anaesthetic considerations for endovascular abdominal ... considerations for endovascular... ·...
TRANSCRIPT
ARTICLE IN PRESS
Current Anaesthesia & Critical Care (2008) 19, 150–162
0953-7112/$ - sdoi:10.1016/j.c
�Correspondfax: +44 161 27
E-mail addr
www.elsevier.com/locate/cacc
FOCUS ON: VASCULAR ANAESTHESIA
Anaesthetic considerations for endovascularabdominal aortic aneurysm repair (EVAR)
A.C. Pichela,�, F. Serracino-Inglottb
aDepartment of Anaesthesia, Manchester Royal Infirmary, Manchester M13 9WL, UKbDepartment of Vascular Surgery, Manchester Royal Infirmary, Manchester M13 9WL, UK
KEYWORDSEndovascular aorticaneurysm repair;Perioperativemanagement;Anaesthesiatechniques
ee front matter & 2008acc.2008.04.006
ing author. Tel.: +44 1616 8027.ess: adam.pichel@cmm
Summary Over the previous decade, the management of vascular disease haschanged considerably. Abdominal aortic aneurysm can now be definitively treated bymeans of endovascular stenting. Though significant short- and long-term morbidityhas been reported, this less invasive procedure is increasing in popularity and hasbeen championed by some as an alternative option for high-risk patients who mightotherwise be offered conservative management. We review the perioperativemanagement of endovascular abdominal aortic aneurysm repair (EVAR) and coverthe issues pertinent to anaesthetists.& 2008 Elsevier Ltd. All rights reserved.
Introduction
Patients who present for abdominal aortic surgeryrepresent a group carrying a high risk of significantmorbidity and mortality due to the very nature ofthe surgery and the commonly associated co-morbidities. The aetiology of aortic aneurysm ismultifactorial, and relates to the degradation ofelastin within the aortic arterial wall coupled withdisruption of collagen. This causes weakening ofthe wall and can eventually lead to rupture, due toa reduction in the tensile strength of the aorticwall. Abdominal aortic aneurysm (AAA) is a life-threatening condition and a successful outcomewill depend on many factors, including surgical and
Elsevier Ltd. All rights reserve
276 4551;
c.nhs.uk (A.C. Pichel).
anaesthetic expertise, adequate hospital infra-structure to deal effectively with complications(e.g. cardiology, critical care and renal support)and also general co-operation on perioperativemanagement between different specialties. Arecent report by NCEPOD has called for animprovement in how services in the UK aredelivered to these patients, and suggested thatperhaps centralising aortic surgery to producesmaller numbers of centres with a large volume ofaortic work may reduce poor outcome.1 Preopera-tive assessment soon after diagnosis, led by aconsultant anaesthetist with a special interest invascular surgery is considered by many to bebeneficial. It helps to reduce last minute cancella-tions on the day of surgery, unplanned admissionsto critical care and inappropriate referrals forinvestigations that will not necessarily changeperioperative management. It also allows time to
d.
ARTICLE IN PRESS
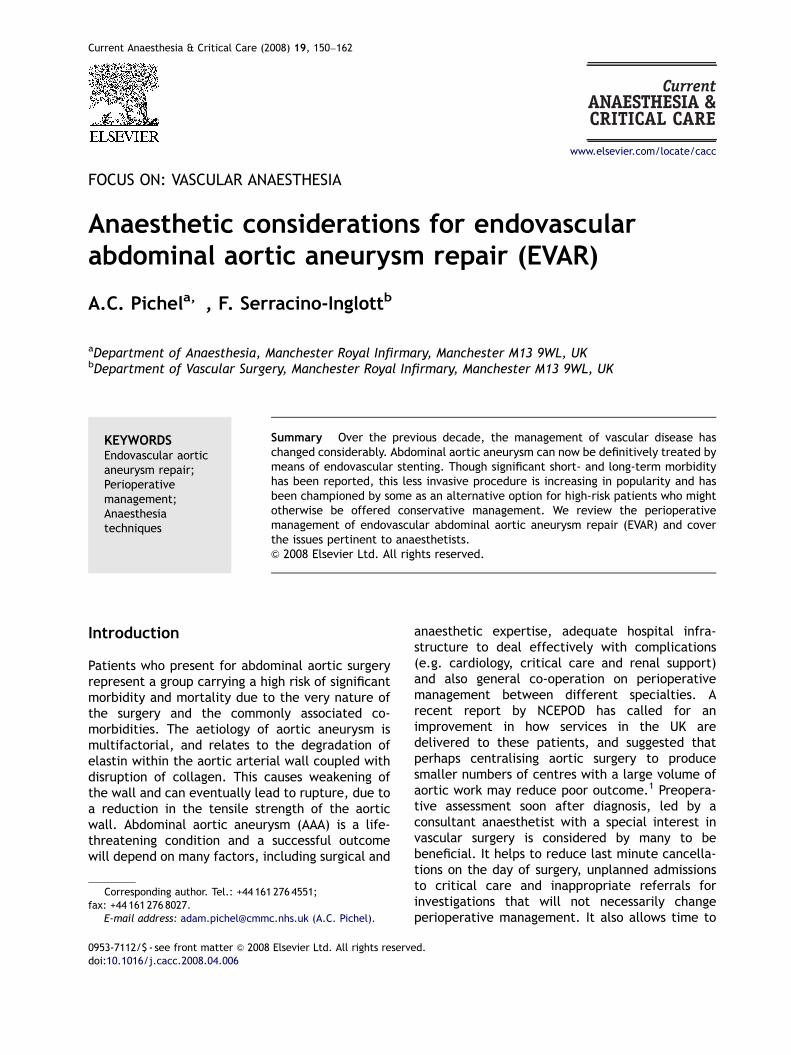
Table 1 Risk of rupture with increasing size ofaortic aneurysm.
Reproduced from Rutherford RB, Vascular Surgery, Phila-delphia, WB Saunders, 1989.
Anaesthetic considerations for EVAR 151
develop a risk profile for each patient, encouragemultidisciplinary discussion, and to plan the pa-tient’s whole package of care. Structured clinicsprovide a means of disseminating information to allclinicians caring for the patient and provide a focusfor future research and audit.
Patients who present for AAA surgery may beoffered either a conventional open repair orendovascular repair (EVAR). Once the decision tooperate has been made, the surgery should beexpedited in order to improve long-term prognosisfrom the vascular disease.1 As the size of the AAAincreases the annual risk of rupture increasesexponentially, and related complications of AAAsuch as distal limb embolisation and thrombosismay also lead to significant morbidity and mortal-ity. Abdominal aortic aneurysms are five times morecommon in men, with an incidence of 1.5% inpatients over 50 years old, the majority occurringbelow the origin of the renal arteries. Theincidence of the disease is much higher in smokersand is considered a significant risk factor.2 Thebenefit of aneurysm screening has been advocatedby many since The Multicentre Aneurysm ScreeningStudy was published in 2002.3 Indeed over the nextdecade we expect to see an increase in the numberof patients diagnosed earlier with AAA due to theproposed introduction of the national screeningprogramme in the UK of men aged between 65years.
Indications and planning for surgery
Many AAAs are discovered incidentally whilstinvestigating back pain or urinary symptoms inmiddle aged or elderly men. Routine abdominalultrasonography commonly accounts for the unex-pected detection of aortic aneurysms. Once dis-covered, the decision to operate is made afterconsideration of the size and on symptoms. Patientsare usually offered surgery once the antero-poster-ior diameter reaches approximately 5.5 cm. Afterthis, the annual risk of rupture increases to abovethe average risk of death following open repair(see Table 1). Not only this, but once aorticaneurysms reach this size they generally increasein an exponential manner, markedly increasing theannual risk of rupture.4 The 30-day mortalityassociated with ruptured AAA is widely believedto be approximately 80%; of those that reachhospital alive and undergo emergency surgery,approximately 40% will die within 30 days ofsurgery. Hence, there is a big incentive for oursurgical colleagues to offer an elective operation asearly as possible. Medical therapies that have been
shown to be of value in the reduction in the growthof AAA in animals include statins5 and tetracy-clines. However, they are not thought to beeffective in humans and surgery remains the onlyviable alternative to treatment.
Elective surgery prevents death and morbidityfrom rupture, the surgical options being eitheropen or endovascular aneurysm repair (EVAR).Open repair carries with it significant risk ofmorbidity and mortality, much of this risk isconcentrated into the perioperative period. Themortality in the in the UK for elective open infra-renal AAA repair is approximately 6.2–7.5%.1,6,7
The 30-day mortality with EVAR ranges from 1.7% inpatients deemed fit for open repair8 up to 9% inthose deemed unfit for open repair.9 Open repairutilises a large number of intensive care bed days,requires lengthy hospital stay and consumes manyother hospital resources. If the correct package ofcare is not available on the day of operation(in particular a lack of bed capacity in criticalcare) then this leads to postponement, addingfurther to the cost.
Since the early 1990s EVAR has grown inpopularity as a minimally invasive alternative. Thistechnique was pioneered by Parodi et al.10 andVolodos et al.11 In essence it is the placement of anendograft under fluoroscopic guidance to excludethe aneurysm sac. The aneurysm is accessed via thefemoral arteries and will be described in more

ARTICLE IN PRESS
A.C. Pichel, F. Serracino-Inglott152
detail below. In recent years, there have been twolarge randomised trials which have compared out-comes following EVAR with outcomes followingconventional open repair.8,12 In the EVAR 1 trial,patients who were considered fit for open repairwere randomised to either EVAR or open repair.8
Aneurysm related mortality and morbidity rateswere 3% lower compared to open. However, theEVAR1 trial demonstrated an increased need for re-intervention and the cost per case was muchgreater than open repair. Complications thatrequire re-intervention include endoleak, throm-bosis, kinking of the graft and device migration.
EVAR was initially hoped to be a viable alter-native for those thought unfit for open repair, theEVAR 2 randomised patients considered unfit foropen repair to either conservative management orEVAR. However, the results of the EVAR 2 weredisappointing in this respect. EVAR still hadconsiderable 30-day mortality (9%) and long-termsurvival was no different in each group.9 Theproblems with this trial, which have led tonumerous criticisms by authorities in the UnitedStates are the significant crossover between thetwo groups, a long delay between randomisationand treatment such that some patients in the EVARgroup actually died before their operation. Anotherconcern is that the term unfit for open repair wassubjective. However, it still remains to be seenwhether the advantages of reduced perioperativecomplications will continue to be outweighed bypoorer mid-term and long-term outcome. The allcause mortality after EVAR as compared with openrepair was similar after 4 years of follow up in theEVAR 1. Similar conclusions were drawn from themid-term results of the DREAM trial conducted inHolland.12 A recent retrospective analysis followed115 patients who were deemed to have a highperioperative risk of death for open aortic sur-gery.13 Of these, 92 entered the study and under-went EVAR providing they had favourable anatomy.The authors quoted an operative mortality of 4.3%,the survival rate at 3 years was 85% and long-termtechnical success was high (as defined by types ofendoleak). However, patients over the age of 80were considered high risk, which is at odds withmany authorities and probably based on thefindings of one study which demonstrated highermortality rates following open aortic aneurysmrepair in those over 80 years of age.14 Manyconsider physiological age and co-morbidities tobe more important considerations than chronologi-cal age alone. Indeed, commonly used cardiac riskindices such as Lee et al.’s do not consider age as asignificant independent risk factor for periopera-tive cardiac mortality and morbidity.15 Considering
only 18% of patients were classified as ASA 4, ascompared to the majority of patients who wereenrolled into EVAR 2, it would appear that thepatient population were not at all similar andhence should not be compared.
If developments in endograft technology andimaging continue to gather pace, EVAR may becomethe first choice operation for all patients with AAA.
Surgical conduct of EVAR (see Figures 1–3)
EVAR involves the use of a stent-graft to excludeaneurysms of the abdominal aorta. A stent-graft isa self-expandable stent, similar to that used whentreating occlusive vessel disease, with an outer(endo-skeleton) or inner (exo-skeleton) lining offabric. This fabric is either Dacron or polytetra-fluorethylene (PTFE), very similar to the graft usedfor open aneurysm repair. The stent-graft ispositioned between normal artery proximal to theaneurysm and normal artery distal to the aneurysm,such that blood flows from normal artery throughthe stent-graft and back into normal artery. Theremaining blood in the aneurysm sac will thus clotoff and the aneurismal sac should remain static orshrink with time. The area where the stent-graft isin contact with normal artery is known as thesealing zone. The outward radial force of the stentis what causes a seal in this area preventing theflow of blood outside the stent-graft and intothe aneurismal sac. The proximal sealing zone isthe non-aneurysmal infra-renal aortic neck. Sincealmost all AAAs extend to the aortic bifurcation orbeyond, the distal sealing zone is both commoniliac arteries for purely aortic aneurysms and theexternal iliac arteries for aorto-iliac aneurysms. Allcurrent devices for elective cases are therefore of abifurcated (trouser) configuration.
When considering the endovascular managementof infra-renal AAAs a proximal and distal landing(or sealing zone) of 1.5 cm is recommended. Ashorter landing zone will result in the radial forceof the sealing stent being exerted over a reducedarea and therefore a greater risk that, with time,the stent will migrate distally with loss of the sealbetween normal artery and stent. In an attempt toprevent distal migration most current stent-graftshave a bare suprarenal component, i.e. the mostproximal stent is not covered by graft so that it canbe positioned above the renal arteries, therebyincreasing the surface area over which thestents radial force is applied. There is now goodevidence that having bare metal stents across therenal orifices does not effect renal perfusion andfunction. The stent-graft most commonly used in
ARTICLE IN PRESS
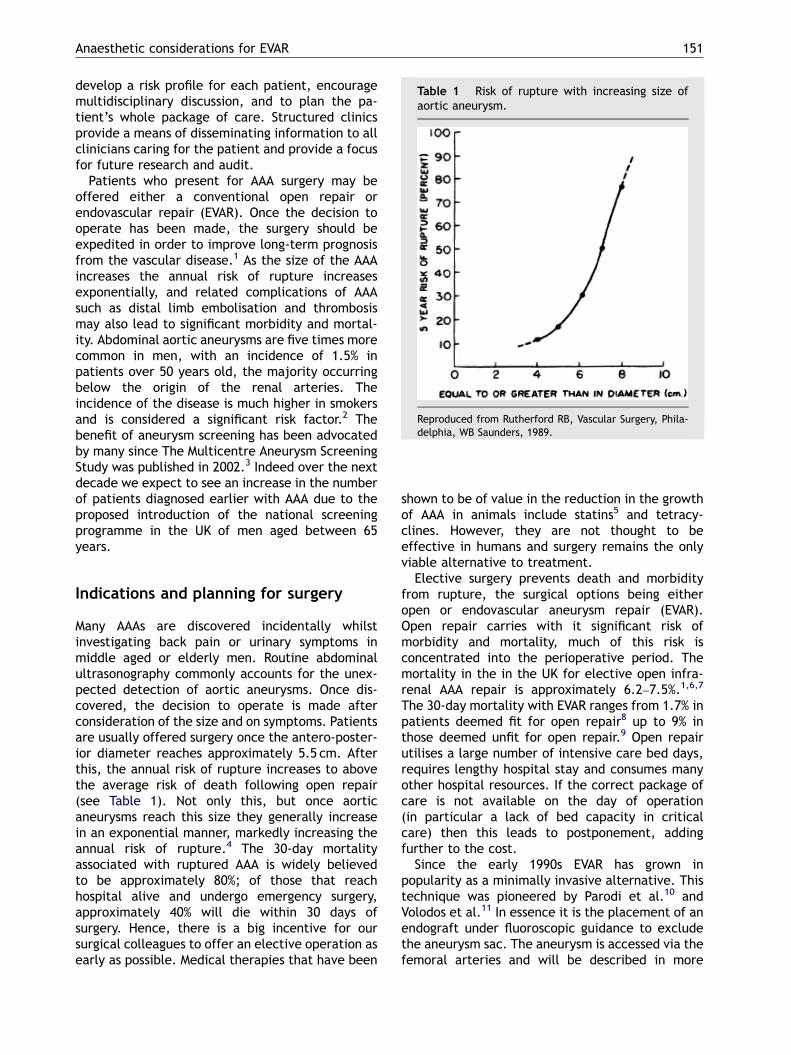
Figure 1 Abdominal aortic aneurysm imaging: (a) pre-operative CT-angiogram and (b) intraoperative angiogramprior to insertion of stent-graft.
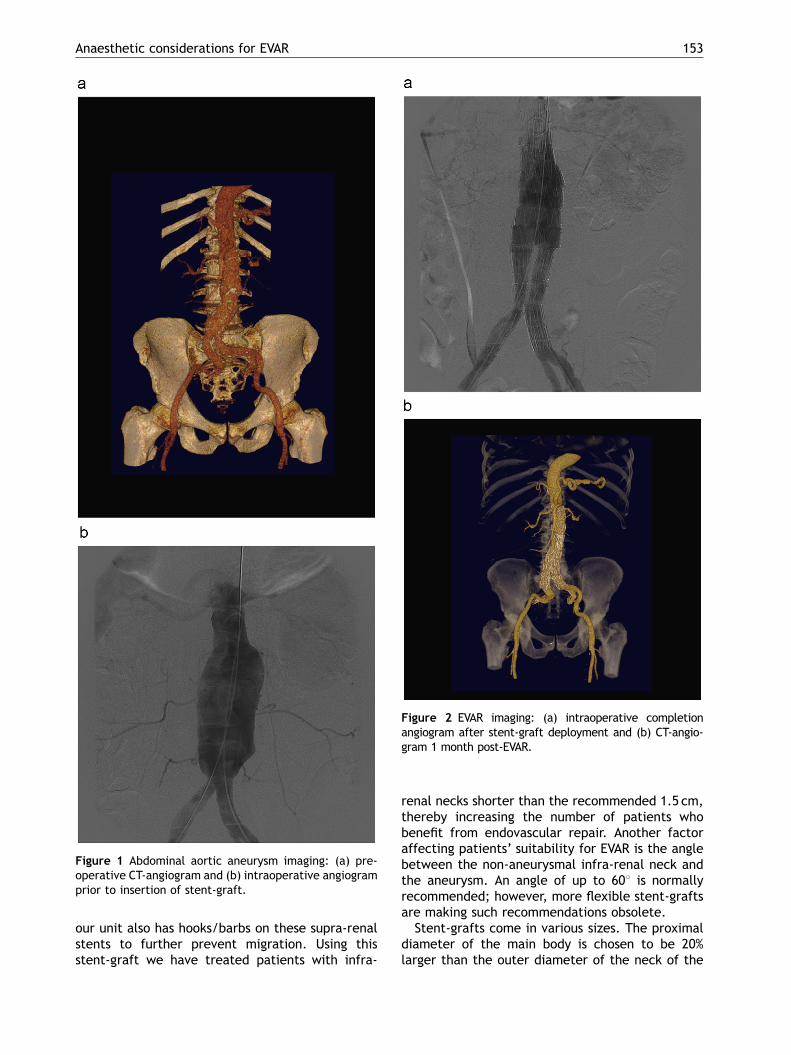
Figure 2 EVAR imaging: (a) intraoperative completionangiogram after stent-graft deployment and (b) CT-angio-gram 1 month post-EVAR.
Anaesthetic considerations for EVAR 153
our unit also has hooks/barbs on these supra-renalstents to further prevent migration. Using thisstent-graft we have treated patients with infra-
renal necks shorter than the recommended 1.5 cm,thereby increasing the number of patients whobenefit from endovascular repair. Another factoraffecting patients’ suitability for EVAR is the anglebetween the non-aneurysmal infra-renal neck andthe aneurysm. An angle of up to 601 is normallyrecommended; however, more flexible stent-graftsare making such recommendations obsolete.
Stent-grafts come in various sizes. The proximaldiameter of the main body is chosen to be 20%larger than the outer diameter of the neck of the

ARTICLE IN PRESS
Figure 3 Illustration of how a stent-graft would appearwhen deployed in the aorto-iliac vessels. Reproducedwith kind permission from COOK Medical.
A.C. Pichel, F. Serracino-Inglott154
aneurysm. The distal diameter of the iliac limbs ischosen to be 10% larger than the outer diameter ofthe iliac vessels. The length of the main body andlimbs depends on the type of stent-graft used, butin most cases is dependent on the distance from thelowermost renal artery to the aortic bifurcationand the internal iliac artery origins.
Stent-grafts are packed (compressed) in an outersheath (tube) with a pusher rod at their distal end.When the sheath is withdrawn backwards over thepusher rod, the stent-graft is exposed and opens asa result of the radial force of the self-expandingstent. Most current stent-grafts are trimodular(main body for the aorta and two limbs for eachiliac artery) or bimodular (main body and limb forone iliac as one component and contralateral iliaclimb as the second component). The sheathcontaining the stent-grafts measures 18–22 Fr forthe main body and 14–16 Fr for the iliac limbs. Thestent-grafts are usually introduced through thecommon femoral arteries. Most surgeons will per-form a surgical cut-down onto the vessels due tothe size of the sheaths. Closure devices such asPerclose and Sutura are used in some centres wherea totally percutaneous procedure is performed. Therisk of groin complications is however significant
with these closure devices and we personallyperform a cut-down in both groins using transverseskin crease incisions. We prefer these to long-itudinal incisions since they affect less dermatomesand therefore are associated with less postopera-tive discomfort. We only use longitudinal incisionsif additional procedures such as a femoral crossovergraft or an endarterectomy may be required. Thereare occasions where the iliac arteries may be toosmall to safely advance the sheathed stent-graftwithout damaging these vessels (the main devicerequires an iliac diameter of 7–8mm). In such asituation, one may expose the iliac artery and use aDacron conduit anastamosed to this vessel tointroduce the stent-graft.
Once the common femoral arteries are exposed,a J-wire (similar to that used to introduce a centralvenous line, but much longer) is introduced throughan arterial puncture needle. Under fluoroscopicguidance, the J-wire is advanced proximally to thedescending thoracic aorta. In the case of verytortuous or diseased arteries, the J-wire is swappedfor a hydrophilic (Teruma) wire. Various shapedcatheters are then used to guide this wireproximally. On the side through which the mainbody is to be introduced, the J-wire is exchanged(through a catheter such as a RIM or COBRA) for avery stiff wire (Lunderquist or Mayer wire). Such astiff wire will straighten the vessels making iteasier to advance the device and will also not kink.On the contralateral side, a PIG-TAIL catheter isadvanced over the J-wire and then connected to apower injector such that contrast can be injectedvery rapidly and at high pressures, opacifying theabdominal aorta and its visceral branches. If thepatient is under a general anaesthetic, the anaes-thetist will be asked to suspend respiration when-ever digital subtraction angiography is performed.This is because if there is even the slightestmovement, the X-ray image with contrast will beslightly different from that without contrast, andwhen the latter image is subtracted from theformer, a very blurred picture would result. Thepig is positioned just above the level of the renalorifices as may be determined from the CT-angiograms. The stent-graft is then introducedover the stiff wire and positioned such that thejunction between covered and uncovered stent isjust below the lowermost renal orifice. This areausually has gold-markers stitched to it so that it iseasily identifiable on fluoroscopy. A digital subtrac-tion angiogram is obtained to confirm correctpositioning of the stent-graft in relation to therenal orifices. The stent-graft is moved up anddown as required and further digital subtractionangiograms obtained until one is definitely satisfied
ARTICLE IN PRESS
Anaesthetic considerations for EVAR 155
with the position. When this is the case, the stent-graft is deployed under fluoroscopic control bywithdrawing the outer sheath distally whilst fixingthe position of the pusher rod. The next step is tocannulate the contralateral limb of the main bodyfrom the contralateral common femoral artery. Thisis achieved by using a hydrophilic wire andcatheters of varying shape. This part of theprocedure may sometimes be very fiddly and isthe main factor affecting the duration of theprocedure. Once the contralateral limb is cannu-lated, the hydrophilic wire is swapped for a stiffwire and the contralateral limb stent-graft isinserted and deployed such that its distal edge isjust above the origin of the internal iliac artery.Depending on the type of stent-graft being used anipsilateral limb stent-graft may also be required.Some stent-graft manufacturers recommend that amoulding (semi-compliant) balloon is blown up atall the sealing zones (including the aortic neck) tofurther fix the stents in place. One of the stiff wiresis then swapped for a pigtail and a final digitalsubtraction angiogram obtained to confirm that thestent-graft has been deployed in the correctposition with preservation of both renal andinternal iliac arteries and that there is no fillingof the aneurysm sac. If this is satisfactory, allsheaths, catheters and wires are withdrawn.Vascular clamps are applied proximal and distal tothe arteriotomy resulting from insertion of thestent-grafts. The arteriotomies are closed with afine prolene suture.
As may be seen from above, the main limitationsto perform EVAR are the absence of a proximallanding zone (short or wide neck), and poor access,i.e. the iliac vessels are smaller than 8mm indiameter (to allow a 22 Fr device to be advancedsafely). The absence of a distal landing zone meansthe presence of common iliac aneurysms. This isusually resolved by embolising (putting metalliccoils) in the internal iliac arteries to prevent backbleeding from this vessel into the aneurysm sac andusing the external iliac artery as the distal landing(sealing) zone. Embolising the internal iliac carriesa small risk of buttock claudication, impotence andpelvic ischaemia. In order to prevent such compli-cations, iliac limbs with side branches to perfusethe internal iliac artery are used in our unit. Theuse of such devices requires advanced endovascularskills, significantly lengthens the procedure andmay require higher doses of contrast. The absenceof a proximal landing zone may be resolved by usingcustom made fenestrated devices. These devicesare designed specifically for the individual patientsuch that small holes (fenestrations) are pre-cutinto the graft based on the CT-reconstructions to
correspond with the openings of the appropriaterelevant vessels. The gap between these fenestra-tions and their target vessels is bridged usingcovered stents similar to the bare stents used fortreating renal artery stenosis. Such procedures arevery complex and lengthy. Depending on thenumber of fenestrations, they can take severalhours. High doses of contrast may be required.Since the visceral vessel origins are usually around6mm in diameter there is no room for error and ifthe stent-graft is not deployed in the correctposition the patient could infarct a kidney ordevelop ischaemic bowel.
Preoperative considerations
These patients require careful preoperative assess-ment and present major challenges to the vascularteam, the anaesthetist and critical care. Patientsare usually elderly, have limited cardio-respiratoryreserve and have a high prevalence of coronaryartery disease. Anaesthetists may find themselvesworking with a surgical team that is early on in theendovascular experience and may be asked to workin the radiology department, which in itself maycause logistical difficulties. This may result inincrease in the duration of EVAR, more likelihoodof conversion and increased blood loss thanoriginally anticipated at preoperative assess-ment.16 A gradual continuous loss of blood fromaround the introducer site can lead to significantblood loss over the course of the procedure andmay be easily missed. The average volume of bloodlost during EVAR is approximately 400mL comparedto 800mL with open repair.17 It is important thatwherever EVAR is performed, the specifications ofthe facilities used are adequate to manage conver-sion to open repair in an emergency. The samestandards apply to the personnel involved. There iswidespread variation across the UK with regard tothe location, some prefer to use a vascular theatrewhilst others have used the radiology departmentfrom the start. Clearly depending upon localfacilities and geography the issues vary. Theportable imaging equipment in operating theatresprovides poorer quality images compared to thosethat can be obtained in radiology departments,though this is acceptable for most cases. Theexceptions are obese patients (difficult imaging)and complex fenestrated devices that requirehigher imaging specification to complete theprocedure to a high standard. The ideal scenariowould be to have a custom built vascular imagingtheatre, which for many hospitals is prohibitivelyexpensive. A cheaper alternative is to develop

ARTICLE IN PRESS
A.C. Pichel, F. Serracino-Inglott156
existing radiology suites to the same specificationstandard as a theatre, preferably located near acritical care unit and theatre recovery.
Cardiac
Cardiac complication still accounts for much of thesignificant morbidity and mortality following EVAR.The risk stratification and risk-modification strate-gies that may prove useful have been discussed indetail in the accompanying manuscripts and willnot be discussed in great detail here. Broadlyspeaking the goal is to evaluate the current medicalco-morbidities and in the context of the proposedsurgery to consider further investigations that maychange management. This will help provide aclinical risk profile for the patient and clinicalteam and will hopefully inform the whole perio-perative process. This is achieved by taking acareful history and performing a thorough physicalexamination, followed by routine laboratory inves-tigations. Of particular importance is to considerthe functional capacity of the patient which can beassessed subjectively using the Duke Activity StatusIndex.18 However, more objective measures ofcardiopulmonary fitness can be obtained fromcardiopulmonary exercise testing. This should becombined with a risk assessment specific to thesurgery planned and use a clinical risk index such asLee’s Revised Cardiac Risk Index15 to identify thosepatients at greatest risk of a perioperative cardiacevent. Guidelines from the American Collegeof Cardiology and American Heart Association(ACC/AHA) are a useful reference point for thecardiac evaluation of AAA patients, and anaesthe-tists should be familiar with their recommenda-tions.19 In terms of surgery specific risk; theACC/AHA place EVAR in the intermediate riskcategory for cardiac complications. In general EVARhas many advantages that make it a very attractiveoption (Table 2). It is as yet unclear as to whether
Table 2 Advantages of EVAR over open AAArepair.
Advantages of EVAR over open repair
Minimally invasiveReduced blood lossReduced stress responseNo cross clampImmediate 30-day survival advantageEarlier ambulationShorter hospital stayReduced need for intensive care facilities
the same preoperative assessment should accom-pany those intended for EVAR compared with thoselisted for open repair. The authors currently feelthat whilst EVAR is still a relatively new procedureand because there is the possibility of having toconvert to open repair, an identical assessmentshould take place. Not only that, the patientpopulation is the same, they have the samepathology and many centres will offer EVAR topatients who are considered ‘‘unfit’’ for openrepair. A significant number of patients do not havemany years left to live, and repairing their aorticaneurysm may hasten their death. Risk stratifica-tion using CPET may give clinicians more confidenceto balance the risk versus benefit of EVAR and helpinform the consent process.
Respiratory
Anaesthetists should make an assessment of theseverity of respiratory disease present, exclude anactive respiratory infection and ensure that opti-mal medical therapy is in place. A concise review ofthe patients’ recent oral steroid usage and previousneed for non-invasive ventilation may prove helpfulin planning which type of EVAR procedure isundertaken. There are variations from ‘‘standardEVAR’’ (e.g. use of an iliac bifurcation device) thatmay confer some ‘‘vascular’’ advantage but mayput the patient at more risk owing to an increase inthe length of the procedure, the use of greatervolumes of intravenous contrast and also the needfor general anaesthesia. For those with smokingrelated lung disease, the practice of using smallgroin incisions, use of regional or local anaesthesiaand early ambulation are likely to reduce the risk ofpulmonary basal atelectasis and respiratory infec-tions. Though respiratory failure is not as commonafter EVAR, a significant number of patients stillsuffer postoperative respiratory complications(10.9% after open repair versus 2.9% after EVAR).12
Many patients undergo EVAR using regional anaes-thesia, but complex EVAR usually requires generalanaesthesia because patients may become restlessand agitated if required to lie still for many hoursand because of increased risk of blood loss andassociated coagulopathy.
Prediction of postoperative respiratory complica-tions in specific patients is difficult in minimallyinvasive techniques due to their relatively lowincidence. Forced spirometry (with reversibilitiesfor the effects of bronchodilators if appropriate) toconfirm a particular diagnosis and assess severity iscommonplace, but as yet no single investigationlends itself to predict respiratory complications in

ARTICLE IN PRESS
Table 3 Clinical risk factors associated withcontrast-induced nephropathy.
Chronic renal impairmentDiabetes MellitusPerioperative dehydrationVolume of contrast usedAdvanced agePerioperative use of other nephrotoxic drugs(including those who have been given contrast
Anaesthetic considerations for EVAR 157
EVAR. As a general rule, it is desirable to convertthose on short acting beta agonists to longer actingagents in the perioperative period so as to minimisethe potential side effects related to the withdrawalof shorter acting agents. Other adjuncts availablethat are considered by many to be helpful inreducing the incidence of significant pulmonarycomplications are chest physiotherapy, incentivespirometry and early ambulation.
within the last 10 days)
Renal
The prevalence of chronic renal impairment variesbetween 3% and 20% of patients undergoing thistype of surgery.20,21 These patients are more likelyto suffer a clinically significant renal insult becausethey have a reduced safety margin.22 Chronic renalimpairment is associated with long-standing hyper-tension, diabetes mellitus, atherosclerosis andrenal artery stenosis and may also be related tothe close proximity of the aneurysm. Contrast-induced nephropathy (CIN) is a potential complica-tion following EVAR and has been defined as anabsolute increase in serum creatinine of 44 mmol/Lor a relative increase of 25% from baseline,provided other causes of renal dysfunction areexcluded.23,24 The contrast media available are alltri-iodinated benzene derivatives, varying only intheir degree of ionisation and osmolarity. Neweragents with no ionicity, lower osmolarity and beingwater soluble are associated with a lower incidenceof CIN in high-risk patients.25 Part of the difficultyin defining the problem lies in the definition of‘‘significant renal damage’’, the spectrum rangesfrom a minor decrease in creatinine clearance insome studies, which is barely detectable withroutine blood testing to those who go on to requirerenal replacement therapy. Though serum creati-nine is useful and easy to measure reference point,it is more helpful to use estimated GFR to identifythose patients with modest reductions in theirrenal function (despite normal serum creatininelevels). Anaesthetists need to consider whether aclinically significant renal insult is likely and also tolook at strategies to reduce this risk. Risk factorsassociated with the development of CIN are listedin Table 3. The degree of pre-existing renalimpairment is an important factor in affectingnumerous outcome measures. Patients with abaseline creatinine greater than 2.5mg/dL appearto have a higher incidence of perioperativemortality, length of ITU stay, incidence of post-operative renal and cardiac failure compared withthose with normal preoperative values.26 Strategiesto reduce CIN include: generous perioperative
intravenous fluid administration,27 minimal use ofcontrast, increasing the interval between contrastCT angiography and EVAR (to spread the cumulativerenal insult over a longer period) and perhaps toconsider less complex procedures in those withsignificant renal impairment (e.g. creatinine great-er than 2.5mg/dL). Adequate hydration withintravenous fluids prior to radiological procedureappears to confer considerable benefit.28 Thepostoperative use of antiplatelets should be con-sidered in relation to chronic renal impairment too.
There has been much interest in the use ofprophylactic antioxidants to prevent CIN, in parti-cular N-acetylcysteine. Some meta-analyses29 havesuggested a benefit but individual studies lookingspecifically at its use in EVAR have not demon-strated this effect.30
Anaesthesia techniques
General considerations
Any anaesthetic should be tailored to patient andsurgical factors, and options with EVAR are numer-ous. Early attempts at EVAR were lengthy proce-dures involving teams who were unfamiliar with thetechnique, and the incidence of perioperativesurgical complications was greater, which tendedto favour the use of general anaesthesia. In theearly days of thoracic EVAR, surgeons oftenrequested cardiac standstill at the point of stentdeployment which also favoured general anaesthe-sia, but this practice is now no longer thought to benecessary.
Although conversion to open repair rates are low(less than 2%) the anaesthetist needs to beprepared for open repair and massive haemor-rhage.31 The bare minimum of general manage-ment should include the use of two large-boreintravenous cannulae, invasive arterial monitoring,a urinary catheter and immediate access to arapid infusion device. Regular intraoperative and

ARTICLE IN PRESS
A.C. Pichel, F. Serracino-Inglott158
postoperative measurements of haematocrit, hae-moglobin blood gas exchange and clotting para-meters are easily done from an arterial pressureline. It is also more comfortable for awake patientsin theatre not to be subjected to very frequentnon-invasive blood pressure measurementsthroughout the duration of the procedure. Patientsare cross matched for the same as for open repair(usually six units of packed red cells). The use offorced air warming devices and intravenous fluidwarmers is strongly recommended as duration caneasily exceed 3 h and large volumes of fluidoccasionally need to be administered.
There is wide variation amongst anaesthetistswith regards to the preferred method of monitoringintravascular volume and cardiac output in thosepatients with moderate cardiac and/or renal fail-ure. The use of a central venous catheter,pulmonary artery catheter, oesophageal Doppleror pulse contour analysis may be beneficial inguiding meticulous fluid balance in these patientsundergoing EVAR. However, whether or not thesepractices will reduce cardiac or renal complicationsfollowing EVAR is not currently known. For the vastmajority of patients, central venous access (with itsattendant risks) is an unnecessary procedure andshould be limited to those with cardiac/renalfailure and to those in whom larger fluid shifts orblood loss is anticipated or where complex proce-dures are planned (e.g. fenestrated stents).
When considering regional anaesthesia, thoughtmust be given to the concomitant perioperative useof anticoagulants and dual antiplatelet agents.Most patients are given approximately 100 IU/kgof unfractionated heparin before stent deploy-ment, and most are on at least one antiplateletdrug therapy. There is debate over the optimaltiming of regional anaesthesia in patients who areprescribed clopidogrel alone, or in combinationwith aspirin. If regional anaesthesia is the preferredchoice, the only sensible recommendation in thoseundergoing elective EVAR is to stop clopidogrel atleast 7–10 days prior to surgery (as per themanufacturers’ recommendations). This is providedthat the patient has not had a drug eluting coronarystent inserted within the last 18 months. Cessationof clopidogrel in these circumstances can precipi-tate fatal perioperative in-stent thrombisis.32
In some more complex cases, the vascular teammay wish to start clopidogrel as soon as possibleafter EVAR due to concerns over side branchperfusion. However, it is necessary to remove anindwelling epidural catheter before starting clopi-dogrel. This also needs to be timed with theintraoperative use of unfractionated heparin. It isour practice not to give heparin earlier than an
hour after the insertion of an epidural and thecatheter is removed at least 4 h after the last dose.The clotting profile is also checked and theactivated partial tissue thrombolastin time mustbe less than 1.5 times the normal range beforeremoval. Clopidogrel is then administered 1 h afterthe removal of the epidural catheter. Followingprophylactic doses of low molecular weight hepar-ins (LMWH), most authorities agree that insertion ofa neuraxial block is safe after 12 h have elapsed,and that LMWH should not be given until 4 h haveelapsed from the insertion of a neuraxial block.These times increase to 24 h following the admin-istration of treatment doses of LMWH.
The pain experienced by patients after two smallgroin incisions is mild and we do not continue theepidural infusion outside of the theatre. Mostpatients manage pain adequately with paracetamoland codeine phosphate. The patient mobilisesfaster and cardiovascular stability is better pre-served. This practice may have the added advan-tage of allowing earlier detection of lower limbischaemia (of which pain is a presenting symptom).Although it is not used, the epidural catheter is notactually removed, but left in situ for 12 h, hence ifthere are postoperative complications that neces-sitate the patient returning to theatre for emer-gency surgery it can be used again (e.g. for limbischaemia).
General versus regional or localanaesthesia
As experience in EVAR has increased, the use ofregional/local anaesthesia has also increased.There are variations in EVAR such as the use ofiliac bifurcated devices or fenestrated endograftsand/or concomitant open surgery (e.g. femoro–
femoro crossover graft) that increase the durationand complexity of the procedure, favouring the useof general anaesthesia. Many patients cannottolerate lying still for more than 3 h and developa tendency to become restless which can beincompatible with the latter half of the procedurewhere a certain amount of patient co-operation isrequired (e.g. breath holding).
There is growing evidence that the use ofregional or local anaesthesia may confer a reduc-tion in postoperative complications in patientsundergoing EVAR.33 The EUROSTAR data base wasanalysed by this group, who looked at 5557 patientswho had undergone EVAR from numerous centresacross Europe. They looked at many variables andoutcomes including: duration of stay, admission toICU, pulmonary, renal and cardiac complications.

ARTICLE IN PRESS
Anaesthetic considerations for EVAR 159
They concluded that cardiac complications weresignificantly reduced in those patients who hadlocal or regional anaesthesia. Not only this, butthat duration of stay in ITU and duration of hospitallength of stay were reduced too. However, it shouldbe noted that the local anaesthesia group onlyrepresented 6% of all the cases analysed, and mostof those were from the same tertiary centre.
Those who are able to tolerate EVAR under LA aregenerally a highly selected group; usually withmore favourable arterial access, undergoing noadditional procedures and are less likely to beoverweight (making surgical access straightfor-ward). Unfortunately many patients do not reachthese criteria. However in this paper by Ruppertet al., regional anaesthesia (combined spinaland/or epidural) also seemed to be associated witha better complication profile than GA. Approxi-mately 25% of patients analysed had undergoneregional anaesthesia and represented a group moresimilar to those that underwent general anaesthe-sia. They demonstrated a statistically significantreduction in cardiac mortality of 2.9%, compared tothose under GA who had a rate of 3.7%, but did notreport a reduction in pulmonary or renal morbidityunlike other studies such as that by Verhoevenet al.34 This prospective non-randomised studyfollowed 239 patients undergoing EVAR in onehospital. Local anaesthesia infiltration was used asthe standard technique; again regional or generalanaesthesia was reserved for those who wereoverweight, had difficult surgical access or requiredadditional surgical procedure. There was no statis-tically significant difference between the differentanaesthesia groups in relation to perioperativemortality. They did however, show fewer renaland respiratory complications in those who hadlocal anaesthesia. This is most likely because of thelower risk profile of this group, and it is unwise todraw strong conclusions from this study due to thefact it was non-randomised, was subject tosignificant patient selection bias and because thehigher risk patients received different types ofanaesthetics. Other studies have concluded thatthe risk profile of the patient appears to be moreimportant than the influence of any given anaes-thetic technique.35 The ACC/AHA do not advocate aspecific mode of anaesthesia for patients withcardiac disease as the evidence base has not beensubstantiated.19 This re-iterates the great impor-tance placed upon preoperative risk stratificationin vascular patients.
In a retrospective analysis by Bettex et al.36
different modes of anaesthesia were compared in91 patients listed for infra-renal aortic aneurysmrepair with EVAR. They compared local infiltration
with epidural and general anaesthesia. As onemight expect, more fluid was given in the regionaland GA groups, and they demonstrated a largedifference in the eventual postoperative destina-tion of patients according to which type ofanaesthesia was used. Whereas 70% of patientswent to ITU in the GA group, only 27% of thoseoperated on under LA were admitted to ITU withthe regional group being approximately 50%(po0.01). The length of stay in hospital was alsosignificantly less in the LA group (3 days versus 5.5days in the GA group, po0.01).
All these studies report that EVAR under regionalor local anaesthesia is feasible and effective, andnone appears to show worse outcomes. However,no definitive evidence exists that they are superiortechniques over general anaesthesia. The evidencesupporting the use of regional or general anaes-thesia for EVAR is lacking, most studies on thissubject are descriptive in nature and should beinterpreted with caution.33–36 The choice of anaes-thesia will inevitably be tailored to the individualcase. It is also worth bearing in mind that thetechnical success of EVAR does not appear to berelated to the mode of anaesthesia.13,33–36
Postoperative management andcomplications
The complications following EVAR can be of suchmagnitude (see Table 4) that close postoperativesurveillance is crucial. Currently in the UK, it seemsthat most go to a level 2 critical care area, but willdepend upon local facilities and guidelines. We donot start EVAR without the availability of an HDUbed, though some of our patients are discharged tothe vascular ward, provided that certain clinicalcriteria are met as follows: preoperatively thepatient is stratified into low risk on the grounds ofclinical co-morbidities, the procedure plannedis standard EVAR on an infra-renal aortic aneurysm,the procedure (including anaesthesia) wassmoothly executed with no apparent immediatecomplications and the patient is cardiovascularlystable and passing urine in recovery. For the restwho go to HDU, continued invasive blood pressuremonitoring allows regular measurement of gasexchange, haemoglobin, haematocrit, serum elec-trolytes and clotting parameters. Regular lowerlimb arterial assessment both clinically and withDoppler is essential.
Patients are usually eating and drinking on thesame day; however, continued intravenous fluidtherapy is encouraged to reduce the likelihoodof CIN.

ARTICLE IN PRESS
Table 4 Surgical and medical complications ofEVAR.
Surgical Medical
Maldeployment,malpositioning of graft
Acute coronarysyndromes
Stent-graft limb thrombosisleading to lower limbischaemia (usually occurs infirst 24 h). If a patient is athigh risk for such acomplication (e.g. totousiliacs) leave epidural inplace for 424 h to facilitatereturn to theatre forthrombectomy
Acute congestivecardiac failure
Graft migration (unusualwith new stent-grafts thathave a suprarenal bare stentwith hooks)
Acute renalfailure/contrast-inducednephropathy
Type 1 endoleak—failure ofthe stent graft to seal at theproximal and distal landingzones
Arrhythmia
Type 2 endoleak—backbleeding from the lumbarvessels or inferiormesenteric arteries
Respiratoryinfection
Type 3endoleak—dislocation ofthe limbs from the mainbody or a tear in the fabric
Venousthromboembolism
Type 4 endoleak—porosityand endotension
Cerebrovascularaccident
Rupture of iliac artery(commoner in women whohave smaller arteries thanmen; may result in sudden,refractory hypotension)
Postimplantationsyndrome
Distal and renalembolisation leading totrash foot and renalinfarction,respectively(uncommon)
Graft infection (very rare)
Paralysis (extremely rare inpatients with infra-renalAAA)
A.C. Pichel, F. Serracino-Inglott160
A common though often relatively benign com-plication noted after EVAR is postimplantationsyndrome. The clinical characteristics of whichinclude pyrexia, leukocytosis and elevated inflam-
matory markers.37 Clinically it appears similar tosepsis, but without the presence of infection.Serious life-threatening complications such asmulti-organ failure and coagulopathy may occurbut are rare.38 Exclusion of larger aneurysms withendografts may result in significant fibrinolysissecondary to thrombus generated within theaneurysm sac leading to a state of coagulopathy.However, the majority of cases of postimplantationsyndrome are self-limiting and usually settle within2 weeks of surgery. It is important to exclude aninfectious cause, and symptomatic managementwith antipyretics and intravenous fluids is all that isusually necessary. Otherwise most patients aredischarged within 4 days of surgery.
Conclusion
Although the benefits to short-term morbidity andmortality are accepted, the long-term complica-tion rates make the decision to undertake EVAR inhigh-risk patients with limited life expectancy verydifficult, and can only be done on an individualbasis. Randomised trials focusing on the benefits ofEVAR in higher risk patients need to be conductednow that experience with the technique hasincreased significantly.
Future developments in endovascular surgery aregathering pace, as are the indications and treat-ment possibilities. Treatment of ruptured aorticaneurysms under local infiltration is being prac-ticed in some UK centres, including our own. Thecomplex type 4 thoraco-abdominal aortic aneurysmcan also be stented with custom made endografts.These procedures are exciting developments thatwill continue to challenge anaesthetists in theyears ahead. As the range of patients beingconsidered for EVAR continues to widen, includingthose who were assessed previously unfit for opensurgery, the anaesthetist must continue to beintegral in their preoperative assessment in orderto impact upon outcome.
Acknowledgement
The authors would like to thank Dr. F. Farquharson,Consultant Vascular Radiologist, Manchester RoyalInfirmary, for the CTangiogram images of a pre- andpost-EVAR abdominal aortic aneurysm.
References
1. NCEPOD 2005. Abdominal aortic aneurysm: a service in needof surgery?
ARTICLE IN PRESS
Anaesthetic considerations for EVAR 161
2. Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN,Bandyk D, et al. Prevalence and associations of abdominalaortic aneurysm detected through screening. AneurysmDetection and Management (ADAM) Veterans Affairs Coop-erative Study Group. Ann Intern Med 1997;126(6):441–9.
3. Ashton HA, Buxton MJ, Day NE, Kim LG, Marteau TM, ScottRA, et al. The Multicentre Aneurysm Screening Study (MASS)into the effect of abdominal aortic aneurysm screening onmortality in men: a randomised controlled trial. Lancet2002;360(9345):1531–9.
4. Lederle FA, Johnson GR, Wilson SE, Ballard DJ, Jordan Jr.WD, Blebea J, et al. Rupture rate of large abdominal aorticaneurysms in patients refusing or unfit for elective repair.JAMA 2002;287(22):2968–72.
5. Steinmetz EF, Buckley C, Shames ML, Ennis TL, Vanvickle-Chavez SJ, Mao D, et al. Treatment with simvastatinsuppresses the development of experimental abdominalaortic aneurysms in normal and hypercholesterolemic mice.Ann Surg 2005;241(1):92–101.
6. Bayly PJ, Matthews JN, Dobson PM, Price ML, Thomas DG. In-hospital mortality from abdominal aortic surgery in GreatBritain and Ireland: Vascular Anaesthesia Society audit. Br JSurg 2001;88(5):687–92.
7. National vascular database 2004./http://www.vascularsociety.org.uk/Docs/nvdr2004.pdfS.
8. EVAR trial participants. Endovascular aneurysm repair versusopen repair in patients with abdominal aortic aneurysm(EVAR trial 1): randomised controlled trial. Lancet 2005;365(9478):2179–86.
9. EVAR trial participants. Endovascular aneurysm repair andoutcome in patients unfit for open repair of abdominal aorticaneurysm (EVAR trial 2): randomised controlled trial. Lancet2005;365(9478):2187–92.
10. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminalgraft implantation for abdominal aortic aneurysms. Ann VascSurg 1991;5(6):491–9.
11. Volodos NL, Karpovich IP, Troyan VI, Kalashnikova YuV,Shekhanin VE, Ternyuk NE, et al. Clinical experience of theuse of self-fixing synthetic prostheses for remote endopros-thetics of the thoracic and the abdominal aorta and iliacarteries through the femoral artery and as intraoperativeendoprosthesis for aorta reconstruction. Vasa Suppl 1991;33:93–5.
12. Prinssen M, Verhoeven EL, Buth J, Cuypers PW, van SambeekMR, Balm R, et al. A randomized trial comparing conven-tional and endovascular repair of abdominal aortic aneur-ysms. N Engl J Med 2004;351(16):1607–18.
13. Jean-Baptiste E, Hassen-Khodja R, Bouillanne PJ, Haude-bourg P, Declemy S, Batt M. Endovascular repair of infrarenalabdominal aortic aneurysms in high-risk-surgical patients.Eur J Vasc Endovasc Surg 2007;34(2):145–51.
14. Haug ES, Romundstad P, Aune S, Hayes TB, Myhre HO.Elective open operation for abdominal aortic aneurysm inoctogenarians—survival analysis of 105 patients. Eur J VascEndovasc Surg 2005;29(5):489–95.
15. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ,Polanczyk CA, Cook EF, et al. Derivation and prospectivevalidation of a simple index for prediction of cardiac risk ofmajor noncardiac surgery. Circulation 1999;100(10):1043–9.
16. Kahn RA, Moskowitz DM, Manspeizer HE, Reich DL, McCon-ville JC, Marin ML, et al. Endovascular aortic repair isassociated with greater hemodynamic stability comparedwith open aortic reconstruction. J Cardiothorac Vasc Anesth1999;13(1):42–6.
17. Moore WS, Matsumura JS, Makaroun MS, Katzen BT, DeatonDH, Decker M, et al. Five-year interim comparison of the
Guidant bifurcated endograft with open repair of abdominalaortic aneurysm. J Vasc Surg 2003;38(1):46–55.
18. Hlatky MA, Boineau RE, Higginbotham MB, Lee KL, Mark DB,Califf RM, et al. A brief self-administered questionnaire todetermine functional capacity (the Duke Activity StatusIndex). Am J Cardiol 1989;64(10):651–4.
19. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E,Fleischmann KE, et al. ACC/AHA 2007 Guidelines onPerioperative Cardiovascular Evaluation and Care for Non-cardiac Surgery: Executive Summary—A Report of theAmerican College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Writing Committee toRevise the 2002 Guidelines on Perioperative CardiovascularEvaluation for Noncardiac Surgery): Developed in Collabora-tion With the American Society of Echocardiography,American Society of Nuclear Cardiology, Heart RhythmSociety, Society of Cardiovascular Anesthesiologists, Societyfor Cardiovascular Angiography and Interventions, Societyfor Vascular Medicine and Biology, and Society for VascularSurgery. Circulation 2007;116(17):1971–96.
20. Carpenter JP, Fairman RM, Barker CF, Golden MA, VelazquezOC, Mitchell ME, et al. Endovascular AAA repair in patientswith renal insufficiency: strategies for reducing adverserenal events. Cardiovasc Surg 2001;9(6):559–64.
21. Hua HT, Cambria RP, Chuang SK, Stoner MC, Kwolek CJ,Rowell KS, et al. Early outcomes of endovascular versus openabdominal aortic aneurysm repair in the National SurgicalQuality Improvement Program-Private Sector (NSQIP-PS).J Vasc Surg 2005;41(3):382–9.
22. Goldenberg I, Matetzky S. Nephropathy induced by contrastmedia: pathogenesis, risk factors and preventive strategies.CMAJ 2005;172(11):1461–71 [Erratum in: CMAJ 2005November 8;173(10):1210].
23. Barrett BJ, Parfrey PS. Clinical practice. Preventing nephro-pathy induced by contrast medium. N Engl J Med 2006;354(4):379–86.
24. Morcos SK. Contrast media-induced nephrotoxicity—
questions and answers. Br J Radiol 1998;71(844):357–65.25. Chalmers N, Jackson RW. Comparison of iodixanol and
iohexol in renal impairment. Br J Radiol 1999;72(859):701–3.
26. Park B, Mavanur A, Drezner AD, Gallagher J, Menzoian JO.Clinical impact of chronic renal insufficiency on endovas-cular aneurysm repair. Vasc Endovascular Surg 2006–2007;40(6):437–45.
27. Solomon R, Werner C, Mann D, D’Elia J, Silva P. Effects ofsaline, mannitol, and furosemide to prevent acute decreasesin renal function induced by radiocontrast agents. N Engl JMed 1994;331(21):1416–20.
28. Bader BD, Berger ED, Heede MB, Silberbaur I, Duda S, RislerT, et al. What is the best hydration regimen to preventcontrast media-induced nephrotoxicity? Clin Nephrol 2004;62(1):1–7.
29. Pannu N, Manns B, Lee H, Tonelli M. Systematic review of theimpact of N-acetylcysteine on contrast nephropathy. KidneyInt 2004;65(4):1366–74.
30. Moore NN, Lapsley M, Norden AG, Firth JD, Gaunt ME, VartyK, et al. Does N-acetylcysteine prevent contrast-inducednephropathy during endovascular AAA repair? A randomizedcontrolled pilot study. J Endovasc Ther 2006;13(5):660–6.
31. Blankensteijn JD, de Jong SE, Prinssen M, van der Ham AC,Buth J, van Sterkenburg SM, et al. Two-year outcomes afterconventional or endovascular repair of abdominal aorticaneurysms. N Engl J Med 2005;352(23):2398–405.
32. Vicenzi MN, Meislitzer T, Heitzinger B, Halaj M, Fleisher LA,Metzler H. Coronary artery stenting and non-cardiac

ARTICLE IN PRESS
A.C. Pichel, F. Serracino-Inglott162
surgery—a prospective outcome study. Br J Anaesth 2006;96(6):686–93.
33. Ruppert V, Leurs LJ, Steckmeier B, Buth J, Umscheid T.Influence of anesthesia type on outcome after endovascularaortic aneurysm repair: an analysis based on EUROSTARdata. J Vasc Surg 2006;44(1):16–21 [discussion 21].
34. Verhoeven EL, Cina CS, Tielliu IF, Zeebregts CJ, Prins TR,Eindhoven GB, et al. Local anesthesia for endovascularabdominal aortic aneurysm repair. J Vasc Surg 2005;42(3):402–9.
35. De Virgilio C, Romero L, Donayre C, Meek K, Lewis RJ,Lippmann M, et al. Endovascular abdominal aortic aneurysmrepair with general versus local anesthesia: a comparison of
cardiopulmonary morbidity and mortality rates. J Vasc Surg2002;36(5):988–91.
36. Bettex DA, Lachat M, Pfammatter T, Schmidlin D, Turina MI,Schmid ER. To compare general, epidural and localanaesthesia for endovascular aneurysm repair (EVAR). EurJ Vasc Endovasc Surg 2001;21(2):179–84.
37. Velazquez OC, Carpenter JP, Baum RA, Barker CF, Golden M,Criado F, et al. Perigraft air, fever, and leukocytosis afterendovascular repair of abdominal aortic aneurysms. Am JSurg 1999;178(3):185–9.
38. Cross KS, Bouchier-Hayes D, Leahy AL. Consumptive coagu-lopathy following endovascular stent repair of abdominalaortic aneurysm. Eur J Vasc Endovasc Surg 2000;19(1):94–5.