allisonbeale pharmacology203lecturer - laulima · iupac= international unionofpureand ......
TRANSCRIPT
Introduction
Allison Beale Pharmacology 203 Lecturer
Announcements
Face-‐‑to-‐‑Face (F2F): • Please silence phones • Late, leave early, or get up during class – Equivalent to absent
• Absent – w/o accepted excuse, 10% off final grade
Both F2F and online: • NO late work • NO make ups or retakes of quizzes
EVERYONE! It is your responsibility to
check Laulima for postings, to familiarize yourself with due dates and deadlines, and to be
ready for class.
A Beale PHRM 203 Introduction 2
WWW Resources
• Food and Drug Administration (FDA) – www.fda.gov
• Drugs @ FDA • Medwatch • Recalls, labels, safety
• National Institutes of Health (NIH) – hXp://dailymed.nlm.nih.gov • Labels from FDA, but incomplete
– www.clinicaltrials.gov/ • Info about clinical trials
• Drug Enforcement Administration (DEA) – www.justice.gov/dea/pubs/scheduling.html • The lists of controlled drugs
• General – www.drugs.com
• Commercial cooperator with FDA
– www.drugbank.ca/ • David Wishart at the University of Alberta
A Beale PHRM 203 Introduction 3
Syllabus Overview • Office = 118 Hale Imiloa, WCC • Hours – TBA
• Phone – use email • Emphasis of PHRM 203 – Pharmacokinetics • Absorption, distribution, metabolism, excretion
– Pharmacodynamics • Sites & mechanisms of action • Toxicity vs therapeutic value • Interactions between drugs
• The Student Learning Outcomes (SLOs) for PHRM 203:
– Describe the basic mechanisms of action – Demonstrate knowledge of pharm.
terminology and concepts. – Describe variables that affect drug
action including individual differences – Define pharmacokinetics for specific
drugs – Describe significant drug interactions – Use pharmacokinetics to determine
dosing schedules and routes of administration
– List the therapeutic uses for each drug class
– Identify frequent complications & side effects associated of major drug classes
A Beale PHRM 203 Introduction 4
The SLOs for this course have been used to create questions to see if you have
mastered the material.
• Course contents: – Principles of PHRM – Anatomy & PHRM of the major organ systems including the: • Nervous system, heart, lungs, kidneys, gastrointestinal tract and blood.
– Pain & Inflammation – Chemotherapy of cancer and bacterial, protozoal, helminthic and viral diseases
– Vitamins, minerals, supplements and herbals
• Instructional methods – Lecture – Self-‐‑study – Research – Discussion – Quizzes and exams
– Reading
Syllabus Overview: content
A Beale PHRM 203 Introduction 5
• Quizzes – 10-‐‑20 points each – Matching – No make up or retest
• Midterm – One worth 200-‐‑300 pts – Multiple choice – 75% from SLO review ?’s
• Final Exam – Comprehensive – Worth at least 500 points – Multiple choice – 75% from review ?’s
• Make up exams – By arrangement at Library Resources CTR
– WILL NOT be same exam as given in class
Syllabus Overview: exams
NO RETESTS ON ANY EXAM or QUIZ
A Beale PHRM 203 Introduction 6
• Extra credit – A number of opportunities
1. Placebos 2. Viper venom (as medication) 3. Navigating the PHRM website 4. Hallucinations 5. From lab to pharmacy 6. Improving healthcare 7. Lab tests 8. CombaXing depression 9. Fat chance (about weight loss) 10. Nightmare bacteria 11. Omega-‐‑3 fish oil 12. E-‐‑café survey
– Worth 10 points each – No make up or LATE work accepted – No emailed copies for face-‐‑to-‐‑face
section – Most require completing a worksheet
and answering questions in Tests, Tasks and Surveys in Laulima
• AXendance to face-‐‑to-‐‑face section – Required – Late, leave early, get up during
class without prior arrangement • Even if you return • Equivalent to absent
– Absent • 10% off final grade FOR EVERY
UNEXCUSED ABSENCE! • Unless valid excuse (e.g., doctor’s
note) – Don’t expect to be reminded.
• Absenteeism may require withdrawal
• AXendance online section – Required to access PHRM 203
website at least three times/week. • This is tracked by Laulima
Syllabus Overview
A Beale PHRM 203 Introduction 7
Syllabus Overview
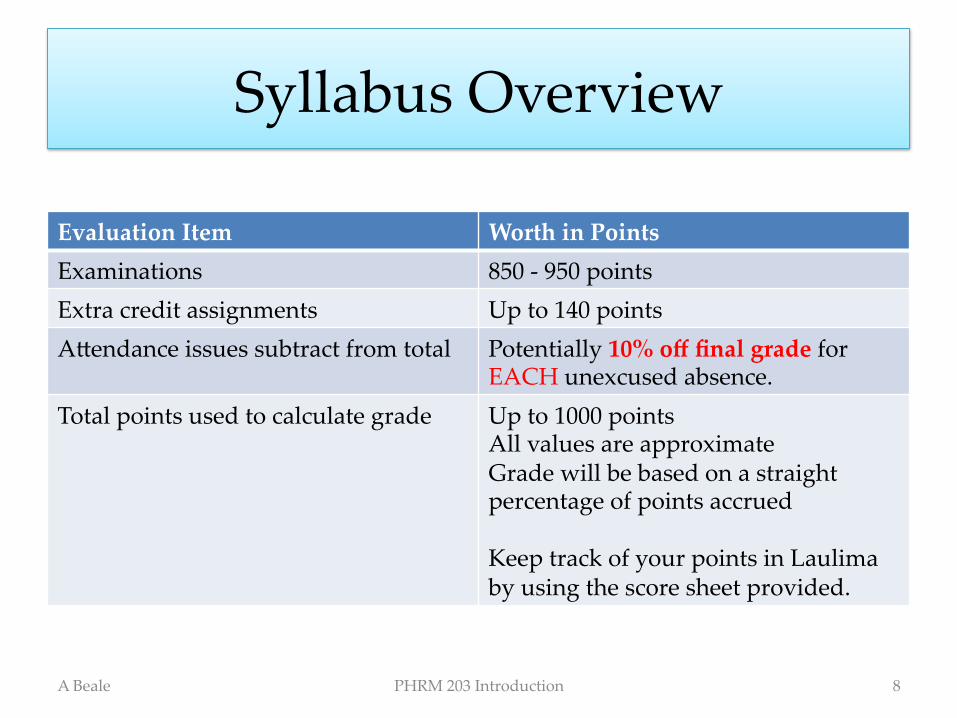
Evaluation Item Worth in Points Examinations 850 -‐‑ 950 points Extra credit assignments Up to 140 points AXendance issues subtract from total Potentially 10% off final grade for
EACH unexcused absence. Total points used to calculate grade Up to 1000 points
All values are approximate Grade will be based on a straight percentage of points accrued Keep track of your points in Laulima by using the score sheet provided.
A Beale PHRM 203 Introduction 8
Pharmacology
Physiology
Anatomy
Chemistry
Pharmacology requires an understanding of concepts from: • Anatomy
• The structure of organs, tissues, cells and subcellular parts
• Physiology • How organs, tissues
and cells function • Chemistry
• Properties of endogenous chemicals
• Properties of pharmaceuticals
A Beale PHRM 203 Introduction 9
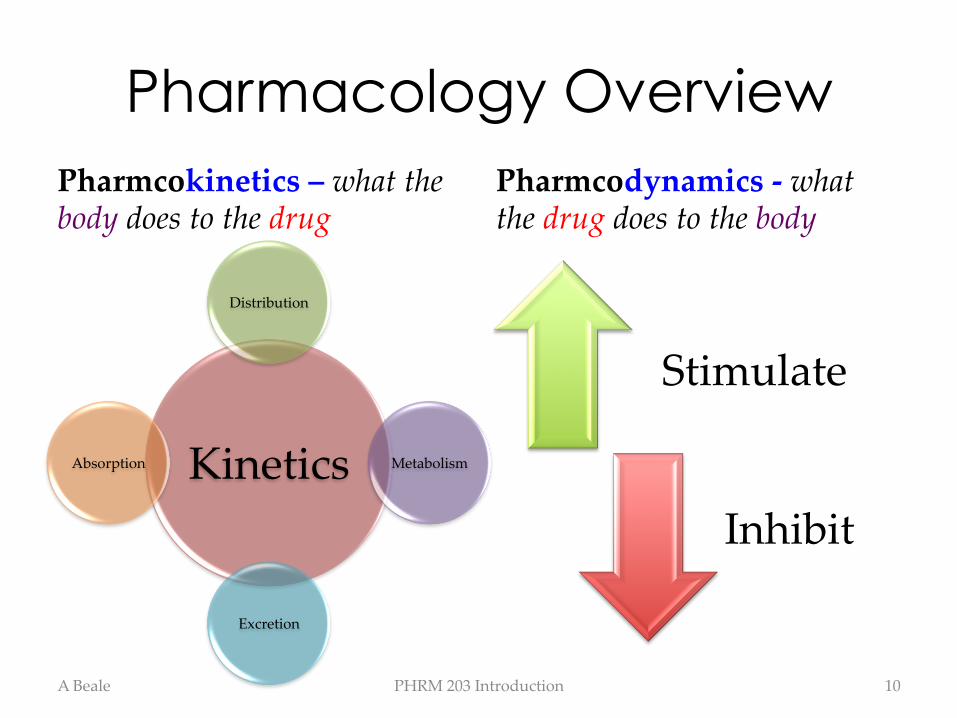
Pharmacology Overview Pharmcokinetics – what the body does to the drug
Kinetics
Distribution
Metabolism
Excretion
Absorption
Pharmcodynamics -‐‑ what the drug does to the body
Stimulate
Inhibit
A Beale PHRM 203 Introduction 10
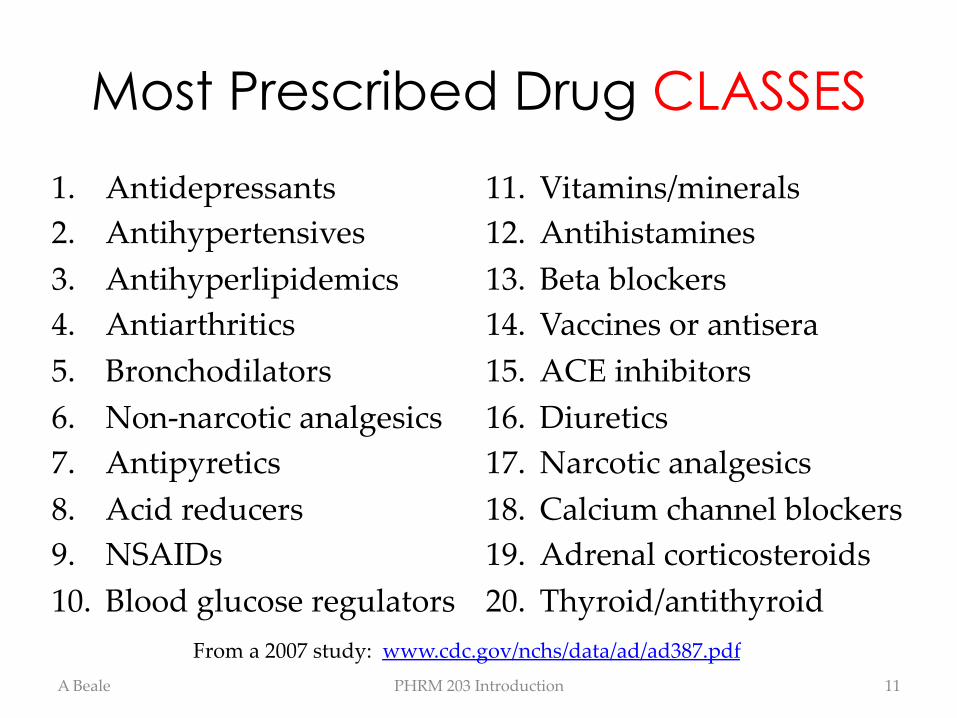
Most Prescribed Drug CLASSES
1. Antidepressants 2. Antihypertensives 3. Antihyperlipidemics 4. Antiarthritics 5. Bronchodilators 6. Non-‐‑narcotic analgesics 7. Antipyretics 8. Acid reducers 9. NSAIDs 10. Blood glucose regulators
11. Vitamins/minerals 12. Antihistamines 13. Beta blockers 14. Vaccines or antisera 15. ACE inhibitors 16. Diuretics 17. Narcotic analgesics 18. Calcium channel blockers 19. Adrenal corticosteroids 20. Thyroid/antithyroid
A Beale PHRM 203 Introduction 11
From a 2007 study: www.cdc.gov/nchs/data/ad/ad387.pdf
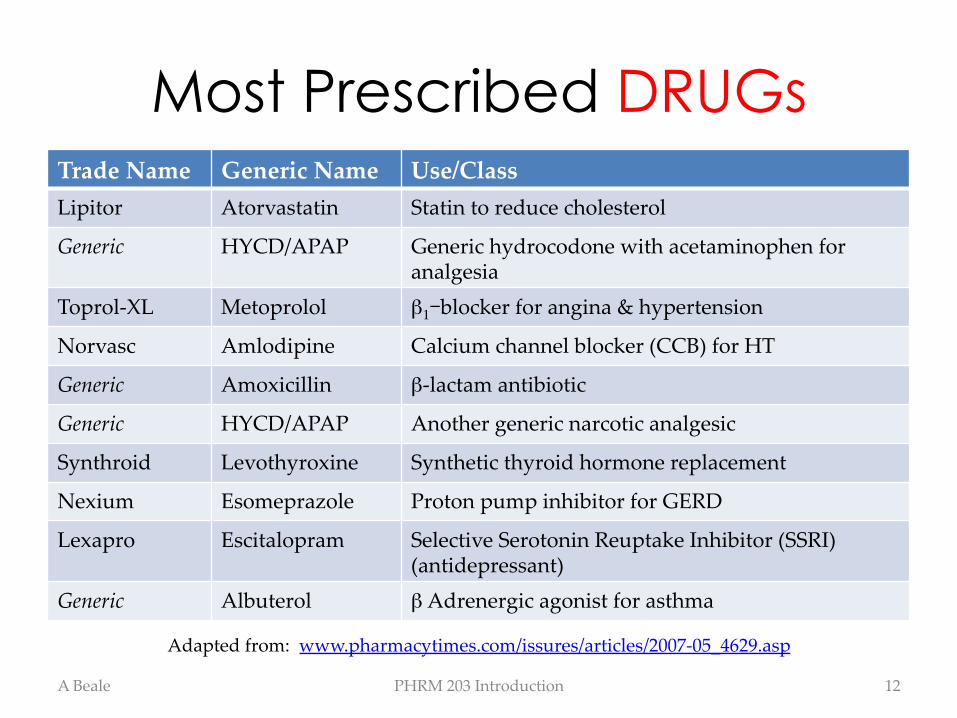
Most Prescribed DRUGs Trade Name Generic Name Use/Class Lipitor Atorvastatin Statin to reduce cholesterol
Generic HYCD/APAP Generic hydrocodone with acetaminophen for analgesia
Toprol-‐‑XL Metoprolol β1-blocker for angina & hypertension
Norvasc Amlodipine Calcium channel blocker (CCB) for HT
Generic Amoxicillin β-‐‑lactam antibiotic
Generic HYCD/APAP Another generic narcotic analgesic
Synthroid Levothyroxine Synthetic thyroid hormone replacement
Nexium Esomeprazole Proton pump inhibitor for GERD
Lexapro Escitalopram Selective Serotonin Reuptake Inhibitor (SSRI) (antidepressant)
Generic Albuterol β Adrenergic agonist for asthma
A Beale PHRM 203 Introduction 12
Adapted from: www.pharmacytimes.com/issures/articles/2007-‐‑05_4629.asp
Drug Names
• Chemical name (Systematic, IUPAC) – (2S)-‐‑1-‐‑[(2S)-‐‑2-‐‑methyl-‐‑3sulfonylpropanoly]pyrrolidine-‐‑2-‐‑carboxylic acid
• Generic name – Captopril
• Nonproprietary • US Adopted Names (USAN)
– May contain “stem” (e.g., “pril”)
• Trade name – Capoten
• Proprietary/Registered Trade Mark
A Beale PHRM 203 Introduction 13
IUPAC = International
Union of Pure and Applied Chemists
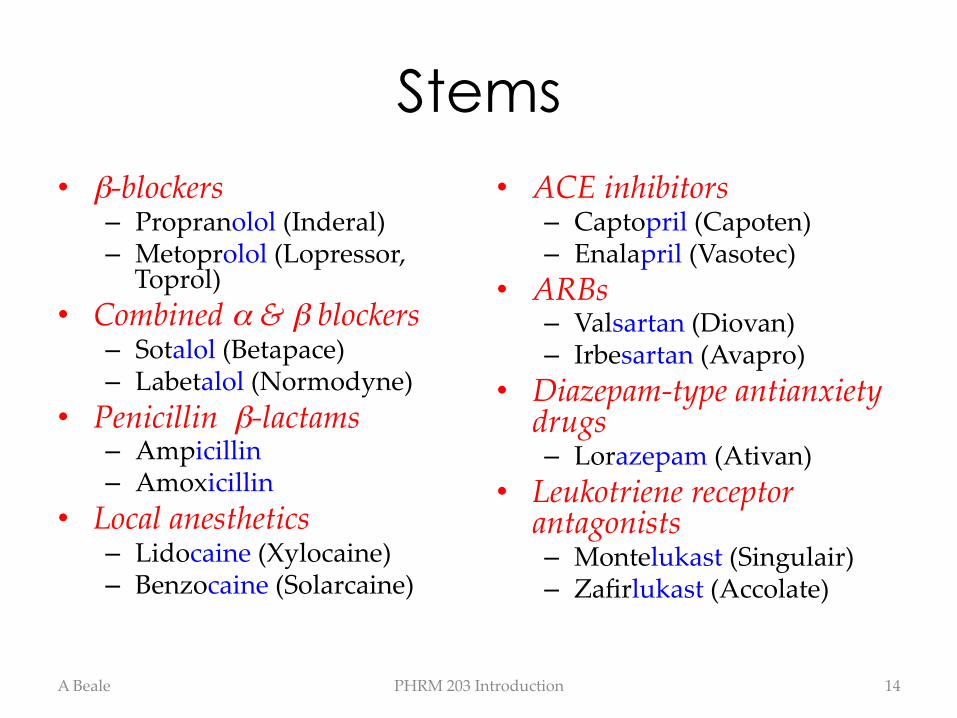
Stems • β-‐‑blockers
– Propranolol (Inderal) – Metoprolol (Lopressor,
Toprol) • Combined α & β blockers
– Sotalol (Betapace) – Labetalol (Normodyne)
• Penicillin β-‐‑lactams – Ampicillin – Amoxicillin
• Local anesthetics – Lidocaine (Xylocaine) – Benzocaine (Solarcaine)
• ACE inhibitors – Captopril (Capoten) – Enalapril (Vasotec)
• ARBs – Valsartan (Diovan) – Irbesartan (Avapro)
• Diazepam-‐‑type antianxiety drugs – Lorazepam (Ativan)
• Leukotriene receptor antagonists – Montelukast (Singulair) – Zafirlukast (Accolate)
A Beale PHRM 203 Introduction 14
Ingredients
• Active ingredient • Inert or Inactive ingredients – Fillers
• Sugar, wax, varnish – Lubricants – Adhesives – Disintegrants – Enteric coatings
• Typical tablet – 5-‐‑10 % active drug – 80% fillers – 10% other ingredients added to ensure proper disintegration • Time and place
A Beale PHRM 203 Introduction 15
Example: Captopril (Capoten) tablet contains captopril, microcrystalline cellulose, corn
starch, lactose, and stearic acid
Pharmaceutical Preparations
• Drugs for two markets – Prescription
• Dentists • Physicians • Veterinarians
– Over the counter • The general public
• Products supplied in various forms: – Tablets/capsules/lozenges
– Popsicles – Solutions/suspensions – Patches (skin) – Aerosols – Ointments, creams, gels, lotions
– Suppositories – Powders
A Beale PHRM 203 Introduction 16
See Introduction Board Notes Handout
Routes of Administration
Enteral • Orally
– Sublingual (technically parenteral, but some is swallowed)
– Buccal – Simply swallow the thing – Enteric tube
• Rectally
Parenteral • Injection
– IV – IM – SC – Also, IA, epidural,
intrathecal, intra-‐‑articular, etc.
• Transdermal • Topical • Inhalation
A Beale PHRM 203 Introduction 17
See Intro Board Notes

Drug Discovery
Discovery • Collection of field
samples – Biological
• Animal, plant, fungal… – Mineral
• Characterization and screening – High-‐‑throughput screening
• Large computer databases
• Synthesis
At end of discovery process • Drug is believed to have
activity against a particular – Receptor (or target molecule) – Disease organism
• There are many unknowns – Safety – Toxicity – Kinetics
• Dosage and scheduling – Dynamics
A Beale PHRM 203 Introduction 18
Drug Development Experimental Studies 1. In Vitro
– Cell culture – Test tube
2. In Vivo – In animals
1. Major organ toxicity 2. Type of toxicity
– Acute, Sub-‐‑acute – Chronic – Teratogenic – Mutagenic/carcinogenic
Where do drugs come from? • Plants
– Naturally occurring • Artemisia annua extract
– Processed • Morphine from opium poppy
– Recombinant DNA technology • Bovine pancreatic trypsin inhibitor gene
(Aprotinin) spliced into corn • Tissue plasminogen activator (tPA) gene
spliced into yeast • Microbes
– Bacteria and fungi • Antibiotics
• Animals – Glandular extracts
• Insulin, thyroid, growth hormone, adrenal extract
• “Spit” from leaches (bivalirudin), snakes (eptifibatide, captopril) or lizards (exenatide)
• Minerals – Lithium, calcium, iron, potassium
• Purely synthetic – Usually based on a drug originally obtained
from a plant, animal, microbe or mineral. For instance, fentanyl.
A Beale PHRM 203 Introduction 19
Drug Development
Proposing Clinical Trials • Once the experimental
studies are completed – Company submits
application to FDA • Investigational New Drug (IND) application
• Reports on current findings
• Proposes clinical trial(s) • IND allows interstate transport and use of drug
Phase 1 Clinical Trials • Usually designed to
determine HUMAN pharmacokinetics (ADME) – Healthy, paid, “volunteers” – Young, white males mostly
• Also looking for: – Biological effects – Interactions – Safety
A Beale PHRM 203 Introduction 20
Find clinical trial info: www.clinicaltrials.gov/
Phase 2 Clinical Trials • Usually testing efficacy
– Sick volunteers • Often no other treatment alternative (very sick)
• More than Phase 1 – No placebos usually, but
may have various dosage regimens
• Looking to understand: – Therapeutic efficacy – Dose ranges
Phase 3 Clinical Trials • Usually testing potency
and safety – Many more sick volunteers – Often many locations – Placebos in double blind or
cross-‐‑over studies
• Looking to understand: – Safety, efficacy and potency
in the target population
A Beale PHRM 203 Introduction 21
Drug Development
Phase 4 Clinical Trials • Usually post-‐‑marketing trials for approved drugs – Seeking new label
indication, regimen, combination or other new use
– Placebos used in double blind or cross-‐‑over studies
• Looking to understand: – If additional indications are
warranted – Adverse reactions – PaXerns of drug use – Possible combinations
Post-‐‑Marketing Surveillance • MedWatch
– www.fda.gov/medwatch/ – Monitoring of safety after the drug is released for sale
– ADR reports are solicited via voluntary reporting
– Very important for • Ideosyncratic reactions • Rare reactions
A Beale PHRM 203 Introduction 22
Drug Development
Average drug is tested in <1500 people prior to marketing; rare effects may require 10,000’s of
exposures before showing up!
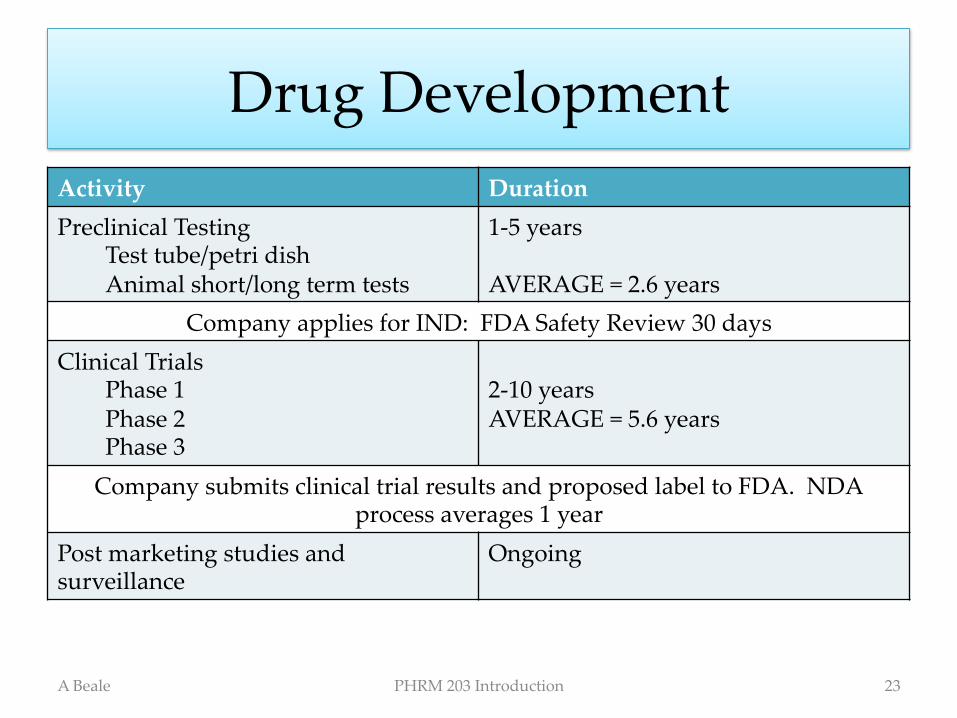
Drug Development Activity Duration Preclinical Testing
Test tube/petri dish Animal short/long term tests
1-‐‑5 years AVERAGE = 2.6 years
Company applies for IND: FDA Safety Review 30 days Clinical Trials
Phase 1 Phase 2 Phase 3
2-‐‑10 years AVERAGE = 5.6 years
Company submits clinical trial results and proposed label to FDA. NDA process averages 1 year
Post marketing studies and surveillance
Ongoing
A Beale PHRM 203 Introduction 23
Regulations FDA
• www.fda.gov/ – Information, definitions – Regulations
• Pure Food & Drug Act 1906 • Food Drugs & Cosmetic Act 1938 – Orphan Drugs – Accelerated Drug
approval
DEA • www.justice.gov/dea/pubs/csa.html
• Harrison Narcotics Act • Comprehensive Drug
Abuse Prevention & Control Act – Prescription limits – Dispensing controls
A Beale PHRM 203 Introduction 24
In Hawaii, the Narcotics Enforcement Division of the Department of Public Safety enforces the Uniform Controlled Substances Act (Chp 329 of the Hawaii Revised Statutes)
Controlled Substances
Schedule 1 criteria • High potential for abuse • No currently accepted therapeutic use (in the US)
• Lack of safety, even when used under medical supervision – No Rx’s
• Except medical marijuana • Production set by DEA
Schedule 1 examples • γ-‐‑hydroxybutyric acid (GHB) • Ibogaine • Cannabis & hashish • Potent psychodelics
– Dimethyltryptamine – Psilocybin, peyote & mescaline – LSD
• Heroin & certain other opioids • 3,4 methylenedioxymeth-‐‑
amphetamine (MDMA, ecstasy)
• Federal Analog Act materials
A Beale PHRM 203 Introduction 25
Schedule 2 Criteria • High potential for abuse • Currently accepted therapeutic use
• Abuse may lead to severe psychological or physical dependence – Available by Rx – Distribution controlled by
DEA
Schedule 2 Examples • Cocaine • Methylphenidate (Ritalin)
and dexmethylphenidate (Focalin)
• Opium • Most Opioids
– Methadone, oxycodone, fentanyl, pure codeine and hydrocodone (including combination products)
• Some barbiturates – Secobarbital & pentobarbital
A Beale PHRM 203 Introduction 26
Controlled Substances
Schedule 3 Criteria • Potential for abuse is
lower than 1 or 2 • Currently accepted therapeutic use
• Abuse may lead to moderate or low physical or high psychological dependence – Only available by Rx – Distribution controlled by
DEA
Schedule 3 Examples • Anabolic steroids
– Testosterone, Oxandrolone • Some barbiturates • A few Opioids
– Buprenorphine • Dronabinol (synthetic THC) • Ketamine • “Xyrem”
– GBH used to treat narcolepsy – only dual listed drug
A Beale PHRM 203 Introduction 27
Controlled Substances
Schedule 4 Criteria • Low abuse potential • Currently accepted therapeutic use
• Abuse may lead to limited physical or psychological dependence – Only available by Rx – Distribution controlled by
DEA
Schedule 4 Examples • Benzodiazepines and
relatives • Long-‐‑acting barbiturates
(phenobarbital) • Tramadol • Diet drugs
– Phentermine, sibutramine…
• Chloral hydrate
A Beale PHRM 203 Introduction 28
Controlled Substances
Schedule 5 Criteria • Low abuse potential • Therapeutic use • Limited physical or psychological dependence – Available only by Rx
Schedule 5 Examples • Certain Antidiarrheals
– Opium preparations – Diphenoxylate
preparations
• Pregabalin (Lyrica) • Pyrovalerone (an appetite
suppressant)
A Beale PHRM 203 Introduction 29
Controlled Substances
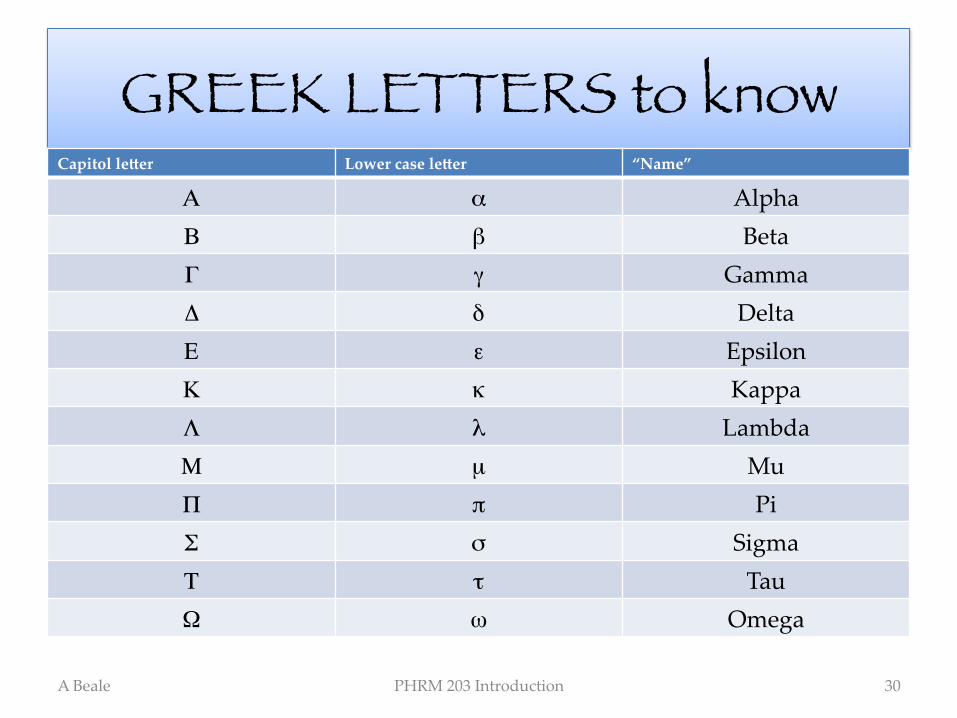
GREEK LETTERS to knowCapitol leXer Lower case leXer “Name”
Α α Alpha Β β Beta Γ γ Gamma Δ δ Delta Ε ε Epsilon Κ κ Kappa Λ λ Lambda Μ µ Mu Π π Pi Σ σ Sigma Τ τ Tau Ω ω Omega
A Beale PHRM 203 Introduction 30