an integrated sonographic approach to urolithiasis
TRANSCRIPT

An Integrated Sonographic Approach to Urolithiasis
Val Smalley, Dean Benjamin, Joe Bocko, Edwin Hutsal
Arnot Ogden Medical Center, Elmira NY
An Integrated Sonographic Approach to Urolithiasis
Purpose: To assess feasibility of an integrated sonographic examination combining greyscale, color and spectral Doppler in identifying and qualifying urinary tract obstruction in patients being evaluated for persistent renal colic using computed tomography (CT) as the reference standard. Materials and Methods: From Nov. 2016 to Dec. 2017 7 patients with renal colic were enrolled following preceding non-enhanced Computed Tomography Abdomen Pelvis (CTAP). Research protocol included initial patient hydration (750-1000mL water), followed by a 15-30 minute delay, and subsequent 20-25 minute ultrasound (US) examination. US examination imaging of the bilateral urinary collecting systems included: greyscale images of the kidney, visualized ureter, and bladder; renal resistive index (RI) (interlobar arteries, 3 locations); and ureteral vesicular jet characteristics (peak velocity, frequency, duration).Results: In five of seven patients with a recent urolith identified by CT, multiple sonographic parameters identified the presence of a urolith; 2/7 patients with an elevated renal RI > 10% obstructed side; 4/5 patients with marked asymmetry (percentage terms) in UVJ characteristics with evidence of decreased flow on the obstructed side (underhydration likely accounted for absence of UVJ in remaining 1/5); and 4/5 with greyscale urinary tract dilation and/or direct stone visualization. In the remaining two patients US findings were consistent with no persistent stone/urinary obstruction.Conclusion: An integrated sonographic approach combining greyscale, color and spectral Doppler findings will identify uroliths 3mm or larger in diameter and determine if urinary obstruction is potentially significant (potential nephron loss) based on an abnormal renal resistive index (elevation > 0.7, asymmetrically increased >10%) on the obstructed side. Given the inherent lack of ionizing radiation implementation would especially benefit women (child-bearing age, gravid), pediatric and adolescent patients, and patients with recurring urolithiasis.

Introduction
Renal and ureteral stones are a common primary care problem influenced by urine composition (genetics, patient habits) and presenting with complaints ranging from sharp episodic flank pain (renal colic) and genital-urinary discomfort to vague abdominal pain.
A non-enhanced CT Abdomen and Pelvis is a common examination in the evaluation of suspected urolithiasis and uses ionizing radiation to generate images with a commensurate average effective dose of 14 mSv (1,650 days of equivalent background radiation).1
Ultrasound in contrast uses sound waves (mechanical energy) to generate grayscale (specular reflection) and Doppler (moving reflections) images.

Introduction
It has been demonstrated that greyscale ultrasound has sensitivity of up to 98% in identifying urinary obstruction2 but a low specificity due to the presence of 10-26% false positives (abnormal vessels, parapyelic cysts, large extrarenal pelvis).3
Hydronephrosis not related to an obstructing urolith may be seen with certain medications (thiazide diuretics), uretero-pelvic junction (UPJ) obstruction, vesico-ureteral reflux, and etiologies of chronic obstruction.

Introduction
Ultrasound greyscale images may reveal urinary tract dilation which may not be present during the first 48 hours of acute obstruction. Not all urinary tract dilation is due to an obstructing urolith.
If significant urinary tract obstruction occurs reflexive physiologic increased intrarenal arterial pressure occurs, which if it persists, will result in parenchymal atrophy (nephron loss). In the absence of urosepsis a ureteral stent is typically placed by 30 days post initial obstruction to prevent nephron loss.
Introduction
Ultrasound greyscale images (as well as non-enhanced Computed Tomography) provide anatomical but not direct functional information regarding the significance of obstruction.
The complete loss (nonvisualization) of a ureteral vesicular jet on the obstructed side has been observed however this is not the case with incomplete obstruction.4 Comparing differences in ureteral jet characteristics (frequency, duration, maximal velocity) between obstructed and unobstructed collecting systems provides additional information in identifying/characterizing urinary tract obstruction.5

Material and Methods
This study was approved by the institutional review board and informed written consent was obtained from patients. From November 2016 to December 2017 7 patients with renal colic were enrolled ages 40-80 (average age 3). All patients had been previously examined by non-enhanced CT AP for renal colic within the preceding 10 weeks ( 2-same day preceding research US; 2-7,8 days; 2-16,17 days; and 10 weeks prior). The patient initially examined by CT 10 weeks prior was reexamined by CT 6 days later following the research US.
All patients had unilateral urinary obstruction only and no history of prior urologic intervention.

Material and Methods (greyscale imaging)
A Phillips IU22 ultrasonography unit with a 3-5 MHz convex probe were used. Dynamic spatial compounding was applied except for calculus resolution.
An initial attempt was made to hydrate patients by requesting them to drink 750-1000 mL of water. Following a 15-30 minute waiting period, patients were scanned by one of two experienced sonographers (collective experience of 45 years), without sonographer knowledge of the symptomatic/obstructed side.
Initial sonographic greyscale images of the of the bilateral urinary collecting systems were obtained of the kidney, visualized ureter, and bladder. The characteristics of a suspected urinary calculus included noting position, size, and the presence of both shadowing and color Doppler twinkle artifact.

Material and Methods (color Doppler)
Next using color Doppler the renal resistive index (RI) was next obtained of the renal parenchymal interlobar arteries in 3 locations of each kidney.
Subsequently transverse color Doppler imaging of bladder floor for expected bilateral uretero-vesicular junction (UVJ) jets was performed for five minutes. In one patient imaging was extended beyond the initial five minute period given total absence of ipsilateral UVJ with subsequent visualization of jets on the involved side. The frequency of UVJ jets/5 minute period (per side) was recorded.

Material and Methods (spectral Doppler)
Following the recording of UVJ frequency the first five UVJ spectral wave forms were recorded per side noting duration and maximal velocity. Spectral Doppler UVJ waveforms were typically recorded using a baseline scale up to 6.6 seconds. Angle correction for maximal UVJ velocity measurements was not done.
The total examination time was typically twenty five minutes. In the patient without ipsilateral UVJ jets during the initial five minute period the total examination time was extended an additional five minutes.
Images were reviewed by an Attending Radiologist with 45 years experience.

Results (Grayscale)
In 2 out of 7 patients sonographic grayscale and Doppler findings were consistent with passage of prior stones (5x8 mm and 2x3 mm, both mid ureteral, identified 1 week prior). In 4 of 5 patients sonographic greyscale imaging identified a persistent calculus through a combination of urinary tract dilation and direct stone visualization (distal ureter, UVJ). In 1 of 7 patients greyscale findings did not identify urinary tract dilation or directly visualize a stone. Color Doppler RIs were not elevated or asymmetric. However, there was a marked discrepancy in UVJ jet duration on the right relative to the left, mean/median of 1.9 s vs. 6.6 s. Subsequent CTAP demonstrated a mid ureteral 4 mm calculus. UVJ jet velocities were similar.

Results (color Doppler):
In two of the five patients with calculi (identified during exam, subsequent CT), both presented with acute renal colic and ureteral calculi (proximal ureter 8x5 mm, UVJ 9x5 mm) identified on preceding same day CTAP. Both of these patients had significantly elevated renal RI (10%, 14%) on the obstructed side versus the non-obstructed side. Ureteral vesicular jet characteristics differed as well (discussed in spectral Doppler results).The remaining three of five patients with confirmed calculi (3 mm, 5 mm, 10x5 mm) showed similar renal RIs.

Results (spectral Doppler)
In the two patient with acute ureteral calculi (proximal ureter, UVJ) and elevated renal RIs on the obstructed side, UVJ jet characteristics (frequency, duration, velocity) also differed. In the patient with the UVJ 9x5 mm stone, the obstructed versus non obstructed side showed similar urinary jet however velocities were higher on the obstructed side with similar duration: frequency - 20 versus 21; velocities (mean, median) - 63 cm/s, 58 cm/s versus 50 cm/s, 48 cm/s; duration (mean, median) - 6.1 s, 5.5 s versus 6.8 s, 5.2 s.In the patient with a proximal ureteral 8x9 mm stone, the obstructed versus non obstructed side showed UVJ jet increased frequency but decreased velocity and duration: frequency – 15 versus 6; velocities (mean, median) - 26 cm/s, 26 cm/s versus 34 cm/s, 34 cm/s; duration (mean, median) – 1.6 s, 1.7 s versus 2.6 s, 2.7 s.

Results (spectral Doppler)
In the patient with no grey scale findings, symmetric renal RIs, and mid ureteral 4 mm stone subsequently identified on CT, UVJ jet characteristics on the obstructed side versus the non-obstructed side showed increased frequency, similar velocity, and decreased duration: frequency - 8 versus 0 initially; velocities (mean, median) - 41 cm/s, 41 cm/s versus 48 cm/s, 48 cm/s; duration (mean, median) - 1.9 s, 1.9 s versus 6.6 s, 6.6 s.In one patient with a UVJ 3 mm stone and minimal urinary tract dilation a continuous UVJ jet was visualized during the 5 minute period precluding visualization/recording of the unobstructed side.In two patients with bladder volumes less than 120 cc (hydration?, enlarged prostate) UVJ jets were not visualized at all.

Discussion and Conclusions
Despite the small number of participants with acute/recent urinary tract obstruction at the time of examination, apparent trends emerged in renal RIs and UVJ characteristics, as they relate to identifying and qualifying urinary obstruction. Using the renal RI to qualify urinary obstruction beyond grayscale ultrasound is described in the literature.6,7 Acute ureteral obstruction results in a change in intrarenal hemodynamics through the release of vasoactive factors (tromboxan A2, angiotensin II, endothelin, and nitric oxide).8,9 These result in an increase in intrarenal arterial/arteriole resistance measurable at the level of the renal interlobar arteries. Renal resistive index is higher than 0.7 during the first three years of life, between ages 4-60, 0.70 is considered the upper limit of normal.10,11 As a patient ages this value tends to increase.12 An increase in the renal RI is detectable in both vascular and parenchymal disease processes (renal vein thrombosis, renal insufficiency, renal artery stenosis, etc.).13,14 Thus in the context of urinary obstruction, an acute abnormally elevated renal RI is suggestive of decreased renal perfusion, which if it persists will potentially result in nephron loss.

Discussion and Conclusions
Combining the renal RI with ureteral jet characteristics is a more recent development in identifying and qualifying urinary tract obstruction. In 1998, Catalano et al. proposed the color Doppler ultrasonography (CDU) evaluation of the ureteric jet in patients with renal colic. Catalano determined in the case of severe obstruction there is UVJ absence or marked reduction in frequency and flow on the obstructed side.15 In 2005, Pepe et al. reported in evaluation of renal colic the combined CDU evaluation of both the renal RI and UVJ jet, has better diagnostic accuracy than conventional US, sensitivity and specificity of 98.9 and 90.9% versus 94.8 and 55.5%, respectively.16

Discussion and Conclusions
In 2013, Jandaghi et al. in the evaluation of renal colic combined color and spectral Doppler in the detailed evaluation of ureteral jet characteristics (frequency, duration, maximal velocity) between the obstructed and contralateral side in patients 55 patients with renal colic (46 with stone confirmed by CT). Jandaghi reported that when compared to the contralateral normal side, the obstructed side showed less frequency (0.59 vs 3.04 jets/min; P<0.05), shorter duration (1.24 vs. 5.26 s; P<0.05), and lower peak velocity (5.41 vs. 32.09 cm/s; P<0.05).17 Further Jandaghi derived cut-off points of 1.5 jets/minute, 2.5 s, and 19.5 cm/s for difference of ureteral jet frequency, duration, and peak velocity between obstructed and contralateral normal ureters yielding sensitivities of 97.8, 95.6, and 100% and specificities of 87, 87.9, 97.8%, respectively for the diagnosis of ureteral obstruction.18
Discussion and Conclusions
In this study both patients with acute ureteral calculi on the obstructed side demonstrated asymmetrically elevated renal RIs (9-10%,14%) with mild moderate hydronephrosis and hydroureter. Stone location appeared to influence UVJ jet characteristics; UVJ stone position increased ipsilateral UVJ jet velocity; proximal to mid ureteral stone position decreased ipsilateral jet velocity. UVJ jet measures of overall flow volume appeared to have the most consistent correlation with obstruction, variable for jet frequency, but typically decreased jet duration on the obstructed side. Overall unobstructed (normal) side UVJ jet spectral wave forms appeared more focused and less phasic. Obstructed UVJ jet spectral wave forms (if visualized) almost invariably showed episodic to constant phasicity with decrease flow volume (area under the spectral waveform curve). This was especially apparent in patients with an identified ureteral/UVJ calculus two or more weeks prior.

Discussion and Conclusions
In addressing differences in obstructed versus unobstructed ureteral jet characteristics in this study, versus values reported by Jandaghi et al., multiple factors are likely responsible. Only 5 of 7 patients in thus study had a confirmed persistent calculus (Jandaghi et al. - 46, Pepe et al. - 90). In this study with practicality in mind (hospital resources, funding, patient desire to participate) the protocol sought to only increase the standard US renal bladder evaluation by 10 minutes on average, 15 minutes maximum. Only 5 minutes were spent obtaining color Doppler real-time recording of simultaneous bilateral UVJ jet frequencies (Jandaghi et al. - 10 minute video recorded period). Similarly only 3-5 minutes total were spend obtaining ipsilateral consecutive UVJ spectral waveforms (0- 5 per side). Further, in this study angle correction (30-60 degrees) for UVJ maximal velocity was not done which inevitably added error to our maximal UVJ jet velocity measurements. Angle correction would have added minimal time to date acquisition, and this was the UVJ characteristic Jandaghi et al. reported had the highest sensitivity and specificity of all, 100% and 97.8%.

Discussion and Conclusions
Taken together findings in this relatively abbreviated CDU of ureteral obstruction suggest the following conclusions:UVJ jet analysis in the context of incomplete ureteral obstruction is affected by stone position. Consistent with Jandaghi et al.’s findings UVJ jet velocities were lower on the obstructed side except when the stone is at the UVJ itself (analogous to crimping the end of a garden hose with your finger, increasing flow velocity but decreasing overall flow rate). Universally flow was decreased on the obstructed side (area under the spectral wave form). In certain patients UVJ frequency was actually increased on the obstructed side but with decreased flow rate. In these patients it took longer than five minutes to acquire UVJ jet spectral waveforms bilaterally to make a reasonable comparison (at least three waveforms on the non-obstructed side). Chronicity of obstruction increased the phasicity of the obstructed UVJ wave form.

Discussion and Conclusions
A limitation of UVJ jet analysis in two patients in this study was bladder volume of less than 110 cc, attributed to hydration status and confounding prostate hypertrophy in the second patient. This resulted in nonvisualization of UVJ jets. Jandaghi et al. reported a similar experience in 9 of 55 patients.19 Interestingly in 2011, Moesenbergen et al. found in their distal ureteral calculi follow-up research (158 patients with CT confirmed calculi, ultrasound FU with CT as the reference standard), almost all residual calculi were in the distal 3.5 cm ureter, and the 16% not visualized were in patients with a bladder volume of less than 110cc.20
Greyscale stone measurement in this study was within 1.4 mm of maximal stone dimension on CT, consistent with Kanno et al.’s US findings in 428 patients with ureteral calculi using CT as the reference standard.21

Discussion and Conclusions
This integrated sonographic urolithiasis protocol while not unique in its components successfully identified an obstructing urolith in all patients by utilizing its grey scale and Doppler components. When greyscale and color Doppler failed to suggest the presence of a ureteral stone, asymmetry in spectral UVJ jet waveforms correctly suggested the presence of one. Through adequate bladder filling (>110 cc) and optimized Doppler technique (incorporating a longer baseline of 15 s duration, velocity angle correction) it is anticipated inherent UVJ jet differences would be consistently more discernible and approximate the experience of cited authors. The inclusion of the renal RI is not only valuable in diagnosing obstruction but useful for urology as a baseline reference for potential ureteral stent placement.

Discussion and Conclusions
Beyond the decreased exposure to ionizing radiation that CT inevitably involves there are special situations an effective integrated ultrasound examination may be especially beneficially: evaluation of obstetric patients (fetal position permitting) given that thermal and cavitation indices are standard inclusion in US equipment; and transvaginal sonography of the distal ureter and UVJs avoids obesity and bladder volume issues, and would enable visualization of a retro-cecal appendix if appendicitis is in the differential. Lastly, it represents a potential public health cost-saving measure: standard CT technical charge - $3,380, standard US retroperitoneal complete charge - $735.

CT evidence of renal moderate hydronephrosis and right proximal ureter 8 x 9 mm calculus
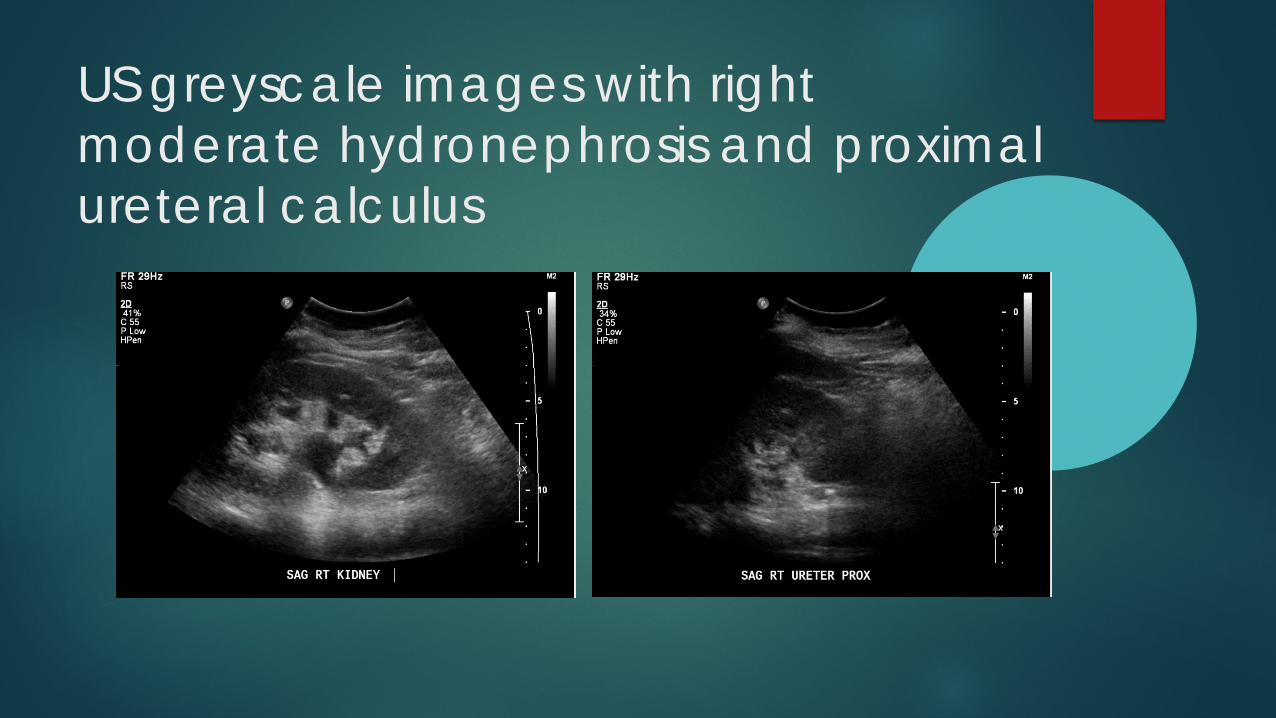
US greyscale images with right moderate hydronephrosis and proximal ureteral calculus

Elevation of the right renal RI on the obstructed side (> 10%, <7.0 normal)

Decreased UVJ velocity and duration on the obstructed right side (left unobstructed)

Right UVJ 9 x 5 mm stone with mild hydronephrosis
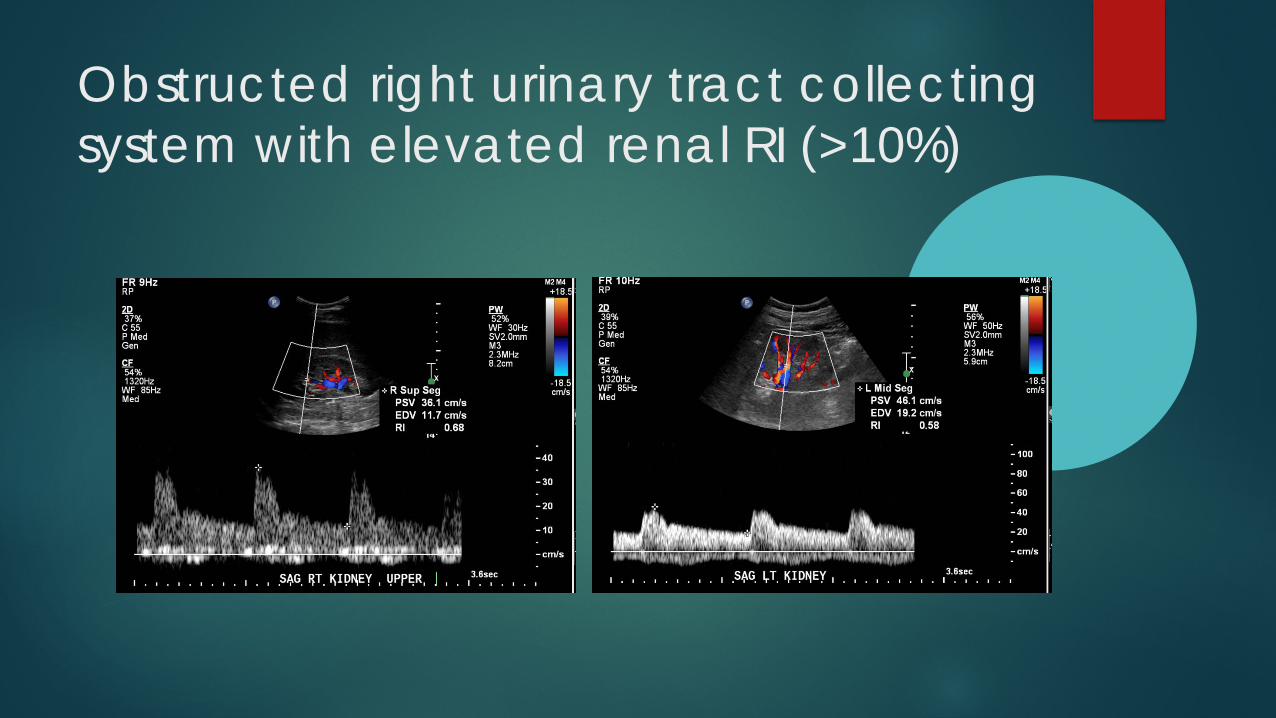
Obstructed right urinary tract collecting system with elevated renal RI (>10%)

RT UVJ 9 mm x 5 mm stone confirmed with color Doppler twinkle artifact

Obstructed right side with slightly higher velocity but decreased flow duration/flow rate (area under the spectral waveform)
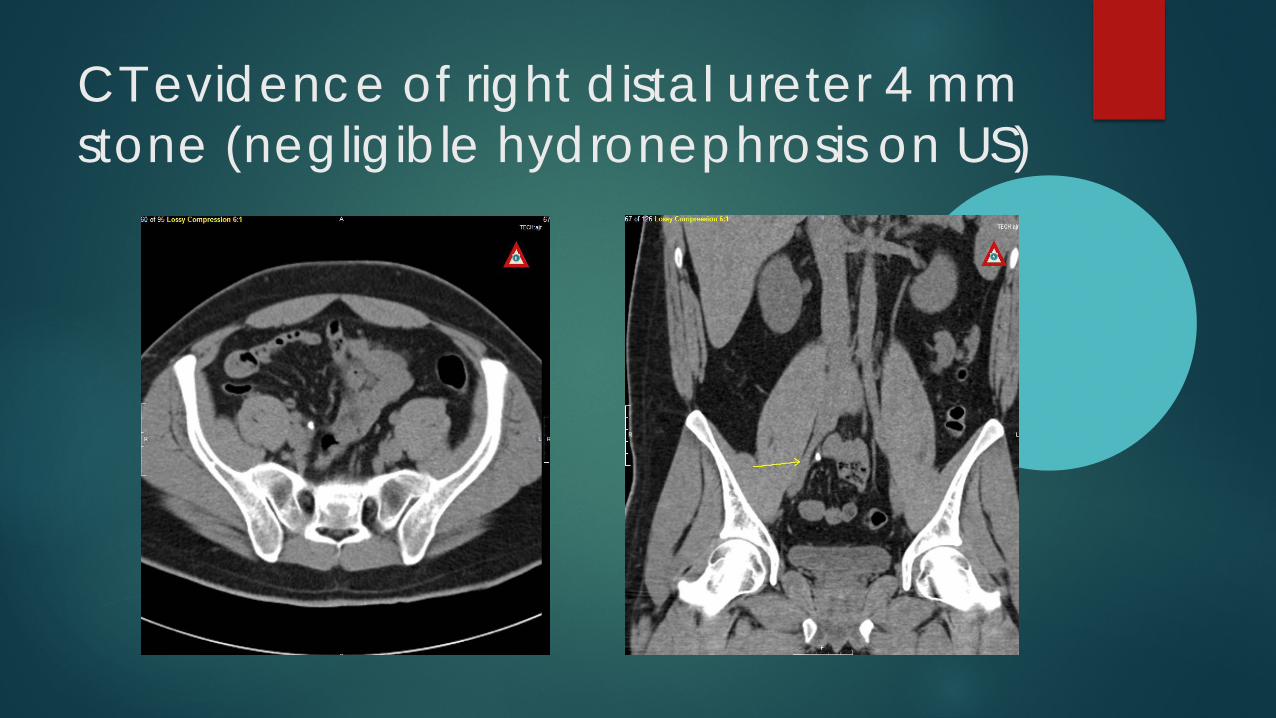
CT evidence of right distal ureter 4 mm stone (negligible hydronephrosis on US)

Similar renal RIs between the obstructed right collecting system (4mm stone) and unobstructed left

Decreased UVJ jet velocity and duration on the obstructed right side (unobstructed left)

Left distal ureter minimally obstructing 3 mm stone

Elevated UVJ velocity on side of obstruction, 3mm UVJ calculus

The exception to UVJ jet velocities (and flow?) when an obstructing stone (left) is at the UVJ itself

Left mid ureter 11 mm x 5 mm stone with moderate hydro. Prostatic enlargement and low bladder volume precludes UVJ visualization

References1. Bushberg JT (2012) The Essential Physics of Medical Imaging. Wolters Kluwer/Lippincott Williams & Wilkins, Philadelphia 957.
2. Platt JF. Duplex Doppler evaluation of native kidney dysfunction: obstructive and non-obstructive disease. Am J Roentgenology 1992;158:1035-42.
3. Rawashdeh YF, Djurhuus JC, Mortensen J, Horlyck A, Frokiaer J. The intrarenal resistive index as a pathophysiological marker of obstructive uropathy. J Urol 2001;165:1397-404.
4. Jandaghi AB, Falahatkar S, Alizadeh A, Kanafi A (2012) Assessment of ureterovesicular jet dynamics in obstructed ureter by urinary stone with color Doppler and duplex Doppler examinations. Urolithiasis (2013) 41:159-163.
5. Ibid. Ellenbogen PH, Scheible FW, Talner LB, Leopold GR. Sensitivity of gray scale ultrasound in detecting urinary tract obstruction. American Journal of Roentgenology 1978;130:731-3.
6. Scola FH, Cronan JJ, Schepps B. Grade 1 hydronephrosis: pulse Doppler evaluation. Radiology 1989;171:515-7.
8. Felsen D, Shulsinger D, Gross SS, Kim FY, Marion D, Vaughan ED. Renal hemodynamic and ureteral pressure changes response to ureteral obstruction: the role of nitric oxide. J Urology 2003;169:373-6.
9. Huang A, Palmer LS, Hom D. The role of nitric oxide in obstructive uropathy. J Urology 2000;163:1276-81.
10. Keogan MT, Kliewer MA, Hertzberg BS. Renal resistive indexes: variability in Doppler US measurement in a healthy population. Radiology 1996;199:165-9.
11. Bude RO, Di Pietro MA, Platt JF, Age dependency of the renal resistive index in healthy children. Radiology 1992;184:469-73.
12. Terry JD, Rysavy JA, Frick MP. Intrarenal Doppler: characteristics of aging kidneys. J Ultrasound Medicine 1992;11:647-51.

References13. Klahr S. Pathophysiology of obstructive uropathy: a 1991 update. Semin Nephrol 1991;11:156-
158.14. Mostbeck GH, Zontsich T, Turretschek K. Ultrasound of the kidney: obstruction and medical
diseases. Eur Radiol 2001;11:1878-89.15. Catalano O, De Sana G, Nunziata A. The color Doppler US evaluation of the jet in patients
with urinary colic. Radiol Med 1998;95:614-7.16. Pepe P, Motta L, Pennisi M, Aragona F. Functional evaluation of the urinary tract by color-
Doppler ultrasonography (CDU) in 100 patients with renal colic. European Journal of Radiology. 2005;53:131-135.
17. Moesbergen TC, de Ryke RJ, Dunbar S, Wells JE, Anderson NG Radiology (2011) 260:575-80.18. Kanno T, Masashi K, Hiromasa S, Ryuichi N, Takashi O, Yoshito, H, Hitoshi Y Urology (2014)
84:534-538.19. Jandaghi AB, Falahatkar S, Alizadeh A, Kanafi A (2012) Assessment of ureterovesicular jet
dynamics in obstructed ureter by urinary stone with color Doppler and duplex Doppler examination. Urolithiasis (2013) 41:159-163.
20. Ibid.21. Ibid.