american thoracic society documents thoracic society documents ... chest physicians/american...
TRANSCRIPT
AMERICAN THORACIC SOCIETYDOCUMENTS
An Official American Thoracic Society/American College of ChestPhysicians Policy Statement: Implementation of Low-Dose ComputedTomography Lung Cancer Screening Programs in Clinical PracticeRenda Soylemez Wiener, Michael K. Gould, Douglas A. Arenberg, David H. Au, Kathleen Fennig, Carla R. Lamb,Peter J. Mazzone, David E. Midthun, Maryann Napoli, David E. Ost, Charles A. Powell, M. Patricia Rivera,Christopher G. Slatore, Nichole T. Tanner, Anil Vachani, Juan P. Wisnivesky, and Sue H. Yoon; on behalf of theATS/CHEST Committee on Low-Dose CT Lung Cancer Screening in Clinical Practice
THIS OFFICIAL POLICY STATEMENT OF THE AMERICAN THORACIC SOCIETY (ATS) AND THE AMERICAN COLLEGE OF CHEST PHYSICIANS (CHEST) WAS APPROVED BY
THE ATS BOARD OF DIRECTORS, JUNE 2015, AND BY THE CHEST BOARD OF REGENTS, APRIL 2015
Rationale: Annual low-radiation-dose computed tomography(LDCT) screening for lung cancer has been shown to reduce lungcancer mortality among high-risk individuals and is nowrecommendedbymultipleorganizations.However, LDCTscreening iscomplex, and implementation requires careful planning to ensurebenefits outweigh harms. Little guidance has been provided for siteswishing to develop and implement lung cancer screening programs.
Objectives: To promote successful implementation of comprehensiveLDCT screening programs that are safe, effective, and sustainable.
Methods: The American Thoracic Society (ATS) and AmericanCollege of Chest Physicians (CHEST) convened a committee withexpertise in lung cancer screening, pulmonary nodule evaluation, andimplementation science. The committee reviewed the evidence fromsystematic reviews, clinical practice guidelines, surveys, and theexperience of early-adopting LDCT screening programs and
summarized potential strategies to implement LDCT screeningprograms successfully.
Measurements and Main Results:We address steps that sitesshould consider during themain three phases of developing an LDCTscreening program: planning, implementation, and maintenance.We present multiple strategies to implement the nine core elementsof comprehensive lung cancer screening programs enumerated ina recent CHEST/ATS statement, which will allow sites to select thestrategy that best fits with their local context and workflow patterns.Although we do not comment on cost-effectiveness of LDCTscreening, we outline the necessary costs associated with starting andsustaining a high-quality LDCT screening program.
Conclusions: Following the strategies delineated in this policystatement may help sites to develop comprehensive LDCT screeningprograms that are safe and effective.
ContentsOverviewIntroductionMethodsResults
PlanningImplementationMaintenance
Conclusions
Overview
This policy statement offers pragmaticstrategies to assist medical centers andhealthcare systems that seek to establishcomprehensive low-radiation-dosecomputed tomography (LDCT) lung cancerscreening programs that are safe andeffective. The strategies listed herein addressthe nine core components of LDCT
screening programs proposed by theAmerican Thoracic Society (ATS) andAmerican College of Chest Physicians(CHEST) and are consistent with therequirements for coverage of LDCTscreening issued by the Center for Medicareand Medicaid Services (CMS; for Medicarebeneficiaries) and the U.S. PreventativeServices Task Force (USPSTF; for theprivately ensured). For each component, we
R.S.W. was supported by National Institutes of Health grant K07 CA138722 and resources from the Edith Nourse Rogers Memorial VA Hospital (Bedford, MA).C.G.S. was supported by Veterans Affairs Health Services Research and Development Career Development Award CDP 11-227 and resources from the VAPortland Health Care System (Portland, OR).
The views presented here do not necessarily represent those of the Department of Veterans Affairs, the Center for Medical Consumers, or the United Statesgovernment.
Am J Respir Crit Care Med Vol 192, Iss 7, pp 881–891, Oct 1, 2015
Copyright © 2015 by the American Thoracic Society
DOI: 10.1164/rccm.201508-1671ST
Internet address: www.atsjournals.org
American Thoracic Society Documents 881

summarize multiple successful strategies forprograms to consider, allowing individualprograms to choose the strategy that best fitstheir localwork environment.We conclude that:
d Implementation of LDCT screeningbegins with several planning steps,including formation ofa multidisciplinary steering committee,engaging and educating primary careproviders (PCPs), engaging localleadership, establishing a business model,and marketing the program.
d During the implementation phase,programs should be attentive toestablishing systems to screen the rightpatients at the right time, to performingshared decision making to help eligiblepatients decide whether to undergoscreening, and to standardizing processesfor performing LDCT scans, reportingLDCT results, evaluating screen-detectednodules, communicating results topatients and their providers, andmanaging incidentally detectedabnormalities.
d Smoking cessation is a critical corollaryto LDCT screening, and LDCT screeningprograms should either incorporatecounseling into the program or refercurrent smokers and recent quitters toexternal smoking cessation resources.
d To maintain performance, programsshould collect data on patients undergoingLDCT screening in a registry that shouldbe periodically reviewed to ensure theprogram is achieving quality metrics.
Introduction
The National Lung Screening Trial (NLST)demonstrated that LDCT screening of high-risk individuals can reduce lung cancer death(1). On average, NLST participants hada 1.66% risk of lung cancer death in the next6.5 years; after three rounds of annual LDCTscreening, that risk was reduced to 1.33%(a 20% relative risk reduction). Multipleorganizations recommend LDCT screening forindividuals at high risk for lung cancer (2–8).
However, LDCT screening may causeharm (Table 1), a salient concern given thatmost individuals undergoing screening donot have cancer and therefore cannotbenefit from screening (9, 10). Moreover,LDCT screening is a complex processrequiring careful coordination. The processbegins with selecting appropriate
candidates for screening and discussingscreening trade-offs with patients, includesannual screening LDCT scans, and extendsthrough evaluation of suspicious findingsand treatment of screen-detected cancers.
To optimize the balance of benefits andharms at the population level, guidelinesrecommend LDCT screening be conductedin “effective screening settings” (2).The ATS and CHEST recently issued astatement delineating nine coreprogrammatic components designed toensure safe, effective screening (Table 2)(11). This companion statement summarizesstrategies for designing and implementingcomprehensive LDCT screening programsthat include these core elements. Theproposed strategies are consistent withthe coverage requirements from CMS (12)and address the “considerations forimplementation” noted by the USPSTF (3),which sets coverage requirements for privateinsurers (Table 3).
Methods
In developing this statement, we wereguided by two implementation scienceframeworks: the RE-AIM model (13) andthe Promoting Action on ResearchImplementation in Health Services(PARIHS) model (14). The RE-AIM modelasserts that to translate evidence into practicein a sustainable way with fidelity tothe original intervention, one mustconsider Reach, Effectiveness, Adoption,Implementation, and Maintenance(Table 2). The PARIHS frameworkasserts that successful implementation is
a function of evidence, context, andfacilitation. We drew on several sourcesof evidence: systematic reviews (10,15–17) and guidelines (2–8, 18) on LDCTscreening, national surveys of clinicians’perceptions about implementation of LDCTscreening and formative evaluations ofexisting LDCT screening programs (19–21),and the expert opinion of our multi-stakeholder committee.
The committee Chair (R.S.W.) andCo-Chair (M.K.G.) convened a team withexpertise on LDCT screening, pulmonarynodule evaluation, and/or implementationscience, and early adopters of LDCTscreening. To understand diverse contextsand facilitation strategies for implementingLDCT screening programs, we selecteda multidisciplinary group withrepresentation from primary care,pulmonology/interventional pulmonology,radiology, thoracic surgery, and nursing,from various settings, including academiccenters, community hospitals, integratedhealth systems, and the Department ofVeterans Affairs. We also included a patientand a consumer advocate. Conflicts ofinterest were disclosed and vetted throughstandard ATS procedures. During moderatedsessions the committee discussed strategiesto implement the ideal elements ofcomprehensive LDCT screening programsand iteratively drafted the statement.
Results
We have organized our results into threesections: planning, implementation, andmaintenance (Table 2). First we address the
Table 1. Trade-offs of Low-Radiation-Dose Computed Tomography Screening forLung Cancer*
Potential Benefits Potential Harms
Mortality benefits Harms related to test characteristics20% relative decrease in lung cancer death(from 1.66 to 1.33%, or 3 fewer deathsper 1,000 screened)
Radiation exposure from screening CT
7% relative reduction in all-cause mortality
False reassurance (aggressive cancersmay develop in intervals betweenscreening examinations)
Overdiagnosis of clinically insignificantcancers (15–20% of tumors detected)
Psychosocial benefits and behavioral changes Harms related to findings of testReassurance if normal CT False positives and other incidental findingsTeachable moment for smoking cessation Potential harms from downstream
evaluation of findings
Definition of abbreviation: CT = computed tomography.*See Reference 10.
AMERICAN THORACIC SOCIETY DOCUMENTS
882 American Journal of Respiratory and Critical Care Medicine Volume 192 Number 7 | October 1 2015
planning steps to consider before launchingscreening programs (19). We then addresseach of the CHEST/ATS core elementsneeded to implement programs with fidelityto the NLST intervention (11). Finally, wediscuss how to maintain programs thatsustain quality, effectiveness, and safety.
Planning
Multidisciplinary Steering CommitteeThe experience of the early-adopting LDCTscreening programs represented by ourcommittee highlights the importance ofconsidering local context and workflow issues.LDCT screening and evaluation and treatmentof screen-detected nodules requiresinvolvement of pulmonology, primary care,radiology, thoracic surgery, interventionalradiology, andmedical and radiation oncology.All these parties should be represented ona steering committee that plans the screeningprogram. Some programs assembled a steeringcommittee composed of members from anexisting lung cancer tumor board, capitalizingon established working relationships,
communication channels, and clinical expertiseto create a highly functional multidisciplinaryteam. Steering committees should have clearlydefined leaders to act as liaisons andchampions for the program (19). A patientmember may provide valuable perspective.
Engaging PCPsA lesson learned from early-adopting LDCTscreening programs is the importance ofinvolving and educating PCPs from the outset.Because PCPs are tasked with preventivehealthcare and see a broader patient base thanspecialists, it is critical to obtain PCP supportto reach the target population for screening(20). Failure to include PCPs duringplanning, to solicit PCP concerns aboutimplementation, to incorporate PCP feedbackon workflow issues, or to educate PCPs onthe trade-offs of LDCT screening may createbarriers to implementing a successfulprogram. These may include slow uptake ofscreening or overzealous uptake with referralof inappropriate patients. Successful programsperformed early outreach to PCPs, includingeducational sessions that emphasized LDCT
screening as a tool to improve quality of careand outcomes for individuals at high risk forlung cancer (19, 21).
Engaging Local Leadership andEstablishing a Business ModelIt is critical to ensure local hospital orhealthcare system leadership supports thedevelopment of an LDCT screening program(19). Leadership can help spread the word,leverage support of reluctant departments,and provide necessary resources.Comprehensive screening programs requireinitial and ongoing investment of resources tobe sustainable. A business model should beestablished early. The main costs arepersonnel related, but equipment andinformation technology (IT) costs must alsobe considered (Table 4) (20).
Program MarketingFinally, marketing can help raise awareness ofthe screening program among the public aswell as clinicians within and outside the healthsystem (20). Some sites have hostedcommunity screening days to provide a
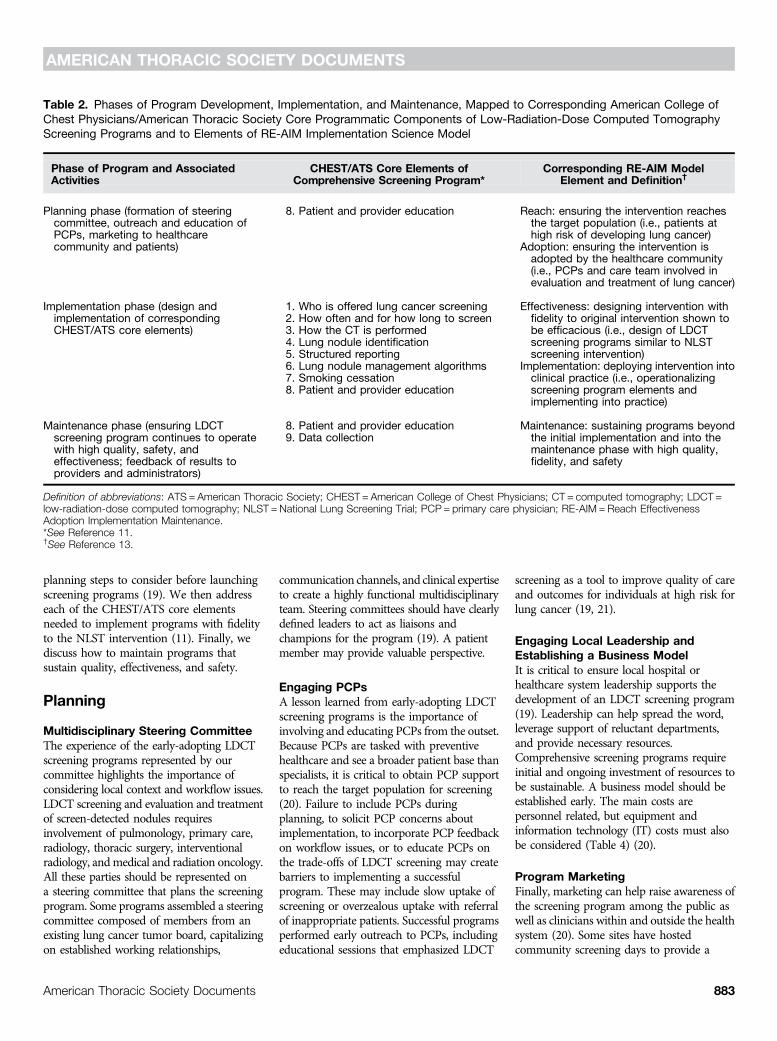
Table 2. Phases of Program Development, Implementation, and Maintenance, Mapped to Corresponding American College ofChest Physicians/American Thoracic Society Core Programmatic Components of Low-Radiation-Dose Computed TomographyScreening Programs and to Elements of RE-AIM Implementation Science Model
Phase of Program and AssociatedActivities
CHEST/ATS Core Elements ofComprehensive Screening Program*
Corresponding RE-AIM ModelElement and Definition†
Planning phase (formation of steeringcommittee, outreach and education ofPCPs, marketing to healthcarecommunity and patients)
8. Patient and provider education Reach: ensuring the intervention reachesthe target population (i.e., patients athigh risk of developing lung cancer)
Adoption: ensuring the intervention isadopted by the healthcare community(i.e., PCPs and care team involved inevaluation and treatment of lung cancer)
Implementation phase (design andimplementation of correspondingCHEST/ATS core elements)
1. Who is offered lung cancer screening Effectiveness: designing intervention withfidelity to original intervention shown tobe efficacious (i.e., design of LDCTscreening programs similar to NLSTscreening intervention)
2. How often and for how long to screen
Implementation: deploying intervention intoclinical practice (i.e., operationalizingscreening program elements andimplementing into practice)
3. How the CT is performed4. Lung nodule identification5. Structured reporting6. Lung nodule management algorithms7. Smoking cessation8. Patient and provider education
Maintenance phase (ensuring LDCTscreening program continues to operatewith high quality, safety, andeffectiveness; feedback of results toproviders and administrators)
8. Patient and provider education Maintenance: sustaining programs beyondthe initial implementation and into themaintenance phase with high quality,fidelity, and safety
9. Data collection
Definition of abbreviations: ATS = American Thoracic Society; CHEST = American College of Chest Physicians; CT = computed tomography; LDCT =low-radiation-dose computed tomography; NLST =National Lung Screening Trial; PCP = primary care physician; RE-AIM = Reach EffectivenessAdoption Implementation Maintenance.*See Reference 11.†See Reference 13.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 883
needed service and increase awareness of theprogram. Other marketing strategies includedirect-to-consumer advertising, informationalwebsites, and telephone access lines to permitself-referrals (19, 20, 22). Any direct-to-consumer advertising must be clear about thetarget population (high-risk individuals) andshould not be coercive or overly optimisticabout potential benefits (23).
Implementation
Establishing Systems to OfferScreening to the Right People at theRight TimeCHEST/ATS Components 1: Who is offeredlung cancer screening; 2: How often and forhow long to screen
The CHEST/American Society ofClinical Oncology guidelines, endorsed bythe ATS (2), suggest that screening beoffered to individuals who meet NLSTcriteria (aged 55–74 yr, who smoked withinthe past 15 yr, with at least 30 pack-yearstotal, without severe comorbidities thatlimit life expectancy). However, werecognize that many programs will followcriteria set by payers. Both CMS (12)and the USPSTF (3) follow the NLST criteriabut extend the upper age limit: Medicarebeneficiaries are covered for LDCT screeningthrough age 77 years and the privatelyinsured through age 80 years. Guidelinesrecommend offering annual LDCTscreening until the individual reaches theupper age limit, has been tobacco-freefor more than 15 years, or is no longer
healthy enough to benefit from screening(2, 3).
Perhaps the most important questionfor implementation is how to ensure thatscreening is provided to appropriateindividuals (20–22). The purpose oflimiting the scope of screening is to ensurethat benefits outweigh harms; individualsat lower risk of lung cancer or withlimited life expectancy are less likely tobenefit, and therefore the balance ofbenefits to harms is less favorable (24, 25).How best to incorporate informationabout how the risk:benefit ratio changesdepending on personal characteristics (e.g.,comorbidities) has not been resolved but isimportant to consider when selectingpatients for screening or prioritizingresources (26).
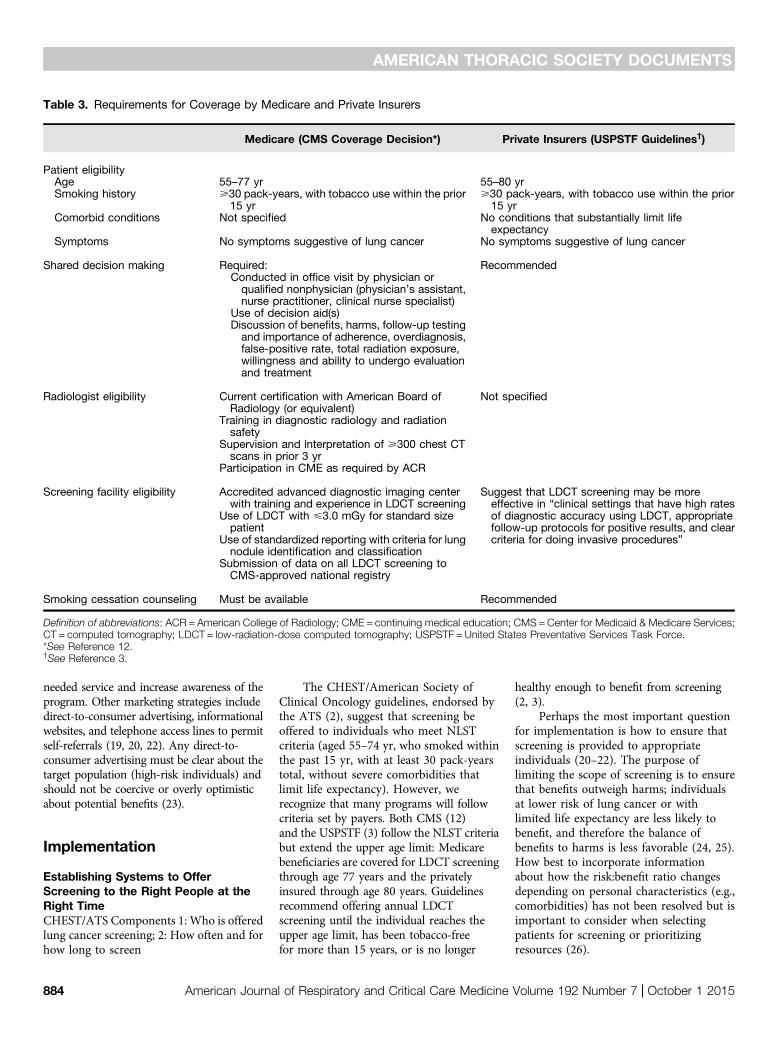
Table 3. Requirements for Coverage by Medicare and Private Insurers
Medicare (CMS Coverage Decision*) Private Insurers (USPSTF Guidelines†)
Patient eligibilityAge 55–77 yr 55–80 yrSmoking history >30 pack-years, with tobacco use within the prior
15 yr>30 pack-years, with tobacco use within the prior15 yr
Comorbid conditions Not specified No conditions that substantially limit lifeexpectancy
Symptoms No symptoms suggestive of lung cancer No symptoms suggestive of lung cancer
Shared decision making Required: RecommendedConducted in office visit by physician orqualified nonphysician (physician’s assistant,nurse practitioner, clinical nurse specialist)
Use of decision aid(s)Discussion of benefits, harms, follow-up testingand importance of adherence, overdiagnosis,false-positive rate, total radiation exposure,willingness and ability to undergo evaluationand treatment
Radiologist eligibility Current certification with American Board ofRadiology (or equivalent)
Not specified
Training in diagnostic radiology and radiationsafety
Supervision and interpretation of >300 chest CTscans in prior 3 yr
Participation in CME as required by ACR
Screening facility eligibility Accredited advanced diagnostic imaging centerwith training and experience in LDCT screening
Suggest that LDCT screening may be moreeffective in “clinical settings that have high ratesof diagnostic accuracy using LDCT, appropriatefollow-up protocols for positive results, and clearcriteria for doing invasive procedures”
Use of LDCT with <3.0 mGy for standard sizepatient
Use of standardized reporting with criteria for lungnodule identification and classification
Submission of data on all LDCT screening toCMS-approved national registry
Smoking cessation counseling Must be available Recommended
Definition of abbreviations: ACR = American College of Radiology; CME = continuing medical education; CMS=Center for Medicaid & Medicare Services;CT = computed tomography; LDCT = low-radiation-dose computed tomography; USPSTF = United States Preventative Services Task Force.*See Reference 12.†See Reference 3.
AMERICAN THORACIC SOCIETY DOCUMENTS
884 American Journal of Respiratory and Critical Care Medicine Volume 192 Number 7 | October 1 2015
Electronic medical record tools. Severalearly-adopting LDCT screening programswith high-functioning electronic medicalrecords (EMRs) have successfullyimplemented EMR-based tools as a first-pass step to limit screening to individualswho meet eligibility criteria and toreinforce education of referring providers.These include clinical reminders that areonly displayed for eligible patients anddecision support systems that promptproviders to confirm patient eligibilitywhen ordering a screening LDCT (21, 27).Implementing EMR-based tools requiresa commitment from IT to create tools andmaintain their performance (19).
Human review. Human review canreinforce (or replace, if insufficient ITcapability) EMR-based strategies. In someprograms, the screening programcoordinator (often a nurse or midlevelprovider) confirms eligibility with thepatient directly or through chart review asa gate-keeping step (19, 22). An addedadvantage is that human review canidentify comorbidities that might limitcancer treatment or life expectancy—contraindications that cannot be readilydetected by EMR-based strategies. Finally,human review is necessary if there isa mechanism for patients to self-refer forscreening, as these individuals would be
circumventing EMR-based gatekeeping.Human review can also ensure that self-referred patients have an appropriateclinician (e.g., PCP, pulmonologist) toreceive the results of the screening LDCT; ifthe patient cannot identify such a clinician,the screening program should offer to assignone. In many health systems, the onus ofhuman review may fall on PCPs, againhighlighting the need for PCP engagementand education.
Strategy for those who do not meeteligibility criteria. Screening individuals atlower risk for lung cancer or individualswith severe comorbidities will likely createan unfavorable balance of benefits to harms
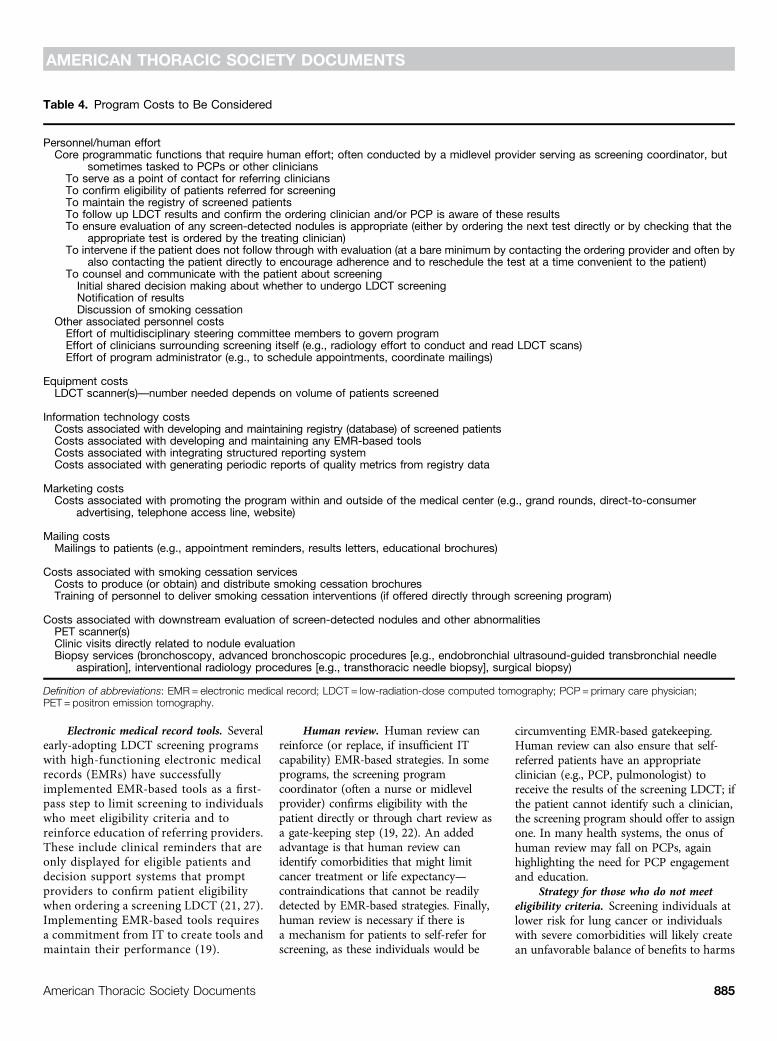
Table 4. Program Costs to Be Considered
Personnel/human effortCore programmatic functions that require human effort; often conducted by a midlevel provider serving as screening coordinator, but
sometimes tasked to PCPs or other cliniciansTo serve as a point of contact for referring cliniciansTo confirm eligibility of patients referred for screeningTo maintain the registry of screened patientsTo follow up LDCT results and confirm the ordering clinician and/or PCP is aware of these resultsTo ensure evaluation of any screen-detected nodules is appropriate (either by ordering the next test directly or by checking that the
appropriate test is ordered by the treating clinician)To intervene if the patient does not follow through with evaluation (at a bare minimum by contacting the ordering provider and often by
also contacting the patient directly to encourage adherence and to reschedule the test at a time convenient to the patient)To counsel and communicate with the patient about screeningInitial shared decision making about whether to undergo LDCT screeningNotification of resultsDiscussion of smoking cessation
Other associated personnel costsEffort of multidisciplinary steering committee members to govern programEffort of clinicians surrounding screening itself (e.g., radiology effort to conduct and read LDCT scans)Effort of program administrator (e.g., to schedule appointments, coordinate mailings)
Equipment costsLDCT scanner(s)—number needed depends on volume of patients screened
Information technology costsCosts associated with developing and maintaining registry (database) of screened patientsCosts associated with developing and maintaining any EMR-based toolsCosts associated with integrating structured reporting systemCosts associated with generating periodic reports of quality metrics from registry data
Marketing costsCosts associated with promoting the program within and outside of the medical center (e.g., grand rounds, direct-to-consumer
advertising, telephone access line, website)
Mailing costsMailings to patients (e.g., appointment reminders, results letters, educational brochures)
Costs associated with smoking cessation servicesCosts to produce (or obtain) and distribute smoking cessation brochuresTraining of personnel to deliver smoking cessation interventions (if offered directly through screening program)
Costs associated with downstream evaluation of screen-detected nodules and other abnormalitiesPET scanner(s)Clinic visits directly related to nodule evaluationBiopsy services (bronchoscopy, advanced bronchoscopic procedures [e.g., endobronchial ultrasound-guided transbronchial needle
aspiration], interventional radiology procedures [e.g., transthoracic needle biopsy], surgical biopsy)
Definition of abbreviations: EMR = electronic medical record; LDCT = low-radiation-dose computed tomography; PCP = primary care physician;PET = positron emission tomography.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 885

(2, 28). It is critical to educate and reassurelow-risk patients and their providers (20).Although verbal counseling may be ideal,some programs use personalized letterssupplemented by generic educationalbrochures (e.g., Consumer Reports/Choosing Wisely patient page [29]).Targeted feedback should be provided toclinicians who repeatedly refer low-riskindividuals for screening.
Deciding Whether to Screen:Shared Decision MakingCHEST/ATS Component 8: Patient andprovider education
Guidelines recommend (2–8), and CMSrequires (12), shared decision making—discussing the potential benefits and harmsof LDCT screening with patients andincorporating patient preferences. Thepurpose of shared decision making is not toconvince every patient to undergo LDCTscreening but rather to allow individuals toweigh trade-offs based on their personal riskprofiles and make informed choices aboutwhether LDCT screening is right for them. Itmay be informative for programs to monitorhow often eligible individuals are offeredshared decision making and how ofteninformed patients accept LDCT screening.
Designating and educating clinicians toperform shared decision making. Animportant consideration is who willperform shared decision making. Someprograms have tasked PCPs with shareddecision making at the time of referral forLDCT screening (19). The advantage isthat patients have a prior relationshipwith PCPs that may facilitate theseconversations. However, PCPs may be lessfamiliar with the nuances of LDCTscreening and have competing demandsduring visits (21, 33–35). Accordingly,some programs have empowered screeningcoordinators to perform shared decisionmaking (30). Health educators may helpengage patients in shared decision making(31). Of note, CMS requires that shareddecision making occur during an in-person visit with a physician, midlevelprovider, or clinical nurse specialist(Table 3) (12).
A critical early step is educating theclinician(s) who will conduct shareddecision making (20, 22). Clinicians shouldbe well-versed in the benefits and harms ofLDCT screening (Table 1) and how trade-offsvary depending on the patient’s personal riskprofile and comorbidities (24, 26). Important
elements to include in a conversation beforea screening decision is made (32) are thatnodules are commonly found (approximately25–50% of screening examinations [33]), thatmost (z95%) nodules detected by screeningare benign (1), and that the detection ofa lung nodule and its subsequent evaluationmay cause distress, physical complications, orother harms (17, 39–44).
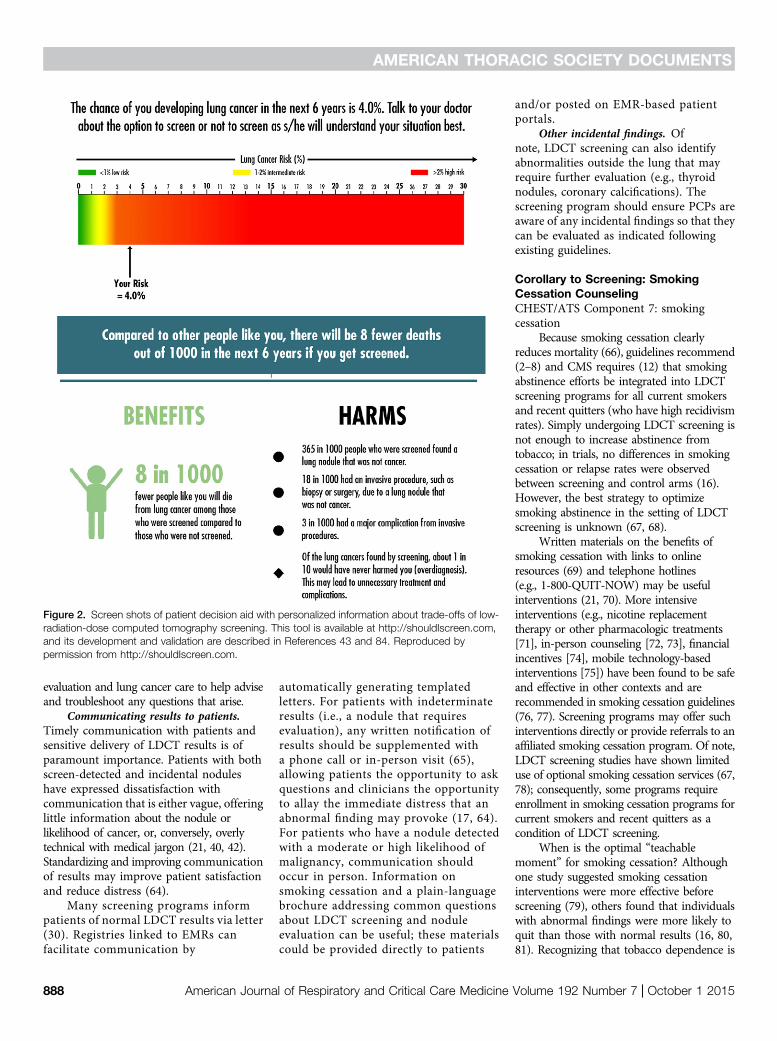
Available tools. Fortunately, there aretools to help clinicians remember therelevant facts during discussions withpatients (34), and CMS requires use of sucha tool to facilitate shared decision making(Table 3) (12). The American ThoracicSociety has developed a patient decisionaid, available at http://www.thoracic.org/patients/patient-resources/resources/decision-aid-lcs.pdf. Validated riskcalculators (24, 35–41) may be particularlyuseful to tailor the expected trade-offs ofLDCT screening to the individual and havebeen incorporated into web-based decisiontools (Figures 1 and 2). It is reasonable tosupplement verbal discussions with plainlanguage materials (21, 24, 25) or videodecision aids (42) the patient can review athome. Of note, these tools are still undergoingtesting (42, 43), and the best format fordecision tools remains unclear (44).
The Screening Process:Standardizing LDCT Screening andFollow-up of Abnormal FindingsCHEST/ATS Components 3: How the CT isperformed; 4: Lung nodule identification;5: Structured reporting
Standardizing several elements canimprove quality of care in LDCT screeningprograms (19).
LDCT performance. To minimizepatient harms, protocols to reduce radiationexposure have been developed, such as thetechnical specifications delineated by theAmerican College of Radiology and Societyof Thoracic Radiology (45). Per thesespecifications, screening scans should benoncontrast helical studies performed withradiation dose less than or equal to 3 mGy formost patients, acquired and viewed at lessthan or equal to 2.5-mm slice thickness (,1mm preferred). All technicians responsiblefor performing screening LDCT scans shouldbe trained in the protocol.
Structured reporting. Becauseinterpretation of LDCT results andrecommendations for follow-up can varybetween radiologists (46–48), and becauseradiologists’ recommendations are the
strongest predictor of nodule evaluationreceived (49), standardized reports thatprovide specific recommendations linked tothe findings (20–22) may improve care.To facilitate a standardized process, theAmerican College of Radiology developeda structured reporting system similar to thatused for mammography: the Lung ImagingReporting and Data System (Lung-RADS)(50). Lung-RADS categorizes LDCT findingsbased on likelihood of cancer and links eachcategory with specific recommendations.Although reducing false positives,Lung-RADS may decrease sensitivitycompared with NLST criteria, and its effectson clinical endpoints such as lung cancermortality are unknown (51, 52). Someprograms have established similar structuredreporting systems based on other noduleevaluation algorithms (21). Structuredreports may help promote guideline-concordant nodule evaluation (53). It maybe beneficial to perform a quality checkusing a training set of screening LDCTs toensure consistent application of thestructured reporting system, particularly ifradiologists who are not specifically trainedin thoracic imaging read screening LDCTs.
Evaluation of screen-detected nodules.CHEST/ATS Component 6: Lung nodulemanagement algorithms
Several guidelines and algorithms havebeen proposed for pulmonary noduleevaluation (4, 50, 54, 55). Adherence tothese algorithms can reduce resource useassociated with nodule evaluation and doesnot appear to worsen clinical outcomes (49,52). One approach being studied to riskstratify nodules and facilitate evaluation isvolumetric analysis (56, 57).
One of the biggest perceived barriers tosuccessful implementation of LDCTscreening programs is concern about whowill direct evaluation of screen-detectednodules. Although some early-adoptingsites defer nodule evaluation topulmonologists given their expertise, mostagreed that the volume could quicklyoverwhelm pulmonary workload (27).Many early-adopting programs havetasked PCPs with evaluation of small lungnodules (<8 mm), assisted (often heavily)by automated systems or a screeningcoordinator trained on nodule evaluationalgorithms (19, 58).
SUBCENTIMETER NODULES. Themajority of screen-detected pulmonarynodules will have a low likelihood ofmalignancy, and guidelines suggest that
AMERICAN THORACIC SOCIETY DOCUMENTS
886 American Journal of Respiratory and Critical Care Medicine Volume 192 Number 7 | October 1 2015

nodules less than or equal to 8 mm canbe safely followed with radiographicsurveillance without invasive testing (4, 50,54, 55). Assuming the nodule does notenlarge during surveillance, guidelinesdelineate straightforward algorithms ofserial LDCT scans at regular intervals,which can be followed by PCPs or otherclinicians not specifically trained inpulmonary medicine. Outreach andeducational presentations can enhance PCPcomfort with nodule evaluation algorithms.
HIGHER-RISK NODULES. For largerpulmonary nodules (.8 mm) or smallnodules that grow during surveillance,pulmonologists and other specialistsoften become involved in evaluation toassess the need for invasive testing.Many programs involved amultidisciplinary tumor board, ora dedicated pulmonary nodule reviewbetween radiology and pulmonology, toassist in decision making surrounding
evaluation of nodules with a higherlikelihood of cancer (20–22).
Adherence with follow-up. Regardless ofnodule size, it is essential to establishmechanisms to prevent loss to follow-up.Two such strategies are development ofregistries with data on all patients who haveundergone LDCT screening (a CMSrequirement [12]) and designation ofa screening program coordinator (58, 59).
REGISTRY. Registries help monitorrecommended follow-up, whether for repeatscreening in 1 year or earlier testing forevaluation of a screen-detected nodule(58, 60). Some programs are facilitating entryof patients into registries via automatedmethods to identify screen-detected nodulesthrough the EMR and/or by tasking theinterpreting radiologist with flagging positivescans (58, 61). However, even the mostadvanced EMR-based registries requirehuman review to check, maintain, and updatethe registry (58). The registry should ideally
contain information on patient and nodulecharacteristics, the recommended evaluation,adherence to evaluation, and test results (58).The registry should be maintained ina database that can be sorted to facilitateclinical care and quality monitoring.
COORDINATOR. Simply maintaininga registry is insufficient to ensure all patientsreceive appropriate care (62). Thus, itis important to have a clinician whoproactively directs, or at least monitorsand intervenes on, the screening andevaluation process (58), performing the coreprogrammatic functions in Table 4. Many sitesdesignate a midlevel provider or nurse toperform these activities (63); however, sitesmay opt to assign these responsibilities toa pulmonologist or other physician witha specific interest in LDCT screening. Thecoordinator should have unfettered access tothe clinical director(s) of the screeningprogram and an established relationship withthe specialists responsible for nodule
Figure 1. Screen shots of online calculator, developed by the Memorial Sloan Kettering Cancer Center, to predict personalized expected benefits of low-radiation-dose computed tomography screening. This tool is available at http://nomograms.mskcc.org/Lung/Screening.aspx, and the risk predictionmodel is supported by References 35–37. Reproduced by permission from http://nomograms.mskcc.org/Lung/Screening.aspx.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 887
evaluation and lung cancer care to help adviseand troubleshoot any questions that arise.
Communicating results to patients.Timely communication with patients andsensitive delivery of LDCT results is ofparamount importance. Patients with bothscreen-detected and incidental noduleshave expressed dissatisfaction withcommunication that is either vague, offeringlittle information about the nodule orlikelihood of cancer, or, conversely, overlytechnical with medical jargon (21, 40, 42).Standardizing and improving communicationof results may improve patient satisfactionand reduce distress (64).
Many screening programs informpatients of normal LDCT results via letter(30). Registries linked to EMRs canfacilitate communication by
automatically generating templatedletters. For patients with indeterminateresults (i.e., a nodule that requiresevaluation), any written notification ofresults should be supplemented witha phone call or in-person visit (65),allowing patients the opportunity to askquestions and clinicians the opportunityto allay the immediate distress that anabnormal finding may provoke (17, 64).For patients who have a nodule detectedwith a moderate or high likelihood ofmalignancy, communication shouldoccur in person. Information onsmoking cessation and a plain-languagebrochure addressing common questionsabout LDCT screening and noduleevaluation can be useful; these materialscould be provided directly to patients
and/or posted on EMR-based patientportals.
Other incidental findings. Ofnote, LDCT screening can also identifyabnormalities outside the lung that mayrequire further evaluation (e.g., thyroidnodules, coronary calcifications). Thescreening program should ensure PCPs areaware of any incidental findings so that theycan be evaluated as indicated followingexisting guidelines.
Corollary to Screening: SmokingCessation CounselingCHEST/ATS Component 7: smokingcessation
Because smoking cessation clearlyreduces mortality (66), guidelines recommend(2–8) and CMS requires (12) that smokingabstinence efforts be integrated into LDCTscreening programs for all current smokersand recent quitters (who have high recidivismrates). Simply undergoing LDCT screening isnot enough to increase abstinence fromtobacco; in trials, no differences in smokingcessation or relapse rates were observedbetween screening and control arms (16).However, the best strategy to optimizesmoking abstinence in the setting of LDCTscreening is unknown (67, 68).
Written materials on the benefits ofsmoking cessation with links to onlineresources (69) and telephone hotlines(e.g., 1-800-QUIT-NOW) may be usefulinterventions (21, 70). More intensiveinterventions (e.g., nicotine replacementtherapy or other pharmacologic treatments[71], in-person counseling [72, 73], financialincentives [74], mobile technology-basedinterventions [75]) have been found to be safeand effective in other contexts and arerecommended in smoking cessation guidelines(76, 77). Screening programs may offer suchinterventions directly or provide referrals to anaffiliated smoking cessation program. Of note,LDCT screening studies have shown limiteduse of optional smoking cessation services (67,78); consequently, some programs requireenrollment in smoking cessation programs forcurrent smokers and recent quitters as acondition of LDCT screening.
When is the optimal “teachablemoment” for smoking cessation? Althoughone study suggested smoking cessationinterventions were more effective beforescreening (79), others found that individualswith abnormal findings were more likely toquit than those with normal results (16, 80,81). Recognizing that tobacco dependence is
Figure 2. Screen shots of patient decision aid with personalized information about trade-offs of low-radiation-dose computed tomography screening. This tool is available at http://shouldIscreen.com,and its development and validation are described in References 43 and 84. Reproduced bypermission from http://shouldIscreen.com.
AMERICAN THORACIC SOCIETY DOCUMENTS
888 American Journal of Respiratory and Critical Care Medicine Volume 192 Number 7 | October 1 2015

a disease that requires repeated interventions,some programs offer interventions atmultiple time points: the initial referral forscreening, results delivery, and 3 to 4 weeksafter results delivery (20, 22).
One promising strategy may be to trainclinicians who discuss LDCT screening withpatients (e.g., screening coordinators) todeliver tailored smoking cessationinterventions (e.g., motivationalinterviewing, nicotine replacement therapy).Resources are available online to trainclinicians in these skills (82). It may be usefulto highlight to patients the link betweensmoking and findings from screeningLDCT, analogous to informing patients oftheir spirometric “lung age” as a tool topromote smoking cessation (16, 83).
Maintenance
CHEST/ATS Component 9: Data collectionPeriodic review of quality metrics can
help ensure screening programs are operatingas intended (58). The ATS and CHEST have
proposed quality metrics to be monitoredannually, including: (1) appropriateness ofwho is screened (>90% should meet criteria);(2) adherence with structured reporting bythe radiologist (>90% should use structuredreports); (3) appropriateness of noduleevaluation (tracking of how many patientsreceive full course of surveillance, how manyinvasive tests are performed and how manycomplications occur, how many cancersare diagnosed and their stages); and (4)adherence with smoking cessationinterventions (how many smokers wereoffered and participated in interventions)(11). These data can be collected andmaintained in the registry. If periodic reviewof these data reveals deficiencies, the steeringcommittee should make a plan for correctiveaction. Meanwhile, high performance onquality metrics can serve to reinforceenthusiasm for the program if shared withstaff and referring providers (19). Of note,CMS requires that data on all LDCTscreening performed at a site be reported to anational registry (12).
Conclusions
We have outlined pragmatic strategies toimplement comprehensive programs withfidelity to the LDCT screening interventionshown to be efficacious in the NLST.Recognizing that “one size does not fit all,”we have provided guidance on differentstrategies to achieve the nine corecomponents of effective screeningprograms (11) to allow sites to tailorprograms to fit their local context.Although we have not discussed explicitcost calculations, ensuring adequatepersonnel and resources are dedicated tothe screening program is critical todeveloping and sustaining high-quality,smoothly functioning programs and shouldnot be underestimated. The experience ofearly-adopting screening sites demonstratesthat the strategies outlined herein canproduce effective and successful programsthat are consistent with guidelinerecommendations for LDCT screening(20–22, 58). n
This official statement was prepared by an ad hoc subcommittee of the ATS and CHEST. The committee included representation from several ATS assemblies(Thoracic Oncology, Clinical Problems, Nursing, and Behavioral Sciences and Health Services Research). We also included a patient who underwent LDCTscreening (identified through the ATS Public Advisory Roundtable) and a medical consumer advocate representing the Center for Medical Consumers.
Members of the subcommittee are as follows:
RENDA SOYLEMEZ WIENER, M.D., M.P.H.(Chair)
MICHAEL K. GOULD, M.D., M.S. (Co-Chair)DOUGLAS A. ARENBERG, M.D.DAVID H. AU, M.D., M.S.WILLIAM C. BLACK, M.D.1
FRANK DETTERBECK, M.D., PH.D.1
KATHLEEN FENNIG, R.N.2
EDWARD HIRSCHOWITZ, M.D.1
JAMES JETT, M.D.1
LINDA KINSINGER, M.D., M.P.H.1
CARLA R. LAMB, M.D.PETER J. MAZZONE, M.D., M.P.H.DAVID E. MIDTHUN, M.D.MARYANN NAPOLI
3
DAVID E. OST, M.D.CHARLES A. POWELL, M.D.
M. PATRICIA RIVERA, M.D.CHRISTOPHER G. SLATORE, M.D., M.S.NICHOLE T. TANNER, M.D., M.S.C.R.ANIL VACHANI, M.D.JUAN P. WISNIVESKY, M.D., DR.P.H.SUE H. YOON, MSN, N.P.-C.1These individuals were members of thesubcommittee but were not members of thewriting committee.
2Patient representative.
3Center for Medical Consumers.
Author Disclosures: M.K.G. receivedresearch support paid to his institutionfrom Archimedes and is an author forUpToDate. P.J.M. has served on advisorycommittees for Oncimmune and Varianand receives research support paid to hisinstitution from Metabolomx and IntegratedDiagnostics. D.E.M. receives research
support paid to his institution fromIntegrated Diagnostics. C.A.P. served asa consultant for Pfizer. A.V. receivesresearch support paid to his institutionfrom Integrated Diagnostics, AllegroDiagnostics, Janssen Research &Development, and Transgenomic; andserved on the advisory committee forAllegro Diagnostics. J.P.W. is a member ofEHE International; served as a consultantfor Merck, IMS Health, Bristol-MyersSquibb, and Quintiles; and received researchsupport from Sanofi. R.S.W., D.A.A., D.H.A.,K.F., C.R.L., M.N., D.E.O., M.P.R., C.G.S.,N.T.T., and S.H.Y. reported no relevantcommercial relationships.
Acknowledgment: The authors also thank ATSstaff members John Harmon, Miriam Rodriguez,and Judy Corn, M.S.Ed. and CHEST staff memberJenny Nemkovich for their assistance withorganizing and facilitating committee logistics,meetings, and conference calls.
References
1. Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, FagerstromRM, Gareen IF, Gatsonis C, Marcus PM, Sicks JD; National Lung ScreeningTrial Research Team. Reduced lung-cancer mortality with low-dosecomputed tomographic screening. N Engl J Med 2011;365:395–409.
2. Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB. Screeningfor lung cancer. Diagnosis and management of lung cancer,3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e78S–e92S.
3. Moyer VA; U.S. Preventive Services Task Force. Screening for lungcancer: U.S. Preventive Services Task Force recommendationstatement. Ann Intern Med 2014;160:330–338.
4. National Comprehensive Cancer Network. NCCN clinical practiceguidelines in oncology (NCCN guidelines): lung cancer screening,version 1.2015. 2014 [accessed 2014 Dec 14]. Available from: http://www.nccn.org/professionals/physician_gls/pdf/lung_screening.pdf
5. Jaklitsch MT, Jacobson FL, Austin JH, Field JK, Jett JR, Keshavjee S,MacMahon H, Mulshine JL, Munden RF, Salgia R, et al. The AmericanAssociation for Thoracic Surgery guidelines for lung cancer screening using
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 889
low-dose computed tomography scans for lung cancer survivors andother high-risk groups. J Thorac Cardiovasc Surg 2012;144:33–38.
6. American Lung Association Lung Cancer Screening Committee. Providingguidance on lung cancer screening to patients and physicans. 2012[accessed 2015 Apr 13]. Available from: http://www.lung.org/lung-disease/lung-cancer/lung-cancer-screening-guidelines/lung-cancer-screening.pdf
7. Field JK, Smith RA, Aberle DR, Oudkerk M, Baldwin DR, Yankelevitz D,Pedersen JH, Swanson SJ, Travis WD, Wisbuba II, et al.; IASLC CTScreening Workshop 2011 Participants. International association forthe study of lung cancer computed tomography screening workshop2011 report. J Thorac Oncol 2012;7:10–19.
8. Wender R, Fontham ET, Barrera E Jr, Colditz GA, Church TR, Ettinger DS,Etzioni R, Flowers CR,Gazelle GS, Kelsey DK, et al. AmericanCancer Societylung cancer screening guidelines. CA Cancer J Clin 2013;63:107–117.
9. Harris RP, Sheridan SL, Lewis CL, Barclay C, Vu MB, Kistler CE, Golin CE,DeFrank JT, Brewer NT. The harms of screening: a proposed taxonomy andapplication to lung cancer screening. JAMA Intern Med 2014;174:281–285.
10. Humphrey LL, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP,Zakher B, Fu R, Slatore CG. Screening for lung cancer with low-dosecomputed tomography: a systematic review to update the US PreventiveServices Task Force recommendation. Ann Intern Med 2013;159:411–420.
11. Mazzone P, Powell CA, Arenberg D, Bach P, Detterbeck F, Gould MK,Jaklitsch MT, Jett J, Naidich D, Vachani A, et al. Componentsnecessary for high-quality lung cancer screening: American Collegeof Chest Physicians and American Thoracic Society PolicyStatement. Chest 2015;147:295–303.
12. Centers for Medicare & Medicaid Services. Decision memo for screeningfor lung cancer with low dose computed tomography (LDCT) (CAG-00439N). 2015 [accessed 2015 Feb 21]. Available from: http://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=274&NcaName=Screening1for1Lung1Cancer1with1Low1Dose1Computed1Tomography1(LDCT)&MEDCACId=68&IsPopup=y&bc=AAAAAAAAAgAAAA%3d%3d&
13. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impactof health promotion interventions: the RE-AIM framework.Am J Public Health 1999;89:1322–1327.
14. Rycroft-Malone J, Kitson A, Harvey G, McCormack B, Seers K, TitchenA, Estabrooks C. Ingredients for change: revisiting a conceptualframework. Qual Saf Health Care 2002;11:174–180.
15. Bach PB, Mirkin JN, Oliver TK, Azzoli CG, Berry DA, Brawley OW, Byers T,Colditz GA, Gould MK, Jett JR, et al. Benefits and harms of CT screeningfor lung cancer: a systematic review. JAMA 2012;307:2418–2429.
16. Slatore CG, Baumann C, Pappas M, Humphrey LL. Smoking behaviorsamong patients receiving computed tomography for lung cancerscreening: systematic review in support of the U.S. PreventiveServices Task Force. Ann Am Thorac Soc 2014;11:619–627.
17. Slatore CG, Sullivan DR, Pappas M, Humphrey LL. Patient-centeredoutcomes among lung cancer screening recipients with computedtomography: a systematic review. J Thorac Oncol 2014;9:927–934.
18. American Academy of Family Physicians. Clinical Preventive Servicerecommendation: lung cancer. 2013 [accessed 2014 Sept 24].Available from: http://www.aafp.org/patient-care/clinical-recommendations/all/lung-cancer.html
19. McKee A, McKee B, Wald C, Lamb C, Hesketh PJ, Flacke S. Rescuelung, rescue life: translating the NLST results into clinical practice.Oncology Issues 2014;Mar–Apr:20–29.
20. McKee BJ, McKee AB, Flacke S, Lamb CR, Hesketh PJ, Wald C. Initialexperience with a free, high-volume, low-dose CT lung cancerscreening program. J Am Coll Radiol 2013;10:586–592.
21. Mazzone P. The rationale for, and design of, a lung cancer screeningprogram. Cleve Clin J Med 2012;79:337–345.
22. Arenberg D, Kazerooni EA. Setting up a lung cancer screeningprogram. J Natl Compr Canc Netw 2012;10:277–285.
23. Bach P. CT scam: don’t believe the hype about lung-cancer screenings.2010 [accessed 2014 Dec 8]. Available from: http://www.slate.com/articles/health_and_science/medical_examiner/2010/11/ct_scam.html
24. Kovalchik SA, Tammemagi M, Berg CD, Caporaso NE, Riley TL, KorchM, Silvestri GA, Chaturvedi AK, Katki HA. Targeting of low-doseCT screening according to the risk of lung-cancer death. N EnglJ Med 2013;369:245–254.
25. Bach PB, Gould MK. When the average applies to no one: personalizeddecision making about potential benefits of lung cancer screening.Ann Intern Med 2012;157:571–573.
26. Pinsky PF, Church TR, Izmirlian G, Kramer BS. The National LungScreening Trial: results stratified by demographics, smoking history,and lung cancer histology. Cancer 2013;119:3976–3983.
27. Federman DG, Kravetz JD, Lerz KA, Akgun KM, Ruser C, Cain H, AndersonEF, Taylor C. Implementation of an electronic clinical reminder toimprove rates of lung cancer screening. Am J Med 2014;127:813–816.
28. Wiener RS, Ouellette DR, Diamond E, Fan VS, Maurer JR, Mularski RA,Peters JI, Halpern SD; American Thoracic Society; American College ofChest Physicians. An official American Thoracic Society/AmericanCollege of Chest Physicians policy statement: the Choosing Wisely topfive list in adult pulmonary medicine. Chest 2014;145:1383–1391.
29. Consumer Reports. CT scans to find lung cancer: when you needthem–and when you don’t. 2014 [accessed 2014 Dec 1]. Availablefrom:http://www.choosingwisely.org/doctor-patient-lists/ct-scans-to-find-lung-cancer-in-smokers/
30. Wiener RS, Koppelman E, Slatore CG, Clark JA. Patients’ impressionsof communication with their clinicians surrounding low-dose CT lungcancer screening: a qualitative study [abstract]. Am J Respir CritCare Med 2015;191:A6120.
31. Stacey D, Kryworuchko J, Bennett C, Murray MA, Mullan S, Legare F.Decision coaching to prepare patients for making health decisions:a systematic review of decision coaching in trials of patient decisionAIDS. Med Decis Making 2012;32:E22–E33.
32. Presidential Commission for the Study of Bioethical Issues. Anticipate andcommunicate: ethical management of incidental and secondary findingsin the clinical, research, and direct-to-consumer contexts. 2013[accessed 2014 Dec 1]. Available from: http://bioethics.gov/node/3183
33. Wahidi MM, Govert JA, Goudar RK, Gould MK, McCrory DC. Evidencefor the treatment of patients with pulmonary nodules: when is itlung cancer? ACCP evidence-based clinical practice guidelines(2nd edition). Chest 2007;132:94S–107S.
34. National Cancer Institute. Patient and physician guide: NationalLung Screening Trial (NLST) [accessed 2015 Apr 13].Available from: http://www.cancer.gov/newscenter/qa/2002/NLSTstudyGuidePatientsPhysicians
35. Bach PB, Elkin EB, Pastorino U, Kattan MW, Mushlin AI, Begg CB,Parkin DM. Benchmarking lung cancer mortality rates in current andformer smokers. Chest 2004;126:1742–1749.
36. Bach PB, Kattan MW, Thornquist MD, Kris MG, Tate RC, Barnett MJ,Hsieh LJ, Begg CB. Variations in lung cancer risk among smokers.J Natl Cancer Inst 2003;95:470–478.
37. Cronin KA, Gail MH, Zou Z, Bach PB, Virtamo J, Albanes D. Validationof a model of lung cancer risk prediction among smokers. J NatlCancer Inst 2006;98:637–640.
38. Spitz MR, Hong WK, Amos CI, Wu X, Schabath MB, Dong Q, Shete S,Etzel CJ. A risk model for prediction of lung cancer. J Natl CancerInst 2007;99:715–726.
39. Tammemagi MC, Katki HA, HockingWG, Church TR, Caporaso N, Kvale PA,Chaturvedi AK, Silvestri GA, Riley TL, Commins J, et al. Selection criteriafor lung-cancer screening. N Engl J Med 2013;368:728–736.
40. Cassidy A, Myles JP, van Tongeren M, Page RD, Liloglou T, Duffy SW,Field JK. The LLP risk model: an individual risk prediction model forlung cancer. Br J Cancer 2008;98:270–276.
41. McRonald FE, Yadegarfar G, Baldwin DR, Devaraj A, Brain KE, Eisen T,Holemans JA, Ledson M, Screaton N, Rintoul RC, et al. The UK LungScreen (UKLS): demographic profile of first 88,897 approachesprovides recommendations for population screening. Cancer PrevRes (Phila) 2014;7:362–371.
42. Volk RJ, Linder SK, Leal VB, Rabius V, Cinciripini PM, Kamath GR, MundenRF, Bevers TB. Feasibility of a patient decision aid about lung cancerscreeningwith low-dose computed tomography.PrevMed 2014;62:60–63.
43. Lau YK, Caverly TJ, Cherng ST, Cao P, West M, Arenberg D, Meza R.Development and validation of a personalized, web-based decisionaid for lung cancer screening using mixed methods: a studyprotocol. JMIR Res Protoc 2014;3:e78.
44. Lillie SE, Partin MR, Rice K, Fabbrini AE, Greer NL, Patel S, MacDonaldR, Rutks I, Wilt TJ. The effects of shared decision making on cancerscreening: a systematic review. 2014. VA ESP Project No. #09-009.
AMERICAN THORACIC SOCIETY DOCUMENTS
890 American Journal of Respiratory and Critical Care Medicine Volume 192 Number 7 | October 1 2015

45. Kazerooni EA, Austin JH, Black WC, Dyer DS, Hazelton TR, Leung AN,McNitt-Gray MF, Munden RF, Pipavath S; American College of Radiology;Society of Thoracic Radiology. ACR-STR practice parameter for theperformance and reporting of lung cancer screening thoracic computedtomography (CT): 2014 (Resolution 4). J Thorac Imaging 2014;29:310–316.
46. Gierada DS, Pilgram TK, Ford M, Fagerstrom RM, Church TR, Nath H,Garg K, Strollo DC. Lung cancer: interobserver agreement oninterpretation of pulmonary findings at low-dose CT screening.Radiology 2008;246:265–272.
47. Pinsky PF, Gierada DS, Nath PH, Kazerooni E, Amorosa J. Nationallung screening trial: variability in nodule detection rates in chest CTstudies. Radiology 2013;268:865–873.
48. Singh S, Pinsky P, Fineberg NS, Gierada DS, Garg K, Sun Y, Nath PH.Evaluation of reader variability in the interpretation of follow-up CTscans at lung cancer screening. Radiology 2011;259:263–270.
49. Wiener RS, Gould MK, Slatore CG, Fincke BG, Schwartz LM, WoloshinS. Resource use and guideline concordance in evaluation ofpulmonary nodules for cancer: too much and too little care. JAMAIntern Med 2014;174:871–880.
50. American College of Radiology. Lung CT screening reporting anddata system (Lung-RADS) [accessed 2015 Apr 13]. Available from:http://www.acr.org/Quality-Safety/Resources/LungRADS
51. Pinsky PF, Gierada DS, Black W, Munden R, Nath H, Aberle D, KazerooniE. Performance of Lung-RADS in the national lung screening trial:a retrospective assessment. Ann Intern Med 2015;162:485–491.
52. McKee BJ, Regis SM, McKee AB, Flacke S, Wald C. Performance ofACR Lung-RADS in a clinical CT lung screening program. J Am CollRadiol 2015;12:273–276.
53. Woloshin S, Schwartz LM, Dann E, Black WC. Using radiology reportsto encourage evidence-based practice in the evaluation of small,incidentally detected pulmonary nodules: a preliminary study.Ann Am Thorac Soc 2014;11:211–214.
54. MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, Naidich DP, PatzEF Jr, Swensen SJ; Fleischner Society. Guidelines for management ofsmall pulmonary nodules detected on CT scans: a statement from theFleischner Society. Radiology 2005;237:395–400.
55. Gould MK, Donington J, Lynch WR, Mazzone PJ, Midthun DE, NaidichDP, Wiener RS. Evaluation of individuals with pulmonary nodules:when is it lung cancer? Diagnosis and management of lung cancer,3rd ed: American College of Chest Physicians evidence-basedclinical practice guidelines. Chest 2013;143:e93S–120S.
56. Horeweg N, van Rosmalen J, Heuvelmans MA, van der Aalst CM,Vliegenthart R, Scholten ET, ten Haaf K, Nackaerts K, Lammers JW,Weenink C, et al. Lung cancer probability in patients with CT-detectedpulmonary nodules: a prespecified analysis of data from the NELSONtrial of low-dose CT screening. Lancet Oncol 2014;15:1332–1341.
57. Horeweg N, Scholten ET, de Jong PA, van der Aalst CM, Weenink C,Lammers JW, Nackaerts K, Vliegenthart R, ten Haaf K, Yousaf-KhanUA, et al. Detection of lung cancer through low-dose CT screening(NELSON): a prespecified analysis of screening test performanceand interval cancers. Lancet Oncol 2014;15:1342–1350.
58. Kinsinger LS, Atkins D, Provenzale D, Anderson C, Petzel R.Implementation of a new screening recommendation in health care:the Veterans Health Administration’s approach to lung cancerscreening. Ann Intern Med 2014;161:597–598.
59. Alsamarai S, Yao X, Cain HC, Chang BW, Chao HH, Connery DM, DengY, Garla VN, Hunnibell LS, Kim AW, et al. The effect of a lung cancercare coordination program on timeliness of care. Clin Lung Cancer2013;14:527–534.
60. Goulart BH, Ramsey SD. Moving beyond the national lung screeningtrial: discussing strategies for implementation of lung cancerscreening programs. Oncologist 2013;18:941–946.
61. McClure MA, Rice KL, Lindsey B. Novel automated lung noduletracking system: 5 year preliminary results [abstract]. Am J RespirCrit Care Med 2013;187:A2349.
62. Moseson EM, Slatore CG, Golden SE. Adherence to Fleischner Societyguidelines among veterans with pulmonary nodules in a clinicalregistry [abstract]. Am J Respir Crit Care Med 2014;189:A2251.
63. Hunnibell LS, Slatore CG, Ballard EA. Foundations for lung nodulemanagement for nurse navigators. Clin J Oncol Nurs 2013;17:525–531.
64. Slatore CG, Golden SE, Ganzini L, Wiener RS, Au DH. Distress andpatient-centered communication among veterans with incidental(not screen-detected) pulmonary nodules: a cohort study. Ann AmThorac Soc 2015;12:184–192.
65. Wiener RS, Gould MK, Woloshin S, Schwartz LM, Clark JA. What doyou mean, a spot?: a qualitative analysis of patients’ reactions todiscussions with their physicians about pulmonary nodules.Chest 2013;143:672–677.
66. Gellert C, Schottker B, Brenner H. Smoking and all-cause mortality inolder people: systematic review and meta-analysis. Arch Intern Med2012;172:837–844.
67. van der Aalst CM, de Koning HJ, van den Bergh KA, Willemsen MC,van Klaveren RJ. The effectiveness of a computer-tailored smokingcessation intervention for participants in lung cancer screening:a randomised controlled trial. Lung Cancer 2012;76:204–210.
68. Clark MM, Cox LS, Jett JR, Patten CA, Schroeder DR, Nirelli LM,Vickers K, Hurt RD, Swensen SJ. Effectiveness of smoking cessationself-help materials in a lung cancer screening population. LungCancer 2004;44:13–21.
69. Folan P, Massucci D; Tobacco Control Committee of the AmericanThoracic Society. American Thoracic Society series on tobacco:resources to help you stop using tobacco [accessed 2015 Apr 13].Available from: http://www.thoracic.org/patients/patient-resources/resources/resources-stop-using-tobacco.pdf
70. Stead LF, Hartmann-Boyce J, Perera R, Lancaster T. Telephonecounselling for smoking cessation. Cochrane Database Syst Rev2013;8:CD002850.
71. Cahill K, Stevens S, Perera R, Lancaster T. Pharmacologicalinterventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev 2013;5:CD009329.
72. Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J,Lancaster T. Physician advice for smoking cessation. CochraneDatabase Syst Rev 2013;5:CD000165.
73. Stead LF, Lancaster T. Behavioural interventions as adjuncts topharmacotherapy for smoking cessation. Cochrane Database SystRev 2012;12:CD009670.
74. Volpp KG, Troxel AB, Pauly MV, Glick HA, Puig A, Asch DA, Galvin R, ZhuJ, Wan F, DeGuzman J, et al. A randomized, controlled trial of financialincentives for smoking cessation. N Engl J Med 2009;360:699–709.
75. Whittaker R, McRobbie H, Bullen C, Borland R, Rodgers A, Gu Y.Mobile phone-based interventions for smoking cessation. CochraneDatabase Syst Rev 2012;11:CD006611.
76. Clinical Practice Guideline Treating Tobacco Use and Dependence2008 Update Panel, Liaisons, and Staff. A clinical practice guidelinefor treating tobacco use and dependence: 2008 update. A U.S.Public Health Service report. Am J Prev Med 2008;35:158–176.
77. Leone FT, Evers-Casey S, Toll BA, Vachani A. Treatment of tobaccouse in lung cancer. Diagnosis and management of lung cancer, 3rded: American College of Chest Physicians evidence-based clinicalpractice guidelines. Chest 2013;143:e61S–e77S.
78. MacRedmond R, McVey G, Lee M, Costello RW, Kenny D, Foley C,Logan PM. Screening for lung cancer using low dose CT scanning:results of 2 year follow up. Thorax 2006;61:54–56.
79. Ferketich AK, Otterson GA, King M, Hall N, Browning KK, Wewers ME.A pilot test of a combined tobacco dependence treatment and lungcancer screening program. Lung Cancer 2012;76:211–215.
80. Tammemagi MC, Berg CD, Riley TL, Cunningham CR, Taylor KL.Impact of lung cancer screening results on smoking cessation.J Natl Cancer Inst 2014;106:dju084.
81. Taylor KL, Cox LS, Zincke N, Mehta L, McGuire C, Gelmann E. Lungcancer screening as a teachable moment for smoking cessation.Lung Cancer 2007;56:125–134.
82. Smoking Cessation Leadership Center. Tobacco cessation education:a training program for faculty [accessed 2015 Apr 13]. Available from:http://smokingcessationleadership.ucsf.edu/webinars/tobacco-cessation-education
83. Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rateof telling patients their lung age: the Step2quit randomised controlledtrial. BMJ 2008;336:598–600.
84. Lau YK, Caverly TJ, Cherng ST, Cao P, West M, Arenberg DA, Meza R.Improving lung cancer screening decision-making througha personalized, web-based decision aid. Am J Prev Med (In press)
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 891