analysis of costs associated with administration of ... · pdf filejmcp analysis of costs...
TRANSCRIPT

844 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
ABSTRACT
BACKGROUND: An estimated $8.1 billion (in 2004 dollars) is spent annually on total health care costs for the treatment of breast cancer in the United States. Breast cancer has traditionally been treated with intravenous (IV) cancer therapies that entail not only the drug acquisition cost, but additional costs of personnel time, supplies, and equipment used in the preparation and administration of the IV drug. A systematic study of the costs of IV administration in the metastatic breast cancer (MBC) population has not been performed.
OBJECTIVE: To assess the cost components, overall and by payer type and patient age group, for administering a single-agent IV breast cancer drug to women with MBC in the United States.
METHODS: Women diagnosed with MBC (ICD-9-CM codes 174.XX and 196.XX-198.XX) reported any time between January 1, 2003, and May 31, 2006, and receiving single-agent IV breast cancer therapy (including intramuscular fulvestrant) during a visit were identified (using HCPCS and CPT codes) from an administrative claims database supporting 46 general/oncology clinics in the United States. Study drugs were either FDA-approved for breast cancer or recommended for use as preferred single agents per National Comprehensive Cancer Network (NCCN) clinical practice guidelines for breast cancer. Costs were estimated using the con-tracted allowed payment, which is the amount that the provider is eligible to receive from all parties, including payers and patients. Costs were mea-sured using 2 approaches—average cost per IV-administration visit and average cost per patient per month (PPPM).
RESULTS: Over the 41-month study period (through May 31, 2006), 46,273 patients had a breast cancer diagnosis, of which 8,533 (18.4%) were metastatic; 828 (9.7%) of these patients received 1 of 11 single-agent IV breast cancer drugs over 7,406 visits. Mean (SD) total payments across all drugs and cost components were $2,477 ($1,842) per visit and $4,966 ($3,841) PPPM, of which IV administration costs were 10.2% of per-visit and 11.4% of PPPM costs, and other drugs and services provided dur-ing IV administration were 30.8% of per-visit and 32.2% of PPPM costs. In both the per-visit and PPPM analyses, approximately 80% of costs for other drugs and services (approximately 25% of total treatment costs) were attributed to (a) antihypercalcemic agents (e.g., zoledronic acid: 6%-8% of total treatment cost), (b) colony-stimulating factors (CSFs) (e.g., pegfilgrastim, epoetin: 6%-7%), or (c) other anticancer agents being used off-label or for other conditions (e.g., bevacizumab, irinotecan, carboplatin, vincristine: 11%-12%). The remaining 20% of costs for other drugs and services (about 6% of total costs) were attributable primarily to antiemetic agents (e.g., palonosetron, granisetron) and miscellaneous or unclassified products. Non-protein-bound paclitaxel was the most commonly used IV therapy at a mean cost of $2,804 per visit, with IV administration account-ing for $353 (12.6%) and other services accounting for $1,237 (44.1%) of total costs per visit. The second most commonly used IV therapy was tras-tuzumab at a mean cost of $2,526 per visit, with IV administration account-ing for $214 (8.5%) and other services accounting for $336 (13.3%) of total costs per visit.
CONCLUSIONS: For patients being administered a single FDA-approved or NCCN-recommended IV drug for treatment of MBC, IV administration costs accounted for approximately 10%-11% of total cost, and the study drugs accounted for 56%-59%. Other drugs and services accounted for
31%-32%, most of which was attributable to antihypercalcemic agents, CSFs, anticancer drugs being used off-label for breast cancer or for other conditions, and antiemetic agents. Although costs of IV administration are 10%-11% of total IV chemotherapy costs for MBC and would clearly be avoided with the use of oral agents, the extent to which other costs would be avoided or incurred with use of oral agents is unknown and requires further research.
J Manag Care Pharm. 2008;14(9):844-57
Copyright © 2008, Academy of Managed Care Pharmacy. All rights reserved.
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
Gregory B. Kruse, MPH, MSc; Mayur M. Amonkar, PhD; Gregory Smith, BA; Dean C. Skonieczny, MBA, BSE; and Spyros Stavrakas, PhD
RESEARCH
• Breast cancer is the most frequently diagnosed cancer inwomenand thesecondmostcommoncauseofcancerdeath inwomenofallagesintheUnitedStates.In2008,anestimated250,230U.S.womenwillbediagnosedwithbreastcancer.
• ThetotalannualcostofdiagnosingandtreatingMBCin theUnitedStatesisanestimated$8.1billion(in2004dollars)forhospitalandmedicalcosts,includingdrugcostsandthecost of personnel time and supplies/equipment involved in thepreparation, administration, andmanagement of the infusedandinjectabledrugs.
• Limited informationexistson the additional costs above thecost of the cancer drug incurredwith the administration of IVtherapy inpatientswithMBC.Thesecosts, inadditiontothedirectdrug cost,havebeen reported to range from30%acrossallcancersto50%inpatientswithlungcancer.
What is already known about this subject
What this study adds
• Examining 828 patients with MBC with 7,406 visits for treatment with a single IV-administered breast cancer drugovera41-monthtimeperiod,themeantotalpaymentsacrossall drugs and cost components were $2,477 per visit and$4,966PPPM.CostsotherthanthebreastcancerIVdrugcostaccountedfor41%-43%oftotalpayments,ofwhich10%-11%wasattributabletoIVadministrationand31%-32%wasattrib-utabletoother drugs and services.
• Approximately 80% of the costs for other drugs and services (25% of totalMBC treatment cost) were attributable to anti-hypercalcemic agents (e.g., zoledronic acid, pamidronate),CSFs(e.g.,pegfilgrastim,filgrastim,epoetin,darbepoetin),and off-label anticancer drugs. Antiemetics (e.g., palonosetron,granisetron)accountedforabout9%ofother drugs and services.

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 845
In the United States, breast cancer is the most frequentlydiagnosedcancerinwomenandrankssecondamongcancerdeaths inwomenafter lungcancer.1 In2008,anestimated
250,230womenintheUnitedStateswillreceiveadiagnosisofbreast cancer—182,460 (72.9%) with invasive/metastatic and67,770with in situ cancer—and 40,480womenwill die fromthedisease.1Anestimated$8.1billion(in2004dollars)intotalhealthcarecostsisspentannuallyonthediagnosisandtreatmentofbreastcancerintheUnitedStates.2
The various options that are available to treat breast cancercan be divided into 2 categories, local treatment or systemictreatment. Local treatment, involving surgery and/or radiation,isdirectedonly at the cancer cells in thebreast area.Systemictreatmentistheuseofmedicationsthattravelinthebloodstreamtoaffectortreatcancercells.Systemictreatmentsincludechemo-therapy, hormonal therapy, and targeted therapies (treatmentsthat identify and attack specific cancer cells without harmingnormalcells)andareoftenusedincombinationwithsurgeryorradiation,particularlyinearlybreastcancer.
Systemictreatmentsmayalsobeusedaloneinmoreadvancedstageswhencancerhasmetastasizedtootherpartsofthebody.In the United States, commonly used chemotherapy agentsapproved by the U.S. Food and Drug Administration (FDA)for metastatic breast cancer (MBC) include taxanes (docetaxeland paclitaxel), anthracyclines (doxorubicin and epirubicin),gemcitabine, andcapecitabine (anoral agent).Commonlyusedendocrineagentsarearomataseinhibitors(anastrozole,letrozole,orexemestane)orestrogenmodulators(fulvestrantortamoxifen).Trastuzumab and lapatinib are newer targeted therapies avail-ableforpatientswithbreastcancerwithtumorsthatoverexpressErbB2 (or HER2), a growth factor receptor gene, representingapproximately 25%-30% of the patient population with breastcancer.3TheNationalComprehensiveCancerNetwork(NCCN),anot-for-profitallianceof21leadingcancercentersintheUnitedStates,developsguidelinesfortreatmentofmanytypesofcancerandmayrecommendagentsthathavenotreceivedFDAapproval.Forexample, theNCCNtreatmentguidelines forbreastcancerincludesvinorelbineasoneofseveralpreferredsingleagentsforrecurrentormetastaticbreastcancer.4
Most patients have traditionally been treated with chemo-therapyadministeredintravenouslyeitheraloneor incombina-tionand,hence,incuradditionalcostsabovethedrugacquisitioncost.Theseadditionalcostsincludethecostofpractitionertimeforintravenous(IV)administrationandotherservicesthatmaybeprovidedduringtheclinicvisit,rangingfromthemanagementofadverseeventsassociatedwiththeadministrationtotheneedfor additional supportive care agents, specialized equipment,supplies,andotherpersonneltime.Severaloralanticancerdrugs(e.g., tamoxifen, capecitabine, lapatinib, sorafenib, sunitinib,and dasatinib) have been approved, and numerous others areindevelopment.UseoforalagentsmayleadtocostsavingsforpayersbyavoidingthecostassociatedwiththeIVadministration
and related costs. Other potential advantages of oral cancertherapiesincludeconvenienceandeaseofadministration,whichare particularly important when patients require treatmentoveraprolongedperiodof timebecauseofadvances incancer management.5-9
Most published studies on the economic burden of cancer,includingbreastcancer, lacksufficientdetail toprovideaclearunderstandingofall thecost factorsassociatedwiththecancertherapy.10-13Onepublishedreviewofthecostsofcancersuggeststhatcostsotherthancancerdrugcosts,suchasIVadministrationprocedures, other oral and IV drugs, evaluation and manage-ment,laboratoryservices,andradiology,accountfor30%oftotalcosts,whereasa study in lungcancer reports thesecosts tobearound41%.14-15
Theobjectiveofthisstudywastoassessthecostcomponents,fromapayerperspective,ofprovidingIVtherapywithasingleFDA-approved or NCCN-recommended agent to women withMBCintheUnitedStates.Thisstudyusedanovelprovider-payercontract database to categorizeMBC claims into the followingcostcomponents:IVbreastcancertherapies,IVadministration,and other supportive services. These costs were examined by IVbreastcancerdrug,payertype,andpatientagegroup.
■■ MethodsData SourceDataforthisstudywereobtainedfromthedatabaseofMedicalPresent Value Inc. (MPV), a contract management companylocatedinAustin,Texas(www.mpv.com).MPVmaintainsacon-tractandclaimsmanagementsystemthatsupports46general/oncology clinics in theUnitedStates andcontains informationon more than 46,000 patients with breast cancer (identifiedby International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 174.XX, Table 1). The databasecontains a complete history of diagnoses (ICD-9-CM codes),procedures,anddrug therapies receivedby thepatientswithinthe clinics, as well as patient demographics (e.g., age, gender,and geographic region), insurance type (e.g., managed care,indemnity,Medicare,andMedicaid),andinsuranceproducttype(e.g., health maintenance organization and preferred providerorganization),includingthird-partypayersforprivateinsurance.Foreverypatientclinicvisit,MPVmaintains theservicedates,total charged, and total contracted payments, with individualservices,procedures,anddrugsbrokenoutbylineitem(CurrentProceduralTerminology,FourthEdition[CPT-4]andHealthcareCommonProcedureCodingSystem[HCPCS]codes).
Treatmentcostswereestimatedusingthecontractedallowedpaymentforaclaim,notthepracticecharges,basedonadjudica-tionoftheclaimbythepatient’sthird-partyinsuranceplan.Thiscontractedpaymentisdefinedastheamountthattheprovideriseligibletoreceivefromallparties,includingprimaryandsecond-arypayersandthepatient,basedonthecontractualagreementwith thepayer.Because thecontractedpayment represents the
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population

846 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
actualpaymenttoprovidersfrompayers,itdepictsamoreaccu-rateanddetailedviewofthetrueeconomicburdenofIVadmin-istration to payers thanwould charges; on average, contractedpaymentswereapproximately51%ofprovider-submittedchargesduringthestudyperiod.
Basedonan Internet searchofFDA-approvedbreast cancerdrugs, NCCN clinical practice guidelines, and other sources,
15drugswere identified (seeAppendix)ofwhich11 therapieswerecommonbreast cancer treatments identifiedandassessedinthisstudy(henceforthreferredtoas“studydrugs”):cyclophos-phamide,docetaxel,doxorubicin,fluorouracil,fulvestrant,gem-citabine,non-protein-boundpaclitaxel,protein-boundpaclitaxel,trastuzumab, vinblastine, and vinorelbine (Table 2). All thesedrugsareadministered intravenouslyexcept fulvestrant,whichisadministeredintramuscularly.
Study CohortThe study cohort consisted of female patients diagnosed withMBC.Patients(a)had1ormoreclaimswithadiagnosisofbreastcancer (ICD-9-CM code 174.XX)and 1 ormore claimswith adiagnosis of secondary malignant neoplasms of lymph nodes(ICD-9-CM code 196.XX), respiratory and digestive systems(ICD-9-CM code 197.XX), and/or other specified sites (ICD-9-CMcode198.XX)betweenJanuary1,2003,andMay31,2006(Table1);(b)receivedatleast1ofthe11single-agentIVbreastcancer treatments (Table2)during a clinic visit; and (c)had aminimumof1monthfollow-up.Diagnosescouldbereportedinanypositionontheclaim(e.g.,primary,secondary,ortertiary.)Atotalof46,273patientswithadiagnosisofbreastcancerwereidentified,ofwhom8,533alsohadasecondarymalignantneo-plasmdiagnosis.Furtherrestrictingthesampletopatientsreceiv-ingasingle-agentIVbreastcancerdrugandminimumfollow-upofatleast1monthinthedatasetresultedin828eligiblepatients(Figure1).Patientrecordswererestrictedtothestartingdateofthemetastaticdiagnosisandwerefolloweduntileithertheenddate of the study period or the date on which the patient no longerreceivedcareattheclinicordied.
Thisstudyfocusesonlyonsingle-agentvisitsforIVtreatment, defined as visits duringwhich patients received a single FDA-approved or NCCN-recommended breast cancer drug. Thisdecisionwasmade for several reasons.First, single-agentvisitscomprisedamajority(73%)oftheIVvisitsinthedata.Second,ifvisitsinwhichmultipletherapieswereadministeredhadbeenusedastheunitofanalysis,thenumberofvisitsforthevariousunique combination therapies would have been significantlysmaller,limitingtheinterpretabilityoftheresults.Forexample,18ofthe33combinationtherapiesidentifiedinthedatawouldhavecontributed10orfewervisitstothedataset,comparedwithan average of 673 visits for single-agent breast cancer therapy(7,406 total visits divided by 11 breast cancer agents). Third,previous research has shown that costs incurred in additiontobreast cancerdrugcosts arehigher for combination therapythan formonotherapy. For example, costs associated with theadministration of trastuzumab-based combination therapieswereestimatedin1studytobeabout30.3%oftotalcosts(10.9%for IV administration and19.4% forother visit-related servicesand drugs provided during IV administration), whereas costsassociatedwithadministrationoftrastuzumabalonewere21.8%of total costs (8.5% for IV administration and 13.3% for other
TABLE 1 ICD-9-CM Codes Used to Identify the Study Cohort
174Malignantneoplasmoffemalebreast
174.0Nippleandareola
174.1Centralportion
174.2Upper-innerquadrant
174.3Lower-innerquadrant
174.4Upper-outerquadrant
174.5Lower-outerquadrant
174.6Axillarytail
174.8Otherspecifiedsitesoffemalebreast
174.9Breast(female),unspecified
196Secondaryandunspecifiedmalignantneoplasmoflymphnodes
196.0Lymphnodesofhead,face,andneck
196.1Intrathoraciclymphnodes
196.2Intra-abdominallymphnodes
196.3Lymphnodesofaxillaandupperlimb
196.5Lymphnodesofinguinalregionandlowerlimb
196.6Intrapelviclymphnodes
196.8Lymphnodesofmultiplesites
196.9Siteunspecified
197Secondarymalignantneoplasmofrespiratoryanddigestivesystems
197.0Lung
197.1Mediastinum
197.2Pleura
197.3Otherrespiratoryorgans
197.4Smallintestine,includingduodenum
197.5Largeintestineandrectum
197.6Retroperitoneumandperitoneum
197.7Liver,specifiedassecondary
197.8Otherdigestiveorgansandspleen
198Secondarymalignantneoplasmofotherspecifiedsites
198.0Kidney
198.1Otherurinaryorgans
198.2Skin
198.3Brainandspinalcord
198.4Otherpartsofnervoussystem
198.5Boneandbonemarrow
198.6Ovary
198.7Adrenalgland
198.8Otherspecifiedsites
ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification.

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 847
FIGURE 1 Selection of Patients with Metastatic Breast Cancer Receiving IV Monotherapya
aAn unknown number of the 8,533 patients with metastatic breast cancer were either treated at other oncology clinics or not treated at all.IV=intravenous.
Patients with a breast cancerdiagnosis from January 1, 2003
to May 31, 2006N=46,273
Patients with a secondarymalignant neoplasm diagnosis
N=8,533 (18.4%)
Patients with monotherapy orcombination therapy IV
administration visitN=999 (11.7%)
Patients with monotherapy IVadministration visits only
N=828 (82.9%)
visit-relatedservicesanddrugsprovidedduringIVadministra-tion).16Toaddress theconcernofpotentialbiasbyfocusingonmonotherapy, a sensitivity analysiswas performed to comparetheprimarycostcategoriesofmonotherapywiththe27%ofvisitswhere2ormore(combination)approvedorrecommendedbreastcancertherapieswereadministered.
Although patients receiving more than 1 FDA-approved orNCCN-recommendedregimenwereexcludedfromthestudysam-ple,patientsreceivinganFDA-approvedorNCCN-recommendedagentcoupledwithanoff-labelagentwereretainedforanalysis.Thisdecisionwasmadebecauseoff-labeluseofanticanceragentsisprevalentincancertreatment.Atotalof170(20.5%)patientswere using both an FDA-approved or NCCN-recommendedtreatmentandatleast1off-labelanticancertreatment.
Outcome Measures and AnalysisCostswere calculated using 2 approaches: average cost per IVadministration visit and average cost per patient per month(PPPM).IVadministrationvisitswereselectedbasedonadminis-trationofanIVtherapyduringaclinicvisitandidentifiedbytheclaimIDanddate.Allservices,materials,anddrugsidentifiedbytheclaimlineitemsduringthesevisitswereusedintheIVther-apyadministrationvisitcostanalysis.TocalculatePPPMcosts,therapydurationinmonthsforeachpatientwascalculatedusingIVstudydrugstartandenddates.StartdatesweredeterminedusingthefilingdateoftheappropriateJ-codeclaim(Table2)fol-lowinga30-daywashoutperiod(i.e.,nostudydrugIVtherapyprescribed in prior 30 days). End dateswere determined by a30-daywashout period following the last IV therapy claim forastudydrugortheendofthestudyperiod.PatientscouldhavestoppedIVtherapyforseveralreasons,includingdiscontinuationofthetherapy,switchingtoanothermonotherapyorcombinationtherapy,receivingcareinahospitaloranothertreatmentfacility,ordeath.ThelineitemsfromthevisitsidentifiedintheIVvisitanalysis were then aggregated into therapy months based ontherapydurationandreportedonaPPPMbasis.
It is important tonote that someof themonotherapy visitswereexcludedinthePPPManalysis.Thispatternoccurredwhenthemonotherapyvisitsofapatientobtainingdifferentdrugsover-lappedoneanother.Althoughthesepatientscouldbeincludedinthemonotherapyvisitanalysisbecausetheywerereceivingonly1IVbreastcancerstudydrugduringeachvisit, thePPPMcal-culationwouldinvolvecombiningmultiplestudydrugtherapieswithinthesamepatient-month.Forexample,ifapatientreceiveddrugAfor2monthsandthendrugBfor2months,allthesevisitswouldbeincludedinboththemonotherapyandPPPManalyses.However,ifapatientreceiveddrugAinmonths1-4andreceiveddrugBinmonths3and4,allthesevisitswouldbeincludedintheIVvisitanalysissincetheyweresingle-agentvisits,butonlydrugAformonths1and2wouldbeincludedinthePPPManaly-sisbecausethepatientwasreceivingcombinationtherapyfromadurationviewpointduringmonths3and4.Tomaintain the
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
AgentCommon Brand
Name(s) HCPCS Code(s)Protein-bound paclitaxel
Abraxane J9264
Doxorubicinb Adriamycin, Rubex
J9000-J9001
Fluorouracilb Adrucil J9190
Docetaxel Taxotere J9170
Non-protein-bound paclitaxel
Taxol J9265
Vinblastineb Vinblastine J9360
Trastuzumab Herceptin J9355
Gemcitabine Gemzar J9201
Fulvestrant(IM) Faslodex J9395
Cyclophosphamideb Cytoxan,Neosar J9070,J9080,andJ9090-J9097
Vinorelbineb Navelbine J9390a Two additional drugs—epirubicin and thiotepa—met study criteria for inclusion but are not shown in the table because no patients in the study cohort received them.b Available generically.HCPCS = Health Care Procedure Coding System; IM = intramuscular.
TABLE 2 Breast Cancer Drugs and HCPCS Codes a

848 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
consistency of examining monotherapy across both measures,the PPPM analysis was restricted to therapy durations wherepatientsreceivedonly1therapy.
Wecategorizedthevariousbillablecomponentsinto1of3cost categories: (1) IV breast cancer study drug; (2) administration ofallIVmedications,includingthebreastcancerstudydrug;and(3)othervisit-relatedservicesanddrugs.TheIVadministrationcategoryincludedallcodesandcostsassociatedwiththedurationof administration (e.g., CPT code 96413 covers chemotherapyadministrationviaintravenousinfusiontechniqueupto1hourforasingleorinitialdrug).Thelastcategory,othervisit-relatedser-vicesanddrugs,wasdividedfurtherinto4categories:(3a)otherinjectabledrugs(e.g.,antianemiadrugsepoetinanddarbepoetin)andconcomitantoraldrugs(e.g.,diphenhydramine,granisetron, and ondansetron), (3b) evaluation and management services, (3c)suppliesandequipment,and(3d)miscellaneousadministra-tion-relatedservices.Concomitantoraldrugsarethosewhichareadministeredasaninitialdoseassupportivecareatthetimeofchemotherapytreatmentandarebilledduringthatvisit.Topro-videadditionaldetailontheotherinjectabledrugsandconcomi-tantoraldrugsadministeredduringthesevisits,wedividedthiscategory into11drugcategories: antihypercalcemicdrugs, col-ony-stimulatingfactors(CSFs),anticanceragents(usedinanoff-labelindicationorforotherconditions),antiemeticagents,saline
solution, corticosteroids, heparin, antihistamines, histamine-2 (H2) antagonists, iron, and miscellaneous/unclassified agents.For patients using both a study drug and 1 or more off-labelanticanceragents,costsfortheoff-labeldrugwereplacedintothe“othervisit-relatedservices”category(c-1).
For each of the 3major cost components—IV study drug, IV administration, and other visit-related costs—drug, payertype,andpatientagegroupswerecomparedusingtheKruskal-Wallistest,anonparametricone-wayanalysisofvariance.
■■ ResultsStudy Cohort CharacteristicsAtotalof828eligiblepatientswith7,406visitsforIVtherapyforanyofthe11studydrugswereidentified.Demographiccharacter-isticsarepresentedinTable3.Morethanthree-quarters(76.7%)ofthepatientswereyoungerthan65yearsofage.Geographically,the patients were more representative of the southern and westernUnitedStatesthanofotherregions,andfewpatientswerefromthenortheasternUnitedStates.Themajority(about65%)ofpatients had private insurance (i.e., employer-based, managedcare,orindemnityhealthinsurance);23.4%hadMedicare,3.3%Medicaid,and8.1%otherorunknowninsurancetype.
Overall Payments for Patients With MBCPaymentamountsoverall andbycostcategory for theper-visitand PPPM analyses are presented in Table 4. The mean (SD)totalpaymentsacrossalldrugsandcostcategorieswere$2,477($1,842) per visit and $4,966 ($3,841) PPPM. In the per-visit analysis,IVbreastcancerdrugmeanpaymentamountaccountedfor59.0%($1,463)of the total,with IVadministration respon-sible for 10.2% ($252) and other services provided at the visitaccountingfortheremaining30.8%($763).ThePPPManalysisexhibited abreakdown similar to that of theper-visit analysis:$2,800(56.4%)forIVcancerdrug,$568(11.4%)forIVadmin-istration,and$1,598(32.2%)forothervisit-relatedservicesanddrugs.Inbothanalyses,99%ofcostsforthecategory“otherser-vicesprovidedatvisit”wereattributabletodrugcostsforotherinjectabledrugsandconcomitantoraldrugs.
The antihypercalcemic/bone resorption agents such as zoledronic acid and pamidronate comprised the highest-costdrugcategory in thevisit analysis, accounting for24.7%($188per visit) of the cost of other visit-related services, followed by CSFs such as pegfilgrastim, filgrastim, epoetin, and dar-bepoetin, which accounted for another 20.2% ($154 per visit) of the category. An additional $273 per visit (35.8%) of the other visit-related services cost was attributable to anticancerdrugs that may be used off-label or to treat other conditions,including antineoplastic agents (e.g., bevacizumab), platinumagents (e.g., carboplatin), and chemotherapeutic agents (e.g., vincristine).
Other drugs with high prevalence included the supportivecare antiemetics (e.g., palonosetron, granisetron; $65.97 per
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
TABLE 3 Study Cohort Characteristics
Metastatic Breast Cancer
Patient CohortCharacteristic Count %
Overall 828 100.0
Age (Years) Youngerthan45 145 17.5
45-54 229 27.7
55-64 261 31.5
65-74 129 15.6
75orolder 64 7.7
Geographic Region Northeast 5 0.6
Midwest 175 21.1
South 241 29.1
Southwest 134 16.2
West 273 33.0
Payer TypeManagedCare(HMO,POS,andPPO) 452 54.6
Indemnity 88 10.6
Medicare 194 23.4
Medicaid 27 3.3
Other/Unknown 67 8.1
HMO = health maintenance organization; POS = point of service; PPO = preferred provider organization.

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 849
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
visit),salineproducts(usedfordilutionorreconstitutionoftheIVproduct;$11.17pervisit),andothersupportivecareconcomi-tantoraldrugs,suchasdexamethasonesodiumphosphate(e.g.,to avoid the occurrence of severe hypersensitivity reactions inpatientsreceivingnon-protein-boundpaclitaxel;$4.51pervisit),diphenhydraminehydrochloride(toavoidseverehypersensitivityreactions; $0.47 per visit), andH2 antagonists (e.g., ranitidine;$0.39pervisit).
The remaining other visit-related costs were services andequipmentprovidedduringtheIVadministrationvisit.Themostfrequentlybilledproceduresintheevaluationandmanagementservicescategorywerephysicianassessments forchemotherapyadministration or side-effects related to chemotherapy, includ-ingnauseaand/orvomiting, fatigue,andpain ($4.31pervisit).Duringthesevisits, themostcommonsuppliesandequipmentusedwereIVneedles,sterilewater,dressingpads,andinfusionsupplies($1.87pervisit).Finally,themiscellaneousadministra-tion-relatedservicescategoryprimarilyincludedfluidcollectionand laboratories such as metabolic panels and red and whitebloodcellcounts($2.24pervisit).AsimilarpatternforthesecostcategorieswasobservedinthePPPManalysis.
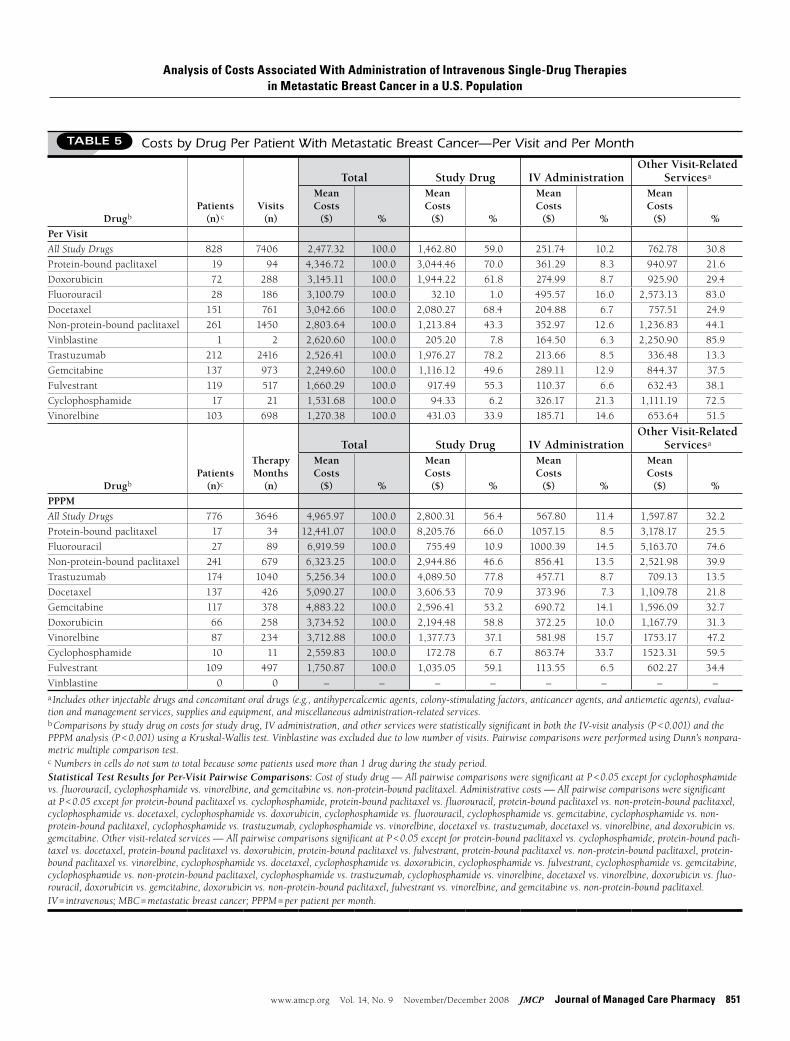
Payments by IV Cancer DrugPayments in total and for each of the 11 breast cancer drugs(includingintramuscular[IM]fulvestrant)and3costcategories,by visit and PPPM, are presented in Table 5. Among the 828patients,themostcommonlyuseddrugsincludednon-protein-boundpaclitaxel (31.5%ofpatients) and trastuzumab (25.6%),whereastheleastcommonlyuseddrugsincludedprotein-boundpaclitaxel(2.3%)andcyclophosphamide(2.1%).
Average total contracted payments significantly differed bydrug in theper-visit (P <0.001) andPPPM (P <0.001) analyses.Thehighesttotalpaymentspervisitwereobservedforprotein-boundpaclitaxel($4,347)anddoxorubicin($3,145).Thelowesttotalpaymentswereobservedforvinorelbine($1,270)andcyclo-phosphamide($1,532).InthePPPMcostanalysis,protein-boundpaclitaxel and fluorouracil had the highest average total PPPMcosts($12,441and$6,920,respectively),whereasIMfulvestrantandcyclophosphamidehadthelowestaveragetotalcosts($2,560and$1,751,respectively).ExaminingIVbreastcancerdrugcostsalone, themost expensive treatmentspervisit andPPPMwereprotein-boundpaclitaxel, docetaxel, and trastuzumab,whereasfluorouracilandcyclophosphamideweretheleastexpensive.
TABLE 4 Overall Costs Per Patient With Metastatic Breast Cancer (N = 828) by Visit and Month
CONTRACTED PAYMENTS ($)
Per Visit No. of Visits Mean % of Total
% of Other Services
Provided at Visit SD Median
Total 7406 2,477.32 100 NA 1,842.00 1,998
1.IVstudydrug 1,462.80 59.0 NA 1,153.00 1,079
2.IVadministration(alldrugs) 251.74 10.2 NA 217.00 201
3.Othervisit-relatedservicesanddrugs 762.78 30.8 100 1,392.00 160
3a.Otherinjectabledrugsandconcomitantoraldrugsa 754.37 30.5 98.9 1,390.02 149
•Antihypercalcemicagents(e.g.,zoledronicacid) 188.33 7.6 24.7 405.61 0
•Colony-stimulatingfactors(e.g.,pegfilgrastim,filgrastim, epoetin,anddarbepoetin)
153.80 6.2 20.2 438.74 0
•Antineoplasticagents(bevacizumab)b 171.77 6.9 22.5 1,037.16 0
•Platinumagents(e.g.,carboplatinandoxaliplatin)b 74.49 3.0 9.8 382.78 0
•Chemotherapeuticagents(e.g.,irinotecanandvincristine)b 26.83 1.1 3.5 203.79 0
•Antiemeticagents(e.g.,palonosetronandgranisetron) 65.97 2.7 8.6 230.94 0
•Salinesolution,dextrosewater 11.17 0.5 1.5 14.15 6
•Corticosteroids(e.g.,dexamethasone) 4.51 0.2 0.6 20.68 0
•Heparin 3.40 0.1 0.4 14.65 0
•Antihistamine(e.g.,diphenhydramine) 0.47 0.0 0.1 1.37 0
•Histamine-2receptorantagonists(e.g.,ranitidine) 0.39 0.0 0.1 1.49 0
•Iron 0.03 0.0 0.0 1.44 0
•Miscellaneous/unclassifiedagents 53.19 2.1 7.0 341.68 0
3b.Officevisit:evaluationandmanagementservicesc 4.31 0.2 0.6 22.61 0
3c.Suppliesandequipmentd 1.87 0.1 0.2 32.52 0
3d.Miscellaneousadministration-relatedservicese 2.24 0.1 0.3 21.10 0
Continued on next page

850 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
AlthoughIVbreastcancerdrugcostvariationwasexpected,weobserved that the costs associatedwith administration andwithothervisit-relatedservicesanddrugsalsovariedsignificantlybetweenagents(P <0.001).CostsassociatedwithIVadministra-tionrangedfrom$110to$496pervisitacrossdrugs,representing6.3%to21.3%oftotalcosts,andfrom$114to$1,057PPPMacrossdrugs,representing6.5%to33.7%oftotalcosts.Costsassociatedwithothervisit-relatedservicesanddrugsalsovariedsignificantlyacross therapies (P <0.001), showing greater variation than didcostsassociatedwithIVadministration.Thesecostsvariedfrom$336to$2,573pervisitand$602to$5,164PPPMacrossdrugs.
These costs as a percentage of total costs ranged from 13.3% (trastuzumab)to85.9%(vinblastine)onaper-visitbasisandfrom13.5%(trastuzumab)to74.6%(fluorouracil)onaPPPMbasis.
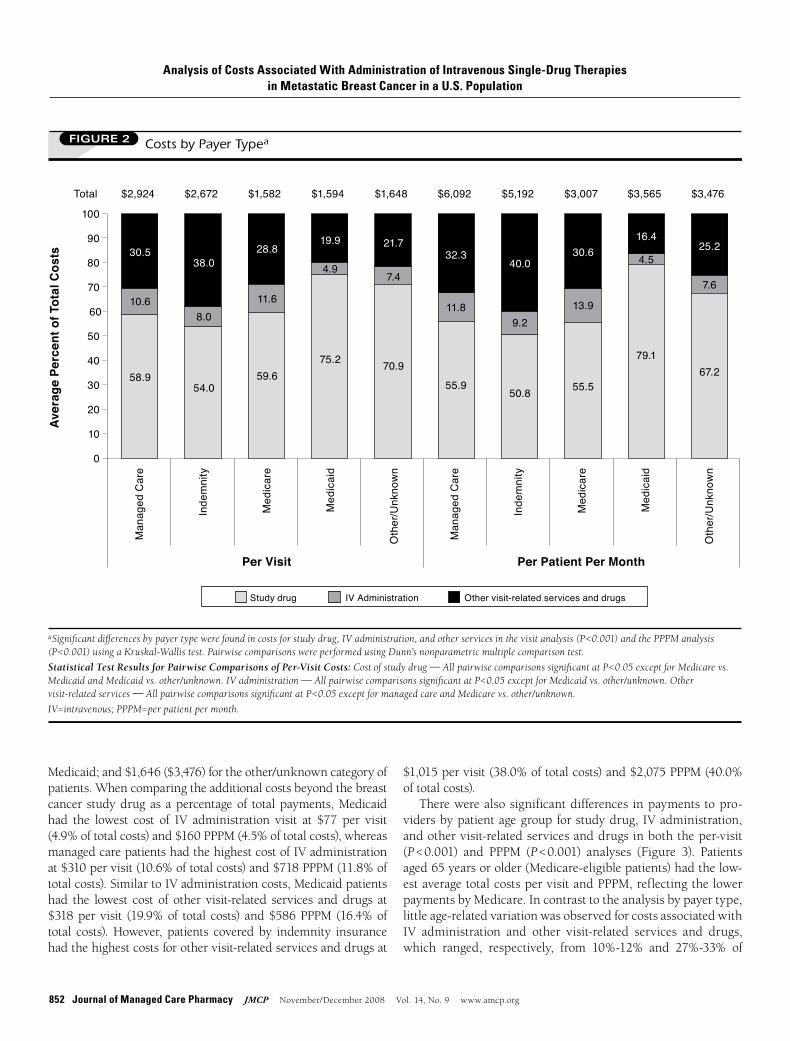
Payment by Payer Type and Patient AgeSignificantdifferencesincostsforstudydrug,IVadministration,andothervisit-relatedservicesanddrugswereobservedacrosspayertypesinboththeper-visit(P <0.001)andPPPM(P <0.001)analyses(Figure2).Theoverallmeanpaymentpervisit(PPPM)was $2,924 ($6,092) for managed care; $2,672 ($5,192) forindemnity; $1,582 ($3,007) for Medicare; $1,594 ($3,565) for
TABLE 4 Overall Costs Per Patient With Metastatic Breast Cancer (N = 828) by Visit and Month(continued from previous page)
PPPM
No. of Therapy-Monthsf Mean % of Total
% of Other Services
Provided at Visit SD Median
Total 3646 4,965.97 100 NA 3,841.00 4250
1.IVstudydrug 2,800.31 56.4 NA 2,399.00 2595
2.IVadministration(alldrugs) 567.80 11.4 NA 562.00 427
3.Othervisit-relatedservicesanddrugs 1,597.87 32.2 100 2,597.00 756
3a.Otherinjectabledrugsandconcomitantoraldrugsa 1,577.27 31.8 98.7 2,593.04 745
•Antihypercalcemicagents(e.g.,zoledronicacid) 319.42 6.4 20.0 586.41 0
•Colony-stimulatingfactors(e.g.,pegfilgrastim,filgrastim, epoetin,darbepoetin)
363.19 7.3 22.7 853.10 0
•Antineoplasticagents(bevacizumab)b 362.51 7.3 22.7 1,925.71 0
•Platinumagents(e.g.,carboplatin,oxaliplatin)b 172.12 3.5 10.8 703.18 0
•Chemotherapeuticagents(e.g.,irinotecan,vincristine)b 41.06 0.8 2.6 381.34 0
•Antiemeticagents(e.g.,palonosetron,granisetron) 159.28 3.2 10.0 435.90 0
•Salinesolution,dextrosewater 21.60 0.4 1.4 30.56 10
•Corticosteroids(e.g.,dexamethasone) 11.48 0.2 0.7 44.51 1
•Heparin 6.58 0.1 0.4 31.35 0
•Antihistamine(e.g.,diphenhydramine) 1.07 0.0 0.1 2.95 0
•Histamine-2receptorantagonists(e.g.,ranitidine) 1.03 0.0 0.1 3.83 0
•Iron 0.05 0.0 0.0 1.56 0
•Miscellaneous/unclassifiedagents 117.34 2.4 7.3 503.38 0
3b.Officevisit:evaluationandmanagementservicesc 11.37 0.2 0.7 74.19 0
3c.Suppliesandequipmentd 3.67 0.1 0.2 21.45 0
3d.Miscellaneousadministration-relatedservicese 5.56 0.1 0.3 38.06 0a Includes other injectable drugs administered and oral drugs administered as an initial dose for supportive care at the time of chemotherapy treatment during the breast cancer IV administration visit.b Breast cancer chemotherapy therapy was restricted to FDA-approved or National Comprehensive Cancer Network guideline-recommended agents. These anticancer agents were not indicated for breast cancer during study period.c Primarily includes physician assessments for chemotherapy administration or side effects related to chemotherapy including nausea and/or vomiting, fatigue, and pain; these codes include G9021-G9024 (chemotherapy assessment for nausea and vomiting) and G9029-G9032 (chemotherapy assessment for lack of energy [fatigue]). Side effects related to chemotherapy accounted for about 60% of total costs in this category.d Includes non-coring needles, sterile water, dressing pads, and infusion supplies.e Includes fluid collection and laboratories such as blood collection by venipuncture, metabolic panels, red and white blood cell count, and lactate dehydrogenase.fPatients receiving administrations of 2 or more different drugs at separate visits during the same month were included in the per-visit analysis (monotherapy during visit) but excluded from PPPM analysis (multiple drugs received during the month).Source: Medical Present Value Inc., Phynance database, Austin, Texas (www.mpv.com).IV = intravenous; NA = not applicable; PPPM = per patient per month.
www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 851
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
Drug bPatients
(n) cVisits
(n)
Total Study Drug IV AdministrationOther Visit-Related
Services a
Mean Costs
($) %
Mean Costs
($) %
Mean Costs
($) %
Mean Costs
($) %Per VisitAll Study Drugs 828 7406 2,477.32 100.0 1,462.80 59.0 251.74 10.2 762.78 30.8
Protein-boundpaclitaxel 19 94 4,346.72 100.0 3,044.46 70.0 361.29 8.3 940.97 21.6
Doxorubicin 72 288 3,145.11 100.0 1,944.22 61.8 274.99 8.7 925.90 29.4
Fluorouracil 28 186 3,100.79 100.0 32.10 1.0 495.57 16.0 2,573.13 83.0
Docetaxel 151 761 3,042.66 100.0 2,080.27 68.4 204.88 6.7 757.51 24.9
Non-protein-boundpaclitaxel 261 1450 2,803.64 100.0 1,213.84 43.3 352.97 12.6 1,236.83 44.1
Vinblastine 1 2 2,620.60 100.0 205.20 7.8 164.50 6.3 2,250.90 85.9
Trastuzumab 212 2416 2,526.41 100.0 1,976.27 78.2 213.66 8.5 336.48 13.3
Gemcitabine 137 973 2,249.60 100.0 1,116.12 49.6 289.11 12.9 844.37 37.5
Fulvestrant 119 517 1,660.29 100.0 917.49 55.3 110.37 6.6 632.43 38.1
Cyclophosphamide 17 21 1,531.68 100.0 94.33 6.2 326.17 21.3 1,111.19 72.5
Vinorelbine 103 698 1,270.38 100.0 431.03 33.9 185.71 14.6 653.64 51.5
Drug bPatients
(n)c
Therapy Months
(n)
Total Study Drug IV AdministrationOther Visit-Related
Services a
Mean Costs
($) %
Mean Costs
($) %
Mean Costs
($) %
Mean Costs
($) %PPPMAll Study Drugs 776 3646 4,965.97 100.0 2,800.31 56.4 567.80 11.4 1,597.87 32.2
Protein-boundpaclitaxel 17 34 12,441.07 100.0 8,205.76 66.0 1057.15 8.5 3,178.17 25.5
Fluorouracil 27 89 6,919.59 100.0 755.49 10.9 1000.39 14.5 5,163.70 74.6
Non-protein-boundpaclitaxel 241 679 6,323.25 100.0 2,944.86 46.6 856.41 13.5 2,521.98 39.9
Trastuzumab 174 1040 5,256.34 100.0 4,089.50 77.8 457.71 8.7 709.13 13.5
Docetaxel 137 426 5,090.27 100.0 3,606.53 70.9 373.96 7.3 1,109.78 21.8
Gemcitabine 117 378 4,883.22 100.0 2,596.41 53.2 690.72 14.1 1,596.09 32.7
Doxorubicin 66 258 3,734.52 100.0 2,194.48 58.8 372.25 10.0 1,167.79 31.3
Vinorelbine 87 234 3,712.88 100.0 1,377.73 37.1 581.98 15.7 1753.17 47.2
Cyclophosphamide 10 11 2,559.83 100.0 172.78 6.7 863.74 33.7 1523.31 59.5
Fulvestrant 109 497 1,750.87 100.0 1,035.05 59.1 113.55 6.5 602.27 34.4
Vinblastine 0 0 – – – – – – – –a Includes other injectable drugs and concomitant oral drugs (e.g., antihypercalcemic agents, colony-stimulating factors, anticancer agents, and antiemetic agents), evalua-tion and management services, supplies and equipment, and miscellaneous administration-related services.b Comparisons by study drug on costs for study drug, IV administration, and other services were statistically significant in both the IV-visit analysis (P < 0.001) and the PPPM analysis (P < 0.001) using a Kruskal-Wallis test. Vinblastine was excluded due to low number of visits. Pairwise comparisons were performed using Dunn’s nonpara-metric multiple comparison test.c Numbers in cells do not sum to total because some patients used more than 1 drug during the study period.Statistical Test Results for Per-Visit Pairwise Comparisons: Cost of study drug — All pairwise comparisons were significant at P < 0.05 except for cyclophosphamide vs. fluorouracil, cyclophosphamide vs. vinorelbine, and gemcitabine vs. non-protein-bound paclitaxel. Administrative costs — All pairwise comparisons were significant at P < 0.05 except for protein-bound paclitaxel vs. cyclophosphamide, protein-bound paclitaxel vs. fluorouracil, protein-bound paclitaxel vs. non-protein-bound paclitaxel, cyclophosphamide vs. docetaxel, cyclophosphamide vs. doxorubicin, cyclophosphamide vs. fluorouracil, cyclophosphamide vs. gemcitabine, cyclophosphamide vs. non-protein-bound paclitaxel, cyclophosphamide vs. trastuzumab, cyclophosphamide vs. vinorelbine, docetaxel vs. trastuzumab, docetaxel vs. vinorelbine, and doxorubicin vs. gemcitabine. Other visit-related services — All pairwise comparisons significant at P < 0.05 except for protein-bound paclitaxel vs. cyclophosphamide, protein-bound pacli-taxel vs. docetaxel, protein-bound paclitaxel vs. doxorubicin, protein-bound paclitaxel vs. fulvestrant, protein-bound paclitaxel vs. non-protein-bound paclitaxel, protein-bound paclitaxel vs. vinorelbine, cyclophosphamide vs. docetaxel, cyclophosphamide vs. doxorubicin, cyclophosphamide vs. fulvestrant, cyclophosphamide vs. gemcitabine, cyclophosphamide vs. non-protein-bound paclitaxel, cyclophosphamide vs. trastuzumab, cyclophosphamide vs. vinorelbine, docetaxel vs. vinorelbine, doxorubicin vs. fluo-rouracil, doxorubicin vs. gemcitabine, doxorubicin vs. non-protein-bound paclitaxel, fulvestrant vs. vinorelbine, and gemcitabine vs. non-protein-bound paclitaxel.IV = intravenous; MBC = metastatic breast cancer; PPPM = per patient per month.
TABLE 5 Costs by Drug Per Patient With Metastatic Breast Cancer—Per Visit and Per Month
852 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
Medicaid;and$1,646($3,476)fortheother/unknowncategoryofpatients.Whencomparingtheadditionalcostsbeyondthebreastcancer studydrugas apercentageof totalpayments,Medicaidhad the lowest cost of IV administration visit at $77 per visit(4.9%oftotalcosts)and$160PPPM(4.5%oftotalcosts),whereasmanagedcarepatientshadthehighestcostofIVadministrationat$310pervisit(10.6%oftotalcosts)and$718PPPM(11.8%oftotalcosts).SimilartoIVadministrationcosts,Medicaidpatientshad the lowest cost of other visit-related services anddrugs at$318pervisit (19.9%of total costs) and$586PPPM(16.4%oftotal costs).However, patients coveredby indemnity insurancehadthehighestcostsforothervisit-relatedservicesanddrugsat
$1,015pervisit(38.0%oftotalcosts)and$2,075PPPM(40.0%oftotalcosts).
Therewerealsosignificantdifferences inpaymentstopro-vidersbypatientagegroupforstudydrug,IVadministration, andothervisit-relatedservicesanddrugsinboththeper-visit(P <0.001) and PPPM (P <0.001) analyses (Figure 3). Patientsaged65yearsorolder(Medicare-eligiblepatients)hadthelow-estaveragetotalcostspervisitandPPPM,reflectingthelowerpaymentsbyMedicare.Incontrasttotheanalysisbypayertype,littleage-relatedvariationwasobservedforcostsassociatedwith IV administration and other visit-related services and drugs,which ranged, respectively, from 10%-12% and 27%-33% of
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
FIGURE 2 Costs by Payer Typea
aSignificant differences by payer type were found in costs for study drug, IV administration, and other services in the visit analysis (P<0.001) and the PPPM analysis (P<0.001) using a Kruskal-Wallis test. Pairwise comparisons were performed using Dunn’s nonparametric multiple comparison test.Statistical Test Results for Pairwise Comparisons of Per-Visit Costs: Cost of study drug � All pairwise comparisons significant at P<0.05 except for Medicare vs. Medicaid and Medicaid vs. other/unknown. IV administration � All pairwise comparisons significant at P<0.05 except for Medicaid vs. other/unknown. Other visit-related services � All pairwise comparisons significant at P<0.05 except for managed care and Medicare vs. other/unknown.IV=intravenous; PPPM=per patient per month.
Total $2,924 $2,672 $1,582 $1,594 $1,648 $6,092 $5,192 $3,007 $3,565 $3,476
Ave
rage
Per
cent
of T
otal
Cos
ts
100
90
80
70
60
50
40
30
20
10
0
38.030.5
10.6
58.954.0
8.0
28.8
11.6
59.675.2
4.9
19.9 21.7
7.4
70.9
55.9
11.8
32.340.0
9.2
50.8 55.5
13.9
30.616.4
4.5
79.167.2
7.6
25.2
Man
aged
Car
e
Inde
mni
ty
Med
icar
e
Med
icai
d
Oth
er/U
nkno
wn
Man
aged
Car
e
Inde
mni
ty
Med
icar
e
Med
icai
d
Oth
er/U
nkno
wn
Per Visit Per Patient Per Month
Study drug IV Administration Other visit-related services and drugs

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 853
totalper-visitcosts.In the sensitivity analysis limited to patients taking 2 or
more study drugs (combination therapy), results were similarto those observed for the monotherapy patients. Costs for IVadministrationandothervisit-relatedcostswere38.3%of totalcostpervisit(detaileddatanotshown),comparedwith41.0%for monotherapies.
■■ DiscussionTheobjectiveof this studywas toevaluate thecostsassociatedwith theadministrationof single-agent IV therapies inpatientswithMBC.Toestimatethecostcomponents,weexaminedmorethan800patientswithMBCwithmorethan7,400clinicvisitsfroma large,nationalpracticemanagementsystem.Costswere
analyzedonaper-visitandPPPMbasis.Theresultsshowedaver-agecontractedpaymentsof$2,477pervisitand$4,966PPPM,withIVadministrationaccountingfor10%-11%ofthetotalandcosts for other visit-related drugs, including antihypercalcemicagents, CSFs, and anticancer drugs being used off-label or forotherconditions,accountingfor31%-32%ofthetotalcost.
Thesecostsabovethedrugacquisitioncostfortheprincipalchemotherapydrugrepresenta significanteconomicburden topayers.EventhoughthisstudyfocusedonMBC,theseIVadmin-istrationandothervisit-relatedcostshavealsobeenreportedtocompriseasignificantportionoftotalcostsforearlystagebreastcancer.17Resultsofthepresentstudyarecomparabletothoseofapreviousstudybasedonadministrativeclaimsdataforlungcan-cer,whichreportednon-lungcancerdrugcostsassociatedwith
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
FIGURE 3 Costs by Patient Age Groupa
aSignificant differences by age group were found in costs for study drug, IV administration, and other services in the visit analysis (P<0.001) and the PPPM analysis (P<0.001) using a Kruskal-Wallis test. Pairwise comparisons were performed using Dunn’s nonparametric multiple comparison testStatistical Test Results for Per-Visit Pairwise Comparisons: Cost of study drug � All pairwise comparisons significant at P<0.05 except for groups aged (years) 45-54 vs. 55-64. Administrative costs � All pairwise comparisons significant at P<0.05 except for groups aged (years) less than 45 vs. 45-54, less than 45 vs. 55-64, 45-54 vs. 55-64, 45-54 vs. older than 75, and 65-74 vs. older than 75. Other visit-related services � All pairwise comparisons significant at P<0.05 except for groups aged (years) less than 45 vs. 45-54, less than 45 vs. 65-74, less than 45 vs. older than 75, 45-54 vs. 55-64, 45-54 vs. 65-74, 45-54 vs. older than 75, and 65-74 vs. older than 75.IV=intravenous, PPPM=per patient per month.
Total $2,628 $2,527 $2,754 $1,815 $1,676 $5,562 $5,271 $5,787 $3,129 $3,071
Ave
rage
Per
cent
of T
otal
Cos
ts
100.0
75.0
50.0
25.0
0.0
31.626.7
10.4
62.958.4
10.0
33.0
9.8
57.2 61.6
10.6
27.8 31.5
12.4
56.160.2
12.1
27.734.2
11.3
54.5 56.2
10.6
33.228.3
11.5
60.347.3
15.4
37.3
Per Visit Per Patient Per Month
<45 45-54 55-64 65-74 >74 <45 45-54 55-64 65-74 >74
Study drug IV Administration Other visit-related services and drugs

854 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
IVadministrationandrelatedservicestobe50%and41%oftotalpaymentspervisit,forsmallcelllungcancerandalltypesoflungcancer,respectively.15
In assessing the payment breakdown based on individual IV cancer drug, variability was observed for costs associatedwith administration andmore so for the costs associatedwithother visit-related services and drugs. Part of the variation inthese costs can be explained by the lower drug costs of thegeneric breast cancer therapies. For example,mean total costspervisitforgenericfluorouraciltreatmentwere$3,101,ofwhichdrug costs were only $32 (1.0%), costs for IV administrationwere $496 (16.0%), and costs for other visit-related servicesand drugs were $2,573 (83.0%). In contrast, the correspond-ing total cost ($4,347) breakdown for branded protein-boundpaclitaxelwas$3,044 (70.0%) for the studydrug,$361 (8.3%)for IV administration, and $941 (21.6%) for other services.For example, to avoid the occurrence of severe hypersensitiv-ity reactions, patients receiving non-protein-bound paclitaxelshould be premedicated with corticosteroids (such as dexam-ethasone), diphenhydramine, and H2-blockers such as raniti-dineorcimetidine;however, thecost for theseagents is low— $4.51per visit for corticosteroids, $0.47per visit for antihista-mines,and$0.39pervisitforH2-blockers.
It isalsopossiblethattheolderagentsmayhavebeencom-binedwithnewer,nonapproved,andnonrecommendedantican-ceragents.Forexample,bevacizumabwasneitherFDA-approvednorNCCN-recommendedasasingleagentforbreastcancerforthe studyperiod, andmayhavebeenusedmore frequently incombinationwitholderdrugs(e.g.,fluorouracil);thistreatmentpatternwouldresultinhighcostsforthe“othervisit-relatedser-vicesanddrugs”category.
Contracted allowed payments were also found to vary considerably by payer type. As expected, patients enrolled ingovernment-funded programs (Medicaid and Medicare) hadloweroverall payments thandidmanaged care and indemnityinsuredpatients.Thisdifferenceisprobablyattributabletodiffer-encesinreimbursementratesforadministrationofIVtherapiesbetweengovernment-fundedandprivateinsurance.Additionally,the analysis showed thatMedicaid patients incurred less than25%of totalpayments for additional costs abovebreast cancerstudydrugcosts,whereasmanagedcareandindemnityinsuredpatients incurred more than 40% of total payments for thesecosts.However, the percentage of costs other than breast can-cer study drug costs as a percentage of total costswas similar(40%pervisitand44%PPPM)inbothMedicareandmanagedcare. The patient age group analysis showed that, as in thepayertypeanalysis,patientswithMBCaged65yearsandolder (i.e., Medicare eligible) had the lowest overall payments. Fewdifferences in costs among the remaining age groups wereobserved.
AlthoughthisstudydoesnotcomparethetotalcostsoforaltherapieswiththoseofIVtherapiesformetastaticbreastcancer,
theincreasingavailabilityanduseofeffectiveoraltherapiesmighthelp provide cost offsets in the treatment of MBC. The costsspecificallyassociatedwithadministrationoftheIVtherapyaresubstantial and would clearly be avoided with the use of oralagents. Some of the other costs associatedwith the drugs and services provided at the time of IV administration (e.g., drugsusedtodiluteorreconstitutetheIVproductortomanagesideeffectsassociatedwithaparticularIVtherapy)maypossiblybeavoidedwiththeuseoforalagents.Evenifanall-IVcombinationtherapy is partially replacedwith an oral therapy (i.e., IVplus IVreplacedbyIVplusoral),someofthecostsassociatedwithIVadministration(dependsuponlengthoftimerequiredtoadmin-ister 2 or more IV therapies) might be avoided. However, theextentofcostavoidanceforservicesotherthanIVadministrationisunknownandwasnotmeasuredby this study.Wealsodidnotassessthepossibilityofanyaddedcostsassociatedwithoralagentssuchasnoncomplianceortreatmentofpossiblesideeffectswithoralagents(e.g.,gastrointestinalsideeffects).
Research evidence about costs of treatment with IV- administered versus oral chemotherapeutic drugs is limited. A recent non-peer-reviewed study delivered in a poster pre-sentation by Giuliani et al. evaluated the economic impact oftreatment with (a) oral capecitabine plus IV cisplatin versus (b) IV fluorouracil plus IV cisplatin among patients withadvanced gastric cancer in an Italian clinic.18 The costs of the 2regimenswereestimatedbasedontrialdataonactualdoseandthenumberofadministrations.Theadverseeventprofileswereusedtoestimatethecostsoftreatingtheseevents.Indirectcostsfortimeandtravelforstudydrugadministrationwereestimated.Theoralplus IV regimen received5.2 cyclesof therapyversus 4.6cyclesintheallIVregimen.Theoralcapecitabine-containingregimenhad17.6fewerhospitaloutpatientclinicvisitsthandidthe IV fluorouracil-containing regimen; the difference yieldeda net cost saving of approximately $2,686 per patient, but nostatisticaltestswerereported.Additionally,duetotheadditional 17.6 visits for infusion of fluorouracil, patients incurred sub-stantiallygreater indirect costs in termsof lost timeand travelexpenses. In a randomizedmulticenter study of patients withsmallcell lungcancer,Pashkoetal.compared(a) IVetoposideplusIVcisplatin(n=41)versus(b)oraletoposideplusIVcispla-tin (n=42) and reported a cost savings of 17% ($2,002 for the IVversus$1,653fortheoralregimen,adifferenceof$349)for thepatientsreceivingtheoralplusIVregimenbutdidnotreporttheresultsofstatisticaltests.19
AsdemonstratedbyGiulianietal.,inadditiontothepossibledirectcostsavingsofanoralcancertherapyfromapayerperspec-tive,theremaybeadditionalbenefitsfromapatientperspectiveintermsoftimeandindirectcostsavingsresultingfromfewerclinicvisitsforIVadministration.18Severalstudieshavedemonstratedpatient preferences for oral over IV cancer therapies, providedthatefficacyisnotcompromisedbyreceivinganoralagent.20-22 Fallowfield et al.20 found greater preference for daily tablets of

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 855
endocrine therapy over monthly IM injections among womenwith breast cancer. The major reasons for preference of oraltherapy includedconvenienceanddislike forneedles,althoughalmost49%ofpatientsindicatedthattheysometimesforgotandabout13%optednottotaketheirmedicationatcertaintimes.InastudybyLiuetal.,103patientswithcancerwereaskedabouttheir preference for oral or IV chemotherapy.21 Patients weretold initiallythat frequencyof laboratoryevaluationsandclinicvisitstoseeadoctorandrisksoftoxicitiesoforalorintravenousregimenswerecomparable.Almost90%ofpatientsexpressedapreference for oral chemotherapy. The predominant reason forthis result appeared to be problems with IV access (pain and difficulty starting an IV line) or convenience of administrationoutsideaclinicsetting.Gornasetal.reportedinaposterpresen-tation the resultsof a surveyof218 femalepatientswithMBCwhowereeligiblefororalcapecitabine;patientswereaskedaboutfactors that influenced their preference for oral therapy.23 Themost common reason for choosing oral capecitabine, cited by71%ofpatients,wasitsmoreconvenientformofdrugdelivery.Otherreasonsgivenincludedapreferencetoreceivedrugsina“morefriendlyway”andtostayathomeduringtherapy.However,unlikeinjectabledrugsthatarecoveredunderthemedicalben-efit,oraldrugstypicallywouldbecoveredunderthepharmacybenefit—hence, any impact on patient out-of-pocket expenseswouldneedtobeweighedagainstthesepatientbenefits.
LimitationsFirst,weexcludedcombinationdrugregimensfromthisanalysis.However,thismethodexcludedonly13%ofpatientswithMBCand27%ofIVvisitsrecordedinthedatabaseforthestudyperiod.Asensitivityanalysisexaminingcostsforthecombinationtherapyvisits showed results that were similar to those of the studyanalyses for monotherapy patients, including cost percentagesacross breast cancer IV therapy, IV administration, and otherdrugsandvisit-relatedcosts.FocusingonmonotherapyregimenspermittedustocaptureamajorityoftheIVvisitsandreportthecostcomponentsbytherapy.
Second,weobservedIVbreastcancertreatmentforonly11.7%ofthepatientswithMBC.SomeofthesepatientswithMBCwerereferredtofacilitiesthatwerenotcapturedinthedata.Third,theaccuracy of diagnostic coding of breast cancer andmetastasis,andothercodingoradministrativeerrors,mayhaveaffectedthevalidityof the cost estimates.For example, somepatientswithMBCmayhavenotreceivedasecondarymetastatic ICD-9-CMcodeandthuswerenotincludedinthisstudy.Fourth,giventhelimited time frameof the study, it ispossible that thepatients’
entire history of IV breast cancer therapymay not have beencaptured.However,thispotentiallimitationhasbeenaddressedbyusingmethodsthatarenotreliantoncompletepatienttherapyhistories but based on estimating costs per IV administrationvisitorcostpermonth,whicharelesspronetoloss-to-follow-upproblems.
Fifth,becausehealthcareservicesdeliveredatnon-IVadmin-istration visits were excluded in this study, it is possible thatother medical costs not measured in claims for the day of IVadministrationdifferbetweenpatientsonalternativetherapiesor insurance types. For example, if a patient returned to thefacilityatalaterdateforissuesrelatedtotheIVtherapybutanIVstudydrugwasnotadministeredduringthisvisit,thesecostswouldnotbecaptured.Furthermore,duetothenatureofadmin-istrativedata(wedidnothaveaccesstopatientmedicalrecords),only minimal patient information was available.We were notabletoexaminetheimpactofclinical(e.g.,diseaseseverityandcomorbidities) and nonclinical factors (e.g., formulary status ofdrugs)oncostsacrosstherapies.Also,althoughwewereabletomeasurethetotalamountthattheprovideriseligibletoreceivefrombothpayersandthepatientfromout-of-pocketpayments,wewereunabletodeterminewhatportionofthisaggregatedpay-mentwaspaidbythepatient.
Finally, although costs of IV administration are substantialandwouldclearlybeavoidedwiththeuseoforalagents,wedidnotdirectlycomparetotalcostsfortreatmentusingoralversusIVchemotherapeuticagents.Wealsodidnotassessthepossibilityofaddedcostsassociatedwithoralagents,suchasnoncomplianceortreatmentforgastrointestinalorothersideeffects.
■■ ConclusionsAmongpatientswithMBCtreatedwithanIV-administeredbreastcancerdrug,IVbreastcancerdrugsaccountedfor56%-59%oftotal cost, IV administration costs accounted for 10%-11% oftotalcosts,and31%-32%oftotalcostswereattributabletootherdrugs and services, primarily antihypercalcemic agents, CSFs,andanticancerdrugsbeingusedoff-labelorforotherconditions.Theuseof safeandeffectiveoralbreast cancer therapiescouldpotentiallyoffsetsomeofthecostsoftreatingpatientswithMBCbyreducingpersonneltime,clinicvisits,andsuppliesandequip-mentassociatedwithIVadministration.FutureresearchshouldincludeadirectcomparisonoforalversusIVdrugcostsinorderto investigate thesepotential implicationsaswell as togainanunderstandingofboththecostsandclinicalimplicationsoforalversusIVtherapieswhenadministeredassequentialorcombina-tiontherapy.
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population

856 Journal of Managed Care Pharmacy JMCP November/December 2008 Vol. 14, No. 9 www.amcp.org
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
DISCLOSURES
Funding for this study was provided by GlaxoSmithKline. Amonkar andSmith are employees of GlaxoSmithKline, and Stavrakas reported previ-ous service as a consultant to GlaxoSmithKline. Skonieczny is employedbyMedical Present Value Inc.,which provides services tomedical groups,includingmethodstomaximizerevenue. All authors contributed to the concept and study design. Skoniecznycollectedthedata,withassistancefromStavrakas.ThedatawereinterpretedprimarilybyKruseandAmonkar.ThemanuscriptwaswrittenprimarilybyKruse,Amonkar, andSmith.Kruse,Amonkar, andSmithmade the largestcontributiontomanuscriptrevision. TheauthorsacknowledgetheeditorialassistanceofMaijaM.Rothenberg,BalagotCommunications,Chicago,Illinois.
REfERENCES
1.AmericanCancerSociety.Cancer Facts & Figures 2008.Atlanta:American CancerSociety;2008.Availableat:www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf.AccessedSeptember15,2008.
2.In2004dollars,asreportedinBrownML,RileyGF,SchusslerN, EtzioniR.EstimatinghealthcarecostsrelatedtocancertreatmentfromSEER-Medicaredata.Medical Care.2002;40(Suppl8):IV-104–17.
3.SlamonDJ,Leyland-JonesB,ShakS,etal.Useofchemotherapyplus amonoclonalantibodyagainstHER2formetastaticbreastcancerthat overexpressesHER2.N Engl J Med.2001;344(11):783-92.
4.NationalComprehensiveCancerNetworks.The NCCN Breast Cancer Clinical Practice Guidelines in Oncology (Version 2.2008).NationalComprehensiveCancerNetwork,Inc.,2008.Availableat:www.nccn.org. AccessedAugust20,2008.
5.SharmaS,SaltzLB.Oralchemotherapeuticagentsforcolorectalcancer.Oncologist.2000;5:99-107.
6.O’NeillVJ,TwelvesCJ.Oralcancertreatment:developmentsin chemotherapyandbeyond.Br J Cancer.2002;87:933-37.
7.BornerM,ScheithauerW,TwelvesC,MarounJ,WilkeH.Answeringpatients’needs:oralalternativestointravenoustherapy.Oncologist. 2001;6(Suppl4):12-16.
8.DeMarioMD,RatainMJ.Oralchemotherapy:rationaleandfuture directions.J Clin Oncol.1998;16:2557-67.
9.Batlle,JF.ArranzEE.,deCastroCarpeno,J.,etal.Oralchemotherapy:potentialbenefitsandlimitations.Clin Transl Oncol.2004;6:335-40.Availableat:www.springerlink.com/content/8p000g35554xq621/. AccessedOctober9,2008.
10.FiremanBH,QuesenberryCP,SomkinCP,etal.Costofcareforcancerinahealthmaintenanceorganization.Health Care Financ Rev.1997;18:51-76.
11.LegorretaAP,BrooksRJ,LeibowitzAN,SolinLJ.Costofbreastcancertreatment.A4-yearlongitudinalstudy.Arch Intern Med.1996;156:2197-201.
12.TaplinSH,BarlowW,UrbanN,etal.Stage,age,comorbidity,anddirectcostsofcolon,prostate,andbreastcancercare.J Natl Cancer Ins. 1995;87(6):417-26.
13.RaoS,KubisiakJ,GildenD.Costofillnessassociatedwithmetastaticbreastcancer.Breast Cancer Res Treat.2004;83:25-32.
14.BachPB.Costsofcancercare:aviewfromtheCentersforMedicareandMedicaidServices.J Clin Oncol.2007;25:187-90.
15.DuhMS,WeinerJR,LefebvreP,NearyMP,SkarinAT.Costsassociatedwithintravenouschemotherapyadministrationinpatientswithsmallcelllungcancer:Aretrospectiveclaimsdatabaseanalysis.Curr Med Res Opin. 2008;24(4):967-74.
16.KruseGB,AmonkarMM,SkoniecznyD,SmithGL.Ananalysisof costsassociatedwithadministrationoftrastuzumab-basedcombination IVtherapiesinmetastaticbreastcancerpatientsinaU.S.population. Posterpresentedat:2007InternationalSocietyforPharmacoeconomics andOutcomesResearchAnnualMeeting;May19-23,2007;Arlington,VA.
17.KruseGB,AmonkarMM,SkoniecznyD,SmithGL.Costsofadministra-tionofintravenous(IV)therapiesinearlyversuslate-stagebreastcancerinaU.S.population.Posterpresentedat:2007AmericanSocietyofClinicalOncologyAnnualMeeting;June1-5,2007;Chicago,IL.
18.GiulianiG,FalconeA,GarrisonL.Economicevaluationofthecostoftreatingadvancedgastriccancer(AGC)withcapecitabine/cisplatin(XP)vs.5-FU/cisplatin(FP)regimensinanItaliansetting.Posterpresentedat:2007AmericanSocietyofClinicalOncologyAnnualMeeting;June1-5,2007;Chicago,IL.
19.PashkoS,JohnsonDM.Potentialcostsavingsoforalversusintravenousetoposideinthetreatmentofsmallcelllungcancer.Pharmacoeconomics. 1992;1(4):293-97.
20.FallowfieldL,AtkinsL,CattS,etal.Patients’preferenceforadministra-tionofendocrinetreatmentsbyinjectionortablets:resultsfromastudyofwomenwithbreastcancer.Ann Oncol.2006;17:205-10.
21.LiuG,FranssenE,FitchMI,WarnerE.Patientpreferencesfororal versusintravenouspalliativechemotherapy.J Clin Oncol.1997;15:110-15.
22.TwelvesC,GollinsS,GrieveR,SamuelL.Arandomisedcross-overtrialcomparingpatientpreferencefororalcapecitabineand5-fluorouracil/leucovorinregimensinpatientswithadvancedcolorectalcancer.Ann Oncol. 2006;17:239-45.
23.GornasM,SzczylikC.Oraltreatmentofmetastaticbreastcancer(MBC)withcapecitabine(X):Whatinfluencesthedecision-makingprocess?Posterpresentedat:2007AmericanSocietyofClinicalOncologyAnnualMeeting;June1-5,2007;Chicago,IL.
GREGORY B. KRUSE, MPH, MSc, is a Doctoral Candidate at The Wharton School, University of Pennsylvania, Philadelphia. MAYUR M. AMONKAR, PhD, is Director, Global Health Outcomes, GlaxoSmithKline, Collegeville, Pennsylvania. GREGORY SMITH, BA, is Director, Health Systems Strategies, GlaxoSmithKline, Philadelphia, Pennsylvania. DEAN C. SKONIECZNY, MBA, BSE, is Director, Medical Present Value Inc., Austin, Texas. SPYROS STAVRAKAS, PhD, is Partner, Market Strategies Group, Willow Grove, Pennsylvania.
AUTHOR CORRESPONDENCE: Gregory B. Kruse, MPH, MSc, The Wharton School, University of Pennsylvania, 3641 Locust Walk, Philadelphia, PA 19104. Tel: 215.868.2553; E-mail: [email protected]
Authors

www.amcp.org Vol. 14, No. 9 November/December 2008 JMCP Journal of Managed Care Pharmacy 857
Analysis of Costs Associated With Administration of Intravenous Single-Drug Therapies in Metastatic Breast Cancer in a U.S. Population
APPENDIX Supplemental Information on Study Drug Selection a
Drug fDA Approved for Breast CancerListed as Preferred Single IV Chemotherapeutic
Agent for MBC in NCCN GuidelinesProtein-boundpaclitaxel Yes Yes
Doxorubicin Yes Yes
Fluorouracil Yes Nob
Docetaxel Yes Yes
Non-protein-boundpaclitaxel Yes Yes
Vinblastine Yes No b
Trastuzumab Yes No c
Gemcitabine Yes Yes
Fulvestrant(IM) Yes No
Cyclophosphamide Yes No
Vinorelbine No Yes
Epirubicind Yes Yes
Thiotepad Yes No
Bleomycind No No
Mitoxantroned No Noa These 15 drugs were identified in the initial search of single-agent breast cancer drugs using a combination of sources, including the FDA Web site, NCCN guidelines, and cancer organization- and health-related Web sites to identify single-agent therapies for MBC. All other drugs not on the above list that may have been used for breast cancer during the study period without FDA approval for this indication or NCCN recommendation would fall into the “other drug” category and would represent “off-label” use (e.g., bevacizumab, irinotecan).b Listed as “other active chemotherapeutic agent” for treatment of MBC.c Considered as targeted therapy and hence may not be listed in the “preferred single chemotherapeutic agent” category by NCCN.d No patients in the present study cohort were administered the last 4 drugs. Epirubicin and thiotepa are FDA approved, and 1 drug (epirubicin) is listed in NCCN guidelines. Bleomycin and mitoxantrone are neither FDA approved nor NCCN recommended for breast cancer.FDA = U.S. Food and Drug Administration; IM = intramuscular; MBC = metastatic breast cancer; NCCN = National Comprehensive Cancer Network.