alvin goo- perioperative bridge · 11/3/2015 6 recommendations for major surgery • discontinue...
TRANSCRIPT

11/3/2015
1
Peri‐Operative Bridging WSPA Annual MeetingNovember 21 th 2015
Alvin Goo, Pharm.D. Clinical Associate Professor
University of Washington School of Family Medicine and Pharmacy
Speaker Declaration
• Dr. Goo declares that neither he, nor any member of his family, has had a financial interest, arrangement or affiliation with an organization providing support for this continuing medical education activity.

11/3/2015
2
Objectives
• Analyze the evidence regarding perioperative bridging with low molecular weight heparin and newer oral anticoagulants
• Discuss the limitations of the evidence regarding perioperative bridging
• Assess the hemorrhagic and thrombotic risk of perioperative bridging
• Apply your knowledge of perioperative bridging when providing your recommendations
Discussion• Options for perioperative anticoagulation?
o Continue therapeutic Vitamin K Antagonist (VKA)
o Hold VKA with Low Molecular Weight Heparin (LMWH therapeutic dosing) bridging before and after
o Hold VKA with LMWH bridging (therapeutic or low dose) after procedure
o Hold VKA with LMWH bridging (therapeutic or low dose) prior to procedure
o Hold VKA without bridging
• Should we bridge with LMWH?

11/3/2015
3
CHEST Guidelines
• Lack of randomized trials to guide practice
Douketis JD et al. CHEST 2012;141(2):e326S‐e350S
TE Risk Management recommendations during interruption of VKA
Grade of Evidence
High Bridge 2C
Moderate Bridge or No‐bridge approach based on assessment of individual patient and surgery‐related risk factors
N/A
Low No Bridge 2C
TE = Thromboembolism
CHEST GuidelinesLevel of Risk
AnnualTE Rate
Mechanical heart valve AFib Venousthromboembolsim(VTE)
High >10% MVRCaged‐ball or tilting disk AVRRecent (w/in 6 mo) Stroke/TIA
CHADS2 = 5 or 6Recent (w/in 3 mo) stroke/TIARheumatic valvularheart disease
Recent (w/in 3 mo) VTESevere thrombophilia (deficient protein C or S, antiphospholipid)
Mod 5‐10% Bileaflet AVR and 1+ of the following: AF, stroke/TIA, HTN, DM, CHF, age > 75
CHADS2 = 3 or 4 VTE in past 3‐12 moNon‐severe thrombophilia (Factor V Leiden)Recurrent VTEActive cancer
Low <5% Bileaflet AVR w/o AF or other risk factors for stroke
CHADS2= 0‐2, with no prior stroke/TIA
VTE > 12 months ago, no other risk factors
Douketis JD et al. CHEST 2012;141(2):e326S‐e350S
Hemorrhagic Risk
High Risk Moderate Risk Low Risk
AA repairUrologic surgery/proceduresNephrectomy or kidney biopsyProstate surgeryPolypectomy, especially >1‐2cmOrgan surgeryBowel resectionCardiac surgery, CABGMajor orthopedic surgeryInter cranial or Spinal surgery/ Epidural procedure
Renal biopsyColon polyp resectionPacemaker / DefibplacementInvasive dental or Ophthalmic procedure
Cataract surgeryDental procedureCutaneous surgery
Douketis JD et al. CHEST 2012;141(2):e326S‐e350S

11/3/2015
4
Hemorrhagic Risk Factors
• Bridging with heparin
• Re initiation of heparin within 24 hours
• Mitral valve replacement
• Active cancer
• History of prior bleeding
Tafur AJ et al. J Thromb Haemost 2012;10(2):261‐267
HAS‐Bled
• Hypertension SBP > 160 1• Abnl renal or liver function
o Chronic dialysis, renal transplant, Sc ≥ 2.3 1o Cirrhosis, Bili > 2x ULN w/ LFT > 3x ULN 1
• Stroke 1• Bleeding hx or anemia 1• Labile INR 1• Elderly > 65yrs old 1• Drugs
o Antiplatelet agent or NSAIDs 1o ETOH >8 drinks/week 1
Dental Case
• 64 yr old female anticoagulated with warfarin for a‐fib and scheduled for dental extractions and dental bridge.
• No history of previous stroke or TIA
1. Discontinue warfarin 5 days prior to procedure and bridge with Enoxaparin 1mg/kg Q12
2. Continue warfarin, use prohemostatic mouthwash
3. Continue warfarin
4. Stop warfarin 2 days before procedure and resume after the procedure

11/3/2015
5
Recommendation
• Minor dental surgery: o Continue warfarin with co administration of prohemostaticagent
Or
o Discontinuation of warfarin 2‐3 days before the procedure and resume after the procedure
Grade 2C
University of Washington Anticoagulation Clinic
http://depts.washington.edu/anticoag/home/node/3
Douketis JD et al. CHEST 2012;141(2):e326S‐e350S
Dental Procedure
Low bleeding risk Moderate bleeding risk High bleeding risk
Supraginival scalingSimple restorationsLocal anesthetic injections
Subgingival scalingRestorations (subgingival)Root canalExtractionsRegional anesthetic injections
Root removal(apicoectomy) Bone removalMultiple extractions
Manage dental bleeding
Compression (gauze, tea bag) Gelatin sponge Gelfoam, Surgicel, Avitene
SuturingElectrocauteryThrombin powderTranexamic acid rinse 5%Aminocaproic acid rinse5%
http://depts.washington.edu/anticoag/home/content/local‐methods‐prevent‐or‐control‐bleeding
Mitral Valve Case
• 56 yo female is schedule for Colonoscopy due to hematochezia.
• Hx: A‐fib, Rheumatic heart disease, MVR
1. Discontinue warfarin 5 days prior to procedure and bridge with Enoxaparin 1mg/kg Q12 pre and post
2. Discontinue warfarin 5 days prior and bridge with low dose LMWH pre and post
3. Discontinue warfarin 5 days pre op and resume after procedure
4. Continue 50% of warfarin starting 5 days preop
11/3/2015
6
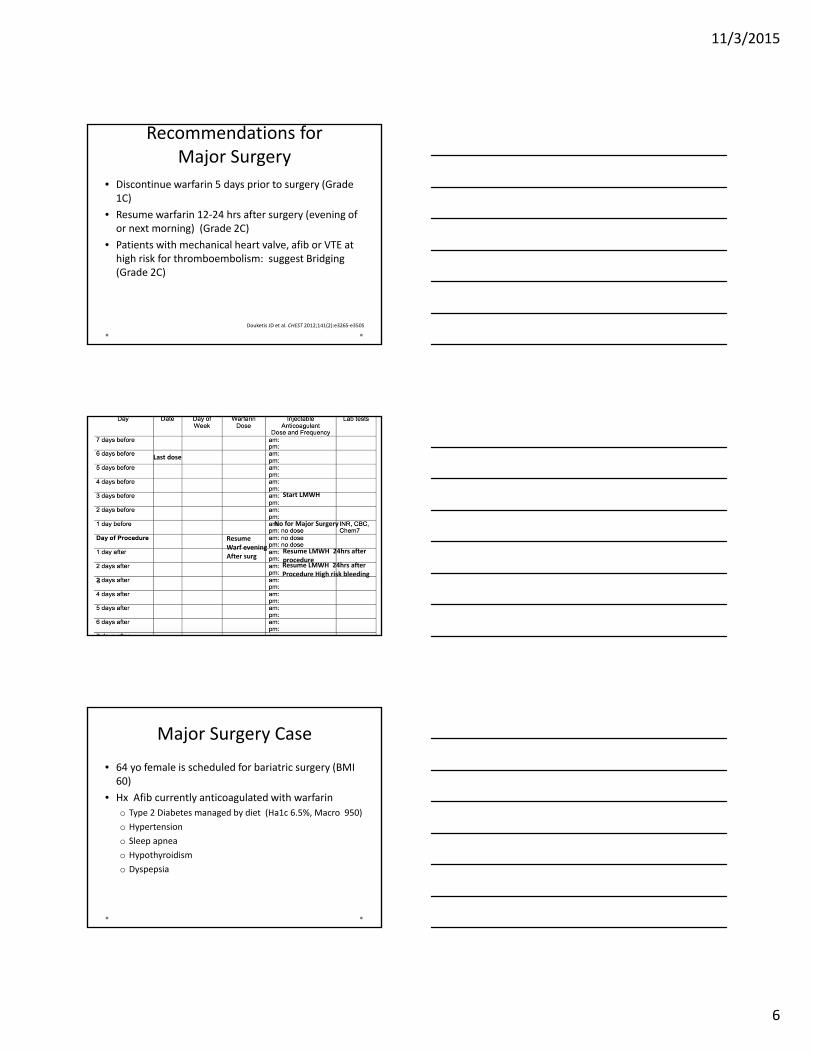
Recommendations for Major Surgery
• Discontinue warfarin 5 days prior to surgery (Grade 1C)
• Resume warfarin 12‐24 hrs after surgery (evening of or next morning) (Grade 2C)
• Patients with mechanical heart valve, afib or VTE at high risk for thromboembolism: suggest Bridging (Grade 2C)
Douketis JD et al. CHEST 2012;141(2):e326S‐e350S
Last dose
No for Major Surgery
3
Resume LMWH 24hrs after procedure
Start LMWH
ResumeWarf evening After surg
Resume LMWH 24hrs after Procedure High risk bleeding
Major Surgery Case
• 64 yo female is scheduled for bariatric surgery (BMI 60)
• Hx Afib currently anticoagulated with warfarin
o Type 2 Diabetes managed by diet (Ha1c 6.5%, Macro 950)
o Hypertension
o Sleep apnea
o Hypothyroidism
o Dyspepsia

11/3/2015
7
Options
• Discontinue warfarin 5 days preop, provide LMWH bridging (therapeutic) pre and post op
• Discontinue warfarin 5 days preop, administer low dose LMWH pre and post op
• Continue warfarin but reduce by 50% starting 5 days preop
• Stop warfarin 5 days preop and resume after procedure and consider LMWH post op if immobile
StudiesCohort Study Type Patients Procedure(s)
Wysokinski et al. 2008
Pro 345 patients with AFCHADS2 = 1.9‐2.2History of stroke = 24‐43%History of CAD = 28‐47%
Various (21% orthopedic, 20% GI, 18% urologic, 14% cardiovascular, etc.)
Garcia et al. 2008 (ACTION)
Pro 1024 patients53% AF (83% CHADS2=0‐2, 14% CHADS2=3, 3% CHADS2>4)15% VTE13% MHV (40% MVR)9% history of stroke7% considered “high risk for TE”
1293 minor outpatient surgeries (colonoscopy, dental, ophthalmologic)
Ahmed et al. 2010
Ret 459 patientsAF 70‐90% (CHADS2=2.5‐2.6)MHV 1‐19%VTE 5‐10%
Pacemaker or ICD implant
Wysokinski WE et al. Mayo Clin Proc 2008;83(6):639‐645Garcia DA et al. Arch Intern Med 2008; 168(1):63‐69
Ahmed I et al. Heart Rhythm 2010;7(6):745‐749
StudiesCohort Study Bridging Strategy Outcomes (no bridge v bridge)
Wysokinski et al. 2008
Patient TE Risk:Low = hold VKA w/o bridgeHigh = hold VKA + bridgeProcedure Bleed Risk:High = interrupt VKALow = continue VKA
90‐day symptomatic TE:1.8% v 1.5%90‐day major bleed:2.3% v 3.0%90‐day minor bleed:1.1% v 4.6%
Garcia et al. 2008 (ACTION)
92% held w/o bridge, 8% bridged (near‐exclusively LMWH)AF: 3% bridgedVTE: 10% bridgedMHV: 29% bridged
30‐day TE: 0.6% v 0%30‐day major bleed:0.2% v 3.7%30‐day “significant” bleed:0.6% v 9.3%
Ahmed et al. 2010
Compared 3 strategies:Continue warfarinHold warfarin + bridgeHold warfarin w/o bridge
Hematoma: 0.5% v 5.7% v 1.8%TIA: 0% v 0.8% v 3.5%Hospital LOS (d): 1.2 v 2.3 v 1.2
Wysokinski WE et al. Mayo Clin Proc 2008;83(6):639‐645Garcia DA et al. Arch Intern Med 2008; 168(1):63‐69
Ahmed I et al. Heart Rhythm 2010;7(6):745‐749

11/3/2015
8
Endoscopic Bridging Considerations
Diagnostic / Screening Moderate –High thrombotic risk
Low thrombotic risk
Low biopsy riskDiagnosticRemoval of polyps <1cmpolyps (< 3)
Continue warfarin Consider holding warfarinand proceed when INR< 1.5
Large polyp removal(>1 cm)
Hold warfarin and periprocedural bridge anticoagulation
Consider holding warfarinand proceed when INR< 1.5
SphicterotomyEsophageal dilationFine needle aspiration
Hold warfarin and periprocedural bridge anticoagulation
Consider holding warfarinand proceed when INR< 1.5
Endoscopy Case• 66yo male Hx of A‐fib, HTN. No hx of stroke or TIA, DM, vascular disease, or CHF. Scheduled for a repeat colonoscopy and possible polypectomy (previous colonoscopy 2 polyps resected)
1. Discontinue warfarin 5 days prior to procedure and bridge with Enoxaparin 1mg/kg Q12 pre and post
2. Discontinue warfarin 5 days prior and bridge with low dose LMWH pre and post
3. Discontinue warfarin 5 days pre op and resume after procedure
4. Continue warfarin at therapeutic dose

11/3/2015
9
Endoscopy Case
• Bleeding risk of procedure:
o High if polypectomy > 1cm
• Thrombotic risk:
o Afib, HTN
o CHADS2 = 1
• Options
o Bridge
o Hold warfarin (4‐5 days)
o Continue therapeutic warfarin
Endoscopic Biopsy
• Consecutive pts currently receiving antithromboticswere evaluated
• GI endoscopy indication: cancer screening, examination of bleeding or anemia
• 1034 pt underwent EGD while taking antithrombotics
• ASA 44.8%
• Warfarin 34.7%
• Thienopyridine 16.1%
• Dabigatran 4.8%
Fujita M, et al. Dig endoscopy 2015;27(1):25
Results
• 359 pts taking warfarin
• Endoscopic biopsy were carried out on 206 ptsreceiving warfarin
• Mean INR 1.77± 0.67 (range 0.98‐5.98)
• Hemostatic procedures after biopsy was required:
3/206 pts receiving warfarin 1.5%
34/3465 control pts 0.98%
p=0.51
Fujita M, et al. Dig endoscopy 2015;27(1):25

11/3/2015
10
Pacemaker Case• 65 yr African American with uncontrolled A‐fib, HTN, type 2 diabetes, stroke 4 years ago. Afib remains uncontrolled and pt is symptomatic. Failed to respond to cardioversion (electrical and pharmacotherapy) is scheduled for pace maker placement.
Pacemaker Implantation
• 65 yo male with Afib is scheduled for pacemaker implant.
• Hx HTN, Afib, new onset DM, previous stroke
• No Hx of CHF
• Options: o Continue warfarin during procedure
o Discontinue warfarin and bridge with LMWH pre and post procedure
o Discontinue warfarin and bridge with LMWH post procedure
o Reduce warfarin by 50% prior to procedure
BRUISE Control 2013
• Randomized, non‐blinded trial
• 681 patients with TE risk 5% or more undergoing pacemaker or ICD placement
o 88% AF (mean CHADS2= 3.4)
o 30% MHV (50% MVR, 50% bileaflet AVR)
o 5% VTE
• Continue warfarin vs. therapeutic‐dose bridging
Birnie DH et al. N Engl J Med 2013;368(22):2084‐2093

11/3/2015
11
BRUISE Control Results
• Terminated early (pre‐specified)
• TE : 1 stroke + 1 TIA in warfarin group, 1 MI in bridging group
Outcome Continuewarfarin n=338
Bridge N=343
P‐value
Pocket hematoma
3.5% 16% <0.001
Any TE 0.6% 0.3% NS
Prolonged hospitalization
1.2% 4.7% 0.006
Mortality 1.2% 0% 0.12 (NS)
Birnie DH et al. N Engl J Med 2013;368(22):2084‐2093
COMPARE Radiofrequency Ablation
• 1584 pts undergoing radiofrequency catheter ablation were randomized to: holding VKA with LMWH bridging and IV heparin, or continuation of VKA
• All pts receive IV heparin bolus prior to the trans septal puncture
• CHADS2 > 1
• INR 2‐3 3‐4 weeks prior to ablation
Di Biase L, et al. Circulation 2014;129:2638
COMPARE Results
Endpoint Bridge Warfarin maintained
p
N=790 N=794
Stroke or TIA 4.9% 0.25% <0.001
Stroke 3.7% 0.25% <0.001
TIA 1.3% 0 <0.001
Major bleeding
0.76% 0.38% 0.31
Minor bleeding
22% 4.1% <0.001
Di Biase L, et al. Circulation 2014;129:2638

11/3/2015
12
COMPARE
Bridge vs Uninterrupted Warfarin AFCA Registry
• Prospective registry that followed Pts with Afibundergoing Coronary Stenting
Uninterrupted AC n=290 Bridge n=161 P
Major CV events 11 (3.8%) 10 (6.2%) 0.25
Death 6 (2.1%) 4 (2.5%) 0.73
Stent thrombosis 6 (2.1%) 2 (1.2%) 0.72
All Bleeding 35 (12.1%) 30 (18.6%) 0.07
Major bleeding 4 (1.4%) 4 (2.5%) 0.25
Access site bleeding 16 (5.5%) 18 (11.2%) 0.03
Lahtela H, et al. Circ J 2012;76:1363
ORBIT‐AF Registry
• Outcomes Registry for Better Informed Treatment of A‐Fib
• No interruption n=5172
• No Bridge 1608
• Bridge 592
• Mean CHADS2 2.4
• Mean CHA2DS2‐VASc 4
Steinberg BA, et al. Circ 2015;3:131(5):488

11/3/2015
13
Unadjusted Outcomes
0
1
2
3
4
5
6
Total events Bleeding Thrombotic
Overall
No Bridge
Bridging
Steinberg BA, et al. Circ 2015;3:131(5):488
30 Day Postop Events
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
MI Embolism Major Bleed CVD hosp Bleed hosp
Overall
No Bridging
Bridging
Steinberg BA, et al. Circ 2015;3:131(5):488
Total Knee Arthroplasty
• Case control study in patients undergoing Total knee arthroplasty
• 61 warfarin and 61 control patients undergoing TKA
• INR 2‐2.2 on the day of surgery
• Indication for warfarin 54.1% a‐fib
• No difference in total transfusions rates
• No difference in total complications rates
Phillips A, et al. J Orthoped Surg and Research 2015;10:16
11/3/2015
14
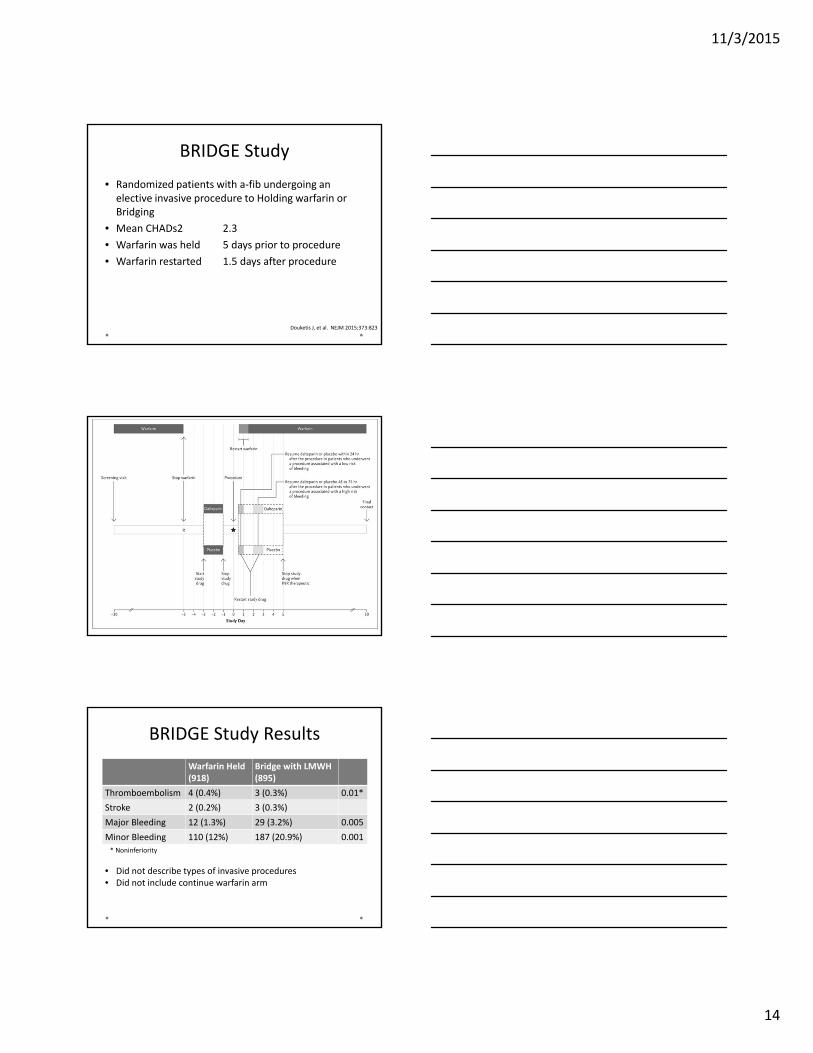
BRIDGE Study
• Randomized patients with a‐fib undergoing an elective invasive procedure to Holding warfarin or Bridging
• Mean CHADs2 2.3
• Warfarin was held 5 days prior to procedure
• Warfarin restarted 1.5 days after procedure
Douketis J, et al. NEJM 2015;373:823
BRIDGE Study Results
Warfarin Held(918)
Bridge with LMWH(895)
Thromboembolism 4 (0.4%) 3 (0.3%) 0.01*
Stroke 2 (0.2%) 3 (0.3%)
Major Bleeding 12 (1.3%) 29 (3.2%) 0.005
Minor Bleeding 110 (12%) 187 (20.9%) 0.001
* Noninferiority
• Did not describe types of invasive procedures• Did not include continue warfarin arm

11/3/2015
15
Perioperative Bridging Options• High Risk Bleeding
o Interruption of warfarin is recommended
• Low Risk Bleedingo Continue warfarin anticoagulation
• High Risk for Thrombosiso Recommend Peri and post operative bridging
• Moderate Risk for Thrombosiso Further studies are needed to clarify the approacho Bridging with LMWH is associated with greater risk of bleedingo Discuss risk of thrombosis vs risk of hemorrhage o Consider holding warfarin (< 7 days total) or continue with warfarin during
procedure
• Low Risk for Thrombosiso Recommend avoiding bridging
• Minimize subtherapeutic days (< 5)
Bridging Regimens
• Therapeutic dose LMWH
o Enoxaparin 1mg/kg Q12 hr
• Intermediate dose
o Enoxaparin 40mg Q12h
• Low dose (prophylactic) LMWH
o Enoxaparin 40mg daily
Peri operative management of Newer Oral Anticoagulants

11/3/2015
16
RE‐LY Perioperative Bridging Outcomes Warfarin Dabigatran
Bridged (391) Not Bridged (1033)
Bridged (418)
Not Bridged (2291)
Any MajorBleeding
26 (6.6%) 16 (1.5%) 27 (6.5%) 42 (1.8%)
Life threatening Bleed
7 (1.8%) 5 (0.5%) 10 (2.4%) 12 (0.5%)
Fatal Bleed 0 2 (0.2%) 0 1 (0.0)
Stroke 2 (0.5%) 2 (0.2%) 2 (0.5%) 4 (0.2%)
PulmonaryEmbolism
2 (0.5%) 0 0 2 (0.1%)
Any thrombotic event
7 (1.8%) 3 (0.3%) 5 (1.2%) 13 (0.6%)
Douketis JD etal. Thromb Haemost 2014:113(3)
Dabigatran vs Warfarin Ablation AnticoagulationMeta Analysis
• 9 cohort studies, 1 case study
• Uninterrupted warfarin
• Dabigatran held 12‐24hrs prior to procedure
Shurrab M, et al. Canadian J Card 2013;29(10):1203

11/3/2015
17
Prospective Dresden NOAC Surgical or interventional procedures• Minimal:
o Superficial skin / oral mucosal surgeries, skin biopsieso Wound revisionso Non‐extraction dental procedures
• Minor relevant bleeding risko Transluminal cardiac, arterial and venous interventionso Pace maker related surgeryo Pleura and ascites punctureo Cataract surgeryo Arthroscopy, endoscopy, laparoscopyo Organ biopsieso Dental extractiono Hernia repairo Intramuscular and paravertebral injections
• Majoro Open pelvic, abdominal and thoracic surgeryo Brain surgeryo Major orthopedic and trauma surgeryo Vascular surgery
Beyer‐Westerdorf J, et al. Eur H J 2014:35:1888
Outcome Day 30 after procedure
• Use of bridging increased with severity of surgical procedure
• Cardiovascular events were similar those with bridging (1.6%; 95% CI 0.4‐3.9%) vs
without bridging (0.8%; 95% CI 0.3‐1.9%)
• Major bleeding were more frequent in patients receiving bridging (2.7%; 95% CI 1.1‐5.5%) vs those without bridging (0.5%; 95% CI 0.1‐1.4%) p=0.010
Beyer‐Westerdorf J, et al. Eur H J 2014:35:1888
30 Day OutcomesOutcome Procedure Without
Bridging (606)With Bridging (257) p
Major Cardiovascular
MinimalMinorMajorAll
04 (0.7%)1 (0.2%)5 (0.8%)
01 (0.4%)3 (1.2%)4 (1.6%)
>.990.830.0820.265
Major bleeding MinimalMinorMajorAll
02 (0.3%)1 (0.2%)3 (0.5%)
01 (0.4%)6 (2.3%)7 (2.7%)
0.990.6540.0040.010
Any Bleeding MinimalMinorMajorAll
2 (0.3%)21 (0.5%)4 (0.7%)27 (4.5%)
1 (0.4%)8 (3.1%)10 (3.9%)19 (7.4%)
0.6540.730.0010.059
Beyer‐Westerdorf J, et al. Eur H J 2014:35:1888

11/3/2015
18
Perioperative Management of Newer oral Anticoagulants
CrCl T ½ Time of last dose of Dabigatran before procedure
CrCl T1/2 Standard Bleed Risk High Bleed Risk
>80ml/min 14hrs At least 24hrs 48hrs
50‐79ml/min 17hrs At least 24hrs 48‐72hrs
30‐49ml/min 19hrs At least 48hrs 72‐96 hrs
15‐29ml/min 22‐35hrs Not indicated Not indicated
Time of last dose of Apixaban
Standard bleed risk High bleed risk
24hrs 24‐48hrs
Time of last dose of Rivaroxaban
Standard bleed risk High bleed risk
24hrs 24‐48hrs
Preop use of LMWH is not recommended
Perioperative Management of Newer oral Anticoagulants
CrCl(ml/min)
Risk of Bleeding
Rivaroxaban Apixaban Dabigatran Edoxaban
Hold NOAC
≥ 80 LowHigh
≥24≥48
≥ 24≥ 48
≥ 24≥ 48
No data
50‐79 LowHigh
≥ 24≥ 48
≥ 24≥ 48
≥ 36≥ 72
30‐49 LowHigh
≥ 24≥ 48
≥ 24≥ 48
≥ 48≥ 96
15‐29 LowHigh
≥ 36≥ 48
≥ 36≥ 48
Not indicated
≤ 15 Not indicated
Heidbuchel H, et al. Eur Heart J 2013;34:2094Lai A, et al. BJS 2014;101: 742
Restarting NOAC Postoperative
Low Bleeding RiskHigh Bleeding
Risk
Start 24hrs post op Immobile Mobile
LMWH 6‐8hrs postopRestart NOAC 48‐72hrs
Restart NOAC 48‐72hrs
Lai A, et al. BJS 2014;101:742

11/3/2015
19
Coming Soon
PERIOP 2 ‐ A Safety and Effectiveness Study of LMWH Bridging Therapy Versus Placebo Bridging Therapy for Patients on Long Term Warfarin and Require Temporary Interruption of Their Warfarin.
Tapered Warfarin or Interrupted Warfarin With Heparin Bridging for Pacemaker or Defibrillator Implantation (PACE)