an a plastic anemia cp
TRANSCRIPT
Objectives
Topic description: This topic deals on the discussion of aplastic anemia. It covers an overview of this type of anemia, the anatomy and physiology of the hematologic system, analysis of our client’s clinical manifestations, physical assessment findings, client’s growth and development, the pathophysiology of our client’s condition, and the nursing diagnoses with their corresponding interventions and outcomes of care.
Central Objective: At the end of the presentation, the listeners will gain knowledge, develop skills and cultivate positive attitudes in caring for patients with aplastic anemia.
Specific Objectives: At the end of this case presentation, the listeners shall:
State the formed elements of blood and its corresponding functions
Identify the expected developmental tasks and roles of patients in the school-age and early adolescent years
Explain the predisposing factors of aplastic anemia
Detect signs and symptoms of aplastic anemia
Trace the pathophysiology correctly
Review nursing principles and concepts learned during the lecture classes.
Apply the nursing concepts in the care of the client.
Recognize interventions appropriate in taking care of patients with aplastic anemia
Evaluate the effectiveness of the nursing interventions done in taking care of patients with aplastic anemia
1

A variety of blood cells course through the bloodstream — red blood cells, white blood cells and platelets. All are important to the
health of many people. Red blood cells carry oxygen, white blood cells fight infection, and platelets help the blood to clot. In aplastic
anemia, the body stops producing enough new blood cells. This means a person is fatigued and at higher risk of infections and
uncontrolled bleeding. A rare and serious condition, aplastic anemia can develop at any age. Aplastic anemia’s symptoms result from a
shortage of one or more types of blood cells and it can occur suddenly or develop slowly over weeks or months. The illness may be brief, or
it may become chronic. Treatment for aplastic anemia may include medications, blood transfusions or a bone marrow transplant. Once
considered nearly always fatal, aplastic anemia has a much better prognosis today, thanks to advances in treatment.
Unfortunately, there's no prevention for most cases of aplastic anemia. However, avoiding exposure to insecticides, herbicides,
organic solvents, paint removers and other toxic chemicals may lower the risk of the disease. This is especially important if a person
already had aplastic anemia that was caused by toxic chemicals. Exposure to the same compound a second time may cause the condition
to return.
However, in our patient’s case, he needs a compatible donor for his blood type which is A+. He needed blood transfusions so as to
improve circulation and to bring back the normal functioning of his hematologic system.. Because of financial constraints, they were not
able to secure all the required number of blood bags to be transfused so they have to remain in the hospital. Our patient’s history is very
vague for us to trace the pathophysiology of his condition. We really dig deep within just to know the past illnesses, medications, and daily
activities, and even the heredofamilial diseases that he could acquire from his parents. Unluckily, we found no exact evidence or proof for
the existence of his condition.
2

As nurses, we have to educate our client regarding the importance of self care to prevent complications. We must teach him to avoid
excessive exercise because his condition can cause fatigue and shortness of breath. Next, avoiding contact sports because of the risk of
bleeding and observe practices to avoid infections such as washing hands. Since aplastic anemia is a very serious condition that could lead
to another problem if not treated, prompt intervention is necessary to prevent its further complications. Medical management and
supportive therapy is necessary to improve the prognosis of the condition.
DEMOGRAPHIC DATA
Name: Pajunar, Jerome P. Nationality: Filipino Sex: male
Age: 13 years and 1 month old Address: Canaway, Siaton, Negros Oriental Birth place: Siaton, Negros Oriental
Birth date: March 14, 1995 Religion: Roman Catholic Room No#: reverse isolation room
Father’s Name: Uldarico Pajunar Mother’s Name: Vicenta Pahayat Pajunar Height: 148 cm
Year level: incoming grade 4 student Admitted on: April 16, 2008 at 3:10 pm Weight: 27 kgs
Doctor-in-charge: Dr. Gutierrez
History of present illness:
1 week prior to admission, body malaise was noted followed by pallor on the extremities. Episodes of fainting were experienced while in
school. Experienced nose bleeds and gum bleeds 10 days PTA. Factors that have aggravated his condition were his constant work in the
household and late sleeping during the night because of discos. Consulted to Dr. Uy and was referred to NOPH for blood transfusion.
Chief Complaints: pallor, fainting, and body malaise noted 1 week PTA, with epistaxis and gum bleeding 10 days PTA
Health history:
3

Medication: Paracetamol, Neozep, Medicol, and antitussives
Allergies: no known allergies
Smoke, Alcohol & drugs: haven’t tried smoking, drinking alcohol or intake of drugs
Family illness: no heredofamilial disease
Immunizations: completed all immunization doses except for MMR
Childhood illnesses: measles, mumps and chicken pox
Injuries: knee injury due to vehicular accident when he was 10 y.o.
Accidents: vehicular accident when he was 10 y.o.
Hospitalization: has been admitted to the hospital last 1st week of March due to pallor on the extremities, lips and muscle weakness
4

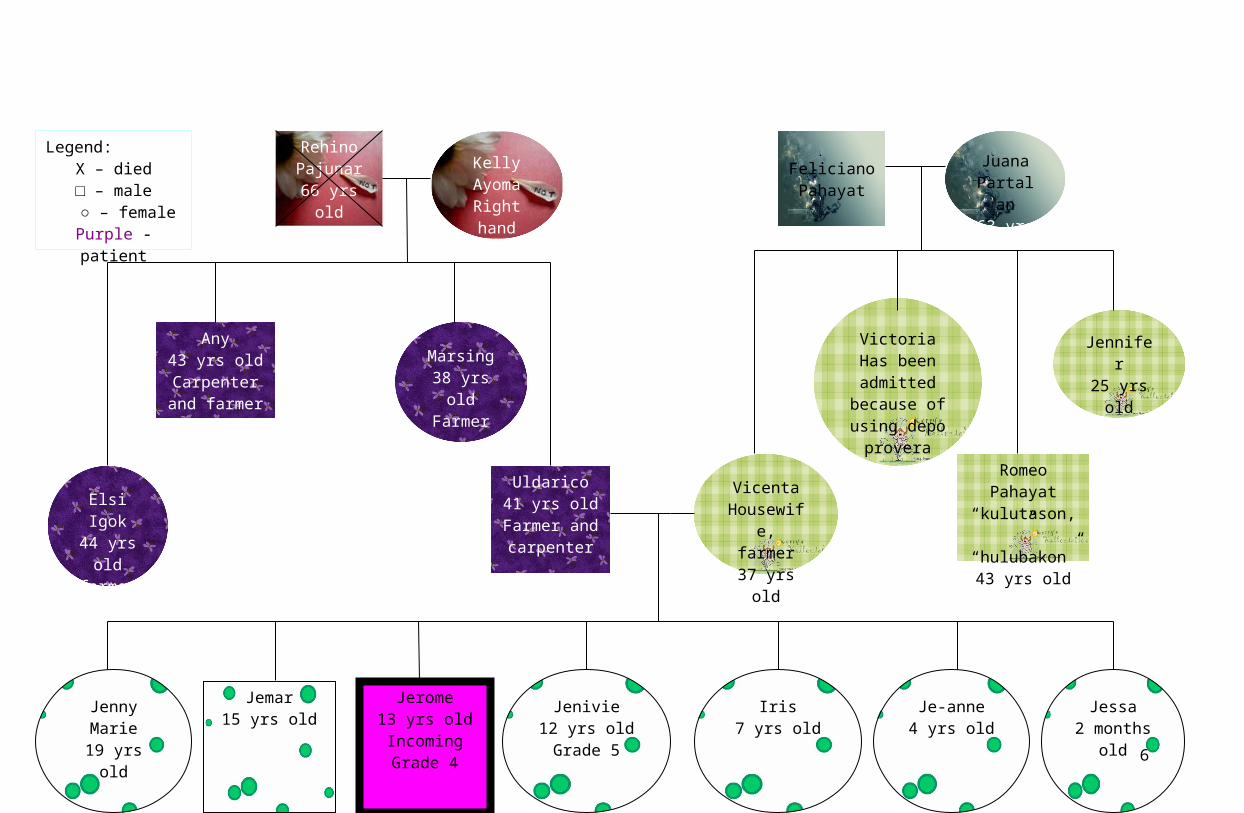
Rehino Pajunar
66 yrs old Died
because of ulcer
Any43 yrs old
Carpenter and farmer
Feliciano Pahayat
Jerome13 yrs old
Incoming Grade 4
Uldarico41 yrs old
Farmer and carpenter
Romeo Pahayat“kulutason,” “hulubakon”
43 yrs old
Jenivie12 yrs oldGrade 5
Iris7 yrs old
Elsi Igok44 yrs old
farmer
Jennifer25 yrs old
Juana Partalan
63 yrs old
Marsing38 yrs old
Farmer
VictoriaHas been admitted
because of using depo
provera
Kelly Ayoma
Right hand got burned68 yrs old
VicentaHousewife,
farmer37 yrs old
Jenny Marie19 yrs old
Jemar15 yrs old
Je-anne4 yrs old
Jessa2 months
old
Legend:X – died□ – male
○ – femalePurple - patient
5
Growth and Development of a school age transition to
adolescence
Normal growth and development Manifested by the client
Biological Development:
Rapidly, accelerating growth
Body proportion is slimmer look with longer legs, and a low center of gravity. These proportions make climbing, bicycle riding, and other activities easier.
Double their strength and physical capabilities.
Loose tooth stage or primary teeth are lost and ugly duckling stage where permanent teeth starts to grow, 28 sets of teeth
Fewer stomach upsets, increase stomach capacity, bladder capacity increases, heart and respiratory rates steadily decrease and blood pressure increases
Secondary sex characteristics have appeared: weight increases,
Has grown fast as the mother verbalized and that he is even taller than his older brother Jemar and has a height of 14 8 cm
Looks slim, with long lower extremities. Likes to climb trees and bicycle riding, and usually does it after school to play with other playmates at home.
At this time, he is weak and can not do household chore and play intensively because he easily gets tired and dizzy
No tooth was lost but most of the right and left molar teeth are decayed and mostly experience toothache
Eat small amount of food and sometimes vomits the food. Urinates 6 to 7 times per day. Heart rate is 102 beats per min, respiratory rate is 28 cpm and blood pressure is 120/70 mmHg
Weight has slightly increased due to poor intake of food. Fine strands of
6

pubic hair starts to appear, sebaceous gland secretion increases, and respiration increases
Psychosocial Development:
Identity vs Role Confusion (Erikson)
Accepting their changed body image
Establishing a value system or what kind of person they want to be
Develop a stable, coherent picture of oneself
Learn from others what it is they ought to keep doing and what it is they want to change
Cognitive Development:
Concrete operational Thought (Piaget)
Able to reason through any problem that they can actually visualize
Decentering, Accommodation, Conservation, class inclusion
hair start to appear in the pubic area, increased in sebaceous gland secretion, respiration increased due to lack of O2 supply in the body parts because of low RBC count
Right now changes in his body are still on the run so he is still trying to accept the changes in his body
He wants to be a doctor someday to help the sick people like him right now and to help his family in their finances
Right now, for him, he is sick and he needs treatment to be cured. He considers his past experiences that triggered him to be like what he is right now and he wants to be cured so that he could help his family and continue schooling.
Sometimes asks his parents about right doings and changes his bad attitude if reprimanded by parents.
Reasons about why they lack financial resources and tries to convince his mother about the solution of going to the governor to ask for help for the finances in the hospital
Able to project his self to others situations, like for example, being in the shoes of his parents. He really did understand why it is not easy for them to provide all the daily needs for their family. He was also able to adapt to the happenings to fit what is perceived and understand that there are some reasons why people do things and knows to identify changes and
7
Explores newfound ability for limited abstract thought
Formal Operational Thinking (Piaget)
Able to think in abstract terms, thinks about possibilities through hypotheses
Using a future-time perspective
Moral Development:
Preconventional Reasoning (Kohlberg)
Able to judge and act by intentions rather than consequences. Rules and judgments become less absolute and authoritarian and begin to be more on needs and desires of others.
Take into account a different point of view to make judgment
Conventional Reasoning
Absolute moral guidelines are seen to emanate from authorities such as parents or teachers.
able to differentiate it
When he was at home, he is observant of his uncle making furniture so he tries to apply it and was able to complete the task even not that good.
Sometimes judges immediately when he cannot understand or not able to perceive it correctly and do not think of possibilities
Thinks about his family and said that he want to finish studying to support his family
Able to do things which he wants to do but is still a little afraid if does something wrong because of the punishment that his parents would do to him. Use of judgment is appropriate and thinks of others rather than himself as he verbalized that “I felt sad because now that I’m here in the hospital, my parents expenses are increasing each day. I really wanted to go home to have no problem at all.”
He does not do judgment directly, listens or observe the opposite side before he judges, in cases of friendship conflict.
He abides by the parent’s rules and learned to work or live with the rules of the parent and his family by doing household chores before playing outside
8
Spiritual Development:
They picture God as human
View illness or injury as a punishment for a real or imagined misdeed.
Differentiate natural and supernatural
Their petitions to their God in prayers tend to be very tangible and is less concerned when prayers are less answered
Language Development:
Able to apply minimum-distance principle (ability to think about language and to comment on its properties)
Provide directive that others can correctly interpret without visual data
Able to think about quality of their own and other’s speech and to evaluate and clarify messages
Social Development:
Seeks peer affiliations to counter instability generated by rapid change
Upsurge of close, idealized friendships with members of the same sex
Believes in God and that He would heal his disease and prays to him fervently in order to be heard
Doesn’t view that his condition a punishment but views but it as a trial that he needs to overcome and is very positive that the God he believes in would heal him
Can differentiate between facts and fiction stories and able to identify fiction movies. “I believe in God even he if I haven’t seen him” as he verbalized
Because of lack of money to supply the medication and support persons to help in the finances, he puts his trust to God and offers his life to him as he verbalized
Able to appreciate jokes and riddles and easily laugh at double meaning words
Can provide direction properly when he was asked about how far was the place where her father worked
Asks about words of double meaning to elaborate more and sometimes laugh at his mistakes as he mispronounces words and correct it or ask for correction
Talks to peers and to mother about the changes in his body
Most of his friends are boys and he would hang out with them after school and loves to go to disco with them
9
No major conflict over parental control Follows rules made or implemented by the parents but sometimes violate them but talks to parents about it and settles it
Functional Health Patterns
Usual Function Patterns Initial Appraisal Ongoing Appraisal
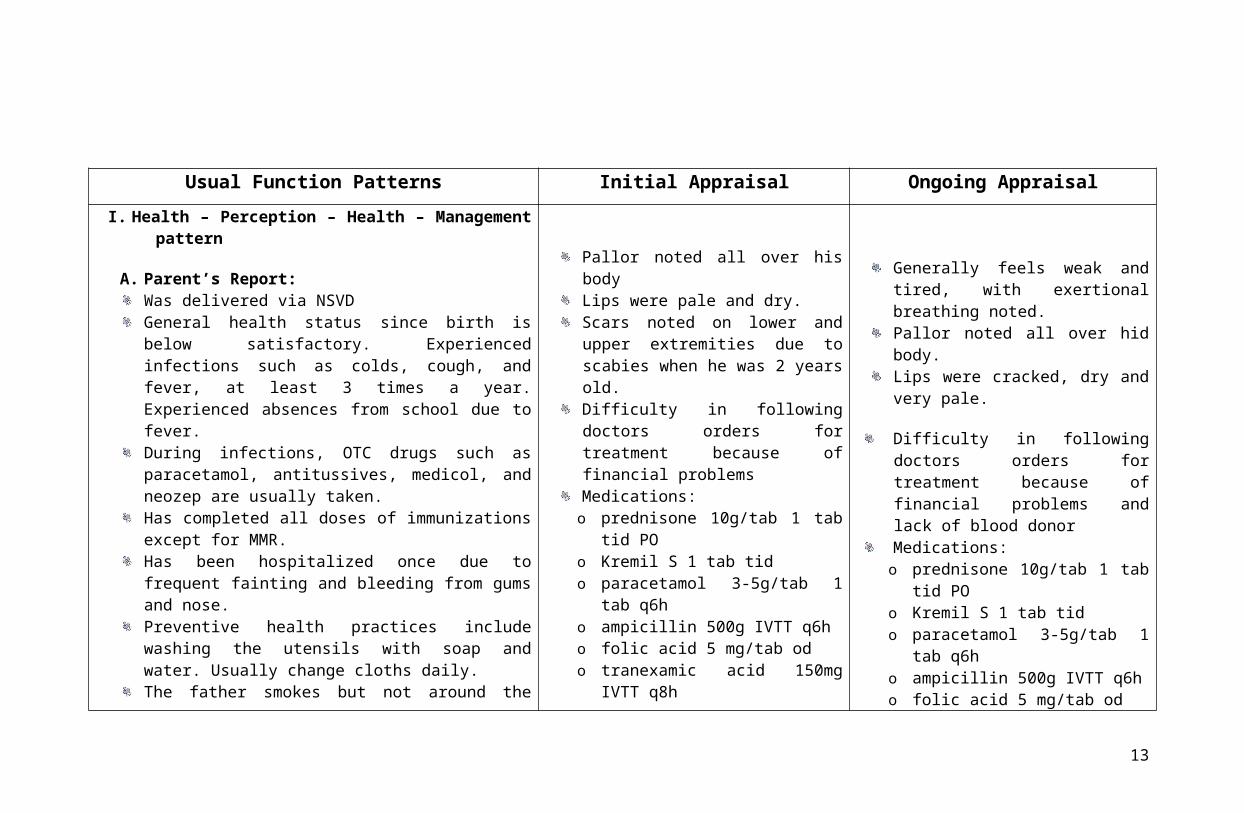
I. Health – Perception – Health – Management pattern
A. Parent’s Report:Was delivered via NSVDGeneral health status since birth is below satisfactory. Experienced infections such as colds, cough, and fever, at least 3 times a year. Experienced absences from school due to fever.During infections, OTC drugs such as paracetamol, antitussives, medicol, and neozep are usually taken.Has completed all doses of immunizations except for MMR.Has been hospitalized once due to frequent fainting and bleeding from gums and nose.Preventive health practices include washing the utensils with soap and water. Usually change cloths daily.The father smokes but not around the child.A scar is present at the left knee due to vehicular accident experienced at age 10.Sharp objects and medicines at home are kept out of children’s reach.
Pallor noted all over his bodyLips were pale and dry. Scars noted on lower and upper extremities due to scabies when he was 2 years old.Difficulty in following doctors orders for treatment because of financial problemsMedications:o prednisone 10g/tab 1 tab tid POo Kremil S 1 tab tido paracetamol 3-5g/tab 1 tab q6ho ampicillin 500g IVTT q6ho folic acid 5 mg/tab odo tranexamic acid 150mg IVTT q8ho phytomenadione 1 ampule IVTT statoLaboratory Values
Generally feels weak and tired, with exertional breathing noted.Pallor noted all over hid body.Lips were cracked, dry and very pale.
Difficulty in following doctors orders for treatment because of financial problems and lack of blood donorMedications:o prednisone 10g/tab 1 tab tid POo Kremil S 1 tab tido paracetamol 3-5g/tab 1 tab q6ho ampicillin 500g IVTT q6ho folic acid 5 mg/tab odo tranexamic acid 150mg IVTT q8ho phytomenadione 1 ampule IVTT stat
10
B. Parent (self): parents/family’s general health status
Family’s general health status has been good
The child’s hospitalization was the first ever crisis the family has encountered regarding health.
o Hemoglobin – 3.4 g%o Hematocrit – 9.3 vol%o WBC – 3,400/cummo Neutrophil – 12 %o Lymphocyte – 79 %o Monocyte – 6 %o Eosinophil – 3 %o Platelet – 22,000/cummVital Signs:o temp 37.9 0Co pulse 111 bpm, regular, boundingo respi 28 cpm, with use of
accessory muscles
o BP 120/70 mmHg
Laboratory Values:
o Hemoglobin – 7.9 g%o Hematocrit – 20.9 vol%o Platelet – 10,000/cumm
Vital Signs:o temp 38.2 0Co pulse 121 bpm, regular, boundingo respi 31 cpm, with use of
accessory muscleso BP 124/72 mmHg
II. Nutritional – Metabolic Pattern
A. Parent’s report:
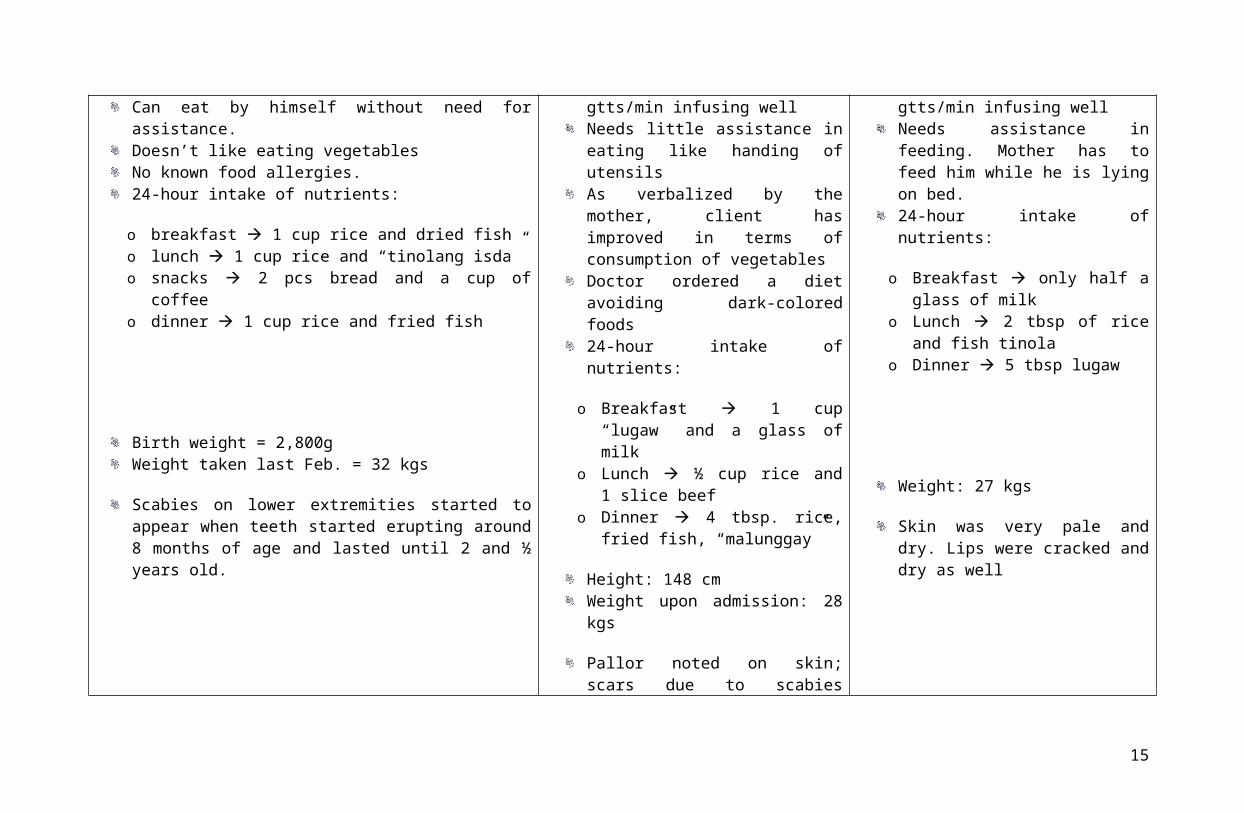
Client has good appetite.No feeding discomforts.No supplements.Can eat by himself without need for assistance.Doesn’t like eating vegetablesNo known food allergies.24-hour intake of nutrients:
o breakfast 1 cup rice and dried fisho lunch 1 cup rice and “tinolang isda”o snacks 2 pcs bread and a cup of coffee
Food consumption became less. He vomited after eating.D5.3 NaCl running at 41 gtts/min infusing wellNeeds little assistance in eating like handing of utensilsAs verbalized by the mother, client has improved in terms of consumption of vegetablesDoctor ordered a diet avoiding dark-colored foods24-hour intake of nutrients:
o Breakfast 1 cup “lugaw” and a
Food consumption became even less. He has the tendency to refuse eating.D5.3 NaCl running at 41 gtts/min infusing wellNeeds assistance in feeding. Mother has to feed him while he is lying on bed.24-hour intake of nutrients:
o Breakfast only half a glass of milk
o Lunch 2 tbsp of rice and fish tinola
11

o dinner 1 cup rice and fried fish
Birth weight = 2,800gWeight taken last Feb. = 32 kgs
Scabies on lower extremities started to appear when teeth started erupting around 8 months of age and lasted until 2 and ½ years old.
glass of milko Lunch ½ cup rice and 1 slice beefo Dinner 4 tbsp. rice, fried fish,
“malunggay”
Height: 148 cmWeight upon admission: 28 kgs
Pallor noted on skin; scars due to scabies evident on lower extremities
o Dinner 5 tbsp lugaw
Weight: 27 kgs
Skin was very pale and dry. Lips were cracked and dry as well
III. Elimination Pattern
A. Parent’s report:
He gets to defecate once a day, usually in the morningStool is light brown, soft and formed and moderate in amountNo discomfort felt during bowel eliminationUrination is 6-7 times in a dayUrine is light yellow, clear and in considerable amounts
Experience of perspiration in doing numerous activities such as making a chair or playing with younger siblings
Defecated twice of soft, formed and dark brown stool.No discomfort felt upon defecation Urination is between 5-6 times for the dayUrine is light yellow, clear and in small amounts
He was not perspiring. Slight body odor noted probably because of failure to take a bath
Was not able to move bowel for that dayUrinated 4 times and no discomfort upon doing soUrine was yellow, clear and in moderate amountHe was perspiring heavily in the head, face and neck
Slight body odor still noted
IV. Activity – Exercise Pattern
A. Parent’s report:
He takes a bath once a day in a water pump near their house, together with other siblingsDuring classes, he takes a bath early in the morning, around 5:30 am
Was not able to have a complete bath since admissionThe mother would wipe his whole body with wet cloth every other day
Has not taken a bathHe refused to be wiped with wet cloth on his bodyHe only stayed lying on bed. He can’t tolerate sitting even for just a little
12
Uses bathing soap (Zest)During school days, he wears his school uniform. When at home, usually wears sando and shortsAt home, time is mostly spent looking over and playing with younger siblings. He also likes making small wooden chairs as his type of play. He helps in taking care of their animals like their cow, pig and chicken He easily gets tired. He can’t tolerate activities like running, as he usually catches his breath with this activityClient is said to be a strong child. He doesn’t fear the dark. He would even walk alone at night to look for his father. He also wants doing things and solving problems on his own as much as possible, and only asks for help when he can no longer manage it by himself.He needs no assistance in bathing, feeding, toileting, dressing and grooming.
He would either lie on his bed or sit on the sideHe played with her younger sister when it came to visitThe mother sees his child as still strong. He once told his mother that he wants to get well right away so he can finish his studies so he could help his family in their financial problem.Needs little assistance in eating but he can walk his way to the bathroom Respi rate 28 cpm, with use of accessory muscles
Pulse rate 111 bpm, regular, bounding
while. He was too weak to do soHe avoided any interaction and covered his face with his arms. He even refused when pulse rate was to be taken, thinking that he would be asked to stand up.Looked very frail and weak and was having fever.Cannot eat by himself without being fed. He used a bedpan for urination because he can’t tolerate going to the bathroom anymoreRespi rate 31 cpm
Pulse rate 121 bpm
V. Sleep – Rest Pattern
A. Parent’s report
During classes, the child sees to it that he gets enough rest. He would sleep at 8pm and wakes up at 5am, having about 9 hours of sleep.But on Fridays, he usually stays late until 12mn as he would go with his aunts to a disco in their barangay. He would wake up 7am the next day, getting only 7hrs of sleep.They haven’t observed him having nightmares, nor did the child tell them he has experienced so.The other members would usually sleep more or less the same time with the patient, except during Fridays that they are able to sleep earlier.
His total hours of sleep during the night were 6 hours only.He wakes up during the night to urinateHe didn’t appear to be well-restedHis eyeballs were slightly sunken
There was a change in the usual sleeping pattern of the child. He didn’t get enough rest during the night. He was able to sleep well already in the morning.
Not well-rested as evidenced by sunken eye balls
13

VI. Cognitive Perceptual PatternA. Parent’s report:
Is very responsive to questionsResponds when asked and easily obeys when a command is given, doesn’t likes noise, is fascinated with things in which he has newly seen and loves to manipulate objects Has a low voice and can speak fluently and can form different sentencesHas a long attention span and loves to play and walk aroundNo problem about his vision, can hear clearly, and can feel the objects being touched
Can tell his name, address, and even his cell number
Is not so responsive and is experiencing fatigueResponds briefly when asked but sometime doesn’t response when being talked because he want to rest, gets irritated when noise is presentUsually vocalized 3 to 4 words when asked due to fatigue and doesn’t elaborate more on the word he is saying
No pain present but is experiencing muscle weakness and doesn’t want to do something because of the feeling of fatigue
Responds but very brief and doesn’t want to interact with us nor his parents because he just wants to rest Sometimes doesn’t listens when being talked and gets easily irritated with noise
Still is experiencing fatigue and muscle weakness
VII. Self Perception – Self Concept PatternA. Parents report:
Mother verbalized that he usually is happy and has a good mood and interacts with his brothers and sister with a smile on his face and doesn’t easily gets angry
B. Child’s report:
Doesn’t easily gets irritated and always smile but gets angry when exposed to an environment which is very noisy
Have many friends and most of his aunts like him because he is very responsible
Still smiles when were around but most of the time feels sad thinking of his condition
Is very afraid of needles that he collapsed during his first and second blood transfusion seeing the needle inserted in his arm
Usually stay in bed and always wants to rest and the smile on his face was gone because he has a fever so he feels so weak
Still is afraid of needles and had collapsed again for the third time during his blood transfusion
14
He is good most of the time and loves to play and do house hold chores
Doesn’t want to be alone but sometimes feels lonely when he is the only one left in the house
Very irritable especially when disturbed while restingStill has many friends and this friends of his want to visit him to the hospital but is not permittedEstablishes eye contact when being talked and answers the questions being asked but briefly
Stands up sometimes in a slouch posture and is feeling weak
Always thinking about his condition and feels sad thinking he cannot play and do his favorite stuffs
Doesn’t wants to stand up and is always lying down
VIII. Role/ Relationship Pattern
A. Parent’s Report:
Most of the time, he is with his younger sibling and attending to them when parents are working He usually disciplines his younger siblings if they have done something wrong and he usually help his father to look for money for financial problemsMostly interacts with his youngest sibling and is the one attending to her and usually plays with herSometimes feels sad when left alone in the house but can manage to be separated to parentsHe is dependent on his parents in terms of basic needs and learns how to deal with household chores and problems at schoolUsually after doing household chores in the morning, he plays with his friends and every after school, he plays with them and stays home at nightMother and father don’t have a problem in disciplining him. Sometimes if violated the rules, he is reprimanded and remains quiet
Cannot attend to his youngest sibling because of his condition right nowCannot interact with his younger sibling because they are just left at home with her grandmother and he is hear in the hospitalDoesn’t want to be left alone in the hospital He is very dependent to his parents because of his condition Cannot play most of the time because of muscle weakness
Relationship with his parents is more strengthen because now is that time that he really needs our help as verbalized by his mother
Misses his siblings because he haven’t seen them foe quite a whileHe is not allowed to roam around and interact with other patients because of his condition Due to muscle weakness and fatigue, he usually keeps on lying in bed and wants to restUnable to play anymore
15
Easily adjust to school activities
B. Parent:
Parents try to supervise the child in things that he do and is satisfied with every achievement that their child has done
Relationship with the child is good and parents trust him when left alone in the house because parents go to work from 7 am in the morning until 5 pm in the afternoonSexuality Reproductive Pattern
A. Parent’s Report:
The child uses boy’s stuff and wears boy’s clothes and hangs out with his peer boys.He tries to answer some of the questions about sexuality appropriately based on his learning but tries to avoid or doesn’t answer the question if he doesn’t have knowledge on it
B. Parent:
Has no problems about their sexual life and has no history of illness about it
He is shy to answer questions when asked about his reproductive system
He is still shy when asked about his reproductive system
X. Coping Stress Tolerance Pattern
A. Parent’s Report:
If faced with problems, he usually tries to fix it on his own but as soon as his patience ran out, he seeks help to his motherIf angry, he usually stays in a corner and doesn’t want to
He is optimistic that he will be cured with his disease right now
Usually gets irritated easily because of fatigue so he just keeps quiet and stays in bed and sleep
16

talk or play
B. Parent:
Mostly when problems arise, they talk together with his husband and mother so look for solutionsSometimes ask for help to their parents and to there siblings specially when dealing with financial and emotional problems Due to many children, they cannot attend to each one’s needs
His parent, aunts and uncle is taking turn in taking care of him in the hospital and looking for blood donors His mother is the one who is with her mostly in the hospital and his father visits him during weekendFinancial support for hospitalization was taken care by the governor
Is continuously looking for blood for transfusion and needs 4 packs of blood and is trying to look for financial support for the blood and medications
XI. Value – Belief Pattern
A. Parent
Verbalized that he wants to finish his studies and help his family about the financesPuts on “kinias sa saging” when wound is present Believes that scabies of his son was triggered by the eruption of his teeth at the age of 8 months to 1 yr and a half
Mother verbalized that his child wants to get well and go back to his normal routine and even tried to convince her to look for donor
Prays to God fervently so that he would be healed of his disease right now
Mother requested us to offer some prayers for his child
Still hopes that God will cure his disease
17

Physical Assessment PAST MEDICAL HISTORY
Had experienced cough and colds and was intervened by taking OTC medications such as medicol and neozep. Had experienced
measles, mumps, and chicken pox while he was still 5-7 years old. Received complete doses of immunizations except for MMR. Has no
heredofamilial diseases such as diabetes, hypertension, tuberculosis and others.
REVIEW OF SYSTEMS:
General: Last February, he weighed 32 kgs; upon admission, his weight was 28 kgs; at present, he only weighs 27 kgs. Feels weak and tired
and has fever.
Skin: skin color is pale and yellowish. It is dry and scars are present due to scabies. Small unexplained bruises noted in the left upper arm. No
lumps, and sores noted.
HEENT: had not experienced head injury. Eye bags are slightly sunken. Had not experienced infection or any pain in the ears. Had experienced
colds, during early years of life. Has a complete set of teeth and dental caries been noted at the left and right molars. Had no canker sores but
had experienced bleeding from gums and lips. Was not able to go to the dentist.
18

Neck: no lumps, no pain, and no stiffness noted
Breasts: absence of pain
Respiratory: rate and depth are increased and use of accessory muscles was noted upon inhalation.
Cardiovascular: negative heart murmurs; chest pain and discomfort.
Gastointestinal: loss of appetite and vomiting was noted. Passage of soft, and formed brownish stools at least once in two days.
Urinary: urinates 7x a day when already admitted, but usually urinates 5-6x a day.
Genital: no foul odor, and no abnormal discharges noted.
Musculoskeletal: no presence of redness and swelling. Weakness and fatigue is noted.
Neurologic: had experienced episodes of fainting, and experienced convulsions once while he was still 1 year old. Had not experienced
seizures or any other involuntary movement.
Hematologic: had experienced anemia and bleeding from nose and gums
Endocrine: had experienced excessive sweating before and during admission.
PHYSICAL ASSESSMENT FINDINGS
I. General Survey
Client is awake, coherent, lying in bed. IVF present at Left metacarpal vein running at 41 gtts/min, infusing well. Weakness and fatigue
was noted.
Vital signs:
T = 37.9 0C ht = 148 cm
P = 111 bpm, regular, bounding wt = 27 kgs
R = 28 cpm, silent, use of accessory muscles BP = 120/70 mmHg
19

II. HEENT (head, eyes, ears, nose and throat)
Health History: to assess for presence of discoloration such as paleness, jaundice and bleeding, it is important to asses the eyes, ears,
nose, and throat. Our client never experienced head injury or any other deviations of the head. No experiences of memory loss but
experienced episodes of fainting and convulsions. No experiences of sore eyes, or eye pain. Had no experiences of ear infection and
any pain in the ears. Had experienced tonsillitis at age 6 years old.
Head
His head is symmetric and round. It is normally hard, without lumps or tenderness palpated. Hair is black, thick, with no lice present
and is evenly distributed all throughout his head.
Eyes
His eyelashes are evenly distributed and curved outward along the lid margin. Skin on both eyelids has no presence of redness,
swelling or lesions. Conjuctiva is pale, and moist. Sclera is white. Cornea is transparent, smooth and no opacities. Iris and cornea is
round flat and evenly colored. Pupils are normally equal in size. The eyes constrict as light is shone unto it. Has normal direct and
consensual pupillary response. Eyes turn inward when focusing on a near object. Was able to follow the 6 direction-gaze without
moving his head accordingly. The client can read at 14 inches what the normal eye can read at 14 inches.
Ears
Her ears are equal in size. Auricle is aligned with the outer canthus of each eye. Skin in the ears is pale just like the color of entire
body, smooth with no lesions, lumps, or nodules. Presence of cerumen on both ears. The client was able to hear and repeat the words
that were instructed to him during the auditory acuity. Verbalized cleaning of his ears is done once a week if cotton buds are
available. No inappropriate discharges noted coming out from the ears.
Nose
20

The color is pale with brown pigmentation, smooth, symmetric with no tenderness. Septum is red and swollen because of presence of
oxygen inhalation. Nose bleeding was noted and was wiped by mother. Frontal and maxillary sinuses are non-tender to palpation.
Mouth
Has complete set of teeth with presence of dental caries in the left and right molars. Frequent complaints of tooth ache especially
when the mouth was inspected. Gums are pale, dry, with no ulcerations present. Lips are cracked, dry, and bleeding was noted after
he brushed his teeth. Tongue is dry and is pale just like his gums.
Pharynx
No lumps and tenderness palpated in the pharynx. No bulging of lymph noted.
Neck
Neck is symmetrical without bulging masses. The adam’s apple moves up symmetrically as the client swallows. Upon palpation of the
thyroid, the lobes are smooth, firm, and nontender. Nodes have no swelling or enlargement and no tenderness.
III. Integumentary System
Health History
To check for presence of dehydration, dryness, and discoloration, thus, assessing the skin and its parts are important aspect in
determining deviations of its structures. Patient’s skin is brown in color with fair complexion before the occurrence of his condition. Had
experienced cuts or breaks in the skin as evidenced by presence of scars. Scars were also present in the posterior extremities due to
scabies and vehicular accident. Had experienced skin itching and redness at the lower extremities due to insect bite. Presence of
macules (moles) in the lower left posterior leg. Had experienced bruises as reported. Had undergone chicken pox, mumps, and measles
as reported by mother but had not experienced any skin allergies. Has presence of skin dryness and is febrile PTA. Has no history of hair
21

loss. Hair is shiny and thick and is equally distributed throughout the head. Had not experienced nail injury and nails are cut and
cleaned by himself every 2 weeks.
Skin
The skin is pale and yellowish in color and is distributed throughout the body. Presence of slight pain and redness at injection site and at
blood transfusion site. Skin is dry and is warm to touch because of his high temperature. Skin is slightly rough due to presence of
abrasions and scars. The skin does not lift up easily upon pinching and returns to place slowly. Presence of macules (moles) in the lower
left posterior leg. Scars from chicken pox were present all over the body in distributed manner.
Nails
The fingernails are not so short with minimal dirt underneath it. Nail beds are pale and capillary refill is absent. It is in 160 degrees
angle and is concave in shape. The toenails are pale and yellowish in color with minimal dirt underneath it. No abnormal pigmentation
noted in the toe nails. Has still delayed capillary refill.
Hair
Hair is thick and coarse, black and dry, and is equally distributed all throughout the head. No dandruffs or scaliness noted in the hair. No
alopecia noted in any part of the head. Uses shampoo or soap every other day upon washing the hair. Had not used any hair treatment
formulas or any hair wax. Usually cuts his hair every 2 months.
IV. Respiratory System (Anterior and Posterior Chest)
Health History
As diagnosed to have aplastic anemia wherein oxygenation may be impaired, the respiratory system should be assessed to check for
presence of deviations from normal. Patient has no family history of lung cancer, tuberculosis, and any other respiratory conditions. Had
22
experienced cough and colds during the past year. Mother usually gives OTC drugs such as paracetamol, medicol, neozep for fever,
cough, and colds. Had not experienced hemoptysis or coughing out of blood streaked sputum. Respiratory rate before admission was
regular, silent and effortless. Had no experiences of difficulty in breathing as reported. Patient had no history of any allergy to dust or
other foreign organisms present in the air.
Inspection
Anterior thorax is symmetric with not so good expansion. Use accessory muscle is noted upon inhalation. There is no abnormal
retraction of the interspaces. No deformities in the chest noted. Respiration is deep, silent, with use of accessory muscle. Respiration
rate is 28 cpm. Posterior chest wall is symmetric in both sides and there are no abnormal retractions noted in the interspaces.
Palpation
In the anterior chest, there are no tender areas palpated as evidenced by absence of facial grimacing and crying. There are no bruises,
lesions, masses present in the chest. Posterior chest is warm to touch. No tender or painful areas palpated as evidenced by absence of
crying. No bruises, lesions, or masses present in the posterior chest. Chest expansion is deep and symmetrical as evidenced by equal
movement of thumbs placed on the back. Upon assessing the tactile fremitus, equal vibrations are heard in the anterior and posterior
chest.
Percussion
Resonant sounds are heard in the areas around the lung fields. Diaphragm was percussed and dull sounds were heard. There are no any
other abnormal percussion notes heard in the anterior and posterior chest.
Auscultation
23

Breath sounds are louder in the lower posterior lung fields and also is loud in the upper anterior lung fields compared to other part of
the chest. There are no silent gaps present between sounds. Respiratory rate is 28 cycles per minute, and is deep with use of accessory
muscles. Vesicular and bronchovesicular sounds are heard over most of both lungs and 1st and 2nd ICS and also between the scapula.
THE BLOODTHE BLOOD
The primary roles of blood in general are to integrate body functions and to meet the The primary roles of blood in general are to integrate body functions and to meet the
needs of specific tissues. This is accomplished through transportation, regulation, and protectionneeds of specific tissues. This is accomplished through transportation, regulation, and protection
mechanisms. Blood transports oxygen, nutrients, waste products, and hormones from one place tomechanisms. Blood transports oxygen, nutrients, waste products, and hormones from one place to
another. Regulation is accomplished through buffers in the blood, plasma proteins, and heatanother. Regulation is accomplished through buffers in the blood, plasma proteins, and heat
transport, such as muscle-generated temperature. The protection function of the blood includestransport, such as muscle-generated temperature. The protection function of the blood includes
antibodies and phagocytes to protect against disease as well as factors that participate in hemostasis.antibodies and phagocytes to protect against disease as well as factors that participate in hemostasis.
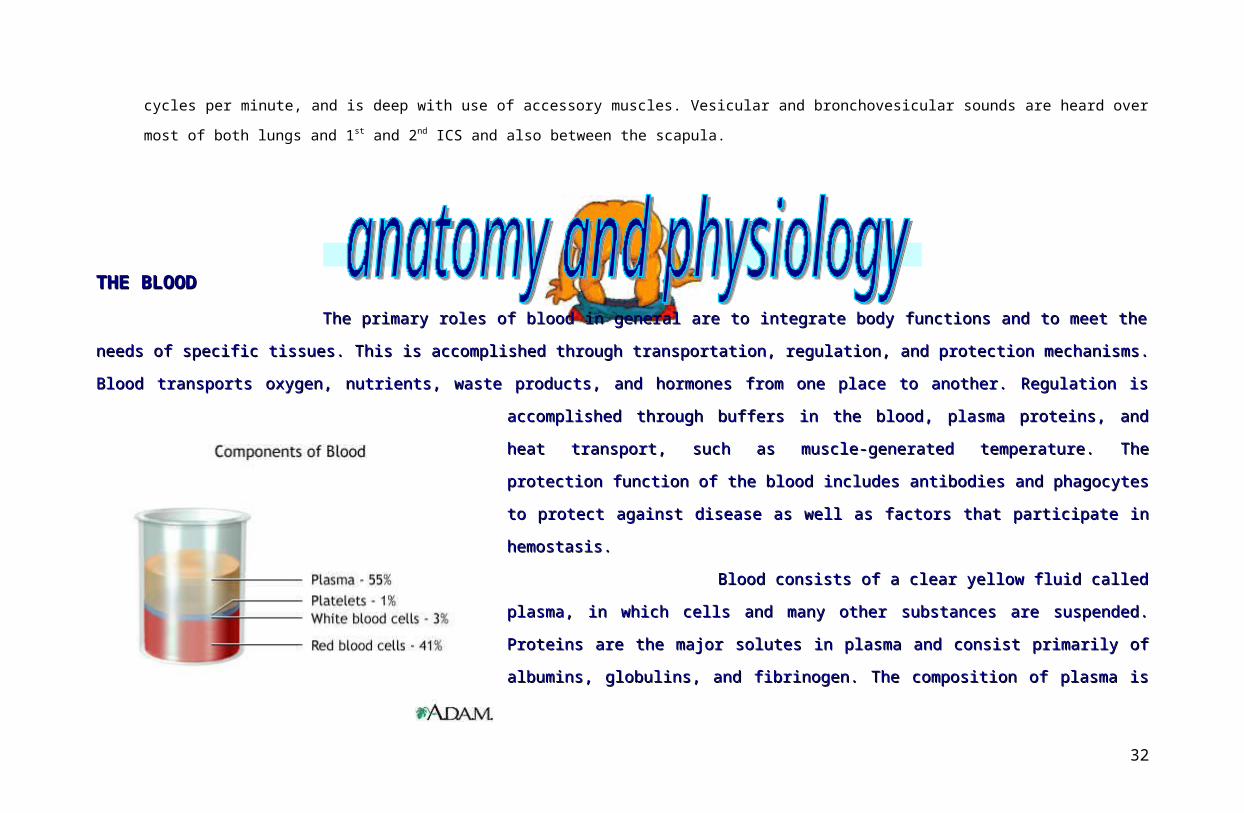
Blood consists of a clear yellow fluid called plasma, in which cells and many other Blood consists of a clear yellow fluid called plasma, in which cells and many other
substances are suspended. Proteins are the major solutes in plasma and consist primarily ofsubstances are suspended. Proteins are the major solutes in plasma and consist primarily of
albumins, globulins, and fibrinogen. The composition of plasma is similar to that of interstitial fluid,albumins, globulins, and fibrinogen. The composition of plasma is similar to that of interstitial fluid,
except that it has a much higher protein concentration which maintains the intravascular volume byexcept that it has a much higher protein concentration which maintains the intravascular volume by
the exertion of colloid osmotic pressure. In addition to holding water in the intravascular spaces,the exertion of colloid osmotic pressure. In addition to holding water in the intravascular spaces,
plasma proteins bind such substances as lipids and such metals as iron, contribute to blood viscosity,plasma proteins bind such substances as lipids and such metals as iron, contribute to blood viscosity,
and participate in the coagulation of blood. They are also important in regulating acid-base balance. and participate in the coagulation of blood. They are also important in regulating acid-base balance.
The blood volume is the sum of volumes of plasma and formed elements of blood in the vascular system. Although numerous factors affect blood The blood volume is the sum of volumes of plasma and formed elements of blood in the vascular system. Although numerous factors affect blood
volume, it remains relatively stable in the healthy person. Several compensatory mechanisms contribute to this stability; for example, decreased RBC volume isvolume, it remains relatively stable in the healthy person. Several compensatory mechanisms contribute to this stability; for example, decreased RBC volume is
24

followed by increased plasma volume, thereby returning total blood volume to its normal level. In this situation, the total blood volume may be normal, but the ratiofollowed by increased plasma volume, thereby returning total blood volume to its normal level. In this situation, the total blood volume may be normal, but the ratio
of plasma to cells is altered.of plasma to cells is altered.
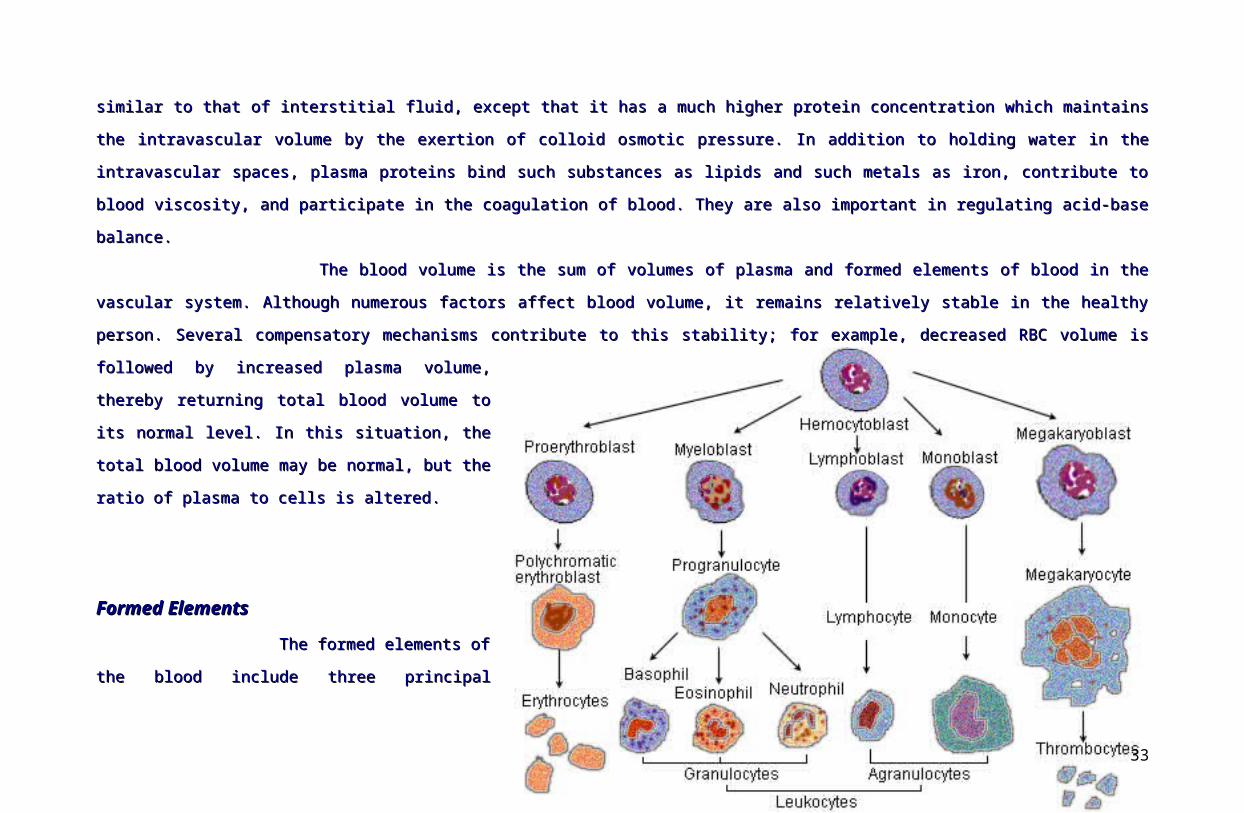
Formed Elements Formed Elements
The formed elements of the blood include three principal components: red blood cells, white blood cells, and platelets. Although RBCs and WBCs are The formed elements of the blood include three principal components: red blood cells, white blood cells, and platelets. Although RBCs and WBCs are
whole cells, platelets are cell fragments. Unlike RBCs andwhole cells, platelets are cell fragments. Unlike RBCs and
platelets, which have just a few roles, WBCs have a numberplatelets, which have just a few roles, WBCs have a number
of specialized functions. The percentage of total bloodof specialized functions. The percentage of total blood
volume occupied by RBCs is called the hematocrit. Avolume occupied by RBCs is called the hematocrit. A
significant drop in hematocrit indicates anemia, a lower-than-significant drop in hematocrit indicates anemia, a lower-than-
normal number of RBCsnormal number of RBCs
Formation of Blood CellsFormation of Blood Cells
Although some lymphocyte has a lifetime Although some lymphocyte has a lifetime
measured in years, most formed elements of the blood aremeasured in years, most formed elements of the blood are
continually dying and being replaced within hours, days, orcontinually dying and being replaced within hours, days, or
weeks. Negative feedback systems regulate the number ofweeks. Negative feedback systems regulate the number of
RBCs and platelets in the circulation, and their numbersRBCs and platelets in the circulation, and their numbers
normally remain steady. The abundance of different types ofnormally remain steady. The abundance of different types of
WBCs, however, varies in response to challenges byWBCs, however, varies in response to challenges by
invading pathogens and other foreign antigens. invading pathogens and other foreign antigens.
25

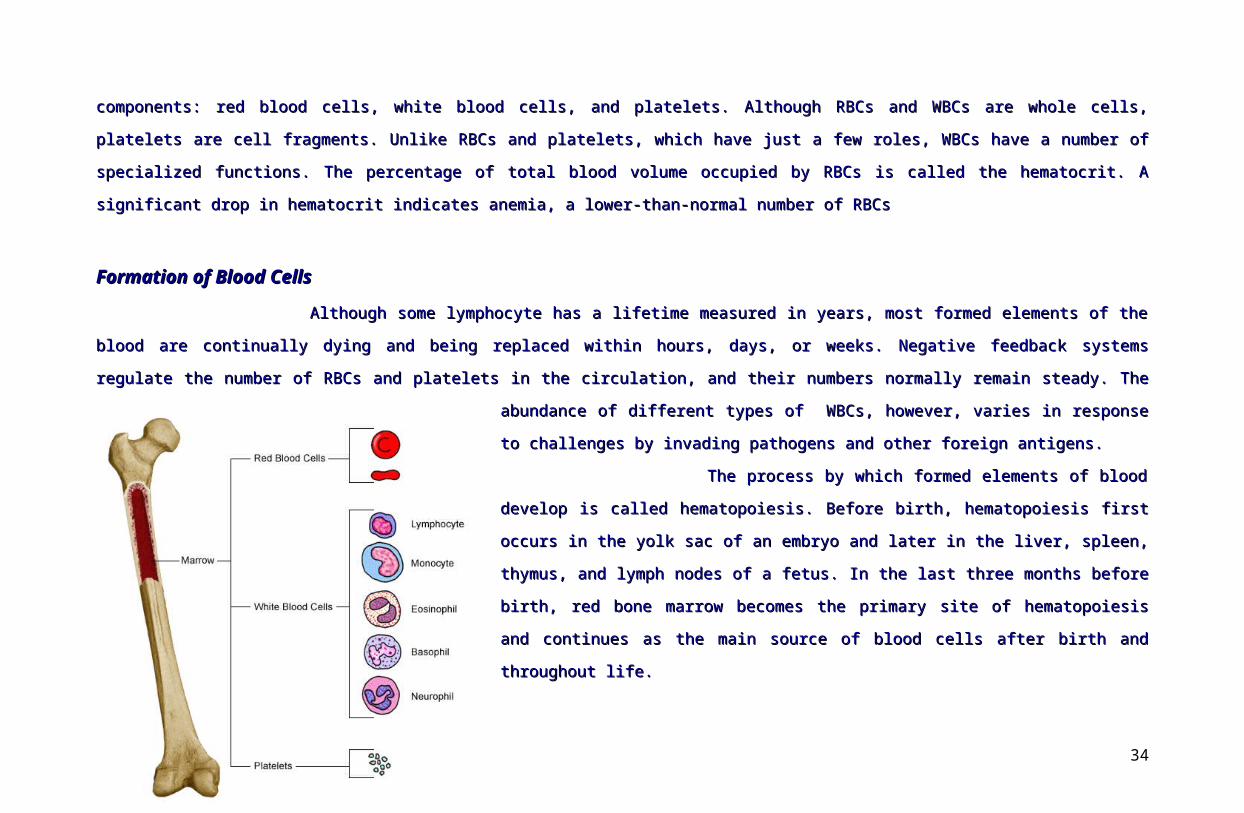
The process by which formed elements of blood develop is called hematopoiesis. Before The process by which formed elements of blood develop is called hematopoiesis. Before
birth, hematopoiesis first occurs in the yolk sac of an embryo and later in the liver, spleen, thymus,birth, hematopoiesis first occurs in the yolk sac of an embryo and later in the liver, spleen, thymus,
and lymph nodes of a fetus. In the last three months before birth, red bone marrow becomes theand lymph nodes of a fetus. In the last three months before birth, red bone marrow becomes the
primary site of hematopoiesis and continues as the main source of blood cells after birth andprimary site of hematopoiesis and continues as the main source of blood cells after birth and
throughout life.throughout life.
Red bone marrow is highly vascularized connective tissue located in the microscopic Red bone marrow is highly vascularized connective tissue located in the microscopic
spaces between trabeculae of spongy bone tissue. It is present chiefly in bones of the axial skeleton,spaces between trabeculae of spongy bone tissue. It is present chiefly in bones of the axial skeleton,
pectoral and pelvic girdles, and the proximal epiphyses of the humerus and femur. About 0.05-0.1%pectoral and pelvic girdles, and the proximal epiphyses of the humerus and femur. About 0.05-0.1%
of red bone marrow cells are derived from mesenchymal cells called pluripotent stem cells, whichof red bone marrow cells are derived from mesenchymal cells called pluripotent stem cells, which
has the capacity to develop into several different types of cells. has the capacity to develop into several different types of cells.
Pluripotent stem cells produce two further types of stem cells, called myeloid stem cells
and lymphoid stem cells. Myeloid stem cells begin their development in red bone marrow and give
rise to red blood cells, platelets, monocytes, neutrophils, eosinophils, and basophils. Lymphoid stem
cells begin their development in red bone marrow but complete it in lymphatic tissues and give rise
to lymphocytes.
During hematopoiesis, the myeloid stem cells differentiate into progenitor cells which are
also known as colony-forming units (CFUs). After the CFU designation is an abbreviation that designates the mature elements in blood that they will produce: CFU-
E ultimately produces erythrocytes (RBCs), CFU-Meg produces megakaryocytes, the source of platelets, and CFU-GM ultimately produces granulocytes
(speciafically neutrophils) and monocytes.
Several hormones are called hemopoietic growth factors regulate the differentiation and prolifieration of particular progenitor cells. Erythropoeitin or EPO
increases the number of red blood cell precursors. The main producers of EPO are cells in the kidneys that lie between the kidney tubules. Thrombopoietin or TPO
is a hormone produced by the liver that stimulates the formation of platelets from megakaryocytes. Cytokines, which are small glycoproteins, are produced by the
26
red bone marrow cells, leukocytes, macrophages, fibroblasts, and endothelial cells. Cytokines stimulate proliferation of progenitor cells in red bone marrow and
regulate the activities of cells involved in nonspecific defenses (ie, phagocytes) and immune responses (such as B cells and T cells). Two important families of
cytokines that stimulate white blood cell formation are colony-stimulating factor (CSFs) and interleukins.
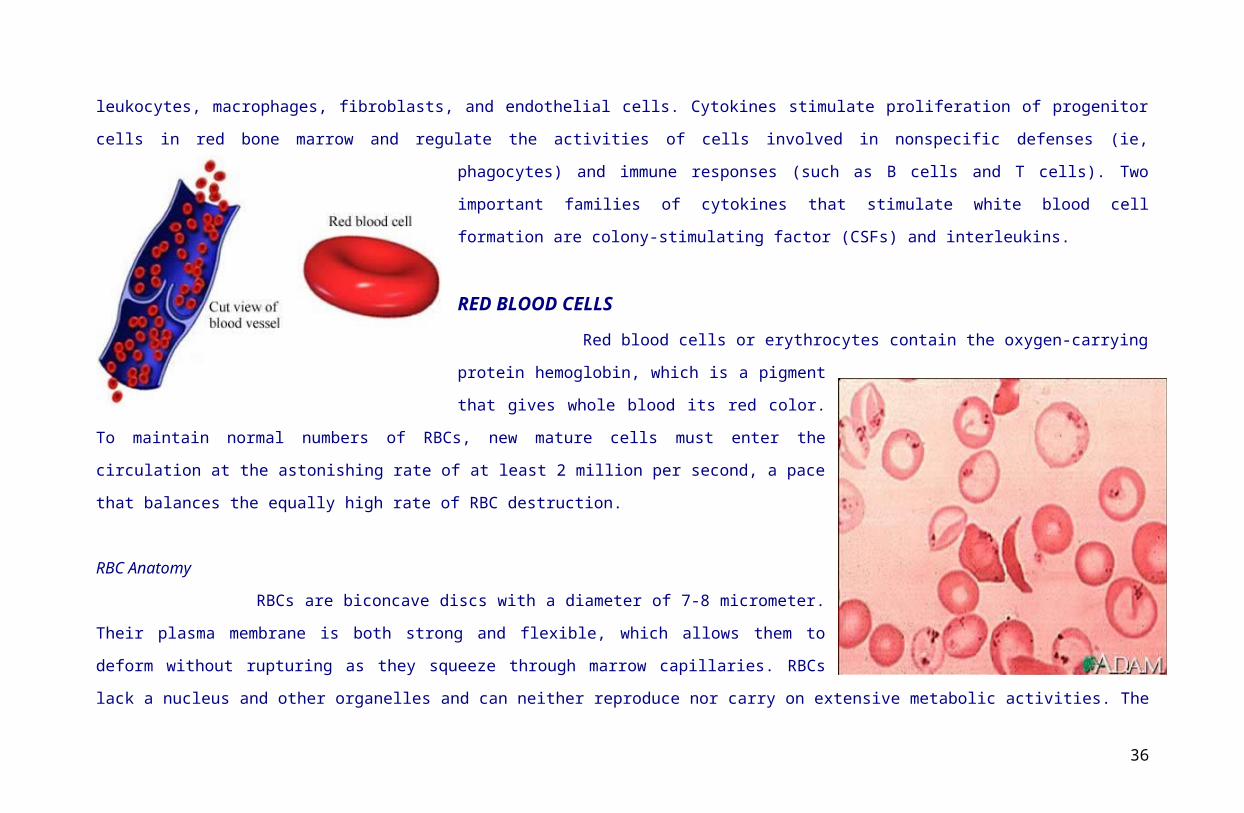
RED BLOOD CELLS
Red blood cells or erythrocytes contain the oxygen-carrying protein hemoglobin, which is a
pigment that gives whole blood its red color. To maintain normal numbers of RBCs, new mature cells must
enter the circulation at the astonishing rate of at least 2
million per second, a pace that balances the equally high
rate of RBC destruction.
RBC Anatomy
RBCs are biconcave discs with a diameter of 7-8 micrometer. Their plasma membrane is both strong
and flexible, which allows them to deform without rupturing as they squeeze through marrow capillaries. RBCs
lack a nucleus and other organelles and can neither reproduce nor carry on extensive metabolic activities. The
cytosol of RBCs contain hemoglobin molecules, which were synthesized before loss of the nucleus during RBC
production and which constitute about 33% of the cell’s weight.
RBC Physiology
Red Blood cells are highly specialized for their oxygen transport function. Their internal space is always available for oxygen transport because of the
absence of nucleus. Moreover, RBCs lack mitochondria and generate ATP anaerobicallly. Hence, they do not use up any of the oxygen they transport. Each RBC
contains about 280 million hemoglobin molecules and each can carry up to four oxygen molecules.
27
A hemoglobin molecule consists of a protein called globin, composed of four polypeptide chains plus four nonprotein pigments called hemes. The oxygen
picked up in the lungs is transported bound to the iron of the heme group. As blood flows through tissue capillaries, the iron-oxygen reaction reverses. Hemoglobin
releases oxygen, which diffuses first into the interstitial fluid and then into cells. Hemoglobin also transports about 13% of the total carbon dioxide and blood
flowing through tissue capillaries picks up carbon dioxide. As blood flows through the lungs, the carbon dioxide is released from hemoglobin and then exhaled.
Hemoglobin also plays an important role in the regulation of blood flow and blood pressure. The gaseous hormone nitric acid, which is produced by the endothelial
cells that line blood vessels, binds to hemoglobin. Under some circumstances, hemoglobin releases nitric oxide and causes vasodilation which will then improves
blood flow and enhances oxygen delivery to cells near the site of nitric acid release.
Red Blood cells have an average life span of 105-120 days because of the wear and tear their plasma membranes undergo as they squeeze through blood
capillaries. Without a nucleus and other organelles, RBCs cannot synthesize new components to
replace damaged ones. The plasma membrane becomes more fragile with age, and the cells are
more likely to burst especially as they squeeze through narrow channels in the spleen.
Erythropoiesis: Production of RBCs
The production of RBCs starts in the red bone marrow with a precursor cell called a
proerythroblast in a process called Erythropoiedis. The proeyhthroblast divides severeal times,
producing cells that begin to synthesize hemoglobin. Loss of nucleus causes the center of the cell
to indents, producing a distinctive biconcave shape. Normally, eythropoiesis and red blood cell
destruction proceed at roughly the same pace. If the oxygen-carrying capacity of the blood falls
because eythropoiesis is not keeping up with RBC destruction, a negative feedback system steps
up RBC production. The controlled condition is the amount of oxygen delivered to body tissues.
Cellular oxygen deficiency, called hypoxia, may occur if too little oxygen enters the blood. Whatever the cause, hypoxia stimulates the kidneys to step up the
28
release of erythropoietin. This hormone circulates through the blood to the red bone marrow, where it speeds the development of proeryhtroblasts into reticulocytes.
When the number of circulating RBC increases, more oxygen can be delivered to body tissues.
WHITE BLOOD CELLS
WBCs or leukocytes, unlike RBCs, have nucleus and do not contain hemoglobin. They are classified as either granular or agranular, depending on
whether they contain conspicuous chemical-filled cytoplasmic vesicles (originally called granules)
that are made visible by staining. Granular leukocytes include neutrophils, eosinophils, and
basophils; agranular leukocytes include lymphocytes and monocytes. Monocytes and granular
leukocytes develop from a myeloid stem cell. In contrast, lymhocytes develop fro a lymphoid stem
cell.
The skin and mucous membranes of the body are continuously exposed to microbes
and their toxins. Some of these microbes can invade deeper tissues to cause disease. Once the
pathogens enter the body, the general function of the WBCs is to combat them by phagocytosis or
immune responses. To accomplish these tasks, many WBCs leave to bloodstreamand collect at
points of pathogen invasion or inflammation. Once the granulocytes and monocytes leave the
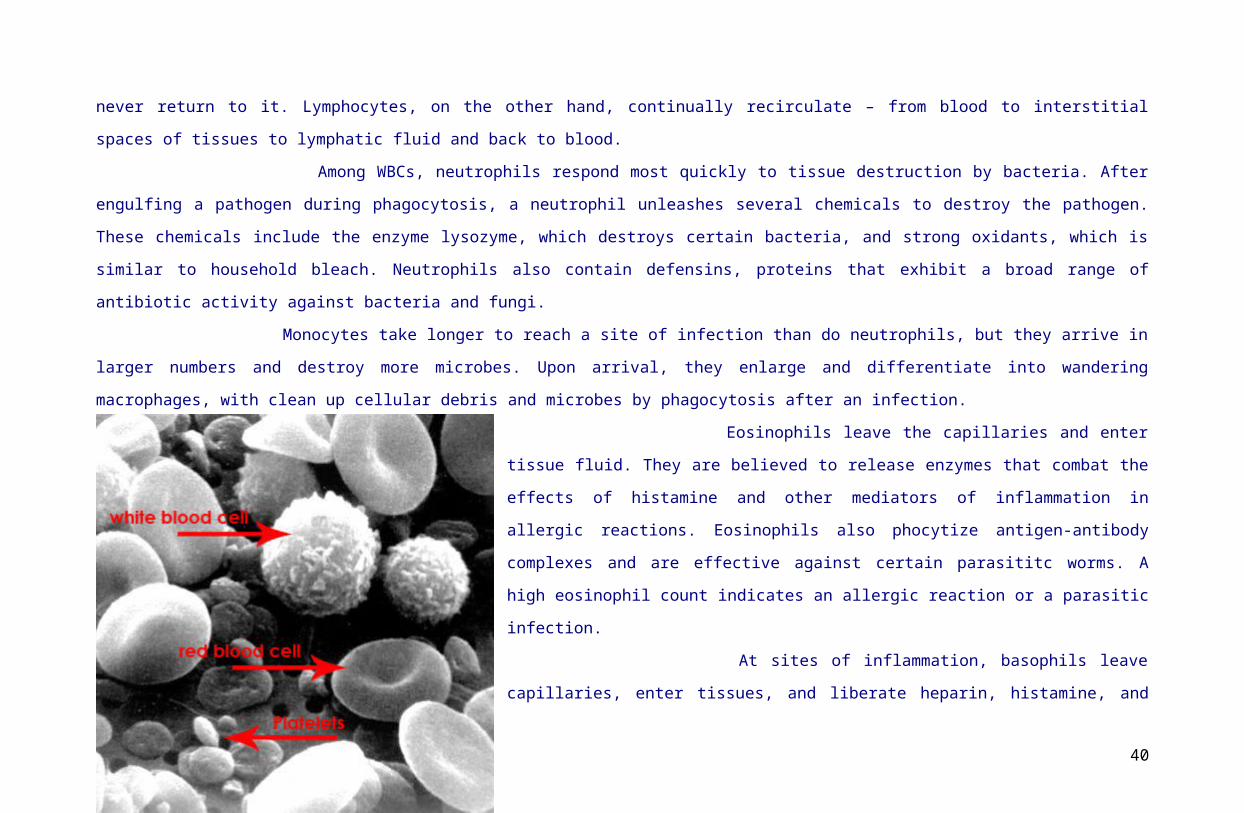
bloodstream to fight injury or infection, they never return to it. Lymphocytes, on the other hand,
continually recirculate – from blood to interstitial spaces of tissues to lymphatic fluid and back to
blood.
Among WBCs, neutrophils respond most quickly to tissue destruction by bacteria. After engulfing a pathogen during phagocytosis, a neutrophil
unleashes several chemicals to destroy the pathogen. These chemicals include the enzyme lysozyme, which destroys certain bacteria, and strong oxidants, which is
similar to household bleach. Neutrophils also contain defensins, proteins that exhibit a broad range of antibiotic activity against bacteria and fungi.
29

Monocytes take longer to reach a site of infection than do neutrophils, but they arrive in larger numbers and destroy more microbes. Upon arrival, they
enlarge and differentiate into wandering macrophages, with clean up cellular debris and microbes by phagocytosis after an infection.
Eosinophils leave the capillaries and enter tissue fluid. They are believed to release enzymes that combat the effects of histamine and other mediators of
inflammation in allergic reactions. Eosinophils also phocytize antigen-antibody complexes and are effective against certain parasititc worms. A high eosinophil
count indicates an allergic reaction or a parasitic infection.
At sites of inflammation, basophils leave capillaries, enter tissues, and liberate heparin,
histamine, and serotonin. These substances intensify the inflammatory reaction and are involved in
hypersensitivity reactions.
Lymphocytes are the major soldiers in immune system battles. There are three main
types of lyphocytes which are the B cells, T cells, and natural killer cells. An increase in the number
of circulating WBCs usually indicates infection or inflammation.
PLATELETS
Under the influence of the hormone thrombopoetin, myeloid stem cells develop into
megakaryocyte-colony-forming cells that, in turn, develop into precursor cells called
megakaryoblasts. Megakayoblasts transform into megakaryocytes, huge cells that splinter into
2000-3000 fragments. Each fragment, enclosed by a piece of the plasma membrane, is a platelet
(thrombocyte). Platelets break off from the megakaryocytes in red bone marrow and then enter the
blood circulation. Platelets, like RBCs, are disc-shape and have no nucleus. These cells help stop
blood loss from damaged blood vessels by forming a platelet plug. Their granules also contain chemicals that, once released, promote blood clotting. Platelets have
a short life span, normally just 5 to 9 days. Aged and dead platelets are removed by fixed macrophages in the spleen and liver.
30
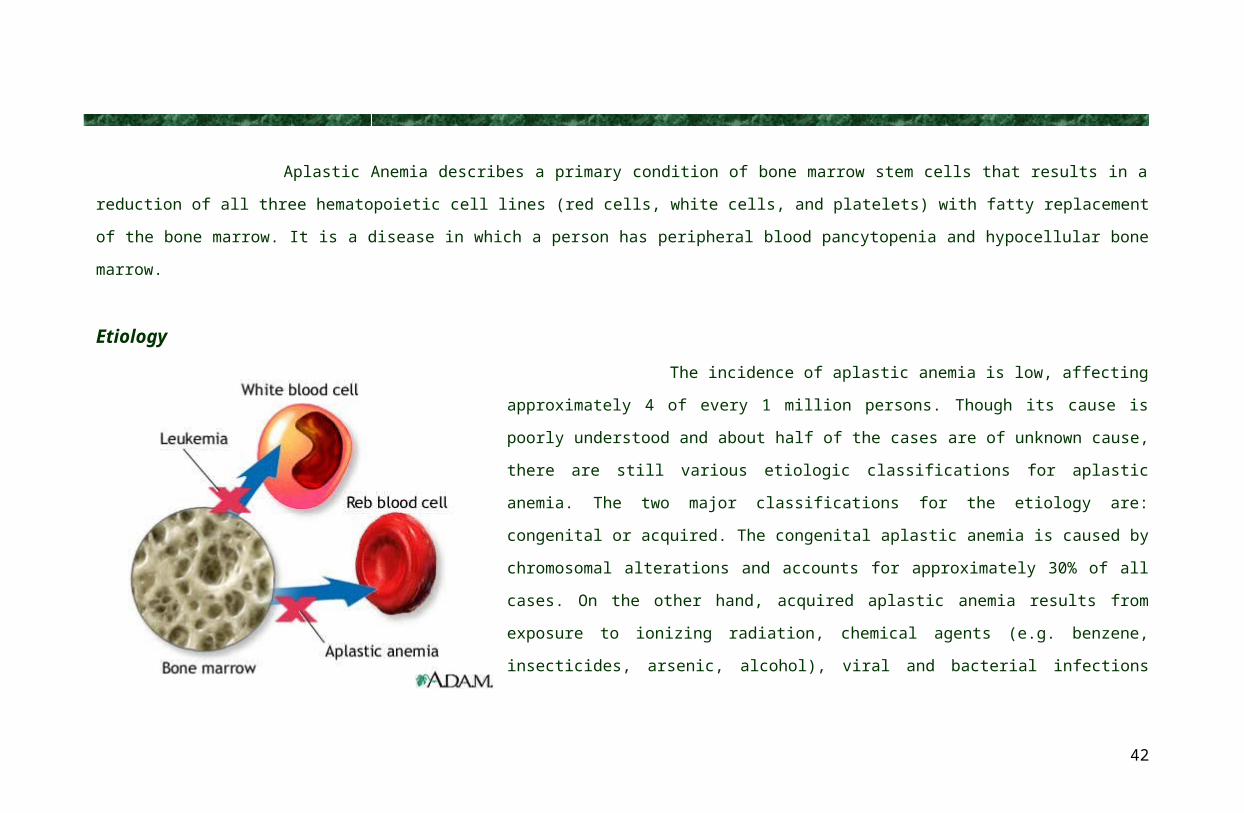
Aplastic Anemia describes a primary condition of bone marrow stem cells that results in a reduction of all three hematopoietic cell lines (red cells, white
cells, and platelets) with fatty replacement of the bone marrow. It is a disease in which a person has peripheral blood pancytopenia and hypocellular bone marrow.
Etiology
The incidence of aplastic anemia is low, affecting approximately 4 of every 1 million
persons. Though its cause is poorly understood and about half of the cases are of unknown cause,
there are still various etiologic classifications for aplastic anemia. The two major classifications for
the etiology are: congenital or acquired. The congenital aplastic anemia is caused by chromosomal
alterations and accounts for approximately 30% of all cases. On the other hand, acquired aplastic
anemia results from exposure to ionizing radiation, chemical agents (e.g. benzene, insecticides,
arsenic, alcohol), viral and bacterial infections (e.g. hepatitis, parvovirus, biliary tuberculosis, and
prescribed medications (e.g antimicrobial agents such as chloramphenicol, anticonvulsants, and
anti-inflammatory drugs).
Clinical Manifestations
The onset of aplastic anemia may be insidious, or it may strike with suddenness and great
severity. It can occur at any age. Clinically, the patient may have symptoms caused by suppression of any or all bone marrow elements. The initial presenting
symptoms include weakness, fatigability, and pallor. Petechiae and ecchymoses often are present on the skin, and there may be bleeding from the nose, gums,
31
vagina, of gastrointestinal tract because of decreased platelet levels (thrombocytopenia). The decrease number of neutrophils (neutropenia) is an indicative of
susceptibitlity to infection and may be febrile.
Diagnostic Studies
The diagnosis is confirmed by laboratory studies. Because all marrow elements are affected, hemoglobin, WBC,
and platelet values are often decreased in aplastic anemia. The reticulocyte count and the bleeding time is prolonged. Bone
marrow biopsy, aspiration, and pathologic examination may be done for any anemic state. However, the findings are
especially important in aplastic anemia because the marrow is hypocellular, with increased yellow marrow (fat content), a
finding sometimes referred to as “dry tap”.
Management
Management of aplastic anemia is based on identifying and removing the causative agent (when possible) and providing supportive care until
pancytopenia reverses.
The prognosis of aplastic anemia is poor (approximately 75% fatal). However, advances to medical management, including
bone marrow transplantation and immunosuppressive therapy with antithymocyte globulin (ATG) and cyclosporine, have improved
outcomes significantly, producing remission in 50% of patients. ATG, a purified gamma globulin solution, is obtained from horses or
rabbits immunized with human T lymphocytes. Side effects during the infusion are common and may include fever and chills. The
sudden onset of a rash or bronchospasm may herald anaphylaxis and requires prompt management. Serum sickness, as evidenced by
fever, rash, arthralgias, and pruritus, may develop in some patients and may take weeks to resolve. Immunosuppressants prevent
32
the patient’s lymphocytes from destroying the stem cells. If relapse occurs (ie, the patient becomes pancytopenic again), reinstitution of the same immunologic
agents may induce another remission.
It is presumed that the lymphocytes of patients with aplastic anemia destroy the stem cells and consequently impair the production of erythrocytes,
leukocytes, platelets. Despite its severity the aplastic anemia can be treated in most people. Those who are younger than 60 years, who are otherwise healthy, and
who have compatible donor can be cured of the disease by bone marrow transplant or peripheral blood stem cell transplant.
Supportive therapy plays a major role in the managemtent of aplastic anemia. Any offending agent is discontinued. The patient is supported with
transfusions of packed RBCs and platelets as necessary. Death is usually caused by hemorrhage or infection.
Nursing management include assessment for signs of infection and bleeding since patients with aplastic anemia are vulnerable to problems related to
erythrocyte, leukocyte, and platelet deficiencies. Specific interventions are delineated in the sections on neutropenia and thrombocytopenia.
Pathophysiology
Normally, your bone marrow supplies the right numbers of blood cells to keep you healthy. Aplastic anemia develops when damage occurs to your bone
marrow, slowing or shutting down the production of new blood cells — a serious problem. Factors that can temporarily or permanently injure bone marrow include:
High-dose radiation and chemotherapy treatments. While these cancer-fighting therapies kill cancer cells, they can also damage healthy cells, including
stem cells in bone marrow. Secondary aplastic anemia can be a temporary side effect of these treatments.
Exposure to toxic chemicals. Exposure to toxic chemicals, such as some used in pesticides and insecticides, may cause secondary aplastic anemia.
Exposure to benzene — an ingredient in gasoline — also has been linked to secondary aplastic anemia.
Use of certain drugs. Some medications, such as those used to treat rheumatoid arthritis and some antibiotics, can cause secondary aplastic anemia.
Autoimmune disorders. An autoimmune disorder, such as lupus, in which your immune system begins attacking healthy cells, may involve stem cells in
the bone marrow.
A viral infection. Viral infections that affect bone marrow may play a role in the development of aplastic anemia in some people.
33
Unknown factors. In about half of cases, doctors aren't able to identify the cause of aplastic anemia. This is called idiopathic aplastic anemia.
In aplastic anemia, the bone marrow is described in medical terms as aplastic or hypoplastic — meaning that it's empty, or contains very few blood cells. In
line with these risk factor, as a whole, they attack the healthy cells of the bone marrow causing alterations in its normal functioning. There are two theories that
could support this assumption: (1) seed or stem-cell – deficiency theory, and (2) the microenvironmental deficiency theory.
The seed or stem-cell – deficiency theory proposes that, a common stem cell population is irreversibly altered, rendering it incapable of proliferation and
differentiation. An intrinsic derangement of hemopoietic proliferation capacity that is essentially compatible with life has to be considered a premalignant condition.
This primarily diseased tissue can be destroyed by immune mechanisms in an attempt to achieve self-cure Failure of the immune mechanisms can lead to absence of
bone marrow cytokines and colony-stimulating factors present in the red bone marrow. On the other hand, the microenvironmental deficiency theory proposes that
the stem cell environment (i.e. the marrow) is altered so as to inhibit differentiation of stem cells to precursor cells thereby inhibiting erythopoiesis. These two
theories can now lead to decreased production of RBCs, WBCs, and platelets, because of the alterations in hematopoiesis. Signs and symptoms may be manifested
before diagnosis was made. In decreased RBC production, tissue hypoxia can occur as a result of decreased oxygen-carrying capacity of the blood. Tissue hypoxia
creates additional demands and effects on the pulmonary and hematologic systems. The rate and depth of breathing increases in an effort to increase oxygen
availability and is accompanied by an increase in the release of oxygen from hemoglobin. All of these may cause an individual to experience shortness of breath and
a rapid, pounding heart beat, dizziness, and fatigue. The skin, mucous membranes, lips, nail beds, and conjunctiva become pale because of reduced hemoglobin
concentration and tissue hypoxia may lead to delayed wound healing and loss of skin elasticity. On the other hand, decreased oxygen supply to the gastrointestinal
tract often produces abdominal pain, nausea, vomiting, and loss of appetite.
Compensatory mechanisms may either be present in response to meet the normal oxygen demands of the body. For example, during hypoxemia, wherein
there is a reduced oxygen level in the blood, may lead to cardiovascular dysfunction by causing dilation of arterioles, capillaries, and venules, thus increasing flow
through them. Increased peripheral blood flow and venous return further contributes to an increase in heart rate and stroke volume. These identified compensatory
mechanisms may lead to heart failure. Another compensatory mechanism when the anemia is severe or acute in onset is peripheral blood vessel constriction,
34

diverting blood flow to essential vital organs. Decreased blood flow detected by the kidneys activates the rennin-angiotensin response , causing salt and water
retention in an attempt to increase blood volume. Prompt intervention is necessary and palliation of associated symptoms. Therapies include transfusion,
administration of supplemental vitamins or iron, medications to prevent complications.
35
Etiology
CongenitalIdiopathic
Drugs: Antibiotics (Chloramphenicol)Antiinflammatory (Phenylbutazone)Anticonvulsant (Phenytoin)
Acquired
Radiation:Chemotherapeutic agents
Viral or bacterial infection:
Hep non- A/BMononucleosis or Epstein-Barr VirusMumps, Measles
Toxic agents:BenzeneInsecticidesPaint thinnerLacquers
Autoimmune disease:
SLEStrong affinity to bone marrow
Bone marrow toxicity
Attacking healthy cells in the bone marrow causing alteration in the function of the bone marrow
36
Stem-cell deficiency theory: proposes that a common stem cell population is irreversibly altered, rendering it incapable of proliferation and differentiation
Microenvironmental deficiency theory: proposes that the stem cell environment (ie, the marrow) is altered so as to inhibit erythropoeisis
Absence of bone marrow cytokines (precursor to cell differentiation) and colony-stimulating factors
Altered differentiation of blood vessels. Myeloid stem cells and lymphoid stem cells cannot differentiate to precursor cells.
Altered hematopoeisis
Management:CBC Monitoring
Mngt:Bone marrow biopsy,/transplant, immunosuppressive therapy

37
Decreased RBCs, decreased hemoglobin (anemic condition)
Decreased clotting factors (platelets): Thrombocytopenia
Decreased neutrophils (neutropenia)
Decreased oxygen-carrying capacity of the blood (hypoxemia)
Bleeding and hemorrhagic tendencies
Weak immune responses
Inability to defend the body against invading pathogens
Petechiae, ecchymosis, epistaxis, bleeding from gums and from GIT
infection
Tissue hypoxia
Decreased hemoglobin concentration
Respiratory: Increase rate and depth of respiration, “exertional dyspnea”
Impaired wound healing and loss of elasticity
CNS: dizziness, fainting, lethargy
Weakness and increased fatigue
GI: abdominal pain, nausea, vomiting, loss of appetite
Kremil-S
tranexamic acid, phytomenadione
folic acid
paracetamol and ampicillinMngt:Blood transfusions

38
Pale mucous membranes, lips, nail beds, and conjunctiva
Compensatory mechanisms
Dilation of arterioles, capillaries, venules, thus increasing blood flow through them
Increase peripheral blood flow and venous return, further contributes to an increase in heart rate
Decreased blood flow detected by the kidneys and activates the renin-angiotensin response
Peripheral blood vessel constriction, diverting blood flow to essential vital organs
vasoconstriction
Legend: management and treatment
red – clinical manifestations the client green – medical management applied to patient violet – 3 types of aplastic anemia
O2 inhalation
Water and salt retention
Decreased urine output
Heart failure

Blood transfusions
People with severe aplastic anemia usually need blood transfusions.
Platelet transfusions reduce the risk of life-threatening bleeding caused by very low numbers
of platelets.
Red blood cell transfusions reduce problems with being very tired and short of breath.
Transfusions are an important treatment to manage the symptoms of aplastic anemia. For
patients with severe aplastic anemia, doctors try to give as few transfusions as possible to:
Limit the amount of iron that builds up in the body from red blood cell transfusions. Large
amounts of iron in the body cause organ damage. Patients who need many red blood cell
transfusions may receive additional treatment to remove iron from the body. Iron-chelating
should be instituted if iron overload occurs. Became iron chelating therapy became available,
this complication was a leading cause of death.
Reduce risks the immune system will develop antibodies (immune cells) that attack transfused
platelets.
Prepare for the possibility of a transplant. For patients treated with transplant, having many
transfusions increases transplant risks.
39
In addition, it is common to treat the blood with radiation and to filter the white blood cells out of the blood before it is given in a
transfusion. These steps help reduce the risks of an immune system reaction against transfused platelets and risks of a potential
transplant, as well as risks of other possible complications.
If there is any chance a patient may receive a transplant, the doctor will avoid giving the patient blood donated by a family
member. If that family member is later found to be a suitable donor for a transplant, the patient's immune system may react
against the transplant.
Infection prevention
People with severe aplastic anemia are at risk for life-threatening infections. Even a common infection like a cold could become
serious. To help prevent infection, people with severe aplastic anemia need to protect themselves from germs. Steps to take may
include avoiding crowds and sick people.
Fungal infections are a major. Clients should be treated with a broad-based
antibiotic with gram-negative and staphylococcal coverage. For clients with
febrile neutropenia, antipseudomonal therapy should be initiated. Antifungal
agents should be considered for those with persistent fever.
Bone Marrow Biopsy
40

In a bone marrow biopsy, cells are collected through a hollow needle inserted into the outer edge of a hipbone, scapula, or from
the patella which contains marrow is removed with a special needle. The marrow sample is examined with a microscope for the
presence of abnormal cells.
Bone Marrow Transplantation (BMT)
For many patients with severe or very severe aplastic
anemia, a bone ma rrow transplant is the preferred
standard treatment. A transplant replaces the abnormal
cells in the bone marrow with healthy blood-forming cells
from a family member or unrelated donor.
The donor for a transplant must closely match the
patient's tissue type. The best donor is usually a matched
sibling. Unrelated donors are only used if
immunosuppressive therapy is unsuccessful.
A transplant can offer the best chance for a cure of
aplastic anemia, but it is not an option for all patients. A
transplant may be a good option for patients who have a
suitable donor or and are healthy enough to tolerate a
41
transplant. Children and young adults tend to do better than older patients, but advances in transplant have enabled older
patients to undergo a transplant successfully.
Transplants for aplastic anemia can have serious risks. However, doctors have developed treatment methods to address many of
these risks and transplant outcomes have improved in the last decade.
One risk that is greater for patients with aplastic anemia than for many other diseases is graft rejection or graft failure (when the
transplanted cells do not grow and make blood cells for the body). Having many transfusions increases the risk of graft rejection
because the patient's immune system may develop antibodies that can react against the transplanted cells. Today, doctors give
aplastic anemia patients as few transfusions as possible. The transfused blood is also commonly treated with radiation and filtered
to remove the white blood cells. These practices have improved transplant outcomes.
Another serious risk of transplant for patients with aplastic anemia is graft-versus-host disease (GVHD). This is a common
transplant complication that can range from mild to severe. For patients who receive a transplant to treat leukemia or another
cancer, GVHD may be associated with a beneficial graft-versus-leukemia effect. However, there is no benefit to GVHD for patients
with aplastic anemia. Advances in the treatment of GVHD have reduced this risk, but doctors continue to search for better
treatments.
Immunosuppressive therapy
Immunosuppressive therapy is one of two standard treatments that have the potential to offer a person with severe aplastic
anemia a longer life. The other treatment, a transplant, is often recommended as the first treatment for children and young adults
with a suitable sibling donor. Immunosuppressive therapy is often recommended as the first treatment for patients who:
Are older than age 60
42

Are unable to tolerate a transplant because of other health problems or older age.
Do not have a suitable donor for transplant.
Will be treated with transplant, but are waiting for a suitable donor to be found.
Choose immunosuppressive therapy after weighing the potential risks and benefits of all options.
Combination therapy is used and usually includes cyclosporine (Neoral, Sandimmune), ATG (antithymocyte globulin), ALG
(antilymphocyte globulin), cyclosporine A, and methylprednisolone, with or without cytokine support. Because a central venous
catheter is required for immunosuppressive therapy, clients should be carefully monitored for the development of infection.
The immune system is made up of organs and cells that work together to protect the body from infection and disease. The immune system uses white blood cells to
fight infections. The white blood cells mark and attack cells that they do not recognize as belonging in the body. Immunosuppressive therapy uses drugs that
suppress (weaken) the immune system. This treatment is based on the widely accepted theory that aplastic anemia is a result of the immune system attacking the
bone marrow. Immunosuppressive therapy weakens the immune system's response and allows the marrow to make more blood cells. For many people,
immunosuppressive therapy raises blood counts to normal or near normal levels and leads to long-term survival.
Growth factors
Growth factors are drugs that help the body make more blood cells. A person with aplastic anemia may be given growth factors to
try to reduce the need for red blood cell transfusions. However, in many cases of aplastic anemia, the marrow does not respond to
growth factors.
Growth factors may also be given after treatment with immunosuppressive therapy or transplant. In this case, growth factors often
are effective. They can help speed up new blood cell production, reducing a person's need for transfusions and reducing infection
risks.
43

Diet Adjustments
For clients who are neutropenic or are on immunosuppressive therapy, foods that are likely to harbor bacteria, fungi, or mold (ex. raw meat, dairy products, certain
fruits and vegetables) should be avoided.
Laboratory Exams
Laboratory Exam Results Normal Values Implication
Hemoglobin
4-16-08
3.4
4-22-08
7.9 13-16 g% Hemoglobin (Hgb or Hb) is the protein molecule in red blood cells that carries oxygen as blood circulates throughout the body. Hemoglobin gives blood its red color. The hemoglobin test measures the amount of hemoglobin in a patient’s blood and gives a good indication of a blood cell’s ability to transport oxygen.
Hematocrit 9.3 20.9 42-50 g% Hematocrit (Hct) refers to the percentage of blood consisting of red blood cells. Hematocrit (meaning “to separate blood”) is an indicator of both the number and the size of red blood cells.
WBC 3,400 5-10T/cumm WBC is commonly used to indicate the presence of an infection such as appendicitis, a blood disease such as
44

leukemia or to monitor the body’s response to cancer treatment.
Neutrophil Seg 12 55-60% The absolute neutrophil count (ANC) indicates whether white blood cells are being produced normally.
Lymphocyte 79 20-35% Lymphocytes react with antigen and generate diverse antibodies that protect the host against infection. The patient’s increased results indicate the presence of infection.
Monocyte 6 1-6% Monocytes help in phagocytosis. His result is within normal limits.
Eosinophil 3 1-4% It’s function is for phagocytosis, antibody-mediated defense against parasites, allergic reactions and recovery phase infection. His result is within normal limits.
Platelet Count 22,000 10,000 150-400T/cumm This test counts the number of platelets within a specific amount (usually a cubic millimeter) of blood. Platelets are the smallest type of blood cell and play a major role in blood clotting. Too few platelets can lead to uncontrolled bleeding.
Bloodtyping A+ Blood typing is a means of determining the presence of ABO antibodies as well as the Rh factor. The test was requested by the physician not only to detect the blood type of the client but also to detect the blood of perspective donors.
45
PharmacologyGeneric Name: prednisone
Brand Name: Novo-prednisone
Drug Class: Corticosteroid, Glucocorticoid
Action: enters target cells and binds to intracellular corticosteroid receptors, initiating many complex reactions that are
responsible for its anti-inflammatory and immunosuppressive effects.
Indications:
hematologic disorder: thrombocytopenia purpura and erythroblastopenia
hypercalcemia associated with cancer
replacement therapy in adrenal cortical in sufficiency
Contraindications:
contraindicated with infection, specially tuberculosis, fungal infections, amebiasis, vaccinia and varicella, and antibiotic
resistant infections; lactation
use cautiously with kidney or liver disease, hypertension, seizure disorders, diabetes mellitus, pregnancy
Adverse effects:
46
vertigo, headache, paresthesia, insomnia, seizure, cataracts, hypotension, shock, hypertension and CHF fluid retention, Na+
and fluid retention, hypocalcemia, hypokalemia, irregular menses, increase blood sugar, abdominal distention, nausea and
vomiting, muscle weakness, immunosuppression impaired wound healing
Nursing Responsibilities:
do not stop intake of the drug without consulting health care provider
avoid exposure to infection
teach patient to report unusual weight gain, swelling of extremities, muscle weakness, black or tarry stool, fever, or any
other infections
Increase dosage as ordered when patient is subjected to stress.
Generic Name: ampicillin
Brand Name: Ampicin, novo-ampicillin
Drug class: Antibiotic, Penicillin
Action: bacterial action against sensitive organisms; inhibits synthesis of bacterial cell wall, causing cell death.
Indication:
Treatment of infection caused by strains of Shigella, Salmonella, E. coli, H. influenza, P. mirabibis, N. gonorrhoeae,
enterococci, gram negative organisms,
Meningitis caused by Neisseria meningitides
Contraindications:
Contraindicated with allergies to penicillins, cephalosporins, or other allergies.
Use cautiously with renal failure and lactation
Adverse effect:
47

Seizure, nausea and vomiting, diarrhea, abdominal pain, nephritis, anemia, thrombocytopenia, leucopenia, neutropenia,
prolonged bleeding time, rash, fever, wheezing, anaphylaxis, phlebitis, thrombosis at injection site, and superinfection like
oral and rectal moniliasis, vaginismus
Nursing Responsibilities:
Check IV site carefully for signs of thrombosis or drug reaction
Do not give IM injection on the same site; atrophy can occur. Monitor injection site.
Administer oral drug in an empty stomach, 1 hour before or 2 hours after meals with full glass of water, do not give with fruit
juice or soft drink
Report pain or discomfort at sites, unusual bleeding or bruising, mouth sores, rash, hives, fever, itching, severe diarrhea,
difficulty breathing.
Do not use for self treatment without prescription of a physician
Generic Name: folic acid (folate)
Brand Name: Folvite
Drug Class: folic acid, vitamin supplement
Action: required for nucleoprotein synthesis and maintenance of normal erythropoiesis.
Indication: treatment of megaloblastic anemias due to sprue, nutritional deficiency, pregnancy, infancy, and childhood
Contraindications:
Contraindicated with allergy to folic acid preparations, pernicious, normocyctic anemia.
Use cautiously during lactation
Nursing Responsibility:
Administer orally if at all possible. With severe GI malabsorption or severe disease, give IM, IV, or subcutaneously
48

Test using schilling test and serum vitamin B12 levels due to rule out pernicious anemia. It masks the signs of pernicious
anemia while the neurologic deterioration continues.
Tell patient to report rash, difficulty breathing, pain or discomfort at injection site.
Generic name: tranexamic acid (cyklokapron)
Brand Name: Hemostan
Drug Class: Hemostatics
Action:
Is a competitive inhibitor of plasminogen activation and may directly interfere with the action of plasmin at high
concentrations. Thrombin time is prolonged, but the drug has no effect on platelet aggregation or coagulation time.
Indications
:
Antihemorrhagic & antifibrinolytic for effective hemostasis in various surgical & clinical cases, in traumatic injuries, post-
tooth extraction & other dental procedures.
prevention of heavy bleeding such as heavy periods, nose bleeds
Prevention of bleeding during tooth extraction in hemophiliacs (people who lack a clotting factor) Hereditary angioneurotic
edema (excess fluid around the body)
Adverse Reaction:
GI disorders, nausea, vomiting, anorexia, headache may appear, impaired renal insufficiency, hypotension when IV infusion
is too rapid.
Diarrhea, giddiness, visual abnormalities
49
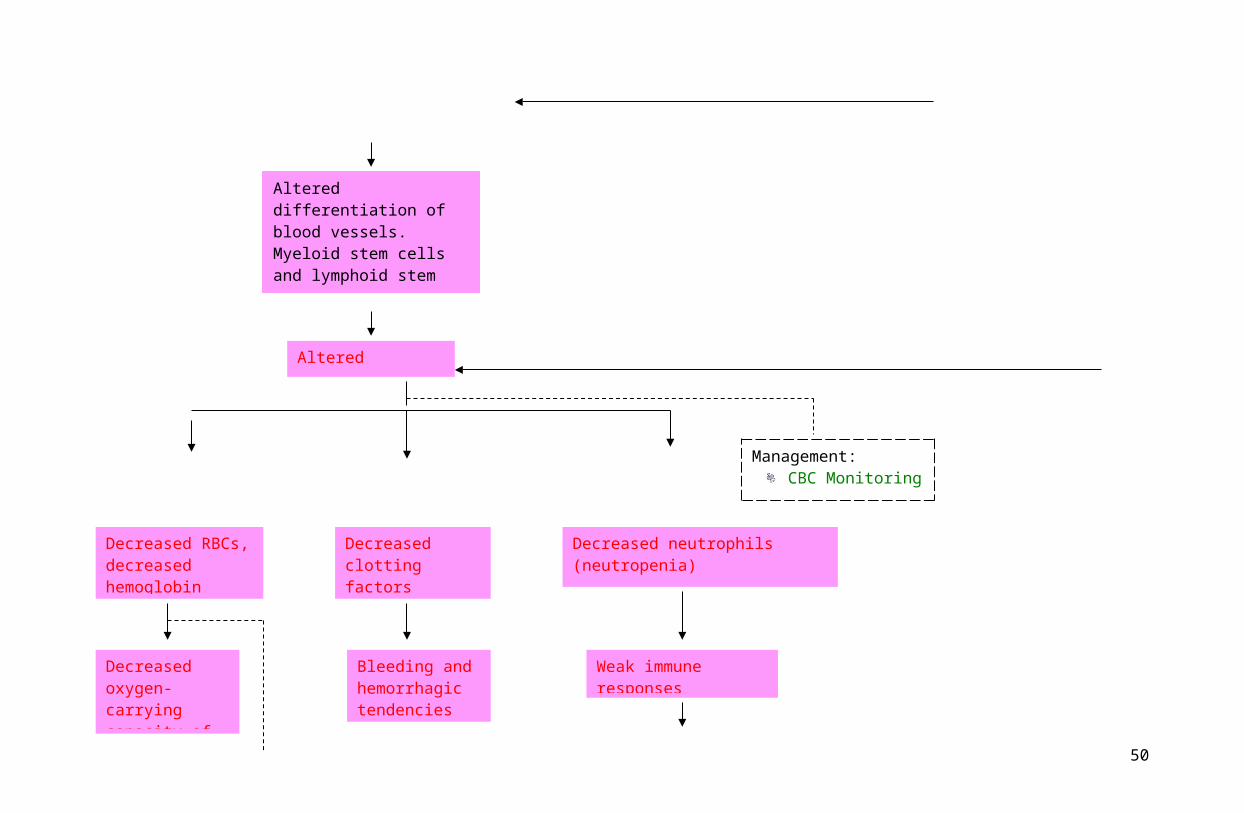
Nursing responsibilities:
Close mentoring for signs of clot formation such as chest pain, change in color, temp., or pain in the extremities, dyspnea,
abdominal pain, changes in neurological signs or changes in peripheral pulse.
If bleeding continues to be severe, emergency treatment may be instituted while aminocaproic acid is being given. Fresh
whole blood or fibrinogen may be infused to provide clotting factors
Not advisable to use for prolonged periods in patients predisposed to thrombosis.
May be taken with or without food.
Before taking tranexamic acid make sure the doctor or pharmacist knows:
If you are pregnant, trying for a baby or breast-feeding.
If you have a history of thromboembolic disease (where a blood clot forms and travels in the bloodstream).
If you have kidney problems.
If you suffer from undiagnosed irregular menstrual bleeding.
Generic Name: aluminum magnesium
Brand Name: Kremil S
Drug Class: Antacids & Antiulcer
Action: reduces total acid load in gastrointestinal tract, elevates gastic pH to reduce pepsin activity, strengthens gastric mucosal
barrier, and increases esophageal sphincter tone.
Indication: acid indigestion
Contraindications:
Patients with renal failure. Partial intestinal obstruction, appendicitis, fecal impaction, gastric outlet obstruction &
constipation. Phosphate depletion, low serum phosphate & osteomalacia.
50
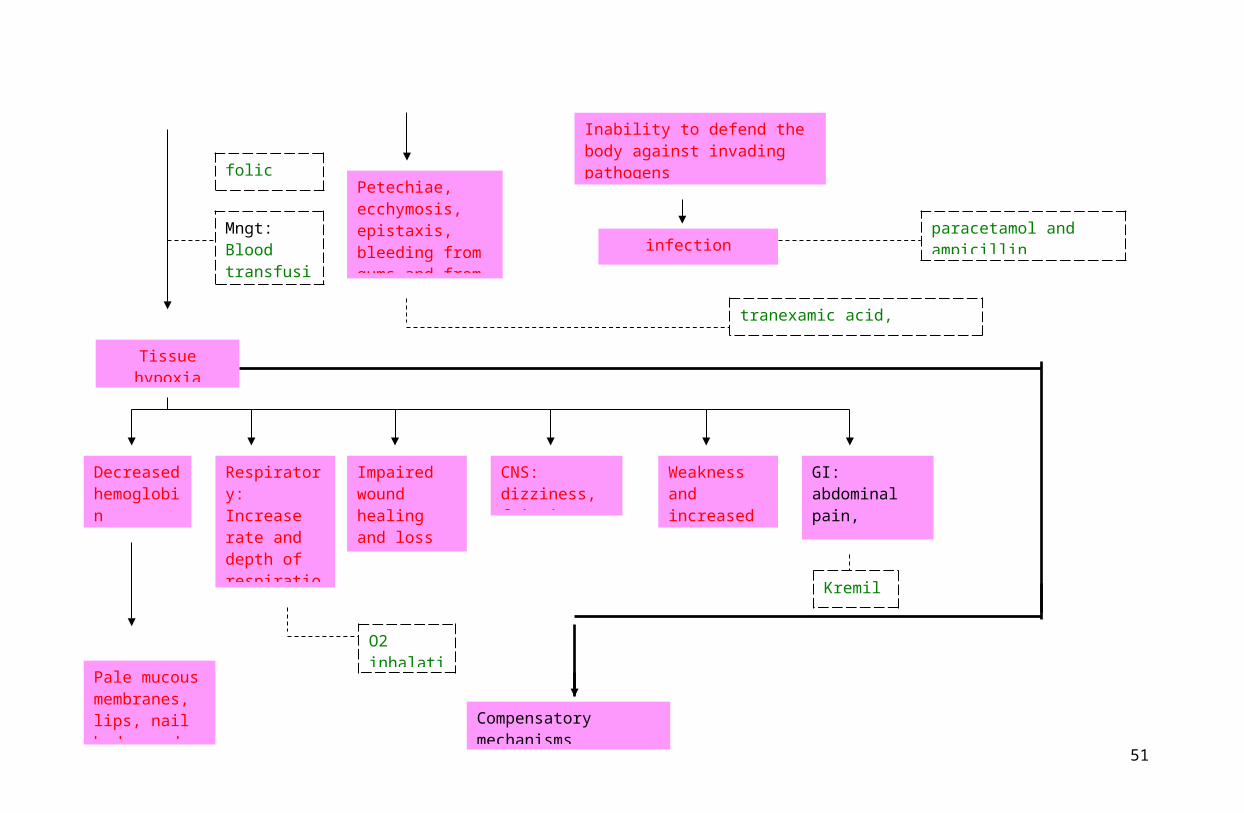
Adverse Reaction:
Mild constipation, diarrhea, increased urine pH, hypokalemia.
Nursing
responsibilities:
Urge patient to notify prescriber about signs and symptoms of gastrointestinal bleeding, such as tarry stool, or coffee-ground
vomitus.
Monitor magnesium level with mild renal impairment. Symptomatic hypermagnesemia usually occur in severe renal failure.
Drug has a low sodium content and is good for patients with sodium restriction
Generic name: Phytomenadione (menadiol)
Brand name: Cycomin apm, Vitakay
Drug class: Haemostatics
Action:
Promotes hepatic synthesis of blood clotting factor II, VII, IX, and X; probably by functioning as an essential cofactor for
microsomal system that activate the precursors of clotting factors.
Indication
s
Treatment of hemorrhage or threatened hemorrhage associated w/ a low blood level of prothrombin.
Treatment for vit. K deficiency caused by antibacterial therapy
Adverse Drug Effects:
Rarely, severe, shock-like reactions, phlebitis; flushing of the face, sweating, chest constriction on too rapid administration.
51
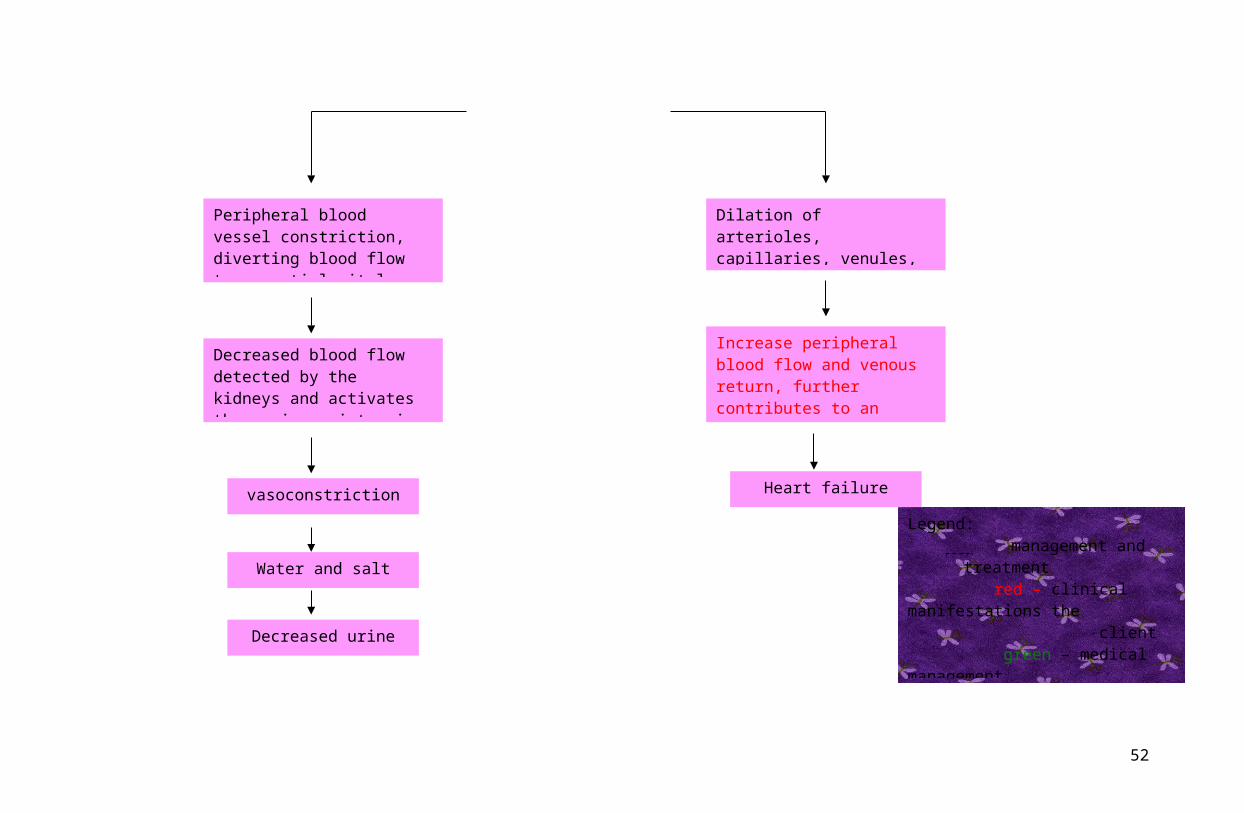
Dizziness, nausea and vomiting, tachycardia, weak pulse, chills, fever, hypotension, dyspnea, anaphylaxis
Nursing Responsibilities:
Assess and record baseline data. (V/S, weight, skincolor, Temp., lab exams)
Before taking phytomenadione make sure the doctor or pharmacist knows:
if you are pregnant, trying for a baby or breast-feeding
if you have ever had an allergic reaction to this or any other medicine
if you are taking any other medicines, including those available to buy without a prescription, herbal and complementary
medicines
Take the medication exactly as directed by the doctor. Never take more than the prescribed dose.
Monitor prothrombin time.
Generic Name: paracetamol
Brand Name: Tempra, Tylenol
Classification: antipyretic and analgesic
Action:
Analgesic mechanism of action has not been completely established
Elevates pain threshold by blocking Prostaglandin synthesis in the CNS
Decreases elevated temperature by locking the action of endogenous pyrogens
Indications:
52
relief of mild to moderate pain, dysmenorrhea
Reduction of elevated temperature associated with colds, bacterial and viral infections
Contraindications:
Glucose -6- phosphate dehydrogenase deficiency
Cautious use in patients with kidney disease
Adverse reaction:
Urticaria, hypoglycemia, CNS stimulation, cyanosis, hemophylactic anemia, leucopenia, kidney damage, psychological
changes
Acute poisoning is characterized by chills, diarrhea, fever, skin eruptions, palpitations, depression, convulsion,
Hepatotoxicity (5-8g/day)
Nursing responsibilities:
Administer with food or after meals, full glass of water
Caution patients with excessive or prolonged use.
Drug should be use cautiously in rheumatic conditions because of its non-antinflammatory effect.
Teach patient to notify nurse or doctor if rashes, bleeding, and changes in voiding pattern occurs.
53

Cues & Evidences Nursing Diagnosis Objectives Interventions Rationale Evaluation
Subjective: Complained
difficulty breathing after going to the comfort room
Complained headache upon awakening
Objective: Respiratory rate: 31
cpm, with use of accessory muscles
Pulse rate of 121 bpm
Exertional breathing noted
Weak and lethargic
Very pale skin color
Impaired gas exchange related to decreased oxygen-carrying capacity of the blood
Within our care, the client will be able to demonstrate improved ventilation and adequate oxygenation as evidenced by:
Vital sings within normal limits:o T= 36.5-37.5 oCo P=70-85 bpm,
strong, and regular
o R= 16-20 cpm, silent and effortless
o BP=112/60 mmHg
reduced cyanosis in the nail beds
Independent Monitor respiratory
rate, depth, and effort, including use of accessory muscles, nasal flaring, and abnormal breathing patterns.
Auscultate breath sounds every 1-2 hours.
Monitor vital signs; note changes in cardiac rhythm.
- Increased respiratory rate, use of accessory muscles, nasal flaring, abdominal breathing, and a look of panic in the client’s eyes may be seen with hypoxia.
- The presence of crackles and wheezes may alert the nurse to airway obstruction, which may lead to or exacerbate existing tissue hypoxia.
- Compensatory changes in vital sings and development of dysrhythmias reflect effects of hypoxia on
At the end of our care, the client was able to demonstrate improved ventilation and adequate oxygenation as evidenced by:
Not met. Respiratory rate (31cpm) and pulse rate (121 bpm) still above normal limits
Not met. There was
still use of accessory muscles during inhalation because of difficulty breathing
54

Pale and cracked, dry lips
Excessively perspiring
Very poor capillary refill
Lab results:o Hemoglobin –
3.4 g%o Hematocrit – 9.3
vol% O2 inhalation 3-
4L/min Medications:
o Folic Acid
minimize the use of accessory muscles
participation in treatment regimen such as breathing exercises and effective coughing, within the level of his ability
exert additional movements in the arms and legs
Observe for cyanosis particularly in the lips and nail beds;
Assist in turning, coughing, and deep-breathing exercises.
Encourage patient to alternate periods physical activity. Schedule rest periods as indicated.
Promote adequate fluid intake of 6-8 glasses per day
Collaborative Administer
supplemental humidified oxygen as indicated.
cardiovascular system.
- changes reflect diminished circulation/hypoxia potentiating capillary occlusion.- Promotes optimal chest expansion, mobilization of secretions, and aeration of all lung fields; reduces risk of stasis of secretions/pneumonia.
- Protects from excessive fatigue and reduces oxygen demands. The hypoxic client has limited reserves; inappropriate activity can increase hypoxia.
- Sufficient intake is necessary to provide for mobilization of secretions.
- Maximizes oxygen transport to tissues.
Not met. Presence of cyanosis in the nail beds was not reduced.
Not met. Was not able to participate in deep breathing and coughing due to fatigability
Not met. Not able to perform physical activities because of severe fatigability.
Not met. Fluid intake is only 3 glasses for that day.
Met. O2 inhalation of having 3-4 L/min
55

Administer packed RBCs as indicated.
Administer meds as ordered:
o prednisone 10g/tab 1 tab tid PO
o Kremil S 1 tab tido paracetamol 3-
5g/tab 1 tab q6ho ampicillin 500g
IVTT q6ho folic acid 5
mg/tab odo tranexamic acid
150mg IVTT q8h
o phytomenadione 1 ampule IVTT stat
- Increases number of oxygen-carrying cells.
- for effective outcomes of therapy
Not met. Only 4 out 8 blood bags were administered because of inability to secure it.
Met. All medications were administered as ordered.
56
Cues & Evidences Nursing Diagnosis Objectives Interventions Rationale Evaluation
Subjective:
Complains of fatigue
and weakness.
Objective:
Weakness noted
Has non-productive
cough for 2 days
Presence of IV fluid
at left metacarpal
vein running for 41
microdrops/minute
Has poor appetite
Bleeding on the lips
when he brushed his
teeth
Lab results:
High risk for infection related to inadequate secondary defenses
Within our care, the client will remain free from signs and symptoms of infection as evidenced by:
free of any evidence of new bleeding
vital signs within normal range:
o T= 36.5-37.5 oCo P=70-85 bpm,
strong, and regular
o R= 16-20 cpm, silent and effortless
o BP=112/60 mmHg
Observe ways to prevent infection such as washing
Independent Take vital signs every
4hours.
Use appropriate hand hygiene.
Limit and screen visitors.
Monitor the client’s risk for bleeding; evaluate results of clotting studies and platelet counts.
Have the client use a
- Changes in vital signs can indicate the onset of bleeding or infection.
- Improved adherence to hand hygiene has been shown to lessen outbreaks of infection in health care facilities, to reduce transmission of antimicrobial-resistant organisms.
- It minimizes exposure to infectious microorganisms.
- Laboratory studies give a good indication of the seriousness of the bleeding disorder.
- This action helps
At the end of our care, the client was able to remain free from signs and symptoms if infection as evidenced by:
Met. There was no evidence of new bleeding noted.
Not met. Vital signs were still above normal:
T 38.2 oC P 121 bpm R 31 cpm BP 124/72 mmHg
Met. He also verbalized precautions to take to prevent bleeding such as frequent hand
57
- WBC – 3,400/cumm
- Neutrophil – 12
- Lymphocyte – 79 %
- Monocyte – 6 %
- Eosinophil – 3 %
hands
Take necessary precautions to prevent bleeding in the lips and gums.
Minimize frequent visitors which may be a source of pathogens
Observe strict reverse isolation techniques by being in a private room, away from other patients
very soft child’s toothbrush.
Dependent Monitor for and
report signs of infection (e.g., fever, chills, flushed skin, drainage, edema, redness, abnormal lab values and pain)
Administer medications as orederd: o prednisone
10g/tab 1 tab tid PO
o Kremil S 1 tab tido paracetamol 3-
5g/tab 1 tab q6ho ampicillin 500g
IVTT q6ho folic acid 5
mg/tab odo tranexamic acid
150mg IVTT q8ho phytomenadione
1 ampule IVTT stat
prevent trauma to the oral mucosa, which result in bleeding.
- The immune system is stimulated with the onset of infection, which results in classic signs of infection. Antibiotics must be given promptly in neutropenic clients because a delay increases morbidity and mortality.
-following required treatment regimen is essential to improve the prognosis of the condition
washing.
Not met. Client was not able to secure a new soft, bristled toothbrush.
Not met. Visitors often come and go. Strict reverse isolation precautions were also not met because of lack of knowledge of the disease condition.
Met. All meds were administered.
58

Give medications orally or intravenously only; avoid giving them intramuscularly, subcutaneously or rectally. Apply pressure for a longer time than usual to
invasive sites.
- Additional pressure is needed to stop bleeding sites of clients with bleeding disorders.
Cues & Evidences Nursing Diagnosis Objectives Interventions Rationale Evaluation
Subjective:
Mother verbalized
that the child eats
very little only
February of this year,
he weighed 32kgs
Objective:
Weakness
Imbalanced nutrition: less than body requirements related to weakness and poor appetite
Within our care, the client will have improved nutritional status as evidenced by:
progressive weight gain or stable weight.
laboratory values within normal range.
Independent Determine or measure
the child’s body weight
Observe and record patient’s food intake
Provide
- Determining the child’s body weight can provide baseline data for future comparisons to check on the improvement of his nutritional status.
- Monitors caloric intake or insufficient quality of food consumption.
- Mealtime usually is a
At the end of our care, objectives were not met as evidenced by:
There was decrease in weight. From 28 kgs, weight decreased to 27 kgs.
Laboratory values remained to be below normal.
59

noted
Decrease tolerance
for activity
Decreased
consumption; intake
of only 2-4 tbsp of
rice
Weight upon
admission: 28 kgs
Weight during
assessment: 27 kgs
absence of signs of malnutrition.
consumption of adequate nourishment.
Verbalization appropriate of nutritional requirements
companionship at mealtime to encourage nutritional intake.
Consider six small nutrient-dense meals versus three larger meals daily to reduce the feeling of fullness.
Encourage mother to offer foods rich in iron, and vitamin B12, C and folic acid.
Do health teaching to the child and to the significant other as to the importance of consuming adequate nutrition.
Encourage the client’s family to bring foods usually preferred by the client, provided
time for social interaction; often clients will eat more food if other people are present at mealtimes.
- Eating small, frequent meals reduces the sensation of fullness and decreases the stimulus to vomit.
- Heme iron in meat, fish, and poultry is absorbed more readily than nonheme iron in plants. Vitamin C increases the solubility of iron. Vitamin B12 and folic acid are necessary for erythropoiesis.
- Knowledge of the importance of consuming adequate nourishment can foster compliance.
- Offering foods usually preferred by the client will help increase consumption and have
He had pale and dry skin, looked frail and weak
He displayed poor appetite. Ate only 2 tbsp of rice.
He was too weak to verbalize nutritional requirements. He avoided any interactions because he wants to rest.
60

that these foods are nutritious and safe to eat.
Build on the strengths in the client’s food habits.
Collaborative Administer folic acid
5mg 1 tab OD as indicated
Administer phytomenadione 1 ampule IVTT as ordered
good appetite.
- Accepting the client’s preferences shows respect and would give encouragement to the patient to comply with interventions.
- required for nucleoprotein synthesis and maintenance of normal erythropoiesis.
- Promotes hepatic synthesis of blood clotting factor II, VII, IX, and X; probably by functioning as an essential cofactor for microsomal system that activate the precursors of clotting factors.
61
Cues & Evidences Nursing Diagnosis Objectives Interventions Rationale Evaluation
Subjective:
Mother verbalized
that PTA, client
can’t tolerate
running even for just
a short while; he
would usually catch
his breath
Patient verbalized
that he would just lie
Activity intolerance related to low hemoglobin levels
Within our care, the client will tolerate activity as evidenced by:
report of an increase in activity tolerance including ADLs.
pulse, respirations and blood pressure within patient’s normal range.
Independent Determine cause of
activity intolerance and determine whether cause is physical, psychological, or motivational
Asses the client daily for appropriateness of activity and bed rest orders.
- Determining the cause of a disease can help direct appropriate interventions.
- Inappropriate prolonged bed rest orders may contribute to activity intolerance.
At the end of our care, objectives were not met as evidenced by:
Client remained in lying in bed most of the time.
Pulse, respirations, and blood pressure remained to be above normal
62

down while student
nurse held his hand
to count for the pulse
Objective:
He usually lies on his
bed
Can’t tolerate sitting
on top of bed for long
Needs to be fed and
prefers lying down
while eating
Can’t tolerate going
to the bathroom
during urination; uses
a bedpan instead
Respiratory rate:
31cpm
Ordered oxygen
therapy at
3-4L/minute
Lab results:
display of laboratory values (hemoglobin and hematocrit) within acceptable range.
normal skin color and skin is warm and dry with activity
When getting up the client, observe for symptoms of intolerance such as nausea, pallor, dizziness, visual dimming, and impaired consciousness, as well as changes in vital signs.
Perform range of motion exercises if the client if the client is unable to tolerate activity.
Allow for rest periods before and after planned exertion periods such as meals, baths, treatments, and physical activity.
Place objects within client’s reach.
- Heart rate and blood pressure responses to orthostasis vary widely. Vital signs changes by themselves and should not define orthostatic intolerance.
- Inactivity rapidly contributes to muscle shortening and changes in periarticular and cartilaginous joint structure. These`factors contribute to contracture and limitation of motion.
- Rest periods decrease oxygen consumption and promote client comfort.
- Placing objects within his reach conserves energy.
Laboratory results remained to be below normal: Hgb 7.9 g% Hct 20.9 vol% Platelet10T/
cumm
Skin was still very pale
63

o Hemoglobin – 3.4 g%
o Hematocrit – 9.3 vol%
o Platelet – 22,000/cumm
Provide emotional support and encouragement to the client to gradually increase activity.
Collaborative Monitor laboratory
studies (Hb/Hct and RBC count).
Provide supplemental oxygen as indicated.
Administer packed RBCs as indicated. Monitor closely for transfusion reactions.
- Fear of breathlessness, pain, or falling may decrease willingness to increase activity.
- Identifies deficiencies in RBC components affecting oxygen transport and treatment needs
- Maximizing oxygen transport to tissues improves ability to function.
- Increases number of oxygen-carrying cells; corrects deficiencies to reduce risk of hemorrhage in acutely compromised individuals.
64
List of Nursing Diagnoses
Impaired gas exchange related to decreased oxygen-carrying
capacity of the blood
Ineffective protection related to abnormal blood profiles secondary
to aplastic anemia
Imbalanced nutrition: less than body requirements related to
weakness and poor appetite
65

Activity intolerance related to low hemoglobin levels
Ineffective tissue perfusion related to decreased hemoglobin
concentration in the blood
Fatigue related to decreased oxygen supply to the body
Disturbed body image related to severe pallor
Ineffective therapeutic regimen management related to economic
difficulties
SynthesisThe entire pediatric rotation was one of the most promising and most unforgettable experiences that we ever had. We had difficult y in
dealing with pediatric patients because they are afraid of medical health members because of their perception and anticipation that we will do
something harm to them. We were very grateful that we were rotated in Negros Oriental Provincial Hospital Pediatrics Ward because it is in
66
there that we deal with sick infants and children and some of them are less fortunate when talking about financial constraints. We have
encountered different childhood diseases and disorders and learn how to deal and care for them if situation persist. We had an amazing
experience that within 3 weeks of the rotation, we learned many things that would be a great help of our future career. We took this rotation
not as a challenge but a stepping stone to success because we know that we would undergo hardships and its topics are really difficult to
tackle. Perseverance and dedication to ones duty and work made us face every trial that we have encountered.
This rotation made us realize that we, people, especially children can acquire different diseases if there is no proper care, and safety
preventions because their immune system is not yet well developed. It is through proper prevention and control of illness that would help us in
minimizing transmission of diseases. These patients were a big help to us because without them, we could not practice our skills and
knowledge that we have learned in school. We conducted health teachings that would help our clients and families gain knowledge about the
proper prevention and safety methods in caring for their children. Despite the difficulties and the hardships that we had face during the
rotation, we still enjoyed this rotation and we’re very thankful that we extended our help to the pediatric patients and their families even in
our own little ways. Now that the rotation is almost over, we will miss the fun and the laughter that we have shared with our patients but the
knowledge and the learning that we have learned from them will always be in our minds and hearts.
We could still remember that when we had our first assessment of our patient, he smiled, was jolly, energetic, and optimistic that he
would get well with the help of the hospital staff and emotional support from his family. His condition served as an encouragement and a
challenge for us to do appropriate intervention and to do everything that we could to help him in his condition. We wish that he would recover
from his illness, able to surpass the trials that he is facing right now and is able to go back to his normal life as a kid with good health. We will
surely miss our client who was there to strengthen our knowledge and skills and made an impression out of our lives. We would also miss
other patients there and the staff nurses especially our clinical instructor who is with us in every step of the way. Thanks to this rotation, we
have developed the skill and the knowledge to be a more competitive burse in the days to come.
67
Articles
Katy's StoryKatelyn Rose Hubbell turned four years old on June 26th
1997, and had a big party at her home in Fisher, Illinois. She was a happy, healthy little girl, until July 11, 1997 when she was diagnosed with a life threatening bone marrow failure disease called Severe Aplastic Anemia. In case you didn't know, bone marrow is the soft spongy material inside your bones that is home to stem cells. Stem Cells are the little factories that produce the three types of blood cells, that along with a liquid called plasma, makes up your blood. In people with Aplastic Anemia, the workers in the "factory" go on strike. They do not produce enough blood cells to keep the patient alive.
On June 17th of 1998, Katy underwent a second round of immunosuppressive therapy, only this time with a much stronger drug, Cytoxan. Cytoxan (a.k.a. Cyclophosphamide) is a chemotherapy drug often used to treat cancer patients. It is a powerful immunosuppressant, "wiping the slate clean" so to speak, as it kills off peripheral blood cells in an attempt to stop Katy's t-cells from attacking her stem cells. Nearly 10 months post her Cytoxan therapy, it became clear that Katy was not responding. Her blood counts were still slipping daily, she was still dependent upon twice-monthly platelet transfusions, and required daily Epogen and Neupogen injections to stimulate her red and white blood cells. As a result, Katy's doctors planned a Bone Marrow Transplant for
Katy on May 7th, 1999, at Texas Children's Hospital in Houston.
We are happy to report that Katy's bone marrow transplant was a success, and her new marrow is working beautifully! We thank God, and her hero bone marrow donor, Ernie, every day for this miracle of new life. Katy still suffers some side effects from the toxicity of the chemo/radiation therapy that she received before her transplant. She suffered some permanent neurological damage, which may take years to fully reveal itself. She is growth hormone deficient, and requires nightly HGH injections in order to grow and feel good. Radiation to her eyes has caused cataracts to form which will eventually require surgery. Despite these new challenges, Katy continues to amaze us, and every day with our smiling little girl is a gift.
One year after her BMT, Katy Rose experienced some unexpected complications. On May 20th, 2000 she had a terrible nosebleed, and an emergency CBC showed that her platelets had plummeted to only 14,000. We rushed back to Houston, and a bone marrow biopsy confirmed that her graft was solid, but somehow her platelets and red blood cells were being destroyed once they entered her peripheral bloodstream. She was treated with high dose steroids, and over a period of 6 weeks, her counts normalized, and she was back on track to recovery from her transplant.
68

Reaction:
Katelyn, despite with her happy birthday party, was diagnosed to have aplastic anemia which served as a trial to her and her family as well. Immunosuppressive therapy was implemented on her care but despite the medication and the therapy, after 10 months, it was not successful so she has to undergo another therapy for her bone marrow to be cured. Bone marrow transplantation was the next option of the doctor attending her care. They found a donor named Ernie and was thankful of him for the bone marrow that he donated for Katelyn. After the operation, another problem arises and that is the toxicity of chemotherapy and developed a cataract on her eyes due to radiation therapy. Despite these complications, she still managed to smile and be
strong. They thought that she would get well after sometime but another challenge came up and that is nosebleeding because of very low platelet. It was confirmed that the transplant was good but the RBC was destroyed on the peripheral bloodsteam. Steroids were introduced to treat the recent complication and after 6 weeks, she had recovered and is recovering for her transplant.
Kate had undergone many treatment and management of complications but despite these trials, she still manages to be strong and never lose hope that she will be cured because she subdues herself to the treatment for her own.
IMMUNOSUPPRESSANT THERAPY OF PATIENTS WITH APLASTIC ANEMIASurvival and Mortality
Overall survival of all patients at 7 years post treatment was 55%. Patients younger than 50 years had better survival than those older than 50 years. Patients with absolute neutrophil counts of less than 200/µL at presentation had worse survival than those with higher absolute neutrophil counts. Excess deaths in severely neutropenic patients occurred mainly in the first few months after diagnosis. There were 12 deaths in 48 patients with severe neutropenia within
3 months of treatment compared with 3 deaths in 74 patients without severe neutropenia. Sex, ethnicity, etiology, and duration of disease were not correlated with survival. Post treatment status was strongly associated with long-term prognosis, as defined by response criteria (blood cell counts inconsistent with severe aplastic anemia, transfusion-independence) or by blood cell counts. For patients classified as responders at 3 months, actuarial survival at 5 years was 86% compared with 40% for non-responders. For patients surviving to 3 months, the median platelet and reticulocyte counts were each approximately 50_103/µL. Survival of patients who had either or both counts above the median
69

value was 90% (64/71 alive) at 5 years compared with 42% (12/34 alive) for patients with both counts below the median. There were no deaths from disease more than 3 years after treatment among patients classified as responders at 3 months. For patients who responded qualitatively, quantitative counts were still of prognostic importance. Survival for responders with more robust blood cell count recovery was 91% at 5 years compared with 47% for responders with both counts below the median. Sixteen patients (13%) died before their 3-month evaluation (mostly due to fungal infection). Despite persistent thrombocytopenia, few patients died of hemorrhage. Six patients died due to complications following bone marrow transplant (immunosuppression failed in these patients). A total of 7 patients who entered the study ultimately underwent bone marrow transplantation (all from matched, unrelated donors): 4 were nonresponders and died due to transplant complications; 3 were patients classified as responders at 3 or 6 months who later evolved to myelodysplasia. Only 1 responder who relapsed with a new finding of monosomy 7 survived after a matched unrelated transplant.
Reaction:
55% survive only survives after immunosuppressive treatment and most of them are under 5o yrs of age. Most of the survivors have
neutrophil count higher than 200/ul. Patients die with severe neutrophil count or have Neutrogena during the treatment. For those who respond positively to the treatment for the first 3 months, they have higher survival percentage. Most of the patients who survived for the first three months of treatment has a platelet of 50-103/uL. Most of the survivors of the first three months of treatment survive after 3 years post treatment. Despite the treatment, patient still die because of hemorrhage due to thrombocytopenia. Also, they day because of immunosuppresion after bone marrow transplant.
Death is very evident with this disease but still there are ways to prevent and control this aplastic anemia. Despite the present or advanced treatment of today they still cant develop a treatment for aplastic anemia that could have a high percentage for survival without any adverse side effects. Most of the present treatments have side effects so some of the patients instead of responding positively to treatment, they become more ill and disease becomes more complicated.
REFERENCES:
70
Black, J. & Jacob, E. (2005). Medical-surgical nursing. 7th ed. USA: W.B. Saunders Co.
Blanchard, R. & Loeb, P.E. (2007). Nurse’s drug handbook 2007. WA: Blanchard & Loeb Publishers, LLJ.
Bullock, B.L. (1996). Pathophysiology: Adaptations and alterations in function. 4th ed. Philadelphia: Lippincott Williams & Wilkins.
Lewis, S.M., et al. (2004). Medical-surgical nursing: Assessment & management of clinical problems. 6 th ed. USA: Mosby, Inc.
McCance, K., & Huether, S. (2004). Understanding Pathophysiology. 3rd ed. St. Louis: Mosby Inc.
Porth, C. (2005). Pathophysiology: Concepts of altered health states. 7th ed. Philadelphia: Lippincott Wiliams & Wilkins.
Smeltzer, S.C. & Bare, B.G. (2004). Medical-surgical nursing 10th ed. Philadelphia: Lippincott Williams & Wilkins.
Smeltzer, S.C & Bare, B.G. (1992). Medical-surgical nursing 7th ed. Philadelphia: Lippincott Company.
Tortora, G., & Grabowski, S. (2003). Principles of Anatomy and Physiology. 10 th ed. United States: John Wiley & Sons, Inc.
Whaley, D. & Wong, D. (1995). Nursing Care of infants and children. 5th ed. St. Louis: Mosby-Year Book, Inc.
71