analgesic nephropathy kingdom: incidence, clinical
TRANSCRIPT

J Clin Pathol 1981;34:1255-1260
Analgesic nephropathy in the United Kingdom:incidence, clinical features and pathogenesisJ RODNEY COVE-SMITH
From North Ormesby Hospital, Middlesbrough, Cleveland TS3 6HJ
Phenacetin came into use in 1887, just 10 years afterthe first case of renal papillary necrosis wasreportedl 2 but the association between the excessiveuse of phenacetin-containing analgesics and thedevelopment of renal damage was not recogniseduntil 1953,3 since when there has been gradualrecognition that excessive analgesic consumption is amajor cause of chronic renal disease in many parts ofthe world.The initial emphasis on phenacetin has given way
to the realisation that many analgesic mixtures arenephrotoxic. Such mixtures are readily available tothe public and are widely advertised, not just for painrelief, but as tonics and general panaceas. Despiterestrictions on the sale of phenacetin and its majormetabolite paracetamol in several countries, abuse ofanalgesic mixtures has continued and there is nodefinite evidence that the incidence of analgesicnephropathy is declining.Renal damage in analgesic nephropathy is due to a
combination of renal papillary necrosis and chronicinterstitial nephritis. In many cases the disease runs arapidly progressive course with death from renalfailure within a few years of the initial presentation.
This paper is based on a study carried out inNottingham, and outlines the major features ofanalgesic nephropathy in the United Kingdom. Theclinical features of analgesic nephropathy are nowwidely recognised yet many patients have alreadydeveloped severe renal failure by the time the historyof analgesic abuse is obtained.4 5 Unless the asso-ciation with a high analgesic consumption isrecognised, the renal damage is often attributed tobacterial infection and the condition labelled"pyelonephritis." Several studies have shown, how-ever, that bacterial urinary tract infection in the adultrarely leads to end-stage renal failure,5 6 andHeptinstall has emphasised that the small, scarredkidney often labelled "chronic pyelonephritis" is theend result of many different pathological processes;in many cases the original disease cannot bedetermined.7
Early diagnosis of analgesic nephropathy is
important since complete withdrawal of analgesicsbefore significant renal damage has occurred willresult in improvement in renal function.
Renal papillary necrosis
Necrosis of the renal papillae was first reported byvon Friedreich in 1877 in the kidneys of an elderlyman with hydronephrosis secondary to prostatichypertrophy. He postulated that the increased pres-sure in the renal pelvis led to flattening of the papillaand kinking of the papillary vessels, resulting inlocal ischaemia.2 One hundred years later the exactmechanisms responsible for renal papillary necrosisremain uncertain, but local ischaemia is believed toplay an important role.Most of the early cases of papillary necrosis were
described in patients with urinary tract obstructionor diabetes mellitus, but in the 1950s a "new" form ofrenal papillary necrosis was reported from Switzer-land and Sweden8 associated with the consumptionof large quantities of phenacetin-containinganalgesics.
First reports of "phenacetin nephropathy" in theUnited Kingdom came in 1964. Sanerkin andWeaver9 emphasised that the chronic interstitialnephritis of phenacetin abuse was essentiallyindistinguishable from chronic non-obstructivepyelonephritis, except for the presence of papillarynecrosis, and that the apparent scarcity of thecondition in the United Kingdom might reflect thefailure of clinicians and pathologists to recognise it.They suggested "that particular enquiry should
always be made into phenacetin intake in allpatients with chronic pyelonephritis and at necropsyspecial attention should be paid to the renalpapillae."
In 1966 Dawborn et al.'0 presented convincingevidence that renal papillary necrosis was theprimary lesion with cortical changes occurring as asecondary event; these included tubular dilatation,interstitial nephritis and a decrease in the size of thekidneys.
1255
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from

Cove-Smith
Between 1953 and 1970 there was a marked rise inthe number of diagnosed cases of renal papillarynecrosis, particularly in Scandinavia, Switzerlandand Australia. This probably reflected both a trueincrease in incidence of the disease and increasedawareness of it.
INCIDENCE IN THE UNITED KINGDOM
After the initial reports of analgesic nephropathy inBritain in 1964, several larger series were reported,mainly from Scotland. In 1970 Koutsaimanis and deWardener,11 on the basis of 16 patients seen at oneLondon hospital, estimated that the incidence ofanalgesic nephropathy in England and Waleswould be around 500 new cases per year.A survey of chronic renal disease in Nottingham in
1973 suggested that analgesic nephropathy mightaccount for at least 10% of cases of chronic renalfailure.12 This survey was subsequently extended toinclude all reported cases of renal disease seen at thetwo major Nottingham hospitals between 1970 and1975. Information about the patients came fromfour sources:
(1) Patients referred to the nephrologists forinvestigation or treatment.
(2) Survey of chronic renal disease, 1973.(3) Survey of case notes of patients with renal
disease.(4) Survey of all necropsies performed in the two
hospitals 1970-5.In all cases where analgesic nephropathy wassuspected, or renal papillary necrosis was present,case notes and radiographs were carefully examinedand the patient and relatives questioned aboutanalgesic intake. The reasons for any excessiveanalgesic consumption were documented andchanges in renal function correlated with thequantity of analgesics consumed. By the time thediagnosis was made, in all cases, more than 1 kilo-gram of analgesics had been taken and in themajority more than 2 kilograms equivalent to 6tablets a day for 5 years.As part of the survey 20 229 necropsy reports
were examined for the presence of renal disease. Thenecropsy rate in the Nottingham hospitals was 65 %,which is higher than that reported in many otherseries.13 14 Nevertheless the survey probably under-estimated the true incidence of papillary necrosis, forin only about half of the necropsy reports was thereevidence that the papillae had been examined.
Table 1 indicates the causes of renal papillarynecrosis in the Nottingham survey. The incidence issimilar to that in other series from Europe and theUK which ranges from 0-16-1-7 .1516 Gloor reporteda significant increase in the incidence of papillarynecrosis from 0-94 o of all necropsies in 1939-50 to
Table 1 Causes of renal papillary necrosis: necropsystudy, Nottingham hospitals 1970-5
Nco of necropsiesTotal number of necropsies in surves 20 229
Renal papillary necrosis, tottl 83 (0-41 )unilateral I01bilateral 73f
Attributed to:diabetes mellitus 30obstruction --analgesic nephropathy 20acute pyelonephritis 7other 4
1 71 % in 1951-62, which he attributed to an increasein cases of analgesic nephropathy.17 During the sameperiod the incidence of papillary necrosis due todiabetes and urinary tract obstruction remainedunchanged.
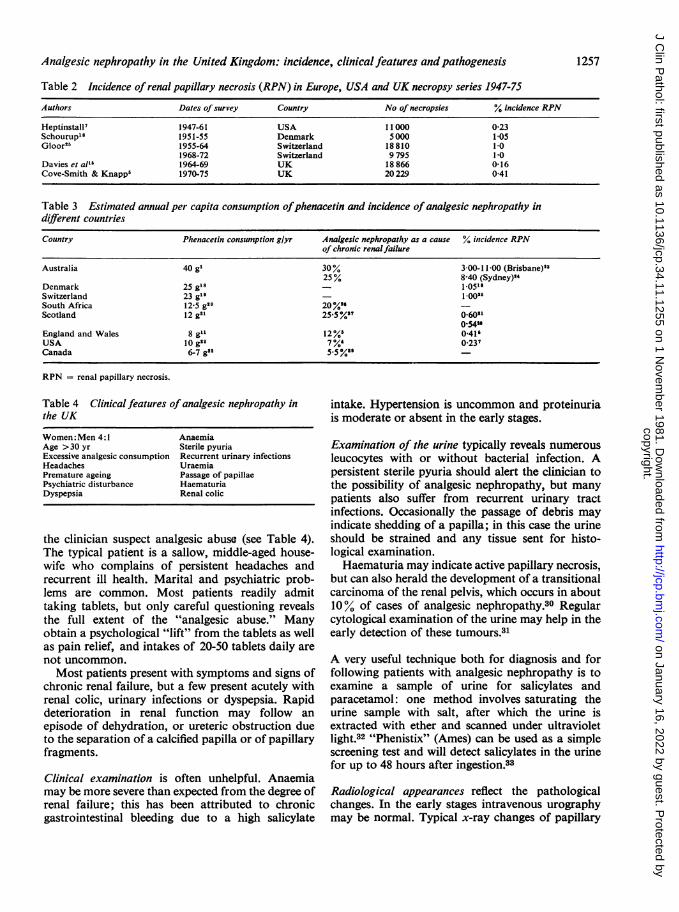
Tables 2 and 3 list the major necropsy seriesreporting renal papillary necrosis in various coun-tries. The incidence in these countries differs largelyas a result of the presence of analgesic nephropathyand can be related to the per capita consumption ofanalgesic preparations, estimated to be at least fourtimes as high in Australia as in the United States orGreat Britain. One necropsy series in Australia sug-gested an incidence of renal papillary necrosis as highas 11 % of women who lived in Brisbane;23 the sameauthors claimed that one third of all deaths fromrenal disease were due to analgesic abuse. A similarstudy from Sydney showed that analgesic nephro-pathy accounted for 25 % of patients with non-terminal renal failure during 1976.24
It is clear that this condition has now reachedepidemic proportions in many parts of the world andthe evidence from Nottingham suggests that in theUK analgesic nephropathy accounts for at least 12 ,'of cases of chronic renal failure. Unfortunately,although the condition is potentially curable, manypatients still die before the association with analgesicingestion is recognised. Unless a careful drug historyis taken and the clinical features recognised thediagnosis will be missed.
Clinical features of analgesic nephropathy
Apart from the history of analgesic abuse there maybe little to distinguish the clinical picture from otherforms of renal disease. For this reason the historyfrom any patient presenting with renal problemsshould include a careful enquiry into the intake oftablets, powders and medicines. Particular attentionshould be paid to a history of headache, migraine orarthritis, and a list compiled of all medications,especially those bought "over-the-counter."
There are a number of features which should make
1256
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from
Analgesic nephropathy in the United Kingdom: incidence, clinicalfeatures andpathogenesis
Table 2 Incidence of renal papillary necrosis (RPN) in Europe, USA and UK necropsy series 1947-75
Authors Dates of survey Country No ofnecropsies % incidence RPN
Heptinstall' 1947-61 USA 11000 0-23Schourup'l 1951-55 Denmark 5000 105Gloor2" 1955-64 Switzerland 18810 1.0
1968-72 Switzerland 9795 1.0Davies et al'l 1964-69 UK 18 866 0-16Cove-Smith & Knapp' 1970-75 UK 20229 0-41
Table 3 Estimated annual per capita consumption ofphenacetin and incidence of analgesic nephropathy indifferent countries
Country Phenacetin consumption g/yr Analgesic nephropathy as a cause % incidence RPNof chronic renalfailure
Australia 40 gl 30% 3-00-1100 (Brisbane)"25% 8-40 (Sydney)"4
Denmark 25 gl8 _ 1-0511Switzerland 23 g19 - 1.00"rSouth Africa 12-5 g20 20%"Scotland 12 g21 25-5%2? 060"1
054"England and Wales 8 gll 12%' 0-41'USA 10 g22 7%' 0 237Canada 6-7 g22 5-5%9'
RPN = renal papillary necrosis.
Table 4 Clinical features of analgesic nephropathy inthe UK
Women: Men 4:1 AnaemiaAge >30 yr Sterile pyuriaExcessive analgesic consumption Recurrent urinary infectionsHeadaches UraemiaPremature ageing Passage of papillaePsychiatric disturbance HaematuriaDyspepsia Renal colic
the clinician suspect analgesic abuse (see Table 4).The typical patient is a sallow, middle-aged house-wife who complains of persistent headaches andrecurrent ill health. Marital and psychiatric prob-lems are common. Most patients readily admittaking tablets, but only careful questioning revealsthe full extent of the "analgesic abuse." Manyobtain a psychological "lift" from the tablets as wellas pain relief, and intakes of 20-50 tablets daily arenot uncommon.Most patients present with symptoms and signs of
chronic renal failure, but a few present acutely withrenal colic, urinary infections or dyspepsia. Rapiddeterioration in renal function may follow anepisode of dehydration, or ureteric obstruction dueto the separation of a calcified papilla or of papillaryfragments.
Clinical examination is often unhelpful. Anaemiamay be more severe than expected from the degree ofrenal failure; this has been attributed to chronicgastrointestinal bleeding due to a high salicylate
intake. Hypertension is uncommon and proteinuriais moderate or absent in the early stages.
Examination of the urine typically reveals numerousleucocytes with or without bacterial infection. Apersistent sterile pyuria should alert the clinician tothe possibility of analgesic nephropathy, but manypatients also suffer from recurrent urinary tractinfections. Occasionally the passage of debris mayindicate shedding of a papilla; in this case the urineshould be strained and any tissue sent for histo-logical examination.Haematuria may indicate active papillary necrosis,
but can also herald the development of a transitionalcarcinoma of the renal pelvis, which occurs in about10% of cases of analgesic nephropathy.30 Regularcytological examination of the urine may help in theearly detection of these tumours.31
A very useful technique both for diagnosis and forfollowing patients with analgesic nephropathy is toexamine a sample of urine for salicylates andparacetamol: one method involves saturating theurine sample with salt, after which the urine isextracted with ether and scanned under ultravioletlight.32 "Phenistix" (Ames) can be used as a simplescreening test and will detect salicylates in the urinefor up to 48 hours after ingestion.33
Radiological appearances reflect the pathologicalchanges. In the early stages intravenous urographymay be normal. Typical x-ray changes of papillary
1257
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from

Cove-Smith
necrosis are seen in only 20-30% of cases. The com-monest finding is reduction in size of both kidneyswith irregularity of the outline due to shallow scars,which may often be misinterpreted as "chronicpyelonephritis."
Renal biopsy is generally unhelpful since it merelyshows interstitial nephritis without indicating thecause. Lee et al.34 suggested that demonstration of alipofuscin pigment in the tubules should arousesuspicion of analgesic abuse but this occurs in otherconditions and an accurate drug history shouldalready have alerted the clinician to the possibility ofanalgesic damage.
Management consists of total avoidance of analgesics,careful long-term supervision of hypertension, saltand water balance and urinary tract infections, and aconstant awareness and early detection of seriouscomplications such as urinary tract obstruction andtransitional cell carcinoma. Evidence of cessation ofanalgesic abuse should be obtained by routinescreening of urine for salicylates and paracetamol.
Analgesic nephropathy and "chronic pyelonephritis"
The chief difficulty in diagnosing analgesic nephro-pathy has been to distinguish it from chronicpyelonephritis. For many years the term "chronicpyelonephritis" was applied by pathologists andradiologists to any small scarred kidney, particularlyif inflammatory cells could be demonstrated in therenal parenchyma. It is now realised that scarring andcontraction of the kidney, with interstitial inflam-mation and fibrosis, are the end result of manydifferent processes including damage due to ischaemiaand drugs.7 The term "chronic pyelonephritis" shouldprobably be reserved for cases in which renal damagecan be attributed to bacterial invasion of the renaltissue. Careful examination of cases of chronic non-obstructive pyelonephritis in Britain suggests thatthere are only two major causes:
(1) Damage associated with vesico-ureteric refluxduring childhood or pregnancy (refluxnephropathy).
(2) Analgesic nephropathy.According to the proceedings of the EuropeanDialysis and Transplant Association (1970-77),chronic pyelonephritis accounts for about 200% ofpatients referred to dialysis/transplantation pro-grammes.35 Analgesic nephropathy appeared as aseparate cause of renal failure for the first time in1975. Before this it had been included in "drug-induced pyelonephritis," accounting for some 3 % ofcases. The results of the Nottingham necropsy studysuggest that renal failure due to chronic pyelone-
phritis is a relatively uncommon cause of death inpatients under 65 years of age, and that analgesicnephropathy may have been seriously under-diagnosed,36 because of the lack of a careful enquiryinto analgesic consumption and the problem ofestablishing the presence of papillary necrosis byintravenous urography.The importance of making a distinction between
analgesic nephropathy and chronic pyelonephritishas been emphasised by Gower.37 In a series ofpatients with radiological evidence of pyelonephritishe observed that deterioration in renal functionoccurred more rapidly in the group taking analgesics.Most of the patients with papillary necrosis in hisseries had a history of analgesic abuse and theirsurvival rate was 56°, at 10 years, compared with86", for those without papillary necrosis. In theNottingham series the survival rate was only 440"O at5 years, reflecting the poor renal function of mostpatients at presentation. The prognosis was especiallypoor if the serum creatinine found at the time ofdiagnosis was greater than 400 tumol/l, and themortality rate could be related both to the degree ofrenal failure and the estimated total consumptioni ofanalgesics.
Pathogenesis of analgesic nephropathy
Burry refers to three stages of papillary necrosis *3'8namely, early, intermediate and total.
In the early stage only the papillary tip appears tobe affected, with yellow coloration and some palestreaking of the pyramid; the cortex is normal.
In the intermediate stage the papillae are intact butshrunken and pale with radial streaks marking theupper zone of degeneration. The cortex is oftencoarsely scarred but of normal thickness.The group with total necrosis shows a range of
changes. In the most severely affected kidneys thecortical surface is slightly irregular with raised areascorresponding to the "renal columns". The kidneyis often reduced in size, with scars overlying necroticpapillae. The papillae are brown and withered, some-times remaining in situ, sometimes separated orabsent altogether. Calcification may be present in thepyramids.On microscopy, the necrotic areas are structure-
less and often lack the clear line of demarcation witha zone of leucocytes which is usually seen in theacute lesion associated with diabetes or obstruction.
Cortical changes in total papillary necrosisinclude atrophy and loss of the convoluted tubuleswith increased interstitial fibrosis and variablenumbers of chronic inflammatory cells. The glomerul iare usually spared.The absence of cortical changes in the early stages
1258
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from

Analgesic nephropathy in the United Kingdom: incidence, clinicalfeatures andpathogenesis
of papillary necrosis and the sparing of the columnsof Bertin indicate that papillary necrosis is theprimary lesion with cortical damage occurring as asecondary event. Burry considers that this sequenceof changes is best explained by a direct toxic effect onthe tubules but others suggest that interference withthe papillary blood supply is the primary event.39There is evidence to support both theories, but so farthe agent responsible for the damage has not beenidentified. The early emphasis on phenacetin mayhave been premature; it was a common constituentof many widely used analgesic preparations,together with aspirin, caffeine, codeine and phena-zone, but early attempts to produce papillarynecrosis in animals with phenacetin alone wereunsuccessful. However, medullary damage was laterinduced by massive doses.40 In rats papillarynecrosis is more readily and predictably induced byaspirin but many studies have now demonstratedthat mixtures of aspirin and phenacetin are morenephrotoxic than either drug alone and the lesionproduced by such mixtures is identical with that seenin man.16The difficulty of establishing the substance or
substances responsible for papillary necrosis in mancan be largely attributed to species differences.Experiments in animals cannot readily be extra-polated to man and there are variations evenbetween different strains of rat. In man phenacetin israpidly and almost totally metabolised to para-cetamol. A number of other metabolites have beenidentified but little is known about their renaltoxicity. Bluemle and Goldberg4l showed thatparacetamol is concentrated in the renal medulla andpapilla with tissue: plasma ratios similar to thoseachieved for urea; salicylates on the other hand aredistributed evenly throughout the kidney althoughconcentrations are considerably higher than in theplasma.4' Recent studies suggest that phenacetin orits metabolities or both cause direct oxidativedamage in the renal papillary cells. This action maybe potentiated by salicylates, which inhibit glucose-6-phosphate dehydrogenase (G6PD), an enzymeinvolved in the defence of tissues against oxidativedamage.42
Electron microscopy studies by Molland haveshown damage to medullary interstitial cells in ratsfollowing chronic ingestion of aspirin, and it is sug-gested that this drug may produce medullaryischaemia through inhibition of prostaglandinsynthesis.43 Prostaglandin PGE2, which is synthesisedin the renal medulla, is believed to act locally as avasodilating hormone.44 Thus, salicylates maypotentiate the effect of the toxic metabolites ofphenacetin or paracetamol in the renal papilla. Inanimals this damage is increased by dehydration,
which may also play an important part in man.Aspirin or paracetamol alone have only been
incriminated in a few cases of analgesic nephro-pathy, since most patients take analgesic mixtures.Chronic ingestion of paracetamol alone appears tohave few harmful effects on the kidney,45 and despitethe vast quantities of aspirin consumed throughoutthe world only a handful of cases can be attributed toits use. A study of patients taking large doses ofaspirin for rheumatoid arthritis showed no increasedincidence of papillary necrosis.46 Other drugs whichinhibit prostaglandin synthesis, such as indo-methacin and phenylbutazone, have been incrimi-nated in a few cases of analgesic nephropathy.47
It is now accepted that in the majority of casesanalgesic nephropathy results from the excessiveconsumption of analgesic mixtures, usually con-taining aspirin with either phenacetin or para-cetamol. The synergism between aspirin and phe-nacetin may be the result of some complex metabolicinteraction, but it seems likely that the inhibition ofprostaglandin synthetase in the renal medulla byaspirin causes relative ischaemia and that, par-ticularly in the presence of dehydration, toxicmetabolites of phenacetin, which probably includeparacetamol, are concentrated in the renal papillaand damage the ischaemic tissue.
Phenacetin has recently been replaced by para-cetamol in many analgesic mixtures available "over-the-counter." It is too early to say whether this willlead to a reduction in the incidence of analgesicnephropathy.
In summary, analgesic abuse remains an importantcause of renal damage which is still commonlymissed. The diagnosis depends on a high index ofsuspicion and a careful search for the features ofanalgesic nephropathy. Early diagnosis is importantsince cessation of analgesic intake may result inimprovement in renal function.
References
Ross P. APC as a cause of renal disease. MedJ Aust 1962;2:539-42.
2 von Friedreich N. Ober Nekrose der Nieren papillen beiHydronephrose. Virchows Archiv 1877;69:308.
3 Spuhler 0, Zollinger HU. Die chronisch-interstitielleNephritis. Zeit klin Med 1953;151:1-50.
4 Murray T, Goldberg M. Chronic interstitial nephritis:etiologic factors. Ann Intern Med 1975;82:453-9.
5 Cove-Smith JR, Knapp MS. Analgesic nephropathy: animportant cause of chronic renal failure. Quart J Med1978 ;47:49-69.
6 Bailey RR. The relationship of vesico-ureteric reflux tourinary tract infection and chronic pyelonephritis-reflux nephropathy. Clin Nephrol 1973 ;1 :132-41.
7 Heptinstall RH. Pathology of the kidney. 2nd ed. BostoLittle, Brown and Company, 1974.
Lindvall N. Renal papillary necrosis. Acta Radiol 1960suppl 192:1-153.
1259
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from

Cove-Smith
9 Sanerkin NG, Weaver CM. Chronic phenacetin nephro-pathy. Br MedJ 1964;i:288.
10 Dawborn JK, Fairley KF, Kincaid-Smith P, King WE.The association of peptic ulceration, chronic renal diseaseand analgesic abuse. Quart J Med 1966;35:69-83.
Koutsaimanis KG, de Wardener HE. Phenacetin nephro-pathy with particular reference to the effect of surgery.Br MedJ 1970;iv:131-4.
12 Cove-Smith JR, Knapp MS. Sodium handling in analgesicnephropathy. Lancet 1973 ;ii :70-2.
13 Jacobs LA, Morris JG. Renal papillary necrosis and abuseof phenacetin. MedJAust 1962 ;2:531-8.
14 Cameron HM, McGoogan E, Watson H. Necropsy: ayardstick for clinical diagnoses. Br MedJ 1980;281 :985-8.
15 Davies DJ, Kennedy A, Roberts C. The aetiology of renalmedullary necrosis: a survey of adult cases in Liverpool.J Pathol Bacteriol 1970;100:257-68.
16 Nanra RS, Kincaid-Smith P. Chronic effects of analgesicson the kidney. In: Edwards KDG. Drugs affectingkidney function and metabolism. Prog Biochemii Phar-macol Vol 7. Basel: Karger, 1972: p. 285-323.
17 Gloor FJ. Some morphological features of chronic inter-stitial nephritis (chronic pyelonephritis) in patients withanalgesic abuse. In: Kass EH. Progress in pyelonephritis.Philadelphia: Davis, 1965: p. 287-96.
18 Schourup K. Necrosis of the renal papillae. Acta PatholMicrobiol Scand 1957;41 :462-78.
1 Pletscher A. Ober die Toxikologie des Phenacetin.Bulletin der schweizerischen Akademie ler medizini-schen Wissenschafen 1958;14:100.
20 Levin NW, Rubenstein AH, Abrahams C, Jordaan JC,Posel MM. Phenacetin nephritis, interstitial nephritisand necrotising papillitis associated with chronicingestion of phenacetin. S Afr MedJ 1962 ;36:555-9.
21 Boyd DHA. The use and abuse of phenacetin. Scott Med J1964;9:423-6.
22 Gault MH, Rudwal TC, Engles WD, Dossetor JB.Syndrome associated with the abuse of analgesics. AnnIntern Med 1968 ;68 :906-25.
23 Burry AF, Axelsen RA, Trolove P. Analgesic nephro-pathy: its present contribution to the renal mortality andmorbidity profile. Med J Aust 1974;1:31-6.
24 Stewart JH. Analgesic abuse and renal failure inAustralasia. Kidney Int 1978;13:72-8.
25 Gloor FJ. Changing concepts in pathogenesis and mor-phology of analgesic nephropathy as seen in Europe.Kidney nt 1978;13:27-33.
26 Furman KI, Galasko GTF, Meyers AM, Rabkin R. Post-transplantation analgesic dependence in patients whoformerly suffered from analgesic nephropathy. ClinNephrol 1976;5 :54-6.
27 Murray RM. Genesis of analgesic nephropathy in theUnited Kingdom. Kidney Int 1978;13:50-7.
28 Cochran AJ, Lawson DH, Linton AL. Renal papillarynecrosis following phenacetin excess. Scott Med J 1967;12:246-50.
29 Shimizu A. Incidence of terminal renal failure and facilities
for its management. Ontario Medical Review May1972.
10 Taylor JS. Carcinoma of the urinary tract and analgesicabuse. MedJAust 1972;1:407-9.
Jackson B, Kirkland JA, Lawrence J R, Narayan AS, BrownHE, Mills LR. Urine cytology findings in analgesicnephropathy. J Urol 1978;120:145-7.
32 Dordoni B, Willson RA. Thompson RPH. Williams R.Reduction of absorption of paracetamol by activatedcharcoal and cholestyramine: a possible therapeuticmeasure. Br. MedJ 1973; ii: 86-7.
33 Duggan JM. The Phenistix test in the detection ot analgesicabuse. Med J Aust 1972;1:659.
32 Lee HA, Davidson AR, Burston J. Analgesic nephropathyin Wessex: a clinico-pathological survey. Clin Ncphrol1974 ;2: 197-207.
35 Proceedings of the European Dialysis and TransplantAssociation. Vols VII-XV. Tunbridge Wells: Pitmani,1970-1977.
36 Cove-Smith JR. Analgesic nephropathlv. MD Thesis.Cambridge University, 1979.
Gower PE. A prospective study ot patients with radio-logical pyelonephritis, papillary necrosis and obstructiveatrophy. Quart J Med 1976;45:315-49.
38 Burry AF. The evolution of analgesic nephropathy.Nephron 1967;5:185-201.
:19 Nanra RS, Chirawong P, Kincaid-Smith P. MedullarYischaemia in experimental analgesic nephropathy-thepathogenesis of renal papillarv necrosis. Au.st NZ J Med1973 ;3 :580-6.
1' Fordham C, Huffines WD, Welt LG. Phenacetin-inducedrenal lesions in the rat. In: Kass EH. Progress inpyelonephritis. Philadelphia: Davis, 1965: 325-3 1.
Bluemle LW, Goldberg M. Renal accumulation of sali-cylate and phenacetin: possible mechanisms in thenephropathy of analgesic abuse. J Clin Invest 1968;47:2507-14.
42 Murray TG, Goldberg M. Analgesic-associated nephro-pathy in the USA: Epidemiologic, clinical and patho-genetic features. KidineY Int 1978;13:64-71.
13 Molland EA. Experimental renal papillary necrosis. KidneYInt 1978;13:5-14.
44 Itskovitz HD, Stemper J, Pacholczyk D, McGiff JC.Renal prostaglandins: determinants of intrarenaldistribution of blood flow in the dog. Clin Sci Mol Med1973 ;45, suppl 1 :321s-4s.
45 Edwards OM, Edwards P, Huskisson EC, Taylor RT.Paracetamol and renal damage. Br MedJ 1971 ;ii:87.
46 New Zealand Rheumatism Association Study. Aspirin andthe kidney. Br Med J 1974;i:593-6.
4 Krishnaswamy S, Nanra RS. "Phenacetin" nephropath>:without phenacetin. Auvst NZ J Med 1976;6:88.
Requests for reprints to: Dr JR Cove-Smith, ConsultantNephrologist, North Ormesby Hospital, Middlesbrough,Cleveland TS3 6HJ, England.
1260
copyright. on January 16, 2022 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.11.1255 on 1 Novem
ber 1981. Dow
nloaded from