
FSC-H: FSC-height
SSC-
H: S
SC-h
eigh
t
CTMC
0 200 400 600 800 10000
200
400
600
800
1000PDMC Mucosal-type BMMC
FSC-H: FSC-height
SSC-
H: S
SC-h
eigh
t
(a)
100 101 102 103 104100
101
102
103
1040.26 0.25 0.43 98.9
0.190.47
99.3
0.20.210.67 0.99
98.1
FL4-
H: c
-Kit
APC
CD11
7
100 101 102 103 104100
101
102
103
104
FL4-
H: c
-Kit
APC
CD11
7
100 101 102 103 104100
101
102
103
104
FL4-
H: c
-Kit
APC
CD11
7
CTMCPDMC Mucosal-type BMMC
Fc𝜀RI Fc𝜀RI Fc𝜀RIFL1-H: Fc𝜀RI Fitc FL1-H: Fc𝜀RI Fitc FL1-H: Fc𝜀RI Fitc
(b)
0
20
40
60
80
100
100 101 102 103 104
TLR4-MD2
Max
(%)
0
20
40
60
80
100
100 101 102 103 104
TLR4-MD2
Max
(%)
CTMCPDMC
102 103 104 1050
0
20
40
60
80
100
Max
(%)
TLR4-MD2
Mucosal-type BMMC
(c)
0
20
40
60
80
100
100 101 102 103 104
ST2
Max
(%)
0
20
40
60
80
100
100 101 102 103 104
ST2
Max
(%)
0
20
40
60
80
100
100 101 102 103 104
ST2
Max
(%)
CTMCPDMC Mucosal-type BMMC
(d)CTMCPDMC Mucosal-type BMMC
(e)
Figure 1: Phenotyping of mast cell subsets. Exemplar plots of mast cell phenotyping by flow cytometric analysis are shown in (a)–(d). FSCand SSC parameters of PDMC, mucosal-type BMMC, and CTMC cultured in vitro for 28 days (a) and gating (relative to isotype controls;not shown) of the consequent CD117+Fc𝜀R1+cell population (>98%; (b)) prior to the analysis of their TLR4+expression (c) are shown. Inparallel experiments, ST2 expression of CD117+Fc𝜀R1+cells in the various populations was determined (d). Gray shaded plots (c-d) are isotypecontrols. In (e), exemplar images of toluidine blue staining of the mast cell populations (x10) are shown.The data are representative of at least2 independent experiments.

6 Journal of Parasitology Research
Table1:Differentia
lfun
ctionalrespo
nses
ofmastcellsub
sets.
PDMC
Mucosal-ty
peBM
MC
CTMC
Basal
Fc𝜀RI
LPS
P/I
Basal
Fc𝜀RI
LPS
P/I
Basal
Fc𝜀RI
LPS
P/I
Degranu
latio
n(%
)4.48±0.56
33.24±4.07
2.87±1.4
755.34±4.24
7.46±1.10
17.34±2.19
2.87±1.7
831.97±3.78
3.95±1.0
217.3±2.90
2.173±0.48
25.29±4.62
𝑛=7
𝑛=2
𝑛=4
𝑛=5
𝑛=3
𝑛=5
𝑛=2
𝑛=2
𝑛=2
PGD2(pg/mL)
1804±44
1907±55
3257±338
4711±264
4509±156
2888±370
3229±333
4764±153
𝑛=3
𝑛=5
𝑛=5
𝑛=5
𝑛=2
IL-6
(pg/mL)
70±27
67±32
81.33±7
408±61
37.4±14.7
560±96
2557±696
21976±6589
87±23
114±19
812±217
𝑛=6
𝑛=4
𝑛=3
𝑛=18
𝑛=18
𝑛=4
𝑛=3
𝑛=4
IL-13(pg/mL)
7.81±
1.52
17.91±2.84
25.91±
4.43
248±20
5.88±0.86
366±88
338±116
1578±111
3.94±2.94
18.5±0.45
44.7±1.1
𝑛=6
𝑛=7
𝑛=3
𝑛=6
𝑛=5
𝑛=3
𝑛=1
𝑛=1
MCP
-1(pg/mL)
457±73
387±84
616±109
102±19
504±212
1703±393
862±296
396±58
1410±226
511±
76𝑛=2
𝑛=2
𝑛=3
𝑛=2
𝑛=2
TNF𝛼
15.25±2.48
15.57±2.91
19.62±3.38
32.33±2.94
5.02±2.12
506±159
150±38
3199±916
1.42±0.19
1.41±
0.34
15.62±1.6
1𝑛=1
𝑛=1
𝑛=12
𝑛=9
𝑛=4
𝑛=1
𝑛=2
Dataa
representedas
them
eanvalues±SE
Mwhere
n=nu
mbero
find
ependent
experim
entsor
meanvalues±SD
oftriplicates
amples
inthec
asew
here
datafro
mas
inglee
xperim
entare
presented.

Journal of Parasitology Research 7
Basa
l
XL
ES-6
2
Basa
l
XL
ES-6
2
Basa
l
XL
ES-6
2
CTMC
0
2
4
6
∗∗∗∗
PDMC Mucosal-type BMMC
0
5
10
15
0
5
10
1520
𝛽-h
exam
inid
aser
elea
sed
(%)
𝛽-h
exam
inid
aser
elea
sed
(%)
𝛽-h
exam
inid
aser
elea
sed
(%)
XL+
ES-6
2
XL+
ES-6
2
XL+
ES-6
2
(a)
ES-6
2
0
5
10
15
20
25
0
10
20
30
40
∗∗∗
Basa
l
P/I
ES-6
2
Basa
l
P/I
ES-6
2
Basa
l
P/I
0
20
40
60
𝛽-h
exam
inid
aser
elea
sed
(%)
𝛽-h
exam
inid
aser
elea
sed
(%)
𝛽-h
exam
inid
aser
elea
sed
(%)
P/I+
ES-6
2
P/I+
ES-6
2
P/I+
ES-6
2
(b)
FcεRI
Max
(%)
0
20
40
60
80
100
100 101 102 103 104
FL2-H: Fc𝜀RI(c)
CD117
Max
(%)
0
20
40
60
80
100
100 101 102 103 104
FL4-H: CD117
(d)
ST2M
ax (%
)
0
20
40
60
80
100
100 101 102 103 104
FL1-H: ST2
(e)
Figure 2: Degranulation by mast cell subsets. Mucosal-type BMMC, CTMC and PDMC were sensitised with murine anti-DNP IgE(0.5 𝜇g/mL) in the presence and absence of ES-62 (2𝜇g/mL) overnight. Cells were then stimulated with DNP (0.5 𝜇g/mL) to induce Fc𝜀RIcross-linking (XL; (a)) or PMAplus ionomycin (both 1 𝜇M; (b)) for 30min at 37∘C.Degranulationwas determined as the% 𝛽-hexosaminidaserelease relative to the total enzyme activity of the cells and the data presented are from single experiments representative of at least 2independent experiments. PDMC were sensitised with murine anti-DNP IgE (0.5𝜇g/mL) in the presence and absence of ES-62 (2𝜇g/mL)overnight and analysed for expression of Fc𝜀RI (c), CD117 (d), and ST2 (e). Grey shaded plots (c–e) are relevant isotype controls.
inhibited the degranulation of PDMC and the mucosal-typeBMMC, but not CTMC, in response to Fc𝜀RI signalling(Figure 2(a)). Whilst the responses to LPS were typicallytoo low (Table 1) to show significant effects of ES-62 (datanot shown), degranulation in response to PMA plus iono-mycin was also significantly inhibited in PDMC (Figure 2(b))and likewise observed in CTMC (2/2 experiments) and themucosal-type BMMC (3/5 experiments).
Although PDMC produced little or no chemokines/cytokines in response to either Fc𝜀RI crosslinking or LPS-stimulation (Table 1), generally, the very low levels of MCP-1,IL-6, and IL-13 observed were inhibited by ES-62 (data notshown). With respect to mucosal-type BMMC and CTMC,whilst ES-62 was only able to significantly inhibitMCP-1 pro-duction by Fc𝜀RI-stimulated mucosal-type BMMC (Figures3(a) and 3(b)), it inhibited LPS-stimulated IL-6 production

8 Journal of Parasitology Research
0
200
400
600
800
MCP
-1 (p
g/m
L)
MCP
-1 (p
g/m
L)∗∗∗
Basa
l
XL
ES-6
2
Basa
l
LPS
ES-6
2
Mucosal-type BMMC
0
100
200
300
400
XL+
ES-6
2
LPS+
ES-6
2
(a)
CTMC
0
200
400
600
800
MCP
-1 (p
g/m
L)
Basa
l
LPS
ES-6
2
MCP
-1 (p
g/m
L)
Basa
l
XL
ES-6
2
0100200300
500400
XL+
ES-6
2
LPS+
ES-6
2
(b)
∗∗∗∗∗∗
IL-6
(pg/
mL)
IL-6
(pg/
mL)
Basa
l
XL
ES-6
2
Basa
l
LPS
ES-6
2
0
100
200
300
400
0
200
400
600
XL+
ES-6
2
LPS+
ES-6
2
(c)
0
10
20
30
∗∗∗
IL-6
(pg/
mL)
IL-6
(pg/
mL)
Basa
l
LPS
ES-6
2
Basa
l
XL
ES-6
2
0
100
200
300
XL+
ES-6
2
LPS+
ES-6
2
(d)
0
10
20
30
40
0
5
10
15
∗∗
IL-1
3 (p
g/m
L)
IL-1
3 (p
g/m
L)
Basa
l
XL
ES-6
2
Basa
l
LPS
ES-6
2
XL+
ES-6
2
LPS+
ES-6
2
(e)
0
5
10
20
15
0
20
40
60
∗∗
IL-1
3 (p
g/m
L)
IL-1
3 (p
g/m
L)
Basa
l
XL
ES-6
2
Basa
l
LPS
ES-6
2
XL+
ES-6
2
LPS+
ES-6
2
(f)
Figure 3: Chemokine and cytokine release by mast cell subsets. Mucosal-type BMMC (a), (c) & (e) and CTMC (b), (d) & (f) were sensitisedwith murine anti-DNP IgE (0.5 𝜇g/mL) in the presence and absence of ES-62 (2𝜇g/mL) overnight. Cells were then stimulated with DNP(0.5 𝜇g/mL) to induce Fc𝜀RI cross-linking (XL) or LPS (0.5𝜇g/mL) for 24 h at 37∘C and MCP-1 (a) & (b), IL-6 (c) & (d), and IL-13 (e) & (f)release measured by ELISA. The data presented are single experiments representative of at least 2 independent experiments apart from theIL-13 release from CTMC, which could only be detected in a single experiment.
by both subtypes as well as that seen in mucosal-type BMMCin response to crosslinking of Fc𝜀RI (Figures 3(c) and 3(d)).By contrast, the IL-13 response to Fc𝜀RI crosslinking wassuppressed by ES-62 in both subtypes (Figures 3(e) and3(f)) whilst the Fc𝜀RI-mediated TNF𝛼 response only seen inmucosal-type BMMC was also inhibited by ES-62 (data notshown).
Collectively, therefore, we have shown that ES-62 can tar-get both serosal- and connective-tissue phenotypes to renderthese cells hyporesponsive to proinflammatory stimuli. ThatES-62 canmodulate the responses of bothmature and imma-ture cells is consistent with our previous studies showingthat the parasite product can target immature bone marrowprogenitors of macrophages and dendritic cells to generate
a more anti-inflammatory environment in vivo [37, 39]. Thefinding that ES-62 did not modulate expression of Fc𝜀RI,CD117, or ST2 on resting or sensitized mast cells (Figures2(c)–2(e) and data not shown), however, suggested that itwas not affecting their phenotypic status but rather targetingtheir functional plasticity. The observed differential targetingof particular responses may indicate selective actions in par-ticular microenvironments and consequently, recruitment ofother innate cells such as neutrophils to the site of inflam-mation as well as mast cell promotion of the polarisationof particular immune responses [4, 14], dependent on thesite and type of inflammation (e.g., protective inflammationto fight infection versus aberrant autoimmune or allergichyperinflammation).

Journal of Parasitology Research 9
0 34 68 102 136 170Time (s)
0100200300400500
∗∗∗∗
SensitizedNonsensitized
Intr
acel
lula
rCa2+
(𝜇M
)
(a)
0 34 68 102 136 170Time (s)
∗∗∗∗
SensitizedNonsensitized
0
50
100
Intr
acel
lula
rCa2+
(𝜇M
)
(b)
0
200
400
600
0 34 68 102 136 170Time (s)
ControlEGTA
Intr
acel
lula
rCa2+
(𝜇M
)
(c)
050
100150200250
ControlEGTA
0 34 68 102 136 170Time (s)
Intr
acel
lula
rCa2+
(𝜇M
)
(d)
0 34 68 102 136 170Time (s)
0100200300400500
ControlEGTA
Intr
acel
lula
rCa2+
(𝜇M
)
(e)
0 34 68 102 136 170Time (s)
050
100150200250
ControlEGTA
Intr
acel
lula
rCa2+
(𝜇M
)
(f)
0 34 68 102 136 170Time (s)
050
100150200250
ControlEGTA
Intr
acel
lula
rCa2+
(𝜇M
)
(g)
0 34 68 102 136 170Time (s)
050
100150200250
ControlEGTA
Intr
acel
lula
rCa2+
(𝜇M
)
(h)
Figure 4: Calcium mobilisation in mast cell subsets. Fura-2/AM-loaded resting, nonsensitised (a) & (b) or anti-DNP IgE (0.5 𝜇g/mL)-sensitised (a)–(h) mucosal-type BMMC (e) & (f), CTMC (g) & (h) and PDMC (a)–(d) were stimulated at 50 s with DNP (0.5 𝜇g/mL) toinduce cross-linking (XL) of Fc𝜀R1 (a), (c), (e) & (g) or 0.5𝜇g/mL LPS (b), (d), (f) & (h), and intracellular calcium mobilisation and influxrecorded in real time using excitation-emission ratios of 340/380 nm (a)–(h). For analysis of intracellular mobilisation alone, the cells werestimulated in calcium freeHBSS supplementedwith 100 𝜇MEGTA to remove all extracellular calcium (EGTA). Calcium levels were calculatedfrom 𝑅max and 𝑅min values and the data are presented as the mean calcium values of triplicate samples (base line calcium values subtracted)from a single experiment representative of at least 3 independent experiments.
3.4. ES-62 Targets Calcium and PKC Signalling in Mast Cells.To address how ES-62 may be differentially targeting thefunctional responses of PDMC, the mucosal-type BMMC,and CTMC, we investigated the effects of the parasiteproduct on calcium mobilisation and expression of PKC𝛼,as we had previously shown modulation of these two keysignals in degranulation and cytokine signalling [40–42] tobe crucial to the desensitisation of Fc𝜀RI-mediated humanmast cell responses [35, 36]. Moreover, ES-62 exerts itseffects via subversion of TLR4 signalling whilst the canonicalTLR4 ligand LPS typically acts to enhance Fc𝜀RI functionalresponses [43, 44], the latter accounting at least in part forthe widely established finding that LPS exacerbates airwayhyperresponsiveness [43]. LPS has been reported to do thisby increasing Fc𝜀RI-driven calcium mobilisation by upreg-ulating the Orai1 and Stim1 subunits of the store-operatedcalcium (SOC) channel and hence stimulating calcium influx[43]. In addition, PKC signalling, including that of PKC𝛼,has been shown to be important to LPS/TLR4 responses ina variety of innate cells [45].
As a first step, we investigated whether Fc𝜀RI- andLPS/TLR-signalling induced calcium mobilisation in each ofPDMC, mucosal-type BMMC and CTMC (Figure 4). Inter-estingly we found that not only as expected, IgE-sensitisationof mast cells was essential for Fc𝜀RI-mediated calcium
mobilisation, but also that it enhanced that seen in responseto LPS (PDMC; Figures 4(a) and 4(b)). Moreover, it was clearthat whilst the Fc𝜀RI signal reflected a mix of mobilisationof intracellular calcium and calcium influx, as indicated bythe observed transient spike in the absence of extracellularcalcium (EGTA), the calcium response to LPS in all mastcell subtypes predominantly reflected calcium influx (Figures4(c)–4(h)). Consistent with LPS inducing calcium influx, wealso found as reported previously [43] that LPS enhancedFc𝜀RI-mediated calcium mobilisation (data not shown). Bycontrast, although preexposure to ES-62 did notmodulate thebaseline calcium levels, the parasite product suppressed thesubsequent calcium mobilisation in response to both Fc𝜀RI-crosslinking and LPS/TLR4 signalling in PDMC (Figures 5(a)and 5(b)).
In addition, ES-62 was found to downregulate PKC𝛼expression in PDMC, mucosal-type BMMC and CTMC(Figures 5(c) and 5(d)), suggesting, that as with human mastcells [35], ES-62 was targeting this signal in PDMC, mucosal-type BMMC and CTMC to suppress degranulation andcytokine responses. PKC𝛼 has been shown to be degraded viaboth proteosomal and caveolae/lipid raft, lysosomal routes[46, 47] and our preliminary studies in human mast cellsshowed that the inhibitor of caveolae/lipid raft trafficking,nystatin could protect against such downregulation following

10 Journal of Parasitology Research
0 34 68 102 136 170Time (s)
0
200
400
600
800
∗∗∗∗
XLXL + ES-62
Intr
acel
lula
rCa2+
(𝜇M
)
(a)
0 34 68 102 136 170Time (s)
0
200
100
300
400
500
600
∗∗∗∗
LPSLPS + ES-62
Intr
acel
lula
rCa2+
(𝜇M
)(b)
PDMC
0 2 6 24 ES-62 (h)
Actin
Actin
PKC𝛼
PKC𝛼Mucosal-type
BMMC
(c)
0 2 6 18 ES-62 (h)
ES-62 + NYS
ES-62 + E64d + pepstatin A
ES-62 + LAC
CTMC
𝛽-actin
𝛽-actin
𝛽-actin
PKC𝛼
PKC𝛼
PKC𝛼
(d)
MyD88
MyD88
Actin
Actin
0 2 6 24 ES-62 (h)
PDMC
PKC𝛿
Mucosal-type
BMMC
(e)
Figure 5: ES-62 modulates signalling in mast cell subsets. PDMC were sensitised with murine anti-DNP IgE (0.5𝜇g/mL) in the presenceor absence of ES-62 (2𝜇g/mL) overnight. Following loading with Fura-2/AM such PDMC were stimulated at 50 s with DNP (0.5 𝜇g/mL) toinduce cross-linking (XL) of Fc𝜀R1 (a) or 0.5𝜇g/mL LPS (b) and intracellular calcium mobilisation and influx recorded in real time usingexcitation-emission ratios of 340/380 nm (a) & (b). Calcium levels were calculated from 𝑅max and 𝑅min values and data are presented asthe mean calcium values of triplicate samples from a single experiment representative of at least 3 independent experiments. PDMC andmucosal-type BMMC (c) & (e) were cultured with ES-62 (2𝜇g/mL) for the indicated times and expression of PKC𝛼 ((c), Cell SignallingTechnology), MyD88 ((e), Abcam) and PKC𝛿 ((e), Cell Signalling Technology) analysed byWestern Blotting. In (d), following preincubationfor 1 h with inhibitors of proteosomal degradation (10𝜇M Lactacystin, ENZO Life Sciences; LAC), caveolae/lipid raft trafficking (50𝜇g/mLNystatin; NYS) and lysosomal degradation (E64d + pepstatin A both 10 𝜇g/mL, ENZO Life Sciences), sensitised CTMC were cultured withES-62 (2𝜇g/mL) for the indicated times and expression of PKC𝛼 analysed by Western Blotting. Actin was used as a loading control andES-62-mediated downregulation of PKC𝛼 expression was observed in PDMC, Mucosal-type BMMC, and CTMC in at least 2 independentexperiments.
exposure to ES-62 for 24 h [35]. Furthermore, our earlierstudies [48] had shown that ES-62-mediated downregulationof PKC𝛼 expression inB cells could be prevented by treatmentwith the cysteine protease inhibitor leupeptin; findings alsoconsistent with a lysosomal mechanism [49, 50] of degrada-tion of this key signalling element. We have therefore furtherinvestigated the (differential) mechanisms involved in ES-62-driven degradation of PKC𝛼 in mast cell subtypes. Ourdata in CTMC are consistent with that of our previous studyon human mast cells [35] as they showed that nystatin butnot lactacystin protected against PKC𝛼 degradation and wehave further confirmed the role of an endosomal route byshowing that protection is also afforded by the combination ofthe lysosomal inhibitors, E64d plus pepstatin A (Figure 5(d)).However, our comprehensive analysis of mechanism inPDMC and the mucosal-type BMMC has revealed a morecomplicated scenario in which both nystatin and lactacystin
can offer some protection at differential time points (datanot shown). Interestingly, these findings are consistent withreports that both mechanisms can coexist in cells not onlyin a temporal and spatially distinct manner but can also betriggered to regulate PKC𝛼 expression in response to a singleagonist [46]. Hence, the differential recruitment of one ormore of these degradative pathways may provide a rationalefor fine tuning the level of PKC𝛼 desensitisation requiredto downregulate hyperinflammatory responses; an attractiveproposal gave that CTMC exhibit the least degranulationpotential and are not as effective at producing cytokines asthe mucosal-type BMMC. Overall, as we have also found thatthe inhibitors alone canmodulate PKC𝛼 expression in PDMCandmucosal-type BMMC, these findings collectively indicatethat regulation of this key signalling element in mast cells istightly controlled by a complex anddynamic system involvingboth proteosomal and lysosomal routes of degradation.

Journal of Parasitology Research 11
LPS
LPSTLR4 TLR4 LPS
Ag ES-62 Ag ES-62
PDMC
PDMCCTMC
MyD88
Calcium
CalciumMyD88
Chemokines
Eicosanoids
Degranulation
LPS LPS
?
Ag-induced Ag-inducedLPS-inducedCytokines Cytokines
Cytokines
DegranulationDegranulation
Mucosal-type BMMC
Mucosal-type BMMC
+++
+++
+++
+++
−
−
−−
±
±
±
±++
++
++
+ +
+
+
++
+
PKC𝛼PKC𝛼PKC𝛿
Fc𝜀RI
Fc𝜀RI Fc𝜀RI Fc𝜀RI
Fc𝜀RI
Figure 6: Model of differential desensitisation of mast cell subsets by ES-62. Mucosal-type BMMC, CTMC, and PDMC exhibit differentialfunctional responses to antigen (Ag)-mediated cross-linking of Fc𝜀RI and stimulation with LPS as summarised. The signalling mechanismsunderlying the coupling to these differential responses and their desensitisation by ES-62 have not been fully delineated but our workingmodel is that the Fc𝜀RI-mediated degranulation observed in PDMC involves PKC𝛼 and calcium mobilisation which are effectively targetedby ES-62. Although these cells express TLR4/MyD88, they are uncoupled from downstream functional LPS signalling by an as yet unknownmechanism. By contrast, mucosal-type BMMC exhibit both degranulation (via Ag/Fc𝜀RI) and cytokine (via Fc𝜀RI and LPS/TLR4) responses,requiring recruitment of additional signals such as PKC𝛿 and MyD88 signalling which are both also targeted by ES-62.
Finally, whilst we have shown that ES-62 can suppressthe cytokine responses of both PDMC and the mucosal-type BMMC, it is clear that the levels of cytokines producedby PDMC in response to Fc𝜀RI- and LPS/TLR4 signallingare very low compared to those secreted by mucosal-typeBMMC. We have therefore addressed identifying whichsignals may be contributing to such higher levels of cytokineproduction by also determining the effects of ES-62 onPKC𝛿 expression as this signalling element has not only beenshown to be important for functional responses to Fc𝜀RI- andLPS/TLR4 signalling [40, 45, 51–53] but also to be a target fordownregulation by the parasite product in human mast cellsand B cells [35, 48]. In addition, we have also examined theeffect of ES-62 onMyD88, a pivotal signal transducer of TLR4[45, 51, 54] as we have shown it to be a target of ES-62 in coun-teringTh17 pathology [37] and only the MyD88-, and not theTRIF-dependent pathway of TLR4 signalling, appears to beactive in BMMC [55]. Consistent with the hypothesis thatadditional signals such as MyD88 and PKC𝛿 are required forthe augmented cytokine responses observed in BMMC rela-tive to PDMC, these studies show that whilst MyD88 expres-sion in PDMC is unchanged by exposure to ES-62, culture
with the parasite product results in downregulation of bothMyD88 and PKC𝛿 in mucosal-type BMMC (Figure 5(e)).
4. Conclusions
PDMC, mucosal-type BMMC, and CTMC mast cell popu-lations display differential functional responses with matureserosalmast cells predominantly acting like cells that performa specialised degranulation function. By contrast, BMMC,which have been reported to possess an immature mucosal-like phenotype that can further differentiate into mucosalor serosal mast cells display reduced degranulation andincreased cytokine responses. Consistent with the idea thatBMMC are plastic and can differentiate into either mucosalor serosal mast cells, CTMC display a comparable degran-ulation potential to that of mucosal-type BMMC and acytokine profile intermediate of mucosal-type BMMC andmature serosal/connective tissue PDMC. All three mast cellpopulations can be rendered hyporesponsive by ES-62 butthe selective nature of these effects suggests that ES-62 maybe targeting functions of the individual subtypes that are

12 Journal of Parasitology Research
specific to the particular inflammatory microenvironmentand phenotype.
The mechanisms underlying such desensitisation havenot been fully delineated but our workingmodel (Figure 6) isthat reduced degranulation and low level cytokine secretionreflect desensitisation of Fc𝜀RI- and LPS/TLR4-mediatedcalciummobilisation andPKC𝛼 signallingwhilst suppressionof the high levels of cytokine production by mucosal-typeBMMC in response to these signals requires downregulationof additional signals such as MyD88 and PKC𝛿. Such a rheo-stat effect allowing differential signal strength-dependentdesensitisation of receptor signalling would allow ES-62to provide an appropriate level of hyporesponsiveness thatwould prevent development of aberrant autoimmune andallergic inflammatory disorders whilst allowing appropri-ate levels of inflammation to generate protective immuneresponses to pathogenic infection.
Acknowledgments
The authors would like to thank the Wellcome Trust and theAmerican Asthma Foundation for supporting this researchand the following funding bodies for the awards of Ph Dstudentships toD. Ball (MRC andUofG); K. S. Bell (SULSA);and M. L. Coates (BBSRC). The authors have no conflict ofinterests.
References
[1] J. P. Kinet, “The high-affinity IgE receptor (Fc epsilon RI): fromphysiology to pathology,”Annual Review of Immunology, vol. 17,pp. 931–972, 1999.
[2] J. P. Kinet, “The essential role of mast cells in orchestratinginflammation,” Immunological Reviews, vol. 217, no. 1, pp. 5–7,2007.
[3] J. M. Xu and G. P. Shi, “Emerging role of mast cellsand macrophages in cardiovascular and metabolic diseases,”Endocrine Reviews, vol. 33, pp. 71–108, 2012.
[4] S. J. Galli and M. Tsai, “IgE and mast cells in allergic disease,”Nature Medicine, vol. 18, pp. 693–704, 2012.
[5] O. Malbec, K. Roget, C. Schiffer et al., “Peritoneal cell-derivedmast cells: an in vitro model of mature serosal-typemousemastcells,” Journal of Immunology, vol. 178, no. 10, pp. 6465–6475,2007.
[6] S. J. Galli, M. Grimbaldeston, and M. Tsai, “Immunomodu-latory mast cells: negative, as well as positive, regulators ofimmunity,” Nature Reviews Immunology, vol. 8, no. 6, pp. 478–486, 2008.
[7] S. N. Abraham and A. L. S. John, “Mast cell-orchestratedimmunity to pathogens,” Nature Reviews Immunology, vol. 10,no. 6, pp. 440–452, 2010.
[8] J. Kalesnikoff and S. J. Galli, “New developments in mast cellbiology,” Nature Immunology, vol. 9, no. 11, pp. 1215–1223, 2008.
[9] D. Ribatti and E. Crivellato, “Chapter 4 the controversial roleof mast cells in tumor growth,” International Review of Cell andMolecular Biology, vol. 275, pp. 89–131, 2009.
[10] M. F. Gurish and J. A. Boyce, “Mast cells: ontogeny, homing, andrecruitment of a unique innate effector cell,” Journal of Allergyand Clinical Immunology, vol. 117, no. 6, pp. 1285–1291, 2006.
[11] A. A. Irani, N. M. Schechter, and S. S. Craig, “Two types ofhuman mast cells that have distinct neutral protease compo-sitions,” Proceedings of the National Academy of Sciences of theUnited States of America, vol. 83, no. 12, pp. 4464–4468, 1986.
[12] T. C. Moon, C. D. St Laurent, K. E. Morris et al., “Advancesin mast cell biology: new understanding of heterogeneity andfunction,”Mucosal Immunology, vol. 3, no. 2, pp. 111–128, 2010.
[13] M. Welle, “Development, significance, and heterogeneity ofmast cells with particular regard to the mast cell-specificproteases chymase and tryptase,” Journal of Leukocyte Biology,vol. 61, no. 3, pp. 233–245, 1997.
[14] S. J. Galli, N. Borregaard, and T. A. Wynn, “Phenotypic andfunctional plasticity of cells of innate immunity: macrophages,mast cells and neutrophils,” Nature Immunology, vol. 12, no. 11,pp. 1035–1044, 2011.
[15] A.M. Irani andL. B. Schwartz, “Humanmast cell heterogeneity,”Allergy Proceedings, vol. 15, no. 6, pp. 303–308, 1994.
[16] E. Crivellato and D. Ribatti, “The fundamental contributionof William Bate Hardy to shape the concept of mast cellheterogeneity,” British Journal of Haematology, vol. 150, no. 2,pp. 152–157, 2010.
[17] Y. Kitamura, “Heterogeneity of mast cells and phenotypicchange between subpopulations,” Annual Review of Immunol-ogy, vol. 7, pp. 59–76, 1989.
[18] C. C. Chen, M. A. Grimbaldeston, M. Tsai, I. L. Weissman, andS. J. Galli, “Identification of mast cell progenitors in adult mice,”Proceedings of the National Academy of Sciences of the UnitedStates of America, vol. 102, no. 32, pp. 11408–11413, 2005.
[19] C. B. Franco, C. C. Chen, M. Drukker, I. L. Weissman, and S. J.Galli, “Distinguishing mast cell and granulocyte differentiationat the single-cell level,” Cell Stem Cell, vol. 6, no. 4, pp. 361–368,2010.
[20] H. R. Rodewald, M. Dessing, A. M. Dvorak, and S. J. Galli,“Identification of a committed precursor for the mast celllineage,” Science, vol. 271, no. 5250, pp. 818–822, 1996.
[21] Y. Ogawa and J. A. Grant, “Mediators of anaphylaxis,” Immunol-ogy and Allergy Clinics of North America, vol. 27, no. 2, pp. 249–260, 2007.
[22] B. Echtenacher, D. N. Mannel, and L. Hultner, “Critical pro-tective role of mast cells in a model of acute septic peritonitis,”Nature, vol. 381, no. 6577, pp. 75–77, 1996.
[23] R. Malaviya, T. Ikeda, E. Ross, and S. N. Abraham, “Mast cellmodulation of neutrophil influx and bacterial clearance at sitesof infection through TNF-𝛼,” Nature, vol. 381, no. 6577, pp. 77–80, 1996.
[24] W.Dawicki and J. S.Marshall, “New and emerging roles formastcells in host defence,” Current Opinion in Immunology, vol. 19,no. 1, pp. 31–38, 2007.
[25] A. M. Gilfillan and M. A. Beaven, “Regulation of mast cellresponses in health and disease,” Critical Reviews in Immunol-ogy, vol. 31, no. 6, pp. 475–530, 2011.
[26] M. Arock, A. le Nours, O. Malbec, andM. Daeron, “Ex vivo andin vitro primary mast cells,”Methods in Molecular Biology, vol.415, pp. 241–254, 2008.
[27] K. Nagao, K. Yokoro, and S. A. Aaronson, “Continuous lines ofbasophil/mast cells derived from normal mouse bone marrow,”Science, vol. 212, no. 4492, pp. 333–335, 1981.
[28] D.D.Metcalfe, J. A.Mekori, andM.Rottem, “Mast cell ontogenyand apoptosis,”ExperimentalDermatology, vol. 4, no. 4, pp. 227–230, 1995.

Journal of Parasitology Research 13
[29] C. S. Lantz and T. F. Huff, “Differential responsiveness ofpurified mouse c-kit+ mast cells and their progenitors to IL-3and stem cell factor,” Journal of Immunology, vol. 155, no. 8, pp.4024–4029, 1995.
[30] K. Karimi, F. A. Redegeld, B. Heijdra, and F. P. Nijkamp,“Stem cell factor and Interleukin-4 inducemurine bonemarrowcells to develop into mast cells with connective tissue typecharacteristics in vitro,” Experimental Hematology, vol. 27, no.4, pp. 654–662, 1999.
[31] H. Takano, S. Nakazawa, Y. Okuno et al., “Establishment of theculture model system that reflects the process of terminal dif-ferentiation of connective tissue-type mast cells,” FEBS Letters,vol. 582, no. 10, pp. 1444–1450, 2008.
[32] K. Tsuji, K. Koike, A. Komiyama, A. Miyajima, K. I. Arai, and T.Nakahata, “Synergistic action of interleukin-10 (IL-10) with IL-3, IL-4 and stem cell factor on colony formation from murinemast cells in culture,” International Journal of Hematology, vol.61, no. 2, pp. 51–60, 1995.
[33] C. Benoist and D. Mathis, “Mast cells in autoimmune disease,”Nature, vol. 420, no. 6917, pp. 875–878, 2002.
[34] P. J. Bryce, M. L. Miller, I. Miyajima, M. Tsai, S. J. Galli, andH. C. Oettgen, “Immune sensitization in the skin is enhancedby antigen-independent effects of IgE,” Immunity, vol. 20, no. 4,pp. 381–392, 2004.
[35] A. J. Melendez,M.M.Harnett, P. N. Pushparaj et al., “Inhibitionof Fc𝜀RI-mediated mast cell responses by ES-62, a product ofparasitic filarial nematodes,”Nature Medicine, vol. 13, no. 11, pp.1375–1381, 2007.
[36] W. Harnett and M. M. Harnett, “Helminth-derived immuno-modulators: Can understanding the worm produce the pill?”Nature Reviews Immunology, vol. 10, no. 4, pp. 278–284, 2010.
[37] M. A. Pineda, M. A. McGrath, P. C. Smith et al., “The parasitichelminth product ES-62 suppresses pathogenesis in CIA bytargeting of the IL-17-producing cellular network at multiplesites,” Arthritis & Rheumatism, vol. 64, no. 10, pp. 3168–3178,2012.
[38] J. Noguchi, E. Kuroda, and U. Yamashita, “Strain difference ofmurine bone marrow-derived mast cell functions,” Journal ofLeukocyte Biology, vol. 78, no. 3, pp. 605–611, 2005.
[39] H. S. Goodridge, F. A. Marshall, E. H. Wilson et al., “In vivoexposure of murine dendritic cell and macrophage bone mar-row progenitors to the phosphorylcholine-containing filarialnematode glycoprotein ES-62 polarizes their differentiation toan anti-inflammatory phenotype,” Immunology, vol. 113, no. 4,pp. 491–498, 2004.
[40] L. C. Wu, “Immunoglobulin E receptor signaling and asthma,”The Journal of Biological Chemistry, vol. 286, pp. 32891–32897,2011.
[41] G. Li, J. J. Lucas, and E.W. Gelfand, “Protein kinase C 𝛼, 𝛽I, and𝛽II isozymes regulate cytokine production inmast cells throughMEKK2/ERK5-dependent and -independent pathways,” Cellu-lar Immunology, vol. 238, no. 1, pp. 10–18, 2005.
[42] I. T. Abdel-Raheem, I. Hide, Y. Yanase et al., “Protein kinase C-𝛼mediates TNF release process in RBL-2H3 mast cells,” BritishJournal of Pharmacology, vol. 145, no. 4, pp. 415–423, 2005.
[43] C. Yang, X. Mo, J. Lv et al., “Lipopolysaccharide enhancesFceRI-mediated mast cell degranulation by increasing Ca2+entry through store-operated Ca2+ channels: implications forlipopolysaccharide exacerbating allergic asthma,” ExperimentalPhysiology, vol. 97, no. 12, pp. 1315–1327, 2012.
[44] Y. I. Nigo, M. Yamashita, K. Hirahara et al., “Regulation ofallergic airway inflammation through Toll-like receptor 4-mediated modification of mast cell function,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 103, no. 7, pp. 2286–2291, 2006.
[45] D. J. Loegering and M. R. Lennartz, “Protein kinase C and toll-like receptor signaling,” Enzyme Research, vol. 2011, Article ID537821, 7 pages, 2011.
[46] O. V. Leontieva and J. D. Black, “Identification of two distinctpathways of protein kinase C𝛼 down-regulation in intestinalepithelial cells,” Journal of Biological Chemistry, vol. 279, no. 7,pp. 5788–5801, 2004.
[47] C. Prevostel, V.Alice,D. Joubert, andP. J. Parker, “Protein kinaseC𝛼 actively downregulates through caveolae-dependent trafficto an endosomal compartment,” Journal of Cell Science, vol. 113,part 14, pp. 2575–2584, 2000.
[48] M. R. Deehan, M. M. Harnett, and W. Harnett, “A filarialnematode secreted product differentially modulates expressionand activation of protein kinase C isoforms in B lymphocytes,”Journal of Immunology, vol. 159, no. 12, pp. 6105–6111, 1997.
[49] S. Lee, Y. Sato, and R. A. Nixon, “Lysosomal proteolysisinhibition selectively disrupts axonal transport of degradativeorganelles and causes an Alzheimer’s-like axonal dystrophy,”Journal of Neuroscience, vol. 31, no. 21, pp. 7817–7830, 2011.
[50] K. Xiao and S. K. Shenoy, “𝛽2-adrenergic receptor lysosomaltrafficking is regulated by ubiquitination of lysyl residues in twodistinct receptor domains,” Journal of Biological Chemistry, vol.286, no. 14, pp. 12785–12795, 2011.
[51] K. Newton and V. M. Dixit, “Signaling in innate immunity andinflammation,” Cold Spring Harbor Laboratory Press. In press.
[52] Y. Kim, K. Kim, H. Lee et al., “Celastrol binds to ERKand inhibits Fc𝜀RI signaling to exert an anti-allergic effect,”European Journal of Pharmacology, vol. 612, no. 1–3, pp. 131–142,2009.
[53] Y. Kim, Y. S. Lee, J. H. Hahn et al., “Hyaluronic acid targetsCD44 and inhibits Fc𝜀RI signaling involving PKC𝛿, Rac1, ROS,andMAPK to exert anti-allergic effect,”Molecular Immunology,vol. 45, no. 9, pp. 2537–2547, 2008.
[54] L. A. J. O’Neill and A. G. Bowie, “The family of five: TIR-domain-containing adaptors in Toll-like receptor signalling,”Nature Reviews Immunology, vol. 7, no. 5, pp. 353–364, 2007.
[55] S. Keck, I. Muller, G. Fejer et al., “Absence of TRIF signalingin lipopolysaccharide-stimulated murine mast cells,” Journal ofImmunology, vol. 186, no. 9, pp. 5478–5488, 2011.

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2013, Article ID 329438, 11 pageshttp://dx.doi.org/10.1155/2013/329438
Review Article�elminths� Immunore�ulation and In�ammator�Diseases—Which Side Are Trichinella spp. and Toxocara spp. on?
Carmen Aranzamendi,1 Ljiljana Sofronic-Milosavljevic,2 and Elena Pinelli1
1 Centre for Infectious Disease Control Netherlands, National Institute for Public Health and the Environment (RIVM),P.O. Box 1, 3720 BA Bilthoven, e Netherlands
2 Institute for the Application of Nuclear Energy (INEP), University of Belgrade, Banatska 31b, 11080 Belgrade, Serbia
Correspondence should be addressed to Elena Pinelli; [email protected]
Received 30 September 2012; Accepted 1 December 2012
Academic Editor: Fabrizio Bruschi
Copyright © 2013 Carmen Aranzamendi et al. is is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Macropathogens, such as multicellular helminths, are considered masters of immunoregulation due to their ability to escape hostdefense and establish chronic infections. Molecular crosstalk between the host and the parasite starts immediately aer theirencounter, which in�uences the course and development of both the innate and adaptive arms of the immune response. Helminthscan modulate dendritic cells (DCs) function and induce immunosuppression which is mediated by a regulatory network thatincludes regulatory T (Treg) cells, regulatory B (Breg) cells, and alternatively activatedmacrophages (AAMs). In this way, helminthssuppress and control both parasite-speci�c and unrelated immunopathology in the host such as 1-mediated autoimmune and2-mediated allergic diseases. However, certain helminths favour the development or exacerbation of allergic responses. In thispaper, the cell types that play an essential role in helminth-induced immunoregulation, the consequences for in�ammatory diseases,and the contrasting effects of Toxocara and Trichinella infection on allergic manifestations are discussed.
1. Introduction
Immune responses induced by helminths are predominantlyof the 2 type involving cytokines such as interleukin-3 (IL-3), IL-4, IL-5, IL-9, IL-10, and IL-13.ese cytokinesmediateimmune responses typically characterized by increased levelsof circulating IgE antibodies, eosinophils, basophils, andmast cells [1]. During infection, the immune system isexposed to different helminth-derived molecules, includingproteins, lipids, and glycoconjugates present either at thesurface of the worms or in the excretory-secretory (ES)products [2]. Interaction of helminth-derivedmolecules withhost cells can result in a shi of the immune response,from an in�ammatory towards an anti-in�ammatory type ofresponse. Helminth-derived molecules can modify dendriticcells (DCs) function and downregulate adaptive immuneresponses, through the induction of a regulatory networkthat include regulatory T (Treg) cells, alternatively acti-vated macrophages (AAMs), and regulatory B (Breg) cells.e induced immunosuppresive network, together with
cytokines produced by diverse hematopoietic and non-hematopoietic cells as integral part of immunoregulatorypathways, appears to be essential for parasite survival and itseffect can be extended to other in�ammatory disorders suchas allergies and autoimmune diseases [3, 4]. However, theassociation between helminth infections and allergy does notalways have an unequivocal outcome.While certain helminthinfections protect against allergic diseases (reviewed in[5]), other helminths can exacerbate this immunopathology(reviewed in [6]). Here, the role of DCs, Treg, and otherregulatory cells in helminth-induced immunoregulation, theconsequences for in�ammatory diseases, and the contrastingeffects of Toxocara and Trichinella infections on allergicmanifestations are discussed.
2. Dendritic Cells
DCs are sentinels on alert for possible danger signals toimmediately activate local innate immune responses and

2 Journal of Parasitology Research
subsequently, aer antigen presentation, initiate the properadaptive immune responses. Interaction with DCs deter-mines the function and cytokine production of lympho-cytes. DCs play therefore an essential role in shaping theimmune response and controlling the course of infection[7]. ese cells are located throughout the body forminga complex network that allows them to communicate withdifferent populations of lymphocytes. Different DC subsetsmay have distinct locations, where they acquire antigensto be transported to the draining lymph nodes for T-cellpriming [8]. DCs as well as other innate immune cells possessvarious families of pattern recognition receptors (PRRs) suchas Toll-like receptors (TLRs), NOD-like receptors, RIG-likereceptors, and the C-type lectin receptors (CLRs) that allowthem to recognize a great variety of pathogen-associatedmolecular patterns (PAMPs). Aer pathogen recognition viavarious PRR, DCs produce molecules that induce polariza-tion of different types of responsiveness such as 1-, 2-,17-, or Treg-related. e response of DCs to pathogens ismediated in large part via TLR, with input from other PRRresulting in changes in gene expression that leads to DCsmaturation. Maturation of these cells refers to a transitionfrom a resting state into a more dynamic state in whichthe cells present antigen in the context of MHC, expresscostimulatory molecules such as CD40, CD80, and CD86,and secrete a broad spectrum of cytokines and chemokines[9]. TLR-mediated responses are controlled mainly by theMyD88-dependent pathway, which is used by all TLR exceptTLR3- and by the TIR-domain-containing adapter-inducinginterferon-𝛽𝛽-(TRIF)-dependent pathway, which is used byTLR3 and TLR4 [10]. TLRs have been implicated in therecognition of helminth products byDC. For instance, Lacto-N-fucopentaose III (LNFPIII) produced by trematode Schis-tosomamansoni, and ES-62, a phosphorylcholine-containingprotein secreted by the nematode Acanthocheilonema viteae,can condition DCs to induce 2 responses through TLR4[11]. Likewise, monoacetylated phosphatidyl serine lipidsfrom schistosomes speci�cally instruct DCs to preferentiallyinduce IL-10-producing Treg in a TLR2-dependent manner[12]. is was also demonstrated in TLR2-de�cient micethat showed a reduced number of CD4+CD25+ Treg cellsand immunopathology during schistosomiasis [13]. CLRson DCs also play an important role in sensing helminthglycans. Studies using schistosomal antigens suggest thathelminth glycans may be the conserved molecular patternthat instructs DCs via CLR to drive 2-polarized responses[14]. Other recent studies demonstrate that host-like glycanantigens expressed by many helminths are recognized byDCs via lectin receptors [2]. Schabussova et al. reported onblood group-like glycans from T. canis that bind the lectinDC-SIGN (Dendritic Cell-Speci�c Intercellular adhesionmolecule-3-Grabbing Nonintegrin) [15], which may enablethe activation of signal transduction pathways involving Raf-1 and subsequent modulation of DC maturation resulting inskewing towards a 2 responses [16]. Lewis X antigen, ahost-like glycan expressed on the surface of schistosomes inall life stages which is also present in secreted products suchas the soluble egg antigens (SEAs), also binds to DC-SIGN[17].
DC maturation is considered to be essential for DCsto induce T-cell responses. It has become clear that DCsresponding to helminth products do not mature in theconventional way upon encountering parasitic antigens butacquire a semimatured status and are still capable of inducingT-cell polarization. Several studies support the �ndings thathelminth products fail to directly activate DCs and otherstudies show that helminth products suppress DC mat-uration. For instance, SEA suppresses lipopolysaccharide-(LPS-) induced activation of immature murine DCs, asindicated by decreased MHC class II and costimulatorymolecules expression in addition to IL-12 production. isresulted in increased LPS-induced production of IL-10 byDC aer incubation by SEA [18]. Pretreatment of DCsand macrophages with ES-62 also inhibits their ability toproduce IL-12p70 in response to LPS [19]. In anotherstudy, a mixture of high molecular weight componentsfrom Ascaris suum was found to reduce the LPS-inducedexpression of MHCII, CD80, CD86, and CD40 moleculeson mouse CD11c+ DCs and to hampered T-cell proliferativeresponses in vitro. is inhibitory effect was abolished in IL-10-de�cient mice [20]. Fasciola hepatica tegumental antigenalone did not induce cytokine production or cell surfacemarker expression on murine DCs� however, it signi�cantlysuppressed cytokine production and cell surface markerexpression in DCs matured with a range of TLR and non-TLR ligands [21]. In vitro studies on the impact of T.spiralis excretory/secretory products (TspES) on mice DCsrevealed that these parasitic antigens suppressDCmaturationinduced by LPS derived from different bacteria [22]. In thisstudy, different TLR agonists were used showing that thesuppressive effect of TspES on DC maturation is restrictedto TLR4. ese helminth products were also shown tointerfere with the expression of several genes related to theTLR-mediated signal transduction pathways. For rat bone-marrow-derived DC it has been shown that aer incubationwith TspES these DCs acquire a semimatured status whichis re�ected in moderate upregulation of CD86, signi�cantupregulation of ICAM1 (Intercellular Adhesion Molecule 1),and no upregulation of MHC II, accompanied by impairedproduction of IL-12 p70 [23].
3. Regulatory T Cells
Treg cells control peripheral immune responses and arelikely to play a central role in autoimmune, infectious,and allergic diseases. ree phenotypes of Treg have beendescribed to date, categorized according to their origin,function, and expression of cell surface markers: naturalTreg cells (CD4+CD25+Foxp3+) and inducible Treg cells thatinclude the IL-10-producing Tr1 cells and the Foxp3+ T cellsinduced in the periphery [24]. In spite of the complexityof regulatory cell types, CD4+CD25+Foxp3+ Treg cells arethe most prominent population of immunoregulatory cellsknown so far to be induced during helminth infections [4].
Early studies had already suggested regulatory T-cellactivity during chronic helminth infections in humans.Doetze et al. reported that IL-10 and transforming

Journal of Parasitology Research 3
growth factor-𝛽𝛽 (TGF-𝛽𝛽) production mediated thehyporesponsiveness observed in PBMC from individualswith generalized onchocercosis caused by the �larialnematode Onchocerca volvulus [25]. In a study with �lariasispatients, lymphedema was associated with a de�ciency in theexpression of Foxp3, GITR (glucocorticoid-induced tumour-necrosis-factor-receptor-related protein), TGF-𝛽𝛽, andCTLA-4 (cytotoxic T-lymphocyte antigen 4), known to be expressedby Treg cells [26], while in children infected with intestinalnematodes (Ascaris lumbricoides andTrichuris trichiura) highlevels of IL-10 and TGF-𝛽𝛽 in addition to generalized T-cellhyporesponsiveness were found [27, 28]. Likewise, Schisto-some-infected individuals in Kenya and Gabon had higherCD4+CD25+ and CD4+CD25+Foxp3+ T-cell levels com-pared with uninfected individuals [29]. One of the studiesproviding evidence on the suppressive effect of Treg cells fromhelminth-infected individual is the one reported byWammeset al. [30]. In this study, carried out in Indonesia, Treg cellsfrom geohelminth-infected individuals weremore effective atsuppressing proliferation and IFN-𝛾𝛾 production by effector Tcells in response to malaria antigens and BCG than Treg cellsfromhealthy individuals. A �larial parasite of humans,Brugiamalayi, was found to secrete TGH-2 (transforming growthfactor homologue-2), a homologue of host TGF-𝛽𝛽 [31].Since the recombinant TGH-2 can bind to the mammalianTGF-𝛽𝛽 receptor, it has been suggested that it can promotethe generation of regulatory T cells, as it has been shown formammalian TGF-𝛽𝛽. In another study a signi�cant increasedexpression of Foxp3 and regulatory effector molecules suchas TGF-𝛽𝛽, CTLA-4, PD-1 (programmed death 1) and ICOS(inducible costimulatory molecule) was found in �laria-infected compared to uninfected individuals in response tolive infective-stage larvae or micro�lariae of Brugia malayi[32].
Various studies on the role of Treg cells in helminthinfections have used animal models. In mice, CD25+ Tregcells were shown to restrain the pathology to helminth eggsduring schistosome infection [13] and to Trichuris murisin the gut [33]. Moreover, depletion of CD25+ Treg cellswith combined antibodies to CD25 and GITR resulted inenhanced immunity to �larial nematode Litomosoides sig-modontis in mice [34]. Generation of Treg cells with elevatedexpression of Foxp3 during helminth infection has also beendemonstrated. For instance, infection of BALB/c mice withBrugia pahangi third-stage larvae (L3) resulted in expansionof a population of CD4+CD25+ T cells which was highlyenriched in Foxp3 and IL-10 gene expression [35]. Inductionof Treg cells was demonstrated to be necessary to establisha chronic L. sigmodontis infection since depletion of Tregcells in susceptible mice prior to infection enhanced parasitickilling and cleared the infection [36]. In chronic infectionwith the gastrointestinal helminth Heligmosomoides poly-gyrus, it was established that levels of Foxp3 expressionwithinthe CD4+ T-cell population of mice mesenteric lymph nodeswere signi�cantly increased and that puri�ed CD4+CD25+Treg cells possess suppressive activity in vitro [37, 38].
e effect of TspES on T-cell activation in vitrowas inves-tigated using splenocytes derived from ovalbumin- (OVA)-TCR transgenic D011.10 mice that were incubated with
TspES-pulsed DC+OVA. Results indicate that the presenceof TspES resulted in expansion of CD4+CD25+ T cells thatexpress high levels of Foxp3+. ese Treg cells were shownto have suppressive activity and to produce TGF-𝛽𝛽. Togetherthese results indicate that T. spiralis secretion products caninduce expansion of functional Treg cells in vitro [22].
In a rat model, the infection with T. spiralis is accom-panied with the increase proportion of Foxp3+ Treg cells[23]. In vitro studies showed that DCs stimulated with TspEScaused strong 2 polarization, accompanied by elevatedproduction of the regulatory cytokines IL-10 and TGF-𝛽𝛽[23]. However, unlike the mouse model described previously,conditioned rat DCs generated no increase in the proportionof CD4+CD25+Foxp3+ T cells. In vivo T-cell priming withTspES stimulated DCs resulted in mixed 1/2 cytokineresponse, with the dominance of the 2 type and elevatedlevels of regulatory cytokines. Signi�cant increase in theproportion of CD4+CD25+Foxp3+ cells was found in spleencells of recipients that received TspES stimulated DCs com-pared to the control value obtained from rats that receivedDCs cultivated in medium only.
4. Other Regulatory Cells
Helminth infections may also lead to expansion ofimmunoregulatory cells other than Treg cells, includingalternatively activated macrophages (AAMs) andregulatory B cells. Signals encountered during migration bydeveloping macrophages determine their function at sites ofin�ammation or infection. Among these signals, cytokinesare responsible for the development of highly divergentmacrophage phenotypes: classically activated and AAMs[39]. Prieto-Lafuente et al. reported that the homologues ofthe mammalian cytokine macrophage migration inhibitoryfactor (MIF) expressed by Brugia malayi synergized withIL-4 to induce the development of suppressive AAMs in vitro[40]. One pathway for this effect may be through the MIF-mediated induction of IL-4R expression on macrophages,amplifying in this way the potency of IL-4 itself. us, in a2 environment, MIF may prevent the classical activationof macrophages. e suppressive effect of AAMs on theimmune response is most likely dependent on the expressionof arginase-1 (Arg-1) as indicated by studies in which micemacrophages lacking Arg-1 failed to suppress 2 responses(reviewed in [41]).
B cells possess a variety of immune functions, includ-ing production of antibodies, presentation of antigens, andproduction of cytokines. IL-10-producing regulatory B cellshave great potential to regulate T-cell-mediated in�am-matory responses [5] and to downmodulate experimentalautoimmune encephalomyelitis, collagen-induced arthritis,and in�ammatory bowel disease [42]. In addition, in mousemodels of chronic parasitic in�ammation, such as chronicschistosomiasis, IL-10-producing B cells were also reportedto be associated with protection against anaphylaxis [43].Moreover, H. polygyrus-infected mice induced regulatory Bcells that can downmodulate both allergy and autoimmunityin an IL-10 independent manner [44].

4 Journal of Parasitology Research
5. Helminth Infections andIn�ammator� �iseases
e helminth-induced immunosuppresive network may notonly be bene�cial for the parasite, but it can also have bene�-cial outcomes for the host, reducing allergic and autoimmunediseases [41, 45]. Epidemiological, cross-sectional studiessupport an inverse correlation between allergic diseases andhelminth infection [46, 47] including infections by nema-tode species like A. lumbricoides and Necator americanus[48]. An increased skin reactivity to house dust mites wasfound aer antihelminthic treatment against infection withA. lumbricoides and T. trichiura [49]. Studies performed inanimal model system have con�rmed that helminth infec-tion can protect against allergic disease and in particularlung-associated in�ammation. For instance, S. mansoni-infected BALB/c mice were protected against OVA-inducedexperimental allergic airway in�ammation (EAAI) as indi-cated by reduction of eosinophils in BAL, 2 cytokineproduction, OVA-speci�c IgE levels and reduction of thenumber of in�ammatory cells in lungs. �ere, induction ofCD4+CD25+Foxp3+ regulatory T cells was independent ofIL-10 [50]. Dittrich et al. found that chronic infection withthe �larial parasite Litomosoides sigmodontis suppressed allpathological features of the OVA-induced EAAI model [51].Additionally, these authors observed signi�cantly increasednumbers of Treg cells in spleen and mediastinal lymphnodes in infected OVA-treated mice compared to OVA-controls animals. Suppression of EAAI during the course ofH. polygyrus infection was shown to involve the inductionof Treg cells [52]. Infection with the same parasite resultedalso in the inhibition of allergic response to peanut extract[53].
Several epidemiological studies have investigated the pro-tective effect of parasitic infections in different autoimmunediseases like multiple sclerosis and type 1 diabetes [54].Studies indicate that persons infected with chronic parasiticworm infections have lower rates of in�ammatory boweldisease (IBD) than persons without these infections [55].Experiments carried out using animal models of humanautoimmune diseases have shown that parasites can interferewith autoimmunity. Schistosoma mansoni infection has beenshown to protect from type 1 diabetes [56] and reducesthe severity of EAE [57] while infection with H. polygyrussuppresses the experimental colitis [58]. Infection with L.sigmodontis prevented diabetes in NOD mice. In this study,protection was associated with increased 2 responses andTreg cell numbers [59].
e immunomodulatory effect of helminth-derivedproducts has been extensively studied. Table 1 providesan overview of different helminthic antigens withimmunoregulatory properties. Findings regarding the useof parasite antigens to suppress experimental in�ammatorydiseases are summarized in Table 2.
Although the majority of data suggest that infection withhelminths is associated with a suppression of allergic andautoimmune responses, some examples provide the oppositeview. Epidemiological studies indicate that infection withAscaris spp, Toxocara spp, Fasciola hepatica, hookworms,
or Enterobius vermicularis has no protective effects or evenenhanced allergic responses (reviewed in [95]).
ere are also experimental studies that show that infec-tion with some helminths have a positive association withallergy. A study using a murine model has shown that T.canis infection results in exacerbation of EAAI [96]. Otheranimal experiments provided evidence that parasites likeNippostrongylus brasiliensis [97] and B. malayi [98] couldalso induce or exacerbate allergic responses. Exacerbation ofanaphylaxis has been shown to occur during T. spiralis infec-tion [99]. e links between infections and autoimmunityare complex and there is scarce evidence on the inductionor exacerbation of autoimmune responses by helminths[100].
6. Contrasting Effect ofToxocara and Trichinella Infections onIn�ammator� �iseases
Toxocara canis and Toxocara cati are roundworms of dogsand cats, respectively, that can also infect humans worldwide.Aer ingestion of the infectious Toxocara eggs, the larvaemigrate to the intestine, liver, and lungs. While in dogs andcats under the age of 6 months, the larva migrate back tothe intestine; in humans migration continues to other organswhere they can persist for many years [101]. Toxocara infec-tion results in the induction of 2 cells that make cytokinessuch as IL-4, IL-5, and IL-13, which induce responses tothe parasite such as increased IgE levels and eosinophilia(reviewed in [6]). Trichinella spiralis is also a roundworm thatinfects different mammals including humans and mice. Aeringestion of Trichinella infected meat, the larvae migrate tothe intestine and matures to the adult stage, the parasitesmate, and �nally the newborn larvae (NBL) migrate tostriated muscle cells where they become encysted. Infec-tion with T. spiralis is characterized by the induction ofa 1 type of response at the beginning of the intestinalphase. When the NBL disseminate, a dominant 2 typeof response develops which is essential for parasite expul-sion [102]. Ingestion of both Toxocara spp. and Trichinellaspp. commonly results in chronic infections. Interestinglythese helminths have a contrasting effect on in�ammatorydiseases, while infections with Trichinella spp. can suppress(reviewed in [103]) Toxocara spp. exacerbate in�ammatorydiseases [6]. Studies using animal models for human autoim-mune and allergic diseases indicate that Trichinella infectionameliorates these immune disorders (Table 3). Khan et al.showed that T. spiralis infection reduces the severity ofdinitrobenzenesulphonic-acid- (DNBS-) induced colitis inC57BL/6 mice [88]. Motomura et al. demonstrated that inaddition to the protection exerted by the actual infection,rectal submucosal administration of T. spiralis crude musclelarvae antigen can also protect [78]. T. spiralis infection alsoameliorated autoimmune diabetes in NOD mice [89] andmodulated severity of the disease in the experimental modelof multiple sclerosis (MS), namely, experimental autoim-mune encephalomyelitis (EAE) in Dark Agouti rats in a dose-dependent manner [90]. In this study severity of EAE as

Journal of Parasitology Research 5
T 1: Helminth-derived antigens with immunoregulatory properties.
Helminth Antigen Immunoregulatory mechanism References
Schistosoma mansoni LNFPIII (lacto-N-fucopentaoseIII)/SEA(soluble egg antigen) Interact with TLR4 to produce 2 polarizing DCs [60]
Schistosoma mansoni Schistosome lysophosphatidylserine Interact with TLR2 to induce Treg polarizing DCs [61]
Acanthocheilonemaviteae ES-62
Exert immunomodulatory effects on macrophages andDCs by a TLR4-dependent mechanism withconsequent 2 polarisation
[62–64]
Nippostrongylusbrasiliensis Excretory-secretory antigen (NES) Potently induce 2 type of response via DC [65]
Brugia malayi adultCystatins (cysteine protease inhibitors)CIP-2
Interfere with antigen processing in human cells andinhibits B cells [66, 67]
Cytokine homologue MIF-1/2 Alternatively activate macrophages [68]Brugia malayimicro�lariae
Serpins (serine protease inhibitors)SPN-2
Block neutrophil protease and promote 1 type ofresponse [69]
Brugia malayi L3 larvae ALT-1/2 proteins Inhibit macrophage resistance and present good �larialvaccine candidate [70]
Toxocara canis TES32—C type lectin (CTL) Inhibit TLR responses on DC and compete with hostlectins for ligands, thereby blocking host immunity [71, 72]
Heligmosomoidespolygyrus Excretory-secretory antigen (HES) Induce regulatory T cells through TGF-𝛽𝛽R [37]
Teladorsagiacircumcincta Excretory-secretory antigen Induce generation of Foxp3+ regulatory T cells through
TGF-𝛽𝛽 mimicking effect [73]
Trichinella spiralis
Adult excretory-secretory antigen(AdES); newborn larvae antigen (NBL);crude muscle larvae antigen (MLCr)
All antigens from different life stages inducepolarization towards mixed 1/2 withpredominance of 2 response, via semimatured DC
[74]
Excretory secretory muscle larvae antigenInduce mixed 1/2 response with thepredominance of 2 component and elicit regulatoryarm of immune response
[75]
Excretory secretory muscle larvae antigen Interfere with LPS-induced DC maturation and induceexpansion of Foxp3+ regulatory T cells [22]
Fasciola hepatica ioredoxin peroxides Alternatively activated macrophages [76]
T 2: Suppression of experimental in�ammatory diseases by parasite-derived antigens.
Helminth Antigen Model Reference
Trichinella spiralis Soluble antigens of muscle larvae EAEDNBS-induced colitis
[77][78]
Trichuris suis Soluble antigens of adult worm EAE [77]
Ancylostoma ceylanicum Soluble and excretory-secretory antigens of adult worm DSS-induced colitis [79]Hymenolepis diminuta Soluble antigens of adult worm DNBS-induced colitis [80]Heligmosomoides polygyrus Excretory-secretory antigens (HES) of adult worm EAAI [73]Ancylostoma caninum Excretory-secretory antigens of adult worm TNBS-induced colitis [81]Acanthocheilonema vitae ES-62 Collagen-induced arthritis [82]
Schistosoma mansoniSoluble antigens of adult worm TNBS-induced colitis [81]SEA and soluble adult worm antigen T1D [83]Recombinant proteins (Sm22⋅6, Sm29) and soluble adultworm fraction (PIII) EAAI [84]
Schistosoma japonicum SEA EAAI [85]Nippostrongylus brasiliensis Excretory-secretory antigens (NES) of adult worm EAAI [86]Ascaris suum Soluble antigens of adult worm EAAI [87]EAE: experimental autoimmune encephalomyelitis; DNBS: dinitrobenzene sulfonic acid; TNBS: trinitrobenzene sulfonic acid; DSS: dextran sodium sulfate;T1D: type 1 diabetes; EAAI: experimental allergic airway in�ammation.

6 Journal of Parasitology Research
T 3: Experimental models of 2-mediated in�ammatory dis-eases successfully treated by Trichinella infection or administrationof Trichinella antigens.
Trichinella spp. or theirproducts
Experimentaldisease model Reference
T. spiralis
Exp. colitis [88]T1D [89]EAE [90]EAE [91]EAAI [92]EAAI [22]
T. pseudospiralis EAE [93]EAE [94]
T. spiralis crude muscle larvaeantigen
Exp. colitis [78]EAE [77]
Exp. colitis: experimental colitis; T1D: type 1 diabetes; EAE: experimentalautoimmune encephalomyelitis; EAAI: experimental allergic airway in�am-mation.
judged by cumulative disease index, maximal clinical score,duration of illness, and the number of mononuclear cellsin�ltrating the spinal cord in T. spiralis infected animals wereall reduced in comparison to the uninfected EAE-inducedgroup. In a following study, these authors reported thatalleviation of the disease in infected-EAE rats coincided withreduced IFN-𝛾𝛾 and IL-17 production and increased IL-4, IL-10, and TGF-𝛽𝛽 production. ey suggested that mechanismsunderlying the observed bene�cial effect include 2 andregulatory responses provoked by the parasite. Transfer ofT-cell-enriched spleen cells from T. spiralis-infected ratsthat contained a higher proportion of CD4+CD25+Foxp3+regulatory T cells into rats in which EAE was induced causedamelioration of EAE, which indirectly points to the role ofTreg in restraining in�ammatory conditions [91]. Boles etal. have shown with another Trichinella species, namely, withTrichinella pseudospiralis, that infection results in suppressionof MS in the rat [93]. ese authors used this modelto compare the anti-in�ammatory effects of the intestinaland late migratory phases of T. pseudospiralis infection ondevelopment of myelin-basic-protein- (MBP-) induced MS-like debilitation. Findings from this study indicate that thelate migratory phase of infection which occurred duringthe peak of MBP-induced debilitation signi�cantly improvedperformance scores in mobility, coordination, and strength.Wu et al. also reported on amelioration of clinical severityand delayed onset of EAE aer T. pseudospiralis infection.is effect was associated with suppression of 17 and 1responses induced by infection [94].Trichinella pseudospiralisis markedly different from T. spiralis in that it is smallerin size and that the muscle stage larvae are not surroundedby a capsule [104]. Whether the mechanisms involved inimmunosuppression varies depending on Trichinella speciesremains to be investigated.
Infection with T. spiralis can also ameliorate EAAI [92].In this study, the concentrations of IL-10 and TGF-𝛽𝛽 weresigni�cantly increased and the recruitment of Treg into
draining lymph nodes was elevated as the result of T. spiralisinfection. is protective effect has been recently shown tooccur during acute as well as chronic phases of Trichinellainfection [105]. Protection against EAAI toOVAwas strongerduring the chronic phase of infection and associated withincreased numbers of splenic CD4+CD25+Foxp3+ Treg cellswith suppressive activity. Adoptive transfer of CD4+ T cellsfrom chronically infected mice with elevated numbers ofTreg cells in the spleen induced partial protection againstEAAI [105].e possible mechanisms by which helminths ortheir products could inhibit allergic responses are depicted inFigure 1.
In contrast to the suppressive effect of Trichinella infec-tions on allergic diseases experimental as well as epidemi-ological studies indicate that Toxocara infections are riskfactors for allergies, including allergic asthma [6].
Studies using murine models for toxocariosis indicatethat infection with T. canis leads to persistent pulmonaryin�ammation, eosinophilia, increase levels of circulatingIgE, airway hyperreactivity, and production of -2 typecytokines. Pulmonary in�ammation has been shown todevelop as soon as 48 hours aer infection, it occurs in a dose-dependent manner, and it can persist up to 2 or 3 months.Eosinophil counts also increase in the bronchoalveolar lavage(BAL) of Toxocara-infected mice [106, 107]. Relative quan-ti�cation of cytokine expression in lungs of mice infectedwith different T. canis doses showed that while a proportionalincreased expression of the IL-4, IL-5, and IL-10 transcriptswas observed, the expression of IFN-𝛾𝛾was not different fromthat of uninfected controls [107]. Results from this study indi-cate that infection of mice with T. canis results in a dominant2 type of immune response, independent of the inoculumsize [108]. In addition, infection of BALB/c mice with 1,000T. canis embryonated eggs results in hyperreactivity of theairways that persisted up to 30 days p.i. Evaluation of parasiteburden revealed that few T. canis larvae were still present inthe lungs of infected mice at 60 days p.i. which could explainthe persistent pulmonary in�ammation observed in thesemice [107].
Common features between allergic asthma and toxo-cariosis are the induction of a 2-cell mediated immuneresponse including the production of high levels of IgE,and eosinophilia. In addition, infection with Toxocara spp.shares common clinical features with allergic asthma suchas in�ammation of the airways accompanied with wheezing,coughs, mucus hypersecretion, and bronchial hyperreactiv-ity. In order to study the effect of Toxocara infection onallergic manifestations two murine models were combined,namely, the murine model for toxocariosis described aboveand a murine model for allergic airway in�ammation. Forthis study BALB/c mice were infected with 500 embryonatedT. canis eggs and exposed to OVA sensitization followed byOVA-challenge. Results indicate that infection with T. canisin combination with OVA treatment led to exacerbation ofpulmonary in�ammation; eosinophilia; airway hyperrespon-siveness; increase of OVA speci�c and total IgE; increasedexpression of IL-4 compared to mice that were only T. canisinfected or OVA treated. e observed exacerbation of EAAIwas independent of the timing of infection in relation to

Journal of Parasitology Research 7
Treg
Allergens
Airway hyperreactivity
and inflammation
EoMc
Mucus production, eosinophilia, bronchoconstriction, smooth-
muscle contraction, airway remodelling
Helminths
DC ES
Th2
Breg
DC
B
AAM
Regulatory network
IgE
IL-10TGF-β
IL-10
IL-10
TGF-β
IL-4IL-13
IL-9
IL-5
↑ Arg-1
F 1: Mechanisms involved in immunosuppression induced by helminths and its effect on allergic responses. Helminths can modulatedendritic cells (DCs) function and induce regulatory T (Treg) cells. Other cells from the regulatory network include regulatory B (Breg) cellsand alternatively activated macrophages (AAMs). ese cells create an immunosuppressive (⊣) environment in which increased expressionof arginase 1 (Arg 1) in AAMs and the production of the cytokines IL-10 and TGF-𝛽𝛽 play an essential role in reducing allergic effectormechanisms.
allergen exposure. In conclusion, infection with T. canis leadsto exacerbation of EAAI [96].
Several factors may in�uence the differential effect ofhelminth infections on allergic diseases [6]. One of thesefactors is whether the host is de�nitive or accidental. enormal or de�nitive hosts for T. canis are dogs whereashumans are accidental hosts for this parasite. In an accidentalhost the parasite does not usually develop to the adult stageand in case of Toxocara spp. the continuous migration of thelarvae through different organs including the lungs can causemore damage comparing to what happens in a de�nitive hostwhere migration is transitory. T. spiralis can infect manydifferent mammals including mice and humans in whichthe parasite completes its life cycle. e infected mammal istherefore a de�nitive host for this helminth. And although T.spiralis pass through the lungmicrovascular systemon its wayto the skeletal muscle, it is a rapid process in which the larvaeare usually not trapped in the lungs [109]. It is likely thatthere are differences between parasites of humans such as T.spiralis that have evolved with their host and have developedstrategies to survive without causingmuch damage comparedto parasites such as Toxocara spp. for which humans areaccidental host [6, 110].
In conclusion, helminths induce an anti-in�ammatoryresponse, which could ameliorate in�ammatory diseases�however, this is not a universal property of all helminths anddifferent factors such as the helminth species, and whetherthe host is de�nitive or accidental, the parasite load and acuteversus chronic infectionsmay all in�uence the overall effect ofhelminth infections on in�ammatory diseases. Identi�cationof the helminth molecules that induce immunosuppression
and elucidation of the mechanisms involved is essentialfor the development of alternative strategies for preventionand�or treatment of in�ammatory diseases.
References
[1] J. E. Allen and R. M. Maizels, “Diversity and dialogue inimmunity to helminths,” Nature Reviews Immunology, vol. 11,no. 6, pp. 375–388, 2011.
[2] I. van Die and R. D. Cummings, “Glycan gimmickry byparasitic helminths: a strategy for modulating the host immuneresponse?” Glycobiology, vol. 20, no. 1, pp. 2–12, 2010.
[3] R.Maizels andM.Yazdanbakhsh, “T-cell regulation in helminthparasite infections: implications for in�ammatory diseases,”Chemical Immunology and Allergy, vol. 94, pp. 112–123, 2008.
[4] M. D. Taylor, N. van der Werf, and R. M. Maizels, “T cells inhelminth infection: the regulators and the regulated,” Trends inImmunology, vol. 33, no. 4, pp. 181–189, 2012.
[5] H. H. Smits, B. Everts, F. C. Hartgers, and M. Yazdanbakhsh,“Chronic helminth infections protect against allergic diseasesby active regulatory processes,” Current Allergy and AsthmaReports, vol. 10, no. 1, pp. 3–12, 2010.
[6] E. Pinelli and C. Aranzamendi, “Toxocara infection and itsassociation with allergic manifestations,” Endocrine MetabolicImmune & Disorders Drug Targets, vol. 12, no. 1, pp. 33–44,2012.
[7] H. Moll, “Dendritic cells and host resistance to infection,”Cellular Microbiology, vol. 5, no. 8, pp. 493–500, 2003.
[8] G. T. Belz and S. L. Nutt, “Transcriptional programming ofthe dendritic cell network,” Nature Reviews, vol. 12, no. 2, pp.101–113, 2012.

8 Journal of Parasitology Research
[9] O. Joffre, M. A. Nolte, R. Sp�rri, and C. R. E. Sousa, “In�am-matory signals in dendritic cell activation and the induction ofadaptive immunity,” Immunological Reviews, vol. 227, no. 1, pp.234–247, 2009.
[10] T. Kawai and S. Akira, “e role of pattern-recognition recep-tors in innate immunity: update on toll-like receptors,” NatureImmunology, vol. 11, no. 5, pp. 373–384, 2010.
[11] L. Carvalho, J. Sun, C. Kane, F. Marshall, C. Krawczyk, andE. J. Pearce, “Review series on helminths, immune modulationand the hygiene hypothesis: mechanisms underlying helminthmodulation of dendritic cell function,” Immunology, vol. 126,no. 1, pp. 28–34, 2009.
[12] D. Van der Kleij, E. Latz, J. F. H. M. Brouwers et al.,“A novel host-parasite lipid cross-talk. Schistosomal lyso-phosphatidylserine activates toll-like receptor 2 and affectsimmune polarization,” e Journal of Biological Chemistry, vol.277, no. 50, pp. 48122–48129, 2002.
[13] L. E. Layland, R. Rad, H. Wagner, and C. U. Prazeres da Costa,“Immunopathology in schistosomiasis is controlled by antigen-speci�c regulatory T cells primed in the presence of TLR2,”European Journal of Immunology, vol. 37, no. 8, pp. 2174–2184,2007.
[14] B. Everts, H. H. Smits, C. H. Hokke, and M. Yazdanbakhsh,“Helminths and dendritic cells: sensing and regulating via pat-tern recognition receptors, 2 and Treg responses,” EuropeanJournal of Immunology, vol. 40, no. 6, pp. 1525–1537, 2010.
[15] I. Schabussova, H. Amer, I. van Die, P. Kosma, and R. M.Maizels, “O-Methylated glycans from Toxocara are speci�ctargets for antibody binding in human and animal infections,”International Journal for Parasitology, vol. 37, no. 1, pp. 97–109,2007.
[16] U. Švajger, M. Anderluh, M. Jeras, and N. Obermajer, “C-typelectin DC-SIGN: an adhesion, signalling and antigen-uptakemolecule that guides dendritic cells in immunity,” CellularSignalling, vol. 22, no. 10, pp. 1397–1405, 2010.
[17] S. Meyer, E. Van Liempt, A. Imberty et al., “DC-SIGN medi-ates binding of dendritic cells to authentic pseudo-Lewis Yglycolipids of Schistosoma mansoni cercariae, the �rst parasite-speci�c ligand of DC-SIGN,” e Journal of Biological Chem-istry, vol. 280, no. 45, pp. 37349–37359, 2005.
[18] C. M. Kane, L. Cervi, J. Sun et al., “Helminth antigens modulateTLR-initiated dendritic cell activation,” Journal of Immunology,vol. 173, no. 12, pp. 7454–7461, 2004.
[19] H. S. Goodridge, W. Harnett, F. Y. Liew, and M. M. Harnett,“Differential regulation of interleukin-12 p40 and p35 induc-tion via Erk mitogen-activated protein kinase-dependent and-independent mechanisms and the implications for bioactiveIL-12 and IL-23 responses,” Immunology, vol. 109, no. 3, pp.415–425, 2003.
[20] S. R. Silva, J. F. Jacysyn, M. S. Macedo, and E. L. Faquin-Mauro,“Immunosuppressive components of Ascaris suum down-regulate expression of costimulatory molecules and functionof antigen-presenting cells via an IL-10-mediated mechanism,”European Journal of Immunology, vol. 36, no. 12, pp. 3227–3237,2006.
[21] C. M. Hamilton, D. J. Dowling, C. E. Loscher, R. M. Morphew,P. M. Brophy, and S. M. O’Neill, “e Fasciola hepaticategumental antigen suppresses dendritic cell maturation andfunction,” Infection and Immunity, vol. 77, no. 6, pp. 2488–2498,2009.
[22] C. Aranzamendi, F. Fransen, M. Langelaar et al., “Trichinellaspiralis-secreted products modulate DC functionality and
expand regulatory T cells in vitro,” Parasite Immunology, vol.34, no. 4, pp. 210–223, 2012.
[23] N. Ilic, M. Colic, A. Gruden-Movsesijan, I. Majstorovic, S.Vasilev, and L. Sofronic-Milosavljevic, “Characterization of ratbone marrow dendritic cells initially primed by Trichinellaspiralis antigens,” Parasite Immunology, vol. 30, no. 9, pp.491–495, 2008.
[24] Y. Belkaid and W. Chen, “Regulatory ripples,”Nature Immunol-ogy, vol. 11, no. 12, pp. 1077–1078, 2010.
[25] A. Doetze, J. Satoguina, G. Burchard et al., “Antigen-speci�ccellular hyporesponsiveness in a chronic human helminthinfection is mediated by T(h)3/T(r)1-type cytokines IL-10 andtransforming growth factor-𝛽𝛽 but not by a T(h)1 to T(h)2 shi,”International Immunology, vol. 12, no. 5, pp. 623–630, 2000.
[26] S. Babu, S. Q. Bhat, N. P. Kumar et al., “Filarial lymphedema ischaracterized by antigen-speci�c 1 and 17 proin�amma-tory responses and a lack of regulatory T cells,” PLoS NeglectedTropical Diseases, vol. 3, no. 4, article no. e420, 2009.
[27] J. D. Turner, J. A. Jackson, H. Faulkner et al., “Intensity ofintestinal infection with multiple worm species is related toregulatory cytokine output and immune hyporesponsiveness,”Journal of Infectious Diseases, vol. 197, no. 8, pp. 1204–1212,2008.
[28] C. A. Figueiredo, M. L. Barreto, L. C. Rodrigues et al., “Chronicintestinal helminth infections are associated with immunehyporesponsiveness and induction of a regulatory network,”Infection and Immunity, vol. 78, no. 7, pp. 3160–3167, 2010.
[29] K. Watanabe, P. N. M. Mwinzi, C. L. Black et al., “T regulatorycell levels decrease in people infected with Schistosomamansonion effective treatment,” American Journal of Tropical Medicineand Hygiene, vol. 77, no. 4, pp. 676–682, 2007.
[30] L. J. Wammes, F. Hamid, A. E. Wiria et al., “Regulatory T cellsin human geohelminth infection suppress immune responsesto BCG and Plasmodium falciparum,” European Journal ofImmunology, vol. 40, no. 2, pp. 437–442, 2010.
[31] N. Gomez-Escobar, W. F. Gregory, and R. M. Maizels, “Iden-ti�cation of tgh-2, a �larial nematode homolog of Caenorhab-ditis elegans daf-7 and human transforming growth factor 𝛽𝛽,expressed in micro�larial and adult stages of Brugia malayi,”Infection and Immunity, vol. 68, no. 11, pp. 6402–6410, 2000.
[32] S. Babu, C. P. Blauvelt, V. Kumaraswami, and T. B. Nutman,“Regulatory networks induced by live parasites impair both1and2pathways in patent lymphatic �lariasis: implications forparasite persistence,” Journal of Immunology, vol. 176, no. 5, pp.3248–3256, 2006.
[33] R. D’Elia, J. M. Behnke, J. E. Bradley, and K. J. Else, “RegulatoryT cells: a role in the control of helminth-driven intestinalpathology and worm survival,” Journal of Immunology, vol. 182,no. 4, pp. 2340–2348, 2009.
[34] M. D. Taylor, L. LeGoff, A. Harris, E. Malone, J. E. Allen, andR. M. Maizels, “Removal of regulatory T cell activity reverseshyporesponsiveness and leads to �larial parasite clearance invivo,” Journal of Immunology, vol. 174, no. 8, pp. 4924–4933,2005.
[35] V. Gillan and E. Devaney, “Regulatory T cells modulate 2responses induced by Brugia pahangi third-stage larvae,” Infec-tion and Immunity, vol. 73, no. 7, pp. 4034–4042, 2005.
[36] M. D. Taylor, N. van der Werf, A. Harris et al., “Early recruit-ment of natural CD4+Foxp3+ Treg cells by infective larvaedetermines the outcome of �larial infection,” European Journalof Immunology, vol. 39, no. 1, pp. 192–206, 2009.

Journal of Parasitology Research 9
[37] C. A. M. Finney, M. D. Taylor, M. S. Wilson, and R. M. Maizels,“Expansion and activation of CD4+CD25+ regulatory T cellsin Heligmosomoides polygyrus infection,” European Journal ofImmunology, vol. 37, no. 7, pp. 1874–1886, 2007.
[38] S. Rausch, J. Huehn, D. Kirchhoff et al., “Functional analysisof effector and regulatory T cells in a parasitic nematodeinfection,” Infection and Immunity, vol. 76, no. 5, pp. 1908–1919,2008.
[39] S. Gordon, “Alternative activation of macrophages,” NatureReviews, vol. 3, no. 1, pp. 23–35, 2003.
[40] L. Prieto-Lafuente, W. F. Gregory, J. E. Allen, and R. M. Maizels,“MIF homologues from a �larial nematode parasite synergizewith IL-4 to induce alternative activation of host macrophages,”Journal of Leukocyte Biology, vol. 85, no. 5, pp. 844–854, 2009.
[41] R.M.Maizels, E. J. Pearce, D. Artis, M. Yazdanbakhsh, and T. A.Wynn, “Regulation of pathogenesis and immunity in helminthinfections,” Journal of Experimental Medicine, vol. 206, no. 10,pp. 2059–2066, 2009.
[42] S. Fillatreau, D. Gray, and S. M. Anderton, “Not always the badguys: B cells as regulators of autoimmune pathology,” NatureReviews Immunology, vol. 8, no. 5, pp. 391–397, 2008.
[43] N. E. Mangan, R. E. Fallon, P. Smith, N. Van Rooijen, A.N. McKenzie, and P. G. Fallon, “Helminth infection protectsmice from anaphylaxis via IL-10-producing B cells,” Journal ofImmunology, vol. 173, no. 10, pp. 6346–6356, 2004.
[44] M. S. Wilson, M. D. Taylor, M. T. O’Gorman et al., “Helminth-induced CD19+CD23hi B cells modulate experimental allergicand autoimmune in�ammation,” European Journal of Immunol-ogy, vol. 40, no. 6, pp. 1682–1696, 2010.
[45] Y. Osada and T. Kanazawa, “Parasitic helminths: new weaponsagainst immunological disorders,” Journal of Biomedicine &Biotechnology, vol. 2010, Article ID 743758, 9 pages, 2010.
[46] C. Flohr, R. J. Quinnell, and J. Britton, “Do helminth parasitesprotect against atopy and allergic disease?” Clinical and Exper-imental Allergy, vol. 39, no. 1, pp. 20–32, 2009.
[47] W.Harnett andM.M.Harnett, “Parasitic nematodemodulationof allergic disease,” Current Allergy and Asthma Reports, vol. 8,no. 5, pp. 392–397, 2008.
[48] F. G. Selassie, R. H. Stevens, P. Cullinan et al., “Total and speci�cIgE (house dust mite and intestinal helminths) in asthmaticsand controls from Gondar, Ethiopia,” Clinical and ExperimentalAllergy, vol. 30, no. 3, pp. 356–358, 2000.
[49] A. M. J. Van Den Biggelaar, L. C. Rodrigues, R. Van Reeet al., “Long-term treatment of intestinal helminths increasesmite skin-test reactivity in Gabonese schoolchildren,” Journalof Infectious Diseases, vol. 189, no. 5, pp. 892–900, 2004.
[50] L. G. G. Pac��co, F. A. V. Marinho, C. T. Fonseca et al.,“Schistosoma mansoni antigens modulate experimental allergicasthma in a murine model: a major role for CD4+ CD25+Foxp3 + T cells independent of interleukin-10,” Infection andImmunity, vol. 77, no. 1, pp. 98–107, 2009.
[51] A.M.Dittrich, A. Erbacher, S. Specht et al., “Helminth infectionwith Litomosoides sigmodontis induces regulatory T cells andinhibits allergic sensitization, airway in�ammation, and hyper-reactivity in a murine asthma model,” Journal of Immunology,vol. 180, no. 3, pp. 1792–1799, 2008.
[52] M. S. Wilson, M. D. Taylor, A. Balic, C. A. M. Finney, J.R. Lamb, and R. M. Maizels, “Suppression of allergic airwayin�ammation by helminth-induced regulatory T cells,” Journalof Experimental Medicine, vol. 202, no. 9, pp. 1199–1212, 2005.
[53] M. E. H. Bashir, P. Andersen, I. J. Fuss, H. N. Shi, and C. Nagler-Anderson, “An enteric helminth infection protects against anallergic response to dietary antigen,” Journal of Immunology, vol.169, no. 6, pp. 3284–3292, 2002.
[54] H. Okada, C. Kuhn, H. Feillet, and J. F. Bach, “e ’hygienehypothesis’ for autoimmune and allergic diseases: an update,”Clinical and Experimental Immunology, vol. 160, no. 1, pp. 1–9,2010.
[55] J. V. Weinstock and D. E. Elliott, “Helminths and the IBDhygiene hypothesis,” In�ammatory Bowel Diseases, vol. 15, no.1, pp. 128–133, 2009.
[56] A. Cooke, P. Tonks, F. M. Jones et al., “Infection with Schisto-soma mansoni prevents insulin dependent diabetes mellitus innon-obese diabetic mice,” Parasite Immunology, vol. 21, no. 4,pp. 169–176, 1999.
[57] A. C. La Flamme, K. Ruddenklau, and B. T. Bäckström,“Schistosomiasis decreases central nervous system in�amma-tion and alters the progression of experimental autoimmuneencephalomyelitis,” Infection and Immunity, vol. 71, no. 9, pp.4996–5004, 2003.
[58] D. E. Elliott, T. Setiawan, A.Metwali, A. Blum, J. F. Urban, and J.V. Weinstock, “Heligmosomoides polygyrus inhibits establishedcolitis in IL-10-de�cient mice,” European Journal of Immunol-ogy, vol. 34, no. 10, pp. 2690–2698, 2004.
[59] M. P. Hübner, J. omas Stocker, and E. Mitre, “Inhibition oftype 1 diabetes in �laria-infected non-obese diabetic mice isassociated with a T helper type 2 shi and induction of FoxP3+regulatory T cells,” Immunology, vol. 127, no. 4, pp. 512–522,2009.
[60] P. G. omas, M. R. Carter, O. Atochina et al., “Maturation ofdendritic cell 2 phenotype by a helminth glycan uses a toll-likereceptor 4-dependent mechanism,” Journal of Immunology, vol.171, no. 11, pp. 5837–5841, 2003.
[61] D. Van der Kleij, E. Latz, J. F. H. M. Brouwers et al.,“A novel host-parasite lipid cross-talk. Schistosomal lyso-phosphatidylserine activates toll-like receptor 2 and affectsimmune polarization,” e Journal of Biological Chemistry, vol.277, no. 50, pp. 48122–48129, 2002.
[62] H. S. Goodridge, E. H. Wilson, W. Harnett, C. C. Campbell,M. M. Harnett, and F. Y. Liew, “Modulation of macrophagecytokine production by ES-62, a secreted product of the �larialnematode Acanthocheilonema viteae,” Journal of Immunology,vol. 167, no. 2, pp. 940–945, 2001.
[63] M. Whelan, M. M. Harnett, K. M. Houston, V. Patel, W.Harnett, and K. P. Rigley, “A �larial nematode-secreted productsignals dendritic cells to acquire a phenotype that drivesdevelopment of 2 cells,” Journal of Immunology, vol. 164, no.12, pp. 6453–6460, 2000.
[64] H. S. Goodridge, F. A. Marshall, K. J. Else et al., “Immunomod-ulation via novel use of TLR4 by the �larial nematodephosphorylcholine-containing secreted product, ES-62,” Jour-nal of Immunology, vol. 174, no. 1, pp. 284–293, 2005.
[65] M. J. Holland, Y. M. Harcus, P. L. Riches et al., “Proteinssecreted by the parasitic nematode Nippostrongylus brasilien-sis act as adjuvants for 2 responses,” European Journal ofImmunology, vol. 30, no. 7, pp. 1977–1987, 2000.
[66] W. F. Gregory and R. M. Maizels, “Cystatins from �larialparasites: evolution, adaptation and function in the host-parasite relationship,” International Journal of Biochemistry andCell Biology, vol. 40, no. 6-7, pp. 1389–1398, 2008.
[67] B. Manoury, W. F. Gregory, R. M. Maizels, and C. Watts, “Bm-CPI-2, a cystatin homolog secreted by the �larial parasiteBrugia

10 Journal of Parasitology Research
malayi, inhibits class II MHC-restricted antigen processing,”Current Biology, vol. 11, no. 6, pp. 447–451, 2001.
[68] F. H. Falcone, P. Loke, X. Zang, A. S. MacDonald, R. M.Maizels, and J. E. Allen, “A Brugia malayi homolog ofmacrophage migration inhibitory factor reveals an importantlink between macrophages and eosinophil recruitment duringnematode infection,” Journal of Immunology, vol. 167, no. 9, pp.5348–5354, 2001.
[69] X. Zang and R. M. Maizels, “Serine proteinase inhibitors fromnematodes and the arms race between host and pathogen,”Trends in Biochemical Sciences, vol. 26, no. 3, pp. 191–197, 2001.
[70] W. F. Gregory, A. K. Atmadja, J. E. Allen, and R. M. Maizels,“e abundant larval transcript-1 and -2 genes of Brugiamalayiencode stage-speci�c candidate vaccine antigens for �lariasis,”Infection and Immunity, vol. 68, no. 7, pp. 4174–4179, 2000.
[71] A. Loukas, A. Doedens, M. Hintz, and R. M. Maizels, “Identi�-cation of a new C-type lectin, TES-70, secreted by infective lar-vae ofToxocara canis, which binds to host ligands,” Parasitology,vol. 121, part 5, pp. 545–554, 2000.
[72] A. Loukas and R. M. Maizels, “Helminth C-type lectins andhost-parasite interactions,” Parasitology Today, vol. 16, no. 8, pp.333–339, 2000.
[73] J. R. Grainger, K. A. Smith, J. P. Hewitson et al., “Helminthsecretions induce de novo T cell Foxp3 expression and reg-ulatory function through the TGF-𝛽𝛽 pathway,” Journal ofExperimental Medicine, vol. 207, no. 11, pp. 2331–2341, 2010.
[74] N. Ilic, J. J. Worthington, A. Gruden-Movsesijan et al.,“Trichinella spiralis antigens primemixed1/2 response butdo not induce de novo generation of Foxp3+ T cells in vitro,”Parasite Immunology, vol. 33, no. 10, pp. 572–582, 2011.
[75] A. Gruden-Movsesijan, N. Ilic, M. Colic et al., “e impact ofTrichinella spiralis excretory-secretory products on dendriticcells,” Comparative Immunology, Microbiology and InfectiousDiseases, vol. 34, no. 5, pp. 429–439, 2011.
[76] S. Donnelly, S. M. O’Neill, M. Sekiya, G. Mulcahy, and J. P.Dalton, “ioredoxin peroxidase secreted by Fasciola hepaticainduces the alternative activation of macrophages,” Infectionand Immunity, vol. 73, no. 1, pp. 166–173, 2005.
[77] L. M. Kuijk, E. J. Klaver, G. Kooij et al., “Soluble helminth prod-ucts suppress clinical signs in murine experimental autoim-mune encephalomyelitis and differentially modulate humandendritic cell activation,” Molecular Immunology, vol. 51, no. 2,pp. 210–218, 2012.
[78] Y. Motomura, H. Wang, Y. Deng, R. T. El-Sharkawy, E. F. Verdu,andW. I. Khan, “Helminth antigen-based strategy to amelioratein�ammation in an experimental model of colitis,” Clinical andExperimental Immunology, vol. 155, no. 1, pp. 88–95, 2009.
[79] G. G. Cancado, J. A. Fiuza, N. C. de Paiva et al., “Hookwormproducts ameliorate dextran sodium sulfate-induced colitis inBALB/c mice,” In�ammatory Bo�el Diseases, vol. 17, no. 11, pp.2275–2286, 2011.
[80] M. J. G. Johnston, A.Wang, M. E. D. Catarino et al., “Extracts ofthe rat tapeworm,Hymenolepis diminuta, suppress macrophageactivation in vitro and alleviate chemically induced colitis inmice,” Infection and Immunity, vol. 78, no. 3, pp. 1364–1375,2010.
[81] N. E. Ruyssers, B. Y. DeWinter, J. G. DeMan et al., “erapeuticpotential of helminth soluble proteins in TNBS induced colitisin mice,” In�ammatory Bo�el Diseases, vol. 15, no. 4, pp.491–500, 2009.
[82] I. B. McInnes, B. P. Leung, M. Harnett, J. A. Gracie, F. Y.Liew, and W. Harnett, “A novel therapeutic approach targeting
articular in�ammation using the �larial nematode-derivedphosphorylcholine-containing glycoprotein ES-62,” Journal ofImmunology, vol. 171, no. 4, pp. 2127–2133, 2003.
[83] P. Zaccone, Z. Feheérvári, F. M. Jones et al., “Schistosomamansoni antigens modulate the activity of the innate immuneresponse and prevent onset of type 1 diabetes,”European Journalof Immunology, vol. 33, no. 5, pp. 1439–1449, 2003.
[84] L. S. Cardoso, S. C. Oliveira, A. M. Góes et al., “Schistosomamansoni antigens modulate the allergic response in a murinemodel of ovalbumin-induced airway in�ammation,” Clinicaland Experimental Immunology, vol. 160, no. 2, pp. 266–274,2010.
[85] J. Yang, J. Zhao, Y. Yang et al., “Schistosoma japonicum eggantigens stimulate CD4+ CD25 + T cells and modulate airwayin�ammation in a murine model of asthma,” Immunology, vol.120, no. 1, pp. 8–18, 2006.
[86] C. M. Trujillo-Vargas, M. Werner-Klein, G. Wohlleben et al.,“Helminth-derived products inhibit the development of allergicresponses in mice,”American Journal of Respiratory and CriticalCare Medicine, vol. 175, no. 4, pp. 336–344, 2007.
[87] C. Lima, A. Perini, M. L. B. Garcia, M. A. Martins, M. M. Teix-eira, andM. S. Macedo, “Eosinophilic in�ammation and airwayhyper-responsiveness are profoundly inhibited by a helminth(Ascaris suum) extract in a murine model of asthma,” Clinicaland Experimental Allergy, vol. 32, no. 11, pp. 1659–1666, 2002.
[88] W. I. Khan, P. A. Blennerhasset, A. K. Varghese et al., “Intestinalnematode infection ameliorates experimental colitis in mice,”Infection and Immunity, vol. 70, no. 11, pp. 5931–5937, 2002.
[89] K. A. Saunders, T. Raine, A. Cooke, and C. E. Lawrence,“Inhibition of autoimmune type 1 diabetes by gastrointestinalhelminth infection,” Infection and Immunity, vol. 75, no. 1, pp.397–407, 2007.
[90] A. Gruden-Movsesijan, N. Ilic, M. Mostarica-Stojkovic, S.Stosic-Grujicic, M. Milic, and L. Sofronic-Milosavljevic,“Trichinella spiralis: modulation of experimental autoimmuneencephalomyelitis in DA rats,” Experimental Parasitology, vol.118, no. 4, pp. 641–647, 2008.
[91] A. Gruden-Movsesijan, N. Ilic, M. Mostarica-Stojkovic, S.Stosic-Grujicic, M. Milic, and L. Sofronic-Milosavljevic,“Mechanisms of modulation of experimental autoimmuneencephalomyelitis by chronic Trichinella spiralis infection inDark Agouti rats,” Parasite Immunology, vol. 32, no. 6, pp.450–459, 2010.
[92] H. K. Park, M. K. Cho, S. H. Choi, Y. S. Kim, and H.S. Yu, “Trichinella spiralis: infection reduces airway allergicin�ammation in mice,” Experimental Parasitology, vol. 127, no.2, pp. 539–544, 2011.
[93] L. H. Boles, J. M. Montgomery, J. Morris, M. A. Mann, andG. L. Stewart, “Suppression of multiple sclerosis in the ratduring infection with Trichinella pseudospiralis,” Journal ofParasitology, vol. 86, no. 4, pp. 841–844, 2000.
[94] Z. Wu, I. Nagano, K. Asano, and Y. Takahashi, “Infectionof non-encapsulated species of Trichinella ameliorates experi-mental autoimmune encephalomyelitis involving suppressionof 17 and 1 response,” Parasitology Research, vol. 107, no.5, pp. 1173–1188, 2010.
[95] K. J. Erb, “Can helminths or helminth-derived products beused in humans to prevent or treat allergic diseases?” Trends inImmunology, vol. 30, no. 2, pp. 75–82, 2009.
[96] E. Pinelli, S. Brandes, J. Dormans, E. Gremmer, and H. VanLoveren, “Infection with the roundworm Toxocara canis leads

Journal of Parasitology Research 11
to exacerbation of experimental allergic airway in�ammation,”Clinical and Experimental Allergy, vol. 38, no. 4, pp. 649–658,2008.
[97] A. J. Coyle, G. Kohler, S. Tsuyuki et al., “Eosinophils are notrequired to induce airway hyperresponsiveness aer nematodeinfection,” European Journal of Immunology, vol. 28, no. 9, pp.2640–2647, 1998.
[98] L. R. Hall, R. K. Mehlotra, A. W. Higgins, M. A. Haxhiu,and E. Pearlman, “An essential role for interleukin-5 andeosinophils in helminth-induced airway hyperresponsiveness,”Infection and Immunity, vol. 66, no. 9, pp. 4425–4430, 1998.
[99] R. T. Strait, S. C. Morris, K. Smiley, J. F. Urban, and F. D. Finkel-man, “IL-4 exacerbates anaphylaxis,” Journal of Immunology,vol. 170, no. 7, pp. 3835–3842, 2003.
[100] A. S. Gounni, K. Spanel-Borowski, M. Palacios, C. Heusser,S. Moncada, and E. Lobos, “Pulmonary in�ammation inducedby a recombinant Brugia malayi 𝛾𝛾-glutamyl transpeptidasehomolog: involvement of humoral autoimmune responses,”Molecular Medicine, vol. 7, no. 5, pp. 344–354, 2001.
[101] P. A. M. Overgaauw, “Aspects of Toxocara epidemiology:toxocarosis in dogs and cats,” Critical Reviews in Microbiology,vol. 23, no. 3, pp. 233–251, 1997.
[102] N. Ilic, A. Gruden-Movsesijan, and L. Sofronic-Milosavljevic,“Trichinella spiralis: shaping the immune response,” Immuno-logic Research, vol. 52, no. 1-2, pp. 111–119, 2012.
[103] F. Bruschi and L. Chiumiento, “Immunomodulation intrichinellosis: does Trichinella really escape the host immunesystem?” Endocrine Metabolic Immune & Disorders DrugTargets, vol. 12, no. 1, pp. 4–15, 2012.
[104] D. Wakelin, P. K. Goyal, M. S. Dehlawi, and J. Hermanek,“Immune responses to Trichinella spiralis and T. pseudospiralisin mice,” Immunology, vol. 81, no. 3, pp. 475–479, 1994.
[105] C. Aranzamendi, A. de Bruin, R. Kuiper et al., “Protectionagainst allergic airway in�ammation during the chronic andacute phases of Trichinella spiralis infection,” Clinical andExperimental Allergy, vol. 43, no. 1, pp. 103–115, 2013.
[106] J. Buijs, W. H. Lokhorst, J. Robinson, and F. P. Nijkamp, “Tox-ocara canis-induced murine pulmonary in�ammation: analysisof cells and proteins in lung tissue and bronchoalveolar lavage�uid,” Parasite Immunology, vol. 16, no. 1, pp. 1–9, 1994.
[107] E. Pinelli, C. Withagen, M. Fonville et al., “Persistent airwayhyper-responsiveness and in�ammation in Toxocara canis-infected BALB/c mice,” Clinical and Experimental Allergy, vol.35, no. 6, pp. 826–832, 2005.
[108] E. Pinelli, S. Brandes, J. Dormans, M. Fonville, C. M. Hamilton,and J. V. der Giessen, “Toxocara canis: effect of inoculum sizeon pulmonary pathology and cytokine expression in BALB/cmice,” Experimental Parasitology, vol. 115, no. 1, pp. 76–82,2007.
[109] F. Bruschi, S. Solfanelli, and R. A. Binaghi, “Trichinella spiralis:modi�cations of the cuticle of the newborn larva during passagethrough the lung,” Experimental Parasitology, vol. 75, no. 1, pp.1–9, 1992.
[110] P. J. Cooper, “Interactions between helminth parasites andallergy,” Current Opinion in Allergy and Clinical Immunology,vol. 9, no. 1, pp. 29–37, 2009.

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2012, Article ID 154743, 17 pagesdoi:10.1155/2012/154743
Review Article
Human Schistosome Infection and Allergic Sensitisation
Nadine Rujeni, David W. Taylor, and Francisca Mutapi
Institute of Immunology and Infection Research, Centre for Immunity, Infection, and Evolution, School of Biological Sciences,University of Edinburgh, Ashworth Laboratories, King’s Buildings, West Mains Rd, Edinburgh EH9 3JT, UK
Correspondence should be addressed to Francisca Mutapi, [email protected]
Received 14 May 2012; Accepted 28 June 2012
Academic Editor: Maria Ilma Araujo
Copyright © 2012 Nadine Rujeni et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Several field studies have reported an inverse relationship between the prevalence of helminth infections and that of allergicsensitisation/atopy. Recent studies show that immune responses induced by helminth parasites are, to an extent, comparableto allergic sensitisation. However, helminth products induce regulatory responses capable of inhibiting not only antiparasiteimmune responses, but also allergic sensitisation. The relative effects of this immunomodulation on the development of protectiveschistosome-specific responses in humans has yet to be demonstrated at population level, and the clinical significance ofimmunomodulation of allergic disease is still controversial. Nonetheless, similarities in immune responses against helminthsand allergens pose interesting mechanistic and evolutionary questions. This paper examines the epidemiology, biology andimmunology of allergic sensitisation/atopy, and schistosome infection in human populations.
1. Introduction
The major human helminth parasites belong to two phyla,the nematodes (or roundworms) which include intestinalsoil transmitted helminths (STH) and filarial worms (whichcause lymphatic filariasis and onchocerciasis), and theplatyhelminths (or flatworms) which include the flukes (ortrematodes, including schistosomes) and the tapeworms (orcestodes). Although common in most parts of the world sixtyyears ago [1], these parasites are currently mainly prevalentin sub-Saharan Africa, Asia, and South America [2–4], wherethey are responsible for considerable disabilities includingblindness and elephantiasis (filarial worms). Furthermore,helminth infections are responsible for morbidities thatinclude anaemia, stunted growth, poor cognitive develop-ment, and malnutrition [5–7], hence exert a negative socioe-conomic impact in some of the poorest communities in theworld.
Immune-mediated diseases including auto-immune dis-eases (such as type 1 diabetes, inflammatory bowel diseases,and rheumatoid arthritis) and allergic diseases (such asasthma, allergic rhinitis, and atopic eczema) are reportedto be more prevalent in developed countries and in urbanareas of developing countries [8, 9]. But studies from Africa
are demonstrating that allergic diseases are common, if notacknowledged, clinical problems in this region [10]. Immunedisorders have been responsible for increased mortality andmorbidity worldwide [11–13] and they negatively impacton economic growth due to their elevated cost of theirtreatment [14, 15]. There is also mounting evidence thatallergic disorders, especially allergic rhinitis, are associatedwith attention deficit disorder and hyperactivity in children[16, 17].
Increasing rates of childhood allergies have long been apuzzle to epidemiologists [18, 19]. Thus, studying cohortsof children born in 1946, 1958, and 1970, concluded thata “new environmental agent,” contained in breast milk andpossibly infants’ food was responsible for the increase ineczema. Emmanuel, reviewing medical literature publishedfrom 1820 to 1900, suggested that the hay fever “epidemic”was associated with the rapid industrial growth of the 19thcentury since this disorder was rarely described prior thatperiod [19]. It was Strachan who in 1989, observing thatthe rate of hay fever and eczema was consistently negativelyassociated with family size and birth position in house-holds, hypothesized that reduced exposure to childhoodinfections due to increased hygiene was responsible for theallergy epidemics. This hypothesis, currently referred to as
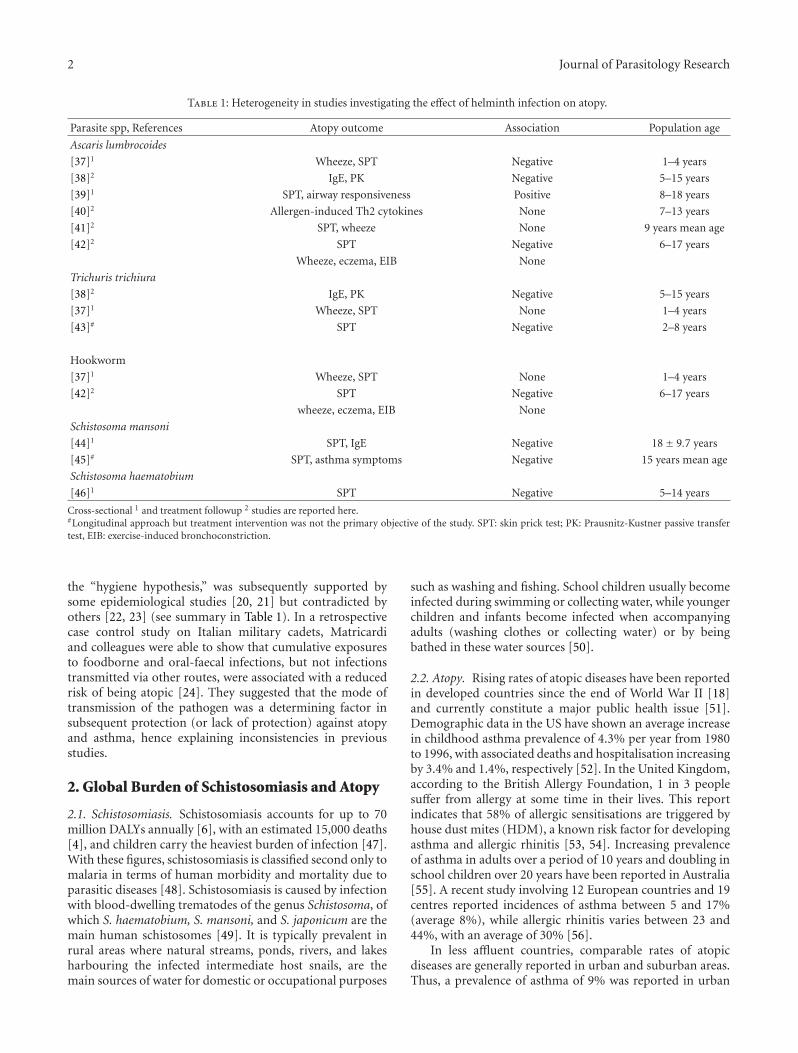
2 Journal of Parasitology Research
Table 1: Heterogeneity in studies investigating the effect of helminth infection on atopy.
Parasite spp, References Atopy outcome Association Population age
Ascaris lumbrocoides
[37]1 Wheeze, SPT Negative 1–4 years
[38]2 IgE, PK Negative 5–15 years
[39]1 SPT, airway responsiveness Positive 8–18 years
[40]2 Allergen-induced Th2 cytokines None 7–13 years
[41]2 SPT, wheeze None 9 years mean age
[42]2 SPT Negative 6–17 years
Wheeze, eczema, EIB None
Trichuris trichiura
[38]2 IgE, PK Negative 5–15 years
[37]1 Wheeze, SPT None 1–4 years
[43]# SPT Negative 2–8 years
Hookworm
[37]1 Wheeze, SPT None 1–4 years
[42]2 SPT Negative 6–17 years
wheeze, eczema, EIB None
Schistosoma mansoni
[44]1 SPT, IgE Negative 18± 9.7 years
[45]# SPT, asthma symptoms Negative 15 years mean age
Schistosoma haematobium
[46]1 SPT Negative 5–14 years
Cross-sectional 1 and treatment followup 2 studies are reported here.#Longitudinal approach but treatment intervention was not the primary objective of the study. SPT: skin prick test; PK: Prausnitz-Kustner passive transfertest, EIB: exercise-induced bronchoconstriction.
the “hygiene hypothesis,” was subsequently supported bysome epidemiological studies [20, 21] but contradicted byothers [22, 23] (see summary in Table 1). In a retrospectivecase control study on Italian military cadets, Matricardiand colleagues were able to show that cumulative exposuresto foodborne and oral-faecal infections, but not infectionstransmitted via other routes, were associated with a reducedrisk of being atopic [24]. They suggested that the mode oftransmission of the pathogen was a determining factor insubsequent protection (or lack of protection) against atopyand asthma, hence explaining inconsistencies in previousstudies.
2. Global Burden of Schistosomiasis and Atopy
2.1. Schistosomiasis. Schistosomiasis accounts for up to 70million DALYs annually [6], with an estimated 15,000 deaths[4], and children carry the heaviest burden of infection [47].With these figures, schistosomiasis is classified second only tomalaria in terms of human morbidity and mortality due toparasitic diseases [48]. Schistosomiasis is caused by infectionwith blood-dwelling trematodes of the genus Schistosoma, ofwhich S. haematobium, S. mansoni, and S. japonicum are themain human schistosomes [49]. It is typically prevalent inrural areas where natural streams, ponds, rivers, and lakesharbouring the infected intermediate host snails, are themain sources of water for domestic or occupational purposes
such as washing and fishing. School children usually becomeinfected during swimming or collecting water, while youngerchildren and infants become infected when accompanyingadults (washing clothes or collecting water) or by beingbathed in these water sources [50].
2.2. Atopy. Rising rates of atopic diseases have been reportedin developed countries since the end of World War II [18]and currently constitute a major public health issue [51].Demographic data in the US have shown an average increasein childhood asthma prevalence of 4.3% per year from 1980to 1996, with associated deaths and hospitalisation increasingby 3.4% and 1.4%, respectively [52]. In the United Kingdom,according to the British Allergy Foundation, 1 in 3 peoplesuffer from allergy at some time in their lives. This reportindicates that 58% of allergic sensitisations are triggered byhouse dust mites (HDM), a known risk factor for developingasthma and allergic rhinitis [53, 54]. Increasing prevalenceof asthma in adults over a period of 10 years and doubling inschool children over 20 years have been reported in Australia[55]. A recent study involving 12 European countries and 19centres reported incidences of asthma between 5 and 17%(average 8%), while allergic rhinitis varies between 23 and44%, with an average of 30% [56].
In less affluent countries, comparable rates of atopicdiseases are generally reported in urban and suburban areas.Thus, a prevalence of asthma of 9% was reported in urban

Journal of Parasitology Research 3
areas of Rwanda [57] while the International Study ofAsthma and Allergies in childhood (ISAAC) reported anoverall prevalence of 10.9% across 22 centres in Africa [58].Reported incidences of allergic rhinitis range from 14% to54% in urban and suburban areas across African countries(reviewed by [59]). Importantly, according to the ISAACphase three, although the prevalence was generally lower,there were more severe symptoms of rhinoconjnnctivitisreported in urban centres of developing countries comparedto those reported in developed countries [8]. However,studies from Africa suggest that allergic conditions may beunderdiagnosed in Africa due to “inappropriate” diagnostictests and these studies call for component-resolved allergytesting in Africa [60]. Indeed a recent study in Zimbabweshowed that schistosome-infection resulted in impaireddiagnosis of cat allergy [61].
3. Atopy and Schistosome Life-Cycle Stages
In schistosome infection, the human immune system isexposed to schistosome larvae (cercariae and schistosomula),adult worm, and egg antigens. Animal studies as well asin vitro studies have demonstrated immunological changesand regulatory mechanisms associated with these differentlife-cycle stages. The surface of cercariae (enriched in car-bohydrates [62]) and the newly transformed schistosomulaactivate the complement cascade [63, 64] and eliciting proin-flammatory responses [65, 66]. An excessive immunologicalreaction to skin stage cercarial antigens results in cercarialdermatitis or swimmer’s itch [67], an allergic conditionalso occurring in contact with nonhuman schistosomesthat is prevalent in developed countries [68–70]. Thisinflammatory reaction is rarely reported in populations inwhich schistosomiasis is endemic, possibly due to regulatoryresponses resulting from multiple exposures as has beendemonstrated in mice [71]. Such regulatory responses maybe induced by skin-stage schistosomula-derived moleculessuch as prostaglandin E2(PGE2) which upregulates IL-10production during skin penetration by the parasite [72].The PGE2 is also secreted by the lung-stage schistosomuladuring migration through the capillary beds of the lungs,and this is thought to diminish eosinophil infiltrates aroundthe parasites (and thus inflammation [73]). In addition,these parasites are capable of inhibiting the expressionof endothelial adhesion molecules such as E-selectin andVCAM-1, limiting leucocyte recruitment in the lungs [74].These anti-inflammatory mechanisms in the lungs havebeen suggested as potential explanations for reduced severityof asthma symptoms in schistosome-infected asthmaticpatients [45], although there are no mechanistic studies fromhuman populations to support this.
Schistosome eggs are major Th2 triggers as demonstratedin murine studies [75, 76], and they induce formation offibrotic lesions or granulomas [77–79]. Indeed, an S. mansoniegg-secreted glycoprotein, omega-1, has recently been identi-fied that conditions dendritic cells for Th2 polarisation [25].However, egg secretions are capable of inhibiting the specificbinding of chemokines such as CXCL8 (IL-8) and CCL3(MIP-1α), therefore blocking chemokine-elicited migration
of neutrophils and macrophages respectively during granu-loma formation [80].
Schistosome adult worm antigens also induce Th2responses and IgE in mice [81], baboons [82], and humans[83]. However, this parasite life stage elicits high levelsof modulatory responses capable of inhibiting antiparasite[84] as well as allergic reactions [85]. The latter studydemonstrated that worm infection induces IL-10, producingB cells that could protect mice against anaphylaxis. Theylater demonstrated that egg-laying worms exacerbate whilesingle sex worms (precluding egg production) inhibit airwayhyperresponsiveness [86].
Together, these studies show that the different parasitelife-cycle stages are associated with different mechanisms ofregulation and inflammation. Although concurrent exposureto all or most antigens is likely in endemic areas, anddespite the fact that they may induce cross-reactive immuneresponses [87], the different parasite life-cycle stages maydifferentially affect atopic responses.
4. Epidemiology
4.1. Schistosomiasis. The epidemiological patterns of schisto-somiasis differ from those of atopy, mainly because of theiraetiology. Indeed, while schistosome infection is acquired asa result of exposure to parasites, atopy is a genetic predis-position (although the clinical manifestations are influencedby environmental factors). In schistosome endemic areas,infection levels follow a convex shape with host age, whereinfection intensity rises to peak in childhood-adolescenceand decline in adulthood [88]. This peak was initially inter-preted as arising from different water contact levels betweenage groups [89]. However, longitudinal studies showed thatwith the same exposure rate, “resistant” individuals wereolder than “susceptible” individuals [90–92], suggestingan age-dependent acquired resistance to reinfection. Inaddition, in communities of different parasite transmission,infection intensity peaks at a younger age in areas of hightransmission compared to low-transmission areas [88, 93–95], a phenomenon referred to as a “peak shift.” This phe-nomenon has been interpreted as reflecting different ratesof development of acquired resistance to infection duringschistosome infection as has been reported for Plasmodiuminfections (which cause malaria) [96, 97]. This interpretationis supported by age-related changes in immune responses,with the peak of antibodies and cytokine associated withprotection coinciding with the decline in infection levels havebeen reported in S. haematobium endemic areas [83, 98, 99].More recently, Black and colleagues observed that the rate ofacquisition of antischistosome protective responses by adultsoccupationally exposed to S. mansoni, following treatment,is dependent on their history of exposure, being faster inthose with a longer history [100]. This study, consistent withearlier studies [101, 102], demonstrated that resistance toschistosome infection/reinfection is acquired independent ofage related physiological changes [103].
4.2. Atopic Diseases. Atopy is the genetic predisposition tobecome excessively sensitised and produce high levels of

4 Journal of Parasitology Research
IgE [104]. However, atopic diseases result from a geneticpredisposition in combination with environmental stimulisuch as allergens, smoke, diet, and/or infectious agents[105, 106]. The epidemiology of atopic diseases is complexas some diseases may become more prominent with agewhile others diminish or disappear [107]. The earliest phasesof atopic diseases usually manifest during the first fiveyears of life and the severity (and prevalence) of clinicalsymptoms seem to increase in late childhood/adolescenceand plateau throughout adulthood [108–110] or decline forsome conditions [111, 112].
It has been suggested that a natural history of allergymanifestations in atopic individuals involves progressionfrom atopic eczema (below one year of age) to asthma orallergic rhinitis (late childhood/adolescence), a phenomenonreferred to as the “atopic/allergic march” [112]. However,this is not always consistent as some children may developatopic dermatitis long after the onset of asthma [113], whilesome atopic individuals may only develop one of theseconditions throughout life. Longitudinal studies indicatethat atopy in infancy predicts the occurrence and severityof asthma [114] and bronchial hyperresponsiveness [115] inlater life. Total and allergen-specific IgE levels also seem toincrease throughout childhood in allergic individuals [116].However, a number of events occurring in the first fewyears of life and in utero are likely to influence the onsetand persistence of disease. Thus, Klinnert and colleagueshave shown that respiratory infections during the first yearof life and parenting difficulties (e.g., postnatal maternaldepression) were independent predictors of the onset ofasthma during early (3 years) and late (6–8 years) childhoodin children at risk [114, 117].
Microbial exposures and diet of pregnant mothers mayalso alter early gene expression in neonates, influencing theonset of allergy in childhood (see [106, 118]). Consistentwith this hypothesis is the finding that maternal exposure tofarm milk and farm animals during pregnancy was associatedwith demethylation within the FOXP3 (Treg transcriptionfactor) locus in cord blood and subsequent elevated levels ofregulatory T cells (Tregs) (and their suppressive activity) inoffspring [119]. Murine studies have also shown that, whenexposed to a methyl rich diet during pregnancy (as maybe the case for folate supplementation in humans), foetalDNA may undergo changes in methylation that results indecreased gene transcription activity, leading to subsequentenhanced development and severity of allergic diseases [120].The study also showed that this diet-associated allergicphenotype was transgenerationally inheritable (persistenceof high levels of IgE and eosinophilia into the F2 generation).
5. Effector Responses in Atopy andSchistosome Infection
5.1. Immunoglobulin E. Identified in the 1960s as a “carrierof reaginic activity” [121, 122], IgE is well known as acentral player in atopic diseases and anaphylactic reactions.This antibody is part of a protein network involving its3 receptors, namely, the FcεRI, the CD23 (or FcεRII) andgalectin-3 [32], all of which can be found in soluble forms
[123, 124]. The FcεRI (also termed high-affinity receptor)is mainly expressed on mast cells and basophils but also onepidermal Langerhans cells [125] and eosinophils [126, 127].Cross-linking of these high-affinity receptors by IgE inducesactivation of mast cells and basophils and their degranula-tion. The galectin-3 receptor is expressed on neutrophils andon trophoblast cells in placentas [128], where it is thought tofacilitate IgE transport [129]. The CD23 receptor facilitatesthe transport of IgE-antigen complexes but is also involvedin the regulation of IgE synthesis [32]. Highly conserved inmammalian lineages [130], IgE is thought to have evolved asa first line of defence against helminth parasites.
IgE antibodies are naturally strongly regulated and havethe lowest concentrations of all antibodies in serum ofhealthy nonatopic individuals [32]. Mechanisms of regula-tion of IgE include its short half-life in serum (12 h formurine monoclonal antibodies [131]), the poor processingof mRNA for the membrane ε heavy chain [132], and thenegative feedback regulation by the CD23 [133]. The latterhas been a subject of investigations in terms of therapeuticapplication in atopic diseases but also in autoimmunediseases [134] and chronic lymphocytic leukaemia [135].
5.2. CD23. CD23 is the low-affinity receptor for IgE anddiffers from the high-affinity FcεRI receptor in structureand function. Thus, while cross-linking of the latter resultsin degranulation of mast cells and release of mediators,engagement of membrane-bound CD23 suppresses theproduction of IgE by B lymphocytes [33]. CD23 has longbeen proposed as a natural regulator for IgE synthesis [133]although elevated levels of CD23+ B cells have been reportedin atopic patients [136]. As initially suggested by Aubryand colleagues [137], CD23 not only binds IgE but alsoCD21, a cell-surface protein expressed on T-cell, B-cell, andfollicular dendritic cells, classically identified as a receptor forcomplement proteins [138] or Epstein-Barr virus [137]. Theinteraction between CD23, IgE, and CD21 may lead to eithernegative or positive regulation of IgE synthesis (reviewed in[34–36]). The binding of IgE stabilises membrane-boundCD23 and inhibits IgE synthesis from activated B cells, whilein the absence of IgE binding, CD23 is cleaved by ADAM10(a disintegrin and metalloprotease protein 10), and thisdestabilisation enhances IgE synthesis [32]. Soluble CD23(sCD23) fragments resulting from the cleavage can bind toIgE with different affinities and outcomes for IgE synthesisdepending on their oligomerization state. Trimers bind IgEwith high affinity and enhance IgE synthesis by their ability toalso bind the CD21 receptor while monomers bind with lowaffinity but do not bind CD21 and hence inhibit IgE synthesis[36, 139].
5.3. Immunoglobulin 4. Serum IgG4 antibodies, the leastabundant among human IgG subclasses, have long beenassociated with IgE-mediated diseases [140–142]. However,rather than the cause of disease, these antibodies seem tobe involved in the regulation of IgE-induced anaphylacticreactions [143]. IgG4 may interfere with antigen recognitionby IgE due to their similar antigenic specificity [144],although different epitope-binding [145]. In a process that

Journal of Parasitology Research 5
involves exchange of fab molecules, IgG4 are structurallyhetero-bivalent (each heavy chain and light chain recognisinga different epitope within a single IgG4 molecule) and oftenfunction as monovalent [141, 146], to bring about anti-inflammatory effects [147]. The interaction between IgG4and a given antigen results in small and non-pathologicalimmune complexes (since these antibodies cannot cross-link antigens) [146]. Furthermore, in contrast to otherIgG subclasses, IgG4 cannot fix complement but inhibitscomplement activation by IgG1 [148]. IgG4 antibodies, inallergy or helminth infection, are secreted in response to highantigen loads [141, 149, 150] but levels of the antibodiesare differentially regulated by the same cytokines [151] asthose regulating IgE, suggesting an important homeostaticmechanism for controlling IgE-mediated responses.
6. Control of Effector Responses in Atopy andSchistosome Infection
In addition to the cross-regulation between Th1 and Th2[152] (and potentially other T cell subsets), there is growingevidence that Th2 cells interact with a complex networkof other T cell subsets as well as B cells and antibodies,naturally or during disease (atopic or infectious). Thus, it hasemerged that Tregs play an important role in the toleranceof ubiquitous antigens and that alterations in Treg function[153, 154] and/or the fine balance between Tregs and Th2cells [155, 156] determines the clinical manifestation ofatopy. Indeed, in healthy (nonatopic) individuals T cellpolarization occurs in contact with environmental allergensbut higher levels of Tregs dampen the effect of Th2 cells,leading to peripheral tolerance [156]. Tregs modulate theactivity of Th2 (and Th1) cells via several mechanismsincluding the secretion of anti-inflammatory cytokines suchas IL-10 and TGF-β [155, 157]. As the description and role ofother recently identified T-helper cells is clarified (e.g., Th17cells shown to be important in nonatopic asthma) regulationof Th2 mediated responses will also become clearer [158].The role of cells such as the T-helper cells recently shownto produce both IL-17 and Th2 cytokines (IL-4, IL-5, IL-9, and IL-13) [159] in pathogenesis is currently underintense investigation. Our own group has recently describeda role for Th17 responses in human schistosome-acquiredimmunity (submitted).
IL-10 producing B cells (Bregs) are also involved in therecruitment of Tregs, hence contributing to the regulationof Th2 responses as demonstrated in murine models ofhelminth infection (see [31]). IL-10 can inhibit effectorfunctions of mast cells and eosinophils, and regulate thegrowth of several cells including B cells, NK cells, mast cells,and dendritic cells. Furthermore, IL-10 modulates IgE : IgG4ratios [154] possibly by indirectly inducing the antibodyswitch to IgG4 in the B-cell progeny while preventing IgEproduction [160].
IgG4 may control IgE-mediated histamine release as hasbeen demonstrated in filarial infection [143]. Furthermore,it has recently been shown that the binding patterns of IgG4antibodies correspond to natural recovery from childhood
IgE-mediated milk allergy [161], suggesting their potentialprotective role in atopic diseases, although this is stillcontroversial [141]. In addition, early observations that IgG4antibodies were highly elevated in sera of patients receivingallergen immunotherapy [162] have prompted the use ofIgE : IgG4 ratio as a marker for successful immunotherapy[142, 163, 164]. In helminth infections, high IgG4 : IgE ratiohas been associated with reduced pathology while favouringa heavy worm load [150, 165, 166]. Interestingly, IgG4 maybe one of the “regulatory antibodies” resulting from IgGsyalilation involved in the control of immune disorders [167,168].
7. Immune Responses in Atopy
The human immune system must distinguish between adangerous pathogen and ubiquitous environmental allergensand has evolved to mount appropriate defensive responses tothe first while tolerating (or ignoring) the latter. However,a certain proportion of individuals fail to tolerate environ-mental allergens and develop allergic diseases such as asthma,atopic dermatitis and allergic rhinitis. These result fromexcessive sensitisation to ordinary exposures to allergens[104]. IgE antibodies are critical effector molecules in thepathogenesis of these diseases [169]. Mast cells and basophilsare coated with specific IgE antibodies and this results inimmediate hypersensitivity (release of mediators) and/orlate-phase inflammatory reaction (cytokine secretion andrecruitment of leucocytes).
In atopic individuals, allergen products (e.g., cysteineproteases) activate epithelial cells, which produce thymicstromal lymphopoietin (TSLP), IL-25, and IL-33 which inturn initiate Th2 polarisation with increased productionof IL-4, IL-5, IL-9, and IL-13 cytokines [170, 171]. Th2cytokines are involved in the class-switching to IgE as wellas the development and recruitment of basophils, mastcells, and eosinophils (see Figure 1(c)). IgE binds to thehigh-affinity FcεRI receptor on mast cells, basophils, andeosinophils which (upon exposure to allergens) results intheir activation and degranulation (via cross-linking ofallergens), with the release of preformed mediators suchas histamine, cysteinyl leukotrienes, and prostaglandin D2
[154, 172].
A complex interplay between innate and adaptiveimmune responses underlies the heterogeneous characteris-tics of atopic diseases. Thus, recruitment of eosinophils intothe lungs of asthmatics may be promoted not just by Th2(IL-5) alone but in conjunction with natural killer T cells(NKT) as well as CD8+ T cells (see [173]). In addition, IL-17-producing T cells (Th17 [174]) may be involved in theseverity of asthma [175]. These promote the recruitmentand activation of neutrophils and lead to corticosteroids—resistant asthma [175]. IL-9-producing T-cell subset (Th9),which probably derive from Th2 cells under the influenceof TGFβ1 [176], may also be involved in the production ofIgE and mast cell recruitment in the lungs [173]. In allergicrhinitis, mast cells accumulate in the epithelium of the nasalmucosa where they secrete inflammatory cytokines (IL-6, IL-8, and TNFα) in addition to Th2 cytokines [177].

6 Journal of Parasitology Research
Parasite burden
APC
IL-25
IL-10
IL-10
IL-1
0
Breg Treg
Th2Th2
Th2
Th2
Th2
CD23?
CTLA4
TGFβ
IL-4 IL-4
IL-5
IL-5IL-3, IL-9 IL-3, IL-9
IL-4, IL-10 IL-4, IL-13
B
BB Eos
Eos
Bas
Bas
AAM
MC
MC
IgE IgE
YY
Y
Y
YY
Y
Allergen
IL-25, IL-33
GITR
IgG4 ≫ IgE
(I)
(II)(III)
(a) Primary infection (b) Secondary/chronic infection (c) Atopic inflammation
Figure 1: Possible regulatory mechanisms in helminth infections. Primary response (a) to parasite antigens involves Th2 polarization,IgE production, and eosinophil, mast cell, and basophil activation (I), mechanisms similar to those observed in allergic sensitisation (c).This Th2-response may be induced by parasite-secreted antigens such as the Omega-1 secreted by S. mansoni eggs [25]. However, withincreasing parasite load or chronic infection (b), regulatory B cells are activated which suppress Th2 responses (II) via IL-10 secretionor CD23 expression [26], and/or contribute to the recruitment of Tregs [27]. Tregs (III), which may also be induced and expanded byparasite antigens [28, 29], either induce anergic Th2 cells (expressing GITR and CTLA4) unable to progress through to effector cells, ormodify downstream effector functions such as B cell switch to IgG4 and/or alternative activation of macrophages, resulting in immunologicaltolerance (reviewed by [30]). This immunosuppression is induced in the context of helminth infection, but may also expand to allergen-induced inflammation (gray line), hence suppressing allergy. DC: dendritic cell; B: B cell, Eos: eosinophil; Bas: basophil; MC: mast cell; GITR:glucocorticoid-induced TNFα-related protein; CTLA4: cytotoxic T lymphocyte antigen 4; AAM: alternatively activated macrophage; Breg:regulatory B cell; Treg: regulatory T cell. The question mark (?) denotes lack of strong evidence. Figure adapted from [30, 31] and collatedinformation from the cited references.
8. Immune Responses duringSchistosome Infection
Acquired immunity to schistosome infection was first pro-posed by Fisher in the 1930s when analysing data fromanimal studies as well as those from hospital-diagnosedS. haematobium infected people [88]. Subsequently, thesusceptibility of schistosome larvae to immune attack wasdemonstrated by in vitro studies showing that sera from S.mansoni infected individuals could damage schistosomula inthe presence of normal human peripheral blood leucocytes[178]. This “antibody-dependent” killing was subsequentlyshown to be eosinophil mediated [178, 179], and studieson monoclonal antibodies led to the identification of IgEantibodies with the highest cytotoxicity for the schistosomula[180–182]. Field studies were conducted to identify antibodyresponses predictive of resistance to reinfection followingchemotherapy. Hagan et al. [83] demonstrated in a multi-variate logistic regression that reinfection with S. haemato-bium was less likely in individuals producing high IgE levelsagainst the worm antigens and more likely in those produc-ing high levels of IgG4 against the worm or egg antigens. Therole of IgE in resistance was also demonstrated by Rihet et al.
[183], who identified specific antigens (120–165 KDa and85 KDa) to which IgE reacted (on immunoblots) and showedthat these antibodies, in contrast to IgM and IgG, were sig-nificantly higher in the sera of the most resistant individuals.This study showed that some of the immunogenic antigenswere readily accessible to IgE on living S. mansoni larvae asthey were located on the outer membrane. However, Dunneand colleagues, working on S. mansoni as well, showedthat IgE (produced following treatment) against adult wormantigens, particularly a 22 kDa tegumental antigen (Sm22),but not against any other life-cycle stages, were associatedwith resistance to reinfection following treatment [184].Both antiadult worm and anti-schistosomula tegument IgEantibodies were associated with resistance to S. mansonireinfection in another study in Brazil [185] while antiegg IgEantibodies also could confer protection against S. japonicumreinfection [186].
Collectively, these studies and several others [187–190]have led to the conclusion that resistance to schistosomeinfection/reinfection is dependent on IgE antibodies. How-ever, data on other antibody isotypes have been reportedwhich correlated with resistance to infection/reinfection. Forexample, IgG3 against the recombinant antigen Sh13 has

Journal of Parasitology Research 7
been associated with resistance to S. haematobium infection[191], while antiworm and cercariae IgM were significantlyhigher in individuals more resistant to reinfection with S.mansoni [185]. Furthermore, a decline in IgA together withan increase in IgG1 were associated with resistance acquiredwith host age as well as following treatment in S. haema-tobium endemic area [192]. IgA against Sm28GST antigenhas also been associated with reduced S. mansoni fecundityand increased host resistance to reinfection [193]. Morerecently, antiworm IgE antibodies, as well as eosinophiliaand the low affinity receptor for IgE (the CD23) have beenshown to correlate with resistance in individuals undergoingmultiple rounds of treatment [100, 194], again suggestingthat IgE may be directly involved in parasite killing viaantibody-dependent cellular cytotoxicity (ADCC) in vivo.However, since schistosomula are more susceptible to ADCC,it is possible that adult-worm-specific antibody responsesmay rather target the incoming larvae, a process termed“concomitant immunity” (as predicted by Fisher [88]) andwell demonstrated in rhesus monkeys [195].
As initially demonstrated by in vitro studies [196–198],ADCC is dependent on Th2 cytokines, and these have beeninvolved in resistance to schistosome infection. Thus, higherratios of IL-4/IFN-γ and IL-5/IFN-γ were produced by spe-cific T-cell clones from S. mansoni resistant than susceptibleindividuals [199] and IL-5 correlated with lower levels ofS. haematobium infection [99] and S. mansoni reinfectionafter treatment [200]. Furthermore, IL-4, IL-5, and IL-10levels were associated with resistance posttreatment whileIFN-γ was associated with susceptibility [201]. However,significantly higher levels of IFN-γ against adult worm andcercariae antigens by PBMCs from resistant individuals com-pared to those from susceptible individuals [202], suggestingthat acquired resistance to human schistosomiasis cannot beexclusively classified into a single T helper cell subset.
Cellular immune responses, although involved in resis-tance, mediate most of schistosome-related pathology [203,204], which can be divided into acute and chronic diseasesbased on disease progression. Acute schistosomiasis is adebilitating febrile disease which often occurs in individualswith no experience of infection. It is characterized byhigh percentage of eosinophilia, which may be reversedby chemotherapy [205], nausea, urticaria, dry cough, andfever [206, 207]. Anatomically, this stage is accompaniedby a dissemination of large and destructive granulomasaround the eggs [67, 208]. Chronic schistosomiasis is oftenreferred to as a Th2 disease and accounts for most humanimmunopathologies in endemic areas [77, 204, 208–210].As infection becomes chronic, schistosome eggs lodge in theliver, gut (S. mansoni), or bladder (S. haematobium), andthe granulomatous response translates into extensive tissuedamage and excessive extracellular matrix protein (ECMP)deposition, leading to fibrosis [210].
9. Immunological Interaction betweenHelminth Antigens and Allergens
9.1. Helminth Infection and the “Mast Cell Saturation”Hypothesis. The earliest protective mechanism of helminth
infection suggested was “mast cell saturation,” wherebyhelminths induce high levels of nonspecific IgE that saturateFc receptors on mast cells, thus inhibiting hypersensitivityreactions [211, 212]. Further supportive evidence for theFc saturation hypothesis came from a study showing thathistamine release of human mast cells from lung fragmentscould be blocked by preexposure of these fragments tohigh total IgE [213]. However, more recent studies onbasophils have shown that high levels of polyclonal IgE andpolyclonal/specific IgE ratios from filarial- and hookworm-infected patients do not prevent antigen-induced histaminerelease [214, 215]. Nevertheless, Mitre and colleagues wereable to show that extremely high ratios of polyclonal/specificIgE, enhanced with polyclonal myeloma IgE in vitro, couldprevent histamine release [214]. Although basophils andmast cells may be differentially regulated [216], these exper-iments suggested that the FcεRI receptor saturation may notbe the primary mechanism by which helminths “protect”against allergy.
9.2. Helminth Infection and Cross-Reactive IgE Responses.Another hypothesis suggested was that helminth parasitesinduce a “clinically irrelevant” allergen-specific IgE response,which would be cross-reactive between helminths andallergens [217]. Cross-reactive anti-tropomyosin IgE anti-bodies between helminths and allergens have recently beendemonstrated, where monkeys infected with Loa loa (filarialparasites) mounted an IgE cross-reacting between filarialtropomyosin and Derp 1 allergen but not with timothygrass [218]. Furthermore, cross-reactivity between ascarisand mites has been reported [219]. However, field studiesreport mixed results on the effects of helminth infections onallergen-specific IgE in endemic areas [220–222]. Our recentstudy has demonstrated that the levels of anti-Derp1 IgEantibodies inversely correlate with S. haematobium infectionintensity in a high schistosome infection area in Zimbabwe[223].
9.3. Helminth-Induced Immunomodulation. Technologicaland scientific advances such as genomic sequences andproteomic approaches have generated molecular and evolu-tionary information on the relationship between helminthparasites and allergic reactivity. Helminth infections aregenerally characterised by a Th2-polarised immune response[25, 84, 224], which is often associated with host resistanceto infection/reinfection [30]. However, this Th2 responseis also associated with pathology [204], consistent withthe role for Th2 in allergic diseases [171]. Nevertheless,helminth parasites are capable of modulating this response toprolong their survival and minimize severe pathology in theirhost [76, 84, 225]. This immunomodulation is thought toaffect unrelated antigens such as allergens, hence dampeningthe clinical manifestation of allergy. Indeed, experimentalstudies have demonstrated helminth-induced suppression ofallergic responses via multiple pathways (Figure 1). However,these observations and mechanisms remain to be rigorouslytested in humans. Furthermore, biological and evolutionarydifferences in the mouse experimental host and the naturalhuman host must be taken into account when extrapolating

8 Journal of Parasitology Research
IgE
mCD23
sCD23
CD21ADAM10
Cleavage sites
B-cell membrane
NNNNN
IgE (Cε) transcription in nucleus
(I)
(II)
(III)(IV)
Figure 2: Interaction between CD23 and its ligands, IgE and CD21. Binding of IgE stabilises membrane-bound CD23 and inhibits IgEsynthesis (I) from activated B cells while in the absence of IgE binding the CD23 is cleaved by ADAM10 (a disintegrin and metalloproteaseprotein 10) and this destabilisation enhances IgE synthesis (II). However, soluble CD23 (sCD23) fragments resulting from the cleavagehave the ability to bind IgE with different affinities depending on their oligomerization state: trimers (III) bind IgE with high affinity whilemonomers (IV) bind with low affinity. Trimers enhance IgE synthesis by their ability to also bind CD21 receptor (III) while monomers failto bind CD21 and inhibit IgE synthesis (IV) (adapted from [32–36]).
mechanistic and phenomenological results from the mouseto the human, for example, differences in the IgE receptors[226].
Human studies investigating the regulatory mechanismsunderlying the protective effect of helminth infections onatopy have primarily focused on IL-10. Thus, parasite-induced IL-10 production and skin prick reactivity werenegatively associated in Ascaris lumbricoides [42] and Schisto-soma haematobium [46] infected populations. Furthermore,allergen-induced IL-10 was associated with reduced Th2responses (IL-4 and IL-5) in asthmatic schistosome infectedpatients [227]. More recently, it has been shown that thefrequency of PBMCs expressing cytotoxic-T-lymphocyteantigen 4 (CTLA-4) and monocytes expressing IL-10 fromasthmatic patients infected with S. mansoni was significantlyhigher compared to their asthmatic uninfected counterparts[228]. However, a study on an Ecuadorian populationshowed no association between skin prick reactivity witheither IL-10 or IL-10-producing T cells induced by Ascarislumbricoides [40].
The TGFβ is another cytokine involved in the modu-lation of immune responses, and is secreted by antigen-presenting cells (APCs) or regulatory T cells [229]. However,there is a paucity of human studies on this cytokine inthe context of atopy and helminth infections. Interestingly,we have observed a negative association between atopyand the levels of soluble CD23 in S. haematobium infectedpopulations (Rujeni et al., manuscript in preparation). TheCD23 is the low affinity receptor for IgE and is involved in theregulation of these antibodies [35]. As illustrated in Figure 2,the soluble CD23 can either upregulate or downregulate IgEsynthesis depending on their size and oligomerization state.
Of note, expression of this receptor has been associated withresistance to schistosome [194] and Ascaris [230] infectionsin humans, and suppressed airway allergy in helminth-infected mice [231].
As illustrated in Figure 1, immunomodulation duringchronic helminth infection is driven by regulatory T andB cells (Tregs and Bregs, resp.), which secrete the abovementioned anti-inflammatory cytokines. Treg cells are eitherrecruited by Bregs or induced and expanded by helminth-derived products [28]. Both T and B regulatory cells cansuppress Th2 cells thereby regulating atopy and helminth-induced pathology [31, 232]. Indeed, a study in our labhas shown that Treg proportions correlate with the levels ofschistosome infection in young children actively acquiringinfection [233].
Helminth molecules have been identified from excretory-secretory (ES) products that are associated with immunomo-dulation during helminth infection. Thus, the ES-62 isa phosphorylcholine-containing glycoprotein secreted byAcanthocheilonema viteae, a rodent filarial nematode [234].This protein presents anti-inflammatory properties and hasbeen successfully tested in mouse models of allergy andautoimmune diseases [235, 236], and it is currently beingexploited as a potential therapeutic agent for inflammatorydiseases in humans [237]. The anti-inflammatory propertiesof this molecule include modulation of B-cell proliferationand cytokine production as well as hyporesponsivenessand desensitization of mast-cell degranulation [237–240].The interleukin-4-inducing principle from S. mansoni eggIPSE/alpha-1, identified as one of the most abundantproteins secreted by S. mansoni eggs [241], has also beenassociated with immunomodulation, possibly by inducing

Journal of Parasitology Research 9
granulomatous responses [242]. Furthermore, IPSE/alpha-1 has been shown to induce antigen-independent IL-4production by murine basophils in vivo [243]. The venomallergen-like (VAL) proteins are another group of helminthES products involved in immunomodulation. Thus, Hewit-son et al. have demonstrated that antibodies to these VALantigens are dominant in susceptible mice in an H. polygyrusinfection model [244]. Sj-VAL-1 is one of the VAL proteinsidentified in S. japonicum egg ES products inducing anantibody response during the first 6 weeks of infection inmice [245].
10. Convergence of Allergic andAntiparasite Responses
There is current interest in determining the common featuresin the induction of immune responses by allergens and byhelminths as well as the evolutionary advantages of main-taining allergic responses. As illustrated above, several studieshave suggested that similarities in antigens may underliethe commonality of Th2 responses elicited by allergens andby helminths. A recent review [246] of allergic responsesindicated that there is relatively little structural similaritybetween different allergens (e.g., house dust mite, foodallergens, and haematophagous fluids) and between allergensand helminth parasites. Instead, this paper suggests that therelationship between allergic and antiparasite Th2 responsesarises from a common response to different classes ofenvironmental challenges which include helminth parasites,venoms and haematophagous fluids, and environmentalirritants such as carcinogens and noxious xenobiotics, sothat this diverse group of stimuli activates responses collec-tively known as “allergic host defences” [246]. Within thisparadigm, these environmental challenges are characterisedonly by the type of response they elicit with multiplepathways leading to the activation of Th2 responses withthe result of protecting against environmental challenges byeither reduced exposure to, or elimination of the “irritant.”In this scenario, allergic reactivity is believed to have evolvedas an important and essential mechanism against harmrather than a harmful overreaction of a misdirected immunesystem [247]. Studies in cancer patients also show a negativeassociation between cancer and atopy which has led tothe suggestion that allergy protects against some types ofcancer [248, 249]. This suggests that the Th2 responsesprotecting against allergens, carcinogens, and helminths arecomplex. This presents a challenge for the developmentof therapeutics relying on helminth products to overcomeallergic responses, since induction of allergic responses aswell as the effector mechanisms maybe tightly regulated, andthe effector responses they elicit may have been selected forredundancy.
11. Conclusions
We have shown similarities in the immunological responsesto schistosome parasites and to allergens. Studies continueto determine the aetiology of the similar responses and theevolutionary pathways that may have led to the development
and maintenance of allergic responses which are paradoxi-cally harmful to the host [246, 247], but may be essential toprotect against harm from environmental challenges [246].The clinical manifestation of atopy is complex with severalstudies from helminth endemic areas having shown thatallergic sensitisation and clinical manifestation of allergycan be dissociated [222]. Furthermore, allergic disease andparasitic infections exist as comorbidities in many patientsand are not mutually exclusive [250]. The role of impairedserological allergy diagnosis in parasitized allergy patientsas well as under diagnosis in developing countries needs tobe addressed to inform future studies. Detailed longitudinaland mechanistic studies relating atopy and clinical disease toschistosome infection and disease in human populations willbe valuable to inform on not only the immunological processoccurring, but more importantly on clinical management ofallergy and schistosomiasis patients.
Acknowledgments
This paper contains some of our work which was fundedby the World Health Organization (Grant no. RPC264), TheWelcome Trust (Grant no. WT082028MA), the Universityof Edinburgh, and the Government of Rwanda. F. Mutapiis funded by the Thrasher Foundation. The authors aregrateful to Laura Appleby for providing comments on themanuscript.
References
[1] N. R. Stoll, “This wormy world,” Journal of Parasitology, vol.33, pp. 1–18, 1947.
[2] GaHI, “Global Atlas of helminth infections,” Consulted,Manta Ray Media Ltd, 2012, http://www.thiswormyworld.org/.
[3] P. J. Hotez, J. H. F. Remme, P. Buss, G. Alleyne, C. Morel, andJ. G. Breman, “Combating tropical infectious diseases: reportof the disease control priorities in developing countriesproject,” Clinical Infectious Diseases, vol. 38, no. 6, pp. 871–878, 2004.
[4] P. J. Hotez, P. J. Brindley, J. M. Bethony, C. H. King, E.J. Pearce, and J. Jacobson, “Helminth infections: the greatneglected tropical diseases,” Journal of Clinical Investigation,vol. 118, no. 4, pp. 1311–1321, 2008.
[5] J. Bethony, S. Brooker, M. Albonico et al., “Soil-transmittedhelminth infections: ascariasis, trichuriasis, and hookworm,”The Lancet, vol. 367, no. 9521, pp. 1521–1532, 2006.
[6] C. H. King and M. Dangerfield-Cha, “The unacknowledgedimpact of chronic schistosomiasis,” Chronic Illness, vol. 4, no.1, pp. 65–79, 2008.
[7] C. H. King, K. Dickman, and D. J. Tisch, “Reassessment ofthe cost of chronic helmintic infection: a meta-analysis ofdisability-related outcomes in endemic schistosomiasis,” TheLancet, vol. 365, no. 9470, pp. 1561–1569, 2005.
[8] N. Aıt-Khaled, N. Pearce, H. R. Anderson et al., “Globalmap of the prevalence of symptoms of rhinoconjunctivitis inchildren: the International Study of Asthma and Allergies inChildhood (ISAAC) Phase Three,” Allergy, vol. 64, no. 1, pp.123–148, 2009.
[9] H. Williams, C. Robertson, A. Stewart et al., “Worldwidevariations in the prevalence of symptoms of atopic eczema inthe international study of asthma and allergies in childhood,”

10 Journal of Parasitology Research
Journal of Allergy and Clinical Immunology, vol. 103, no. 1 I,pp. 125–138, 1999.
[10] E. N. Sibanda, “Inhalant allergies in Zimbabwe: a commonproblem,” International Archives of Allergy and Immunology,vol. 130, no. 1, pp. 2–9, 2003.
[11] R. Beasley, S. Nishima, N. Pearce, and J. Crane, “β-agonisttherapy and asthma mortality in Japan,” The Lancet, vol. 351,no. 9113, pp. 1406–1407, 1998.
[12] P. Davis, R. Jackson, and N. Pearce, “Asthma mortality,” NewZealand Medical Journal, vol. 98, no. 783, p. 604, 1985.
[13] R. Jackson, “Undertreatment and asthma deaths,” TheLancet, vol. 2, no. 8453, p. 500, 1985.
[14] R. Brown, F. Turk, P. Dale, and J. Bousquet, “Cost-effective-ness of omalizumab in patients with severe persistent allergicasthma,” Allergy, vol. 62, no. 2, pp. 149–153, 2007.
[15] R. Gupta, A. Sheikh, D. P. Strachan, and H. R. Anderson,“Burden of allergic disease in the UK: secondary analyses ofnational databases,” Clinical and Experimental Allergy, vol.34, no. 4, pp. 520–526, 2004.
[16] P. Suwan, D. Akaramethathip, and P. Noipayak, “Associationbetween allergic sensitization and attention deficit hyperac-tivity disorder (ADHD),” Asian Pacific Journal of Allergy andImmunology, vol. 29, no. 1, pp. 57–65, 2011.
[17] M. C. Tsai, H. K. Lin, C. H. Lin, and L. S. Fu, “Prevalenceof attention deficit/hyperactivity disorder in pediatric allergicrhinitis: a nationwide population-based study,” Allergy andAsthma Proceedings, vol. 32, no. 6, pp. 41–46, 2011.
[18] B. Taylor, J. Wadsworth, M. Wadsworth, and C. Peckham,“Changes in the reported prevalence of childhood eczemasince the 1939–45 war,” The Lancet, vol. 2, no. 8414, pp. 1255–1257, 1984.
[19] M. B. Emanuel, “Hay fever, a post industrial revolutionepidemic: a history of its growth during the 19th century,”Clinical Allergy, vol. 18, no. 3, pp. 295–304, 1988.
[20] F. D. Martinez, D. A. Stem, A. L. Wright, L. M. Taussig, andM. Halonen, “Association of non-wheezing lower respiratorytract illnesses in early life with persistently diminished serumIgE levels,” Thorax, vol. 50, no. 10, pp. 1067–1072, 1995.
[21] S. O. Shaheen, P. Aaby, A. J. Hall et al., “Measles and atopyin Guinea-Bissau,” The Lancet, vol. 347, no. 9018, pp. 1792–1796, 1996.
[22] J. S. Alm, G. Lilja, G. Pershagen, and A. Scheynius, “EarlyBCG vaccination and development of atopy,” The Lancet, vol.350, no. 9075, pp. 400–403, 1997.
[23] I. L. Strannegard, L. O. Larsson, G. Wennergren, and O.Strannegard, “Prevalence of allergy in children in relation toprior BCG vaccination and infection with atypical mycobac-teria,” Allergy, vol. 53, no. 3, pp. 249–254, 1998.
[24] P. M. Matricardi, F. Rosmini, S. Riondino et al., “Exposure tofoodborne and orofecal microbes versus airborne viruses inrelation to atopy and allergic asthma: epidemiological study,”British Medical Journal, vol. 320, no. 7232, pp. 412–417, 2000.
[25] B. Everts, G. Perona-Wright, H. H. Smits et al., “Omega-1,a glycoprotein secreted by Schistosoma mansoni eggs, drivesTh2 responses,” Journal of Experimental Medicine, vol. 206,no. 8, pp. 1673–1680, 2009.
[26] M. S. Wilson, M. D. Taylor, M. T. O’Gorman et al.,“Helminth-induced CD19+CD23hi B cells modulate exper-imental allergic and autoimmune inflammation,” EuropeanJournal of Immunology, vol. 40, no. 6, pp. 1682–1696, 2010.
[27] S. Amu, S. P. Saunders, M. Kronenberg, N. E. Mangan, A.Atzberger, and P. G. Fallon, “Regulatory B cells prevent andreverse allergic airway inflammation via FoxP3-positive Tregulatory cells in a murine model,” Journal of Allergy and
Clinical Immunology, vol. 125, no. 5, pp. 1114.e8–1124.e8,2010.
[28] H. J. McSorley, Y. M. Harcus, J. Murray, M. D. Taylor, and R.M. Maizels, “Expansion of Foxp3+ regulatory T cells in miceinfected with the filarial parasite Brugia malayi,” Journal ofImmunology, vol. 181, no. 9, pp. 6456–6466, 2008.
[29] J. R. Grainger, K. A. Smith, J. P. Hewitson et al., “Helminthsecretions induce de novo T cell Foxp3 expression andregulatory function through the TGF-β pathway,” Journal ofExperimental Medicine, vol. 207, no. 11, pp. 2331–2341, 2010.
[30] J. E. Allen and R. M. Maizels, “Diversity and dialogue inimmunity to helminths,” Nature Reviews Immunology, vol.11, no. 6, pp. 375–388, 2011.
[31] L. Hussaarts, L. E. P. M. van der Vlugt, M. Yazdanbakhsh,and H. H. Smits, “Regulatory B-cell induction by helminths:implications for allergic disease,” Journal of Allergy andClinical Immunology, vol. 128, no. 4, pp. 733–739, 2011.
[32] H. J. Gould and B. J. Sutton, “IgE in allergy and asthmatoday,” Nature Reviews Immunology, vol. 8, no. 3, pp. 205–217, 2008.
[33] M. Acharya, G. Borland, A. L. Edkins et al., “CD23/Fcepsi-lonRII: molecular multi-tasking,” Clinical and ExperimentalImmunology, vol. 162, no. 1, pp. 12–23, 2010.
[34] R. G. Hibbert, P. Teriete, G. J. Grundy et al., “The structureof human CD23 and its interactions with IgE and CD21,”Journal of Experimental Medicine, vol. 202, no. 6, pp. 751–760, 2005.
[35] D. H. Conrad, J. W. Ford, J. L. Sturgill, and D. R. Gibb,“CD23: an overlooked regulator of allergic disease,” CurrentAllergy and Asthma Reports, vol. 7, no. 5, pp. 331–337, 2007.
[36] S. L. Bowles, C. Jaeger, C. Ferrara et al., “Comparative bind-ing of soluble fragments (derCD23, sCD23, and exCD23) ofrecombinant human CD23 to CD21 (SCR 1-2) and nativeIgE, and their effect on IgE regulation,” Cellular immunology,vol. 271, no. 2, pp. 371–378, 2011.
[37] D. Dagoye, Z. Bekele, K. Woldemichael et al., “Wheezing,allergy, and parasite infection in children in urban and ruralethiopia,” American Journal of Respiratory and Critical CareMedicine, vol. 167, no. 10, pp. 1369–1373, 2003.
[38] N. R. Lynch, I. Hagel, M. Perez, M. C. Di Prisco, R. Lopez, andN. Alvarez, “Effect of anthelmintic treatment on the allergicreactivity of children in a tropical slum,” Journal of Allergyand Clinical Immunology, vol. 92, no. 3, pp. 404–411, 1993.
[39] L. J. Palmer, J. C. Celedon, S. T. Weiss, B. Wang, Z. Fang,and X. Xu, “Ascaris lumbricoides infection is associated withincreased risk of childhood asthma and atopy in rural China,”American Journal of Respiratory and Critical Care Medicine,vol. 165, no. 11, pp. 1489–1493, 2002.
[40] P. J. Cooper, E. Mitre, A. L. Moncayo, M. E. Chico, M.G. Vaca, and T. B. Nutman, “Ascaris lumbricoides-inducedinterleukin-10 is not associated with atopy in schoolchildrenin a rural area of the tropics,” Journal of Infectious Diseases,vol. 197, no. 9, pp. 1333–1340, 2008.
[41] P. J. Cooper, M. E. Chico, M. G. Vaca et al., “Effect ofalbendazole treatments on the prevalence of atopy in childrenliving in communities endemic for geohelminth parasites: acluster-randomised trial,” The Lancet, vol. 367, no. 9522, pp.1598–1603, 2006.
[42] C. Flohr, L. N. Tuyen, R. J. Quinnell et al., “Reduced helminthburden increases allergen skin sensitization but not clinicalallergy: a randomized, double-blind, placebo-controlled trialin Vietnam,” Clinical and Experimental Allergy, vol. 40, no. 1,pp. 131–142, 2010.

Journal of Parasitology Research 11
[43] L. C. Rodrigues, P. J. Newcombe, S. S. Cunha et al., “Earlyinfection with Trichuris trichiura and allergen skin testreactivity in later childhood,” Clinical and ExperimentalAllergy, vol. 38, no. 11, pp. 1769–1777, 2008.
[44] M. I. Araujo, A. A. Lopes, M. Medeiros et al., “Inverse associa-tion between skin response to aeroallergens and Schistosomamansoni infection,” International Archives of Allergy andImmunology, vol. 123, no. 2, pp. 145–148, 2000.
[45] M. Medeiros Jr., J. P. Figueiredo, M. C. Almeida et al., “Schis-tosoma mansoni infection is associated with a reduced courseof asthma,” Journal of Allergy and Clinical Immunology, vol.111, no. 5, pp. 947–951, 2003.
[46] A. H. J. van den Biggelaar, R. Van Ree, L. C. Rodrigueset al., “Decreased atopy in children infected with Schistosomahaematobium: a role for parasite-induced interleukin-10,”The Lancet, vol. 356, no. 9243, pp. 1723–1727, 2000.
[47] P. J. Hotez and A. Fenwick, “Schistosomiasis in Africa: anemerging tragedy in our new global health decade,” PLoSNeglected Tropical Diseases, vol. 3, no. 9, article e485, 2009.
[48] A. Fenwick, J. P. Webster, E. Bosque-Oliva et al., “The Schis-tosomiasis Control Initiative (SCI): rationale, developmentand implementation from 2002–2008,” Parasitology, vol. 136,no. 13, pp. 1719–1730, 2009.
[49] B. Gryseels, K. Polman, J. Clerinx, and L. Kestens, “Humanschistosomiasis,” The Lancet, vol. 368, no. 9541, pp. 1106–1118, 2006.
[50] J. R. Stothard and A. F. Gabrielli, “Schistosomiasis in Africaninfants and preschool children: to treat or not to treat?”Trends in Parasitology, vol. 23, no. 3, pp. 83–86, 2007.
[51] J. Ring, “Davos Declaration: allergy as a global problem,”Allergy, vol. 67, no. 2, pp. 141–143, 2012.
[52] L. J. Akinbami and K. C. Schoendorf, “Trends in childhoodasthma: prevalence, health care utilization, and mortality,”Pediatrics, vol. 110, no. 2, part 1, pp. 315–322, 2002.
[53] J. M. Smith, M. E. Disney, J. D. Williams, and Z. A. Goels,“Clinical significance of skin reactions to mite extracts inchildren with asthma,” British Medical Journal, vol. 1, no. 659,pp. 723–726, 1969.
[54] D. O. Miranda, A. O. Deise Silva, F. C. Jorge et al., “Serum andsalivary IgE, IgA, and IgG4 antibodies to Dermatophagoidespteronyssinus and its major allergens, Der p1 and Der p2, inallergic and nonallergic children,” Clinical and DevelopmentalImmunology, vol. 2011, Article ID 302739, 11 pages, 2011.
[55] J. L. Hopper, M. A. Jenkins, J. B. Carlin, and G. G. Giles,“Increase in the self-reported prevalence of asthma and hayfever in adults over the last generation: a matched parent-offspring study,” Australian Journal of Public Health, vol. 19,no. 2, pp. 120–124, 1995.
[56] D. Jarvis, R. Newson, J. Lotvall et al., “Asthma in adults andits association with chronic rhinosinusitis: the GA(2) LENsurvey in Europe,” Allergy, vol. 67, no. 1, pp. 91–98, 2011.
[57] S. Musafiri, J. van Meerbeeck, L. Musango et al., “Prevalenceof atopy, asthma and COPD in an urban and a rural area ofan African country,” Respiratory Medicine, vol. 105, no. 11,pp. 1596–1605, 2011.
[58] C. K. W. Lai, R. Beasley, J. Crane et al., “Global variationin the prevalence and severity of asthma symptoms: phaseThree of the International Study of Asthma and Allergies inChildhood (ISAAC),” Thorax, vol. 64, no. 6, pp. 476–483,2009.
[59] C. H. Katelaris, B. W. Lee, P. C. Potter et al., “Prevalence anddiversity of allergic rhinitis in regions of the world beyondEurope and North America,” Clinical and ExperimentalAllergy, vol. 42, no. 2, pp. 186–207, 2011.
[60] K. Westritschnig, E. Sibanda, W. Thomas et al., “Analysis ofthe sensitization profile towards allergens in central Africa,”Clinical and Experimental Allergy, vol. 33, no. 1, pp. 22–27,2003.
[61] K. Arkestl, E. Sibanda, C. Thors et al., “Impaired allergydiagnostics among parasite-infected patients caused byIgE antibodies to the carbohydrate epitope galactose-α1,3-galactose,” Journal of Allergy and Clinical Immunology, vol.127, no. 4, pp. 1024–1028, 2011.
[62] J. C. Samuelson and J. P. Caulfield, “The cercarial glycocalyxof Schistosoma mansoni,” Journal of Cell Biology, vol. 100, no.5, pp. 1423–1434, 1985.
[63] J. T. Culbertson, “The cercaricidal action of normal serums,”The Journal of Parasitology, vol. 22, no. 2, 1936.
[64] W. Dias Da Silva and M. D. Kazatchkine, “Schistosomamansoni: activation of the alternative pathway of humancomplement by schistosomula,” Experimental Parasitology,vol. 50, no. 2, pp. 278–286, 1980.
[65] S. J. Jenkins, J. P. Hewitson, S. Ferret-Bernard, and A.P. Mountford, “Schistosome larvae stimulate macrophagecytokine production through TLR4-dependent and -inde-pendent pathways,” International Immunology, vol. 17, no.11, pp. 1409–1418, 2005.
[66] R. A. Paveley, S. A. Aynsley, J. D. Turner et al., “The MannoseReceptor (CD206) is an important pattern recognitionreceptor (PRR) in the detection of the infective stage of thehelminth Schistosoma mansoni and modulates IFNgammaproduction,” International Journal for Parasitology, vol. 41,no. 13-14, pp. 1335–1345, 2011.
[67] J. R. Lambertucci, “Acute Schistosomiasis mansoni: revisitedand reconsidered,” Memorias do Instituto Oswaldo Cruz, vol.105, no. 4, pp. 422–435, 2010.
[68] S. V. Brant and E. S. Loker, “Schistosomes in the southwestUnited States and their potential for causing cercarialdermatitis or swimmer’s itch,” Journal of Helminthology, vol.83, no. 2, pp. 191–198, 2009.
[69] S. J. Fraser, S. J. R. Allan, M. Roworth et al., “Cercarial der-matitis in the UK,” Clinical and Experimental Dermatology,vol. 34, no. 3, pp. 344–346, 2009.
[70] A. Soleng and R. Mehl, “Geographical distribution ofcercarial dermatitis in Norway,” Journal of Helminthology,vol. 85, no. 3, pp. 345–352, 2010.
[71] P. C. Cook, S. A. Aynsley, J. D. Turner et al., “Multiplehelminth infection of the skin causes lymphocyte hypo-responsiveness mediated by Th2 conditioning of dermalmyeloid cells,” PLoS Pathogens, vol. 7, no. 3, Article IDe1001323, 2011.
[72] K. Ramaswamy, P. Kumar, and Y. X. He, “A role for parasite-induced PGE2 in IL-10-mediated host immunoregulation byskin stage schistosomula of Schistosoma mansoni,” Journal ofImmunology, vol. 165, no. 8, pp. 4567–4574, 2000.
[73] V. Angeli, C. Faveeuw, P. Delerive et al., “Schistosoma mansoniinduces the synthesis of IL-6 in pulmonary microvascu-lar endothelial cells: role of IL-6 in the control of lungeosinophilia during infection,” European Journal of Immunol-ogy, vol. 31, no. 9, pp. 2751–2761, 2001.
[74] F. Trottein, S. Nutten, V. Angeli et al., “Schistosoma mansonischistosomula reduce E-selectin and VCAM-1 expression inTNF-alpha-stimulated lung microvascular endothelial cellsby interfering with the NF-kappaB pathway,” EuropeanJournal of Immunology, vol. 29, no. 11, pp. 3691–3701, 1999.
[75] E. J. Pearce, C. M. Kane, J. Sun, J. J. Taylor, A. S. McKee, andL. Cervi, “Th2 response polarization during infection with

12 Journal of Parasitology Research
die helminth parasite Schistosoma mansoni,” ImmunologicalReviews, vol. 201, pp. 117–126, 2004.
[76] E. J. Pearce and A. S. MacDonald, “The immunobiology ofschistosomiasis,” Nature Reviews Immunology, vol. 2, no. 7,pp. 499–511, 2002.
[77] H. M. Coutinho, L. P. Acosta, H. W. Wu et al., “Th2 cytokinesare associated with persistent hepatic fibrosis in human Schis-tosoma japonicum infection,” Journal of Infectious Diseases,vol. 195, no. 2, pp. 288–295, 2007.
[78] S. Henri, C. Chevillard, A. Mergani et al., “Cytokineregulation of periportal fibrosis in humans infected withSchistosoma mansoni: IFN-γ is associated with protectionagainst fibrosis and TNF-α with aggravation of disease,”Journal of Immunology, vol. 169, no. 2, pp. 929–936, 2002.
[79] A. Dessein, B. Kouriba, C. Eboumbou et al., “Interleukin-13in the skin and interferon-γ in the liver are key players inimmune protection in human schistosomiasis,” Immunologi-cal Reviews, vol. 201, pp. 180–190, 2004.
[80] P. Smith, R. E. Fallon, N. E. Mangan et al., “Schistosomamansoni secretes a chemokine binding protein with antiin-flammatory activity,” Journal of Experimental Medicine, vol.202, no. 10, pp. 1319–1325, 2005.
[81] L. A. de Oliveira Fraga, E. W. Lamb, E. C. Moreno etal., “Rapid induction of IgE responses to a worm cysteineprotease during murine pre-patent schistosome infection,”BMC Immunology, vol. 11, article 56, 2010.
[82] M. Nyindo, T. M. Kariuki, P. W. Mola et al., “Role of adultworm antigen-specific immunoglobulin E in acquiredimmunity to Schistosoma mansoni infection in baboons,”Infection and Immunity, vol. 67, no. 2, pp. 636–642, 1999.
[83] P. Hagan, U. J. Blumenthal, D. Dunn, A. J. G. Simpson,and H. A. Wilkins, “Human IgE, IgG4 and resistance toreinfection with Schistosoma haematobium,” Nature, vol. 349,no. 6306, pp. 243–245, 1991.
[84] R. M. Maizels and M. Yazdanbakhsh, “Immune regulationby helminth parasites: cellular and molecular mechanisms,”Nature Reviews Immunology, vol. 3, no. 9, pp. 733–744, 2003.
[85] N. E. Mangan, R. E. Fallon, P. Smith, N. Van Rooijen, A.N. McKenzie, and P. G. Fallon, “Helminth infection protectsmice from anaphylaxis via IL-10-producing B cells,” Journalof Immunology, vol. 173, no. 10, pp. 6346–6356, 2004.
[86] N. E. Mangan, N. Van Rooijen, A. N. J. McKenzie, and P. G.Fallon, “Helminth-modified pulmonary immune responseprotects mice from allergen-induced airway hyperrespon-siveness,” Journal of Immunology, vol. 176, no. 1, pp. 138–147,2006.
[87] R. S. Curwen, P. D. Ashton, D. A. Johnston, and R. A. Wilson,“The Schistosoma mansoni soluble proteome: a comparisonacross four life-cycle stages,” Molecular and BiochemicalParasitology, vol. 138, no. 1, pp. 57–66, 2004.
[88] A. C. Fisher, “A study of the schistosomiasis of the Stanleyvilledistrict of the Belgian congo,” Transactions of the Royal Societyof Tropical Medicine and Hygiene, vol. 28, no. 3, pp. 277–IN1,1934.
[89] K. S. Warren, “Regulation of the prevalence and intensity ofschistosomiasis in man: immunology or ecology?” Journal ofInfectious Diseases, vol. 127, no. 5, pp. 595–609, 1973.
[90] A. E. Butterworth, M. Capron, and J. S. Cordingley, “Immu-nity after treatment of human Schistosomiasis mansoni. II.Identification of resistant individuals, and analysis of theirimmune responses,” Transactions of the Royal Society ofTropical Medicine and Hygiene, vol. 79, no. 3, pp. 393–408,1985.
[91] D. W. Dunne, A. J. Fulford, A. E. Butterworth, D. Koech,and J. H. Ouma, “Human antibody responses to Schistosomamansoni: does antigen directed, isotype restriction resultin the production of blocking antibodies?” Memorias doInstituto Oswaldo Cruz, vol. 82, supplement 4, pp. 101–104,1987.
[92] A. E. Butterworth, A. J. Fulford, D. W. Dunne, J. H. Ouma,and R. F. Sturrock, “Longitudinal studies on human schis-tosomiasis,” Philosophical transactions of the Royal Society ofLondon B, vol. 321, no. 1207, pp. 495–511, 1988.
[93] R. M. Anderson and R. M. May, “Herd immunity to helminthinfection and implications for parasite control,” Nature, vol.315, no. 6019, pp. 493–496, 1985.
[94] A. J. C. Fulford, A. E. Butterworth, R. F. Sturrock, and J. H.Ouma, “On the use of age-intensity data to detect immunityto parasitic infections, with special reference to Schistosomamansoni in Kenya,” Parasitology, vol. 105, no. 2, pp. 219–227,1992.
[95] M. E. J. Woolhouse, P. Taylor, D. Matanhire, and S. K.Chandiwana, “Acquired immunity and epidemiology ofSchistosoma haematobium,” Nature, vol. 351, no. 6329, pp.757–759, 1991.
[96] K. Marsh and R. W. Snow, “Host-parasite interaction andmorbidity in malaria endemic areas,” Philosophical Transac-tions of the Royal Society B, vol. 352, no. 1359, pp. 1385–1394,1997.
[97] M. E. J. Woolhouse, “Patterns in parasite epidemiology: thepeak shift,” Parasitology Today, vol. 14, no. 10, pp. 428–434,1998.
[98] F. Mutapi, P. D. Ndhlovu, P. Hagan, and M. E. J. Woolhouse,“A comparison of humoral responses to Schistosoma haema-tobium in areas with low and high levels of infection,” ParasiteImmunology, vol. 19, no. 6, pp. 255–263, 1997.
[99] F. Mutapi, G. Winborn, N. Midzi, M. Taylor, T. Mduluza,and R. M. Maizels, “Cytokine responses to Schistosomahaematobium in a Zimbabwean population: contrastingprofiles for IFN-γ, IL-4, IL-5 and IL-10 with age,” BMCInfectious Diseases, vol. 7, article 139, 2007.
[100] C. L. Black, P. N. Mwinzi, E. M. Muok et al., “Influence ofexposure history on the immunology and development ofresistance to human Schistosomiasis mansoni,” PLoS NeglectedTropical Diseases, vol. 4, no. 3, article e637, 2010.
[101] D. M. S. Karanja, A. W. Hightower, D. G. Colley et al.,“Resistance to reinfection with Schistosoma mansoni in occu-pationally exposed adults and effect of HIV-1 co-infection onsusceptibility to schistosomiasis: a longitudinal study,” TheLancet, vol. 360, no. 9333, pp. 592–596, 2002.
[102] M. Z. Satti, S. M. Sulaiman, M. M. A. Homeida, S. A. Younis,and H. W. Ghalib, “Clinical, parasitological and immunolog-ical features of canal cleaners hyper-exposed to Schistosomamansoni in the Sudan,” Clinical and Experimental Immunol-ogy, vol. 104, no. 3, pp. 426–431, 1996.
[103] A. J. C. Fulford, M. Webster, J. H. Ouma, G. Kimani, D. W.Dunne, and T. Fulford, “Puberty and age-related changes insusceptibility to schistosome infection,” Parasitology Today,vol. 14, no. 1, pp. 23–26, 1998.
[104] S. G. O. Johansson, T. Bieber, R. Dahl et al., “Revised nomen-clature for allergy for global use: report of the NomenclatureReview Committee of the World Allergy Organization,October 2003,” Journal of Allergy and Clinical Immunology,vol. 113, no. 5, pp. 832–836, 2004.
[105] M. Herr, L. Nikasinovic, C. Foucault et al., “Can early house-hold exposure influence the development of rhinitis symp-toms in infancy? Findings from the PARIS birth cohort,”

Journal of Parasitology Research 13
Annals of Allergy, Asthma and Immunology, vol. 107, no. 4,pp. 303–309, 2011.
[106] S. L. Prescott, “The influence of early environmental expo-sures on immune development and subsequent risk ofallergic disease,” Allergy, vol. 66, no. 95, pp. 4–6, 2011.
[107] J. M. Spergel and A. S. Paller, “Atopic dermatitis and theatopic march,” Journal of Allergy and Clinical Immunology,vol. 112, no. 6, supplement, pp. S118–S127, 2003.
[108] N. Bhattacharyya, J. Grebner, and N. G. Martinson, “Recur-rent acute rhinosinusitis: epidemiology and health care costburden,” Otolaryngology and Head and Neck Surgery. In press.
[109] R. Sporik, S. T. Holgate, and J. J. Cogswell, “Natural historyof asthma in childhood—a birth cohort study,” Archives ofDisease in Childhood, vol. 66, no. 9, pp. 1050–1053, 1991.
[110] M. L. Martinson, J. O. Teitler, and N. E. Reichman, “Healthacross the life span in the United States and England,”American Journal of Epidemiology, vol. 173, no. 8, pp. 858–865, 2011.
[111] C. Y. Hwang, Y. J. Chen, M. W. Lin et al., “Prevalence of atopicdermatitis, allergic rhinitis and asthma in Taiwan: a nationalstudy 2000 to 2007,” Acta Dermato-Venereologica, vol. 90, no.6, pp. 589–594, 2010.
[112] E. G. Weinberg, “The atopic march,” Current Allergy &Clinical Immunology, vol. 18, no. 1, pp. 4–5, 2005.
[113] G. Barberio, G. B. Pajno, D. Vita, L. Caminiti, G. W.Canonica, and G. Passalacqua, “Does a “reverse” atopicmarch exist?” Allergy, vol. 63, no. 12, pp. 1630–1632, 2008.
[114] M. D. Klinnert, H. S. Nelson, M. R. Price, A. D. Adinoff,D. Y. Leung, and D. A. Mrazek, “Onset and persistence ofchildhood asthma: predictors from infancy,” Pediatrics, vol.108, no. 4, p. E69, 2001.
[115] P. O. Van Asperen, A. S. Kemp, and A. Mukhi, “Atopyin infancy predicts the severity of bronchial hyperrespon-siveness in later childhood,” Journal of Allergy and ClinicalImmunology, vol. 85, no. 4, pp. 790–795, 1990.
[116] P. M. Matricardi, A. Bockelbrink, C. Gruber et al., “Longi-tudinal trends of total and allergen-specific IgE throughoutchildhood,” Allergy, vol. 64, no. 7, pp. 1093–1098, 2009.
[117] D. A. Mrazek, M. Klinnert, P. J. Mrazek et al., “Prediction ofearly-onset asthma in genetically at-risk children,” PediatricPulmonology, vol. 27, no. 2, pp. 85–94, 1999.
[118] P. G. Holt and D. H. Strickland, “Soothing signals: transpla-cental transmission of resistance to asthma and allergy,”Journal of Experimental Medicine, vol. 206, no. 13, pp. 2861–2864, 2009.
[119] B. Schaub, J. Liu, S. Hoppler et al., “Maternal farm exposuremodulates neonatal immune mechanisms through regula-tory T cells,” Journal of Allergy and Clinical Immunology, vol.123, no. 4, pp. 774.e5–782.e5, 2009.
[120] J. W. Hollingsworth, S. Maruoka, K. Boon et al., “Inutero supplementation with methyl donors enhances allergicairway disease in mice,” Journal of Clinical Investigation, vol.118, no. 10, pp. 3462–3469, 2008.
[121] K. Ishizaka and T. Ishizaka, “Physicochemical properties ofreaginic antibody. I. Association of reaginic activity with animmunoglobulin other than γA- or γG-globulin,” Journal ofAllergy, vol. 37, no. 3, pp. 169–185, 1966.
[122] K. Ishizaka and T. Ishizaka, “Identification of gamma-E-antibodies as a carrier of reaginic activity,” Journal ofImmunology, vol. 99, no. 6, pp. 1187–1198, 1967.
[123] E. Dehlink, B. Platzer, A. H. Baker et al., “A soluble formof the high affinity IgE receptor, Fc-epsilon-RI, circulates inhuman serum,” PLoS ONE, vol. 6, no. 4, Article ID e19098,2011.
[124] B. Platzer, E. Dehlink, S. J. Turley, and E. Fiebiger, “How toconnect an IgE-driven response with CTL activity?” CancerImmunol Immunother. In press.
[125] T. Bieber, H. De la Salle, A. Wollenberg et al., “Humanepidermal Langerhans cells express the high affinity receptorfor immunoglobulin E (FcεRI),” Journal of ExperimentalMedicine, vol. 175, no. 5, pp. 1285–1290, 1992.
[126] A. S. Gounni, B. Lamkhioued, E. Delaporte et al., “The high-affinity IgE receptor on eosinophils: from allergy to parasitesor from parasites to allergy?” Journal of Allergy and ClinicalImmunology, vol. 94, no. 6, part 2, pp. 1214–1216, 1994.
[127] A. S. Gounni, B. Lamkhioued, K. Ochiai et al., “High-affinityIgE receptor on eosinophils is involved in defence againstparasites,” Nature, vol. 367, no. 6459, pp. 183–186, 1994.
[128] U. Jeschke, D. Mayr, B. Schiessl et al., “Expression ofgalectin-1, -3 (gal-1, gal-3) and the thomsen-friedenreich(TF) antigen in normal, IUGR, preeclamptic and HELLPplacentas,” Placenta, vol. 28, no. 11-12, pp. 1165–1173, 2007.
[129] E. Rindsjo, M. Joerink, N. Papadogiannakis, and A.Scheynius, “IgE in the human placenta: why there?” Allergy,vol. 65, no. 5, pp. 554–560, 2010.
[130] M. Vernersson, M. Aveskogh, and L. Hellman, “Cloning ofIgE from the echidna (Tachyglossus aculeatus) and a compar-ative analysis of ε chains from all three extant mammalianlineages,” Developmental and Comparative Immunology, vol.28, no. 1, pp. 61–75, 2004.
[131] P. Vieira and K. Rajewsky, “The half-lives of serum immuno-globulins in adult mice,” European Journal of Immunology,vol. 18, no. 2, pp. 313–316, 1988.
[132] A. Karnowski, G. Achatz-Straussberger, C. Klockenbusch, G.Achatz, and M. C. Lamers, “Inefficient processing of mRNAfor the membrane form of IgE is a genetic mechanism tolimit recruitment of IgE-secreting cells,” European Journal ofImmunology, vol. 36, no. 7, pp. 1917–1925, 2006.
[133] P. Yu, M. Kosco-Vilbois, M. Richards, G. Kohler, and M. C.Lamers, “Negative feedback regulation of IgE synthesis bymurine CD23,” Nature, vol. 369, no. 6483, pp. 753–756, 1994.
[134] C. Plater-Zyberk and J. Y. Bonnefoy, “Marked ameliorationof established collagen-induced arthritis by treatment withantibodies to CD23 in vivo,” Nature Medicine, vol. 1, no. 8,pp. 781–785, 1995.
[135] J. C. Byrd, T. J. Kipps, I. W. Flinn et al., “Phase 1/2 study oflumiliximab combined with fludarabine, cyclophosphamide,and rituximab in patients with relapsed or refractory chroniclymphocytic leukemia,” Blood, vol. 115, no. 3, pp. 489–495,2010.
[136] N. Aberle, A. Gagro, S. Rabatic, Z. Reiner-Banovac, and D.Dekaris, “Expression of CD23 antigen and its ligands inchildren with intrinsic and extrinsic asthma,” Allergy, vol. 52,no. 12, pp. 1238–1242, 1997.
[137] J. P. Aubry, S. Pochon, P. Graber, K. U. Jansen, and J. Y.Bonnefoy, “CD21 is a ligand for CD23 and regulates IgEproduction,” Nature, vol. 358, no. 6386, pp. 505–507, 1992.
[138] J. J. Weis, T. F. Tedder, and D. T. Fearon, “Identificationof a 145,000 M(r) membrane protein as the C3d receptor(CR2) of human B lymphocytes,” Proceedings of the NationalAcademy of Sciences of the United States of America, vol. 81,no. 3, pp. 881–885, 1984.
[139] N. McCloskey, J. Hunt, R. L. Beavil et al., “Soluble CD23monomers inhibit and oligomers stimulate IGE synthesis inhuman B cells,” Journal of Biological Chemistry, vol. 282, no.33, pp. 24083–24091, 2007.
[140] F. X. Desvaux, G. Peltre, and B. David, “Characterization ofgrass pollen-specific IgE, IgA, IgM classes and IgG subclasses

14 Journal of Parasitology Research
in allergic patients,” International Archives of Allergy andApplied Immunology, vol. 89, no. 2-3, pp. 281–287, 1989.
[141] R. C. Aalberse, S. O. Stapel, J. Schuurman, and T. Rispens,“Immunoglobulin G4: an odd antibody,” Clinical and Exper-imental Allergy, vol. 39, no. 4, pp. 469–477, 2009.
[142] R. C. Aalberse, F. Van Milligen, K. Y. Tan, and S. O. Stapel,“Allergen-specific IgG4 in atopic disease,” Allergy, vol. 48, no.8, pp. 559–569, 1993.
[143] R. Hussain, R. W. Poindexter, and E. A. Ottesen, “Control ofallergic reactivity in human filariasis: predominant localiza-tion of blocking antibody to the IgG4 subclass,” Journal ofImmunology, vol. 148, no. 9, pp. 2731–2737, 1992.
[144] P. Rihet, C. E. Demeure, A. J. Dessein, and A. Bourgois,“Strong serum inhibition of specific IgE correlated to com-peting IgG4, revealed by a new methodology in subjects froma S. mansoni endemic area,” European Journal of Immunology,vol. 22, no. 8, pp. 2063–2070, 1992.
[145] F. Mutapi, C. Bourke, Y. Harcus et al., “Differential recog-nition patterns of Schistosoma haematobium adult wormantigens by the human antibodies IgA, IgE, IgG1 and IgG4,”Parasite Immunology, vol. 33, no. 3, pp. 181–192, 2011.
[146] R. C. Aalberse and J. Schuurman, “IgG4 breaking the rules,”Immunology, vol. 105, no. 1, pp. 9–19, 2002.
[147] M. V. D. N. Kolfschoten, J. Schuurman, M. Losen et al., “Anti-inflammatory activity of human IgG4 antibodies by dynamicFab arm exchange,” Science, vol. 317, no. 5844, pp. 1554–1557, 2007.
[148] J. S. van der Zee, P. Van Swieten, and R. C. Aalberse,“Inhibition of complement activation by IgG4 antibodies,”Clinical and Experimental Immunology, vol. 64, no. 2, pp.415–422, 1986.
[149] R. M. Maizels, E. Sartono, A. Kurniawan, F. Partono, M.E. Selkirk, and M. Yazdanbakhsh, “T-cell activation and thebalance of antibody isotypes in human lymphatic filariasis,”Parasitology Today, vol. 11, no. 2, pp. 50–56, 1995.
[150] T. Adjobimey and A. Hoerauf, “Induction of immunoglob-ulin G4 in human filariasis: an indicator of immunoregula-tion,” Annals of Tropical Medicine and Parasitology, vol. 104,no. 6, pp. 455–464, 2010.
[151] J. Punnonen, G. Aversa, B. G. Cocks et al., “Interleukin 13induces interleukin 4-independent IgG4 and IgE synthesisand CD23 expression by human B cells,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 90, no. 8, pp. 3730–3734, 1993.
[152] T. R. Mosmann, H. Cherwinski, and M. W. Bond, “Twotypes of murine helper T cell clone. I. Definition accordingto profiles of lymphokine activities and secreted proteins,”Journal of Immunology, vol. 136, no. 7, pp. 2348–2357, 1986.
[153] J. H. Lee, H. H. Yu, L. C. Wang, Y. H. Yang, Y. T. Lin, andB. L. Chiang, “The levels of CD4+CD25+ regulatory T cellsin paediatric patients with allergic rhinitis and bronchialasthma,” Clinical and Experimental Immunology, vol. 148, no.1, pp. 53–63, 2007.
[154] S. Dimeloe, A. Nanzer, K. Ryanna, and C. Hawrylowicz,“Regulatory T cells, inflammation and the allergic response-the role of glucocorticoids and Vitamin D,” Journal of SteroidBiochemistry and Molecular Biology, vol. 120, no. 2-3, pp. 86–95, 2010.
[155] M. Akdis, “Immune tolerance in allergy,” Current Opinion inImmunology, vol. 21, no. 6, pp. 700–707, 2009.
[156] A. Taylor, J. Verhagen, C. A. Akdis, and M. Akdis, “Tregulatory cells in allergy and health: a question of allergenspecificity and balance,” International Archives of Allergy andImmunology, vol. 135, no. 1, pp. 73–82, 2004.
[157] R. M. McLoughlin, A. Calatroni, C. M. Visness et al.,“Longitudinal relationship of early life immunomodulatoryT cell phenotype and function to development of allergicsensitization in an urban cohort,” Clinical and ExperimentalAllergy, vol. 42, no. 3, pp. 392–404, 2011.
[158] L. Cosmi, F. Liotta, E. Maggi, S. Romagnani, and F. Annunzi-ato, “Th17 cells: new players in asthma pathogenesis,” Allergy,vol. 66, no. 8, pp. 989–998, 2011.
[159] L. Cosmi, L. Maggi, V. Santarlasci et al., “Identification ofa novel subset of human circulating memory CD4+ T cellsthat produce both IL-17A and IL-4,” Journal of Allergy andClinical Immunology, vol. 125, no. 1, pp. 222.e4–230.e4, 2010.
[160] P. Jeannin, S. Lecoanet, Y. Delneste, J. F. Gauchat, and J. Y.Bonnefoy, “IgE versus IgG4 production can be differentiallyregulated by IL-10,” Journal of Immunology, vol. 160, no. 7,pp. 3555–3561, 1998.
[161] E. M. Savilahti, V. Rantanen, J. S. Lin et al., “Early recoveryfrom cow’s milk allergy is associated with decreasing IgE andincreasing IgG4 binding to cow’s milk epitopes,” Journal ofAllergy and Clinical Immunology, vol. 125, no. 6, pp. 1315.e9–1321.e9, 2010.
[162] M. E. Devey, D. V. Wilson, and A. W. Wheeler, “The IgGsubclasses of antibodies of grass pollen allergens produced inhay fever patients during hyposensitization,” Clinical Allergy,vol. 6, no. 3, pp. 227–236, 1976.
[163] R. J. Bullock, D. Barnett, and M. E. H. Howden, “Immuno-logic and clinical responses to parenteral immunother-apy in peanut anaphylaxis—a study using IgE and IgG4immunoblot monitoring,” Allergologia et Immunopathologia,vol. 33, no. 5, pp. 250–256, 2005.
[164] M. T. Gallego, V. Iraola, M. Himly et al., “Depigmentedand polymerised house dust mite allergoid: allergen content,induction of IgG4 and clinical response,” InternationalArchives of Allergy and Immunology, vol. 153, no. 1, pp. 61–69, 2010.
[165] A. Hoerauf, J. Satoguina, M. Saeftel, and S. Specht, “Immun-omodulation by filarial nematodes,” Parasite Immunology,vol. 27, no. 10-11, pp. 417–429, 2005.
[166] A. Kurniawan, M. Yazdanbakhsh, R. Van Ree et al., “Differ-ential expression of IgE and IgG4 specific antibody responsesin asymptomatic and chronic human filariasis,” Journal ofImmunology, vol. 150, no. 9, pp. 3941–3950, 1993.
[167] Y. Kaneko, F. Nimmerjahn, and J. V. Ravetch, “Anti-inflammatory activity of immunoglobulin G resulting fromFc sialylation,” Science, vol. 313, no. 5787, pp. 670–673, 2006.
[168] D. N. Mekhaiel, C. T. Daniel-Ribeiro, P. J. Cooper, andR. J. Pleass, “Do regulatory antibodies offer an alternativemechanism to explain the hygiene hypothesis?” Trends inParasitology, vol. 27, no. 12, pp. 523–529, 2011.
[169] T. H. T. Nguyen and T. B. Casale, “Immune modulation fortreatment of allergic disease,” Immunological Reviews, vol.242, no. 1, pp. 258–271, 2011.
[170] A. B. Kay, “T lymphocytes and their products in atopic allergyand asthma,” International Archives of Allergy and AppliedImmunology, vol. 94, no. 1–4, pp. 189–193, 1991.
[171] M. Jutel and C. A. Akdis, “T-cell subset regulation in atopy,”Current Allergy and Asthma Reports, vol. 11, no. 2, pp. 139–145, 2011.
[172] W. E. Paul and J. Zhu, “How are T(H)2-type immuneresponses initiated and amplified?” Nature Reviews Immunol-ogy, vol. 10, no. 4, pp. 225–235, 2010.
[173] C. M. Lloyd and E. M. Hessel, “Functions of T cells in asthma:more than just TH2 cells,” Nature Reviews Immunology, vol.10, no. 12, pp. 838–848, 2010.

Journal of Parasitology Research 15
[174] L. E. Harrington, R. D. Hatton, P. R. Mangan et al., “Inter-leukin 17-producing CD4+ effector T cells develop via alineage distinct from the T helper type 1 and 2 lineages,”Nature Immunology, vol. 6, no. 11, pp. 1123–1132, 2005.
[175] W. Al-Ramli, D. Prefontaine, F. Chouiali et al., “TH17-associated cytokines (IL-17A and IL-17F) in severe asthma,”Journal of Allergy and Clinical Immunology, vol. 123, no. 5,pp. 1185–1187, 2009.
[176] M. Veldhoen, C. Uyttenhove, J. van Snick et al., “Trans-forming growth factor-β “reprograms” the differentiation ofT helper 2 cells and promotes an interleukin 9-producingsubset,” Nature Immunology, vol. 9, no. 12, pp. 1341–1346,2008.
[177] R. Pawankar, S. Mori, C. Ozu, and S. Kimura, “Overview onthe pathomechanisms of allergic rhinitis,” Asia Pacific Allergy,vol. 1, no. 3, pp. 157–167, 2011.
[178] A. E. Butterworth, R. F. Sturrock, V. Houba, and P. H. Rees,“Antibody dependent cell mediated damage to schistosomulain vitro,” Nature, vol. 252, no. 5483, pp. 503–505, 1974.
[179] P. Hagan, P. J. Moore, and A. B. Adjukiewicz, “In-vitroantibody-dependent killing of schistosomula of Schistosomahaematobium by human eosinophils,” Parasite Immunology,vol. 7, no. 6, pp. 617–624, 1985.
[180] A. Capron, J. P. Dessaint, M. Capron, and H. Bazin, “SpecificIgE antibodies in immune adherence of normal macrophagesto Schistosoma mansoni schistosomules,” Nature, vol. 253, no.5491, pp. 474–475, 1975.
[181] A. Capron and J. P. Dessaint, “IgE: a molecule in search ofa function,” Annales d’Immunologie, vol. 132, no. 1, pp. 3–8,1981.
[182] C. Verwaerde, J. M. Grzych, H. Bazin, M. Capron, andA. Capron, “Production of monoclonal anti-Schistosomamansoni antibodies. Preliminary study of their biologicalactivities,” Comptes Rendus des Seances de l”Academie desSciences D, vol. 289, no. 10, pp. 725–727, 1979.
[183] P. Rihet, C. E. Demeure, A. Bourgois, A. Prata, and A.J. Dessein, “Evidence for an association between humanresistance to Schistosoma mansoni and high anti larval IgElevels,” European Journal of Immunology, vol. 21, no. 11, pp.2679–2686, 1991.
[184] D. W. Dunne, A. E. Butterworth, A. J. C. Fulford et al.,“Immunity after treatment of human schistosomiasis: asso-ciation between IgE antibodies to adult worm antigens andresistance to reinfection,” European Journal of Immunology,vol. 22, no. 6, pp. 1483–1494, 1992.
[185] I. R. Caldas, R. Correa-Oliveira, E. Colosimo et al., “Sus-ceptibility and resistance to Schistosoma mansoni reinfection:parallel cellular and isotypic immunologic assessment,”American Journal of Tropical Medicine and Hygiene, vol. 62,no. 1, pp. 57–64, 2000.
[186] Z. Zhang, H. Wu, S. Chen et al., “Association betweenIgE antibody against soluble egg antigen and resistance toreinfection with Schistosoma japonicum,” Transactions of theRoyal Society of Tropical Medicine and Hygiene, vol. 91, no. 5,pp. 606–608, 1997.
[187] M. Jiz, J. F. Friedman, T. Leenstra et al., “Immunoglobulin E(IgE) responses to paramyosin predict resistance to reinfec-tion with Schistosoma japonicum and are attenuated by IgG4,”Infection and Immunity, vol. 77, no. 5, pp. 2051–2058, 2009.
[188] C. W. A. Naus, C. J. Van Dam, P. G. Kremsner, F. W.Krijger, and A. M. Decider, “Human IgE, IgG subclass, andIgM responses to worm and egg antigens in Schistosomiasis
haematobium: a 12-month study of reinfection in Cameroo-nian children,” Clinical Infectious Diseases, vol. 26, no. 5, pp.1142–1147, 1998.
[189] A. P. de Moira, A. J. C. Fulford, N. B. Kabatereine, J. H. Ouma,M. Booth, and D. W. Dunne, “Analysis of complex patternsof human exposure and immunity to Schistosomiasis mansonithe influence of age, sex, ethnicity and IgE,” PLoS NeglectedTropical Diseases, vol. 4, no. 9, article e820, 2010.
[190] M. Z. Satti, P. Lind, B. J. Vennervald, S. M. Sulaiman, A. A.Daffalla, and H. W. Ghalib, “Specific immunoglobulin mea-surements related to exposure and resistance to Schistosomamansoni infection in Sudanese canal cleaners,” Clinical andExperimental Immunology, vol. 106, no. 1, pp. 45–54, 1996.
[191] F. Mutapi, T. Mduluza, N. Gomez-Escobar et al., “Immuno-epidemiology of human Schistosoma haematobium infection:preferential lgG3 antibody responsiveness to a recombinantantigen dependent on age and parasite burden,” BMCInfectious Diseases, vol. 6, article 96, 2006.
[192] F. Mutapi, P. D. Ndhlovu, P. Hagan et al., “Chemotherapyaccelerates the development of acquired immune responsesto Schistosoma haematobium infection,” Journal of InfectiousDiseases, vol. 178, no. 1, pp. 289–293, 1998.
[193] J. M. Grzych, D. Grezel, Chuan Bo Xu et al., “IgA antibodiesto a protective antigen in human Schistosomiasis mansoni,”Journal of Immunology, vol. 150, no. 2, pp. 527–535, 1993.
[194] P. N. M. Mwinzi, L. Ganley-Leal, C. L. Black, W. E. Secor,D. M. S. Karanja, and D. G. Colley, “Circulating CD23+ Bcell subset correlates with the development of resistance toSchistosoma mansoni reinfection in occupationally exposedadults who have undergone multiple treatments,” Journal ofInfectious Diseases, vol. 199, no. 2, pp. 272–279, 2009.
[195] S. R. Smithers and R. J. Terry, “Resistance to experimentalinfection with Schistosoma mansoni in rhesus monkeysinduced by the transfer of adult worms,” Transactions of theRoyal Society of Tropical Medicine and Hygiene, vol. 61, no. 4,pp. 517–533, 1967.
[196] C. J. Sanderson, A. O’Garra, D. J. Warren, and G. G. B. Klaus,“Eosinophil differentiation factor also has B-cell growthfactor activity: proposed name interleukin 4,” Proceedingsof the National Academy of Sciences of the United States ofAmerica, vol. 83, no. 2, pp. 437–440, 1986.
[197] C. J. Sanderson, D. J. Warren, and M. Strath, “Identificationof a lymphokine that stimulates eosinophil differentiationin vitro. Its relationship to interleukin 3, and functionalproperties of eosinophils produced in cultures,” Journal ofExperimental Medicine, vol. 162, no. 1, pp. 60–74, 1985.
[198] M. Veith, D. W. Taylor, and K. Thorne, “Studies on theenhancement of human eosinophil function by mononuclearcell products in vitro,” Clinical and Experimental Immunol-ogy, vol. 58, no. 3, pp. 603–610, 1984.
[199] P. Couissinier-Paris and A. J. Dessein, “Schistosoma-specifichelper T cell clones from subjects resistant to infectionby Schistosoma mansoni are Th0/2,” European Journal ofImmunology, vol. 25, no. 8, pp. 2295–2302, 1995.
[200] M. Roberts, A. E. Butterworth, G. Kimani et al., “Immu-nity after treatment of human schistosomiasis: associationbetween cellular responses and resistance to reinfection,”Infection and Immunity, vol. 61, no. 12, pp. 4984–4993, 1993.
[201] T. Mduluza, P. D. Ndhlovu, N. Midzi et al., “Contrastingcellular responses in Schistosoma haematobium infected andexposed individuals from areas of high and low transmissionin Zimbabwe,” Immunology Letters, vol. 88, no. 3, pp. 249–256, 2003.

16 Journal of Parasitology Research
[202] I. R. Viana, A. Sher, O. S. Carvalho et al., “Interferon-gammaproduction by peripheral blood mononuclear cells fromresidents of an area endemic for Schistosoma mansoni,” Trans-actions of the Royal Society of Tropical Medicine and Hygiene,vol. 88, no. 4, pp. 466–470, 1994.
[203] I. R. Caldas, A. C. Campi-Azevedo, L. F. A. Oliveira, A.M. S. Silveira, R. C. Oliveira, and G. Gazzinelli, “HumanSchistosomiasis mansoni: immune responses during acute andchronic phases of the infection,” Acta Tropica, vol. 108, no. 2-3, pp. 109–117, 2008.
[204] C. N. L. De Morais, J. R. De Souza, W. G. Melo et al.,“Cytokine profile associated with chronic and acute humanSchistosomiasis mansoni,” Memorias do Instituto OswaldoCruz, vol. 103, no. 6, pp. 561–568, 2008.
[205] G. Gazzinelli, J. R. Lambertucci, and N. Katz, “Immuneresponses during human Schistosomiasis mansoni. XI.Immunologic status of patients with acute infections andafter treatment,” Journal of Immunology, vol. 135, no. 3, pp.2121–2127, 1985.
[206] A. D. Bastos and I. L. Brito, “Acute pulmonary schisto-somiasis: HRCT findings and clinical presentation,” JornalBrasileiro de Pneumologia, vol. 37, no. 6, pp. 823–825, 2011.
[207] J. Clerinx, E. Bottieau, D. Wichmann, E. Tannich, and M.Van Esbroeck, “Acute schistosomiasis in a cluster of travelersfrom Rwanda: diagnostic contribution of schistosome DNAdetection in serum compared to parasitology and serology,”Journal of Travel Medicine, vol. 18, no. 6, pp. 367–372, 2011.
[208] A. W. Cheever, K. F. Hoffmann, and T. A. Wynn, “Immuno-pathology of Schistosomiasis mansoni in mice and men,”Immunology Today, vol. 21, no. 9, pp. 465–466, 2000.
[209] S. Ikemoto, T. Kishimoto, S. Wada, S. Nishio, and M.Maekawa, “Clinical studies on cell-mediated immunityin patients with urinary bladder carcinoma: blastogenicresponse, interleukin-2 production and interferon-γ produc-tion of lymphocytes,” British Journal of Urology, vol. 65, no.4, pp. 333–338, 1990.
[210] M. S. Wilson, M. M. Mentink-Kane, J. T. Pesce, T. R. Rama-lingam, R. Thompson, and T. A. Wynn, “Immunopathologyof schistosomiasis,” Immunology and Cell Biology, vol. 85, no.2, pp. 148–154, 2007.
[211] M. Bazaral, H. A. Orgel, and R. N. Hamburger, “Theinfluence of serum IgE levels of selected recipients, includingpatients with allergy, helminthiasis and tuberculosis, onthe apparent P-K titre of a reaginic serum,” Clinical andExperimental Immunology, vol. 14, no. 1, pp. 117–125, 1973.
[212] I. Hagel, N. R. Lynch, M. Perez, M. C. Di Prisco, R. Lopez,and E. Rojas, “Modulation of the allergic reactivity of slumchildren by helminthic infection,” Parasite Immunology, vol.15, no. 6, pp. 311–315, 1993.
[213] R. C. Godfrey and C. F. Gradidge, “Allergic sensitisationof human lung fragments prevented by saturation of IgEbinding sites,” Nature, vol. 259, no. 5543, pp. 484–486, 1976.
[214] E. Mitre, S. Norwood, and T. B. Nutman, “Saturation ofimmunoglobulin E (IgE) binding sites by polyclonal IgEdoes not explain the protective effect of helminth infectionsagainst atopy,” Infection and Immunity, vol. 73, no. 7, pp.4106–4111, 2005.
[215] D. I. Pritchard, D. S. W. Hooi, A. Brown, M. J. Bockarie, R.Caddick, and R. J. Quinnell, “Basophil competence duringhookworm (Necator americanus) infection,” American Jour-nal of Tropical Medicine and Hygiene, vol. 77, no. 5, pp. 860–865, 2007.
[216] S. J. Galli, “Mast cells and basophils,” Current Opinion inHematology, vol. 7, no. 1, pp. 32–39, 2000.
[217] M. Yazdanbakhsh, P. G. Kremsner, and R. Van Ree,“Immunology: allergy, parasites, and the hygiene hypothe-sis,” Science, vol. 296, no. 5567, pp. 490–494, 2002.
[218] H. C. Santiago, S. Bennuru, A. Boyd, M. Eberhard, and T.B. Nutman, “Structural and immunologic cross-reactivityamong filarial and mite tropomyosin: implications for thehygiene hypothesis,” Journal of Allergy and Clinical Immunol-ogy, vol. 127, no. 2, pp. 479–486, 2011.
[219] L. Caraballo and N. Acevedo, “Allergy in the tropics: theimpact of cross-reactivity between mites and ascaris,” Fron-tiers in Bioscience, vol. 3, pp. 51–64, 2011.
[220] N. R. Lynch, I. Hagel, M. Vargas et al., “Effect of age andhelminthic infection on IgE levels in slum children,” Journalof Investigational Allergology & Clinical Immunology, vol. 3,no. 2, pp. 96–99, 1993.
[221] N. R. Lynch, M. Palenque, I. Hagel, and M. C. Diprisco,“Clinical improvement of asthma after anthelminthic treat-ment in a tropical situation,” American Journal of Respiratoryand Critical Care Medicine, vol. 156, no. 1, pp. 50–54, 1997.
[222] A. M. J. van den Biggelaar, L. C. Rodrigues, R. Van Ree etal., “Long-term treatment of intestinal helminths increasesmite skin-test reactivity in Gabonese schoolchildren,” Journalof Infectious Diseases, vol. 189, no. 5, pp. 892–900, 2004.
[223] N. Rujeni, N. Nausch, C. D. Bourke et al., “Atopy is inverselyrelated to Schistosome infection intensity: a comparativestudy in zimbabwean villages with distinct levels of Schis-tosoma haematobium infection,” International Archives ofAllergy and Applied Immunology, vol. 158, no. 3, pp. 288–298,2012.
[224] C. J. Oliphant, J. L. Barlow, and A. N. McKenzie, “Insightsinto the initiation of type 2 immune responses,” Immunology,vol. 134, no. 4, pp. 378–385, 2011.
[225] R. M. Maizels, “Parasite immunomodulation and polymor-phisms of the immune system,” Journal of Biology, vol. 8, no.7, article 62, 2009.
[226] H. Kita and G. J. Gleich, “Eosinophils and IgE receptors: acontinuing controversy,” Blood, vol. 89, no. 10, pp. 3497–3501, 1997.
[227] M. I. A. S. Araujo, B. Hoppe, M. Medeiros et al., “ImpairedT helper 2 response to aeroallergen in helminth-infectedpatiente with asthma,” Journal of Infectious Diseases, vol. 190,no. 10, pp. 1797–1803, 2004.
[228] R. R. Oliveira, K. J. Gollob, J. P. Figueiredo et al., “Schistosomamansoni infection alters co-stimulatory molecule expressionand cell activation in asthma,” Microbes and Infection, vol. 11,no. 2, pp. 223–229, 2009.
[229] R. M. Maizels and M. Yazdanbakhsh, “T-cell regulation inhelminth parasite infections: implications for inflammatorydiseases,” Chemical Immunology and Allergy, vol. 94, pp. 112–123, 2008.
[230] I. Hagel, M. Cabrera, P. Sanchez, P. Rodrıguez, and J. J.Lattouf, “Role of the low affinity IgE receptor (CD23) onthe IgE response against Ascaris lumbricoides in WaraoAmerindian children from Venezuela,” Investigacion Clinica,vol. 47, no. 3, pp. 241–251, 2006.
[231] M. S. Wilson, M. D. Taylor, A. Balic, C. A. M. Finney,J. R. Lamb, and R. M. Maizels, “Suppression of allergicairway inflammation by helminth-induced regulatory Tcells,” Journal of Experimental Medicine, vol. 202, no. 9, pp.1199–1212, 2005.
[232] Y. Osada and T. Kanazawa, “Parasitic helminths: newweapons against immunological disorders,” Journal ofBiomedicine & Biotechnology, vol. 2010, Article ID 743758,p. 9, 2010.

Journal of Parasitology Research 17
[233] N. Nausch, N. Midzi, T. Mduluza, R. M. Maizels, andF. Mutapi, “Regulatory and activated T cells in humanSchistosoma haematobium infections,” PLoS ONE, vol. 6, no.2, Article ID e16860, 2011.
[234] W. Harnett and M. M. Harnett, “Helminth-derived immun-omodulators: can understanding the worm produce the pill?”Nature Reviews Immunology, vol. 10, no. 4, pp. 278–284,2010.
[235] A. J. Melendez, M. M. Harnett, P. N. Pushparaj et al.,“Inhibition of Fc epsilon RI-mediated mast cell responsesby ES-62, a product of parasitic filarial nematodes,” NatureMedicine, vol. 13, pp. 1375–1381, 2007.
[236] I. B. McInnes, B. P. Leung, M. Harnett, J. A. Gracie, F.Y. Liew, and W. Harnett, “A novel therapeutic approachtargeting articular inflammation using the filarial nematode-derived phosphorylcholine-containing glycoprotein ES-62,”The Journal of Immunology, vol. 171, no. 4, pp. 2127–2133,2003.
[237] M. M. Harnett, A. J. Melendez, and W. Harnett, “The thera-peutic potential of the filarial nematode-derived immunodu-lator, ES-62 in inflammatory disease,” Clinical & Experimen-tal Immunology, vol. 159, no. 3, pp. 256–267, 2010.
[238] W. Harnett, M. M. Harnett, B. P. Leung, J. A. Gracie,and I. B. McInnes, “The anti-inflammatory potential of thefilarial nematode secreted product, ES-62,” Current topics inMedicinal Chemistry, vol. 4, pp. 553–559, 2004.
[239] W. Harnett and M. M. Harnett, “Filarial nematode secretedproduct ES-62 is an anti-inflammatory agent: therapeuticpotential of small molecule derivatives and ES-62 peptidemimetics,” Clinical and Experimental Pharmacology & Physi-ology, vol. 33, no. 5-6, pp. 511–518, 2006.
[240] M. M. Harnett, D. E. Kean, A. Boitelle et al., “The phospho-rycholine moiety of the filarial nematode immunomodulatorES-62 is responsible for its anti-inflammatory action inarthritis,” Annals of the Rheumatic Diseases, vol. 67, no. 4, pp.518–523, 2008.
[241] G. Schramm, F. H. Falcone, A. Gronow et al., “Molecularcharacterization of an interleukin-4-inducing factor fromSchistosoma mansoni eggs,” The Journal of Biological Chem-istry, vol. 278, no. 20, pp. 18384–818392, 2003.
[242] M.-H. Abdulla, K.-C. Lim, J. H. McKerrow, and C. R.Caffrey, “Proteomic identification of IPSE/alpha-1 as a majorhepatotoxin secreted by Schistosoma mansoni eggs,” PLoSNeglected Tropical Diseases, vol. 5, no. 10, article e1368, 2011.
[243] G. Schramm, K. Mohrs, M. Wodrich et al., “Cutting edge:IPSE/alpha-1, a glycoprotein from Schistosoma mansonieggs, induces IgE-dependent, antigen-independent IL-4 pro-duction by murine basophils in vivo,” The Journal ofImmunology, vol. 178, no. 10, pp. 6023–6027, 2007.
[244] J. P. Hewitson, K. J. Filbey, J. R. Grainger et al., “Helig-mosomoides polygyrus elicits a dominant nonprotectiveantibody response directed against restricted glycan andpeptide epitopes,” The Journal of Immunology, vol. 187, no.9, pp. 4764–4777, 2011.
[245] J. Chen, X. Hu, S. He et al., “Expression and immuneresponse analysis of Schistosoma japonicum VAL-1, a homo-logue of vespid venom allergens,” Parasitology Research, vol.106, no. 6, pp. 1413–1418, 2010.
[246] N. W. Palm, R. K. Rosenstein, and R. Medzhitov, “Allergichost defences,” Nature, vol. 484, no. 7395, pp. 465–472, 2012.
[247] D. Artis, R. M. Maizels, and F. D. Finkelman, “Forum:immunology: allergy challenged,” Nature, vol. 484, no. 7395,pp. 458–459, 2012.
[248] P. W. Sherman, E. Holland, and J. S. Sherman, “Allergies:their role in cancer prevention,” Quarterly Review of Biology,vol. 83, no. 4, pp. 339–362, 2008.
[249] B. E. Zacharia and P. Sherman, “Atopy, helminths, andcancer,” Medical Hypotheses, vol. 60, no. 1, pp. 1–5, 2003.
[250] E. Sibanda, D. Gallerano, E. Wollmann, and R. Valenta,“EFIS-EJI African International Conference on Immunity(AICI),” European Journal of Immunology, vol. 42, no. 5, pp.1070–1071, 2012.

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2012, Article ID 796820, 8 pagesdoi:10.1155/2012/796820
Research Article
Risk Factors for Asthma in a Helminth EndemicArea in Bahia, Brazil
Luciana S. Cardoso,1, 2 Daniela M. Costa,1 Maria Cecılia F. Almeida,1 Robson P. Souza,1
Edgar M. Carvalho,1, 3, 4 Maria Ilma Araujo,1, 3, 4 and Ricardo R. Oliveira1, 5
1 Servico de Imunologia, Hospital Universitario Professor Edgard Santos, Universidade Federal da Bahia,40110-160 Salvador, BA, Brazil
2 Departamento de Ciencias da Vida, Universidade do Estado da Bahia, 41.150-000 Salvador, BA, Brazil3 Instituto Nacional de Ciencia e Tecnologia de Doencas Tropicais (INCT-DT/CNPq), 40110-160 Salvador, BA, Brazil4 Escola Bahiana de Medicina e Saude Publica, 40290-000 Salvador, BA, Brazil5 Faculdade de Farmacia, Universidade Federal da Bahia, 40.170-115 Salvador, BA, Brazil
Correspondence should be addressed to Ricardo R. Oliveira, [email protected]
Received 14 April 2012; Revised 16 June 2012; Accepted 5 July 2012
Academic Editor: William Harnett
Copyright © 2012 Luciana S. Cardoso et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Protective factors associated with atopy or asthma in rural areas include socioeconomic level, overcrowding, and helminthinfection. However, little epidemiological information was originated from schistosomiasis areas. This study aimed to investigatefactors associated with asthma in a schistosomiasis endemic area. A questionnaire was used to obtain information ondemographics, socioeconomic, and environmental features. The ISAAC questionnaire was used to identify individuals withasthma. Parasitological exam was done in all participants and skin prick test to aeroallergens in all asthmatics. Prevalence ofSchistosoma mansoni infection was 57.4% and Ascaris lumbricoides, 30.8%. Asthma was found in 13.1% of the population, and35.1% of them had a positive SPT. Active and passive smoking was positively associated with asthma, whereas A. lumbricoideswas negatively associated. In a schistosomiasis hyperendemic region, current infection with A. lumbricoides is protective againstasthma. However, we cannot rule out the involvement of S. mansoni infection in this process.
1. Introduction
Asthma is the most outstanding allergic disease especially indeveloped countries [1, 2]. However, in developing countriesthe frequency of asthma is much lower, particularly in ruralareas, where the prevalence of parasite infection is high[3–5]. Factors associated with protection against atopy inrural populations include reduced socioeconomic level, poorliving conditions, and increased overcrowding [6]. Moreover,several studies have shown a protective role of differentparasites in the development of asthma or atopy [6–10].
Studies conducted in Venezuela have shown that geo-helminth infections is associated with high levels of total IgEand low levels of allergen-specific IgE, as well as suppressionof allergic reactivity, which is reversible by anthelmintictreatment [11, 12]. Other authors have also shown low
prevalence of positive skin prick test (SPT) for aeroallergensin endemic areas for geohelminths [7, 13] or Schistosomaspp. [9, 14]. We have previously reported that asthmaticindividuals living in regions with high frequency of S.mansoni infection have a mild course of asthma [15], andthat treatment for schistosomiasis leads to a worsening of theclinical manifestations of asthma [3]. It is noteworthy thatin these previous studies conducted with S. mansoni infectedpatients, symptoms of asthma or frequency of positive SPTwas compared to individuals from outside schistosomiasisendemic areas.
The immunological mechanisms involved with protec-tion against the development of asthma are not well known,although it has been proposed the participation of regulatorymolecules [3, 14, 16–20]. Moreover, risk or protective factorsassociated with asthma in helminth endemic areas remain

2 Journal of Parasitology Research
still not well established. Despite a fair amount of epidemi-ological information is available on risk factors for asthmain developed countries, scant attention has been given torisk factors associated with asthma in rural communitiesfrom developing countries, especially in regions endemic forschistosomiasis.
We conducted a cross-sectional study in a rural areaendemic for helminths, including S. mansoni, to evaluatepossible risk and protective factors associated with the pres-ence of asthma. In addition to demographic, socioeconomicand environmental factors, we also evaluated the influenceof current S. mansoni, A lumbricoides, Trichuris trichiura,and hookworm infections with the presence of asthma inindividuals living in the region.
2. Material and Methods
2.1. Subjects and Endemic Area. This study was carried outat Agua Preta, a rural community in the district of Gandu,south of Bahia Brazil, 300 km distant from Salvador, thecapital of the state. This village is composed of about500 inhabitants, who live in poor sanitary conditions.Using a standard questionnaire, age, sex, income, housingconditions, and exposure to pollutants were registered.Additionally, information on water contact was obtainedindividually or from guardians in case of children under 10years old. The International Study of Asthma and Allergies inChildhood (ISAAC) questionnaire, which assess the personalhistory of bronchial asthma and rhinitis in the past 12months, as well as family history of atopy and concomitantpathologies, was applied to each individual aging from6 to 50 years old. In order to exclude individuals withchronic obstructive pulmonary disease (COPD), a clinicalevaluation, chest X-ray and spirometry were performed inall asthmatic individuals. None of the asthmatic individualsincluded in this study had COPD. Subjects who presentedpersonal history of asthma in the past 12 months accordingto ISAAC questionnaire underwent a skin prick test (SPT)for aeroallergens.
Interviews were carried out initially at the health post ofthe region, located at the center of Agua Preta. The recruit-ment strategy consisted in household visits to invite subjectsto the health post. During the last days of the recruitment,when the number of subjects who spontaneously went to thehealth post were lower, new household visits were done inorder to invite and perform a home-based interview for eachindividual who agreed in participate in this study.
The ethical Committee of the Maternity Climerio deOliveira, Federal University of Bahia, approved the presentstudy and informed consent was obtained from individualor their legal guardians. All participants who tested positivefor parasites were treated at the end of the study. Those whohad complaints of allergy were properly instructed regardingindoor environmental control and drug treatment.
2.2. Assessment of Water Contact. The water contact ques-tionnaire was developed based on previous observationscarried out on site about habits of the population regardingthe use of local rivers. Each participant was asked to provide
the frequency and duration of the exposure to the main sevenactivities (farming, bathing, washing clothes, washing hair,washing dishes, fishing, and playing). Subjects were classifiedacross all activities into four categories to reflect the level ofexposure: no exposure, low exposure (<1 h/week), mediumexposure (1–3 h/week), or high exposure (1–3 h/day) [21].
2.3. Fecal Examinations for Parasites. All participantsreceived a plastic container for fecal samples at three timepoints 2–30 days apart. Participants were instructed todeposit stool sample and return the container immediatelyto the collection point, where samples were stored at 4◦C.Each stool sample had a slide prepared and tested by usingthe Kato-Katz method to estimate the number of S. mansoni,A. lumbricoides and T. trichiura eggs per gram of feces (EPG)[22]. Additionally, the Hoffmann-Pons-Janer method wasused to qualitatively investigate the presence of Hookworminfection [23].
2.4. Skin Prick Test. SPTs were performed on all individualsidentified as asthmatic according to the ISAAC criteria.Glycerinated allergens tested included Dermatophagoidespteronyssinus, D. farinae, Blomia tropicalis, Periplaneta Amer-icana, and Blatella germanica (IPI-ASAC). We also usedhistamine (1 : 1000) and saline as positive and negativecontrols, respectively. SPT results were obtained 20 minutesafter application, and a positive skin reaction was defined asa wheal with a mean diameter greater than 3 mm.
2.5. Statistical Analyses. The variable age are expressed asarithmetic mean and standard deviation (SD), whereasparasite load are expressed as geometric mean and 95% ofconfidence interval. Helminth infections were classified intolow, moderate, or high intensity of infection according toWorld Health Organization (WHO) criteria [24]. Parasiteload ranging from 1 to 99 epg for S. mansoni is classifiedas low, 100 to 300 epg moderate, and equal or greater than400 epg high intensity of infection. For A. lumbricoides lowintensity of infection is defined as 1 to 4,999 epg, moderate5,000 to 49,999 epg, and high intensity of infection is equalor greater than 50,000 epg. Light T. trichiura infection isconsidered as parasite load ranging from 1 to 999 epg,moderate 1,000 to 9,999, and high intensity of infectionequal or greater than 10,000 epg. The intensity of hookworminfection was not assessed since the Kato-Katz technique isnot adequate for quantifying hookworm eggs.
Statistical analyses were performed by using the STATAstatistical package version 11.2 (Stata Corp., College Station,TX). A logistic regression model was used to test associ-ation between asthma and covariates in a univariate andmultivariate way. The alpha level for statistical significancewas established as 0.05 for all analyses and odds ratio(OR) was obtained at a 95% of confidence interval (CI).In order to reduce the chance of type I error a P valueadjustment was performed by the Bonferroni correctionin all significant associations. Multivariate analyses wereadjusted for age, gender, number of stool samples evaluated,and/or smoking status. Adjustment for age and gender wasperformed because these could be possible confounding

Journal of Parasitology Research 3
factors, since depending on gender or age lifestyle couldbe significantly different. The adjustment for number ofstool samples analyzed was done because 82.8% of subjectswho had three samples evaluated were asthmatics, and itis well known that the Kato-Katz sensitivity is influencedby the number of samples evaluated, reaching a sensitivityof 91.7% for the diagnosis of schistosomiasis when foursamples are analyzed [25]. For investigating the influenceof helminth infections on asthma, the smoking status wastaken into account since this was positively associated withasthma in this region, which could be responsible for theunderestimation of the real effect that helminth infectionshave on asthma.
3. Results
3.1. Baseline Characteristics of the Studied Subjects. A totalof 427 individuals were included in this study, being 53.2%male. The mean age was 26.9 ± 19.0 years, ranging from 1to 92 years. Approximately 95% of participants reported anaverage income less than the Brazilian national minimumwage (≤$250.00) per month. Regarding the presence ofpollutants 94.4% of the population uses wood burning stoveand 14.5% were active smokers.
The frequency of intestinal parasites was investigated in406 (95.1%) individuals, 214 (52.7%) of whom had onlyone sample analyzed, whereas 160 (39.4%) and 32 (7.9%)subjects had two and three samples evaluated, respectively.The helminth most frequently identified in the region was S.mansoni, affecting 57.4% of the population, followed by T.trichiura (36.9%), hookworm (31.8%), and A. lumbricoides(30.8%). Intensity of infection was assessed for S. mansoni(89 [75–105] epg), A. lumbricoides (1,946 [1,278–2,963]epg), and T. trichiura (120 [97–149] epg).
History of exposure to contaminated water was reportedby 332 (77.8%) subjects, 34.3% of whom had a low level ofexposure, 18.7% medium, and 47.0% were highly exposed.The group highly exposed was composed mainly of female(67.9%), whereas the group with low level of exposure wasrepresented mostly by men (68.4%). Despite the evidentinfluence of gender on the intensity of exposure, age is afactor that apparently did not affect the level of exposure.The group classified as highly exposed had a mean age of27 ± 17 years, while the groups of medium and low level ofexposure had a mean age of 26± 18 and 27± 20 (P > 0.05),respectively. As expected, the group that reported higher levelof exposure also showed higher frequency of schistosomiasis,when compared to the nonexposed group (Table 1).
The prevalence of asthma and rhinitis was evaluated bythe ISAAC questionnaire in 335 individuals, representing allsubjects who were 6 to 50 years old. The prevalence of self-reported wheezing in the past 12 months (here designated as“asthma”) was 13.1%. Skin prick test for aeroallergens wasperformed on 37 out of 44 (84.1%) asthmatic individuals.False positive result, defined as presence of skin reaction inthe negative control saline, was found in only one subject(2.3%). On the other hand, false negative result, definedas no skin reaction detected, even to histamine, was foundin four (9.1%) asthmatic individuals. Among those 32
individuals who had a validated skin prick test result, 13(35.1%) was positive for at least one allergen, whereas 19(64.9%) of them had a negative SPT result.
3.2. Risk Factors Associated with Asthma. Univariate andmultivariate analysis for the association between asthma andpossible risk or protector factors are presented in Table 2.Evaluated variables included gender, age, income, passive oractive smoking, family history of allergy, housing quality,number of people per household, use of wood burningstoves, and level of exposure to fresh water. Multivariateanalyses were adjusted for age and gender.
The frequency of asthmatic individuals living in theendemic area who are active smokers was higher (26.2%)than the prevalence of active smokers among those nonasth-matic subjects (11.8%). In order to obtain the power of thisdifference, we performed a sample size calculation based onthese data and found that 42 individuals in the “Asthmatic”group and 272 in the “nonasthmatic” group have 76.1%power to detect a difference with a significance alpha levelof 0.05.
Only active or passive smoking was positively associatedwith the presence of personal history of asthma in the past12 months, even after adjustment for confounding factors(Table 2). After controlling for age and gender the prevalenceof asthma was 5.45 (CI 95%: 2.09–14.24; P = 0.001) and 3.67(CI 95%: 1.83–7.34; P < 0.001) times higher among activeand passive smokers, respectively, than nonsmokers.
3.3. Association between Asthma and Helminth Infections.The association between helminth infection or intensity ofinfection and asthma is shown in Table 3. Univariate analysisindicates that hookworm infection (OR = 2.54 [1.32–4.91];P = 0.005), moderate intensity of A. lumbricoides infection(OR = 4.01 [1.74–9.28]; P = 0.001), T. trichiura (OR = 2.18[1.13–4.20]; P = 0.020), and S. mansoni (OR = 2.89 [1.29–6.48]; P = 0.010) infection were positively associated withasthma. However when adjusting for the confounding factorsage, gender, number of stool samples evaluated, and smokingstatus, no significant association was observed betweenhookworm (OR = 1.41 [0.54–3.72]; P = 0.486), T. trichiura(OR = 0.95 [0.36–2.54]; P = 0.918), S. mansoni (OR = 1.44[0.48–4.29]; P = 0.517), or any helminth infection (OR= 0.94 [0.19–4.56]; P = 0.935) and asthma. Moreover,no significant association was found between number ofhelminth infections and asthma (data not shown).
Multivariate analysis showed that A. lumbricoides infec-tion is negatively associated with asthma (OR = 0.26 [0.07–0.94]; P = 0.041). When the Bonferroni correction was per-formed this association became nonsignificant (P = 0.984).Nevertheless, we found a significant association betweenA. lumbricoides infection and asthma when controlling forother helminth infections (data not shown). The associationbetween asthma and parasite load was also assessed andwe found that low (OR = 0.27 [0.07–0.94] P = 0.071) ormoderate (OR = 0.29 [0.05–1.83]; P = 0.187) intensity ofA. lumbricoides infection was not associated with asthma.Since only three individuals, all nonasthmatic, showed highintensity of A. lumbricoides infection in the region, we were

4 Journal of Parasitology Research
Table 1: Frequency of S. mansoni infection according to the level of exposure.
S. mansoni Univariate analysis Multivariate analysis
Positive Negative OR (95% CI) P OR (95% CI) P
Level of exposure
No contact 26 (29.5%) 62 (70.5%) 1.00 1.00
Low 62 (55.9%) 49 (44.1%) 2.18 (1.13−4.22) 0.021 2.56 (1.22−5.34) 0.013
Medium 38 (67.9%) 18 (32.1%) 3.17 (1.41−7.15) 0.005 2.67 (1.11−6.42) 0.028
High 107 (70.9%) 44 (29.1%) 4.00 (2.11−7.61) <0.001 3.64 (1.81−7.29) <0.001
Note: Multivariate analysis adjusted by age, gender, and number of stool samples analyzed.
Table 2: Univariate and multivariate analysis for the association between asthma and possible risk or protector factors.
Nonasthmatic Asthmatic Univariate analysis Multivariate analysis
(n = 291) (n = 44) OR (95% CI) P OR (95% CI) P
Gender
Female 141 (85.4%) 24 (14.6%) 1.00
Male 150 (88.2%) 20 (11.8%) 0.78 (0.41–1.48) 0.452
Age (years)
6–10 44 (83.0%) 9 (17.0%) 1.00
11–15 48 (81.4%) 11 (18.6%) 1.12 (0.42–2.96) 0.819
16–20 41 (91.1%) 4 (8.9%) 0.48 (0.14–1.67) 0.247
21–30 82 (88.2%) 11 (11.8%) 0.66 (0.25–1.70) 0.386
31–40 43 (89.6%) 5 (10.4%) 0.57 (0.18–1.83) 0.345
41–50 33 (89.2%) 4 (10.8%) 0.59 (0.17–2.09) 0.416
Income ($)
<250 271 (86.9%) 41 (13.1%) 1.00 1.00
250–500 19 (86.4%) 3 (13.6%) 1.04 (0.30–3.68) 0.947 1.14 (0.31–4.17) 0.847
>500 0 0 — — — —
Active smoker
No 240 (88.6%) 31 (11.4%) 1.00 1.00
Yes 32 (74.4%) 11 (25.6%) 2.66 (1.22–5.81) 0.014 5.45 (2.09–14.24) 0.001
Passive smoker
No 190 (92.7%) 15 (7.3%) 1.00 1.00
Yes 97 (78.2%) 27 (21.2%) 3.53 (1.79–6.94) <0.001 3.67 (1.83–7.34) <0.001
Family history of allergy
No 180 (87.0%) 27 (13.0%) 1.00 1.00
Yes 65 (84.4%) 12 (15.6%) 1.23 (0.59–2.57) 0.581 1.29 (0.60–2.77) 0.508
Housing quality
Brick house 103 (92.0%) 9 (8.0%) 1.00 1.00
Adobe house 107 (84.3%) 20 (15.7%) 2.14 (0.93–4.92) 0.073 2.03 (0.88–4.72) 0.099
Mud house 48 (87.3%) 7 (12.7%) 1.67 (0.59–4.77) 0.337 1.77 (0.61–5.08) 0.290
Number of inhabitants
1–3 95 (87.2%) 14 (12.8%) 1.00 1.00
4–6 148 (88.1%) 20 (11.9%) 0.92 (0.44–1.90) 0.816 0.76 (0.35–1.64) 0.485
>6 43 (81.1%) 10 (18.9%) 1.58 (0.65–3.83) 0.314 1.40 (0.56–3.52) 0.475
Wood burning stove
No 19 (95.0%) 1 (5.0%) 1.00 1.00
Yes 271 (86.3%) 43 (13.7%) 3.01 (0.39–23.1) 0.288 2.83 (0.37–21.88) 0.319
Exposure to fresh water
No contact 57 (87.7%) 8 (12.3%) 1.00 1.00
Low 86 (93.5%) 6 (6.5%) 0.50 (0.16–1.51) 0.217 0.48 (0.15–1.50) 0.207
Medium 41 (85.4%) 7 (14.6%) 1.22 (0.41–3.62) 0.725 1.26 (0.42–3.81) 0.684
High 107 (82.3%) 23 (17.7%) 1.53 (0.64–3.64) 0.335 1.60 (0.66–3.87) 0.293
Note: Multivariate analysis adjusted by age and gender.

Journal of Parasitology Research 5
Table 3: Univariate and multivariate analysis of the association between asthma and helminth infections.
Nonasthmatic(n = 291)
Asthmatic(n = 42)
Univariate analysis Multivariate analysis
33% 45% OR (95% CI) P OR (95% CI) P
Hookworm
Negative 189(90.9%) 19 (9.1%) 1.00 1.00
Positive 90 (79.6%) 23 (20.4%) 2.54 (1.32–4.91) 0.005 1.41 (0.54–3.72) 0.486
A. lumbricoides
Negative 187 (89.0%) 23 (11.0%) 1.00 1.00
Positive 92 (82.9%) 19 (17.1%) 1.68 (0.87–3.24) 0.122 0.26 (0.07–0.94) 0.041
Intensity (epg)
0 193 (89.4%) 23 (10.6%) 1.00 1.00
1–4999 60 (88.2%) 8 (11.8%) 1.12 (0.48–2.63) 0.797 0.27 (0.07–1.12) 0.071
5000–49999 23 (67.6%) 11 (32.4%) 4.01 (1.74–9.28) 0.001 0.29 (0.05–1.83) 0.187
≥50000 3 (100%) 0 — — — —
T. trichiura
Negative 173 (90.6%) 18 (9.4%) 1.00 1.00
Positive 106 (81.5%) 24 (18.5%) 2.18 (1.13–4.20) 0.020 0.95 (0.36–2.54) 0.918
Intensity (epg)
0 175 (90.7%) 18 (9.3%) 1.00 1.00
1–999 96 (80.7%) 23 (19.3%) 2.33 (1.20–4.53) 0.013 1.02 (0.38–2.74) 0.968
1000–9999 7 (87.5%) 1 (12.5%) 1.39 (1.61–11.9) 0.765 0.30 (0.01–8.03) 0.474
≥10000 1 (100%) 0 — — — —
S. mansoni
Negative 113 (93.4%) 8 (6.6%) 1.00 1.00
Positive 166 (83.0%) 34 (17.0%) 2.89 (1.29–6.48) 0.010 1.44 (0.48–4.29) 0.517
Intensity (epg)
0 114 (93.4%) 8 (6.6%) 1.00 1.00
1–99 104 (86.7%) 16 (13.3%) 2.19 (0.90–5.33) 0.084 1.48 (0.45–4.84) 0.520
100–399 34 (73.9%) 12 (26.1%) 5.03 (1.90–13.3) 0.001 3.21 (0.76–13.63) 0.114
≥400 27 (81.8%) 6 (18.2%) 3.17 (1.01–9.89) 0.047 0.69 (0.10–4.82) 0.706
Any helminth
Negative 49 (94.2%) 3 (5.8%) 1.00 1.00
Positive 230 (85.5%) 39 (14.5%) 2.77 (0.82–9.33) 0.100 0.94 (0.19–4.56) 0.935
Note: Multivariate analysis adjusted by age, gender, number of stool samples analyzed, and smoking status.
not able to test the association between high ascariasisparasite load and asthma.
4. Discussion
This study assessed possible risk or protective factors associ-ated with presence of asthma in a population living in a ruralpoor area of Bahia, Brazil. Our results showed that the mainrisk factor associated with presence of asthma is smoking. Wefound no association between socioeconomic variables andthe development of asthma. Additionally, we demonstratedthat current A. lumbricoides infection is associated withprotection against asthma when adjusting for confoundingfactors.
The cross-sectional design, the use of questionnaires toaccess information on the presence of asthma, and risk
factors were the major limitations of this study. The studydesign did not allow us to make causal inferences, andconfounding factors may not be equally distributed betweengroups. However, we performed statistical analysis takinginto account the confounding factors, and reverse causalityis not possible for most of the risk factors evaluated. We arealso aware that the use of questionnaires makes the studyopen to information bias since it depends on the interviewedresponse. Therefore, misclassification of exposure may haveoccurred in the present study. Also, we call attention thatwe did not evaluate past helminth infections and that theparasitological technique used here is not sensitive for verylow parasite burden.
The differentiation between asthma and COPD was oneof our major concerns when planning this study. One wayto reduce this possible misdiagnose was the exclusion of

6 Journal of Parasitology Research
individuals over 50 years of age. Many authors have reportedthat COPD rarely presents clinically before the 5th decadeof life and that the prevalence of COPD occurs primarilyin smokers over 40 years of age [26, 27]. According to thePLATINO study the prevalence of COPD in individuals agingfrom 40 to 49 years in a metropolitan area of Brazil is 8.4%[28]. In our study only 4 (9%) asthmatic individuals agedbetween 41 and 50 years old. Therefore, 91% of subjectsincluded in this study were under 41 years old. Moreover,only 1 out of 4 (25%) asthmatic individual over 40 years ofage was active smoker.
Although we did not observe association between socioe-conomic variables and asthma, other authors have demon-strated that reduced socioeconomic level and overcrowdingare associated with protection against atopy in a rural region[6]. This phenomenon was probably not detected in ourstudy because the overall population was homogeneous inregard to socioeconomic level, being identified only subjectswith an average income less than $500 per month. Addi-tionally, several other studies have showed an associationbetween smoking and risk of asthma, which is consistentwith our data [29–32]. Even though this association is wellknown, its interpretation must be made cautiously, especiallywhen using a questionnaire-based diagnosis of asthma.Because smokers have been reported to have more severeasthma than nonsmokers, it is expected that the use of self-reported questionnaires, such as the ISAAC questionnaire,may overestimate the risk of asthma among smokers [33].However, this bias probably did not interfere in our studysince it has been shown that individuals from endemicareas for schistosomiasis have mild asthma [15]. In order toevaluate the effect of helminth infections in the presence ofasthma statistical analyses were adjusted for smoking status,given that this is an independent determinant factor forasthma.
In the last years researchers showed an increased inter-est in evaluating the role of helminth infections in thedevelopment of allergic diseases. Although several studiesshow that in endemic areas for helminths, infection with A.lumbricoides or other helminths has a negative associationwith atopy, possibly acting as a protective factor against thedevelopment of asthma, none of these studies was conductedin endemic area for schistosomiasis [6–8, 12, 34]. Studiescarried out with individuals from endemic areas infectedwith S. mansoni have showed low reactivity to the skinprick test (SPT) to aeroallergens and fewer symptoms ofasthma compared to asthmatics without infection [10, 15],and an inverse correlation between SPT and presence ofinfection [9]. It is worth noting that none of these previousstudies evaluated the association between SPT or symptomsof asthma and current S. mansoni infection within asthmaticsubjects living in the same region. The prevalence of positiveSPT to aeroallergens in asthmatic individuals included inthis study was 35.1%, which is far below what is found inurban regions from Brazil [10, 35, 36]. Nevertheless, wefound no significant difference in the frequency of positiveSPT among asthmatics currently infected or not by anyhelminth (data not shown). Despite the frequency of positiveskin test has been low, asthmatic subjects from these regions
probably have atopic asthma, demonstrated by the presenceof aeroallergen-specific IgE [10].
The presence of asthma was not associated with currentinfection by S. mansoni in the studied population. However,the prevalence of asthma in the site was only 13.1%, whichis much lower than the frequency observed in adolescents of13 and 14 years old from urban areas of Salvador (24.6%),Feira de Santana (21.5%) or Vitoria da Conquista (30.5%),Bahia, when using the same criteria for defining asthma [5].The prevalence of asthma was representative of the entirestudy population, including individuals from 6 to 50 yearsold. However, when analyzing only the age of 13 and 14years of age, the prevalence was 15%, which is very closeto the frequency observed in the general population in theendemic area and still far from that observed in other centersevaluated in Bahia, Brazil [5]. This is in agreement withother study conducted in different regions of Brazil, whichshowed lower prevalence of asthma and rhinitis in rural thanin urban areas [4].
Thus, the presence of a protective factor for the devel-opment of asthma in an endemic community for helminthsincluding schistosomiasis is evident, which could not beexplained only by the presence of current S. mansoni infec-tion. The fact that these individuals inhabit a region of highendemicity, constantly exposed to S. mansoni reinfection,might be responsible for the low prevalence of asthmaobserved on site, with no significant difference in thefrequency of asthma among currently infected or not. On theother hand, we found in this schistosomiasis endemic areathat individuals currently infected with A. lumbricoides havea lower prevalence of asthma when compared to noninfectedsubjects, which was not observed for the presence of T.trichiura, hookworm, any helminth infection, or even fordifferent intensity of infection. Although this associationhas been lost when performing the Bonferroni correction,it is well established that reducing type I error by P valueadjustments increases the probability of type II error forthose association that are not null. The formal premise forsuch adjustments is the much wider hypothesis that thereis no association between any variables under observation,and that only random processes govern the variability of allobservations. This “universal” null hypothesis presumes thatall observed associations reflect only random variation thatcould be obtained particularly in empiric situations [37, 38].Once this study evaluated associations that are not empiric,but instead evidence-based, such as the association betweenA. lumbricoides infection and asthma, we are confident thatthis association was not due to random variation, andtherefore it would be better to take the risk of making typeI error and call attention to a possible beneficial associationfor asthma.
Studies conducted in urban areas in Brazil have showedcontroversial results for the association between A. lumbri-coides infection and atopy [8, 39]. Although no associationbetween SPT response and A. lumbricoides infection wasfound in asthmatic individuals [39], a recent study showedthat the presence of A. lumbricoides infection is able to reducethe prevalence of positive SPT response but do not affectthe prevalence of asthma [8]. Overall, helminth infection is

Journal of Parasitology Research 7
associated with reduced risk of asthma or atopy in regionswith high frequency of parasite infections [7, 11, 13], whereasin areas with low endemicity, A. lumbricoides infection isassociated with increased risk of atopy and asthma [40,41]. Although A. lumbricoides is a recognized cause oftropical pulmonary eosinophilia, chronic infection induces aregulatory immune response which includes interleukin-10-and transforming growth factor-β-secreting cells [42, 43].In addition to the suppression of allergic inflammation,activation of the regulatory immune response induced byhelminths is responsible for preventing the elimination ofparasites and protects the host from damage that could becaused by excessive inflammatory response [44]. Our find-ings support the hypothesis that exposure to A. lumbricoidesinduces a generalized suppression on the immune response,which seems to be able to reduce the risk of asthma withoutadditive effect by helminth coinfection. This effect was notobserved for other helminth infections probably because A.lumbricoides was the less frequently helminth found in theregion, which results in less exposure and lower rates ofreinfection, allowing thereby the detection of differences inasthma prevalence between individuals currently infected ornot.
In conclusion, our findings indicate that smoking isthe major risk factors associated with asthma in a ruralpopulation endemic for schistosomiasis. However, in ruralendemic areas for helminth infections the prevalence ofasthma is much lower than what is observed in urbanregions, and A. lumbricoides infection is negatively associatedwith the presence of asthma within the population. Althoughwe were unable to show a protective association betweencurrent S. mansoni infection and asthma, we cannot rule outthe possible participation of S. mansoni in modulating theimmune response of allergic diseases, probably because thisis a hyperendemic region where individuals are constantlyreinfected. This study contribute to a better understandingof the role of helminth infections in allergies.
Conflict of Interests
The authors have no conflict of interests concerning the workreported in this paper.
Acknowledgments
The authors thank Leda Maria Alcantara for the collabora-tion in reading parasitological slides; all individuals from theregion of Agua Preta-Gandu, Bahia, Brazil, for participatingin the study; the Health Agent Irene de Jesus for collaboratingin the field work.
References
[1] R. Beasley, U. Keil, E. Von Mutius, and N. Pearce, “Worldwidevariation in prevalence of symptoms of asthma, allergicrhinoconjunctivitis, and atopic eczema: ISAAC,” The Lancet,vol. 351, no. 9111, pp. 1225–1232, 1998.
[2] M. I. Asher, “Worldwide variations in the prevalence of asthmasymptoms: the International Study of Asthma and Allergies
in Childhood (ISAAC),” European Respiratory Journal, vol. 12,no. 2, pp. 315–335, 1998.
[3] M. I. A. S. Araujo, B. Hoppe, M. Medeiros et al., “ImpairedT helper 2 response to aeroallergen in helminth-infectedpatiente with asthma,” Journal of Infectious Diseases, vol. 190,no. 10, pp. 1797–1803, 2004.
[4] D. Sole, V. E. Cassol, A. R. Silva et al., “Prevalence of symptomsof asthma, rhinitis, and atopic eczema among adolescentsliving in urban and rural areas in different regions of Brazil,”Allergologia et Immunopathologia, vol. 35, no. 6, pp. 248–253,2007.
[5] D. Sole, G. F. Wandalsen, I. C. Camelo-Nunes et al., “Preva-lence of symptoms of asthma, rhinitis, and atopic eczemaamong Brazilian children and adolescents identified by theInternational Study of Asthma and Allergies in Childhood(ISAAC)—Phase 3,” Jornal de Pediatria, vol. 82, no. 5, pp. 341–346, 2006.
[6] P. J. Cooper, M. E. Chico, L. C. Rodrigues et al., “Risk factorsfor atopy among school children in a rural area of LatinAmerica,” Clinical and Experimental Allergy, vol. 34, no. 6, pp.845–852, 2004.
[7] P. J. Cooper, M. E. Chico, L. C. Rodrigues et al., “Reducedrisk of atopy among school-age children infected with geo-helminth parasites in a rural area of the tropics,” Journal ofAllergy and Clinical Immunology, vol. 111, no. 5, pp. 995–1000,2003.
[8] N. M. Alcantara-Neves, R. V. Veiga, V. C. C. Dattoli et al., “Theeffect of single and multiple infections on atopy and wheezingin children,” Journal of Allergy and Clinical Immunology, vol.129, no. 2, pp. 359.e1–367.e3, 2012.
[9] M. I. Araujo, A. A. Lopes, M. Medeiros et al., “Inverseassociation between skin response to aeroallergens and Schis-tosoma mansoni infection,” International Archives of Allergyand Immunology, vol. 123, no. 2, pp. 145–148, 2000.
[10] M. Medeiros, M. C. Almeida, J. P. Figueiredo et al., “Lowfrequency of positive skin tests in asthmatic patients infectedwith Schistosoma mansoni exposed to high levels of miteallergens,” Pediatric Allergy and Immunology, vol. 15, no. 2, pp.142–147, 2004.
[11] N. R. Lynch, I. Hagel, M. Perez, M. C. Di Prisco, R. Lopez, andN. Alvarez, “Effect of anthelmintic treatment on the allergicreactivity of children in a tropical slum,” Journal of Allergy andClinical Immunology, vol. 92, no. 3, pp. 404–411, 1993.
[12] N. R. Lynch, R. I. Lopez, and M. C. Di Prisco-Fuenmayor,“Allergic reactivity and socio-economic level in a tropicalenvironment,” Clinical Allergy, vol. 17, no. 3, pp. 199–207,1987.
[13] P. J. Cooper, M. E. Chico, M. Bland, G. E. Griffin, andT. B. Nutman, “Allergic symptoms, atopy, and geohelminthinfections in a rural area of Ecuador,” American Journal ofRespiratory and Critical Care Medicine, vol. 168, no. 3, pp. 313–317, 2003.
[14] A. H. J. Van den Biggelaar, R. Van Ree, L. C. Rodrigues etal., “Decreased atopy in children infected with Schistosomahaematobium: a role for parasite-induced interleukin-10,” TheLancet, vol. 356, no. 9243, pp. 1723–1727, 2000.
[15] M. Medeiros, J. P. Figueiredo, M. C. Almeida et al., “Schisto-soma mansoni infection is associated with a reduced course ofasthma,” Journal of Allergy and Clinical Immunology, vol. 111,no. 5, pp. 947–951, 2003.
[16] L. G. G. Pacıfico, F. A. V. Marinho, C. T. Fonseca et al., “Schisto-soma mansoni antigens modulate experimental allergic asthmain a murine model: a major role for CD4+ CD25+ Foxp3+ T

8 Journal of Parasitology Research
cells independent of interleukin-10,” Infection and Immunity,vol. 77, no. 1, pp. 98–107, 2009.
[17] E. Mitre, S. Norwood, and T. B. Nutman, “Saturation ofimmunoglobulin E (IgE) binding sites by polyclonal IgE doesnot explain the protective effect of helminth infections againstatopy,” Infection and Immunity, vol. 73, no. 7, pp. 4106–4111,2005.
[18] R. R. Oliveira, K. J. Gollob, J. P. Figueiredo et al., “Schistosomamansoni infection alters co-stimulatory molecule expressionand cell activation in asthma,” Microbes and Infection, vol. 11,no. 2, pp. 223–229, 2009.
[19] M. Yazdanbakhsh and P. M. Matricardi, “Parasites and thehygiene hypothesis: regulating the immune system?” ClinicalReviews in Allergy and Immunology, vol. 26, no. 1, pp. 15–23,2004.
[20] L. S. Cardoso, S. C. Oliveira, A. M. Goes et al., “Schistosomamansoni antigens modulate the allergic response in a murinemodel of ovalbumin-induced airway inflammation,” Clinicaland Experimental Immunology, vol. 160, no. 2, pp. 266–274,2010.
[21] A. J. Dessein, M. Begley, C. Demeure et al., “Human resistanceto Schistosoma mansoni is associated with IgG reactivity to a37-kDa larval surface antigen,” The Journal of Immunology,vol. 140, no. 8, pp. 2727–2736, 1988.
[22] N. Katz, P. M. Coelho, and J. Pellegrino, “Evaluation of Kato’squantitative method through the recovery of Schistosomamansoni eggs added to human feces,” Journal of Parasitology,vol. 56, no. 5, pp. 1032–1033, 1970.
[23] W. A. Hoffman, J. A. Pons, and J. L. Janer, “Sedimentationconcentration method in Schistosomiasis mansoni,” PuertoRico Journal of Public Health, vol. 9, pp. 283–298, 1934.
[24] WHO, Prevention and Control of Schistosomiasis and Soil-Transmitted Helminthiasis, Technical Report Series No. 912,World Health Organization, 2002.
[25] A. Ebrahim, H. El-Morshedy, E. Omer, S. El-Daly, and R.Barakat, “Evaluation of the Kato-Katz thick smear and formolether sedimentation techniques for quantitative diagnosis ofSchistosoma mansoni infection,” American Journal of TropicalMedicine and Hygiene, vol. 57, no. 6, pp. 706–708, 1997.
[26] P. Kardos and J. Keenan, “Tackling COPD: a multicomponentdisease driven by inflammation,” MedGenMed Medscape Gen-eral Medicine, vol. 8, no. 3, article 54, 2006.
[27] E. D. Bateman, C. Feldman, J. O’Brien et al., “Guideline forthe management of chronic obstructive pulmonary disease(COPD): 2004 revision,” South African Medical Journal, vol.94, no. 7, part 2, pp. 559–575, 2004.
[28] A. M. B. Menezes, R. Perez-Padilla, J. R. B. Jardim etal., “Chronic obstructive pulmonary disease in five LatinAmerican cities (the PLATINO study): a prevalence study,”The Lancet, vol. 366, no. 9500, pp. 1875–1881, 2005.
[29] K. Toren, T. Gislason, E. Omenaas et al., “A prospective studyof asthma incidence and its predictors: the RHINE study,”European Respiratory Journal, vol. 24, no. 6, pp. 942–946, 2004.
[30] X. Wang, T. T. Mensinga, J. P. Schouten, B. Rijcken, andS. T. Weiss, “Determinants of maximally attained level ofpulmonary function,” American Journal of Respiratory andCritical Care Medicine, vol. 169, no. 8, pp. 941–949, 2004.
[31] T. Sigsgaard, C. Hjort, Ø. Omland, M. R. Miller, and O.F. Pedersen, “Respiratory health and allergy among youngfarmers and non-farming rural males in Denmark: the SUSstudy,” Journal of Agromedicine, vol. 9, no. 2, pp. 223–238,2004.
[32] Ø. Omland, C. Hjort, O. F. Pedersen, M. R. Miller, and T. Sigs-gaard, “New-onset asthma and the effect of environment andoccupation among farming and nonfarming rural subjects,”Journal of Allergy and Clinical Immunology, vol. 128, no. 4, pp.761–765, 2011.
[33] C. Svanes, E. Omenaas, G. E. Eide, O. Fluge, and A. Gulsvik,“Hospitalization for lung disease in early childhood andasthma symptoms in young adulthood,” Respiratory Medicine,vol. 92, no. 8, pp. 1003–1009, 1998.
[34] N. R. Lynch, I. A. Hagel, M. E. Palenque et al., “Relationshipbetween helminthic infection and IgE response in atopic andnonatopic children in a tropical environment,” Journal ofAllergy and Clinical Immunology, vol. 101, no. 2, part 1, pp.217–221, 1998.
[35] A. C. Pastorino, R. D. C. Rimazza, C. Leone, A. P. M. Castro,D. Sole, and C. M. A. Jacob, “Risk factors for asthma inadolescents in a large urban region of Brazil,” Journal ofAsthma, vol. 43, no. 9, pp. 695–700, 2006.
[36] A. C. Pastorino, F. C. Kuschnir, L. K. P. Arruda et al., “Sensi-tisation to aeroallergens in Brazilian adolescents living at theperiphery of large subtropical urban centres,” Allergologia etImmunopathologia, vol. 36, no. 1, pp. 9–16, 2008.
[37] K. J. Rothman, “No adjustments are needed for multiple com-parisons,” Epidemiology, vol. 1, no. 1, pp. 43–46, 1990.
[38] T. V. Perneger, “What’s wrong with Bonferroni adjustments,”BMJ, vol. 316, no. 7139, pp. 1236–1238, 1998.
[39] E. Vieira Ponte, F. Lima, M. I. Araujc, R. Riccio Oliveira, L.Santos Cardoso, and A. A. Cruz, “Skin test reactivity and Derp-induced interleukin 10 production in patients with asthmaor rhinitis infected with Ascaris,” Annals of Allergy, Asthma andImmunology, vol. 96, no. 5, pp. 713–718, 2006.
[40] G. M. Hunninghake, M. E. Soto-Quiros, L. Avila et al., “Sen-sitization to Ascaris lumbricoides and severity of childhoodasthma in Costa Rica,” Journal of Allergy and ClinicalImmunology, vol. 119, no. 3, pp. 654–661, 2007.
[41] L. J. Palmer, J. C. Celedon, S. T. Weiss, B. Wang, Z. Fang, and X.Xu, “Ascaris lumbricoides infection is associated with increasedrisk of childhood asthma and atopy in rural China,” AmericanJournal of Respiratory and Critical Care Medicine, vol. 165, no.11, pp. 1489–1493, 2002.
[42] C. A. Figueiredo, M. L. Barreto, L. C. Rodrigues et al.,“Chronic intestinal helminth infections are associated withimmune hyporesponsiveness and induction of a regulatorynetwork,” Infection and Immunity, vol. 78, no. 7, pp. 3160–3167, 2010.
[43] J. D. Turner, J. A. Jackson, H. Faulkner et al., “Intensity ofintestinal infection with multiple worm species is related toregulatory cytokine output and immune hyporesponsiveness,”Journal of Infectious Diseases, vol. 197, no. 8, pp. 1204–1212,2008.
[44] R. M. Maizels and M. Yazdanbakhsh, “Immune regulation byhelminth parasites: cellular and molecular mechanisms,”Nature Reviews Immunology, vol. 3, no. 9, pp. 733–744, 2003.

Hindawi Publishing CorporationJournal of Parasitology ResearchVolume 2012, Article ID 296856, 11 pagesdoi:10.1155/2012/296856
Clinical Study
The Effect of Antihelminthic Treatment on Subjects withAsthma from an Endemic Area of Schistosomiasis:A Randomized, Double-Blinded, and Placebo-Controlled Trial
Maria Cecilia F. Almeida,1 Givaneide S. Lima,1 Luciana S. Cardoso,1, 2, 3
Robson P. de Souza,1 Regis A. Campos,1 Alvaro A. Cruz,4 Joanemile P. Figueiredo,1
Ricardo R. Oliveira,1, 3, 5 Edgar M. Carvalho,1, 3, 6 and Maria Ilma Araujo1, 3, 6
1 Servico de Imunologia, Universidade Federal da Bahia (UFBA), 40110-160 Salvador, BA, Brazil2 Departamento de Ciencias da Vida, Universidade do Estado da Bahia UNEB, 41.150-000 Salvador, BA, Brazil3 Instituto Nacional de Ciencias e Tecnologia em Doencas Tropicais (INCT-DT/CNPq-MCT), Brazil4 ProAR, Nucleo de Excelencia em Asma, Universidade Federal da Bahia 40110-160 Salvador, BA, Brazil5 Faculdade de Farmacia, UFBA 40110-160 Salvador, BA, Brazil6 Escola Bahiana de Medicina e Saude Publica, EBMSP, Salvador, Bahia, Brazil
Correspondence should be addressed to Maria Ilma Araujo, [email protected]
Received 14 April 2012; Revised 15 June 2012; Accepted 21 June 2012
Academic Editor: Elena Pinelli
Copyright © 2012 Maria Cecilia F. Almeida et al. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
This is a prospective, double-blinded, and placebo-controlled trial evaluating the influence of antihelminthic treatments on asthmaseverity in individuals living in an endemic area of schistosomiasis. Patients from group 1 received placebo of Albendazole orof Praziquantel and from group 2 received Albendazole and Praziquantel. Asthma severity was assessed by clinical scores andby pulmonary function test. There was no significant difference in the asthma scores from D0 to D1–D7 after Albendazole orPraziquantel and from D0 to D30–90 after Albendazole or Praziquantel in both, group 1 and 2. It was observed, however, a clinicalworsening of the overall studied population after 6 months and 12 months of antihelminthic treatments. Additionally, we observedincreased frequency of forced expiratory volume in 1 second (FEV1) < 80% on 12 and 18 months after treatment. The worseningof asthma severity after repeated antihelminthic treatments is consistent with the hypothesis of the protective role conferred byhelminths in atopic diseases.
1. Introduction
Helminthic infections and allergic diseases are highly preva-lent in many parts of the world, and both lead to type 2immune response with secretion of IL-4, IL-5, and IL-13,with a consequent increase in the production of IgE andeosinophilia. Lynch et al. [1] studying the skin prick test(SPT) response in children from an ascariasis endemic areaobserved a decreased reactivity to the test and subsequentlyan increased response after treatment of intestinal helminths[2].
Studies conducted by the Immunology Service (SIM)of the Federal University of Bahia, Brazil, demonstrateda negative association between the cutaneous immediate
hypersensitivity response to the skin prick test to aeroaller-gens and Schistosoma mansoni parasite load, measured bya quantitative assessment of the number of eggs per gramof stool [3]. Over a year-long follow-up study in the stateof Bahia, a group of researchers from SIM compared threepopulations from impoverished areas of the state, includingone group from an endemic area of S. mansoni, one groupfrom a rural nonendemic area, and a third group from aslum area in Salvador, the capital of the state. In the study,it was observed that asthma severity indicators were lowerin individuals living in the endemic areas of schistosomiasiswhen compared to the other two areas in which there wereno recorded cases of S. mansoni transmission [4].

2 Journal of Parasitology Research
Several factors may explain the lower frequency ofpositive SPT and lower asthma severity in populationsinfected with helminths. The possible hypothesis includeshigh production of polyclonal IgE and reduced levels ofallergen-specific IgE [1, 2], high concentrations of antigen-specific IgG4 [5], activation of regulatory cells, and reg-ulatory cytokine production [6]. For instance, IL-10 canpromote a decrease in the release of histamine and othermast cell mediators [7]. Since infection by S. mansoni induceshigh production of IL-10, it is possible that this is the mainmechanism by which the allergic response is suppressedin infected individuals. This hypothesis is reinforced bystudies of van den Biggelaar et al. [6], which showed thatreduced reactivity to SPT in African children infected withS. haematobium was associated with an increase in IL-10 production in vitro by cells of these individuals. Ourhypothesis for the current study is that treatment of helminthinfections, including a drug to treat schistosomiasis, alters theimmune response leading to worsening in asthma outcomes.The aims of this study were, firstly, evaluating early eventsassociated to asthma severity resulting from treatment ofhelminth infections, and secondly, determining the degreeof interference of antihelminthic treatment in the clinicalcourse of asthma in a randomized, double-blinded, andplacebo-controlled trial.
2. Materials and Methods
2.1. Subjects and Study Design. This is a randomized, double-blinded, and placebo-controlled trial with two groups ofasthmatics living in a S. mansoni endemic area. The studywas carried out in Agua Preta, a small village near the cityof Gandu in the State of Bahia in Brazil. Gandu is located280 km south of Salvador, the capital of the State of Bahia.Agua Preta is composed of a residential area in the center ofthe village and surrounding farms. There are approximately800 people living in that community. They live in poorsanitary conditions and agriculture is their predominantoccupation. The Agua Preta community was identified byour group as a community with a frequent infection ofSchistosoma mansoni (49.5% in a survey of 427 residentsin 2006) and helminthic infection in general (prevalence ofAscaris lumbricoides, Trichuris trichiura, and hookworm atthat time was 24.2%, 33.8%, and 22.2%, resp.). Six hundredone individuals from Agua Preta agreed to participate inthis study. They were screened for asthma through a directquestionnaire on the basis of the International Study ofAsthma and Allergies in Childhood (ISAAC) [8]. In addition,questions concerning concomitant illnesses, socioeconomicstatus, and living conditions were asked in a complementaryquestionnaire. Patients were selected as having asthma iftheir responses to the ISAAC questionnaire were consideredby a physician to be indicative of a personal history ofasthma in the past 12 months, and if they were 5 to 50years old. Children under 5 years old were not includeddue to difficulties in performing the pulmonary functiontest. Subjects over 50 years old were not included due toincreased rates of chronic obstructive pulmonary diseasein this age group. Only fifty asthmatic individuals from
the community met the inclusion criteria and they wererandomized either as group 1 (who would receive initiallyplacebo of antihelminthic treatments; n = 25) or group 2(who would receive Albendazole in a split dose of 400 mg,followed by Praziquantel 50 mg/Kg of body weight a weeklater; n = 25). Five individuals from group 1 left thestudy in the first week after the beginning of the study forpersonal reasons, remaining 20 individuals in this group.The loss of these individuals did not alter significantlydemographic features of group 1, such as the age and genderdistribution. At each evaluation, every patient underwenta physical examination, always performed by the samephysician (blind to the type of treatment). At the evaluations,common asthma symptoms and signs were checked, such ascough, dyspnea, and wheezing. In addition, a questionnaireelicited information on asthma (i.e., presence and frequencyof asthma attacks, type of treatment received during theattack at home, emergency department, or hospital) andthe use of prophylactic or symptomatic antiasthma drugs(e.g., antihistamine, inhaled, or oral beta-2-agonist, andinhaled, oral, or parenteral corticosteroid) since the previousevaluation. These parameters were scored as follows: physicalexamination as 0 (normal examination) and 1 (at least oneabnormal finding); asthma exacerbations as 0 (no), 1 (yes,if treated at home), and 2 (yes, if treated at an emergencydepartment or at a hospital); use of antiasthma drugs as 0(no), 1 (yes, except for oral or parenteral corticosteroid use),and 2 (yes, if oral or parenteral corticosteroid had been used)as reported in a previous study [4].
Human subject study guidelines of the US Department ofHealth and Human Service were followed in the conductionof this study. The study was approved by the Ethics Commit-tee of Professor Edgard Santos Hospital. Informed consentwas obtained from all patients or their legal guardians.
In the initial assessment, patients responded to a ques-tionnaire to assess the clinical score of asthma [4] under-went a physical examination, chest radiograph, pulmonaryfunction test, and blood sampling for evaluation of immuneresponse (IL-5, IL-10, and IFN-γ in supernatants of culturesstimulated with SWAP and Der p1). Stool exams for parasiteswere also performed on each patient. The two groupswere then treated with antihelminthics or placebo andreevaluated after the completion of treatment as shown inthe study design flowchart (Figure 1). Chest radiographsand pulmonary function tests were performed at the timeof enrolment and at day 7 after treatment. Spirometrytest was repeated 30 days after treatment. Immunologicalevaluation was performed at enrolment and repeated at 7and 90 days after treatment. After 90 days of enrolment,both placebo and treatment groups were treated with Alben-dazole and Praziquantel. From there, the two groups wereassessed monthly by clinical examination, questionnaire, andpulmonary function test for a total period of 18 monthsaccording to the study design (Figure 1).
2.2. Pulmonary Function Tests, Chest X-Ray, and Skin PrickTest to Aeroallergens (SPT). Pulmonary function tests wereperformed on all subjects at enrollment and at eachvisit thereafter. The parameter used was Forced Expiratory

Journal of Parasitology Research 3
Study design
Clinical evaluations/pulmonary function test
D0 D30 D60 D90 6 m 12 m 18 m
G1: PLAG2: PZQ
D7 (Alb)/D0 (PZQ)
D14 (Alb)/D7 (PZQ)
Fecal exams for parasites (Kato-Katz), SPT to aeroallergens
G1: PLAG2: Alb
G1 and G2: Alb + PZQ
Chest X-ray
D0, D7, and D90 levels of IL-5, IFN-γ, andIL-10 in supernatants of PBMC stimulated withDer p1 and SWAP.
Figure 1: Flowchart of the study design.
Volume in 1 second (FEV1). Results were considered asnormal when FEV1 value was ≥80% [9].
Chest X-ray was performed in a specialized clinic inGandu, at baseline and at D7 after Praziquantel treatment.SPTs were performed on the right forearms of all individualsat enrolment using Dermatophagoides pteronyssinus (Derp), D. farinae (Der f), Blomia tropicalis (Blo t), Periplan-eta americana (Per a), and Blattella germanica (Bla g)glycerinated allergen extracts (FDA Allergenic). Histamine(1 : 1000) and glycerinated saline were used as positive andnegative controls, respectively. A positive skin reaction wasdefined as formation of a wheal with a mean diameter greaterthan 3 mm. The SPT results were read 20 minutes afterapplication, and a SPT response was considered as positive ifthere was at least one positive test of the five tested allergens.
2.3. Immune Response—Cell Culture and Cytokine Measure-ments. All enrolled individuals had their blood taken forimmunological studies. Peripheral blood mononuclear cells(PBMC) from the blood samples of the two groups wereanalyzed for in vitro immune response, which includedmeasurement of IL-10, IL-5, and IFN-γ production byPBMCs in response to soluble S. mansoni adult worm antigen(SWAP, kindly provided by Dr. Alfredo Goes from the FederalUniversity of Minas Gerais, Brazil) and to the antigen 1 fromD. pteronyssinus (Der p1 extract, cosmo Bio Co., Ltd.).
PBMCs from individuals of the study were obtainedthrough the Ficoll-Hypaque gradient and adjusted to theconcentration of 3 × 106 cells/mL in complete RPMImedium (Life technologies GIBCO BRL, Gaithersburg, MD).Cells were cultured in vitro with the antigens Der p1(25 μg/mL) and SWAP (10 μg/mL). The mitogen phyto-hemagglutinin (PHA) in the final concentration of 2 μg/mLwas also used in the cultures. The cultures were incubated
for 72 hours at 37◦C and 5% CO2 and the supernatants werecollected for cytokine measurements. Levels of IL-5, IL-10,and IFN-γ were determined by ELISA sandwich technique,using commercially available kits (R&D Systems) and theresults were expressed in picograms per milliliter based ona standard curve.
2.4. Fecal Examinations for Parasites. Three stool samplesfrom each individual were examined using the Hoffmansedimentation method to identify helminths and entericprotozoa, and the Kato-Katz method was used to estimateparasite load [10].
2.5. Sample Size and Statistical Analysis. Only fifty asthmaticindividuals from the village where the study was carriedout met the inclusion criteria. The power of the study wascalculated taking into account the results of a previous studyfrom our group [4] which demonstrated that the frequencyof asthma symptoms in asthmatic individuals living inan endemic area of schistosomiasis is 18.6%, whereas theprevalence of symptoms in a worm-free population is 58.7%.Based on these data, a sample size of 20 in the placebogroup and 25 in the treated group has 76% power to detecta difference between proportions with a significance alphalevel of 0.05 (two-tailed).
Statistical analyses were performed using the softwareStatistical Package for Social Science (version 9.0 for Win-dows; SPSS). Fisher’s exact test was used to compare propor-tions. The Mann-Whitney U test was used to compare levelsof cytokines between groups, and the Wilcoxon matched-pairs signed rank test was used to compare the levelsof cytokines intragroup before and after antihelminthictreatments. Statistical significance was established at the 95%confidence interval.

4 Journal of Parasitology Research
3. Results
3.1. Features of the Studied Subjects. The study included45 asthmatic patients. They were divided into two groups:one group received placebo of antihelminthic treatments(placebo of Albendazole and placebo of Praziquantel (group1 or placebo group), while the other group received Alben-dazole to treat geohelminths and Praziquantel to treat S.mansoni infection (group 2 or Praziquantel group). Thedemographic data of subjects enrolled in the study are shownin Table 1. S. mansoni parasite burden and infection withother helminths as well as the frequency of positive skin pricktest to aeroallergens are also shown in Table 1.
Gender distribution did not differ significantly betweengroups who received placebos (G1; 50% male) and those whoreceived antihelminthic treatment (G2; 32% male, P > 0.05;Table 1).
The mean age of patients included in the study was17.6 ± 13.1 years. There was no significant difference in themean age between groups (21.3± 15.4 and 14.7± 10.3 yearsin Group 1 and Group 2, resp.) with age ranges from 6 to 20years found in 65% of G1 and in 72% of G2 (P > 0.05) and21 to 50 years in 35% and 28% of G1 and G2, respectively(P > 0.05; Table 1).
The frequency of rhinitis did not differ significantlybetween patients from group 1 and 2, being 50% and 72%,respectively (P > 0.05; Table 1). The frequency of activesmokers was similar between the placebo and Praziquantelgroups (30% and 28%, resp.; P > 0.05), while the frequencyof second-hand smoking exposure was higher in patientsfrom group 1 (90%) then in group 2 (36%; P < 0.0005;Table 1).
There was no significant difference in the frequency ofFEV1≤80% between the placebo and Praziquantel groups atbaseline (5% and 12%, resp.; P > 0.05). A positive responseto the skin prick test to aeroallergens was found in 36% ofpatients from the Praziquantel group compared to 45% ofplacebo group at baseline (P > 0.05; Table 1). The frequencyof positive response to the different aeroallergens such as Derp, Der f, Blo t, Per a and Bla g also did not differ betweenthe two groups of patients (P > 0.05). A positive response tohistamine was found in 100% of patients from group 1 and90.9% of those from group 2 (P > 0.05; Table 1).
The frequency of S. mansoni infection did not differbetween groups (P > 0.05). The S. mansoni parasite burdenalso did not differ significantly between group 1 and group2 (115 ± 49 and 427 ± 228 eggs/g feces, resp.; P > 0.05).Patients were also infected with other helminths, such asAscaris lumbricoides, Trichuris trichiura, and hookworm.However, there was no significant difference in the frequencyof other helminthic infection between groups (Table 1; P >0.05). Co-infection with S. mansoni and one or more otherhelminths were observed in 90% and 100% of patients fromG1 and G2, respectively (P > 0.05; Table 1).
Clinical scores for asthma were initially evaluated atbaseline (day 0 or pretreatment) and for seven consecutivedays during the first week after treatment with placeboor Albendazole (D1 to D7). At day 7 after Albendazoletreatment, patients from group 1 and group 2 were treated
with placebo of Praziquantel and Praziquantel, respectively.They were clinically evaluated and had their asthma scorerecorded during the following seven days. The results ofclinical scores of asthma after treatment with placebo ofAlbendazole and placebo of Praziquantel are shown inFigure 2(a). There was no significant difference in frequencyof asthma scores at D1 to D7 compared to D0 (P > 0.05) inpatients from group 1 who received placebos of Albendazoleand Praziquantel (Figure 2(a)).
There was also no significant difference in the frequencyof asthma scores from D0 to D1–D7 after Albendazol andPraziquantel in group 2 (P > 0.05; Figure 2(b)).
The mid-term effect of Praziquantel treatment on theasthma severity was evaluated during the first 90 days ofposttreatment. Three monthly consecutive evaluations (D30to D90) were performed in each patient in this time period.The mean frequencies of asthma clinical scores are shownin Figure 3(a). There was no significant difference in thefrequency of clinical scores 0, 1, 2, 3, or 4 between D0 (80%,5%, 15%, 0%, 0%) and D30 to D90 (73± 8.8%, 6.7± 6.2%,19±5.7%, 0%, 0%) in the placebo group (Figure 3(a)). In thegroup treated with Praziquantel, the frequency of differentscores (0, 1, 2, 3, and 4) also did not differ from D0 (55%,25%, 20%, 0%, 0%) to D30–D90 (68 ± 5%, 15.7 ± 6.9%,16 ± 5.4%, 0%, 0%; P > 0.05; Figure 3(b)).
The long-term effect of antihelminthic treatment onasthma severity was evaluated in three different time periods,6, 12, and 18 months after-treatments. The placebo groupwas treated with Albendazole and Praziquantel at day 90,when the Praziquantel group received the second treatmentwith these two drugs. Since, after day 90, both groups weretreated with antihelminthics, the groups were combinedinto one group of treated patients thereafter. The frequencyof score zero in the studied population was lower after 6months of treatment (58%) compared to D0 (73%; P <0.05; Figure 3(c)), being the frequency of score one higher(20%) compared to baseline (6%; P < 0.05). Likewise,the frequency of score 2 was higher after 12 monthsof treatment (30%) compared to D0 (15%; P < 0.05,Figure 3(c)).
There was, however, no significant difference in thefrequency of different asthma clinical scores at 18 monthsafter treatments (65%, 15%, 15%, 3%, 0%, to scores 1, 2, 3,and 4, resp.) compared to baseline (73%, 6%, 15%, 2% and2% to scores 1, 2, 3, and 4, resp.; P > 0.05; Figure 3(c)).
The severity of asthma was also evaluated throughpulmonary function test (PFT). The result of FEV1 inpatients from group one and two are shown in Figure 4.There was no significant difference in the frequency ofFEV1 <80% either in Praziquantel or in the placebogroups when the baseline values were compared to D7post Albendazole, D7 after Praziquantel and also to D90after Praziquantel (P > 0.05, Figure 4(a)). On the otherhand, the frequency of FEV1 <80% among all the subjectswith asthma (n = 45) was higher at 12 months (22.2%)and subsequently at 18 months after treatment (34.8%)compared to the frequency at baseline (9%; P < 0.05,Figure 4(b)).

Journal of Parasitology Research 5
Table 1: Baseline characteristics of studied subjects.
Group 1 placebo n = 20 Group 2 Praziquantel n = 25 P value
Gender n
Male n (%) 10 (50) 8 (32) >0.05
Female n (%) 10 (50) 17 (68)
Age group n (%)
Child/teenagers (6–20 years old) 12 (65) 18 (72) >0.05
Adult (21–50 years old) 8 (35) 7 (28) >0.05
Rhinitis n (%) 10 (50) 18 (72) >0.05
Smoking n (%)
Active 6 (30) 7 (28) >0.05
Passive 18 (90) 9 (36) <0.005
Positive SPT response n (%)
Dermatophagoides pteronyssinus 2 (10) 5 (20) >0.05
D. farinae 2 (10) 5 (20) >0.05
Blomia tropicalis 4 (20) 7 (28) >0.05
Periplaneta americana 1 (5) 3 (12) >0.05
Blatella germanica 2 (10) 3 (12) >0.05
Positive total 9 (45) 9 (36) >0.05
Current helminth infections n (%)
Schistosoma mansoni 16 (80) 19 (76) >0.05
Ascaris lumbricoides 10 (50) 14 (56) >0.05
Hookworm 7 (35) 10 (40) >0.05
Trichuris trichiura 10 (50) 13 (52) >0.05
Coinfection (S. mansoni /1 or + helminths) 14 (90) 19 (100) >0.05
100
80
60
40
20
00 1 2 3
Freq
uen
cy o
f pa
tien
ts (
%)
Asthma score
Group 1
D0D1–D7 after Plac AlbD1–D7 after Plac PZQ
(a)
100
80
60
40
20
0
Freq
uen
cy o
f pa
tien
ts (
%)
0 1 2 3
Asthma score
Group 2
D0D1–D7 after AlbD1–D7 after PZQ
(b)
Figure 2: Frequency of clinical scores of asthma in patients from Group 1 at day zero (D0) and one to seven days (D1–D7) after treatmentwith placebo (Plac) of Albendazole (Alb) and placebo of Praziquantel (PZQ) (a); and at day zero (D0) and one to seven days (D1–D7) aftertreatment with Albendazole or Praziquantel (Group 2) (b). Praziquantel was given seven days after the treatment with Albendazole in theGroup 2. Data were represented as mean ± SD. There was no significant difference in the frequency of asthma scores between D0 versusD1–D7 in none of groups (P > 0.05; Chi-square Test for Independence).

6 Journal of Parasitology Research
100
80
60
40
20
0
Freq
uen
cy o
f pa
tien
ts (
%)
0 1 2 3
Asthma score
Group 1
D0D30–D90 after Plac Alb/PZQ
(a)
100
80
60
40
20
0
Freq
uen
cy o
f pa
tien
ts (
%)
0 1 2 3
Asthma score
Group 2
D0D30–D90 after Alb/PZQ
(b)
Score 0Score 1Score 2
Score 3Score 4
80
70
60
50
40
30
20
10
0
∗
∗
∗
Freq
uen
cy o
f pa
tien
ts (
%)
D0 6 m 12 m 18 m
(c)
Figure 3: Frequency of clinical scores of asthma at day zero (D0) and day 30 to day 90 (D30–D90) after treatment with placebo (Plac) ofAlbendazole (Alb) and placebo of Praziquantel (PZQ) (Group 1; (a)); and frequency of clinical scores of asthma at day zero (D0) and day30 to 90 (D30–D90) after treatment with Albendazole and Praziquantel (Group 2; (b)). Data were represented as mean ± SD. (c) showsthe frequency of clinical scores of asthma (0, 1, 2, 3, 4) at day zero (D0) and at 6 months, 12 months and 18 months after treatment withPraziquantel (Figure 3(c)). Patients were evaluated monthly from day 30 to day 90 (D30–D90). After 90 days of enrollment, both placeboand treatment groups were treated with Albendazole and Praziquantel. From there clinical scores of asthma were assessed each 6 months fora total period of 18 months. ∗D0 versus 6 m or D0 versus 12 m, P < 0.05; Fisher’s exact test.
3.2. Cytokine Profile Induced by S. mansoni and D. pteronyssi-nus Antigens in PBMCs of the Studied Population. Wemeasured the cytokines IFN-γ, IL-5, and IL-10 in thesupernatants of PBMC cultures stimulated with the S.mansoni soluble adult worm antigen (SWAP) and the antigen1 of the D. pteronyssinus (Der p1). There was no significantdifference in the levels of IFN-γ between D0 and D7 orD0 and D90 in response to SWAP and Der p1 (P > 0.05,Table 2). The baseline of IL-5 mean levels in response to Derp1 in cultures was lower in the placebo group (150 pg/mL)than in Praziquantel group (463 pg/mL; P < 0.05). Therewas, however, no significant difference between the baseline
mean values and those found at D7 or D90 after treatmentin response to SWAP or Der p1 in either group (P > 0.05;Table 2). On the other hand, in the group of Praziquantel,the mean levels of IL-10 in response to SWAP decreasedfrom 642 pg/mL at D0 to 175.6 pg/mL at D90 after treatment(P < 0.05; Table 2). There was no significant difference in themean level of IL-10 in response to Der p1 comparing baselinevalues with those from D7 and D90 in both placebo andPraziquantel groups (Table 2). There was a high productionof IL-10, IL-5, and IFN-γ in cultures stimulated with themitogen PHA compared to nonstimulated cultures (P <0.05) in both groups of patients (data not shown).

Journal of Parasitology Research 7
Ta
ble
2:Le
vels
ofcy
toki
nes
insu
pern
atan
tsof
PB
MC
cult
ure
sin
the
stu
died
subj
ects
.
Cyt
okin
eA
nti
gen
D0
D7
D90
G1/
plac
ebo
G2/
PZ
QG
1/pl
aceb
oG
2/P
ZQ
G1/
plac
ebo
G2/
PZ
Q
IFN
-γW
ith
out
stim
ulu
s32
.7(3
1.2–
276.
0)31
.6(3
1.2–
91.0
)31
.2(3
1.2–
46.7
)39
.7(3
1.2–
583.
6)31
.2(3
1.2–
130.
7)32
.7(3
1.2–
2563
.0)
SWA
P14
9.5
(42.
0–10
337.
0)88
.0(3
1.2–
2092
.0)
56.0
(43.
8–14
15.0
)13
7.8
(37.
4–15
543.
0)70
.0(1
5.6–
3329
.0)
130.
7(3
1.2–
2563
.0)
Der
p133
8.5
(102
.4–7
475.
0)71
0.0
(149
.0–2
568.
0)11
6.7
(42.
0–42
0.2)
333.
9(3
2.7–
9669
.0)
201.
0(3
1.2–
4818
.0)
149.
4(1
5.6–
1275
.0)
IL-5
Wit
hou
tst
imu
lus
15.6
(15.
6–11
2.0)
15.6
(15.
6-15
.6)
15.6
(15.
6-15
.6)
15.6
(15.
6–40
.7)
15.6
(15.
6–25
.0)
15.6
(15.
6–63
5.0)
SWA
P46
8.5
(15.
6–51
56.0
)31
0.2
(15.
6–59
04.0
)54
2.0
(15.
6–44
44.0
)18
63.0
(15.
6–46
06.0
)16
70.0
(21.
5–44
44.0
)28
50(1
36.0
–444
4.0)
Der
p115
0.0
(15.
6–63
0.0)
a46
3.0
(207
.0–4
606.
0)a
28.8
(15.
6–40
7.4)
60.0
(15.
6–46
06.0
)28
.7(1
5.6–
1720
.0)
352.
0(1
5.6–
3509
.0)
IL-1
0W
ith
out
stim
ulu
s27
.5(1
5.6–
475.
0)28
.0(1
5.6–
102.
0)57
.0(1
6.8–
589.
0)23
.1(1
5.6–
1144
.0)
36.0
(15.
6–44
6.9)
15.6
(15.
6–12
7.0)
SWA
P26
4.5
(26.
0–16
88.0
)64
2.0
(125
.0–1
132.
0)b
288.
0(2
9.4–
641.
0)66
7.3
(15.
6–24
47.0
)24
0.0
(21.
1–63
8.4)
175.
6(6
0.3–
1062
.0)b
Der
p145
1.0
(56.
0–10
60.0
)34
9.0
(177
.0–1
539.
0)92
4.0
(297
.1–2
063.
0)28
8.0
(15.
6–20
86.0
)39
0.0
(54.
3–17
44.0
)20
4.0
(60.
0–63
8.0)
Dat
ash
owed
asm
edia
n(m
inim
um
and
max
imu
mva
lues
)p
g/m
l;a P
lace
boD
0ve
rsu
sP
ZQ
D0P<
0.05
(Man
n-W
hit
ney
t-te
st);
bP
ZQ
D0
vers
us
PZ
QD
90P<
0.05
(Wilc
oxon
mat
ched
-pai
rssi
gns
ran
kste
st).

8 Journal of Parasitology Research
120
100
80
60
40
20
0
D0
D7
Pla
c A
lb
D7
Pla
c P
ZQ
D90
Pla
c P
ZQ D0
D7
Alb
D7
PZ
Q
D90
PZ
Q
5 8.3 9.7 4.912 9.8
19.2 11.8
FEV
1 (p
erce
nta
ge o
f pa
tien
ts)
(a)
120
100
80
60
40
20
0
9 13.922.2
34.8
D0 6 m 12 m 18 m
FEV
1 (p
erce
nta
ge o
f pa
tien
ts)
∗∗
∗
FEV1 <80%FEV1 ≥80%
(b)
Figure 4: Frequency of Forced Expiratory Volume in 1 second (FEV1) <80% at D0, D7 after placebo of Albendazole treatment and D7and D90 after placebo of Praziquantel treatments in the Group 1 and after treatments with Albendazole and Praziquantel in the Group 2(Figure 4(a)). Frequency of FEV1 <80% at day zero (D0) and 6, 12 and 18 months after treatment with Albendazole and Praziquantel (b).Results were considered as normal when FEV1 value was ≥80%. Numbers in the top of the bars represent the percentage of patients whohad FEV1<80%. ∗D0 versus 12 m, P < 0.05; ∗∗D0 versus 18 m, P = 0.0001; Fisher’s exact test.
4. Discussion
The aim of this study was to determine in a randomized,double-blinded, and placebo-controlled trial whether anti-helminthic treatment would interfere with the clinical courseof asthma in individuals living in a S. mansoni endemic area.Additionally, we evaluated the in vitro cytokine profile inresponse to an aeroallergen and to S. mansoni antigen beforeand after antihelminthic treatment. There was no change inthe asthma score during the first weeks after treatment inboth groups, neither was there any variation after 30 to 90days. At day 90, group 1 and group 2 were combined intoone group who received Albendazole and Praziquantel eachthree months thereafter. When comparing the baseline score(D0) of this group, we found a higher frequency of scoreone and two at 6 and 12 months after treatments. The mostlikely straightforward explanation for these findings is thatearly after treatment the antigens released during the parasitekilling maintain the protective effect on asthma severity. Theeffect of the antihelminthic treatments on the clinical score ofasthma was perceived, however, only six to 12 months afterrepeated treatments. Considering that patients remainedliving in the same area using the contaminated water in theiractivities, we believe that only after sequential treatments, theloss of the protective effect of parasite infection over asthmasymptoms could be observed. Although the asthma clinicalscore scale used in this study is not validated, against othermeasures of asthma severity or control, it gives an idea of theclinical course of the disease, when obtained repeatedly. Itconsiders the use of antiasthmatic drugs and corticosteroids,as well as the need for the patient to visit emergency rooms
or the hospital due to asthma attacks. The relevance ofthis score categorization was supported by the results ofpulmonary function test which showed a significantly higherfrequency of patients with abnormal lung function 12 and18 months after antihelminthic treatments. For medical andethical reasons, the group of placebo could not be leftwithout antihelminthic treatment for more than 90 days.Hence, the two groups of patients received Albendazole andPraziquantel thereafter. One may ask if the adverse effect oflong-term treatment on asthma severity we observed in thisstudy would be due some seasonal differences during thefollow-up study. We are aware that it is a limitation in thistype of study design; however, as the study was conducted ina region with a tropical climate with no defined seasons andlow weather variations during the year, this factor may notaffect significantly the asthma severity.
Although our initial hypothesis in this study was that S.mansoni infection protects against asthma, the observationherein does not allow us to rule out the effect of otherhelminth infections in this protection, as have been proposedby other authors in experimental models of OVA-inducedasthma [11–13]. In a polyhelminth endemic area, it isdifficult to establish which parasite is protecting the hostagainst a harmfully Th2-mediated pathological process.Previous systematic reviews and meta-analysis studying theeffect of geohelminth infections on the risk of asthmashowed that these parasites in general do not protect againstasthma, but hookworm was shown to reduce the risk ofthe disease [14, 15]. A clinical trial using Trichuris suis ovaresulted in no significant changes in symptom scores ofallergic rhinitis [16]. Furthermore, treatment of hookworm

Journal of Parasitology Research 9
infection, which leads to a reduction in the worm burden,increased the risk of allergen skin sensitization but didnot interfere with the symptoms of allergic diseases [17],symptom scores of allergic rhinitis [16] and asthma [18].In a systematic review and meta-analysis of epidemiologicalstudies that researched the association between intestinalparasite infection and the presence of atopy, the authorsfound a consistent protective effect on allergic sensitizationin patients with Ascaris lumbricoides, Trichuris trichiura,hookworm, or Schistosoma sp, infection [18]. There isevidence that in S. mansoni infection, the large number ofregulatory cells and high levels of modulators moleculesin the host system lead to a downmodulation not onlyof the parasite immune response, but also the immuneresponse to bystander antigens as revised by Dunne andCooke [19].
A possible explanation for these conflicting observationsmay include the time of exposure to the worm (if acute orchronic) and also the helminthic species. For instance, it wasdemonstrated in a randomized, double-blinded and placebocontrolled trial that Albendazole and Praziquantel treatmentof infected women during pregnancy was associated withincreased risk of eczema and wheeze in the offspring [20].New data presented here reinforce the idea that dewormingmay be associated with asthma worsenings.
Regarding the effect of antihelminthic treatments oncytokine production, we were able to measure IFN-γ, IL-5,and IL-10 in response to Der p1 and to SWAP in supernatantsof PBMC cultures before treatment and 7 and 90 daysafter treatment. Although Th2 molecules such as IL-4, IL-5, and IL-13 are key cytokines involved in the inflammatoryresponse in asthma, IFN-γ has also been associated withasthma severity [21, 22]. The baseline levels of IL-5 inresponse to Der p1 in the present study were higher inthe Praziquantel group compared to the placebo group.However, there was no significant difference in the pre-versus posttreatment levels of this cytokine in the two studiedgroups. On the other hand, the production of IL-10 inresponse to SWAP decreased 90 days after antihelminthictreatment in the Praziquantel group. This result suggests thatthe regulatory mechanisms exerted by the parasites begin todiminish early after treatment.
In the past few years, it has been shown that chronichelminth infections or parasite products induce the pro-duction of T-regulatory cells and molecules such as IL-10.This response has been associated with a down-modulationof allergic inflammatory mediators, such as Th2-cytokines,eosinophils, and histamine in murine models of allergicasthma [7, 12, 23]. We have characterized the in vitroimmune response of asthmatic patients to some S. mansoniantigens and found a high production of S. mansoni antigen-specific IL-10 not only in cells of S. mansoni infected indi-viduals but also in cells of noninfected asthmatic individuals[24]. There was also a significantly higher production of IL-10 and lower production of Th2-cytokine IL-5 in response toDer p1 in PBMC cultures of asthmatic patients infected withS. mansoni compared to non-infected asthmatic patients[25]. Our findings of decreased levels of IL-10 productionafter antihelminthic treatment in the present study, therefore,
are in agreement with our’s [25] and other authors, [26]previous studies.
Other regulatory mechanisms may contribute to thesuppression of allergic inflammation induced by helminths.For instance, Pacıfico et al. showed that T CD4+CD25+ cellsprotect mice against allergen induced airway inflammationthrough an IL-10 independent mechanism [12]. This findingdiffers from other studies, which have demonstrated thatIL-10 is a key cytokine that suppresses the inflammatoryresponse in OVA-induced asthma in mice infected withhelminths. In mice infected with H. polygyrus, for example,the reduction in the number of eosinophils and in the levelsof IL-5 was associated with IL-10 production and migrationof regulatory cells to the draining lymph nodes [27].
It has also been demonstrated that cytotoxic T-lymphocyte antigen 4 (CTLA-4), a molecule rapidly upreg-ulated after T-cell activation that provides negative feedbacksignaling, and limits the immune response as reviewed byDeurloo et al. [28], is involved in the suppression of allergicresponse in asthma [29]. We previously demonstrated thatthe lower levels of Th2-cytokines in asthmatics infectedwith S. mansoni compared to non-infected asthmatics wereassociated with a higher frequency of CD4+ T-cells express-ing CTLA-4 [30]. Based on these findings, it is likely thatthe mechanisms underlying the regulation of inflammatoryresponses in asthma by S. mansoni antigens involve IL-10[31], T-regulatory cells [12], and other mechanisms such asthe expression of CTLA-4 [29, 30].
In the present study, where the number of asthmatic indi-viduals who filled out the inclusion criteria and who agreedto participate was small, there was a significant worseningin the clinical scores of asthma as well as in the pulmonaryfunction after repeated antihelminthic treatments. Thesefindings are consistent with the hypothesis of the protectiverole of helminths on atopic diseases. Changes in clinicalscores of asthma and in the pulmonary function tests wereobserved later after sequential antihelminthic treatments.Based on these results, we argue that the antigens releasedby the parasite when it dies can maintain protection againstatopic diseases. After the clearance of antigens and repeatedantihelminthic treatments to maintain a low parasite load, aloss of protection of parasite infection in the clinical courseof asthma is observed. The data suggests that IL-10 could beimplied in this protection. However, a better understandingof immune events following antihelminthic treatment isstill required and may have practical consequences in thedevelopment of future therapies of allergic diseases.
Acknowledgments
We are very grateful to all volunteers from the community ofAgua Preta - Gandu who agreed to participate in this studyand to the local health agent Irene Jesus for assistance withthe field work. We thank Dr. Irisma Souza for performing theChest-X-ray evaluation and Cristina Toledo for the review ofthe manuscript. This work was supported by the BrazilianNational Research Council (CNPq). MIA, AAC and EMC areinvestigators supported by CNPq.

10 Journal of Parasitology Research
References
[1] N. R. Lynch, I. A. Hagel, M. E. Palenque et al., “Relationshipbetween helminthic infection and IgE response in atopic andnonatopic children in a tropical environment,” Journal ofAllergy and Clinical Immunology, vol. 101, no. 2 I, pp. 217–221,1998.
[2] I. Hagel, N. R. Lynch, M. Perez, M. C. di Prisco, R. Lopez,and E. Rojas, “Modulation of the allergic reactivity of slumchildren by helminthic infection,” Parasite Immunology, vol.15, no. 6, pp. 311–315, 1993.
[3] M. I. Araujo, A. A. Lopes, M. Medeiros et al., “Inverseassociation between skin response to aeroallergens and Schis-tosoma mansoni infection,” International Archives of Allergyand Immunology, vol. 123, no. 2, pp. 145–148, 2000.
[4] M. Medeiros Jr., J. P. Figueiredo, M. C. Almeida et al.,“Schistosoma mansoni infection is associated with a reducedcourse of asthma,” Journal of Allergy and Clinical Immunology,vol. 111, no. 5, pp. 947–951, 2003.
[5] R. Hussain, R. W. Poindexter, and E. A. Ottesen, “Controlof allergic reactivity in human filariasis: Predominant local-ization of blocking antibody to the IgG4 subclass,” Journal ofImmunology, vol. 148, no. 9, pp. 2731–2737, 1992.
[6] A. H. J. van den Biggelaar, R. van Ree, L. C. Rodrigues etal., “Decreased atopy in children infected with Schistosomahaematobium: a role for parasite-induced interleukin-10,” TheLancet, vol. 356, no. 9243, pp. 1723–1727, 2000.
[7] B. Royer, S. Varadaradjalou, P. Saas, J. J. Guillosson, J. P.Kantelip, and M. Arock, “Inhibition of IgE-induced activationof human mast cells by IL-10,” Clinical and ExperimentalAllergy, vol. 31, no. 5, pp. 694–704, 2001.
[8] M. I. Asher and S. K. Weiland, “The international study ofasthma and allergies in childhood (ISAAC),” Clinical andExperimental Allergy, Supplement, vol. 28, no. 5, pp. 52–66,1998.
[9] S. Stanojevic, A. Wade, J. Stocks et al., “Reference ranges forspirometry across all ages: a new approach,” American Journalof Respiratory and Critical Care Medicine, vol. 177, no. 3, pp.253–260, 2008.
[10] N. Katz, P. M. Coelho, and J. Pellegrino, “Evaluation of Kato’squantitative method through the recovery of Schistosomamansoni eggs added to human feces,” Journal of Parasitology,vol. 56, no. 5, pp. 1032–1033, 1970.
[11] D. E. Elliott, J. Li, A. Blum et al., “Exposure to schistosome eggsprotects mice from TNBS-induced colitis,” American Journal ofPhysiology, vol. 284, no. 3, pp. G385–G391, 2003.
[12] L. G. G. Pacıfico, F. A. V. Marinho, C. T. Fonseca et al., “Schisto-soma mansoni antigens modulate experimental allergic asthmain a murine model: a major role for CD4+ CD25+ Foxp3+ Tcells independent of interleukin-10,” Infection and Immunity,vol. 77, no. 1, pp. 98–107, 2009.
[13] H. M. Mo, J. H. Lei, Z. W. Jiang et al., “Schistosoma japonicuminfection modulates the development of allergen-inducedairway inflammation in mice,” Parasitology Research, vol. 103,no. 5, pp. 1183–1189, 2008.
[14] J. Leonardi-Bee, D. Pritchard, and J. Britton, “Asthma andcurrent intestinal parasite infection: systematic review andmeta-analysis,” American Journal of Respiratory and CriticalCare Medicine, vol. 174, no. 5, pp. 514–523, 2006.
[15] C. Flohr, S. K. Weiland, G. Weinmayr et al., “The role ofatopic sensitization in flexural eczema: findings from theinternational study of asthma and allergies in childhood phasetwo,” Journal of Allergy and Clinical Immunology, vol. 121, no.1, pp. 141–147, 2008.
[16] P. Bager, J. Arnved, S. Rønborg et al., “Trichuris suis ovatherapy for allergic rhinitis: a randomized, double-blind,placebo-controlled clinical trial,” Journal of Allergy and Clin-ical Immunology, vol. 125, no. 1–3, pp. 123–130, 2010.
[17] C. Flohr, L. N. Tuyen, R. J. Quinnell et al., “Reduced helminthburden increases allergen skin sensitization but not clinicalallergy: a randomized, double-blind, placebo-controlled trialin Vietnam,” Clinical and Experimental Allergy, vol. 40, no. 1,pp. 131–142, 2010.
[18] J. Feary, J. Britton, and J. Leonardi-Bee, “Atopy and currentintestinal parasite infection: a systematic review and meta-analysis,” Allergy, vol. 66, no. 4, pp. 569–578, 2011.
[19] D. W. Dunne and A. Cooke, “A worm’s eye view of the immunesystem: consequences for evolution of human autoimmunedisease,” Nature Reviews Immunology, vol. 5, no. 5, pp. 420–426, 2005.
[20] H. Mpairwe, E. L. Webb, L. Muhangi et al., “Anthelminthictreatment during pregnancy is associated with increasedrisk of infantile eczema: randomised-controlled trial results,”Pediatric Allergy and Immunology, vol. 22, no. 3, pp. 305–312,2011.
[21] S. H. Cho, L. A. Stanciu, S. T. Holgate, and S. L. Johnston,“Increased interleukin-4, interleukin-5, and interferon-γ inairway CD4+ and CD8+ T cells in atopic asthma,” AmericanJournal of Respiratory and Critical Care Medicine, vol. 171, no.3, pp. 224–230, 2005.
[22] R. Stephens, D. A. Randolph, G. Huang, M. J. Holtzman, andD. D. Chaplin, “Antigen-nonspecific recruitment of Th2 cellsto the lung as a mechanism for viral infection-induced allergicasthma,” Journal of Immunology, vol. 169, no. 10, pp. 5458–5467, 2002.
[23] L. S. Cardoso, S. C. Oliveira, A. M. Goes et al., “Schistosomamansoni antigens modulate the allergic response in a murinemodel of ovalbumin-induced airway inflammation,” Clinicaland Experimental Immunology, vol. 160, no. 2, pp. 266–274,2010.
[24] L. S. Cardoso, S. C. Oliveira, A. M. Goes et al., “Schistosomamansoni antigens modulate the allergic response in a murinemodel of ovalbumin-induced airway inflammation,” Clinicaland Experimental Immunology, vol. 160, no. 2, pp. 266–274,2010.
[25] M. I. A. S. Araujo, B. Hoppe, M. Medeiros Jr. et al., “ImpairedT helper 2 response to aeroallergen in helminth-infectedpatiente with asthma,” Journal of Infectious Diseases, vol. 190,no. 10, pp. 1797–1803, 2004.
[26] L. E. P. M. van der Vlugt, L. A. Labuda, A. Ozir-Fazalalikhanet al., “Schistosomes induce regulatory features in human andmouse CD1dhi B cells: inhibition of allergic inflammation byIL-10 and regulatory T cells,” Plos One, vol. 7, no. 2, Article IDe30883, 2012.
[27] K. Kitagaki, T. R. Businga, D. Racila, D. E. Elliott, J. V.Weinstock, and J. N. Kline, “Intestinal helminths protect in amurine model of asthma,” Journal of Immunology, vol. 177, no.3, pp. 1628–1635, 2006.
[28] D. T. Deurloo, B. C. A. M. van Esch, C. L. Hofstra, F. P.Nijkamp, and A. J. M. van Oosterhout, “CTLA4-IgG reversesasthma manifestations in a mild but not in a more “severe”ongoing murine model,” American Journal of Respiratory Celland Molecular Biology, vol. 25, no. 6, pp. 751–760, 2001.
[29] S. Tsuyuki, J. Tsuyuki, K. Einsle, M. Kopf, and A. J. Coyle,“Costimulation through B7-2 (CD86) is required for theinduction of a lung mucosal T helper cell 2 (Th2) immune

Journal of Parasitology Research 11
response and altered airway responsiveness,” Journal of Exper-imental Medicine, vol. 185, no. 9, pp. 1671–1679, 1997.
[30] R. R. Oliveira, K. J. Gollob, J. P. Figueiredo et al., “Schistosomamansoni infection alters co-stimulatory molecule expressionand cell activation in asthma,” Microbes and Infection, vol. 11,no. 2, pp. 223–229, 2009.
[31] L. M. Araujo, J. Lefort, M. A. Nahori et al., “ExacerbatedTh2-mediated airway inflammation and hyperresponsivenessin autoimmune diabetes-prone NOD mice: a critical role forCD1d-dependent NKT cells,” European Journal of Immunol-ogy, vol. 34, no. 2, pp. 327–335, 2004.