an overview of genital stromal tumors - pathcme.com · vagina or cervix • nodular or...
TRANSCRIPT

An Overview of Genital Stromal Tumors
By Konstantinos Linos MD, FCAP, FASDP
Bone, Soft Tissue and Dermatopathology
Assistant Professor of Pathology
Dartmouth-Hitchcock Medical Center
Geisel School of Medicine at Dartmouth
Hanover, NH, USA

• Book Royalties
Financial disclosures

• Broad variety of soft tissue tumors exclusively in vulvovaginal and inguinoscrotal sites
• Probably originate from a distinct zone of subepithelial stromal cells or subepithelialmesenchyme extending from the endocervix
• Striking morphologic, immunophenotypic and genetic overlap
General

• Fibroepithelial Polyp• Superficial Myofibroblastoma• Cellular angiofibroma• Mammary-type myofibroblastoma• Angiomyofibroblastoma• Deep/”Aggressive” angiomyxoma• Superficial Angiomyxoma• Prepubertal Vulvar Fibroma• Lipoblastoma-Like tumor of the vulva• Smooth Muscle Tumors of the external
genitalia

• Synonyms• Mesodermal stromal polyp• Cellular Pseudosarcomatous fibroepithelial
stromal polyp• Pseudosarcoma botryoides
• Benign polypoid growth of the vagina, vulva or cervix
• Strongly tied to hormonal stimulation
Fibroepithelial Stromal Polyp

• Most often during pregnancy • also in reproductive age women• Postmenopausal women undergoing hormonal
replacement
• Regression in the postpartum period is typical
• Typical clinical presentation is one or more polyps that may be symptomatic
• Usually 1-5cm






Immunohistochemistry
• Consistently reactive for• Desmin• Estrogen Receptor (ER)• Progesetrone Receptor (PR)• Sometimes Smooth Muscle Actin



Enbryonal
Rhabdo-
myosarcoma
Rhabdomyoma

Superficial (cervicovaginal) myofibroblastoma
• Benign tumor that may arise in the vulva, vagina or cervix
• Nodular or polypoid painless mass in adults most commonly in their 50s
• Grossly well-circumscribed, firm and dense mass from 1 to 6.5cm




Immunohistochemistry• Desmin in 75-100% of cases
• ER/PR in 80-100%
• CD34 in 50-85%
• SMA in 0-45%

Cellular Angiofibroma• Synonym
• Angiomyofibroblastoma-like tumor of the male genital tract
• Benign neoplasm in vulvovaginal and inguinoscrotal areas
• Middle-aged patients with a female predominance
• Classically subcutaneous painless nodule usually not exceeding 7cm








Immunohistochemistry
• Inconsistent expression
• Variable expression of CD34, desmin, SMA
• P16 positivity in sarcomatous areas
p16

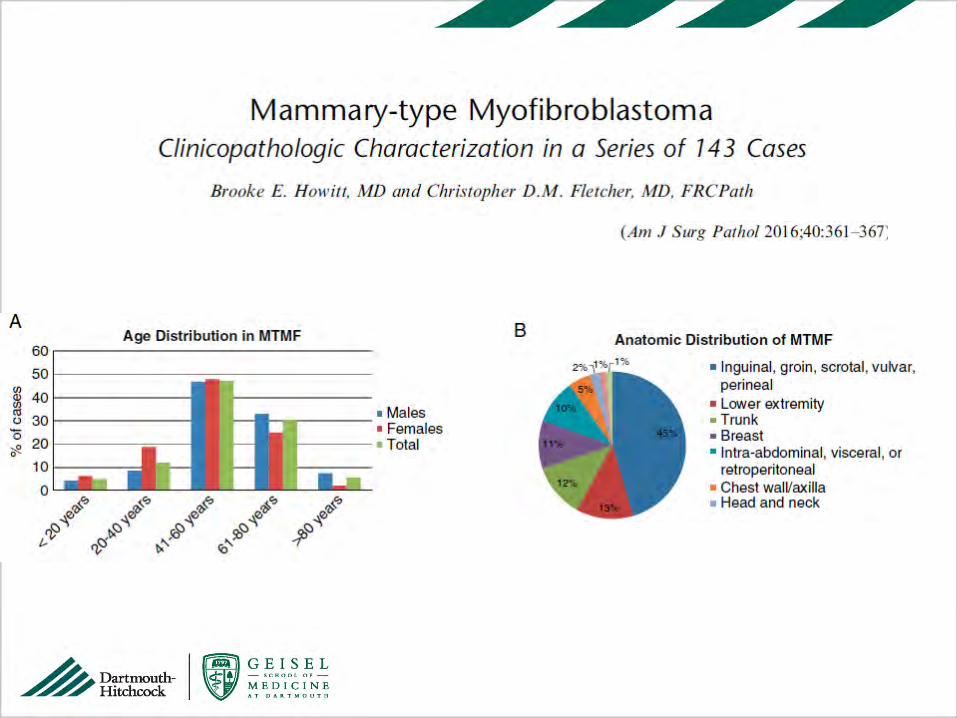
Mammary-type Myofibroblastoma
• Initially described in breast • Can arise anywhere in soft tissue • Predilection for inguinal and pelvic region
• Most cases occur in men
• Median age 53
• Range 1-22cm (median size of 6cm)


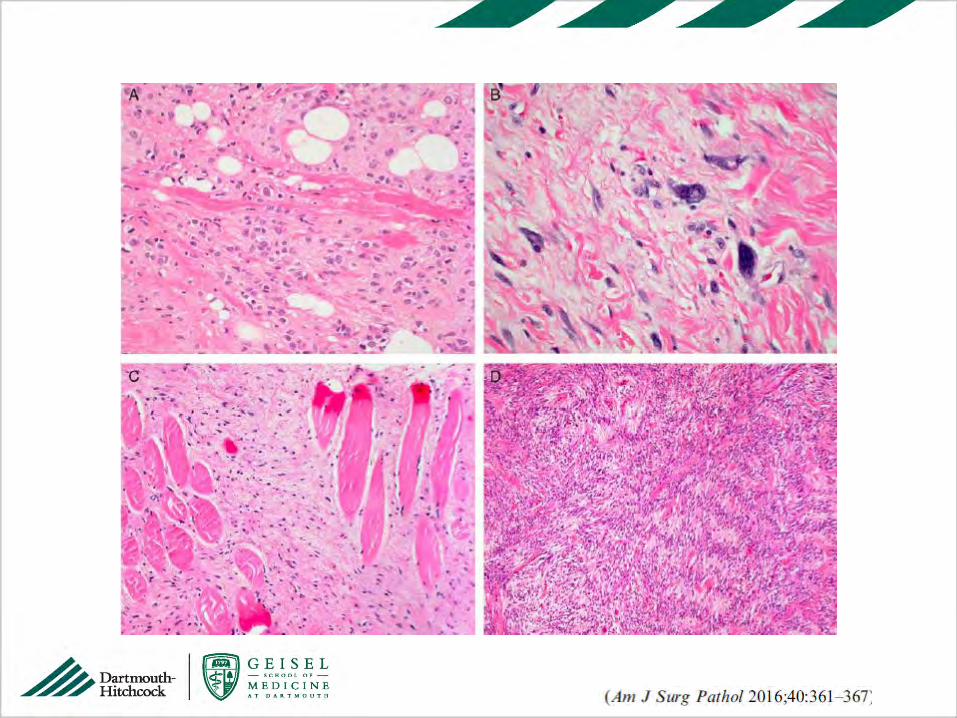

Immunohistochemistry
• Frequently positive for CD34 and Desmin (~90%)
• Rare cases negative for both (~3%)
CD34 Desmin

• Benign tumor
• Local excision curative
• No evidence of significant recurrence risk even in the presence of positive resection margins
Prognosis

RB1 and Genital Stromal Tumors

Mammary-type
myofibroblastoma
Cellular
Angiofibroma
RB1
RB1

• Benign mesenchymal neoplasm of the vulva and vagina
• Uncommonly may present as a penduculatedlesion
• Most grossly well-circumscribed and smaller than 5cm
Angiomyofibroblastoma




Immunohistochemistry • Positive for
Desmin, ER & PR
• Less commonly CD34 and SMA positivity
Desmin


• Synonym: “Aggressive” angiomyxoma• Low Grade, locally infiltrative myxomatous
neoplasm specific to the deep vulvovaginal, perineal and pelvic tissues
• Strong female predisposition • In men in the analogous inguinoscrotal and
perineal regions • Usually 4th decade of life with painless cystic
mass often exceeding 10cm
Deep Angiomyxoma

• Less aggressive course than initially described if completely excised with negative margins
• Potential for local destructive recurrence some times years (often decades) after initial excision• Even tumors as small as 3cm have recurred
multiple times• Grossly soft gelatinous tumor with ill-defined
margins • In recurrent cases may have more fibrous
appearance


Immunohistochemistry• Typically positive for:
• Desmin• SMA• ER/PR• Variable CD34 positivity
• Structural rearrangements of the region 12q15• ~30% of tumors, intragenic/extragenic
• HMGA2 and CDK4 IHCs positive• When positive, useful in confirming the diagnosis
and assessing margins status in a subset of cases

Reactive changes Smooth Muscle Tumor
WDL Superficial Angiomyxoma
Superficial Angiomyxoma• Can also occur in the genital region of women • Include this entity in the differential of
myxoid lesions of the distal female genital tract
• Association with Carney complex less clear with lesions in the genital area
• Typically polypoid and usually less than 5cm• Potential for local nondestructive recurrence in
~30-40% of cases



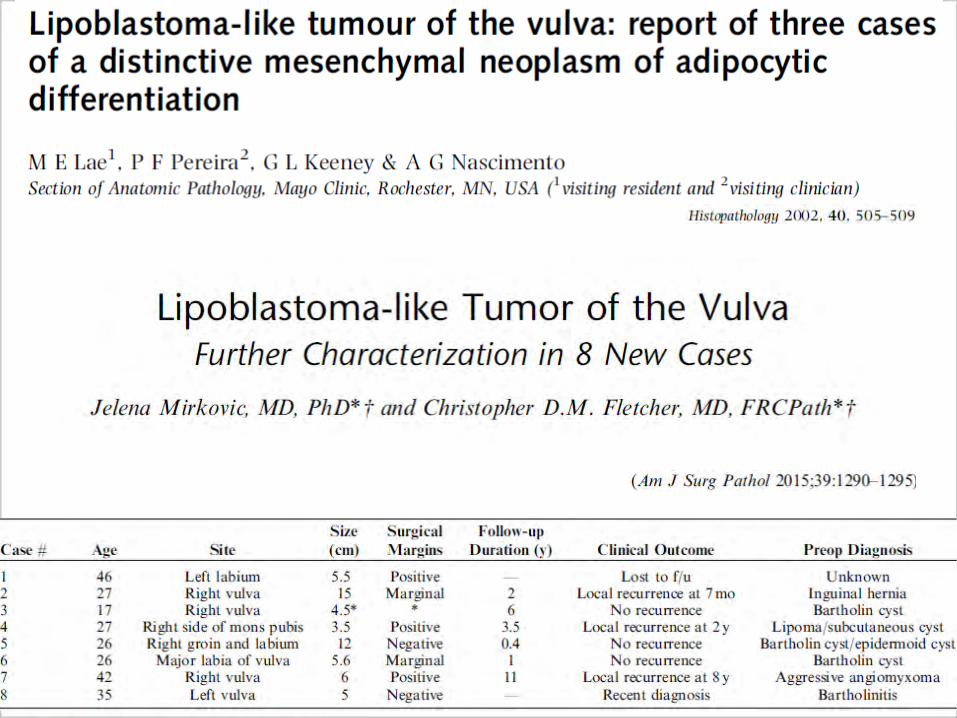
Prepubertal Vulval Fibroma
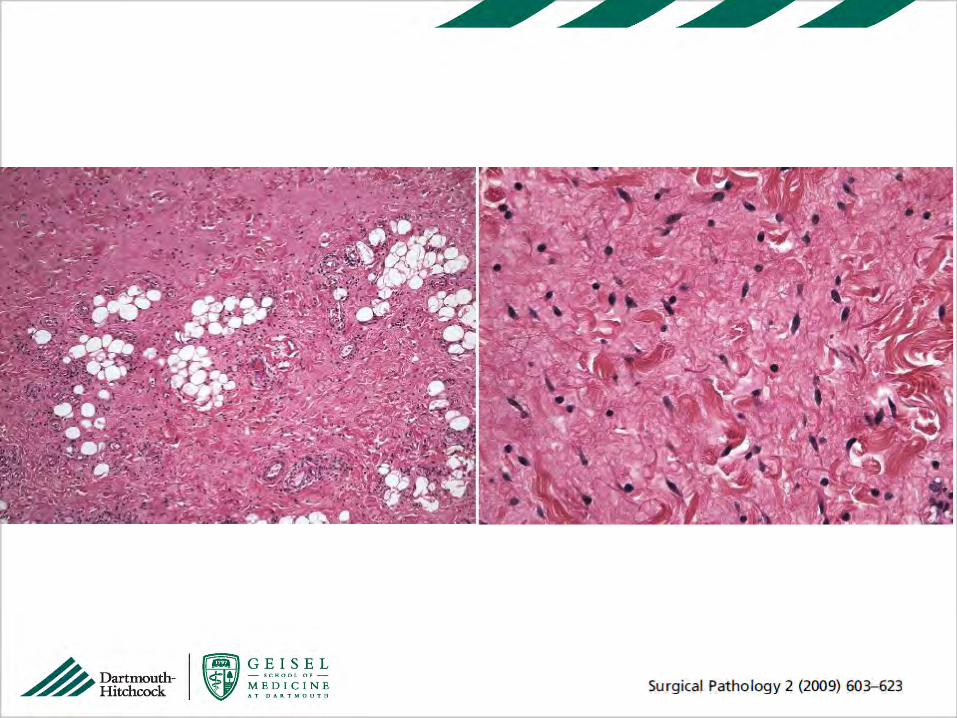

Myxoid Collagenous





Loss of RB1 by IHC
• Lack of PLAG1 and HMGA2
expression suggests it is
distinct from “true”
lipoblastomas
• Loss of Rb1 suggests possible
role of 13q chromosomal
alterations
• Possible relationship with the
Spindle cell lipoma family

Practical approach
• Correct Identification of Aggressive Angiomyxoma is critical
• If above has been excluded and definitive classification is not possible you can use label• “Benign Genital Stromal Tumor”

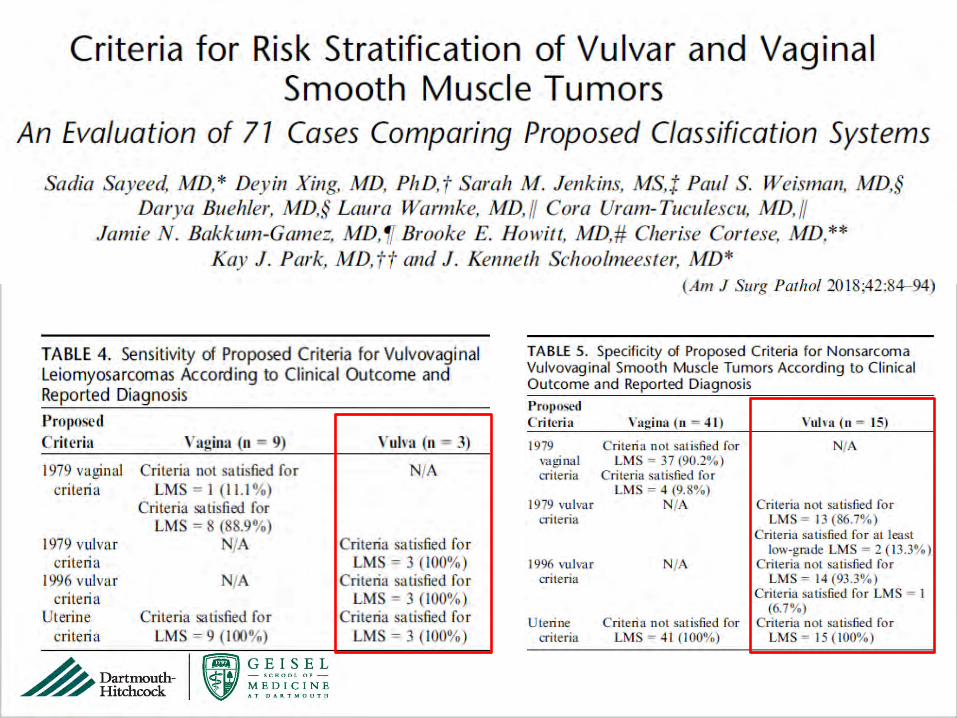
Smooth Muscle Tumors of the External Genitalia
• Smooth muscle tumors of vulva, vagina, and scrotum have similar gross and pathologic features to soft tissue and uterine counterparts
• Criteria for malignancy depend on the specific site
• Soft tissue• Superficial (including nipple)• Genital • Deep seated

Epithelioid morphology
Myxoid changes
LEIOMYOMA

LEIOMYOSARCOMA
Some combination of
• cytologic atypia,
• increased mitotic
activity
• Increased size
• infiltrative growth

Smooth Muscle Tumors of the Vulva
• Leiomyomas of the vulva is one of the more common vulvar mesenchymal neoplasms • Present in 4th to 5th decade as a small (<3cm)
mass• Mutliple leiomyomas may be manifestation of
Alport Syndrome• Hereditary disorder
• Glomerulonephritis, ocular abnormalities & hearing loss
• Mutation in COL4A3, COL4A4, COL4A5



Smooth Muscle Tumors of the Scrotum
• Uncommon and most are leiomyosarcomas• Cytologic atypia, mitotic activity and necrosis
• Rare in this location tumors with absence of atypia or mitotic activity• Extensive sample is necessary before apply the
diagnosis of leiomyoma • Note long-term clinical follow-up
• Any mitotic activity warrants classification as malignant

• Neurofibroma• S100-protein/SOX 10 +
• Solitary Fibrous Tumor• STAT6 positive
• Inflammatory Myofibroblastic Tumor• ALK + in 50-60% of cases
• Sarcomatoid Carcinoma• Diffuse cytokeratin expression• Examine for High Grade Squamous Intraepithelial
lesion or dVIN
Differential Diagnosis
