an investigation of mental imagery in bipolar disorder
TRANSCRIPT

Bipolar Disorders 2016; 18: 669–683 wileyonlinelibrary.com/journal/bdi | 669
Received:26July2016 | Accepted:28October2016DOI:10.1111/bdi.12453
O R I G I N A L A R T I C L E
An investigation of mental imagery in bipolar disorder: Exploring “the mind’s eye”
Martina Di Simplicio1 | Fritz Renner1 | Simon E Blackwell1,6 | Heather Mitchell1 | Hannah J Stratford2 | Peter Watson1 | Nick Myers3,4 | Anna C Nobre3,4 | Alex Lau-Zhu1 | Emily A Holmes1,5
1MedicalResearchCouncilCognitionandBrainSciencesUnit,Cambridge,UK2HighfieldInpatientAdolescentUnit,WarnefordHospital,Oxford,UK3OxfordCentreforHumanBrainActivity(OHBA),UniversityofOxford,Oxford,UK4DepartmentofExperimentalPsychology,UniversityofOxford,Oxford,UK5DepartmentofClinicalNeuroscience,KarolinskaInstitute,Stockholm,Sweden6MentalHealthResearchandTreatmentCenter,Ruhr-UniversitätBochum,Bochum,Germany
CorrespondenceMartinaDiSimplicio,MRCCognitionandBrainSciencesUnit,Cambridge,UK.Email:[email protected]
Funding informationWellcomeTrustClinicalFellowship,Grant/AwardNumber:WT088217;MedicalResearchCouncil(UnitedKingdom),Grant/AwardNumber:MC-A060-5PR50;MedicalResearchCouncilCareerDevelopmentFellowship;NationalInstituteforHealthResearch(NIHR);EuropeanUnion;GermanAcademicExchangeService(DAAD);OxfordInstituteofClinicalPsychologyTraining;CambridgeCommonwealth,European&InternationalTrust
Objectives: Mentalimageryabnormalitiesoccuracrosspsychopathologiesandarehy-pothesizedtodriveemotionaldifficulties inbipolardisorder (BD).AcomprehensiveassessmentofmentalimageryinBDislacking.Weaimedtotestwhether(i)mentalimagery abnormalities (abnormalities in cognitive stages and subjective domains)occurinBDrelativetonon-clinicalcontrols;and(ii)todeterminethespecificityofanyabnormalitiesinBDrelativetodepressionandanxietydisorders.Methods: Participants included 54 subjects in the BD group (depressed/euthymic;n=27ineachsubgroup),subjectswithunipolardepression(n=26),subjectswithanxi-etydisorders(n=25),andnon-clinicalcontrols(n=27)matchedforage,gender,ethnic-ity,education,andpremorbidIQ.Experimentaltasksassessedcognitive(non-emotional)measuresofmentalimagery(cognitive stages).Questionnaires,experimentaltasks,anda phenomenological interview assessed subjective domains including spontaneousimageryuse,interpretationbias,andemotionalmentalimagery.Results: (i) Compared to non-clinical controls, the BD combined group reported agreaterimpactofintrusiveprospectiveimageryindailylife,morevividand“real”nega-tive images (prospective imagery task), and higher self-involvement (picture-wordtask).TheBDcombinedgroupshowednoclearabnormalitiesincognitivestagesofmental imagery.(ii)WhendepressedindividualswithBDwerecomparedtothede-pressedoranxiousclinicalcontrolgroups,nosignificantdifferencesremained—acrossallgroups,imagerydifferenceswereassociatedwithaffectivelabilityandanxiety.Conclusions: Comparedtonon-clinicalcontrols,BDischaracterizedbyabnormalitiesinaspectsofemotionalmentalimagerywithinthecontextofotherwisenormalcogni-tiveaspects.Whenmatchedfordepressionandanxiety,theseabnormalitiesarenotspecific to BD—rather, imagerymay reflect a transdiagnosticmarker of emotionalpsychopathology.
K E Y W O R D S
affectivelability,anxiety,bipolardisorder,cognitivefunctioning,depression,mentalimagery
ThisisanopenaccessarticleunderthetermsoftheCreativeCommonsAttributionLicense,whichpermitsuse,distributionandreproductioninanymedium,providedtheoriginalworkisproperlycited.© 2016 Medical Research Council. Bipolar Disorders publishedbyJohnWiley&SonsLtd.

670 | SIMPLICIO et aL.
1 | INTRODUCTION
Mental imagery comprises the experience of seeing in the “mind’seye,”nowregardedas“aweakformofperception”.1Nowonderthatnegativemental images generate strong emotions, indeed strongerthandoesthinkinginverballanguage.2
Bipolar disorder (BD) is characterized by periods of heightenedemotion (depression and mania),3 both during acute episodes andinter-episodically.4,5Wehavesuggestedthatmentalimagerymayactasan“emotionalamplifier”—fuelingmooddeterioration,moodeleva-tion,andanxietysymptomstypicalinBD.6InitialdatasuggestedthatpatientswithBDpresentwithheightenedemotionalmentalimagerycomparedtonon-clinicalcontrols,7 inparticularhigher trait imageryuse and heightened impact of intrusive mental imagery of futureevents (prospective imagery). Furthermore, those patientswith BDwithgreatestmoodinstabilityreportedagreaterimpactofprospectiveimagery.7Comparedtounipolarpatientswithequivalentlevelsofde-pressedmood,patientswithBDreportedmorecompellingandpreoc-cupyingprospectivesuicidalimages.8ThisisofinterestgiventhatBDhasthehighestsuiciderateofallpsychiatricdisorders.9PatientswithBDalso reportedmore frequent “flashforwards” to futureeventsattimesofpositivemoodthandidpeoplewithunipolardepression,andratedthese“flashforwards”asmorevivid,exciting,andpleasurable.10
However, amore comprehensive assessment ofmental imageryfunctioninBDis lacking.Pearsonetal.11arguedforcomplementingclinicalmeasurementsofimagerywithmoretraditionalcognitive(non-emotional)measures,andforassessmentusingbothobjectivecogni-tivestagemeasures(non-emotional)andsubjectivedomainmeasures(emotional).ThecognitivestagesarebasedonacomputationaltheoryproposedbyKosslyn etal.12 concerning fourmain stagesofmentalimagery: generation, maintenance, inspection and manipulation.Previous studieshave investigatedonly selected stagesof imagery-related processing, with evidence of deficits in cognitive tasks ofimagerygenerationandmanipulation indepressed individuals13 and imagerygeneration inanxious individuals.14Thesubjectivedomainsrelatetospontaneousimageryuse,15thepresenceofimagery-relatedinterpretationbiasesandemotionalmentalimagery16–18andthephe-nomenologicalcharacteristicsofmentalimageryindifferentaffectivestates.16
“Rediscovering” mental imagery in clinical practice can improveassessment.17There isalsoemergingevidenceof imageryasavalidtargettoreducemoodinstabilityinBD.18Therefore,acomprehensiveevaluationofcognitivestagesandsubjectivedomainsofmentalimag-eryinBDcouldfurtherinformourunderstandingofBDpsychopathol-ogyandtreatmentdevelopment,byidentifyingproblematicaspectsofmentalimageryinBDandrefiningtreatmenttargets.
The current study aimed to investigate: (i) whether individualswithBDhavementalimageryabnormalitiescomparedtonon-clinicalcontrolsand(ii)whethermentalimageryabnormalities(whenpresent)arespecifictoindividualswithBDcomparedtoclinicalcontrolswithdepressionandanxiety.Toaddressthesequestions,wecompared(i)patientswithBDandnon-clinicalcontrols;(ii-a)patientswithBDandpatientswithunipolardepressionwithequivalentlevelsofdepressive
symptoms;and(ii-b)patientswithBDandpatientswithanxietydis-orderswithequivalentlevelsofanxietysymptoms.Wealsoexploredwhetherclinicalvariablessuchasdepressiveandanxioussymptom-atology,bipolarphenotype traits,affective labilityandgeneral func-tioning levels predicted scores on mental imagery measures in thewhole sample combined.A range of testswere used encompassingbothcognitivestagesofmentalimageryandassessmentofsubjectiveandemotionaldomains.
2 | MATERIALS AND METHODS
2.1 | Participants
Participantscompletedpre-screeningquestionsviaemailorphonetoassesspotentialeligibility,basedonwhich175wereinvitedtoattendascreeningsession.Atthebeginningofthesession,allparticipantsprovidedwritten informedconsent (ethicalapproval reference:RECSouth Central 11/SC/0182) and the Structured Clinical InterviewforDSM-IV (SCID)Axis IDisorders19wasadministered toestablishdiagnosis.Thetestingbattery includedquestionnaires,experimentaltasksandaphenomenologicalinterview(averageduration4h).Ifpar-ticipantswereunabletocompletetestingoveronesession,asecondsessionwasscheduledwheremoodstatewasreassessed.
The screening session was used to determine whether partici-pantsmetthefollowingDSM-IVdiagnosticcriteria:BD group:DSM-IVdiagnosisofbipolar Idisorder,bipolar IIdisorder,orbipolardisordernototherwisespecified,notcurrent(hypo)manicepisode;unipolar de-pression group:DSM-IVdiagnosisofmajordepressiveepisode(MDE);anxiety disorder group:DSM-IVdiagnosisofanxietydisorderintheab-senceofapresentorpasthistoryofBDandofacurrentprimaryMDE;non-clinical control group:nopastorpresentAxisIdisorderbasedonDSM-IV diagnosis. Exclusion criteria for all participantswere activesuicidal risk, psychotic symptoms, current substance abuse, all as-sessedduringtheSCID,andsevereneurologicalimpairmentreportedduringthescreeningsession.Ofthe175participantswhoattendedthescreeningsession,24wereexcludedbasedonthesecriteria.
Allocationtooneoftheexperimentalgroupswasconfirmedbyaclinician(inthecaseofqueriesabouttheSCID),corroboratedbyscoresofcurrentaffectivestate(i.e.,scoreof≥8ontheHamiltonRatingScalefor Depression [HAM-D]20 to indicate current depression; score of<8ontheHAM-Dtoindicateeuthymia;nochangeinaffectivestatebetween testing sessions).Participantswith adiagnosisofBDwereallocatedtothe“BDdepressed”ortothe“BDeuthymic”grouponthebasisoftheSCID(i.e.,currentMDEornocurrentMDE)andHAM-Dscores.Afurther18participantswereexcludedfromanalysis,basedonaHAM-DscoreinconsistentwiththeSCIDinterview(n=6),achangeinmoodstateacrosstestingsessions(n=1),orafurthercheckbytheclinicianoftheSCID interview/additional information indicatingthattheindividualwasnoteligible(e.g.,currentsubstancedependence,notmeetingSCIDcriteriaforexperimentalgroup,orcurrent(hypo)mania;n=11).Twoparticipantsdidnotcompletethetestingsessions.
The final sample analyzed consisted of 131 participants, com-prising individualswithBD(depressed[n=27]andeuthymic [n=27]),

| 671SIMPLICIO et aL.
unipolardepression(n=26),oranxietydisorders(n=25),and26non-clinicalcontrols,aged18–65years.
2.2 | Assessments
2.2.1 | Clinical characteristics
ClinicalcharacteristicswereassessedusingtheSCIDforDSM-IVAxisIdisorders,includingmaindiagnosisandlifetimeandcurrentcomor-biddisorders,asabove.Currentmedicationwasrecorded.Depressive,(hypo)manic,andanxietysymptomswereassessedusingtheHAM-D,theYoungManiaRatingScale,21theAltmanSelf-RatingManiascale,22 theQuickInventoryofDepressiveSymptomology(QIDS),23andtheBeck Anxiety Inventory (BAI).24 TheMood Disorder Questionnaire(MDQ)25 was administered to assess hypomanic experience. TheAffectiveLabilityScale(ALS)26wasusedtomeasurechangeableaffectandtheFunctionalAssessmentStagingTest27toassessfunctionalim-pairmentinareasincludingoccupationalfunctioning,cognitivefunc-tioning,andinterpersonalrelationships.
2.2.2 | General cognitive function
TheNationalAdultReadingTest28wasusedasanassessmentofpre-morbidIQ.Verbalfluency(asameasureofgeneralexecutivefunction)andverbalworkingmemoryfunctionwereassessedusingtheVerbalFluency Testwith the letters F, A, S29 and Forward and BackwardDigitSpanTask,30respectively.
2.2.3 | Subjective domain of mental imagery
Spontaneous imagery useThespontaneoususeofmentalimageryineverydaylifewasassessedvia the SpontaneousUse of Imagery Scale (SUIS)15 and twoVisualAnalogueScales(VASs).7TheSUISisa12-itemself-reportscalemeas-uringtheuseofnon-emotionalmental imagery indaily life (e.g., If I am looking for new furniture in a store, I always visualize what the furni-ture would look like in particular places in my home.).Eachitemisratedonafive-pointscale,withtotalscoresrangingfrom12to60.Higherscoresindicatemoreuseofmentalimageryindailylife.TheSUIShasaninternalconsistencyofα=0.98andgoodconvergentvalidity.15TwoVASswereusedtoassesstheextenttowhichparticipantshadbeenthinkinginverbalthoughtsorinmentalimagesoverthepastweekona 1 (not at all)to9(all the time)scale.
Imagery interpretation biasThe Ambiguous Scenarios Test (AST-D)31 and the HomographInterpretationTask(HIT)32wereusedtomeasureimageryinterpreta-tionbias.TheAST-Dcomprises24ambiguousscenarios,whichpar-ticipantswereasked to imaginehappening to thempersonally (e.g.,1=You go to a wedding where you know very few other guests. After the party, you reflect on how the other guests behaved.),andthenrateeachimage’s pleasantness from 1 (extremely unpleasant) to 9 (extremely pleasant)andvividness from1 (not at all vivid) to7 (extremelyvivid).
The AST-D has good internal consistency (α=0.82).31 In the HIT,participants arepresentedwith aword and then asked to generateamental image. Thewordswere eight threatening/non-threateninghomographs,forexample,“mug”couldcueeitherabenign(e.g.,imag-iningoneselfdrinkingoutofamug)ornegative(e.g.,imaginingbeingattacked/mugged)mentalimage.Participantsprovidedashortwrittendescriptionofeachimageandthenratedtheirpleasantness(1–9scale)andvividness(1–7scale).Averagevividnessandpleasantnessscoreswerecomputedforbenign,negativeandambiguousmentalimages.
Emotional mental imageryEmotionalmental imagerywas assessed using a PictureWordCue(PW) task,33 the Impact of Future Events Scale (IFES),34 and theProspective Imagery Task (PIT).32,35 TheMental Imagery Interview(MII)(modifiedfromRef.8)wasconductedtogainqualitativedescrip-tionsofthephenomenologyofimagesandverbalthoughtattimesofdifferentacuteaffectivestates(low,elated,andanxiousaffect).
The PW task is a computer-based task examining self-reportedspontaneous use of imagery in response to emotional informationandemotionalcontext.Participantswerepresentedwith20ambig-uous/neutralpictureswithnegativewordcaptionsandinstructedto“combinethepicturewiththeword”(e.g.,pictureofstudentssittinganexamandcaptionword“fail”).Theythenratedfrom1(not at all)to9(extremely)howmuchtheyfoundthemselvesthinkinginmentalimages,orinverbalthoughts,andhowemotionaltheyfoundthepic-ture−wordcombination.Averagetendencytouseimagesandverbalthoughtsandaverageemotionalityofthepicture−wordcombinationswerecomputed.
On the IFES, participants were asked to identify three futureevents they had thought about/imagined over the past 7days andstate whether each was positive or negative. Participants then re-sponded to24 statements aboutprospective imagery in relation tothepastweek,onascalefrom0(not at all)to4(extremely).TheIFEShasacceptabletest−retestreliability(0.73)andagoodinternalconsis-tency(α=0.87).34
ThePITcomprises10positiveand10negativehypotheticalfuturescenarios.Participantswereaskedtogenerateanimageofeachandrateeachimageonafive-pointLikertscaleforvividness,likelihoodoftheeventhappeningtotheminthenearfuture,andhowmuchtheyfeelasthoughtheyareexperiencingtheeventwhilstimaginingit,withhigherratingsindicatingmorevividand“real”prospectiveimagery.Allsubscales of the PIT have demonstrated good internal consistency(0.83<α<0.90).36
The MII is a semi-structured interview, which assesses contentandcharacteristicsofmentalimagesandverbalthoughtsexperiencedwhentheparticipanthasbeenmostanxious,mostlowandmosthighinmood.Participantsarefirstaskedtodescribetheirmostsignificantmental image anchored to each affect state and rate characteristicsofthe imagesuchasvalence,generalemotionalityofthe imageandintensityofonespecificassociatedemotionpereachaffectstate(i.e.,threatening,demotivatingandexciting).Theyare thenasked to rateoverallcharacteristicsofmentalimageryandverbalthoughtsforeachaffectstate (anxious, low,andhigh)suchasfrequency, realness,and

672 | SIMPLICIO et aL.
compellingness.Allratingsusenine-pointLikertscales,withhigherrat-ingsindicatingmorefrequent,real(etc.)imageryorthoughts.
2.2.4 | Cognitive (non- emotional) stages of mental imagery
The following taskswere administered to assess the four cognitivestagesofmentalimagery.11
Imagery generationThe Image Generation Task (IGT)37measures theability togenerateamentalimagebasedonpreviouslyencounteredperceptualinformation.Participantswereasked tomemorize theshapeof fourblockcapitalletterspresentedina4×5grid:“U”and“H”,classifiedassimple(threeorfewersegments),and“S”and“J,”classifiedascomplex(fourormoresegments).Participantswerethenpresentedwithablankgridwithalowercase letter underneath, indicating which letter the participantshouldimagine.An“X”waspresentedinoneofthegridsquaresandparticipantswereaskedtorespond“True”ifthe“X”wouldcovertheimaginedblockletterifitwerepresentinthegridorotherwise“False.”Accuracy and reaction timewere recorded. Socially anxious partici-pantshavepreviouslyshownimagegenerationdeficitsonthistask.14
Imagery maintenanceTheabilitytomaintainmentalimagesinmindwasassessedusingtwovisual working memory tasks. The Short TermMemory (STM) task(adaptedfromRef.38)measuresvisualworkingmemorycapacityasthenumberofitemsthatcanbemaintainedinamentalrepresenta-tionaswellasthequalityofrepresentations.39Participantswerepre-sentedwitharraysconsistingoffourarrowsatdifferentorientations.Atestarrowwasthenpresentedatoneofthepreviousfourlocationsinarandomorientation,andparticipantswereinstructedtorespondbymovingthemouseupordowntorotatethetestarrowclockwiseoranticlockwiseuntil itmatchedtheirmemory for the rememberedarrowandthentoconfirmtheir response.Visual feedbackwaspro-vided immediately afterwards. The angular deviation between theparticipants’ selectedorientationand theoriginalorientationof thearrowprovidedameasureoftheerrorintheparticipants’memoryforthescene.Thedistributionofangularerrorsacrosstrialswasusedtocompute(usingawell-establishedmodelingtechnique39)twocomple-mentaryaccuracymeasures:recallrateandmemoryprecision.Recallratereflectstheproportionoftrialsonwhichparticipantshaveatleastsome information inmindabouttherememberedstimulus,whereasmemoryprecisionreflectshowclearthatinformationis.
TheVisual Patterns Test(VPT)40measuresvisualshort-termmem-oryandmemoryforpositionalsequences.Participantswerepresentedwithasequenceofincreasinglycomplexcheckerboardpatterns,start-ingwitha2×2matrix(withtwocellsfilledin)andprogressingtothelargest5×6matrix (with15filled incells).Eachpatternwasshownto the participant for 3 s and then hidden, at which point partici-pantswereaskedtoreproducethepatternbymarkingsquaresinanemptygridof the same size.Accuracy scoreswerecalculatedusing
themaximumdifficultylevelreachedforwhichtwopatternswerecor-rectlyreproduced.
Imagery inspectionTheLetterCornerClassification(LCC)task41measures image inspec-tionability,involvinginterpretationofanobject-basedspatialcharac-teristicoftheimage.Participantswerefirstpresentedwithfourblockcapitalletters(F,N,Z,andG),markedwithanasteriskinthebottomleftcornerandanarrowtravellingclockwisearoundtheletter.Participantswere instructedtomemorizetheshapeofeach letterandreproduceitonablankpieceofpaper,startingatthepointmarkedbytheaster-iskandfollowingthedirectionofthearrow.Participantsthencatego-rizedthecorneroftheletters.Foreachletter,first,for“topandbottompoints”,participantswereaskedtogoaroundtheshape,startingatthepointmarkedbytheasterisk,indicating“yes”ifthecornerwasattheextremetoporbottomoftheshapeorotherwise“no”.Theletterswerethen removedandparticipants instructed to imagineeach letterandcategorizethecorners.Theletterswerethenpresentedagainandthesameprocedurefollowedfor“outsidepoints”,whichrequireda“yes”re-sponseforcornersontheextremeleftandrightofthefigure.Accuracyandtimetakenforeachletterinbothconditionswererecorded.
Imagery manipulationTwotasksmeasuringtheabilitytomanipulatementalimagesweread-ministered.AcomputerizedversionoftheclassicMentalRotationTask(MRT)42 measured participants’ ability to transform mental images.Participantswereshownpairsofthree-dimensionallinedrawingsandinstructedtodecidewhetherthetwodrawingswerethesameordif-ferentbyusingamentalrotationstrategy.Followingapracticetrial,thetaskincludedtrialswiththreedifficultylevelsbasedonwhethertheangulardisparitybetweenthe twoshapeswas50,100,or150.Accuracyandreactiontimewererecorded.Twomeasureswerecom-puted based on:13,43 the intercept index, representing the sensory/motor componentof the response in the task, and the slope index,representingthespatialabilitycomponentofthetask(i.e.,therotationspeedrelativetotheangularrotationdifficulty).AversionoftheMRTusing lettersofthealphabet44hasshownmentalrotationdeficits inpatientswithunipolardepression.
The Creative Mental Synthesis (CMS) task45 assesses partici-pants’abilitytomentallyconstructarecognizablefigurefromthreealpha-numeric or geometric shapes (e.g., rectangle, capital L, andhorizontalline).Participantswereshowntwosetsofexamplemen-talconstructionsandthencompletedtwotrials.Oneachtrialthreeparts were named, after which participants were given 2 min toclosetheireyesandmentallycombinethestimuli intoa recogniz-ablefigure.Theywerethenaskedtodrawandlabeltheirfinalfig-ure.Threejudgesindependentlyratedeachfigureonthefollowingparameters: recognizability (ofzero,one,or twoof the twotrials),correspondence(betweenthenameofthepatternandthedrawingona1–5scale),creativity(yes/no,forpatternsratedat least4forcorrespondence),wrong patterns (yes/no) and absence of pattern(yes/no).

| 673SIMPLICIO et aL.
2.2.5 | Statistical analysis
First,wetested(i)ifparticipantswithBDhadimageryabnormalitiesbycomparingtheBDgroup(euthymicanddepressedcombined)tonon-clinical control participants onmeasures of cognitive and subjectivedomainsofmentalimagery.Totestforbetween-groupdifferencesontheseaspectsofimageryabnormalities,55statisticaltestswereper-formed. ABD group combining euthymic and depressed individualswasusedtotestreplicationofpreviousdata.7Moreover,aseuthymicindividualswithBDpresentwithdepressionlevelsgreaterthanthoseofnon-clinicalcontrols(albeitsubclinical),wechosetofirstassessthepresenceofimageryabnormalitiesregardlessofaffectstate.Next,wesoughttodeterminethespecificityofanygroupdifferencesbycom-paringthescoresof(ii-a)currentlydepressedparticipantswithBDtothoseofcurrentlydepressedparticipantswithunipolardepression(thisalsoallowscontrolling for the impactofdepressedmoodonmentalimageryabnormalities),and(ii-b)currentlydepressedparticipantswithBDwith concurrent anxiety symptoms to thoseofparticipantswithanxietydisorders(thisalsoallowscontrollingfortheimpactofanxietyonmentalimageryabnormalities;thetwogroupswerealsomatchedonlevelsofdepression).Tolimitthenumberoftests,comparisonsofBDdepressedtoclinicalcontrolgroupswerelimitedto(i)thosevaria-blesthatshowedsignificantgroupdifferencesintheinitialcomparison(BDgroupcombinedversusnon-clinicalcontrols)and(ii) thosecom-parisonsthathadyieldedsignificantdifferencesinpreviousstudies.7,8 Totest fordifferencesbetweendepressedparticipantswithBDandunipolardepressedparticipantsandtotestfordifferencesbetweende-pressedparticipantswithBDwithconcurrentanxietysymptomsandparticipantswithanxietydisorders,38statisticaltestswereperformed.
Pairwisedifferencesbetweenvariablesinthedifferentgroupsasoutlined inour aimswere analyzedusingunpaired t tests if the re-sidualsobtainedusingthesettestsachievednormalitywithP-valuesabove .05 using both the Kolmogorov–Smirnov and Shapiro–Wilktests.WherethegroupvarianceswerefoundtodifferusingLevene’stest,Satterthwaite’scorrectionwasappliedtothedegreesoffreedomofthettest.Wheretheresidualsofapairwisecomparisononanun-transformedresponsedidnotachievenormality,log,squarerootandreciprocaltransformationswereappliedandnormalityoftheresidualsreassessed.Wheretransformationsfailedtoachievenormalresiduals,Mann–WhitneyU testswereusedtoanalyzegroupdifferences.FortheCMS task,Fisher’sexact testwasused to identifygroupdiffer-encesinthenumberofCMStrialsthatwerejudgedasrecognizable,creative,havinggoodcorrespondence,havinga correctpatternandhavingapresentpattern.
To explore the specificity of differences in mental imagery be-tween diagnostic groups further, we computed correlations be-tween the mental imagery variables that showed significant groupdifferences in the initial comparison (BD group combined versusnon-clinicalcontrols)andclinicalvariablesfordepression(QIDSandHAM-D),anxiety (BAI),hypomanicexperiences (MDQ),mood insta-bility (ALS), and overall functioning (FAST). Pearson’s correlationswereused,orKendall’stau,whereinspectionofscatterplotsdidnotsuggestalinearrelationship(96correlationscomputed).Theunique
contribution of these clinical variables in predicting scores on thementalimagerymeasuresacrossgroupswasexploredbyconductingaseriesofmultipleregressionanalyseswitheachofthementalimagerymeasuresasthedependentvariable(16regressionmodels)andwithall clinical variables entered as predictor variables simultaneously.Non-significantpredictorswerethenremovedfromthemodelstep-wiseuntilonlysignificantpredictorsremained.Maniameasureswerenotincludedinthisanalysisasallparticipantspresentedwithlevelsof manic symptoms below clinical significance (see the Limitations section).
Inallanalyses,P-values<.05wereconsideredstatisticallysignifi-cantandnocorrectionsformultipletestingwereapplied.Normalitychecksofmodelresidualsallowedanyundueinfluenceofoutlierstobereducedwithoutlosinginformationbyremovingthem.
3 | RESULTS
3.1 | Participants
DemographicandclinicalcharacteristicsofallgroupsarepresentedinTable1.Therewerenobetween-groupsdifferencesinage,gender,ethnicity,levelofeducation,orpremorbidIQ.
3.2 | Assessments
3.2.1 | General cognitive function
Participants with BD (combined group) had a lower total scoreon the verbal fluency task (mean [M]=41.30, standard devia-tion [SD]=10.56) compared to non-clinical controls (M=48.85,SD=15.29);t(78)=2.58,P=.012,d=0.62.Thetwogroupsdidnotdif-fer in theirperformanceonthedigitspantask:digitspanforwardP=.94; digit span backwards P=.72. There were no differences inanyofthegeneralcognitivefunctioningmeasuresbetweentheBDdepressedgroupandtheunipolardepressiongroup(verbalfluencytaskP=.66;digitspanforwardP=.39;digitspanbackwardP=.36)orbetweentheBDdepressedgroupandtheanxietydisordersgroup(verbalfluencytaskP=.07;digitspanforwardP=.83;digitspanback-ward P=.95).
3.3 | Do individuals with BD show mental imagery abnormalities compared to non- clinical controls?
Scores on assessments of cognitive (non-emotional) stages andsubjective domains ofmental imagery of participantswith BD andnon-clinicalcontrols,andresultsofbetween-groupcomparisonsaresummarized in Tables2–4 (all data referring to the BD combinedgroup).
3.3.1 | Subjective domain of mental imagery
All results related to the subjective domain of mental imagery aredetailed in Table3. ParticipantswithBDdid not significantly differ

674 | SIMPLICIO et aL.
fromnon-clinicalcontrolsintheirspontaneoususeofimageryontheSUIS,anddidnotdifferfromnon-clinicalcontrols intheirratedfre-quencyofthoughtsinaverbalorvisualmodalityoverthepastweek.
ParticipantswithBDdidnotsignificantlydiffer fromnon-clinicalcontrols intheir imageryinterpretationbiasasassessedbypleasant-nessorvividnessratingsontheAST-D.Non-clinicalcontrolparticipants
T A B L E 1 Demographicandclinicalcharacteristicsofparticipants
BD (euthymic) (n=27)
BD (depressed) (n=27)
Unipolar depression (n=26)
Anxiety disorder (n=25)
Non- clinical controls (n=26)
Demographic characteristics
Age,years,mean(SD) 40.41(12.78) 40.44(12.56) 44.31(14.82) 37.60(15.43) 41.50(13.00)
Educationallevel,years,mean(SD) 17.11(2.64) 17.07(4.07) 17.27(3.97) 16.52(3.00) 17.46(2.28)
Gender,female,n(%) 17(63.0) 17(63.0) 18(69.2) 19(76.0) 16(61.5)
EstimatedpremorbidIQ,mean(SD) 114.85(7.96) 113.04(9.19) 112.20(11.50) 111.42(9.44) 112.88(10.75)
Ethnicity
White 26 25 17 21 24
Mixed 0 1 3 2 1
AsianorBritishAsian 0 0 3 1 1
Chinese 1 1 3 0 0
Clinical characteristics
BipolarIdisorder,n(%) 17(63.0) 14(51.9) 0 0 0
BipolarIIdisorder,n(%) 10(37.0) 11(40.7) 0 0 0
BP-NOS,n(%) 0(0.0) 2(7.4) 0 0 0
No.ofdepressiveepisodes,mean(SD) 19.05(23.67) 22.76(30.81) 4.81(9.34) 14.15(29.97) 0
Currentdepression,n(%) 0 27(100.0) 26(100.0) 8(32.0) 0
Currentanxietydisorder,n(%)a 6(22.2) 16(59.3) 11(42.3) 25(100.0) 0
Medications, n
Antidepressants 8 8 7 9 0
Anxiolytics 2 3 0 2 0
Moodstabilizers 19 13 0 0 0
Antipsychotics 14 10 1 0 0
HistoryofAxisIdisorders
Previousdepression,n 27 25 22 17 0
Previousanxiety,n 9 11 7 11 0
Previousother,n 13 12 5 1 0
Ageatillnessonset,years,mean(SD) 21.30(10.01) 16.81(8.38) 26.75(13.10) 19.48(13.18) n/a
Illnessduration,years,mean(SD) 18.67(11.93) 23.77(15.44) 15.88(16.17) 17.38(15.46) n/a
Current clinical symptoms, mean (SD)
QIDSscore 4.37(2.82) 13.22(3.93) 15.50(4.47) 11.32(5.71) 2.04(2.01)
HAM-Dscore 3.19(2.18) 14.93(4.59) 15.23(4.99) 11.40(7.05) 1.31(1.49)
BAIscore 3.62(3.74) 14.41(9.01) 16.38(10.33) 17.96(9.06) 2.00(2.87)
ASRMscore 2.96(2.79) 1.59(2.58) 1.28(1.81) 1.88(1.83) 0.88(1.11)
YMRSscore 2.65(2.38) 2.81(3.71) 1.88(1.93) 2.56(1.89) 0.42(0.86)
FASTscore 7.67(6.74) 26.44(11.92) 31.12(14.53) 23.56(16.29) 4.69(9.44)
ALSscore 62.48(33.56) 82.58(24.54) 67.69(26.40) 70.80(32.59) 22.23(19.62)
MDQscore 14.41(2.00) 13.07(2.89) 7.88(4.93) 6.04(4.11) 2.46(2.89)
ALS,AffectiveLabilityScale;ASRM,AltmanSelf-RatingManiascale;BAI,BeckAnxiety Inventory;BD,bipolardisorder;BD-NOS,bipolardisordernototherwise specified; FAST, FunctionalAssessment StagingTest;QIDS,Quick Inventory ofDepressive Symptomology;HAM-D,HamiltonDepressionRatingScaleforDepression;MDQ,MoodDisorderQuestionnaire;SD,standarddeviation;YMRS,YoungManiaRatingScale.aCurrentanxietydisordertypeswere:socialanxiety(n=12),obsessivecompulsivedisorder(n=9),posttraumaticstressdisorder(n=11),generalizedanxietydisorder(n=20),specificphobia(n=10),panicdisorder(n=12),andagoraphobia(n=2).Pleasenotethatsomeparticipantspresentedwithmultipleanxietydisorders.

| 675SIMPLICIO et aL.
reportedahighernumberofbenignhomographswhichwasmarginallysignificantcomparedtothosewithBD.Thetwogroupsdidnotsignifi-cantlydifferinotherinterpretationbiasratingsfromtheHIT.
Onmeasuresofemotionalmental imagery,participantswithBDscored higher on the PW self-involvement scale compared to non-clinical controlparticipants.The twogroupsdidnotdiffer in anyoftheotherPWtaskscales.ParticipantswithBDreportedastrongerim-pactofemotionalprospectiveimageryontheIFEScomparedtonon-clinical controls. They also reported higher ratings of vividness andsenseofexperiencingfornegativefutureimages,andlowerratingsoflikelihoodforpositivefuturescenariosonthePIT.ThetwogroupsdidnotsignificantlydifferontheremainingPITscales.
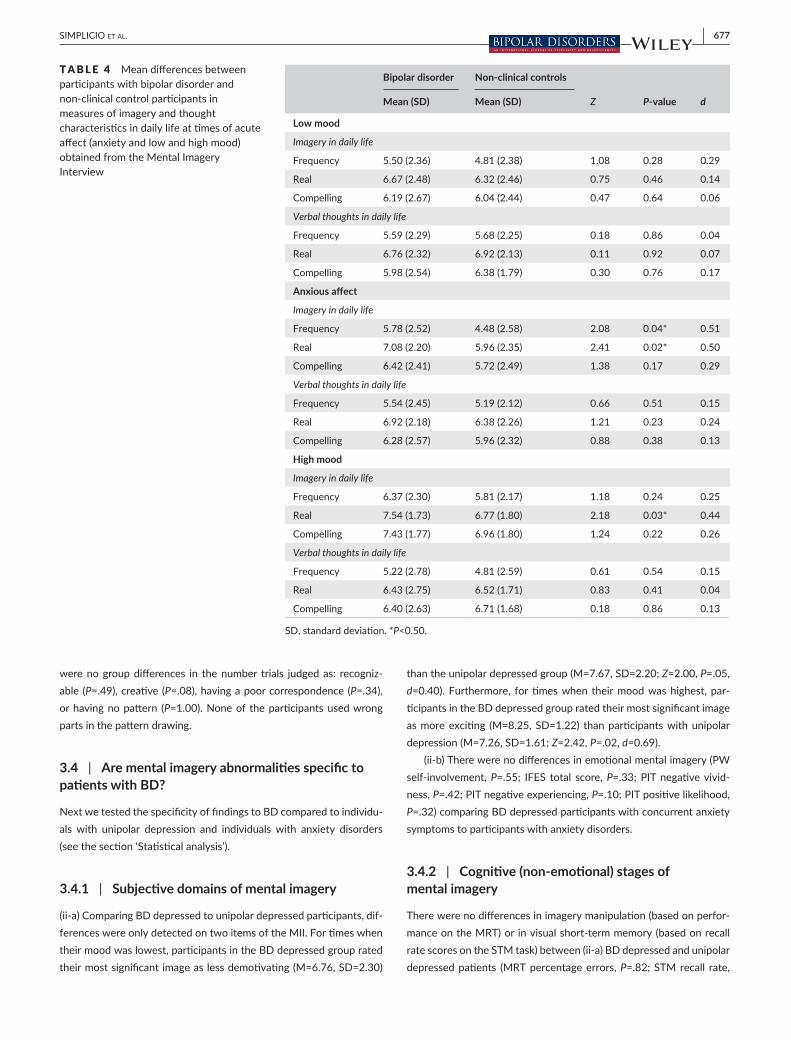
All resultsontheMIIaredetailed inTable3.For thetimewhentheirmoodwasmost low,participantswithBDratedtheirmostsig-nificantmentalimageasmorenegativeandmoredemotivatingcom-paredtonon-clinicalcontrols.Forthetimewhentheirmoodwasmostanxious,participantswithBDratedtheirmostsignificantmentalimageasmorenegative,threateningandemotionalcomparedtonon-clinicalcontrols.Theyalsoratedoverallthinkinginmentalimagestobemore
frequent andmore “real” compared tonon-clinical controls. For thetimewhentheirmoodwasmosthigh,participantswithBDratedtheirmostsignificantimageasmoreexcitingcomparedtonon-clinicalcon-trols.Theyalsoratedoverallmentalimageryasmore“real”comparedtonon-clinicalcontrols.FullresultsarereportedinTable4.QualitativeexamplesofsignificantmentalimagesarereportedinTable5.
3.3.2 | Cognitive (non- emotional) stages of mental imagery
Allresultsrelatedtothecognitive(non-emotional)stagesofmentalim-ageryaredetailedinTable2.ParticipantswithBDdidnotsignificantlydifferintheirperformanceonanypartoftheimagerygenerationtask,indicatingno imageryabnormalities in theBDgroup in termsof im-agerygenerationinanon-emotionalcognitivetask.
Of the two imagerymaintenance tasks,participantswithBDhadahigher recall rateonthevisualSTMtaskcomparedtothose in thenon-clinicalcontrolgroup, indicatingthatparticipantswithBDinthisstudyhadagreater likelihoodof rememberingvisual targetcues ina
T A B L E 2 Meandifferencesbetweenparticipantswithbipolardisorderandnon-clinicalcontrolparticipantsinmeasuresrelatingtothecognitive(non-emotional)stagesofmentalimagery
Bipolar disorder Non- clinical controls
Mean (SD) (n=54) Mean (SD) (n=24) t Z df P- value d
Imagery generation
Imagery Generation Task (IGT)
IGTRTSimpleLetter 2026.48(842.65) 1744.22(662.54) — 1.04 — 0.30 0.36
IGTRTComplexLetter 2175.07(914.24) 1843.46(568.48) 1.64 — 76 0.11 0.40
IGTRTEarly 1964.54(761.72) 1767.53(575.63) 1.13 — 76 0.26 0.28
IGTRTLate 2250.91(1001.15) 1896.33(602.24) 1.61 — 76 0.11 0.39
IGTPercentageErrors 4.40(11.04) 3.39(5.21) — 0.22 — 0.83 0.10
Imagery maintenance
Short- term Memory Task (STM)
STMMemoryPrecision 3.12(3.93) 2.65(0.83) — 0.41 — 0.68 0.14
STM Recall Rate 0.65(0.21) 0.53(0.19) 2.15 — 67 0.04* 0.58
Visual Pattern Task (VPT)
VPTAccuracy 9.25(1.67) 9.43(1.76) 0.45 — 75 0.66 0.11
Imagery Inspection
Letter Corner Classification Task (LCC)
LCCAccuracy 5.30(1.88) 5.11(1.91) — 0.50 — 0.62 0.10
LCCTime 14.50(6.64) 13.02(5.13) — 0.99 — 0.32 0.25
Imagery manipulation
Mental Rotation Task (MRT)
MRTRTEasy 3080.64(722.74) 3015.35(588.61) 0.39 — 73 0.70 0.10
MRTRTMedium 3389.18(697.81) 3265.71(588.76) 0.76 — 73 0.45 0.18
MRTRTDifficult 3510.54(642.93) 3261.41(602.33) 1.62 — 73 0.11 0.40
MRTslope 214.81(175.40) 133.04(166.17) 1.94 — 73 0.06 0.47
MRTintercept 2880.19(810.89) 2933.09(652.66) 0.28 — 73 0.78 0.07
MRT Percentage Errors 28.22(14.54) 20.62(10.85) 2.31 — 73 0.02* 0.57
RT,reactiontime;SD,standarddeviation.*P<0.05.

676 | SIMPLICIO et aL.
non-emotionalvisualshort-termmemorytask.Thegroupsdidnotdiffersignificantlyinmemoryprecision.Instead,ontheVPTtaskparticipantswithBDdidnotsignificantlydifferinaccuracyscoresfromnon-clinicalcontrols, suggesting that participants with BD in this study had noabnormalitiesinvisualshort-termmemoryasassessedwiththeVPT.
ParticipantswithBDdidnotsignificantlydifferfromnon-clinicalcon-trolsintheiraccuracyorcompletiontimeontheLCC,indicatingthatpar-ticipantswithBDinthisstudyhadnodysfunctionsinimageryinspection.
Onimagerymanipulationtasks,participantswithBDdidnotsignifi-cantlydifferfromnon-clinicalcontrolsonanyindicesofmentalrotationspeed,butonaveragehadahighererrorpercentagecomparedtothoseinthenon-clinicalcontrolgroup.As,comparedtonon-clinicalcontrols,
theBDgroupperformedworseontheverbalfluencytest,ataskofex-ecutivefunctionconsideredtobeanindirectmeasureofgeneralcog-nitivefunctioning,wetestedifthiscouldaccountforthehighererrorpercentageontheMRT.TheverbalfluencytesttotalscorewasenteredasacovariateinanANCOVAtestinggroupdifferencesbetweenpar-ticipantswithBDandnon-clinicalcontrolsintheerrorpercentageoftheMRT.Afteraddingverbalfluencyasacovariate,themaineffectofgroupbecamemarginallynon-significant[F(1,75)=3.70,P=.058],indi-catingthatthehighererrorrateofpatientswithBDontheMRTmightbeinpartexplainedbydeficitsingeneralcognitivefunctioning.
Participantswith BD did not differ fromnon-clinical controls intheirperformanceontheCMS.OverthetwotrialsoftheCMS,there
T A B L E 3 Meandifferencesbetweenparticipantswithbipolardisorderandnon-clinicalcontrolparticipantsonmeasuresrelatingtosubjectivedomainsofmentalimagery
Bipolar disorder Non- clinical controls
Mean (SD) Mean (SD) t Z df P- value d
Spontaneous imagery use
Spontaneous Use of Imagery Scale (SUIS)
SUISmeanscore 3.36(0.81) 3.04(0.65) 1.75 — 78 0.08 0.42
VisualAnalogueScales(VASs)
VASVerbal 5.38(2.21) 5.73(1.80) — 0.62 — 0.53 0.17
VASMentalImagery 5.38(2.11) 5.31(1.49) — 0.39 — 0.70 0.04
Imagery interpretation bias
Ambiguous Scenarios Test (AST-D)
AST-DPleasantness 4.83(1.11) 5.17(1.23) 1.23 — 78 0.22 0.30
AST-DVividness 4.45(1.38) 4.60(1.37) 0.48 — 78 0.63 0.11
Homograph Interpretation Task (HIT)
HITno.ofPositiveHomographs 4.91(1.69) 5.62(1.55) — 1.91 — 0.06 0.43
HITno.ofNegativeHomographs 2.89(1.69) 2.27(1.51) — 1.60 — 0.11 0.38
HITPositiveVividness 5.09(1.30) 5.19(1.16) — 0.26 — 0.79 0.08
HITNegativeVividness 4.50(1.94) 4.32(2.04) — 0.44 — 0.66 0.09
Emotional mental imagery
Picture Word Task (PW)
MentalImagery 6.21(1.68) 5.92(1.81) 0.70 — 77 0.49 0.17
Verbal 3.80(1.97) 4.29(2.34) 0.96 — 77 0.34 0.23
Memory 4.20(1.45) 3.53(1.47) 1.91 — 77 0.06 0.46
Emotion 4.77(1.82) 4.53(1.74) 0.55 — 77 0.59 0.13
Self-involvement 4.44(1.69) 3.58(1.75) 2.10 — 77 0.04* 0.50
Impact of Future Events Scale (IFES)
IFESTotalScore 29.87(15.82) 17.42(9.31) 4.36 — 73.83 <0.001* 0.89
Prospective Imagery Task (PIT)
PITNegativeVividness 3.07(0.92) 2.53(0.86) 2.55 — 78 0.013 0.60
PITNegativeLikelihood 2.58(0.67) 2.32(0.66) 1.66 — 78 0.10 0.39
PITNegativeExperiencing 2.66(0.91) 2.18(0.90) 2.18 — 78 0.03* 0.53
PITPositiveVividness 3.08(0.91) 3.33(0.72) 1.33 — 61.49 0.19 0.29
PITPositiveLikelihood 2.89(0.91) 3.43(0.69) 2.93 — 63.29 0.005* 0.64
PITPositiveExperiencing 2.59(0.97) 2.87(0.85) 1.23 — 78 0.22 0.30
SD,standarddeviation.*P<0.50.
| 677SIMPLICIO et aL.
werenogroupdifferences in thenumber trials judgedas: recogniz-able (P=.49),creative(P=.08),havingapoorcorrespondence(P=.34),orhavingnopattern (P=1.00).Noneof theparticipantsusedwrongpartsinthepatterndrawing.
3.4 | Are mental imagery abnormalities specific to patients with BD?
NextwetestedthespecificityoffindingstoBDcomparedtoindividu-als with unipolar depression and individuals with anxiety disorders(seethesection‘Statisticalanalysis’).
3.4.1 | Subjective domains of mental imagery
(ii-a)ComparingBDdepressedtounipolardepressedparticipants,dif-ferenceswereonlydetectedontwoitemsoftheMII.Fortimeswhentheirmoodwaslowest,participantsintheBDdepressedgroupratedtheirmostsignificantimageaslessdemotivating(M=6.76,SD=2.30)
thantheunipolardepressedgroup(M=7.67,SD=2.20;Z=2.00,P=.05,d=0.40).Furthermore, fortimeswhen theirmoodwashighest,par-ticipantsintheBDdepressedgroupratedtheirmostsignificantimageasmoreexciting (M=8.25,SD=1.22) thanparticipantswithunipolardepression(M=7.26,SD=1.61;Z=2.42,P=.02,d=0.69).
(ii-b)Therewerenodifferencesinemotionalmentalimagery(PWself-involvement,P=.55; IFES total score,P=.33;PITnegativevivid-ness,P=.42;PITnegativeexperiencing,P=.10;PITpositivelikelihood,P=.32)comparingBDdepressedparticipantswithconcurrentanxietysymptomstoparticipantswithanxietydisorders.
3.4.2 | Cognitive (non- emotional) stages of mental imagery
Therewerenodifferencesinimagerymanipulation(basedonperfor-manceontheMRT)orinvisualshort-termmemory(basedonrecallratescoresontheSTMtask)between(ii-a)BDdepressedandunipolardepressedpatients (MRTpercentageerrors,P=.82;STMrecall rate,
Bipolar disorder Non- clinical controls
Mean (SD) Mean (SD) Z P- value d
Low mood
Imagery in daily life
Frequency 5.50(2.36) 4.81(2.38) 1.08 0.28 0.29
Real 6.67(2.48) 6.32(2.46) 0.75 0.46 0.14
Compelling 6.19(2.67) 6.04(2.44) 0.47 0.64 0.06
Verbal thoughts in daily life
Frequency 5.59(2.29) 5.68(2.25) 0.18 0.86 0.04
Real 6.76(2.32) 6.92(2.13) 0.11 0.92 0.07
Compelling 5.98(2.54) 6.38(1.79) 0.30 0.76 0.17
Anxious affect
Imagery in daily life
Frequency 5.78(2.52) 4.48(2.58) 2.08 0.04* 0.51
Real 7.08(2.20) 5.96(2.35) 2.41 0.02* 0.50
Compelling 6.42(2.41) 5.72(2.49) 1.38 0.17 0.29
Verbal thoughts in daily life
Frequency 5.54(2.45) 5.19(2.12) 0.66 0.51 0.15
Real 6.92(2.18) 6.38(2.26) 1.21 0.23 0.24
Compelling 6.28(2.57) 5.96(2.32) 0.88 0.38 0.13
High mood
Imagery in daily life
Frequency 6.37(2.30) 5.81(2.17) 1.18 0.24 0.25
Real 7.54(1.73) 6.77(1.80) 2.18 0.03* 0.44
Compelling 7.43(1.77) 6.96(1.80) 1.24 0.22 0.26
Verbal thoughts in daily life
Frequency 5.22(2.78) 4.81(2.59) 0.61 0.54 0.15
Real 6.43(2.75) 6.52(1.71) 0.83 0.41 0.04
Compelling 6.40(2.63) 6.71(1.68) 0.18 0.86 0.13
SD,standarddeviation.*P<0.50.
T A B L E 4 Meandifferencesbetweenparticipantswithbipolardisorderandnon-clinicalcontrolparticipantsinmeasuresofimageryandthoughtcharacteristicsindailylifeattimesofacuteaffect(anxietyandlowandhighmood)obtainedfromtheMentalImageryInterview

678 | SIMPLICIO et aL.
P=.25)orbetween(ii-b)BDdepressedpatientswithconcurrentanxi-etysymptomsandanxiouspatients (MRTpercentageerrors,P=.70;STMrecallrate,P=0.72).
3.5 | Relation between mental imagery measures and depression, anxiety, BD phenotype, affective lability and general functioning
GiventhelackofspecificityofmentalimageryabnormalitiespresentinparticipantswithBD,wenextexploredwhethertheseimageryab-normalitiesarerelatedtocurrentaffectstates(QIDS,HAM-DandBAI)
and traits (MDQandALS) rather thandiagnosticcategories, and tolevelsofgeneralfunctioning(FAST).CorrelationsbetweentheclinicalvariablesandmeasuresofmentalimageryareshowninSupplementary Table S1.Totesttheuniquecontributionoftheassociationsbetweenmental imageryvariablesand theclinical variables,weconductedanumberofmultiple regression analyses (see ‘Statistical analysis’), inwhich each imagery variablewaspredictedby the clinical variables(Supplementary Table S2).Onlythose imageryvariablesthatshowedsignificantgroupdifferencesinthecomparisonbetweenparticipantswith BD and non-clinical control participants (reported in Table2)wereincludedintheseanalyses.
T A B L E 5 Exampleofsignificantimagesforeachaffectstate(anxietyandlowandhighmood)forparticipantswithbipolardisorderandnon-clinicalcontrolstakenfromtheMentalImageryInterviewandmeanemotionalratingsofthesignificantimages
Bipolar disorder Non- clinical controls
Lowmood Asuicideplan—extensiveandintelligent.IwouldgotothecollegebarandtakeoneoftheCO2bottlesusedtopumpGuinnessandtakeitbacktomyroom.IwouldsendanemailtotellpeoplenottocomeinandreleasetheCO2(pp157)
Seeingtheemailrejectingyoufromthejob(pp131)
Thinkingaboutmoldgrowinginthekitchen.Thecornersofthesurfaceshavingmold,greenygraymold.Generaldisorder—lotsofdirtycrockery,lotsoffood.Generalhorror.Smellofmold(pp178)
Whatmymotherlookedlikewhenhealthyandwell.Whatshelookedlikeafteraseriesofstrokes(pp269)
Pictureofahumanbrainwithnastypathology—fearaboutmyownbrain.Upclose,almostimmersive,notascansection,beinginthemiddleofit.Cavitieswithfluidinthem,welllit,softwhiteyellowlight.Quiet(pp185)
Envisagedrivingintothecarpark,walkingupstairsandintotheofficeandnotfeelinghappy(pp294)
Ratings:Mean(SD)
Demotivating**c:7.04(2.23);Emotionala:7.13(2.27);Negative*b:2.13(1.44) Demotivating:4.82(2.59);Emotional:6.77(1.57);Negative:2.96(1.82).
Anxiousstate Paranoidfearoffuture—teacherreprimandingmefornotworking.Expectationorneedforpunishment.Mealoneinaclassroom,teachershouting,aggressivegestures,fingerspointing.Mesittingdownthenstandingup.Heightdifference,Iambeinglookeddownuponphysicallyandmetaphorically(pp153)
Bestfriendandmehavingacupofcoffeehavinganargument(pp129)
Husband’stakenthechildrenaway.Seeingchildrenwithmyhusband,toldtopacktheirbagsandgetinthecar.They’reconfused,they’repacking,doingwhatdadsays.He’spackingaswell.Icanseemyselfupsetintheimage(p177)
Visitingaclientduringmyshadowingday(pp149)
AmanwascuttingdownabushandIcouldseehisgardeningtoolslippingandhecutshisarmoff.Veryvivid,itseemslikemyimaginationrunningover,seemsquitereal.Alotofblood(pp190)
SeeingbosscallmetosayIwasbeingmaderedundant(pp251)
Ratings:Mean(SD)
Threatening**c:7.00(2.21);Emotional:**c7.69(1.45);Negative**c:1.81(1.04) Threatening:5.52(2.25);Emotional:6.24(1.97);2.86(1.31)
High mood Meinaverysuccessfulsituation,writtenabrilliantbook,receivingaccolades.Criticalacclaiminapaper.Imageofmereceivingaward“He’ssoinsightful”receivingitinfrontoffriendsandfamily(pp155)
Trees,breeze,peaceofthecountryside(pp124)
Superbsexwithsomeoneutterlyuntouchable.Seeunderstandingandconversationandabsoluteeverythingbeingtunedinwitheachother.Hugepraisecomingyourway,acceptanceandappreciation.Somebodybeingasinfatuatedwithyouasyouarethem.Seeingahomeandasettingwhereitisallgoingtohappen,stuffgatheredforyoubecauseeverythingisgoingtobepossible(pp163)
Imageofstandinginadoorwayandchattingtoeveryoneandtheyareallsmilingback(friends)(pp142)
Icanseeimagesofthingsingeneralrelativity,e.g.curvedspacetime.Veryreal,Icanbuildonthat.Imagesarepartofmywork,problemsolvingforme.Rubberballinasheet,takinga2Dobjectandmakingitinto3D.Icanseehowtheotherdimensionswork.Youcanwritethealgebra,visualequivalentofalgebraicformula(pp185)
Imageofmyselfasawise,guru-likefigure(pp279)
Ratings:Mean(SD)
Exciting**c:8.06(1.24);Emotionala:7.16(2.04);Positivea:7.76(1.80) Exciting:7.04(1.54);Emotional:6.92(1.44);Positive:7.80(0.91)
pp,participant;SD,standarddeviation.*P<0.05;**P<0.01.a0<d≤0.3.b0.3<d≤0.6.cd>0.6.

| 679SIMPLICIO et aL.
3.5.1 | Cognitive (non- emotional) stages of mental imagery
BD phenotypeAcrossallgroups,higherlevelsofhypomanicexperiences(measuredbytheMDQscores)wereassociatedwithworseperformanceonim-agery manipulationasmeasuredbyahighererrorrateontheMRTtask[β=0.249,t(122)=2.835,P=.005].
Affective labilityAcross all groups, higher levels of affective lability (measured byscoresontheALS)wereassociatedwithbetterperformanceon im-agery maintenanceasmeasuredbyahigherrecallrateontheSTMtask[β=0.229,t(114)=2.513,P=0.013].
3.5.2. | Subjective domains of mental imagery
BD phenotypeAcross all groups, higher levels of hypomanic experiences (meas-ured by the MDQ scores) were associated with higher ratings onhowthreateningthemostsignificant imagewasattimesofanxiousaffectontheMII[β=0.190,t(114)=2.068,P=.041],andonhowexcit-ingthemostsignificantimagewasattimesofelatedmood[β=0.221,t(119)=2.467,P=.015].
Affective labilityAcross all groups, higher affective lability scores (measured on theALS)wereassociatedwithgreater impactofemotionalprospectiveimagery scores on the IFES [β=0.293, t(119)=3.43,P=.001]. Higheraffective lability levels were also associatedwith higher ratings ontheMIIofhownegativethemostsignificant imagewasattimesoflowmood[β=−0.333,t(112)=3.740,P<.001],andhowfrequentlypar-ticipantswere thinking inmental images at times of anxious affect[β=0.250, t(125)=2.885, P=.005] On the PW task, higher affectivelabilitywasassociatedwithhigherratingsofhowself-involvedpar-ticipantsfeltwhengeneratingpicture−wordcombinations[β=0.189,t(122)=2.466,P=.015].
AnxietyAcrossallgroups,higheranxietyscores(measuredontheBAI)wereassociated with greater impact of emotional prospective imageryscoreson the IFES [β=0.415, t(119)=4.23,P<.001];highervividnessratingsofnegativeeventsonthePIT[β=0.343,t(124)=3.54,P=.001],andastrongersenseofexperiencingimaginednegativeeventsonthePIT[β=0.293,t(124)=2.530,P=.013].
Low moodAcrossall groups, lowerdepressionscores (measuredon theQIDS)were associatedwith higher likelihood ratings of positive imaginedevents to happen on the PIT [β=−0.431, t(125) =5.344, P<.001].Higherdepression scores insteadwere significantly associatedwithratingsofhowdemotivatingthemostsignificantimagewasattimesoflowmood[β=0.305,t(111)=3.371,P=.001].
General functioningAcrossallgroups,lowergeneralfunctioning(measuredusingtheFASTscores)wasassociatedwithgreaterimpactofemotionalprospectiveimageryscoreson the IFES [β=0.259, t(19)=2.64,P=.009];andwithhowrealmentalimageswereratedattimesofanxiousaffectontheMII[β=0.244,t(123)=2.792,P=.006].
Clinical and functioningvariables across all groupswere not re-lated to how realmental imageswere rated at times of highmood[F(6,118)=0.96,P=.46,R2=.05].
4 | DISCUSSION
4.1 | Summary of main findings
Ourstudy investigated,first,whetherBDisassociatedwithabnor-malitiesinmentalimagerycomparedtonon-clinicalcontrols;second,whetheranysuchabnormalitiesarespecifictoBDwhencomparedtoclinicalcontrolgroupsmatchedfordepressionandanxiety.Further,weexploredwhetherabnormalitiesinmentalimageryareassociatedwith clinical variables across diagnostic groups. Results show that,comparedtonon-clinicalcontrols, individualswithBDshowlargelyintact performance on experimental tasksmeasuring the cognitive(non-emotional) stagesofmental imagery.However, in thesubjec-tivedomainsofmental imagery,compared tonon-clinicalcontrols,individualswithBDdoshowsomeabnormalitiesinemotionalmentalimagery:namely,agreater impactof intrusiveprospective imageryindailylife,morevividand“real”negativeimagesonaprospectiveimagery task, and higher levels of self-involvement in imagery ona picture−word task. Moreover, on a phenomenological interviewabout times of intense affect (anxious, depressed, or high), it wascharacteristics ofmental imagery, but not of verbal thoughts, thatdistinguishedindividualswithBDfromnon-clinicalcontrols.Resultsfurther indicate that, when compared to clinical control groupsmatchedfordepressionandanxiety,abnormalitiesinemotionalmen-tal imagerywerenot specific toBDbutassociatedwith increasingpsychopathology.
Interestingly, our results show that, across all clinical and non-clinicalgroups,mentalimageryabnormalitiesareassociatedwithse-verityofdepressionandanxiety,aswellaswithBDphenotypeandaffectivelabilitytraits,andgeneralfunctioning.Thisraisesthepossi-bilitythatthesubjectiveexperienceofhighlyemotionalmentalimag-ery(assessedbyarangeofmeasuresacrossdifferentaffectstates)isa transdiagnosticfeatureofpsychopathology,andassociatedinpartic-ularwithaffectivelabilityacrossclinicalandnon-clinicalpopulations.Thisfindingisparticularlyinterestinggiventhataffectlability(includ-ing concurrent anxiety) represents a particularly challenging featureacrossdifferentmentaldisorders.
4.2 | Emotional mental imagery in BD
We replicated previous findings that individualswithBD (euthymicand depressed combined) experience a greater impact of intrusive

680 | SIMPLICIO et aL.
prospectivemental imageryineverydaylife,7andperceiveprospec-tivenegativeimagesasmorevividinanexperimentaltaskcomparedtonon-clinicalcontrols.7Further,weextendedthesefindingsinthatoursampleofparticipantswithBDalsoreportedmorereal (greater“senseofexperiencing”)prospectivenegativementalimagesandper-ceived imaginedpositiveeventsas less likely tooccurcompared tonon-clinical controls. Consistentwith a greater sense of experienc-inganxietyfornegativeprospectiveimages,comparedtonon-clinicalcontrols,participantswithBDalsofeltmoreself-involvedwhenspon-taneouslygeneratingmental imagesbycombiningnegativepicturesand words.
Unlikepreviousstudies,wedidnotfindevidenceofgreaterspon-taneoususeofnon-emotionalmentalimageryinBDcomparedtonon-clinicalcontrols,althoughmeanvalueswereinthesamedirectionasinapreviousstudy.7Thissuggeststhatdifferencesinspontaneousten-dencytovisualizearelikelytobesmallandtestofreplicationinlargersamplesisneededtoverifytheseinconsistencies.
Overall our BD sample reported imagery abnormalities particu-larly forprospective imageryandduringanxiousaffect.This is con-sistentwith the relationshipbetweenanxietyand future thinking.46 Asprospectionplaysanimportantroleinregulatingemotionsandbe-havior,47itispossiblethattheseabnormalitiesinprospectiveimagery(althoughnotlimitedtoBD;seebelow)contributetoemotionalandbehavioraldysregulationtypicalofBD.6Itcouldbefruitfultoinvesti-gatetheeffectofprospectiveimageryonthepresenceandseverityofcomorbidanxiety,whichisakeyclinicalfeatureinBD.48,49Forex-ample,oneparticipantwithBDreportedthatwhenmostanxioustheyrepeatedly experiencevivid negative images of embarrassing them-selvesatasocialevent;theimagesfeelsorealthattheyfurtherfuelanticipatoryanxietytothepointofmakingthemavoidattendingtheevent.Abetterunderstandingofprospectiveanxiety-inducingimag-eryinBDmayalsohaveimplicationsfortherapy,giventhechallengeof treatinganxiety in thisdisorder.18,48Futurestudiescould investi-gatewhethertheexperienceofemotionalmentalimageryinBDdif-fersdependingonthetypeofanxietycomorbidity,followingcurrentcognitiveaccountsofanxietydisorderswhereimageryispredominant,suchassocialanxiety,16orirrelevantifnotsuppressed,suchasgeneralanxietydisorder.50
4.3 | Cognitive stages of mental imagery in BD
Finally,andnoveltothe literature(ascalledforbyPearsonetal.11),theabsenceofmajordysfunctions in the cognitive (non-emotional)stagesofmentalimagerysuggeststhattherearenodeficitsintheabil-ity togenerate,manipulate,andrecall images. Interestingly,ourBDsamplealsoshowedagreaterlikelihoodofrecallingthetargetcuesinoneofthevisualshort-termmemorytaskscomparedtonon-clinicalcontrols.Thus, individualswithBDappear tohaveanoverall intactfunctioningorevenan“advantage”inthisaspectofimageryprocess-ing.Therefore,drawingonmental imagery techniques18,51 could be asuccessfulstrategyintreatmentinterventionsforBDwhereothercognitiveprocessesmaybeimpaired(asinoursamplewithreducedverbalfluency/executivefunctionperformance).52
4.4. | Mental imagery abnormalities as a transdiagnostic phenomenon
Unlike previous studies comparing BD and unipolar depressed pa-tients,8,10 no differences emerged between our clinical groups inprospective imagery measures. In fact, across the whole samplecombined,prospective imageryabnormalities (onIFEStotalandPITnegativescenariosscores)wereassociatedwithseverityofanxioussymptomatologyandaffectivelabilitytraits.Thissuggeststhatincon-sistenciesbetween studiesof clinical groupsmaybe accounted forbytherelativedistributionofaffective labilitytraitsandconcurrentanxietyinthesamples.
Consistentwithpreviousdata,10depressedparticipantswithBDrated theirmost significant image at times of highmood asmoreexcitingcomparedtoparticipantswithunipolardepression.Thismayreflectbothanassociationbetweenmaniaandpositivementalim-agery (even at times of depressedmood) and a deficit in positivemental imagery in unipolar depression51,53,54. The finding is alsoconsistent with recent neuroimaging evidence showing that par-ticipantswithBDandunipolardepressionpresentdifferentneuralresponses to positive stimuli only while depressed.55We did notreplicatepreviousevidenceofnegativeimagesbeingmorecompel-ling inBDcompared tounipolar patients.8This discrepancymightbeaccountedforbylessseverelydepressedsamplesinthepresentstudyormaysuggestthatgreatercompellingnessmightbespecifictosuicidalflashforwardsinpatientswithBD8ratherthananyimageduring low mood.
With regard to the cognitive (non-emotional) stages of mentalimagery,previousstudieshavereportedbiasesinimagerygenerationandmanipulationinunipolardepressedindividualscomparedtocon-trols13,44;however,thesedepression-relatedabnormalitieswereonlypresent inmeasures that indexthesensory/responsecomponentofimagerytasks13 ratherthanspecific imagery (e.g.spatialability)pro-cessing biases. Therefore, discrepancies between studies may beexplainedbydifferencesinsensory-motorretardationsymptomsbe-tweenthesamples.
Overall, our study indicates that mental imagery characteris-tics representingfeaturesofgreateremotionalityand intensity (e.g.,greater intrusive imagery impact, vividness of negative images, andsenseofrealnessofimages)mayrepresentamarkerforgeneralemo-tional psychopathology, and general functioning. This supports ourideathat“bringingbackthemind’seye”topsychiatricassessments17 couldhelp identifyclinicalseverity.Most importantly itcanhelpcli-nicians to understand and normalize aspects of patients’ subjectiveexperiencesthatmayotherwisefeelparticularlyalienanddistressing(suchasintrusivehighlyemotionalmentalimages).Askingaboutmen-tal imagesoffersanalternativeaccesstocapturingdistress inthosepatientswhomay struggle to communicate their subjective experi-encesviatraditionalverbalthoughts.Thetransdiagnosticrelevanceofmental imageryalsohighlightspotential avenues fornew treatmentinterventions: e.g. if depression scores relate to how likely positivefutureimagesfeel,revertingpositiveimagerybiasesmaybeausefultargettoimprovemood.36,51,56

| 681SIMPLICIO et aL.
OurresultsontheassociationbetweenBDphenotypeandaffec-tivelabilitytraits,andgreaterimageryfrequencyandemotionality,areinkeepingwithpreviousfindingsthatindividualswithaBDphenotypearemoresusceptibletointrusiveimageryandtospontaneoususeofimagery.57,58Interestingly,betterperformanceinimagerymaintenanceviavisualshort-termmemorywasalsoassociatedwithaffectivelabil-ity.Futurestudiesshouldinvestigatetherelationshipbetweenbiasesinemotionalmentalimagery,visualshort-termmemoryfunctionandemotionalinstabilityacrosspsychopathology,includinginothercon-ditionswherethisisrelevantsuchasborderlinepersonalitydisorder.Overall,mentalimagerybiasescouldbeconceptualizedasacognitivepsychopathologicaldimension in linewithmostrecentneurosciencedimensionalapproachestounderstandingmentaldisorders(researchdomain criteria59). Future research should investigatehowcurrentlyestablishedcognitiveandneuralmarkersofemotionaldysregulationandaffectivelability60–62relatetoabnormalitiesinemotionalmentalimagerydescribedinoursample.Moreover,asaffectivelabilityoftenrepresentsa therapeuticchallenge, treatment innovationshouldex-plorethepotentialforusingimagery-focusedinterventionsforemo-tionalinstability.18
5 | LIMITATIONS AND CONCLUSIONS
A limitationofour study is theabsenceof statistical correction formultiplecomparisons.Moreover,wedidnotincludea(hypo)manicBDgroupthatwouldallowustoestablishthepresenceofmentalimageryabnormalitiesassociatedwithmaniastatediagnosis.Withregardtoresults fromtheMII, itshouldalsobenotedthat thesewerebasedonretrospectiveaccountsoftimesofintenseaffectandcouldhavebeensubjecttorecall/memorybiases.Futurequalitativestudiesareneeded to analyze in detail potential differences in the image con-tents exemplified inTable5.Our data suggest thatmental imageryabnormalities are typical of acute clinical states of anxiety and de-pression,butarealsoassociatedwithtraitsofBDphenotypeandaf-fective lability. Future studies should include individuals recoveredfromunipolardepressionandanxietydisorderstoclarifyifemotionalmental imageryabnormalitiesalsopersistbeyondacutedepression/anxiety across psychopathology, as they do in our BD sample (eu-thymicanddepressed).Moreover,asourclinicalgroupsallpresentedmoderatetohighlevelsofbothanxietyanddepression,futurestudiescouldattempttoteaseaparttheassociationbetweenmentalimageryabnormalities and anxiety/depression, although thismay be a chal-lengegiventhehighco-occurrenceofthesesymptomsinemotionaldisorders.Nevertheless, theregressionanalysesacrossallgroups inour sample suggest a greater impact of anxiety onmental imagerycharacteristics.Finally, longitudinal ratherthancross-sectionalstud-iesshouldfurtherinvestigatestabilityandchangeofmentalimageryabnormalities inBDover thecourseof illness.FuturestudiescouldalsocompareindividualswithbipolarIandIIdisorderusingsufficientlypoweredsamples.
Inconclusion,thisfirstcomprehensiveinvestigationofarangeofmental imagerymeasures in BD compared to both non-clinical and
clinicalcontrolsconfirmsthatimageryabnormalitiesarepresentinpa-tientswithBDintheemotionalaspectsofmentalimagery,whilethecognitiveprocessesunderpinningmental imageryexperienceremainlargelyintact.Biasesinemotionalmental imageryappearasatrans-diagnosticfeatureofourclinicalgroupsmatchedondepressionandanxietylevelsrelatedtoclinicaldysfunction.Wesuggestthatimageryabnormalitiesareatransdiagnosticprocessesdrivingaffectivelability,and that imagerycanbe targetedvianovelpsychological treatmenttechniques.Imagery-focusedtechniquesholdpromiseacrosspsychi-atricdisorders,17includingaddingtreatmentvaluetoBD.18
ACKNOWLEDGEMENTS
EAH held a Wellcome Trust Clinical Fellowship (WT088217) sup-portingHM.EAH,SEB,andFRwerealsosupportedbytheMedicalResearch Council (United Kingdom) intramural program (MC-A060-5PR50 to EAH) including aMedical ResearchCouncil CareerDevelopment Fellowship to MDS. EAH and ACN were also sup-portedbytheNational InstituteforHealthResearch(NIHR)OxfordBiomedical Research Centre Programme. FR was supported by aMarie Sklodowska-Curie individual Fellowship from the EuropeanUnion and by a postdoctoral research fellowship from theGermanAcademicExchangeService (DAAD).HJSwassupportedduringherdoctorate by the Oxford Institute of Clinical Psychology Training.AL-ZwassupportedbytheCambridgeCommonwealth,European&InternationalTrust.Theviewsexpressedarethoseoftheauthorsandnot necessarily those of theNHS, theNIHR or theDepartment ofHealth. The funding source had no involvement in study design, inthecollectionandanalysisof thedata,or in thedecision tosubmitthepaperforpublication.Wethankthefollowingfortheirhelpwithdata collection and entry: Sophie Wallace-Hadrill, Angela Rylands,EmmyUphoff,RebeccaHewstone,IanClark,AiyshaMalikandNatalieBarnes.WearegratefultotheOxfordHealthNHSFoundationTrustforsupportingtheresearch.FundingtopaytheOpenAccesspubli-cationcharges for thisarticlewasprovidedbytheUnitedKingdomMedicalResearchCouncil(MC-A060-5PR50).DataandmaterialsareavailableviaOpenScienceFrameworkandcanbeaccessedathttps://osf.io/xwrny/,orareotherwiseavailablefromtheauthorsonrequest(withtheexceptionofquestionnairemeasuressubjecttothird-partycopyrightorpotentiallyidentifyingpatientinformation).ProtocolsforstudyproceduresaresubjecttoaMaterialTransferAgreement.
DISCLOSURES
Theauthorsofthispaperdonothaveanycommercialassociationsthatmightposeaconflictofinterestinconnectionwiththismanuscript.
REFERENCES
1. Pearson J, Naselaris T, Holmes EA, Kosslyn SM. Mental imagery:Functionalmechanisms and clinical applications.Trends in cognitive sciences.2015;19:590–602.
2. HolmesEA,MathewsA.Mental imagery inemotionandemotionaldisorders. Clin Psychol Rev.2010;30:349–362.

682 | SIMPLICIO et aL.
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th edn. Arlington, VA: American PsychiatricPublishing;2013.
4. Strejilevich SA, Martino DJ, Murru A, et al. Mood instability andfunctional recovery in bipolar disorders. Acta Psychiatr Scand. 2013;128:194–202.
5. BonsallMB,Wallace-HadrillSMA,GeddesJR,GoodwinGM,HolmesEA. Nonlinear time-series approaches in characterizing mood sta-bilityandmood instability inbipolardisorder.Proc R Soc B: Biol Sci. 2012;279:916–924.
6. HolmesEA,GeddesJR,ColomF,GoodwinGM.Mentalimageryasanemotionalamplifier:Applicationtobipolardisorder.Behav Res Ther. 2008;46:1251–1258.
7. Holmes EA, Deeprose C, Fairburn CG, et al.Mood stability versusmood instability in bipolar disorder: A possible role for emotionalmentalimagery.Behav Res Ther.2011;49:707–713.
8. HalesSA,DeeproseC,GoodwinGM,HolmesEA.Cognitions inbi-polar affecive disorder and unipolar depression: Imagining suicide.Bipolar Disord.2011;13:651–661.
9. HawtonK,SuttonL,HawC,SinclairJ,HarrissL.Suicideandattemptedsuicideinbipolardisorder:Asystematicreviewofriskfactors.J Clin Psychiatry.2005;66:693–704.
10. IvinsA,DiSimplicioM,CloseH,GoodwinGM,HolmesEA.Mentalimagery in bipolar affective disorder versus unipolar depression:Investigatingcognitionsattimesof“positive”mood.J Affect Disord. 2014;166:234–242.
11. Pearson DG, Deeprose C, Wallace-Hadrill SMA, Burnett Heyes S,Holmes EA.Assessingmental imagery in clinical psychology:A re-viewofimagerymeasuresandaguidingframework.Clin Psychol Rev. 2013;33:1–23.
12. Kosslyn SM,ThompsonWL,GanisG.The Case for Mental Imagery. NewYork,NY:OxfordUniversityPress,Inc.;2006.
13. ZarrinparA,DeldinP,KosslynSM.Effectsofdepressiononsensory/motor vs. central processing in visual mental imagery. Cogn Emot. 2006;20:737–758.
14. MorrisonAS,AmirN,TaylorCT.Abehavioralindexofimageryabilityinsocialanxiety.Cogn Ther Res.2011;35:326–332.
15. NelisS,HolmesEA,GriffithJW,RaesF.Mentalimageryduringdailylife: Psychometric evaluation of the Spontaneous Use of ImageryScale(SUIS).Psychol Belgica.2014;54:19–32.
16. HackmannA,SurawyC,ClarkDM.Seeingyourself throughothers’eyes: A study of spontaneously occuring images in social phobia.Behav Cogn Psychother. 1998;26:3–12.
17. DiSimplicioM,McInerneyJE,GoodwinGM,AttenburrowM,HolmesEA.Revealingthemind’seye:Bringing(mental)imagesintopsychia-try.Am J Psychiatry.2012;169:1245–1246.
18. HolmesEA,BonsallMB,HalesSA,etal.Applicationsoftime-seriesanalysis tomoodfluctuations in bipolar disorder topromote treat-ment innovation:A case series.Transl Psychiat. 2016;6:e720. Epub2016/01/27.
19. First MB, Spitzer RL, Gibbon M,Williams JBW. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, PatientEdition.(SCID-I/P).NewYork:BiometricsResearch,NewYorkStatePsychiatricInstitute;2002.
20. HamiltonM.Aratingscalefordepression.J Neurol.1960;23:55–62.21. Young RC, Briggs JT, Ziegler VE, Meyer DA. A rating scale for
mania:Reliability,validity,andsensitivity.Br J Psychiatry.1978;133: 429–435.
22. AltmanEG,HedekerD,PetersonJL,DavisJM.TheAltmanself-ratingmania scale. Biol Psychiatry.1997;42:948–955.
23. RushJA,TrivediMH,IbrahimHM,etal.The16-itemquickinventoryofdepressivesymptomatology(QIDS),clinicianrating(QIDS-C),andself-report (QIDS-SR): A psychometric evaluation in patients withchronicmajordepression.Biol Psychiatry.2003;54:573–583.
24. BeckAT,SteerRA.Beck Anxiety Inventory Manual.SanAntonio,TX:PsychologicalCorporation;1993.
25. HirschfeldRMA,WilliamsJB,SpitzerRL,etal.Developmentandval-idationofascreeninginstrumentforbipolarspectrumdisorder:Themooddisorderquestionnaire.Am J Psychiatry.2000;157:1873–1875.
26. HarveyPD,GreenbergBR,SerperMR.Theaffective lability scales:Development,reliabilityandvalidity.J Clin Psychol.1989;45:786–793.
27. ReisbergB.Functional assessment staging (FAST).Psychopharmacol Bull.1988;24:653–659.Epub1988/01/01.
28. NelsonHE,WillisonJ.National Adult Reading Test Manual,2ndedn.Windsor,ON:NFER-Nelson;1991.
29. StraussE,ShermanEM,SpreenO.A Compendium of Neuropsychological Tests: Administration, Commentary and Norms,3rdedn.NewYork,NY:OxfordUniversityPress;2006.
30. Tulsky DS, Ledbetter MF. Updating to the WAIS-III andWMS-III:Considerations for research and clinical practice. Psychol Assess. 2000;12:253–262.Epub2000/10/06.
31. BernaC,LangTJ,GoodwinGM,HolmesEA.Developingameasureofinterpretationbiasfordepressedmood:Anambiguousscenariostest.Personality Individ Differ.2011;51:349–354.
32. Holmes EA, Lang TJ, Moulds ML, Steele AM. Prospective andpositive mental imagery deficits in dysphoria. Behav Res Ther. 2008;46:976–981.
33. HolmesEA,MathewsA,MackintoshB,DalgleishT.Thecausaleffectof mental imagery on emotion assessed using picture-word cues.Emotion.2008;8:395–409.
34. Deeprose C,MalikA,Holmes EA.Measuring intrusive prospectiveimageryusingtheImpactofFutureEventsScale(IFES):Psychometricproperties and relation to risk for bipolar disorder. Int J Cogn Ther. 2011;4:187–196.
35. StöberJ.Prospectivecognitionsinanxietyanddepression:Replicationandmethodologicalextension.Cogn Emot.2000;14:725–729.
36. Blackwell SE, Rius-Ottenheim N, Schulte-vanMaarenYWM, et al.Optimismandmental imagery:Apossible cognitivemarker topro-motewellbeing?Psychiatry Res.2013;206:56–61.
37. Dror IE, Kosslyn SM. Mental imagery and aging. Psychol Aging. 1994;9:90–102.
38. ZhangW,LuckSJ.Discretefixed-resolutionrepresentationsinvisualworkingmemory.Nature.2008;453:233–235.
39. MyersNE,StokesMG,WaltherL,NobreAC.Oscillatorybrainstatepredicts variability in working memory. J Neurosci: Official J Soc Neurosci.2014;34:7735–7743.Epub2014/06/06.
40. Della SS, Gray C, BaddeleyAD,Wilson L. The Visual Patterns Test: A New Test of Short-Term Visual Recall. Feltam: Thames Valley TestCompany;1997.
41. Farah J, Hammond KM, Levine DN, Calvanio R.Visual and spatialmentalimagery:Dissociablesystemsofrepresentations.Cogn Psychol. 1988;20:439–462.
42. Shepard RN, Metzler J. Mental rotation of 3-dimensional objects.Science.1971;171:701–703.
43. BorstG,KievitRA,ThompsonWL,KosslynSM.Mentalrotationisnoteasilycognitivelypenetrable.Eur J Cogn Psychol2011;23:60–75.
44. RogersMA,BradshawJL,PhillipsJG,ChiuE,MileshkinC,VaddadiK.Mentalrotationinunipolarmajordepression.J Clin Exp Neuropsychol. 2002;24:101–106.
45. FinkeRA,SlaytonK.Explorationsofcreativevisualsynthesisinmen-talimagery.Mem Cognit.1988;16:252–257.
46. Miloyan B, Pachana NA, Suddendorf T. The future is here: A re-view of foresight systems in anxiety and depression. Cogn Emot. 2014;28:795–810.Epub2013/12/11.
47. Szpunar KK, Spreng RN, Schacter DL. A taxonomy of prospec-tion: Introducing an organizational framework for future-orientedcognition. Proc Natl Acad Sci USA. 2014;111:18414–18421. Epub2014/11/25.

| 683SIMPLICIO et aL.
48. StratfordH,BlackwellSE,DiSimplicioMC,CooperM,HolmesEA.Psychologicaltherapyforanxietyinbipolarspectrumdisorders:Asys-tematicreview.Clin Psychol Rev.2014;35:19–34.
49. OttoMW,SimonNM,Wisniewski SR, et al. Prospective12-monthcourseofbipolardisorderinout-patientswithandwithoutcomorbidanxietydisorders.Br J Psychiatry.2006;189:20–25.
50. Dugas M, Koerner N. Cognitive-behavioral treatment for general-ized anxiety disorder: Current status and future directions. J Cogn Psychother.2005;19:61–81.
51. Blackwell SE, Browning M, Mathews A, et al. Positive imagery-based cognitive bias modification as a web-based treatment toolfordepressedadults:Arandomizedcontrolledtrial.Clin Psychol Sci. 2015;3:91–111.
52. ArtsB,JabbenN,KrabbendamL,vanOsJ.Meta-analysesofcognitivefunctioning ineuthymicbipolarpatientsand theirfirst-degree rela-tives.Psychol Med.2008;38:771–785.Epub2007/10/10.
53. HolmesEA,BlackwellSE,Burnett-HeyesS,RennerF,RaesF.Mentalimagery in depression: phenomenology, potentialmechanisms, andtreatmentimplications.Annu Rev Clin Psychol.2016;12:249–280.
54. Morina N, Deeprose C, Pusowski C, Schmid M, Holmes EA.Prospectivementalimageryinpatientswithmajordepressivedisor-deroranxietydisorders.J Anx Disorders.2011;25:1032–1037.
55. RiveMM,MockingRJ,KoeterMW,etal.State-dependentdifferencesin emotion regulation between unmedicated bipolar disorder andmajordepressivedisorder.JAMA Psychiatry.2015;7:687–696.
56. WilliamsAD,BlackwellSE,HolmesEA,AndrewsG.Positiveimagerycognitivebiasmodification (CBM)and internet-basedcognitivebe-haviouraltherapy(iCBT)versuscontrolCBMandiCBTfordepression:Studyprotocolforaparallel-grouprandomisedcontrolledtrial.BMJ Open.2013;3:e004049.
57. MalikA, Goodwin GM, Hoppitt L, Holmes EA. Hypomanic experi-enceinyoungadultsconfersvulnerabilitytointrusiveimageryafter
experimentaltrauma:Relevanceforbipolardisorder.Clin Psychol Sci. 2014;2:675–684.
58. NgRMK,BurnettHS,McManusF,KennerleyH,HolmesEA.BipolarriskandmentalimagerysusceptibilityinarepresentativesampleofChineseadultsresidinginthecommunity.Int J Soc Psychiatry2015;62:94–102.
59. Insel TR, Cuthbert B, Garvey M, et al. Research Domain Criteria(RDoC):Towardanewclassificationframeworkforresearchonmen-taldisorders.Am J Psychiatry.2010;167:748–751.
60. HeisslerJ,KanskeP, SchonfelderS,WessaM. Inefficiencyof emo-tionregulationasvulnerabilitymarkerforbipolardisorder:evidencefromhealthyindividualswithhypomanicpersonality.J Affect Disord. 2014;152-154:83–90.
61. deCardosoAlmeidaJR,PhillipsML.Distinguishingbetweenunipo-lardepressionandbipolardepression:Currentandfuturecinicalandneuroimagingperspectives.Biol Psychiatry.2013;73:111–118.
62. M’BailaraK,ChevrierF,DutertreT,Demotes-MainardJ,SwendsenJ,HenryC.Emotionalreactivityineuthymicbipolarpatients.Encephale. 2009;35:484–490.
SUPPORTING INFORMATION
AdditionalSupportingInformationmaybefoundonlineinthesupport-inginformationtabforthisarticle.
How to cite this article:DiSimplicioM.,RennerF.,BlackwellS.E.,MitchellH.,StratfordH.J.,WatsonP.,MyersN.,NobreA.C.,Lau-ZhuA.andHolmesE.A.(2016),Aninvestigationofmentalimageryinbipolardisorder:Exploring“themind’seye”.BipolarDisorders,18:669–683.doi:10.1111/bdi.12453