analysis of performance and utilization … · analysis of performance and utilization of kangaroo...
TRANSCRIPT
ANALYSIS OF PERFORMANCE AND UTILIZATION OF KANGAROO
MOTHER CARE FOR PRE-TERM AND LOW BIRTH WEIGHT BABIES
DECEMBER 2013
PREPARED FOR MAISHA PROGRAMME BY:
NYINISAELI K. PALLANGYO
FINAL REPORT
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page i
ACRONYMS AND ABBREVIATIONS
ANC Antenatal Care
DRCHCO District Reproductive and Child Health Coordinator
HMT Hospital Management Team
HR Human Resource
KMC Kangaroo Mother Care
LBW Low Birth Weight
MAISHA Mothers and Infants Safe Healthy Alive
MNCH District Reproductive and Child Health Coordinator
MOHSW Ministry of Health and Social Welfare
MOI/C Medical Officer In charge
N/A Not Applicable
RCHCO Reproductive and Child Health Coordinator
RMO Regional Medical Officer
RRCHCO Regional Reproductive and Child Health Coordinator
SC Save the Children
SC UK Save the children-United kingdom
SOW Scope of Work
TBC 1 Tanzania Broadcasting Corporation One
ToR Terms of Reference
TOT Training of Trainers
URT United Republic of Tanzania
USAID United States Agency for International Development
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page ii
TABLE OF CONTENTS
TABLE OF CONTENTS .........................................................................................................ii
LIST OF TABLES .................................................................................................................. vi
LIST OF FIGURES ............................................................................................................. viii
LIST OF ANNEXES ............................................................................................................ viii
1. INTRODUCTION ........................................................................................................... 1
1.1. BACKGROUND OF THE MAISHA PROGRAM .......................................................... 1
1.2. PROGRAM GOAL AND OBJECTIVES....................................................................... 1
1.3. PROGRAM AREAS .................................................................................................... 1
1.4. OBJECTIVE OF THE CONSULTANCY ASSIGNMENT ............................................. 2
1.5. SCOPE AND TASKS OF THE CONSULTANCY ASSIGNMENT ................................ 2
2. OVERVIEW OF PERFOMANCE ASSEMENT PROCEDURE ....................................... 4
2.1. SUPERVISION OF KMC ............................................................................................ 4
2.2. THE KMC SUPERVISION TEAM ............................................................................... 4
2.3. PREPARATION FOR SUPERVISION OF KMC ......................................................... 4
2.3.1. KMC Checklist ........................................................................................................ 4
2.3.2. Re-orientation to the KMC Supervision Checklist .................................................... 5
2.3.3. Assessment and Grading of a Performance Area ................................................... 5
2.3.4. General Health Facility Performance ...................................................................... 5
2.3.5. Provision of Feedback on Initial Assessment .......................................................... 5
2.3.6. Reporting of Assessment Results ........................................................................... 5
3. PERFORMANCE ASSESSMENT FOR MTWARA REGION ......................................... 6
3.1. BASIC INFORMATION ON MTWARA KMC ............................................................... 6
3.2. ASSESSMENT FROM SUPERVISION VISITS .......................................................... 6
3.2.1. First Supervision Visit on 06th August 2012 ............................................................ 6
3.2.2. Second Supervision Visit on 26th June 2012 .......................................................... 7
3.2.3. Average Performance from the two Supervision Visits ............................................ 7
3.2.4. Feedback from the Hospital Management ............................................................... 7
3.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MTWARA FACILITY ........... 8
4. PERFORMANCE ASSESSMENT FOR RUVUMA REGION .......................................... 9
4.1. BASIC INFORMATION ON RUVUMA KMC UNIT ...................................................... 9
4.2. ASSESSMENT FROM SUPERVISION VISITS .......................................................... 9
4.2.1. First Supervision Visit on 16th March 2011 ............................................................. 9
4.2.2. Second Supervision Visit on 15th August 2012 ..................................................... 10
4.2.3. Third Supervision Visit on 14th Feb 2013 .............................................................. 11
4.2.4. Average Performance from the three Supervision Visits ....................................... 12
4.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE RUVUMA FACILITY ......... 12
5. PERFORMANCE ASSESSMENT FOR IRINGA REGION ........................................... 14
5.1. BASIC INFORMATION ON IRINGA KMC ................................................................ 14
5.2. ASSESSMENT FROM SUPERVISION VISITS ........................................................ 14
5.2.1. First Supervision Visit on 17th March 2011 ........................................................... 14
5.2.2. Second Supervision Visit on 4th June 2012 .......................................................... 15
5.2.3. Third Supervision Visit on 11th Feb 2013 .............................................................. 16
5.2.4. Average Performance from the three Supervision Visits ....................................... 16
5.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE IRINGA FACILITY ............ 17
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page iii
6. PERFORMANCE ASSESSMENT FOR TABORA REGION ........................................ 18
6.1. BASIC INFORMATION ON TABORA KMC UNIT ..................................................... 18
6.2. ASSESSMENT FROM SUPERVISION VISITS ........................................................ 18
6.2.1. First Supervision Visit on 17th March 2011 ........................................................... 18
6.2.2. Second Supervision Visit on 19th June 2012 ........................................................ 18
6.2.3. Third Supervision Visit on 14th January 2013 ....................................................... 19
6.2.4. Average Performance from the three Supervision Visits ....................................... 19
6.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE TABORA FACILITY .......... 20
7. PERFORMANCE ASSESSMENT FOR MANYARA REGION ..................................... 21
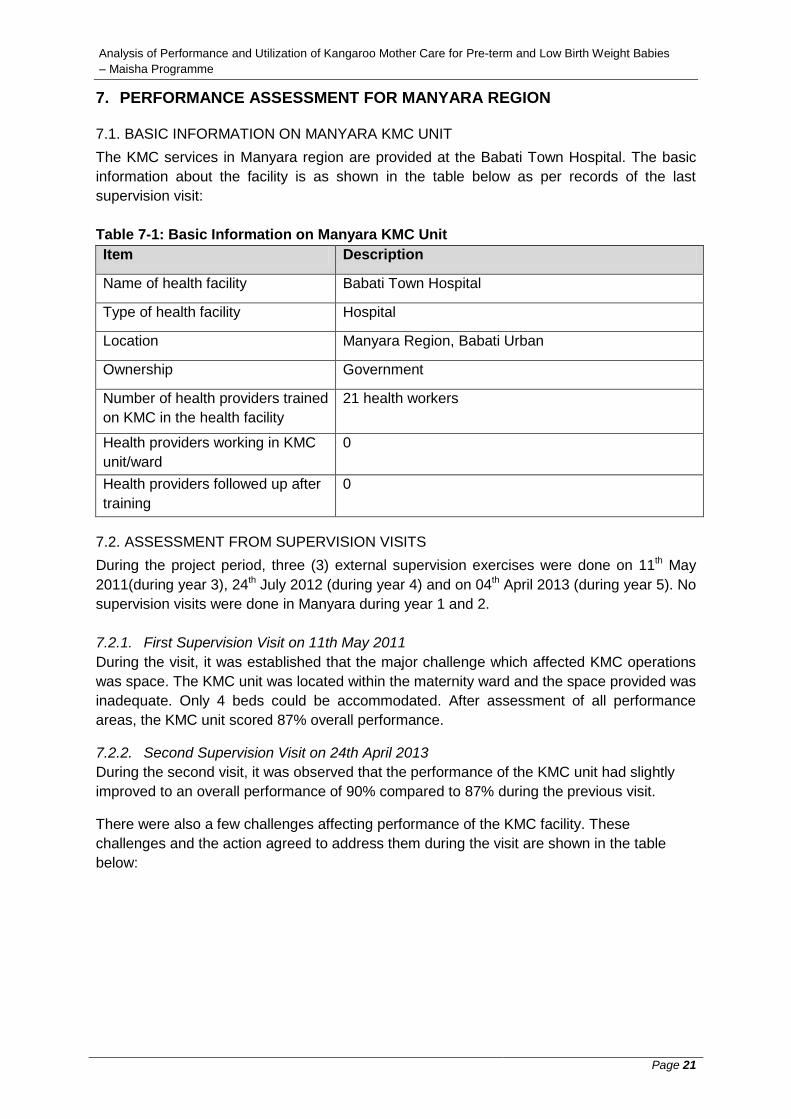
7.1. BASIC INFORMATION ON MANYARA KMC UNIT .................................................. 21
7.2. ASSESSMENT FROM SUPERVISION VISITS ........................................................ 21
7.2.1. First Supervision Visit on 11th May 2011 .............................................................. 21
7.2.2. Second Supervision Visit on 24th April 2013 ......................................................... 21
7.2.3. Third Supervision Visit on 24th April 2013 ............................................................. 22
7.2.4. Average Performance from the three Supervision Visits ....................................... 22
7.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MANYARA FACILITY ....... 23
8. PERFORMANCE ASSESSMENT FOR ARUSHA REGION ........................................ 24
8.1. BASIC INFORMATION ON ARUSHA KMC UNIT ..................................................... 24
8.2. ASSESSMENT FROM SUPERVISION VISITS ........................................................ 24
8.2.1. First Supervision Visit on 11th May 2011 .............................................................. 24
8.2.2. Second Supervision Visit on 12th July 2012.......................................................... 24
8.2.3. Third Supervision Visit on 02nd April 2012 ............................................................. 25
8.2.4. Average Performance from the three Supervision Visits ....................................... 25
8.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE ARUSHA FACILITY .......... 25
9. PERFORMANCE ASSESSMENT FOR KIGOMA REGION ......................................... 27
9.1. BASIC INFORMATION ON KIGOMA KMC UNIT ..................................................... 27
9.2. ASSESSMENT FROM SUPERVISION VISITS ........................................................ 27
9.2.1. First Supervision Visit on 17th May 2011 .............................................................. 27
9.2.2. Second Supervision Visit on 21st May 2012 .......................................................... 27
9.2.3. Third Supervision Visit on 16th January 2013 ........................................................ 28
9.2.4. Average Performance from the three Supervision Visits ....................................... 29
9.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KIGOMA FACILITY........... 29
10. PERFORMANCE ASSESSMENT FOR ZANZIBAR ................................................. 31
10.1. BASIC INFORMATION ON ZANZIBAR KMC UNIT .............................................. 31
10.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 31
10.2.1. First Supervision Visit on 23rd March 2012......................................................... 31
10.2.2. Second Supervision Visit on 06th November 2012 ............................................. 31
10.2.3. Average Performance from the two Supervision Visits ...................................... 32
10.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE ZANZIBAR FACILITY .... 32
11. PERFORMANCE ASSESSMENT FOR KAGERA ................................................... 34
11.1. BASIC INFORMATION ON KAGERA KMC UNIT ................................................. 34
11.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 34
11.2.1. First Supervision Visit on 14th May 2012 ............................................................ 34
11.2.2. Second Supervision Visit on 15th November 2012 ............................................ 35
11.2.3. Average Performance from the two Supervision Visits ...................................... 36
11.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KAGERA FACILITY ...... 36
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page iv
12. PERFORMANCE ASSESSMENT FOR MWANZA REGION .................................... 38
12.1. BASIC INFORMATION ON MWANZA KMC UNIT ................................................ 38
12.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 38
12.2.1. First Supervision Visit on 02nd May 2012 ........................................................... 38
12.2.2. Second Supervision Visit on 09th November 2012 ............................................. 39
12.2.3. Average Performance from the two Supervision Visits ...................................... 39
12.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MWANZA FACILITY ..... 40
13. PERFORMANCE ASSESSMENT FOR MARA REGION ......................................... 41
13.1. BASIC INFORMATION ON MARA KMC UNIT ...................................................... 41
13.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 41
13.2.1. First Supervision Visit on 07th May 2012 ............................................................ 41
13.2.2. Second Supervision Visit on 12th November 2012 .............................................. 42
13.2.3. Average Performance from the two Supervision Visits ...................................... 42
13.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MARA FACILITY ........... 43
14. PERFORMANCE ASSESSMENT FOR SHINYANGA REGION............................... 45
14.1. BASIC INFORMATION ON SHINYANGA KMC UNIT ........................................... 45
14.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 45
14.2.1. First Supervision Visit on 21st June 2012 ........................................................... 45
14.2.2. Second Supervision Visit on 09th January 2013 ................................................. 46
14.2.3. Average Performance from the two Supervision Visits ...................................... 46
14.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE SHINYANGA FACILITY 47
15. PERFORMANCE ASSESSMENT FOR SINGIDA REGION ..................................... 48
15.1. BASIC INFORMATION ON SINGIDA KMC UNIT ................................................. 48
15.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 48
15.2.1. First Supervision Visit on 14th June 2012 ........................................................... 48
15.2.2. Second Supervision Visit on 13th December 2012 ............................................. 49
15.2.3. Average Performance from the two Supervision Visits ...................................... 49
15.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE SINGIDA FACILITY ....... 50
16. PERFORMANCE ASSESSMENT FOR DODOMA REGION .................................... 51
16.1. BASIC INFORMATION ON DODOMA KMC UNIT ................................................ 51
16.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 51
16.2.1. First Supervision Visit on 11th June 2012 ........................................................... 51
16.2.2. Second Supervision Visit on 11th December 2012 ............................................. 52
16.2.3. Average Performance from the two Supervision Visits ...................................... 52
16.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE DODOMA FACILITY ..... 53
17. PERFORMANCE ASSESSMENT FOR TANGA REGION ....................................... 54
17.1. BASIC INFORMATION ON TANGA KMC UNIT .................................................... 54
17.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 54
17.2.1. First Supervision Visit on 30th March 2012 ........................................................ 54
17.2.2. Second Supervision Visit on 29th January 2013 ................................................ 54
17.2.3. Average Performance from the two Supervision Visits ...................................... 55
17.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE TANGA FACILITY ......... 55
18. PERFORMANCE ASSESSMENT FOR MBEYA REGION ....................................... 57
18.1. BASIC INFORMATION ON MBEYA KMC UNIT ................................................... 57
18.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 57
18.2.1. First Supervision Visit on 09th September 2011 ................................................ 57
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page v
18.2.2. Second Supervision Visit on 21st August 2012 .................................................. 57
18.2.3. Third Supervision Visit on 18th February 2013 ................................................... 58
18.2.4. Average Performance from the three Supervision Visits .................................... 58
18.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MBEYA FACILITY ......... 58
19. PERFORMANCE ASSESSMENT FOR RUKWA REGION ...................................... 60
19.1. BASIC INFORMATION ON RUKWA KMC UNIT ................................................... 60
19.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 60
19.2.1. First Supervision Visit on 23rd August 2012 ...................................................... 60
19.2.2. Second Supervision Visit on 20th February 2013 ............................................... 61
19.2.3. Average Performance from the two Supervision Visits ...................................... 61
19.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE RUKWA FACILITY ........ 62
20. PERFORMANCE ASSESSMENT FOR KILIMANJARO REGION ........................... 63
20.1. BASIC INFORMATION ON KILIMANJARO KMC UNIT ........................................ 63
20.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 63
20.2.1. First Supervision Visit on 26th July 2012 ........................................................... 63
20.2.2. Second Supervision Visit on 21st May 2013 ....................................................... 63
20.2.3. Average Performance from the two Supervision Visits ...................................... 64
20.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KILIMANJARO FACILITY
……………………………………………………………………………………………..65
21. PERFORMANCE ASSESSMENT FOR DAR ES SALAAM REGION ...................... 66
21.1. BASIC INFORMATION ON DAR ES SALAAM KMC UNIT ................................... 66
21.2. ASSESSMENT FROM SUPERVISION VISITS ..................................................... 66
21.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE DAR ES SALAAM
FACILITY ............................................................................................................................ 67
22. GENERAL PERFORMANCE OF THE 19 HEALTH FACILITIES PROVIDING KMC 68
22.1. RANKING OF REGIONAL PERFORMANCES ..................................................... 68
22.2. PERFORMANCE PER GRADING CRITERIA ....................................................... 69
23. PERFORMANCE PER ASSESSMENT AREAS ...................................................... 70
23.1. KMC SITE PHYSICAL SETTING .......................................................................... 70
23.2. KMC SERVICES ARE INSTITUTIONALIZED IN THE FACILITY .......................... 70
23.3. THE PROVIDER PREPARES THE MOTHER AND BABY FOR KMC .................. 70
23.4. THE PROVIDER ENSURES THAT THE BABY IS FED CORRECTLY ................. 71
23.5. THE PROVIDER MONITORS THE BABY RECEIVING KMC CORRECTLY ......... 71
23.6. INFECTION PREVENTION AND CONTROL PRACTICES ARE ADHERED ........ 71
23.7. THE MOTHER & HER FAMILY ARE SUPPORTED ............................................. 72
23.8. THE BABY IS DISCHARGED ACCORDING TO GUIDELINES ............................ 72
23.9. THE BABY RECEIVES REGULAR FOLLOW UPS ............................................... 72
23.10. KMC RE-ADMISSION CRITERIA FOLLOWED .................................................... 73
23.11. DISCONTINUATION OF BABIES FROM KMC ..................................................... 73
23.12. KMC SERVICES ARE KNOWN TO THE COMMUNITY ....................................... 74
23.13. MONITORING AND EVALUATION OF KMC SERVICES ..................................... 74
24. ANALYSIS OF DOCUMENTED DATA .................................................................... 75
24.1. BEST PERFORMERS IN DATA DOCUMENTATION ........................................... 75
24.2. ADMISSION OF LBW BABIES AT KMC SITES .................................................... 75
24.3. BABIES DISCHARGED FROM KMC WARD ........................................................ 75
24.4. DEATH OF BABIES AT KMC SITES .................................................................... 76
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page vi
24.5. MOTHERS ABSCONDED WITH THEIR PRE-TERM AND LBW BABIES FROM
KMC WARD ........................................................................................................................ 77
24.6. BABIES LOST TO FOLLOW UP ........................................................................... 77
24.7. PERIOD OF STAY OF BABIES AT KMC SITES ................................................... 78
25. CONCLUSION AND RECOMMENDATIONS ........................................................... 79
25.1. CONCLUSION ...................................................................................................... 79
25.2. RECOMMENDATIONS ............................................ Error! Bookmark not defined.
LIST OF TABLES
Table 1-1: Grading System for Assessment of Performance Area......................................... 5
Table 3-1: Basic Information on Mtwara KMC Unit ................................................................ 6
Table 3-2: Mtwara Challenges and Agreed Action ................................................................ 6
Table 3-3: Average Performance for Mtwara KMC Unit ......................................................... 7
Table 3-4: Information on Newborns including Pre-term and LBW Babies in Mtwara Facility 8
Table 4-1: Basic Information on Ruvuma KMC Unit .............................................................. 9
Table 4-2: Ruvuma Challenges and Agreed Action ............................................................. 11
Table 4-3: Average Performance for Ruvuma KMC Unit ..................................................... 12
Table 4-4: Information on Newborns including Pre-term and LBW Babies in Ruvuma Facility
........................................................................................................................................... 12
Table 5-1: Basic Information on Iringa KMC Unit ................................................................. 14
Table 5-2: Iringa Challenges and Agreed Action ................................................................. 15
Table 5-3: Average Performance for Iringa KMC Unit ......................................................... 16
Table 5-4: Information on Pre-term and LBW Babies in Iringa Facility ................................. 17
Table 6-1: Basic Information on Tabora KMC Unit .............................................................. 18
Table 6-2: Tabora Challenges and Agreed Action ............................................................... 19
Table 6-3: Average Performance for Tabora KMC Unit ....................................................... 19
Table 6-4: Information on Newborns including Pre-term and LBW Babies in Tabora Facility
........................................................................................................................................... 20
Table 7-1: Basic Information on Manyara KMC Unit ............................................................ 21
Table 7-2: Manyara Challenges and Agreed Action ............................................................ 22
Table 7-3: Average Performance for Manyara KMC Unit .................................................... 22
Table 7-4: Information on Newborns including Pre-term and LBW Babies in Manyara Facility
........................................................................................................................................... 23
Table 8-1: Basic Information on Arusha KMC Unit .............................................................. 24
Table 8-2: Arusha Challenges and Agreed Action ............................................................... 24
Table 8-3: Average Performance for Arusha KMC Unit ....................................................... 25
Table 8-4: Information on Newborns including Pre-term and LBW Babies in Arusha Facility
........................................................................................................................................... 26
Table 9-1: Basic Information on Kigoma KMC Unit ............................................................. 27
Table 9-2: Kigoma Challenges and Agreed Action .............................................................. 28
Table 9-3: Average Performance for Kigoma KMC Unit ...................................................... 29
Table 9-4: Information on Pre-term and LBW Babies in Kigoma Facility.............................. 30
Table 10-1: Basic Information on Zanzibar KMC Unit .......................................................... 31
Table 10-2: Average Performance for Zanzibar KMC Unit .................................................. 32
Table 10-3: Information on Pre-term and LBW Babies in Zanzibar Facility .......................... 32
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page vii
Table 11-1: Basic Information on Kagera KMC Unit ............................................................ 34
Table 11-2: Kagera Challenges and Agreed Action ............................................................. 34
Table 11-3: Average Performance for Kagera KMC Unit ..................................................... 36
Table 11-4: Information on Pre-term and LBW Babies in Kagera Facility ............................ 36
Table 12-1: Basic Information on Mwanza KMC Unit .......................................................... 38
Table 12-2: Mwanza Challenges and Agreed Action ........................................................... 38
Table 12-3: Average Performance for Mwanza KMC Unit ................................................... 39
Table 12-4: Information on Newborns including Pre-term and LBW Babies in Mwanza
Facility ................................................................................................................................ 40
Table 13-1: Basic Information on Mara KMC Unit ............................................................... 41
Table 13-2: Mara Challenges and Agreed Action ................................................................ 42
Table 13-3: Average Performance for Mara KMC Unit ........................................................ 43
Table 13-4: Information on Pre-term and LBW Babies in Mara Facility ............................... 43
Table 14-1: Basic Information on Shinyanga KMC Unit ....................................................... 45
Table 14-2: Shinyanga Challenges and Agreed Action ....................................................... 45
Table 14-3: Shinyanga HMT reaction to Outstanding Challenges ....................................... 46
Table 14-4: Average Performance for Shinyanga KMC Unit................................................ 46
Table 14-5: Information on Newborns and LBW Babies in Shinyanga Facility ..................... 47
Table 15-1: Basic Information on Singida KMC Unit ............................................................ 48
Table 15-2: Singida Challenges and Agreed Action ............................................................ 48
Table 15-3: Average Performance for Singida KMC Unit .................................................... 49
Table 15-4: Information on Newborns and Pre-term and LBW Babies in Singida Facility .... 50
Table 16-1: Basic Information on Dodoma KMC Unit .......................................................... 51
Table 16-2: Dodoma Challenges and Agreed Action ........................................................... 52
Table 16-3: Average Performance for Dodoma KMC Unit ................................................... 52
Table 16-4: Information on Newborns including Pre-term and LBW Babies in Dodoma
Facility ................................................................................................................................ 53
Table 17-1: Basic Information on Tanga KMC Unit ............................................................. 54
Table 17-2: Average Performance for Tanga KMC Unit ...................................................... 55
Table 17-3: Information on Newborns including Pre-term and LBW Babies in Tanga Facility
........................................................................................................................................... 56
Table 18-1: Basic Information on Mbeya KMC Unit ............................................................. 57
Table 18-2: Average Performance for Mbeya KMC Unit ...................................................... 58
Table 18-3: Information on Newborns including Pre-term and LBW Babies in Mbeya Facility
........................................................................................................................................... 59
Table 19-2: Sumbawanga Challenges and Agreed Action .................................................. 60
Table 19-2: Average Performance for Rukwa KMC Unit ..................................................... 61
Table 19-3: Information on Newborns including Pre-term and LBW Babies in Rukwa Facility
........................................................................................................................................... 62
Table 20-2: Average Performance for Kilimanjaro KMC Unit ............................................... 64
Table 20-3: Information on Newborns including Pre-term and LBW Babies in Kilimanjaro
Facility ................................................................................................................................ 65
Table 21-1: Basic Information on Dar es Salaam KMC Unit ................................................ 66
Table 21-2: Performance Assessment for Dar es Salaam KMC Unit ................................... 67
Table 21-3: Information on LBW Babies in Dar es Salaam Facility ...................................... 67
Table 22-1: Overall ranking of health facility performances in the 19 selected regions ........ 68
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page viii
Table 22-2: Performance per Grading Criteria..................................................................... 69
Table 23-1: Assessment of KMC Sites Physical Setting ...................................................... 70
Table 23-2: Assessment of Institutionalizing KMC Services in Facility ................................ 70
Table 23-3: Assessment in Preparing the Mother and Baby for KMC .................................. 70
Table 23-4: Assessment in Ensuring that the Baby is Fed Correctly ................................... 71
Table 23-5: Assessment in Provider Monitoring the Baby receive KMC Correctly ............... 71
Table 23-6: Assessment in Adherence to Infection Prevention and Control Practices ......... 71
Table 23-7: Assessment on the Mother and her Family being supported ............................ 72
Table 23-8: Assessment in discharging the Baby from the Facility ...................................... 72
Table 23-9: Assessment on Regular Follow Up to Babies ................................................... 73
Table 23-10: Assessment on Re-admission Criteria ............................................................ 73
Table 23-11: Assessment on Discontinuation of Babies ...................................................... 73
Table 23-11: Assessment on Awareness of KMC Services ................................................. 74
Table 23-11: Assessment on Monitoring and Evaluation ..................................................... 74
Table 24-1: Admission of LBW Babies at KMC Sites........................................................... 75
Table 24-2: Discharge of Babies from KMC Sites ............................................................... 76
Table 24-3: Death of Babies at KMC Sites .......................................................................... 76
Table 24-4: Abscondees at KMC Sites ................................................................................ 77
Table 24-5: Babies Lost to Follow up .................................................................................. 77
Table 24-2: Period of Stay of Babies at KMC Sites ............................................................. 78
LIST OF FIGURES
Figure 1-1: Map of the URT Showing Program Areas ........................................................... 2
LIST OF ANNEXES
ANNEX 1: Sample Checklist

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 1
1. INTRODUCTION
1.1. BACKGROUND OF THE MAISHA PROGRAM
The Mothers and Infants Safe Healthy Alive (MAISHA) Programme is a USAID funded
programme with Jhpiego as the lead, working with the Ministry of Health and Social Welfare
(MOHSW), Save the Children (SC) and several other partners. Through MAISHA support,
SC has taken a lead role in establishing Kangaroo Mother Care (KMC) in 19 regional sites in
Tanzania. This includes providing technical and materials support, and monitoring the
delivery of KMC services and the standard and quality of care for pre-term/low birth weight
babies.
The implementation of KMC in Tanzania started in July 2009 and was anticipated to end in
June 2013 but has been extended to December 2013, to mark the fifth year of funding.
1.2. PROGRAM GOAL AND OBJECTIVES
The overall goal of KMC implementation is to contribute towards reduction in newborn
deaths due to pre-term complications.
The main objective is to support the MOHSW to roll out KMC services in selected regions in
Tanzania mainland and Zanzibar through:
Awareness raising of hospital management teams to establish their support and
ownership of these services
Capacity development of health workers for provision of quality services, health
system strengthening, including provision of basic supplies, tracking the utilization of
KMC services and continuous mentoring of trained staff.
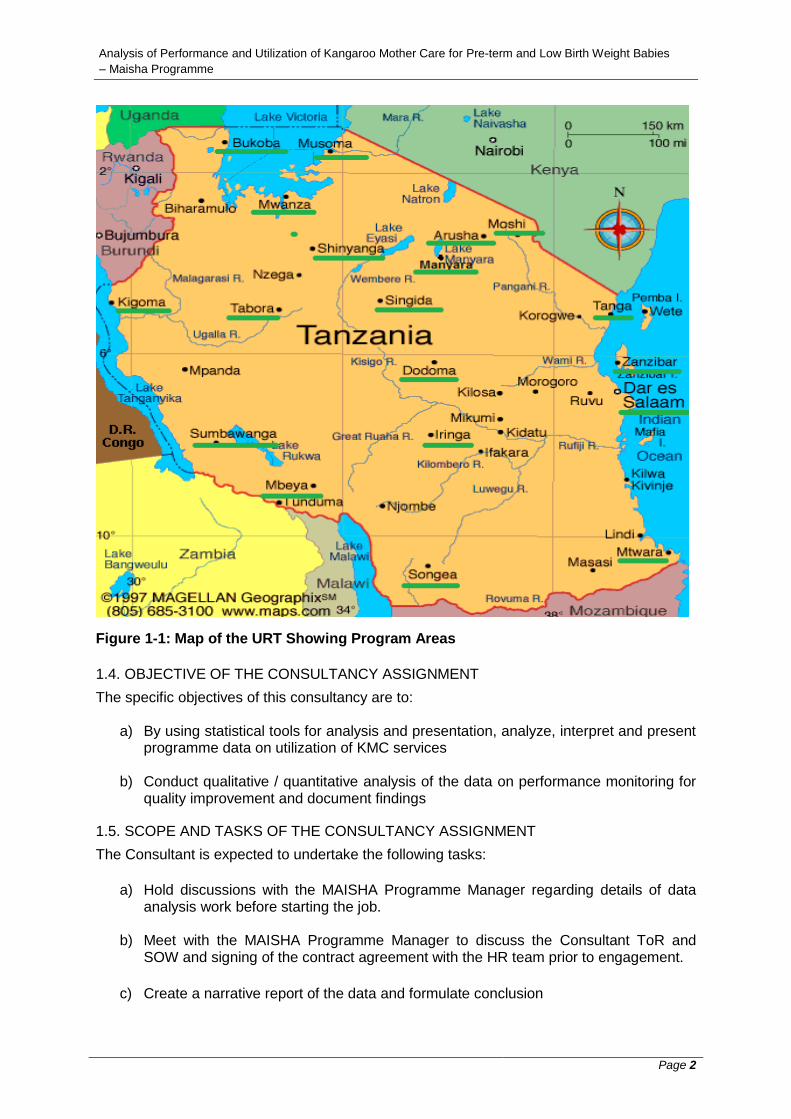
1.3. PROGRAM AREAS
In close collaboration with the MoHSW, SC has supported the establishment of KMC sites in
16 selected regional hospitals in Tanzania mainland namely: Mtwara, Arusha, Kilimanjaro,
Tanga, Manyara, Iringa, Ruvuma, Rukwa, Mara, Mwanza, Shinyanga, Tabora, Kigoma,
Kagera, Singida, Dodoma, two sites at health centre level in Mbeya and Dar-es-Salaam and
one in the maternity hospital in Zanzibar. In total, there are 19 sites as shown on the figure
below:
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 2
Figure 1-1: Map of the URT Showing Program Areas
1.4. OBJECTIVE OF THE CONSULTANCY ASSIGNMENT
The specific objectives of this consultancy are to:
a) By using statistical tools for analysis and presentation, analyze, interpret and present programme data on utilization of KMC services
b) Conduct qualitative / quantitative analysis of the data on performance monitoring for quality improvement and document findings
1.5. SCOPE AND TASKS OF THE CONSULTANCY ASSIGNMENT
The Consultant is expected to undertake the following tasks:
a) Hold discussions with the MAISHA Programme Manager regarding details of data analysis work before starting the job.
b) Meet with the MAISHA Programme Manager to discuss the Consultant ToR and SOW and signing of the contract agreement with the HR team prior to engagement.
c) Create a narrative report of the data and formulate conclusion
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 3
d) Prepare and submit a draft report of the data on the 10th of December 2013 to the Manager MNCH – SCI Tanzania for discussion, comments and further inputs towards final version.
e) The data analysis work submitted to Save the Children under this ToR is the property of Save the Children and cannot be submitted, distributed to or used by any other party, unless arranged otherwise;
f) The consultant is obligated to work within the required deadlines and be available to Save the Children for comments and corrections.
g) The final report should be submitted on the 15th of December 2013
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 4
2. OVERVIEW OF PERFOMANCE ASSEMENT PROCEDURE
2.1. SUPERVISION OF KMC
Supervision for KMC for pre-term and low birth weight babies was divided into two parts.
First part was the internal supervision done by the leaders of the health facilities and the
second part was the external supervision done by supervisors from outside the health
facility. Internal supervision was conducted monthly whereas the external supervision was
done four times a year (once every quarter). Supervision was done at health facilities
providing KMC services and health care providers trained on KMC provision.
2.2. THE KMC SUPERVISION TEAM
Internal supervision
The internal supervision team comprised of:
Medical Officer Incharge
Matron
Nurse and Doctor in charge of Post natal ward/Neonatal ward
Nurse Incharge of Labour ward
External supervision
The external supervision team comprised of supervisors from the following sections:
Representative from the Ministry of Health and social welfare
Representative from the Region
Representative from respective Council
Representative from Non-Governmental Organization (KMC partner)
2.3. PREPARATION FOR SUPERVISION OF KMC
Before conducting the supervision, the supervision team prepared the following:
schedule/supervision plan
set clearly defined objectives
communicated to the supervisee and administrative authority of the health
facility to be supervised.
supervisory tools; KMC checklist , equipment and supplies
reviewed previous supervision reports.
logistics and other resources.
2.3.1. KMC Checklist
The KMC checklist was the most important tool in the supervision exercise. The checklist
was used to assess 13 performance areas. A sample checklist is attached to this report as
Annex 1-1

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 5
2.3.2. Re-orientation to the KMC Supervision Checklist
The supervision team went through the criterion for verification of the performance areas one
by one. If the criterion had been followed, the supervisor would put a tick (√) on the Yes
column a tick (√) on a No column if the criterion had not been followed.
2.3.3. Assessment and Grading of a Performance Area
A grading system was used to estimate the percentage for Yes for each of the performance
areas assessed as shown in the table below:
Table 1-1: Grading System for Assessment of Performance Area
Assessment Percentage Score
Very good 67 – 100 3
Good 33 – 66 2
Weak Less than 33 1
2.3.4. General Health Facility Performance
There were 13 performance areas developed for assessment in each health facility. To get
the general performance of each health facility, the following procedure was followed:
all scores awarded for each performance area were summed up,
the total score was divided by 39, (13 performance areas x 3. Three (3) was
the highest score that could be awarded for any given performance area),
the result was multiplied by 100 to get a percentage and
the overall grading was then concluded as very good, good or weak as per
the grading system above.
2.3.5. Provision of Feedback on Initial Assessment
The supervisors provided feedback as soon as they completed the assessment to the health
providers who were assessed and to the in-charges of various sections (labour, postnatal
and paediatric wards, RCH, store, pharmacy, laboratory, matron/patron and medical officer
in-charge). Feedback was provided immediately on performance areas that had been done
well by congratulating and encouraging them to keep up. Feedback on poorly done areas
was given next with suggestions for improvement provided.
2.3.6. Reporting of Assessment Results
An immediate report summarizing the strengths, major problems or weaknesses, the actions
agreed (between the supervisor and health workers supervised) to solve weaknesses, time
frame, responsible person to ensure that the problems are solved was prepared and
submitted to the management of the hospital, SC and to the MoHSW.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 6
3. PERFORMANCE ASSESSMENT FOR MTWARA REGION
3.1. BASIC INFORMATION ON MTWARA KMC
The KMC services in Mtwara region are provided at the Ligula Regional Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit.
Table 3-1: Basic Information on Mtwara KMC Unit
Item Description
Name of health facility
Ligula Regional Hospital
Type of health facility
Hospital
Location Mtwara Region, Mtwara Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
25: 20 trained by MAISHA, 4 by the Municipal Council
and 1 by Ifakara Health Institute
Health providers working in KMC
unit/ward
2 registered nurses and 1 trained medical attendant
Health providers followed up after
training
4 registered nurses
3.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supportive supervision visits were done on 06th
August 2012 (during year 4) and on 26th June 2013 (during year 5). No supervision visits
were made in Mtwara during year 1, 2 and 3.
3.2.1. First Supervision Visit on 06th August 2012
During the first supervision visit, the following observations were made after assessment of
all performance areas of the KMC:
Generally the performance of the KMC services was very good, with an overall
assessed performance of 87%.
There were a few challenges affecting performance of the KMC facility. These
challenges and the action agreed to address them are shown in the table below:
Table 3-2: Mtwara Challenges and Agreed Action
Challenge Action
Space limitation resulting to increased rate of mothers seeking early discharge
The Medical Officer In charge (MOI/C) to create more space for KMC by breaking an existing wall
Staffing level; acute shortage of skilled staff affecting most of the hospital departments / sections including the KMC unit
The MOI/C to liaise with the Municipality for a possible solution
Reporting; late submission due to workload of staff (one skilled staff can be allocated to manage maternity ward - postnatal and antenatal including neonatal and KMC unit)
The MOI/C to solve this and ensure the computer is working properly
Increasing referrals from neighbouring areas that do not practice KMC e.g Likombe
The MOI/C to liaise with the Municipality for a possible solution

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 7
The population surrounding the regional hospital has not been sensitized on KMC services
3.2.2. Second Supervision Visit on 26th June 2012
During the second supervision visit, the following observations were made:
Generally the performance of the KMC services was still very good, with an overall
assessed performance of 100%.
Some challenges identified during the first supervision visit were being addressed
while others still remained un-addressed:
o Space limitation was still a problem although the HMT had increased the
occupancy from 4 to 6 beds.
o Staffing level was still not good
o Reporting was slowly improving
o Increasing referrals from neighbouring areas was still a challenge
3.2.3. Average Performance from the two Supervision Visits
The Mtwara KMC unit scored an average performance of 94% as shown in the table below:
Table 3-3: Average Performance for Mtwara KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 2 3 2.5
2 KMC services are institutionalized in the facility 3 3 3
3 The provider prepares the mother and the baby for KMC 3 3 3
4 The provider ensures that the baby is fed correctly 3 3 3
5 The provider monitors the baby receiving KMC correctly 3 3 3
6 Infection prevention and control practices are adhered 3 3 3
7 The mother of the baby receiving KMC and her family are supported
3 3 3
8 The baby is discharged from the facility according to guidelines
3
3 3
9 The baby receives regular follow ups 3 3 3
10 KMC readmission criteria 3 3 3
11 Discontinuation of babies from KMC 3 3 3
12 KMC services are known to the community 0 3 1.5
13 Monitoring and evaluation of KMC services 2 3 2.5
Total Score 34 39 36.5
Percentage 87% 100% 94%
3.2.4. Feedback from the Hospital Management
Internal supervisors appreciated the supervision visits done by SC jointly with the MoH,
which they said were very supportive and educative.
The hospital team confirmed to the team of external supervisors that they are able to
continue and sustain the initiative by themselves. The team is also committed to addressing
performance areas found with weaknesses.
The hospital team suggested a refresher training / orientation on KMC for the QI team before
they perform quality assessment exercise of the hospital services.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 8
3.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MTWARA FACILITY
During the project period, 1,515 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 841(56%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 79% were discharged successfully, 5% died, 4% absconded
while 2% were lost to follow up as shown in the table below.
Table 3-4: Information on Newborns including Pre-term and LBW Babies in Mtwara
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
1,515 N/A
LBW admitted in neonatal/postnatal ward
539 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
841 56% of total new born babies admitted at the facility
Total LBW babies 1,380 91% of total new born babies
admitted at the facility
LBW babies discharged from KMC ward
662 79% of LBW babies admitted in KMC
LBW babies died in KMC 39 5% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
34 4% of LBW babies admitted in KMC
LBW babies who are lost to follow
14 2% of LBW babies admitted in KMC
Average days of stay in KMC ward
5 N/A
From the above analysis of information collected from the Mtwara site, 92 (10%) of babies
admitted in the KMC ward are not accounted for. This shows that the site does not keep
proper records of KMC services. It is also evident that there is need for KMC services in the
region as 1,380 babies (91%) out of the 1515 new born babies were pre-term and LBW
babies.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 9
4. PERFORMANCE ASSESSMENT FOR RUVUMA REGION
4.1. BASIC INFORMATION ON RUVUMA KMC UNIT
The KMC services in Ruvuma region are provided at the Songea Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit.
Table 4-1: Basic Information on Ruvuma KMC Unit
Item Description
Name of health facility
Songea Regional Hospital
Type of health facility
Hospital
Location Songea Region, Songea Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
23: 21 health workers and 2 master trainers)
Health providers working in KMC
unit/ward
4
Health providers followed up after
training
2
4.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 16th March
2011(during year 3), 15th August 2012 (during year 4) and on 14th Feb 2013 (during year 5).
No supervision visits were done in Ruvuma during year 1 and 2.
4.2.1. First Supervision Visit on 16th March 2011
The objective of the first supervision visit in Ruvuma was to:
1. Assess if quality KMC services were being implemented
2. Assess if equipments supplied by SC are well utilized
3. Identify challenges faced and solutions for improvements
4. Provide support and mentoring to the gaps identified.
Location and setting of the KMC unit
The unit was within post natal ward, with 6 beds capacity and enough space for
nurse’s duty station within the centre. Warm, well ventilated but needs renovation.
No toilets were in the KMC room or running water to wash hands for infection
control.
The KMC room did not meet KMC standards, however it was reported that the site
was established as a temporary measure, awaiting relocation to a new maternity
ward under construction
KMC Implementation
Found 3 mothers in the ward, one of them practicing KMC but 2 of them not.
One among the 2 had twins both lying on bed and came for follow up.
KMC Register well utilized.
Contact mobile phone numbers of mothers discharged from the site were recorded.
Observations on feeding and counselling techniques done, some improvement on
guiding mothers needed.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 10
Utilization of KMC Equipments
Wall thermometer and digital scale in place and in good working condition.
A manual operated weighing scale to supplement the digital one when need arises
was in place.
Low reading thermometers are still out of stock at the medical stores department
Gaps and Challenges
Lack of KMC supervisory skills – training will be conducted this year, will be
considered during training of health workers from the new regions
No schedule for on duty personnel or maternity organization chart (In charge of
Maternity, KMC person) - Advised to have a schedule in the ward
Shortage of skilled personnel
Mothers don’t turn up for follow up due to long distance from their homes to the
hospital
Some mothers abscond due to lack of food or money to buy food as they come from
far. The hospital doesn’t provide food
Remarks from the KMC team at Ruvuma
Requested for training to district health providers at all levels to enable follow up of
those who default on KMC follow-up visits
Requested for more health workers to be trained on KMC to increase knowledge and
skills hence improve quality of services provided.
Suggestions from the Visiting Team:
The visiting team however advised them to:
Do on the job training – those trained on KMC to train others
Encourage mothers on continuous skin to skin
Conduct community awareness on KMC method to gain support.
The visiting team suggested that they will also increase the frequency of supportive
supervision and mentoring
4.2.2. Second Supervision Visit on 15th August 2012
During the second supervision visit, the following observations were made after assessment
of all performance areas of the KMC:
Generally the performance of the KMC services was very good, with an overall
assessed performance of 97%.The hospital management has given great support to
KMC services and the team working in KMC unit was very committed, ensuring that
the services delivered were at the required standard.
There were a few challenges affecting performance of the KMC facility. These
challenges and the action agreed to address them are shown in the table below:
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 11
Table 4-2: Ruvuma Challenges and Agreed Action
Challenge Action
Due to the increasing demand for KMC services, the present space was not adequate
The hospital management would make
efforts to secure funds from different sources
, part of it would be used to expand the room
for KMC services
Mothers seek for early discharge due to social problem
The KMC team needs to conduct continuous
awareness creation and counseling to both
parents
Lack of KMC awareness resulting to poor or no support to mothers from family members
The hospital management and the KMC
team needs to conduct continuous
awareness creation and counseling to both
parents
Mothers lost for follow up due to distance or social problems
The hospital management to provide air time
to the MOI/C and the matron for
communication to trace and/or remind
mothers lost for follow up
4.2.3. Third Supervision Visit on 14th Feb 2013
During the third supervision visit, the following observations were made:
Generally the performance of the KMC services was still very good, with an overall
assessed performance of 100%. The performance was impressing and they had
done very well in most of the key performance areas.
Most of the performance areas found with gaps during the second supervision visits
had been dealt with:
o In two occasions the KMC team had done awareness creation, advocacy on
KMC services through media. On 13th Feb 2013 they were visited by the
media (TBC 1 and Mwananchi newspaper) accompanied by a visitor from
SC UK. The visitor wanted to learn more about KMC and provided gifts to
the mothers for their babies.
o The KMC team had put in place a workable mechanism of tracking mothers
lost to follow up by involving other health facilities within and outside
Songea Municipality.
o Space limitation was still a challenge. Efforts by the hospital management to
secure funds from external sources did not work as expected. However,
there were little funds that have secured for renovation of the toilets.
o Mothers seeking early discharge due to social problem were still a challenge
and awareness creation was required.
Mothers at the KMC unit had good access to current news from a radio donated by
one nurse working at the KMC unit (Marcelina Wella).
The hospital management was providing continuous support for provision of quality
KMC e.g. giving extra duty allowance for nurses working extra hours; this had really
motivated the staff.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 12
4.2.4. Average Performance from the three Supervision Visits
During the first visit, the checklist for assessment of performance areas from the MOHSW
was not ready. It was ready during the second and third visits. Based on the last two visits,
the Ruvuma KMC unit scored an average performance of 99% as shown in the table below:
Table 4-3: Average Performance for Ruvuma KMC Unit
No. Performance Area 1st Visit
2nd Visit
3rd Visit
Average
1 KMC physical setting
Checklis
t fo
r assessm
ent
had n
ot b
een p
rep
are
d
3 3 3
2 KMC services are institutionalized in the facility 3 3 3
3 The provider prepares the mother and the baby for KMC
3 3 3
4 The provider ensures that the baby is fed correctly 3 3 3
5 The provider monitors the baby receiving KMC correctly
3 3 3
6 Infection prevention and control practices are adhered
3 3 3
7 The mother of the baby receiving KMC and her family are supported
3 3 3
8 The baby is discharged from the facility according to guidelines
3 3 3
9 The baby receives regular follow ups 3 3 3
10 KMC readmission criteria 3 3 3
11 Discontinuation of babies from KMC 3 3 3
12 KMC services are known to the community 2 3 2.5
13 Monitoring and evaluation of KMC services 3 3 3
Total Score 38 39 38.5
Percentage 0% 97% 100% 99%
4.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE RUVUMA FACILITY
During the project period, 1,978 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 768(39%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 69% were discharged successfully, 8% died, 3% were
absconded while 10% were lost to follow as shown in the table below.
Table 4-4: Information on Newborns including Pre-term and LBW Babies in Ruvuma
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
1,978 N/A
LBW admitted in neonatal/postnatal ward
602 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
768 39% of total new born babies admitted at the facility
Total LBW babies 1,370 69% of total new born babies
admitted at the facility
LBW babies discharged from KMC ward
530 69% of LBW babies admitted in KMC
LBW babies died in KMC 61 8% of LBW babies admitted in KMC

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 13
LBW babies absconded from KMC ward
22 3% of LBW babies admitted in KMC
LBW babies who are lost to follow
75 10% of LBW babies admitted in KMC
Average days of stay in KMC ward
7 N/A
Just like for Mtwara region, 80 (10%) of babies admitted in the Ruvuma KMC unit are not
accounted for. This shows that the site does not keep proper records of KMC services. It is
also evident that there is need for KMC services in the region as 1,370 babies (69%) out of
the 1978 new born babies were pre-term and LBW babies.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 14
5. PERFORMANCE ASSESSMENT FOR IRINGA REGION
5.1. BASIC INFORMATION ON IRINGA KMC
The KMC services in Iringa region are provided at the Iringa Regional Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 5-1: Basic Information on Iringa KMC Unit
Item Description
Name of health facility
Iringa Regional Hospital
Type of health facility
Hospital
Location Iringa Region, Iringa Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
21: 20 health workers have formal training, and 1
master trainer
Health providers working in KMC
unit/ward
1
Health providers followed up after
training
4
5.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 17th March
2011(during year 3), 04th June 2012 (during year 4) and on 11th Feb 2013 (during year 5). No
supervision visits were done in Iringa during year 1 and 2.
5.2.1. First Supervision Visit on 17th March 2011
The objective of the first supervision visit in Iringa was to:
1. Assess if quality KMC services were being implemented
2. Assess if equipments supplied by SC are well utilized
3. Identify challenges faced and solutions for improvements
4. Provide support and mentoring to the gaps identified.
Location and setting of the KMC unit
There were 2 small KMC rooms located in Maternity ward. The rooms had 2 beds
each, minimal warmth and too small for a heater provided by SC.
The KMC rooms had containers for water to wash hands to prevent infection but
had no water neither soap
The KMC rooms did not meet KMC standards
Construction of a maternity ward was in plan, when ready the site would be shifted
KMC Implementation
During the visit, mothers were in the ward, some with babies in KMC position, but
some not.
Observations on feeding and counselling techniques for quality KMC service
implementation was not done, the focal person was assisting the doctor on a major
round
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 15
Poor recording of data
Poor filing system
Utilization of KMC Equipments
Wall thermometer to monitor room temperature was not utilized.
Challenges
Lack of KMC supervisory skills; training would be conducted in the same year during
training of health workers from the new regions
Shortage of skilled staff
Mothers do not turn up for follow up due to long distance from their homes to the
hospital
Remarks from the visiting team
The team gave a feedback to the hospital matron. The matron promised to deal with
the problems identified
The team advised on the job training – those trained on KMC to train others
The team encourage mothers on continuous positioning babies skin to skin
The team advised the health workers to continue with Community awareness on
KMC method to gain support.
The visiting team committed themselves to increase the frequency of supportive
visits if budget allowed
5.2.2. Second Supervision Visit on 4th June 2012
During the second supervision visit, the following observations were made after assessment
of all performance areas of the KMC:
General performance of the KMC unit was improving compared to the situation
observed during the first visit on 17th March 2011. The overall assessed performance
was rated at 79% although cleanliness of KMC rooms was not being observed.
There were a few challenges affecting performance of the KMC facility. These
challenges and the action agreed to address them are shown in the table below:
Table 5-2: Iringa Challenges and Agreed Action
Challenge Action
Space limitation In charge of Paediatric ward, Sr. Joyce Mbamba to make a close follow up
Lack of feeding tubes and graduated cups
Focal person to continue improvising cups for feeding Lack of support from HMT- trained staff on
KMC are not allocated to KMC unit
Matron to ensure that at least two trained staff allocated to work at KMC site during reshuffle
Communication gap between staff and HMT. KMC staff were not aware of the visit
HMT to address and look for appropriate solution on the existing communication gap
The community not well informed on KMC concept as a result of this men are reluctant to provide support to their wives enrolled at KMC units
HMT to ensure that KMC concept reaches the community through local media
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 16
Hospital not providing food to all patients as a result of this, patients with no support from relatives are not willing to continue with KMC
KMC focal persons to be proactive in providing names of mother who require food assistance through the existing system
Mothers lost for follow up due to distance and lack of bus fare
HMT to set a mechanism for tracing mothers who are lost to follow up (example providing airtime to KMC focal persons) Shortage of staff and lack of commitment
to implement quality KMC
KMC to be integrated into other hospital services, and be recognized.
5.2.3. Third Supervision Visit on 11th Feb 2013
During the third supervision visit, it was observed that communication gap still continued to
exist with internal supervisors not being informed about the supervision visits on time by the
hospital management. General cleanliness of the KMC rooms, adherence to infection
prevention and control guidelines were also not being observed. Lack of public awareness
on KMC concept, staffing issues and poor follow up on mothers still persist. There is need
for commitment by the hospital management to support KMC services in order for KMC
quality services in the region to be realized. The overall assessment had however improved
to 92% compared to the previous assessment of 79%. The visiting team, however, are of the
opinion that the rated performance of 92% did not represent the actual situation on the
ground.
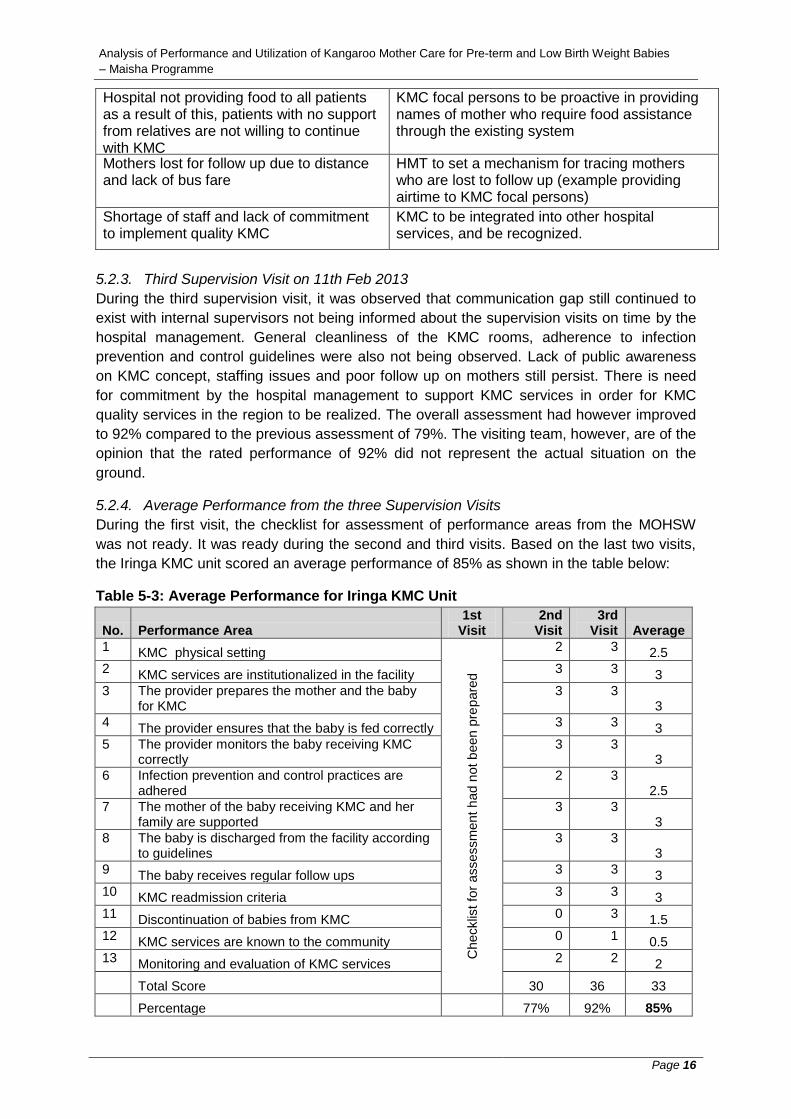
5.2.4. Average Performance from the three Supervision Visits
During the first visit, the checklist for assessment of performance areas from the MOHSW
was not ready. It was ready during the second and third visits. Based on the last two visits,
the Iringa KMC unit scored an average performance of 85% as shown in the table below:
Table 5-3: Average Performance for Iringa KMC Unit
No. Performance Area 1st
Visit 2nd
Visit 3rd
Visit Average
1 KMC physical setting
Checklis
t fo
r assessm
ent
had n
ot b
een p
rep
are
d
2 3 2.5
2 KMC services are institutionalized in the facility
3 3 3
3 The provider prepares the mother and the baby for KMC
3 3 3
4 The provider ensures that the baby is fed correctly
3 3 3
5 The provider monitors the baby receiving KMC correctly
3 3 3
6 Infection prevention and control practices are adhered
2 3 2.5
7 The mother of the baby receiving KMC and her family are supported
3 3 3
8 The baby is discharged from the facility according to guidelines
3 3 3
9 The baby receives regular follow ups
3 3 3
10 KMC readmission criteria 3 3 3
11 Discontinuation of babies from KMC
0 3 1.5
12 KMC services are known to the community
0 1 0.5
13 Monitoring and evaluation of KMC services
2 2 2
Total Score 30 36 33
Percentage 77% 92% 85%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 17
5.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE IRINGA FACILITY
During the project period, 2,808 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 856 (30%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 68% were discharged successfully, 3% died, 0% absconded
while 3% were lost to follow up as shown in the table below.
Table 5-4: Information on Pre-term and LBW Babies in Iringa Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
2,808 N/A
LBW admitted in neonatal/postnatal ward
657 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward 856 30% of total new born babies admitted at the facility
Total LBW babies 1,513 54% of total new born babies
admitted at the facility
LBW babies discharged from KMC ward
581 68% of LBW babies admitted in KMC
LBW babies died in KMC 28 3% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
4 0% of LBW babies admitted in KMC
LBW babies who are lost to follow 25 3% of LBW babies admitted in KMC
Average days of stay in KMC ward 7 N/A
From the results above, 218 (26%) of babies admitted in the Iringa KMC unit are not
accounted for. This shows that the site does not keep proper records of KMC services.
There is demand for KMC services in the region as almost half (54%) of newborn babies
were Pre-term and LBW.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 18
6. PERFORMANCE ASSESSMENT FOR TABORA REGION
6.1. BASIC INFORMATION ON TABORA KMC UNIT
The KMC services in Tabora region are provided at the Kitete Regional Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 6-1: Basic Information on Tabora KMC Unit
Item Description
Name of health facility
Kitete Regional Hospital
Type of health facility
Hospital
Location Tabora Region, Tabora Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 20 health workers, 2 KMC master trainers
Health providers working in KMC
unit/ward
2
Health providers followed up after
training
0
6.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 20th May
2011(during year 3), 19th June 2012 (during year 4) and on 14th January 2013 (during year
5). No supervision visits were done in Tabora during year 1 and 2.
6.2.1. First Supervision Visit on 17th March 2011
During the first supervision visit in Tabora, it was observed that the KMC unit was not
performing well and there was no commitment and support from the hospital management. It
was also observed that there was a serious gap between the hospital management and
staff. Record keeping was also observed to be poor. After assessment of all performance
areas, the KMC unit scored 51% overall performance.
6.2.2. Second Supervision Visit on 19th June 2012
During the second visit, it was observed that there was a great improvement in providing
KMC services compared to the previous assessment done on 20th May 2011. The KMC
room was found clean and neat. Although the KMC staff at the site had not received any
formal KMC training, with the little knowledge they had got through peers had helped them to
make notable changes in the unit. After assessment of all performance areas, the KMC unit
scored 85% overall performance compared to 51% in the first visit.
There were a few challenges affecting performance of the KMC facility. These challenges
and the action suggested to address them are shown in the table below:

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 19
Table 6-2: Tabora Challenges and Agreed Action
Challenge Action
The food provided by the hospital was not sufficient and was also not of good quality
The hospital management to be consulted on the provision of quality and sufficient food for patients including mothers in KMC unit who have no relatives or come from far. Most of the staff were not oriented on
basic KMC concepts
Implementation of KMC services needs to be
institutionalized (orient more staff during
continuing education sessions) and use of media
for mass communication
Space limitation for KMC services
KMC to be integrated into other hospital services,
and be recognized
Staff rotation affect quality of service and the overall KMC implementation
Matron to ensure that staff trained on KMC are
retained in the KMC unit
6.2.3. Third Supervision Visit on 14th January 2013
During the third visit, performance dropped suddenly from 85% to 43%. The KMC team
seemed to have no training on KMC services. From their assessment, the external
supervisors concluded that the KMC staff received little support from the hospital
management. A discussion to analyze the situation and identify factors that contributed to
declining performance was held with the MOI/C. The HMT agreed with the assessment
results of the external supervisors and committed themselves to:
Allocate 2 trained personnel to manage the KMC unit and work in collaboration with the KMC trainers (Dr. Ikandilo and the RCHCO Ms. Mbago)
Ensure that documentation of pre-term data and reporting is done appropriately and timely
Conduct internal supervision of the unit as per the MoHSW KMC guidelines
6.2.4. Average Performance from the three Supervision Visits
Based on the three visits, the Tabora KMC unit scored an average performance of 60% as
shown in the table below:
Table 6-3: Average Performance for Tabora KMC Unit
No. Performance Area 1st
Visit 2nd
Visit 3rd
Visit Average
1 KMC physical setting 2 2 3 2.3
2 KMC services are institutionalized in the facility 2 2 1 1.7
3 The provider prepares the mother and the baby for KMC 2 3 3 2.7
4 The provider ensures that the baby is fed correctly 1 3 2 2.0
5 The provider monitors the baby receiving KMC correctly 0 3 0 1.0
6 Infection prevention and control practices are adhered 3 2 2 2.3
7 The mother of the baby receiving KMC and her family are supported
3 3 3 3.0
8 The baby is discharged from the facility according to guidelines
2 3 0 1.7
9 The baby receives regular follow ups 0 3 0 1.0
10 KMC readmission criteria 3 3 0 2.0

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 20
11 Discontinuation of babies from KMC 2 2 0 1.3
12 KMC services are known to the community 0 2 2 1.3
13 Monitoring and evaluation of KMC services 0 2 1 1.0
Total Score 20 33 17 23.3
Percentage 51% 85% 44% 60%
6.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE TABORA FACILITY
During the project period, 2,431 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 803 (33%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 69% were discharged successfully, 6% died, 4% absconded
while 4% were lost to follow up as shown in the table below.
Table 6-4: Information on Newborns including Pre-term and LBW Babies in Tabora
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
2,431 N/A
LBW admitted in neonatal/postnatal ward
501 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
803 33% of total new born babies admitted at the facility
Total LBW babies 1,304 54% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
557 69% of LBW babies admitted in KMC
LBW babies died in KMC 47 6% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
30 4% of LBW babies admitted in KMC
LBW babies who are lost to follow 30 4% of LBW babies admitted in KMC
Average days of stay in KMC ward 5 N/A
From the results above, 139 (17%) of babies admitted in the KMC unit are not accounted for.
This shows that the site does not keep proper records of KMC services. There is demand for
KMC services in the region as almost half (54%) of new born babies were LBW babies.
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 21
7. PERFORMANCE ASSESSMENT FOR MANYARA REGION
7.1. BASIC INFORMATION ON MANYARA KMC UNIT
The KMC services in Manyara region are provided at the Babati Town Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 7-1: Basic Information on Manyara KMC Unit
Item Description
Name of health facility
Babati Town Hospital
Type of health facility
Hospital
Location Manyara Region, Babati Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
21 health workers
Health providers working in KMC
unit/ward
0
Health providers followed up after
training
0
7.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 11th May
2011(during year 3), 24th July 2012 (during year 4) and on 04th April 2013 (during year 5). No
supervision visits were done in Manyara during year 1 and 2.
7.2.1. First Supervision Visit on 11th May 2011
During the visit, it was established that the major challenge which affected KMC operations
was space. The KMC unit was located within the maternity ward and the space provided was
inadequate. Only 4 beds could be accommodated. After assessment of all performance
areas, the KMC unit scored 87% overall performance.
7.2.2. Second Supervision Visit on 24th April 2013
During the second visit, it was observed that the performance of the KMC unit had slightly
improved to an overall performance of 90% compared to 87% during the previous visit.
There were also a few challenges affecting performance of the KMC facility. These
challenges and the action agreed to address them during the visit are shown in the table
below:
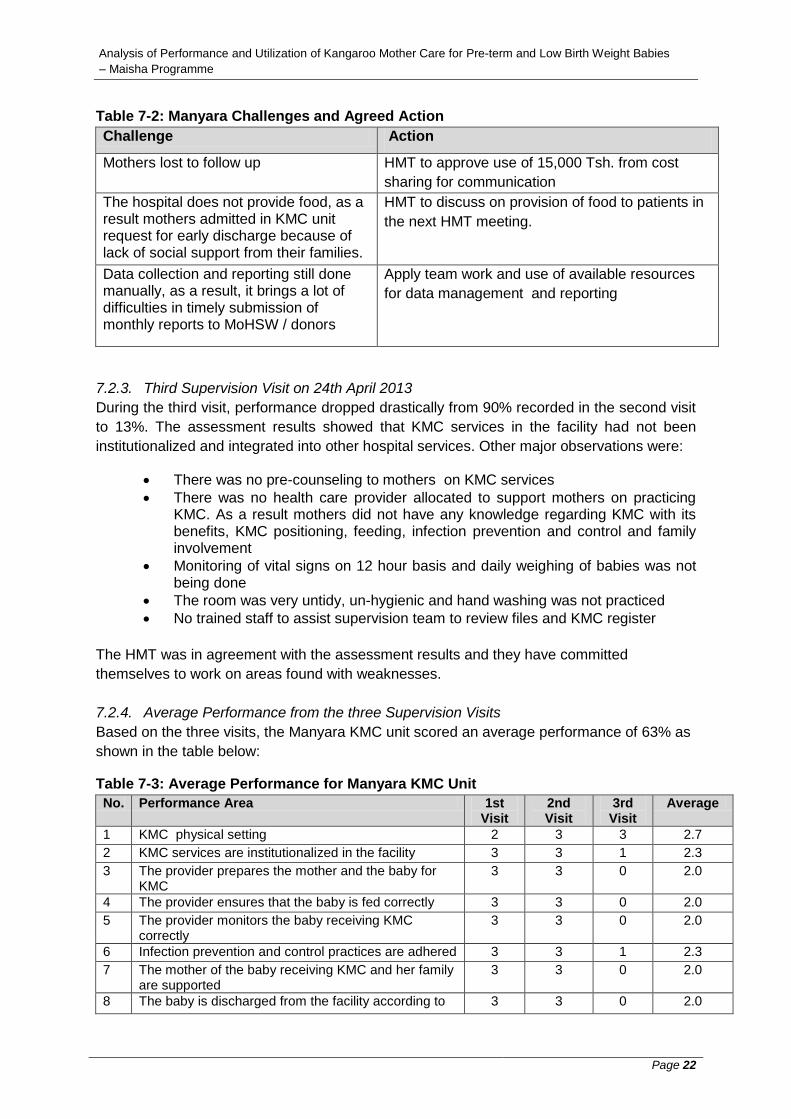
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 22
Table 7-2: Manyara Challenges and Agreed Action
Challenge Action
Mothers lost to follow up
HMT to approve use of 15,000 Tsh. from cost
sharing for communication
The hospital does not provide food, as a result mothers admitted in KMC unit request for early discharge because of lack of social support from their families.
HMT to discuss on provision of food to patients in
the next HMT meeting.
Data collection and reporting still done manually, as a result, it brings a lot of difficulties in timely submission of monthly reports to MoHSW / donors
Apply team work and use of available resources
for data management and reporting
7.2.3. Third Supervision Visit on 24th April 2013
During the third visit, performance dropped drastically from 90% recorded in the second visit
to 13%. The assessment results showed that KMC services in the facility had not been
institutionalized and integrated into other hospital services. Other major observations were:
There was no pre-counseling to mothers on KMC services
There was no health care provider allocated to support mothers on practicing KMC. As a result mothers did not have any knowledge regarding KMC with its benefits, KMC positioning, feeding, infection prevention and control and family involvement
Monitoring of vital signs on 12 hour basis and daily weighing of babies was not being done
The room was very untidy, un-hygienic and hand washing was not practiced
No trained staff to assist supervision team to review files and KMC register
The HMT was in agreement with the assessment results and they have committed
themselves to work on areas found with weaknesses.
7.2.4. Average Performance from the three Supervision Visits
Based on the three visits, the Manyara KMC unit scored an average performance of 63% as
shown in the table below:
Table 7-3: Average Performance for Manyara KMC Unit
No. Performance Area 1st Visit
2nd Visit
3rd Visit
Average
1 KMC physical setting 2 3 3 2.7
2 KMC services are institutionalized in the facility 3 3 1 2.3
3 The provider prepares the mother and the baby for KMC
3 3 0 2.0
4 The provider ensures that the baby is fed correctly 3 3 0 2.0
5 The provider monitors the baby receiving KMC correctly
3 3 0 2.0
6 Infection prevention and control practices are adhered 3 3 1 2.3
7 The mother of the baby receiving KMC and her family are supported
3 3 0 2.0
8 The baby is discharged from the facility according to 3 3 0 2.0
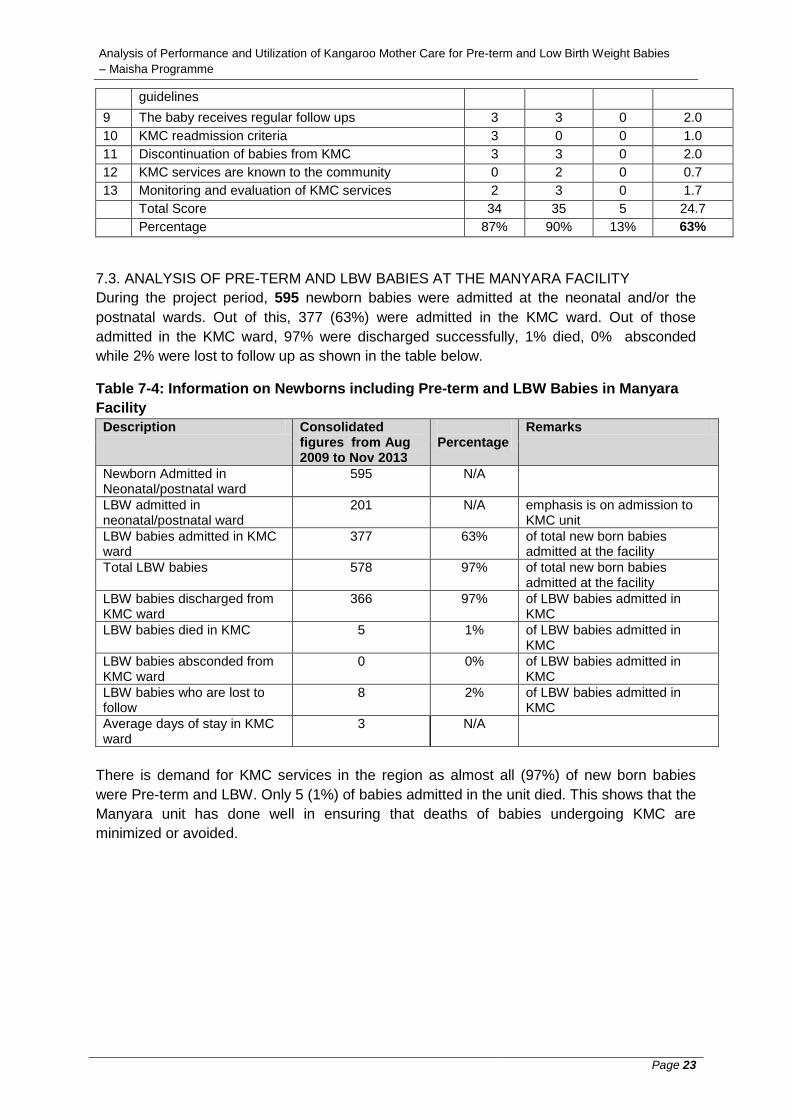
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 23
guidelines
9 The baby receives regular follow ups 3 3 0 2.0
10 KMC readmission criteria 3 0 0 1.0
11 Discontinuation of babies from KMC 3 3 0 2.0
12 KMC services are known to the community 0 2 0 0.7
13 Monitoring and evaluation of KMC services 2 3 0 1.7
Total Score 34 35 5 24.7
Percentage 87% 90% 13% 63%
7.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MANYARA FACILITY
During the project period, 595 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 377 (63%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 97% were discharged successfully, 1% died, 0% absconded
while 2% were lost to follow up as shown in the table below.
Table 7-4: Information on Newborns including Pre-term and LBW Babies in Manyara
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage
Remarks
Newborn Admitted in Neonatal/postnatal ward
595 N/A
LBW admitted in neonatal/postnatal ward
201 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
377 63% of total new born babies admitted at the facility
Total LBW babies 578 97% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
366 97% of LBW babies admitted in KMC
LBW babies died in KMC 5 1% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
0 0% of LBW babies admitted in KMC
LBW babies who are lost to follow
8 2% of LBW babies admitted in KMC
Average days of stay in KMC ward
3 N/A
There is demand for KMC services in the region as almost all (97%) of new born babies
were Pre-term and LBW. Only 5 (1%) of babies admitted in the unit died. This shows that the
Manyara unit has done well in ensuring that deaths of babies undergoing KMC are
minimized or avoided.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 24
8. PERFORMANCE ASSESSMENT FOR ARUSHA REGION
8.1. BASIC INFORMATION ON ARUSHA KMC UNIT
The KMC services in Arusha region are provided at the Mount Meru Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 8-1: Basic Information on Arusha KMC Unit
Item Description
Name of health facility
Mount Meru Regional Hospital
Type of health facility
Hospital
Location Arusha Region, Arusha Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
18 health workers
Health providers working in KMC
unit/ward
3
Health providers followed up after
training
1
8.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 11th May
2011(during year 3), 12th July 2012 (during year 4) and on 02nd April 2013 (during year 5).
No supervision visits were done in Arusha during year 1 and 2.
8.2.1. First Supervision Visit on 11th May 2011
The assessment results during the first visit ranked the KMC performance at 49%.The
hospital was under major rehabilitation and the KMC site had been temporarily shifted to
another location. Mothers were not practicing continuous KMC method due to lack of space
to accommodate all and probably due to insufficient support from KMC staff.
8.2.2. Second Supervision Visit on 12th July 2012
During the second visit, the performance of the KMC unit had improved from the previous
49% recorded in the first visit to 85%. Despite the improvement, several challenges still
existed. These challenges and the suggested actions are shown in the table below:
Table 8-2: Arusha Challenges and Agreed Action
Challenge
Action
Overcrowding due to space limitation Need for more space, at least 3 rooms each with
5 beds. Services could also be established in
other health facilities
No toilets and bathrooms for KMC
mothers
Need of a bathroom and a toilet for KMC mother
to avoid cross infection. The HMT to address this
issue

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 25
Inadequate staff working at neonatal (1
qualified nurse and I medical attendant
per shift looking after 40 babies)
More trained staff to be allocated to neonatal unit
specifically those trained in KMC
No support of secretarial services
KMC services need to be strengthened through
additional support from HMT for provision of staff
to work at KMC site and secretarial services
Inadequate sockets and poor wiring
system in KMC room ( needed for
heaters and suction machine)
Follow up to be made
Inadequate access to KMC services and
follow up of KMC babies
KMC services to be extended to other health
facilities
8.2.3. Third Supervision Visit on 02nd April 2012
During the third visit, the performance of the KMC unit had further improved from the
previous 85% recorded in the second visit to 92%. Despite the improvement, most
challenges identified during the second visit still remained un-addressed. During the third
visit, it was also observed that resuscitation of babies with difficulty in breathing was not
being done at the KMC room. This resulted to delay of the resuscitation process and
exposed babies to cold environment.
8.2.4. Average Performance from the three Supervision Visits
Based on the three visits, the Arusha KMC unit scored an average performance of 75% as
shown in the table below:
Table 8-3: Average Performance for Arusha KMC Unit
No. Performance Area 1st
Visit 2nd Visit
3rd Visit Average
1 KMC physical setting 1 1 2 1.3
2 KMC services are institutionalized in the facility 3 2 2 2.3
3 The provider prepares the mother and the baby for KMC
2 3 3 2.7
4 The provider ensures that the baby is fed correctly 2 3 3 2.7
5 The provider monitors the baby receiving KMC correctly
2 2 3 2.3
6 Infection prevention and control practices are adhered
2 3 3 2.7
7 The mother of the baby receiving KMC and her family are supported
0 3 3 2.0
8 The baby is discharged from the facility according to guidelines
3 3 3 3.0
9 The baby receives regular follow ups 3 3 3 3.0
10 KMC readmission criteria 0 3 3 2.0
11 Discontinuation of babies from KMC 0 3 3 2.0
12 KMC services are known to the community 0 2 2 1.3
13 Monitoring and evaluation of KMC services 1 2 3 2.0
Total Score 19 33 36 29.3
Percentage 49% 85% 92% 75%
8.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE ARUSHA FACILITY
During the project period, 11,570 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 528 (5%) were admitted in the KMC ward. Out of those
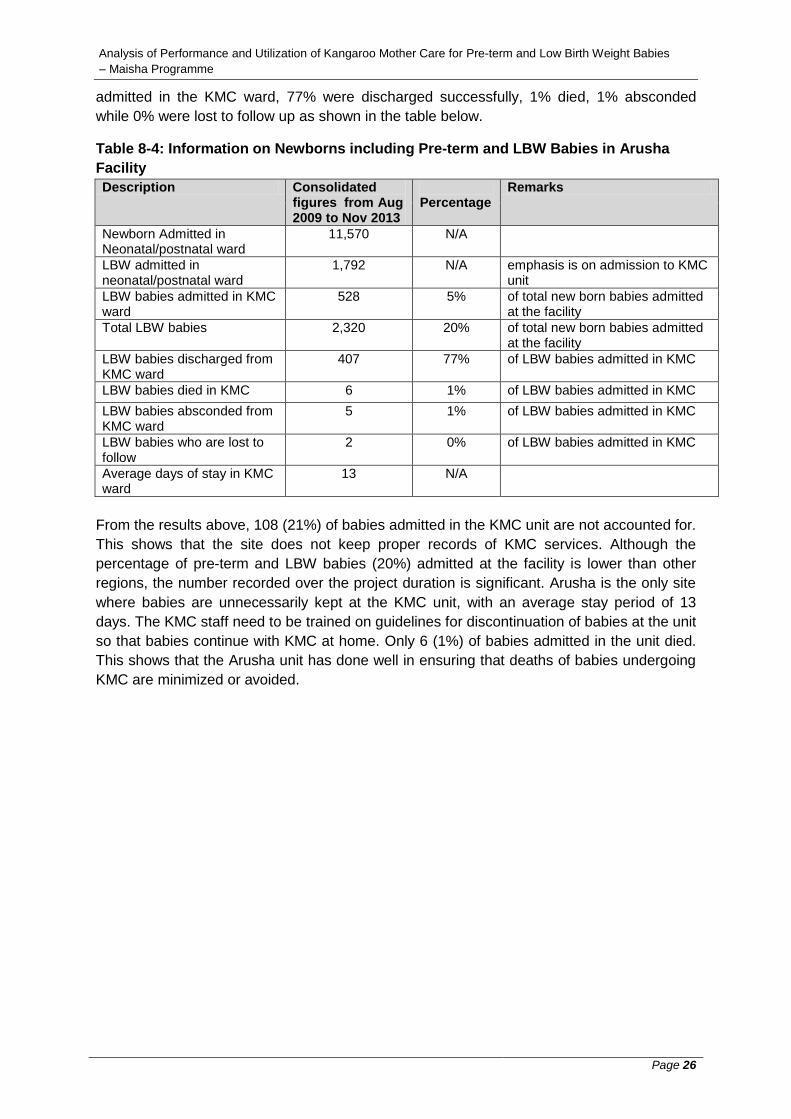
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 26
admitted in the KMC ward, 77% were discharged successfully, 1% died, 1% absconded
while 0% were lost to follow up as shown in the table below.
Table 8-4: Information on Newborns including Pre-term and LBW Babies in Arusha
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage
Remarks
Newborn Admitted in Neonatal/postnatal ward
11,570 N/A
LBW admitted in neonatal/postnatal ward
1,792 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
528 5% of total new born babies admitted at the facility
Total LBW babies 2,320 20% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
407 77% of LBW babies admitted in KMC
LBW babies died in KMC 6 1% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
5 1% of LBW babies admitted in KMC
LBW babies who are lost to follow
2 0% of LBW babies admitted in KMC
Average days of stay in KMC ward
13 N/A
From the results above, 108 (21%) of babies admitted in the KMC unit are not accounted for.
This shows that the site does not keep proper records of KMC services. Although the
percentage of pre-term and LBW babies (20%) admitted at the facility is lower than other
regions, the number recorded over the project duration is significant. Arusha is the only site
where babies are unnecessarily kept at the KMC unit, with an average stay period of 13
days. The KMC staff need to be trained on guidelines for discontinuation of babies at the unit
so that babies continue with KMC at home. Only 6 (1%) of babies admitted in the unit died.
This shows that the Arusha unit has done well in ensuring that deaths of babies undergoing
KMC are minimized or avoided.
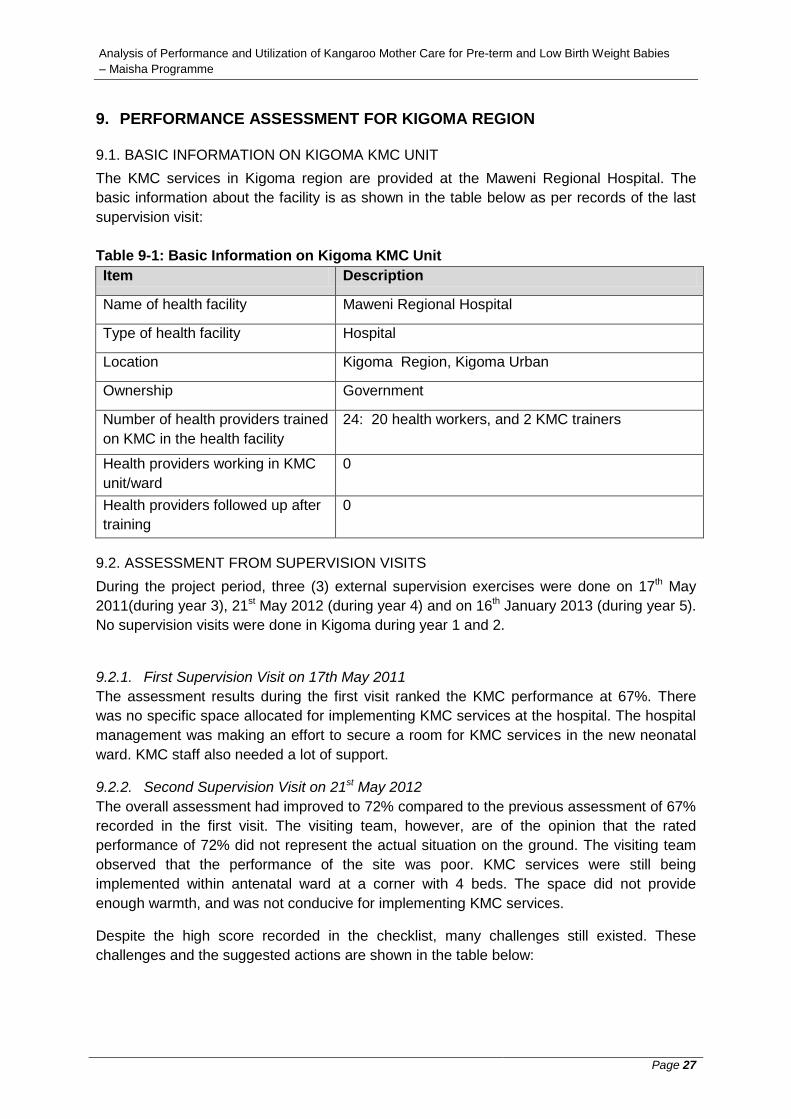
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 27
9. PERFORMANCE ASSESSMENT FOR KIGOMA REGION
9.1. BASIC INFORMATION ON KIGOMA KMC UNIT
The KMC services in Kigoma region are provided at the Maweni Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 9-1: Basic Information on Kigoma KMC Unit
Item Description
Name of health facility
Maweni Regional Hospital
Type of health facility
Hospital
Location Kigoma Region, Kigoma Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
24: 20 health workers, and 2 KMC trainers
Health providers working in KMC
unit/ward
0
Health providers followed up after
training
0
9.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 17th May
2011(during year 3), 21st May 2012 (during year 4) and on 16th January 2013 (during year 5).
No supervision visits were done in Kigoma during year 1 and 2.
9.2.1. First Supervision Visit on 17th May 2011
The assessment results during the first visit ranked the KMC performance at 67%. There
was no specific space allocated for implementing KMC services at the hospital. The hospital
management was making an effort to secure a room for KMC services in the new neonatal
ward. KMC staff also needed a lot of support.
9.2.2. Second Supervision Visit on 21st May 2012
The overall assessment had improved to 72% compared to the previous assessment of 67%
recorded in the first visit. The visiting team, however, are of the opinion that the rated
performance of 72% did not represent the actual situation on the ground. The visiting team
observed that the performance of the site was poor. KMC services were still being
implemented within antenatal ward at a corner with 4 beds. The space did not provide
enough warmth, and was not conducive for implementing KMC services.
Despite the high score recorded in the checklist, many challenges still existed. These
challenges and the suggested actions are shown in the table below:
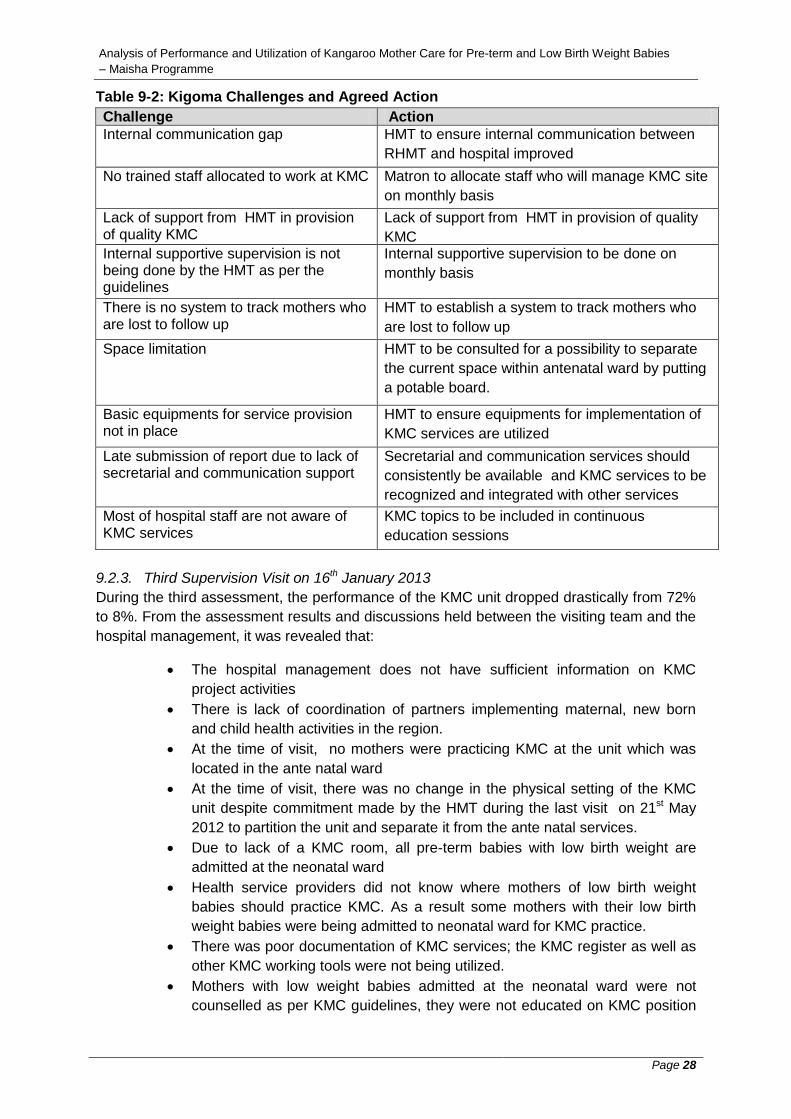
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 28
Table 9-2: Kigoma Challenges and Agreed Action
Challenge Action
Internal communication gap
HMT to ensure internal communication between
RHMT and hospital improved
No trained staff allocated to work at KMC
Matron to allocate staff who will manage KMC site
on monthly basis
Lack of support from HMT in provision of quality KMC
Lack of support from HMT in provision of quality
KMC
Internal supportive supervision is not being done by the HMT as per the guidelines
Internal supportive supervision to be done on
monthly basis
There is no system to track mothers who are lost to follow up
HMT to establish a system to track mothers who
are lost to follow up
Space limitation
HMT to be consulted for a possibility to separate
the current space within antenatal ward by putting
a potable board.
Basic equipments for service provision not in place
HMT to ensure equipments for implementation of
KMC services are utilized
Late submission of report due to lack of secretarial and communication support
Secretarial and communication services should
consistently be available and KMC services to be
recognized and integrated with other services
Most of hospital staff are not aware of KMC services
KMC topics to be included in continuous
education sessions
9.2.3. Third Supervision Visit on 16th January 2013
During the third assessment, the performance of the KMC unit dropped drastically from 72%
to 8%. From the assessment results and discussions held between the visiting team and the
hospital management, it was revealed that:
The hospital management does not have sufficient information on KMC
project activities
There is lack of coordination of partners implementing maternal, new born
and child health activities in the region.
At the time of visit, no mothers were practicing KMC at the unit which was
located in the ante natal ward
At the time of visit, there was no change in the physical setting of the KMC
unit despite commitment made by the HMT during the last visit on 21st May
2012 to partition the unit and separate it from the ante natal services.
Due to lack of a KMC room, all pre-term babies with low birth weight are
admitted at the neonatal ward
Health service providers did not know where mothers of low birth weight
babies should practice KMC. As a result some mothers with their low birth
weight babies were being admitted to neonatal ward for KMC practice.
There was poor documentation of KMC services; the KMC register as well as
other KMC working tools were not being utilized.
Mothers with low weight babies admitted at the neonatal ward were not
counselled as per KMC guidelines, they were not educated on KMC position

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 29
and lying on an elevated bed and there was no staff trained on KMC to
support the mother.
The RMO together with other hospital management team (MOI/C and
matron), committed themselves to make a partition at the antenatal ward for a
space to accommodate four beds. The Medical Officer in charge also
appointed a new KMC focal person; Ms Siyaleo Shilambele to work hand in
hand with the available KMC master trainers who are in the hospital to
revitalize the service. The MOI/C was advised by the supervisors to ensure
that the new focal person gets a formal KMC training through on the job
training where he agreed and requested for a feedback on the training plan by
Friday the 18th of January 2013.
9.2.4. Average Performance from the three Supervision Visits
Based on the three visits, the Kigoma KMC unit scored an average performance of 49% as
shown in the table below:
Table 9-3: Average Performance for Kigoma KMC Unit
No. Performance Area 1st
Visit 2nd
Visit 3rd
Visit Average
1 KMC physical setting 2 3 2 2.3
2 KMC services are institutionalized in the facility 3 0 0 1.0
3 The provider prepares the mother and the baby for KMC
2 3 0 1.7
4 The provider ensures that the baby is fed correctly 3 2 0 1.7
5 The provider monitors the baby receiving KMC correctly
2 2 0 1.3
6 Infection prevention and control practices are adhered
3 2 0 1.7
7 The mother of the baby receiving KMC and her family are supported
3 3 0 2.0
8 The baby is discharged from the facility according to guidelines
3 2 0 1.7
9 The baby receives regular follow ups 2 3 0 1.7
10 KMC readmission criteria 0 3 0 1.0
11 Discontinuation of babies from KMC 2 3 0 1.7
12 KMC services are known to the community 0 1 1 0.7
13 Monitoring and evaluation of KMC services 1 1 0 0.7
Total Score 26 28 3 19.0
Percentage 67% 72% 8% 49%
9.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KIGOMA FACILITY
During the project period, 1,816 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 380 (21%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 80% were discharged successfully, 6% died, 14% absconded
while 13% were lost to follow up as shown in the table below.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 30
Table 9-4: Information on Pre-term and LBW Babies in Kigoma Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
1,816 N/A
LBW admitted in neonatal/postnatal ward
243 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
380 21% of total new born babies admitted at the facility
Total LBW babies 623 34% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
303 80% of LBW babies admitted in KMC
LBW babies died in KMC 24 6% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
15 4% of LBW babies admitted in KMC
LBW babies who are lost to follow
48 13% of LBW babies admitted in KMC
Average days of stay in KMC ward
4 N/A
From the results above, the sum of babies discharged, babies who died, babies absconded
and babies lost to follow up exceeds the number of babies admitted at the KMC site by 10
(3%). This shows that the site does not keep proper records of KMC services.
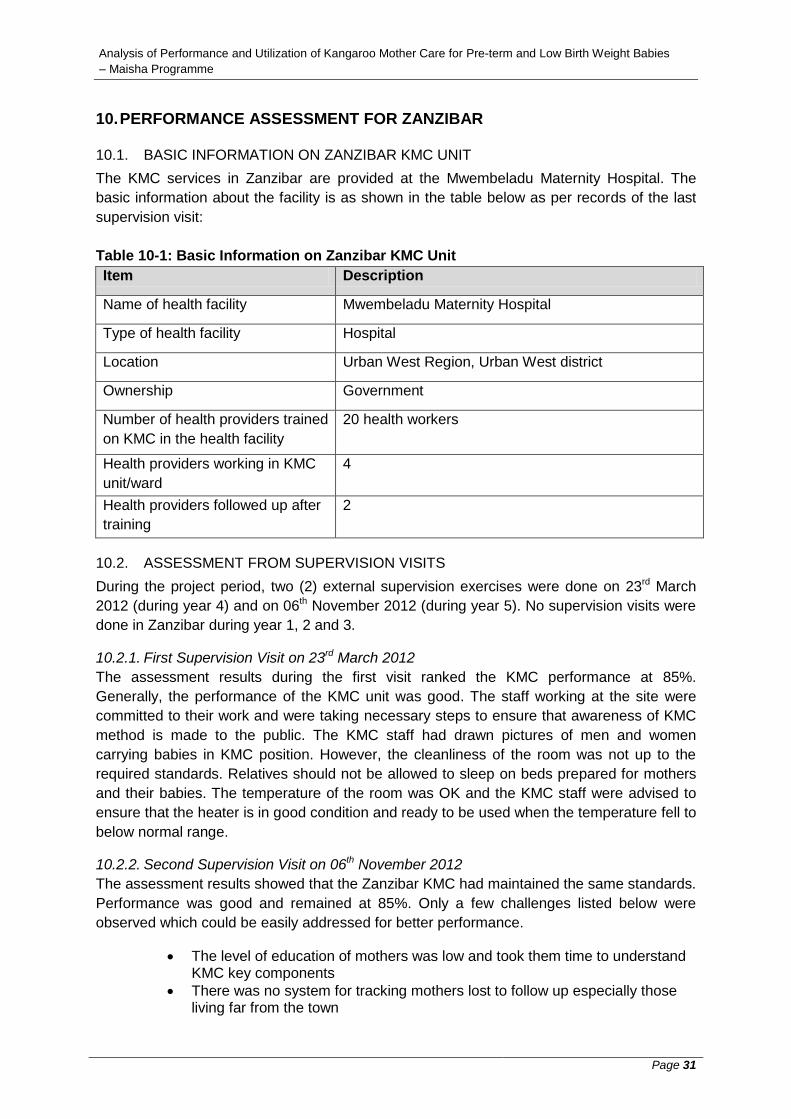
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 31
10. PERFORMANCE ASSESSMENT FOR ZANZIBAR
10.1. BASIC INFORMATION ON ZANZIBAR KMC UNIT
The KMC services in Zanzibar are provided at the Mwembeladu Maternity Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 10-1: Basic Information on Zanzibar KMC Unit
Item Description
Name of health facility
Mwembeladu Maternity Hospital
Type of health facility
Hospital
Location Urban West Region, Urban West district
Ownership
Government
Number of health providers trained
on KMC in the health facility
20 health workers
Health providers working in KMC
unit/ward
4
Health providers followed up after
training
2
10.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 23rd March
2012 (during year 4) and on 06th November 2012 (during year 5). No supervision visits were
done in Zanzibar during year 1, 2 and 3.
10.2.1. First Supervision Visit on 23rd March 2012
The assessment results during the first visit ranked the KMC performance at 85%.
Generally, the performance of the KMC unit was good. The staff working at the site were
committed to their work and were taking necessary steps to ensure that awareness of KMC
method is made to the public. The KMC staff had drawn pictures of men and women
carrying babies in KMC position. However, the cleanliness of the room was not up to the
required standards. Relatives should not be allowed to sleep on beds prepared for mothers
and their babies. The temperature of the room was OK and the KMC staff were advised to
ensure that the heater is in good condition and ready to be used when the temperature fell to
below normal range.
10.2.2. Second Supervision Visit on 06th November 2012
The assessment results showed that the Zanzibar KMC had maintained the same standards.
Performance was good and remained at 85%. Only a few challenges listed below were
observed which could be easily addressed for better performance.
The level of education of mothers was low and took them time to understand KMC key components
There was no system for tracking mothers lost to follow up especially those living far from the town
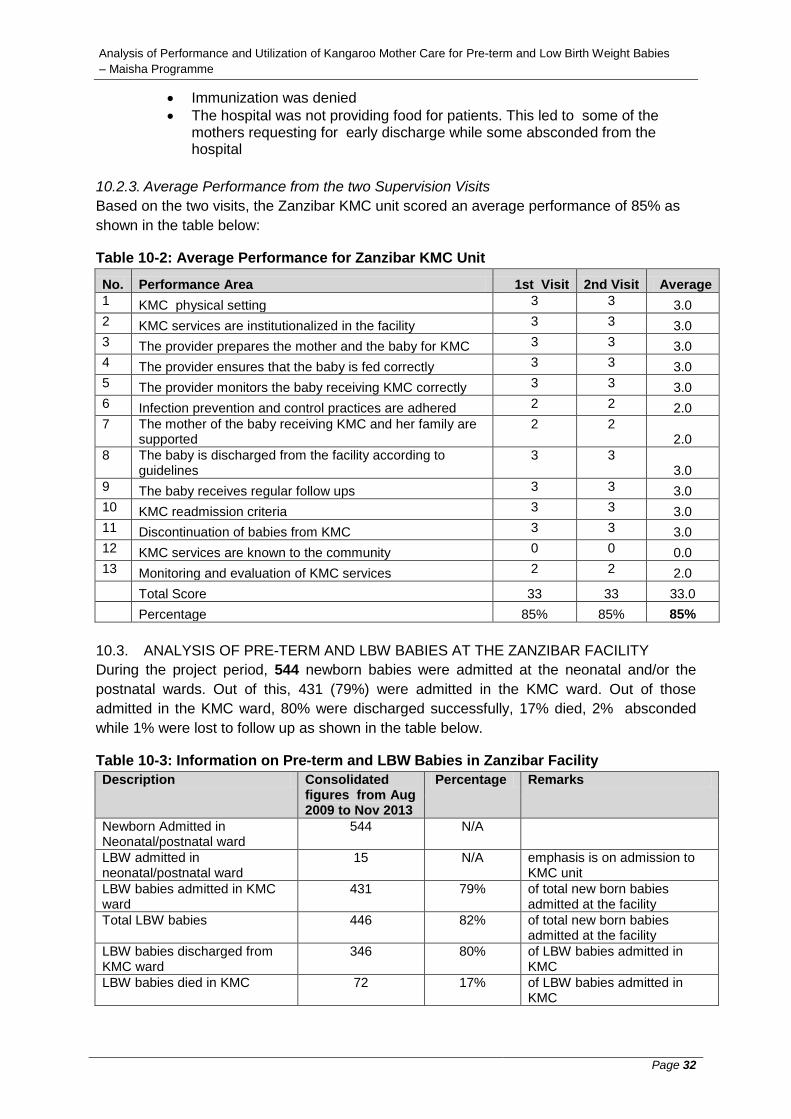
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 32
Immunization was denied
The hospital was not providing food for patients. This led to some of the mothers requesting for early discharge while some absconded from the hospital
10.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Zanzibar KMC unit scored an average performance of 85% as
shown in the table below:
Table 10-2: Average Performance for Zanzibar KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 3 3 3.0
3 The provider prepares the mother and the baby for KMC 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 3 3.0
5 The provider monitors the baby receiving KMC correctly 3 3 3.0
6 Infection prevention and control practices are adhered 2 2 2.0
7 The mother of the baby receiving KMC and her family are supported
2 2 2.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 0 0 0.0
13 Monitoring and evaluation of KMC services 2 2 2.0
Total Score 33 33 33.0
Percentage 85% 85% 85%
10.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE ZANZIBAR FACILITY
During the project period, 544 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 431 (79%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 80% were discharged successfully, 17% died, 2% absconded
while 1% were lost to follow up as shown in the table below.
Table 10-3: Information on Pre-term and LBW Babies in Zanzibar Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
544 N/A
LBW admitted in neonatal/postnatal ward
15 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
431 79% of total new born babies admitted at the facility
Total LBW babies 446 82% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
346 80% of LBW babies admitted in KMC
LBW babies died in KMC 72 17% of LBW babies admitted in KMC

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 33
LBW babies absconded from KMC ward
7 2% of LBW babies admitted in KMC
LBW babies who are lost to follow
4 1% of LBW babies admitted in KMC
Average days of stay in KMC ward
6 N/A
From the results above, all babies admitted in the KMC unit were accounted for. This shows
that the site keeps proper records of KMC services. Out of all babies admitted at the facility,
82% are Pre-term and LBW. This shows that there is high demand of KMC services in
Zanzibar. The number of babies who die at the KMC unit is also high, 72 out of 431 (17%).
There is need to establish and address the causes of death for babies under KMC.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 34
11. PERFORMANCE ASSESSMENT FOR KAGERA
11.1. BASIC INFORMATION ON KAGERA KMC UNIT
The KMC services in Kagera region are provided at the Bukoba Regional Referral Hospital.
The basic information about the facility is as shown in the table below as per records of the
last supervision visit:
Table 11-1: Basic Information on Kagera KMC Unit
Item Description
Name of health facility
Bukoba Regional Referral Hospital
Type of health facility
Hospital
Location Kagera Region, Bukoba Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
24: 20 Health workers, 2 master trainers, 2 master
supervisors
Health providers working in KMC
unit/ward
2
Health providers followed up after
training
2
11.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 14th May
2012 (during year 4) and on 15th November 2012 (during year 5). No supervision visits were
done in Kagera during year 1, 2 and 3.
11.2.1. First Supervision Visit on 14th May 2012
The supervision team observed that the performance of the site was generally good. Both
KMC types were practiced, i.e. at the site (continuous KMC) and at post natal ward
(intermittent KMC). However, at the time of assessment there were no babies at the KMC
room and thus not all performance areas were assessed. Only 7 performance areas were
assessed and rated. For details of performance areas assessed refer to Table 11-3 in sub
section 11.3.3. The overall performance was rated at 71%.
Some challenges were also observed and suggestions for action discussed as shown in the
table below:
Table 11-2: Kagera Challenges and Agreed Action
Challenge Action
No funds for sensitization of the community
HMT to mobilize funds to support sensitization
activities Lack of secretarial and communication services
HMT to ensure that secretarial and
communication services are consistently availed
Internal supportive supervision was not being done by the HMT as per the KMC guidelines
HMT and KMC team to ensure that internal
supportive supervision is on monthly basis

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 35
There was no system to track mothers who are lost to follow up
HMT and KMC team to establish a system to track
mothers who are lost to follow up
Space limitation HMT to allocate a spacious room for implementing
continuous KMC
Understaffing of skilled nursing cadre Matron to allocate staff who will manage KMC site
on monthly basis
Hospital not providing food as a result mothers with no relative support abscond from the hospital
HMT to recognize and integrate KMC services
with other hospital services
11.2.2. Second Supervision Visit on 15th November 2012
During the second visit, the overall assessment improved to 87% compared to the previous
assessment of 71% recorded in the first visit. The performance of the KMC unit was
generally good despite the outstanding challenges that still remained unsolved. The HMT
appreciated the entire assessment procedure which they described as participatory,
supportive and educative. The HMT committed to addressing the outstanding challenges as
follows:
Space limitation: The HMT has already put into its hospital plans to provide
enough space for KMC services
Mothers lost to follow up: The HMT informed the supervision team that
discharged LBW babies will be handed over to respective districts for follow
up.
- Focal person to link with DRCHCO
- Need to convince the council to build waiting mothers home for KMC to
stay
Shortage of trained staff in KMC room and lack of commitment to implement
quality KMC services: The HMT will identify the root causes and solve the
problem
The community not yet sensitized on KMC services: The RRCHCO and
Regional social welfare officer will be involved and the HMT will check the
possibility of providing financial support.
Hospital not providing food and as a result mothers with no relative support
abscond from the hospital: The HMT admitted that they had financial
constraints and would liaise with the social welfare for support.
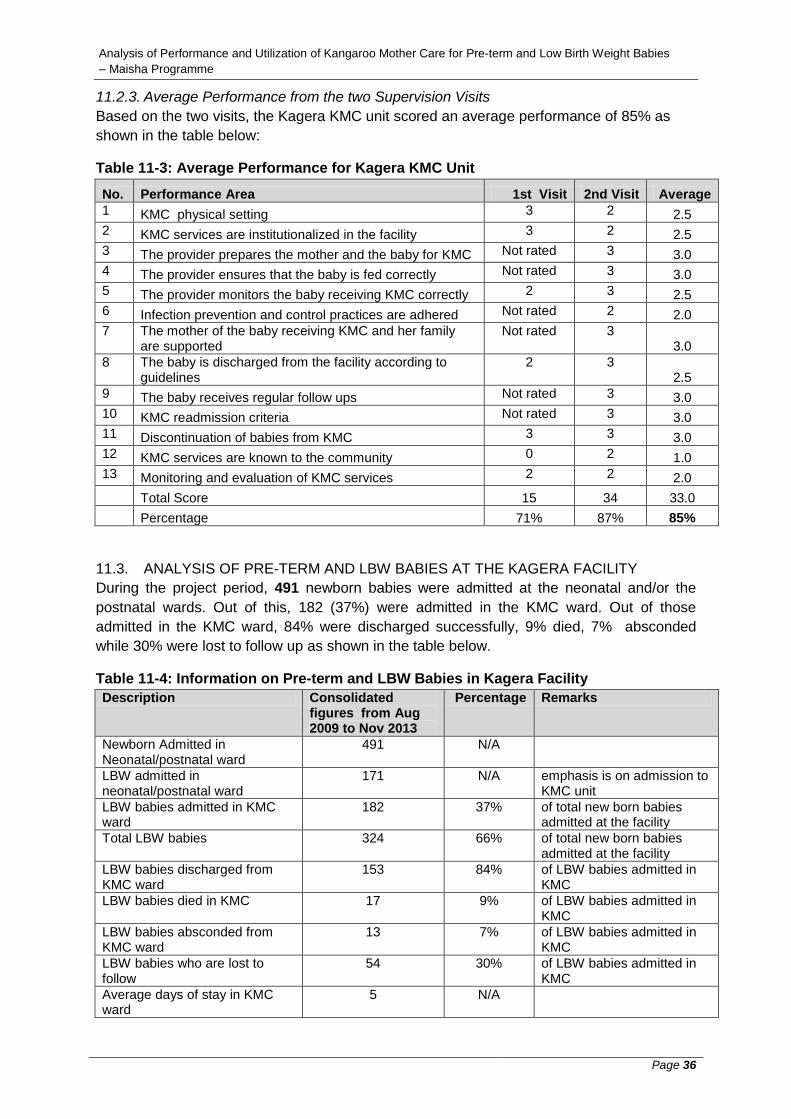
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 36
11.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Kagera KMC unit scored an average performance of 85% as
shown in the table below:
Table 11-3: Average Performance for Kagera KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 2 2.5
2 KMC services are institutionalized in the facility 3 2 2.5
3 The provider prepares the mother and the baby for KMC Not rated 3 3.0
4 The provider ensures that the baby is fed correctly Not rated 3 3.0
5 The provider monitors the baby receiving KMC correctly 2 3 2.5
6 Infection prevention and control practices are adhered Not rated 2 2.0
7 The mother of the baby receiving KMC and her family are supported
Not rated 3 3.0
8 The baby is discharged from the facility according to guidelines
2 3 2.5
9 The baby receives regular follow ups Not rated 3 3.0
10 KMC readmission criteria Not rated 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 0 2 1.0
13 Monitoring and evaluation of KMC services 2 2 2.0
Total Score 15 34 33.0
Percentage 71% 87% 85%
11.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KAGERA FACILITY
During the project period, 491 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 182 (37%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 84% were discharged successfully, 9% died, 7% absconded
while 30% were lost to follow up as shown in the table below.
Table 11-4: Information on Pre-term and LBW Babies in Kagera Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
491 N/A
LBW admitted in neonatal/postnatal ward
171 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
182 37% of total new born babies admitted at the facility
Total LBW babies 324 66% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
153 84% of LBW babies admitted in KMC
LBW babies died in KMC 17 9% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
13 7% of LBW babies admitted in KMC
LBW babies who are lost to follow
54 30% of LBW babies admitted in KMC
Average days of stay in KMC ward
5 N/A

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 37
From the results above, the sum of babies discharged, babies who died, babies absconded
and babies lost to follow exceeds the number of babies admitted at the KMC site by 55
(30%). This shows that the site does not keep proper records of KMC services. Babies lost
to follow up are also significant (30%) and measures need to be put in place to ensure that
the number is reduced or eliminated completely. There is demand for KMC services in the
region as 66% of new born babies were Pre-term and LBW.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 38
12. PERFORMANCE ASSESSMENT FOR MWANZA REGION
12.1. BASIC INFORMATION ON MWANZA KMC UNIT
The KMC services in Mwanza region are provided at the Sekotoure Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 12-1: Basic Information on Mwanza KMC Unit
Item Description
Name of health facility
Sekotoure Regional Hospital
Type of health facility
Hospital
Location Mwanza Region, Mwanza Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 20 general KMC and 2 master trainers
Health providers working in KMC
unit/ward
3 trained nurses
Health providers followed up after
training
3
12.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 02nd May
2012 (during year 4) and on 09th November 2012 (during year 5). No supervision visits were
done in Mwanza during year 1, 2 and 3.
12.2.1. First Supervision Visit on 02nd May 2012
Generally, the performance of the KMC unit at Mwanza is good with an assessed
performance of 85%. The hospital management has provided great support to KMC services
by allocating at least two trained personnel to work at KMC unit. KMC staff are very
committed to ensure the KMC concept at the hospital is a success.
Some challenges were also observed and suggestions for action discussed as shown in the
table below:
Table 12-2: Mwanza Challenges and Agreed Action
Challenge Action
Space limitation: The room was found to be small and not conducive for KMC services. It didn’t meet KMC standards
MO/C to release conference room
Poor security of KMC room which makes it not possible to keep equipment e.g heater, weighing scale etc
A bigger and lockable room is required. Proper hand over of equipment to be exercised by staff during change of shifts
Service providers in KMC room: Only 2 trained staff on KMC. The KMC operation is affected when one staff is off-duty
More staff to be trained and allocated to the unit
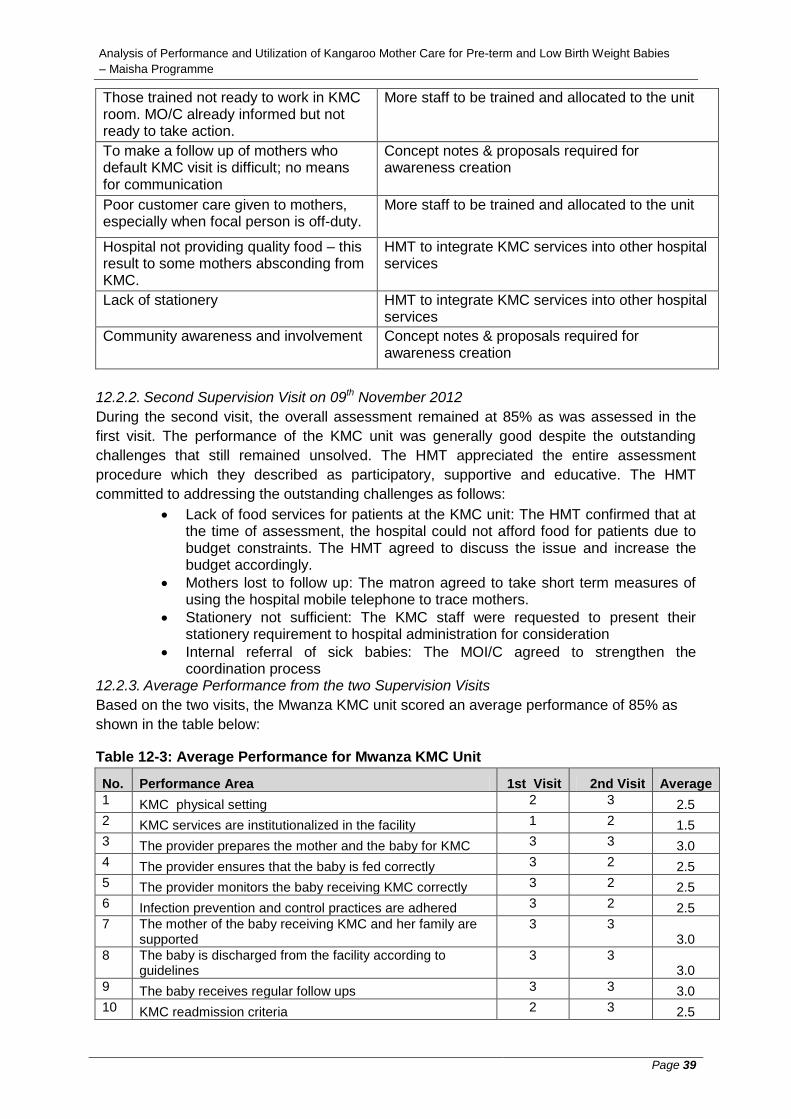
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 39
Those trained not ready to work in KMC room. MO/C already informed but not ready to take action.
More staff to be trained and allocated to the unit
To make a follow up of mothers who default KMC visit is difficult; no means for communication
Concept notes & proposals required for awareness creation
Poor customer care given to mothers, especially when focal person is off-duty.
More staff to be trained and allocated to the unit
Hospital not providing quality food – this result to some mothers absconding from KMC.
HMT to integrate KMC services into other hospital services
Lack of stationery
HMT to integrate KMC services into other hospital services
Community awareness and involvement
Concept notes & proposals required for awareness creation
12.2.2. Second Supervision Visit on 09th November 2012
During the second visit, the overall assessment remained at 85% as was assessed in the
first visit. The performance of the KMC unit was generally good despite the outstanding
challenges that still remained unsolved. The HMT appreciated the entire assessment
procedure which they described as participatory, supportive and educative. The HMT
committed to addressing the outstanding challenges as follows:
Lack of food services for patients at the KMC unit: The HMT confirmed that at the time of assessment, the hospital could not afford food for patients due to budget constraints. The HMT agreed to discuss the issue and increase the budget accordingly.
Mothers lost to follow up: The matron agreed to take short term measures of using the hospital mobile telephone to trace mothers.
Stationery not sufficient: The KMC staff were requested to present their stationery requirement to hospital administration for consideration
Internal referral of sick babies: The MOI/C agreed to strengthen the coordination process
12.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Mwanza KMC unit scored an average performance of 85% as
shown in the table below:
Table 12-3: Average Performance for Mwanza KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 2 3 2.5
2 KMC services are institutionalized in the facility 1 2 1.5
3 The provider prepares the mother and the baby for KMC 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 2 2.5
5 The provider monitors the baby receiving KMC correctly 3 2 2.5
6 Infection prevention and control practices are adhered 3 2 2.5
7 The mother of the baby receiving KMC and her family are supported
3 3 3.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 2 3 2.5
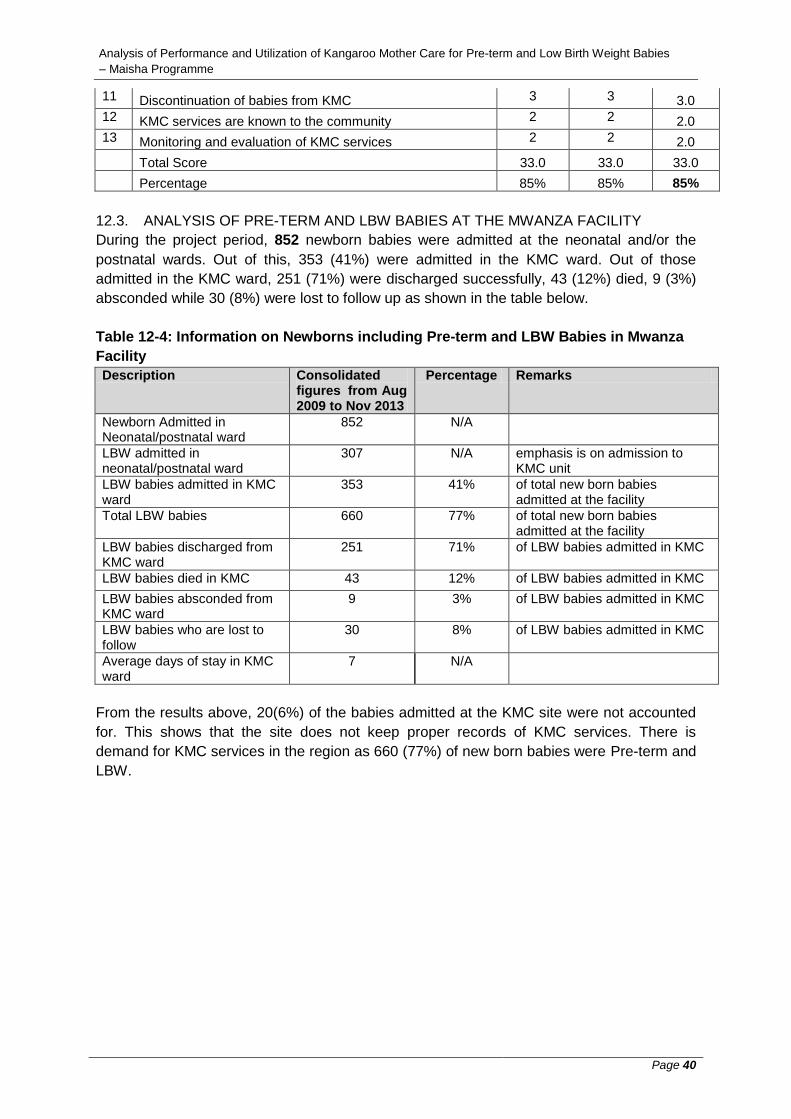
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 40
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 2 2 2.0
13 Monitoring and evaluation of KMC services 2 2 2.0
Total Score 33.0 33.0 33.0
Percentage 85% 85% 85%
12.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MWANZA FACILITY
During the project period, 852 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 353 (41%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 251 (71%) were discharged successfully, 43 (12%) died, 9 (3%)
absconded while 30 (8%) were lost to follow up as shown in the table below.
Table 12-4: Information on Newborns including Pre-term and LBW Babies in Mwanza
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
852 N/A
LBW admitted in neonatal/postnatal ward
307 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
353 41% of total new born babies admitted at the facility
Total LBW babies 660 77% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
251 71% of LBW babies admitted in KMC
LBW babies died in KMC 43 12% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
9 3% of LBW babies admitted in KMC
LBW babies who are lost to follow
30 8% of LBW babies admitted in KMC
Average days of stay in KMC ward
7 N/A
From the results above, 20(6%) of the babies admitted at the KMC site were not accounted
for. This shows that the site does not keep proper records of KMC services. There is
demand for KMC services in the region as 660 (77%) of new born babies were Pre-term and
LBW.
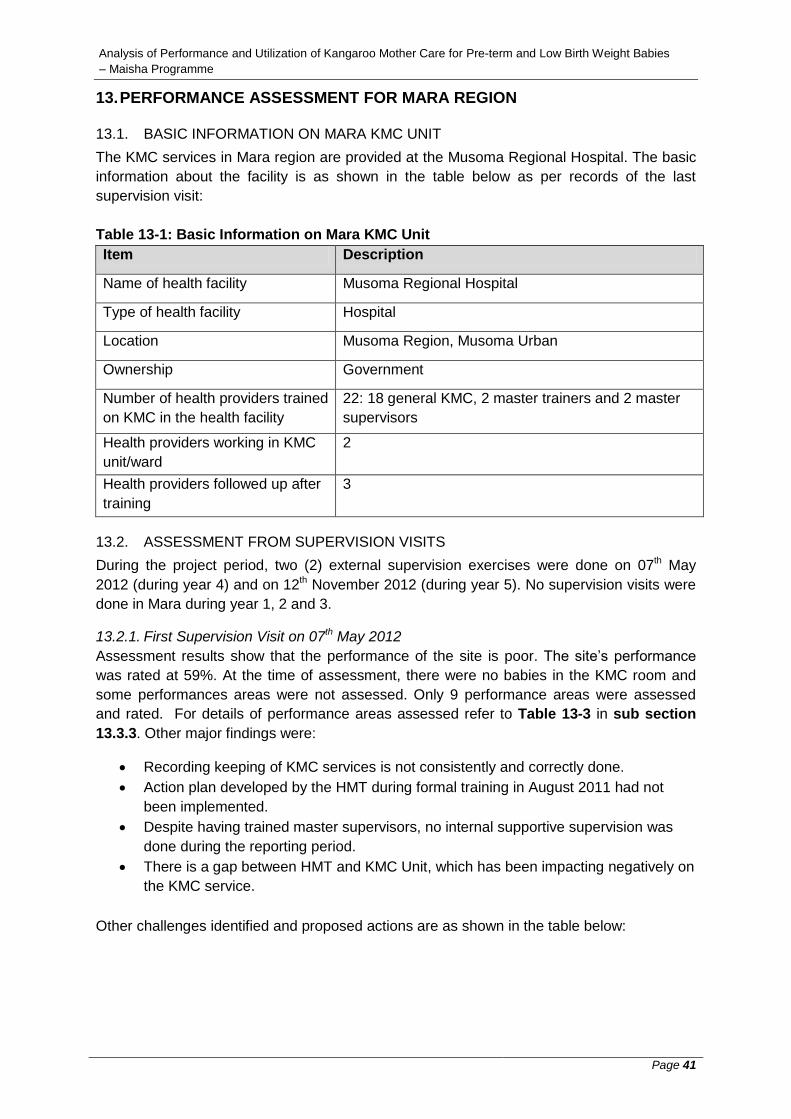
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 41
13. PERFORMANCE ASSESSMENT FOR MARA REGION
13.1. BASIC INFORMATION ON MARA KMC UNIT
The KMC services in Mara region are provided at the Musoma Regional Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 13-1: Basic Information on Mara KMC Unit
Item Description
Name of health facility
Musoma Regional Hospital
Type of health facility
Hospital
Location Musoma Region, Musoma Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 18 general KMC, 2 master trainers and 2 master
supervisors
Health providers working in KMC
unit/ward
2
Health providers followed up after
training
3
13.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 07th May
2012 (during year 4) and on 12th November 2012 (during year 5). No supervision visits were
done in Mara during year 1, 2 and 3.
13.2.1. First Supervision Visit on 07th May 2012
Assessment results show that the performance of the site is poor. The site’s performance
was rated at 59%. At the time of assessment, there were no babies in the KMC room and
some performances areas were not assessed. Only 9 performance areas were assessed
and rated. For details of performance areas assessed refer to Table 13-3 in sub section
13.3.3. Other major findings were:
Recording keeping of KMC services is not consistently and correctly done.
Action plan developed by the HMT during formal training in August 2011 had not
been implemented.
Despite having trained master supervisors, no internal supportive supervision was
done during the reporting period.
There is a gap between HMT and KMC Unit, which has been impacting negatively on
the KMC service.
Other challenges identified and proposed actions are as shown in the table below:
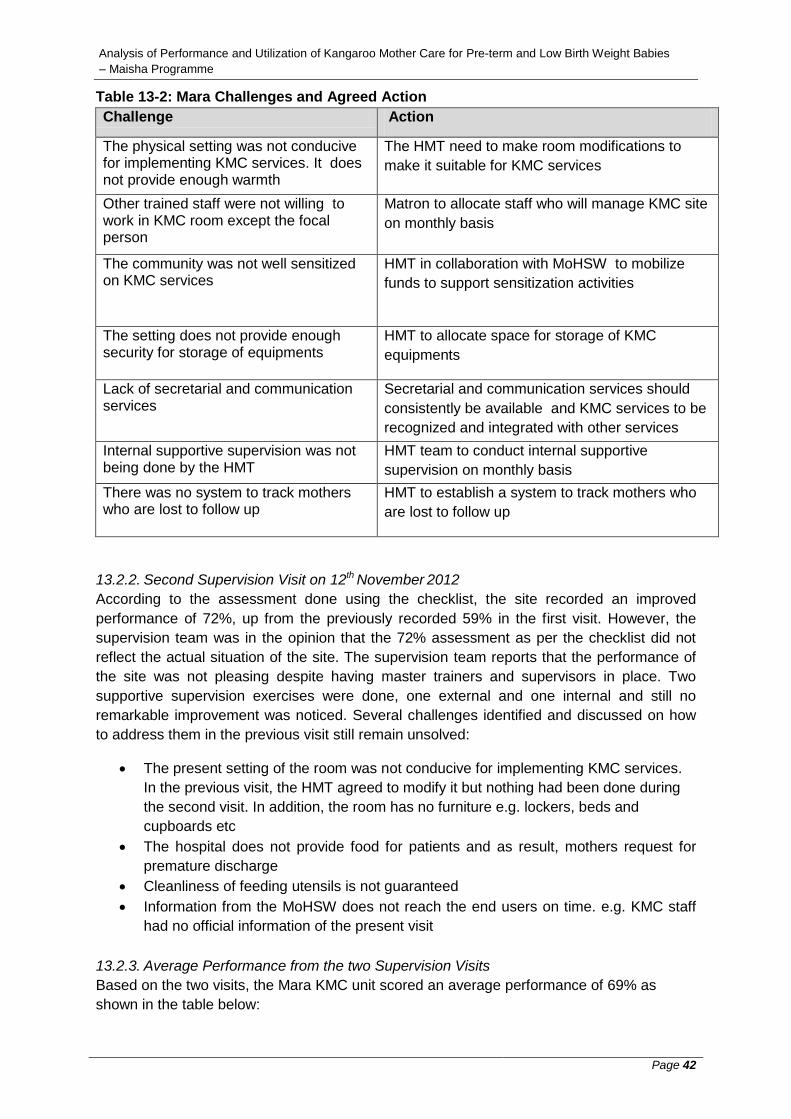
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 42
Table 13-2: Mara Challenges and Agreed Action
Challenge Action
The physical setting was not conducive for implementing KMC services. It does not provide enough warmth
The HMT need to make room modifications to
make it suitable for KMC services
Other trained staff were not willing to work in KMC room except the focal person
Matron to allocate staff who will manage KMC site
on monthly basis
The community was not well sensitized on KMC services
HMT in collaboration with MoHSW to mobilize
funds to support sensitization activities
The setting does not provide enough security for storage of equipments
HMT to allocate space for storage of KMC
equipments
Lack of secretarial and communication services
Secretarial and communication services should
consistently be available and KMC services to be
recognized and integrated with other services
Internal supportive supervision was not being done by the HMT
HMT team to conduct internal supportive
supervision on monthly basis
There was no system to track mothers who are lost to follow up
HMT to establish a system to track mothers who
are lost to follow up
13.2.2. Second Supervision Visit on 12th November 2012
According to the assessment done using the checklist, the site recorded an improved
performance of 72%, up from the previously recorded 59% in the first visit. However, the
supervision team was in the opinion that the 72% assessment as per the checklist did not
reflect the actual situation of the site. The supervision team reports that the performance of
the site was not pleasing despite having master trainers and supervisors in place. Two
supportive supervision exercises were done, one external and one internal and still no
remarkable improvement was noticed. Several challenges identified and discussed on how
to address them in the previous visit still remain unsolved:
The present setting of the room was not conducive for implementing KMC services.
In the previous visit, the HMT agreed to modify it but nothing had been done during
the second visit. In addition, the room has no furniture e.g. lockers, beds and
cupboards etc
The hospital does not provide food for patients and as result, mothers request for
premature discharge
Cleanliness of feeding utensils is not guaranteed
Information from the MoHSW does not reach the end users on time. e.g. KMC staff
had no official information of the present visit
13.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Mara KMC unit scored an average performance of 69% as
shown in the table below:

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 43
Table 13-3: Average Performance for Mara KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 1 2 1.5
3 The provider prepares the mother and the baby for KMC N/A 2 2.0
4 The provider ensures that the baby is fed correctly 0 0 0.0
5 The provider monitors the baby receiving KMC correctly 0 0 0.0
6 Infection prevention and control practices are adhered
N/A 2 2.0
7 The mother of the baby receiving KMC and her family are supported
N/A 3 3.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria N/A 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 0 1 0.5
13 Monitoring and evaluation of KMC services 3 3 3.0
Total Score 16 28 27.0
Percentage 59% 72% 69%
13.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MARA FACILITY
During the project period, 302 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 98 (32%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 58 (59%) were discharged successfully, 18 (18%) died, 7 (7%)
absconded while 15(15%) were lost to follow up as shown in the table below.
Table 13-4: Information on Pre-term and LBW Babies in Mara Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
302 N/A
LBW admitted in neonatal/postnatal ward
83 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
98 32% of total new born babies admitted at the facility
Total LBW babies 181 60% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
58 59% of LBW babies admitted in KMC
LBW babies died in KMC 18 18% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
7 7% of LBW babies admitted in KMC
LBW babies who are lost to follow
15 15% of LBW babies admitted in KMC
Average days of stay in KMC ward
4 N/A
From the results above, all the babies admitted at the KMC site were accounted for. This
shows that the site keeps proper records of KMC services. There is demand for KMC

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 44
services in the region as 181 (60%) of newborn babies were LBW babies. The number of
babies who died is also significant (18 out of 98, 18%) and the causes of death at the site
should be established and addressed to avoid further deaths.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 45
14. PERFORMANCE ASSESSMENT FOR SHINYANGA REGION
14.1. BASIC INFORMATION ON SHINYANGA KMC UNIT
The KMC services in Shinyanga region are provided at the Shinyanga Regional Referral
Hospital. The basic information about the facility is as shown in the table below as per
records of the last supervision visit:
Table 14-1: Basic Information on Shinyanga KMC Unit
Item Description
Name of health facility
Shinyanga Regional Referral Hospital
Type of health facility
Hospital
Location Shinyanga Region, Shinyanga Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 20 health workers and 2 master trainers
Health providers working in KMC
unit/ward
3
Health providers followed up after
training
1
14.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 21st June
2012 (during year 4) and on 09th January 2013 (during year 5). No supervision visits were
done in Shinyanga during year 1, 2 and 3.
14.2.1. First Supervision Visit on 21st June 2012
At the time of assessment, some performances areas were not assessed due to lack of
information. Only 9 performance areas were assessed and rated. For details of performance
areas assessed refer to Table 14-4 in sub section 14.3.3. Assessment results for assessed
areas were very good with the site’s performance rated at 93%. The demand for KMC
services is high and the available space is not enough. Documentation of KMC services is
also not properly done. There is a need for the hospital team of supervisors to conduct
regular internal supervision and document the process and results. Other challenges
identified and proposed actions are as shown in the table below:
Table 14-2: Shinyanga Challenges and Agreed Action
Challenge Action
Mothers are not fed sufficient food with required nutrients by their relatives. As a result, they demand discharge before their babies meet criteria for discharge
The Hospital to ensure that there is a continuous
education on KMC services to parents during
visits to RCH clinics
Space limitation HMT to see the possibility of expansion of the
existing room (renovation)

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 46
No link between the hospital and health facilities located at the community
HMT to look for the possibility of scaling KMC
services to district level (train health workers)
No patients cupboards for storage of mother's belongings and for babies
HMT to ensure availability of a cupboard for
storing mothers belongings and this can be placed
outside the room
14.2.2. Second Supervision Visit on 09th January 2013
During the second visit, all performance areas were assessed and the performance rated at
82%. Previous reported challenges in the first visit still remained unsolved. The available
KMC space was still small and could not meet the demand. Counseling was not properly
done, resulting to poor adherence to KMC practice.
Regarding outstanding challenges affecting KMC services at the hospital, the HMT reacted
as follows:
Table 14-3: Shinyanga HMT reaction to Outstanding Challenges
Challenge Reaction
Space limitation Extension of the ward will be discussed during
HMT meeting with RAS. The room will be
relocated to a new hospital building (Long term
plan) Poor cleaning and storage of feeding
cups
Utensils required to be purchased
No patients cupboards for storage of
mother's belongings and for babies
The cupboards will be purchased at the end of
January 2013
Poor allocation of staff trained on KMC
Re-allocation of staff to be done by the hospital
matron.
There is no system in place to sensitize
the community on KMC concept
Mothers will be sensitized during ANC visits -
Regional RCHCO. RHMT to support Master
TOTs of KMC to sensitize the community.
14.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Shinyanga KMC unit scored an average performance of 83% as
shown in the table below:
Table 14-4: Average Performance for Shinyanga KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 2 2 2.0
3 The provider prepares the mother and the baby for KMC Not rated 3 3.0
4 The provider ensures that the baby is fed correctly Not rated 2 2.0
5 The provider monitors the baby receiving KMC correctly 3 2 2.5
6 Infection prevention and control practices are adhered Not rated 2 2.0
7 The mother of the baby receiving KMC and her family are supported
Not rated 1 1.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 47
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 2 2 2.0
13 Monitoring and evaluation of KMC services 3 3 3.0
Total Score 25 32 32.5
Percentage 93% 82% 83%
14.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE SHINYANGA FACILITY
During the project period, 773 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 361 (47%) were admitted in the KMC ward. Out of those
admitted in the KMC ward, 300 (83%) were discharged successfully, 3 (1%) died, 1 (0%)
absconded while 10 (3%) were lost to follow up as shown in the table below.
Table 14-5: Information on Newborns and LBW Babies in Shinyanga Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
773 N/A
LBW admitted in neonatal/postnatal ward
328 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
361 47% of total new born babies admitted at the facility
Total LBW babies 689 89% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
300 83% of LBW babies admitted in KMC
LBW babies died in KMC 3 1% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
1 0% of LBW babies admitted in KMC
LBW babies who are lost to follow 10 3% of LBW babies admitted in KMC
Average days of stay in KMC ward
6 N/A
From the results above, 47(13%) of the babies admitted at the KMC site were not accounted
for. This shows that the site does not keep proper records of KMC services. There is
demand for KMC services in the region as 689 (89%) of new born babies were LBW babies.
Only 3 (1%) of babies admitted in the unit died. This shows that the Shinyanga unit has done
well in ensuring that deaths of babies undergoing KMC are minimized or avoided.
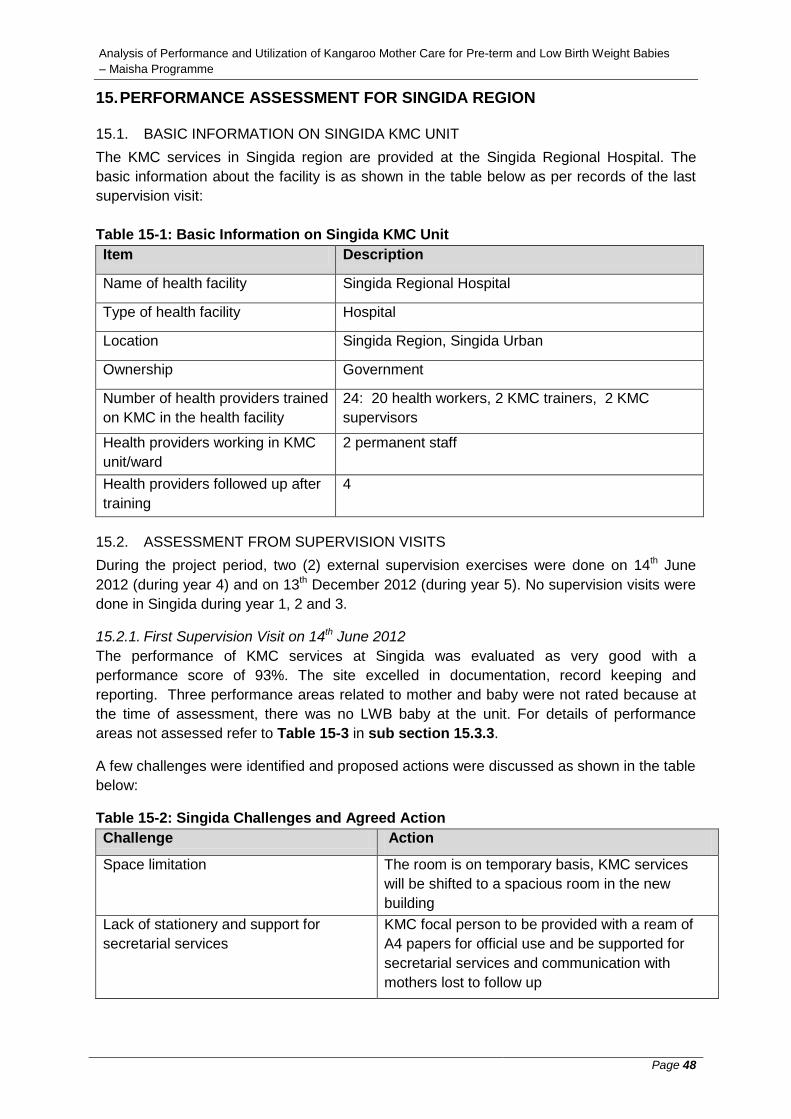
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 48
15. PERFORMANCE ASSESSMENT FOR SINGIDA REGION
15.1. BASIC INFORMATION ON SINGIDA KMC UNIT
The KMC services in Singida region are provided at the Singida Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 15-1: Basic Information on Singida KMC Unit
Item Description
Name of health facility
Singida Regional Hospital
Type of health facility
Hospital
Location Singida Region, Singida Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
24: 20 health workers, 2 KMC trainers, 2 KMC
supervisors
Health providers working in KMC
unit/ward
2 permanent staff
Health providers followed up after
training
4
15.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 14th June
2012 (during year 4) and on 13th December 2012 (during year 5). No supervision visits were
done in Singida during year 1, 2 and 3.
15.2.1. First Supervision Visit on 14th June 2012
The performance of KMC services at Singida was evaluated as very good with a
performance score of 93%. The site excelled in documentation, record keeping and
reporting. Three performance areas related to mother and baby were not rated because at
the time of assessment, there was no LWB baby at the unit. For details of performance
areas not assessed refer to Table 15-3 in sub section 15.3.3.
A few challenges were identified and proposed actions were discussed as shown in the table
below:
Table 15-2: Singida Challenges and Agreed Action
Challenge Action
Space limitation The room is on temporary basis, KMC services
will be shifted to a spacious room in the new
building
Lack of stationery and support for
secretarial services
KMC focal person to be provided with a ream of
A4 papers for official use and be supported for
secretarial services and communication with
mothers lost to follow up
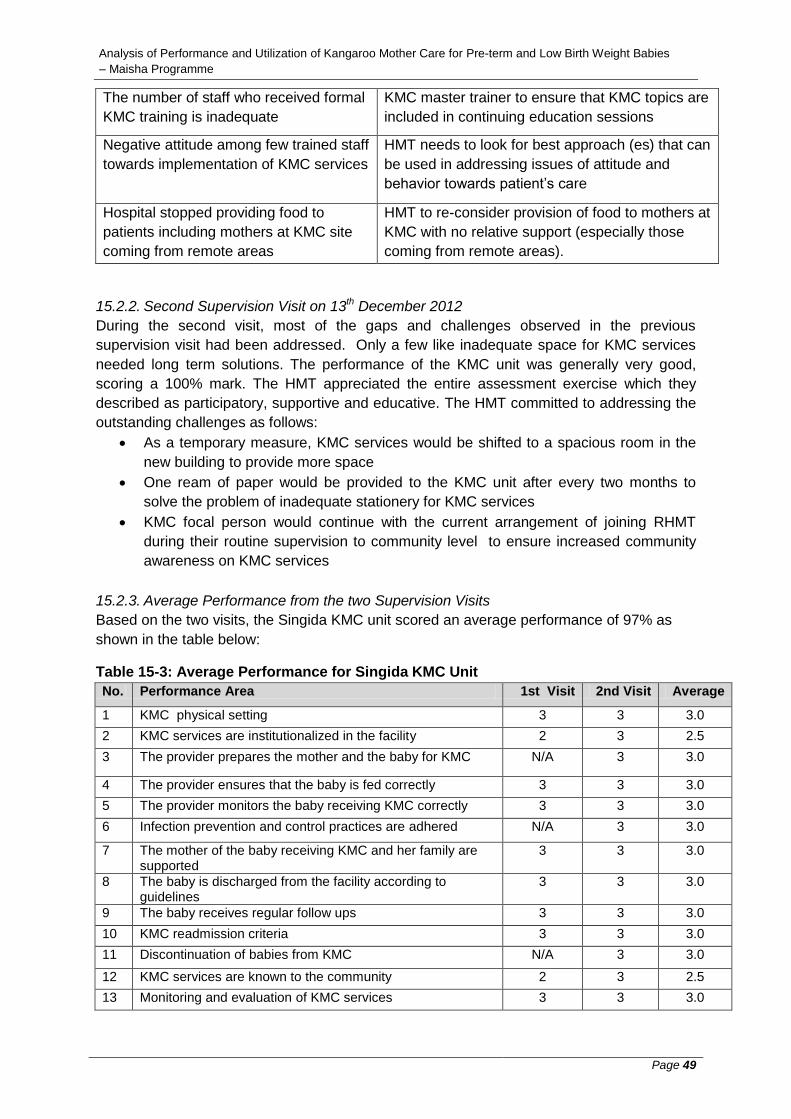
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 49
The number of staff who received formal
KMC training is inadequate
KMC master trainer to ensure that KMC topics are
included in continuing education sessions
Negative attitude among few trained staff
towards implementation of KMC services
HMT needs to look for best approach (es) that can
be used in addressing issues of attitude and
behavior towards patient’s care
Hospital stopped providing food to
patients including mothers at KMC site
coming from remote areas
HMT to re-consider provision of food to mothers at
KMC with no relative support (especially those
coming from remote areas).
15.2.2. Second Supervision Visit on 13th December 2012
During the second visit, most of the gaps and challenges observed in the previous
supervision visit had been addressed. Only a few like inadequate space for KMC services
needed long term solutions. The performance of the KMC unit was generally very good,
scoring a 100% mark. The HMT appreciated the entire assessment exercise which they
described as participatory, supportive and educative. The HMT committed to addressing the
outstanding challenges as follows:
As a temporary measure, KMC services would be shifted to a spacious room in the
new building to provide more space
One ream of paper would be provided to the KMC unit after every two months to
solve the problem of inadequate stationery for KMC services
KMC focal person would continue with the current arrangement of joining RHMT
during their routine supervision to community level to ensure increased community
awareness on KMC services
15.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Singida KMC unit scored an average performance of 97% as
shown in the table below:
Table 15-3: Average Performance for Singida KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 2 3 2.5
3 The provider prepares the mother and the baby for KMC N/A 3 3.0
4 The provider ensures that the baby is fed correctly 3 3 3.0
5 The provider monitors the baby receiving KMC correctly 3 3 3.0
6 Infection prevention and control practices are adhered N/A 3 3.0
7 The mother of the baby receiving KMC and her family are supported
3 3 3.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC N/A 3 3.0
12 KMC services are known to the community 2 3 2.5
13 Monitoring and evaluation of KMC services 3 3 3.0

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 50
Total Score 28 39 38.0
Percentage 93% 100% 97%
15.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE SINGIDA FACILITY
During the project period, 813 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 345 (42%) were admitted in the KMC ward as shown in the
table below.
Table 15-4: Information on Newborns and Pre-term and LBW Babies in Singida Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
813 N/A
LBW admitted in neonatal/postnatal ward
350 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
345 42% of total new born babies admitted at the facility
Total LBW babies 695 85% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
348 101% of LBW babies admitted in KMC
LBW babies died in KMC 5 1% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
0 0% of LBW babies admitted in KMC
LBW babies who are lost to follow
1 0% of LBW babies admitted in KMC
Average days of stay in KMC ward
3 N/A
From the results above, the sum of babies discharged, babies who died, babies absconded
and babies lost to follow exceeds the number of babies admitted at the KMC site by 9 (2%).
This shows that the site does not keep proper records of KMC services. There is demand for
KMC services in the region as 695 (85%) of new born babies were LBW babies. If the data
on deaths is correct, only 5 (1%) of babies admitted in the unit died. This shows that the
Singida unit has done well in ensuring that deaths of babies undergoing KMC are minimized
or avoided.
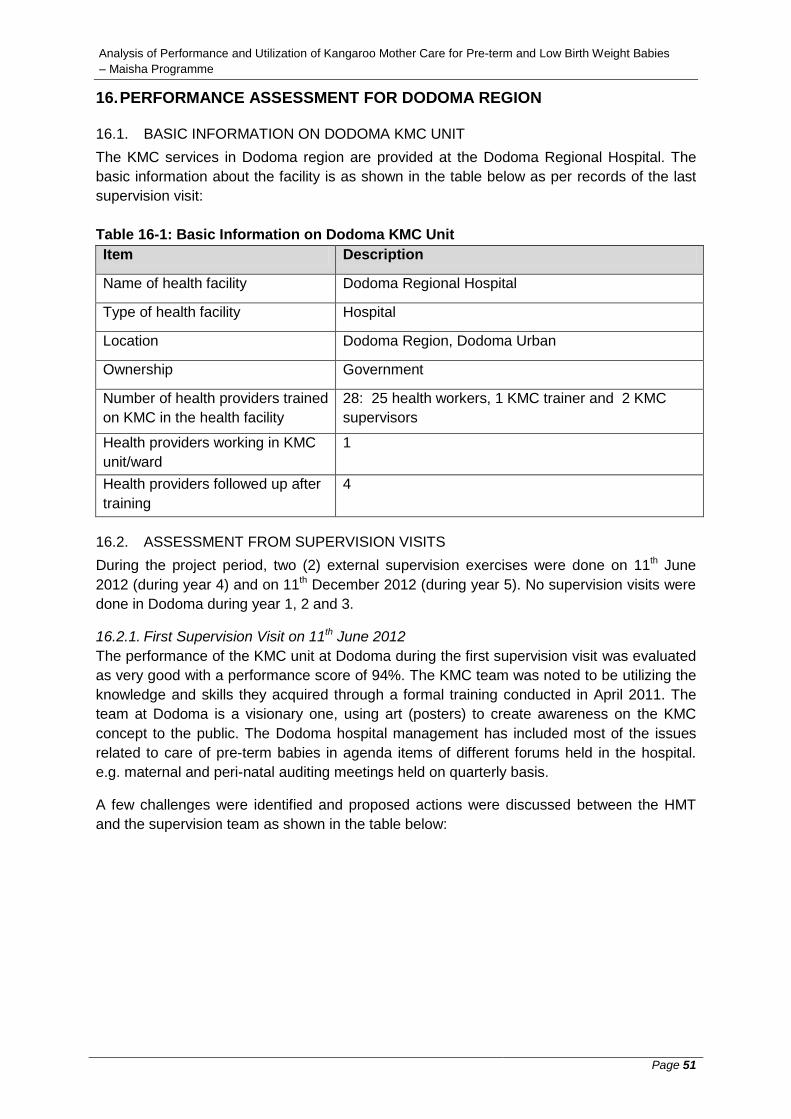
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 51
16. PERFORMANCE ASSESSMENT FOR DODOMA REGION
16.1. BASIC INFORMATION ON DODOMA KMC UNIT
The KMC services in Dodoma region are provided at the Dodoma Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 16-1: Basic Information on Dodoma KMC Unit
Item Description
Name of health facility
Dodoma Regional Hospital
Type of health facility
Hospital
Location Dodoma Region, Dodoma Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
28: 25 health workers, 1 KMC trainer and 2 KMC
supervisors
Health providers working in KMC
unit/ward
1
Health providers followed up after
training
4
16.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 11th June
2012 (during year 4) and on 11th December 2012 (during year 5). No supervision visits were
done in Dodoma during year 1, 2 and 3.
16.2.1. First Supervision Visit on 11th June 2012
The performance of the KMC unit at Dodoma during the first supervision visit was evaluated
as very good with a performance score of 94%. The KMC team was noted to be utilizing the
knowledge and skills they acquired through a formal training conducted in April 2011. The
team at Dodoma is a visionary one, using art (posters) to create awareness on the KMC
concept to the public. The Dodoma hospital management has included most of the issues
related to care of pre-term babies in agenda items of different forums held in the hospital.
e.g. maternal and peri-natal auditing meetings held on quarterly basis.
A few challenges were identified and proposed actions were discussed between the HMT
and the supervision team as shown in the table below:

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 52
Table 16-2: Dodoma Challenges and Agreed Action
Challenge Action
Available space cannot meet demand for
KMC services from neigbouring areas in
the region
HMT to discuss with RHMT to initiate and
establish a functional system that would help
other health facilities (district hospitals) to initiate
KMC services.
The location of the toilets in the present
infrastructure is not user friendly,
mothers cannot use the toilets at night
because the toilets are outside of the
ward
This will be solved once the site is moved to the
new maternity wing
Due to unreliable electricity supply, the
use of oxygen concentrator is limited and
this poses a risk to babies who need
artificial support
HMT to ensure that oxygen flow meters and nasal
proms are available at KMC site for use when the
power is off. There is also a need to have an
additional oxygen concentrator to meet the
demand
Mothers lost to follow up due to various
reasons
HMT with support from RHMT to propose a
workable system that could be used to track
mothers for follow up
16.2.2. Second Supervision Visit on 11th December 2012
During the second visit, most of the gaps and challenges observed in the previous
supervision visit had been addressed while some needed long term solutions. The
performance of the KMC unit was generally very good, scoring a 95% mark. The KMC team
was properly utilizing all their knowledge and skills from formal training to ensure success of
the KMC concept at the hospital.
16.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Dodoma KMC unit scored an average performance of 95% as
shown in the table below:
Table 16-3: Average Performance for Dodoma KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 3 3 3.0
3 The provider prepares the mother and the baby for KMC 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 3 3.0
5 The provider monitors the baby receiving KMC correctly 3 3 3.0
6 Infection prevention and control practices are adhered 3 3 3.0
7 The mother of the baby receiving KMC and her family are supported
3 3 3.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC N/A 3 3.0
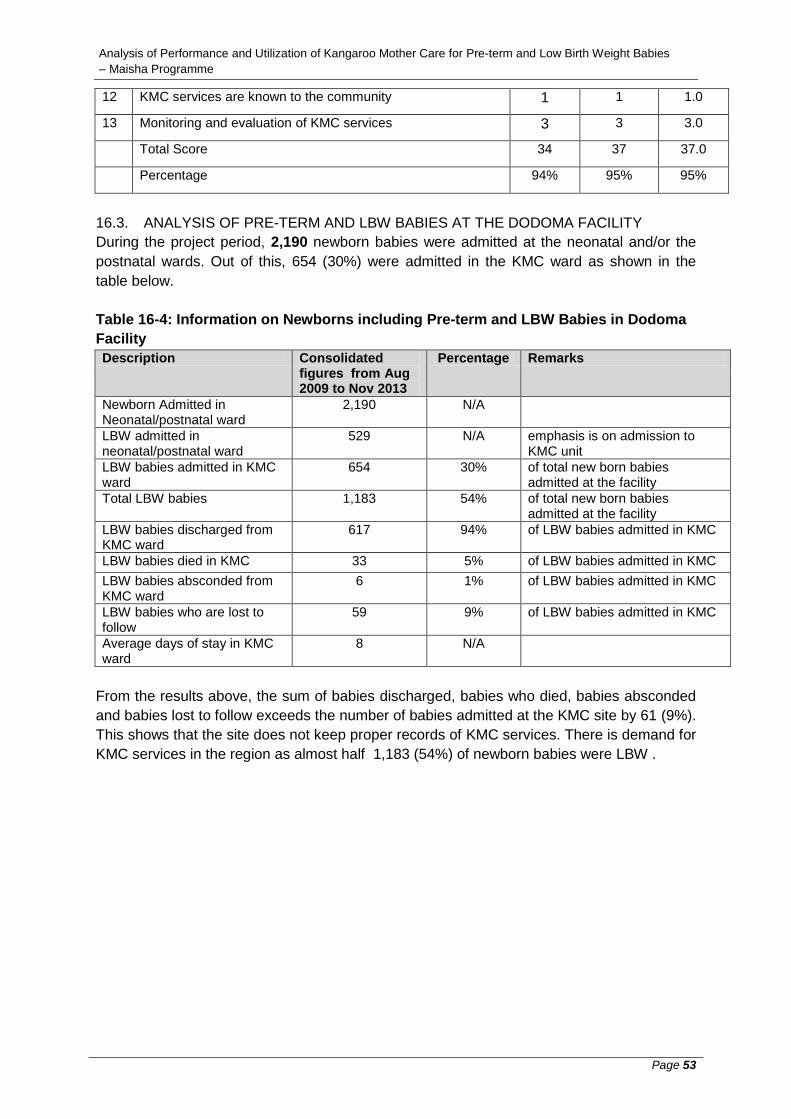
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 53
12 KMC services are known to the community 1 1 1.0
13 Monitoring and evaluation of KMC services 3 3 3.0
Total Score 34 37 37.0
Percentage 94% 95% 95%
16.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE DODOMA FACILITY
During the project period, 2,190 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 654 (30%) were admitted in the KMC ward as shown in the
table below.
Table 16-4: Information on Newborns including Pre-term and LBW Babies in Dodoma
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
2,190 N/A
LBW admitted in neonatal/postnatal ward
529 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
654 30% of total new born babies admitted at the facility
Total LBW babies 1,183 54% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
617 94% of LBW babies admitted in KMC
LBW babies died in KMC 33 5% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
6 1% of LBW babies admitted in KMC
LBW babies who are lost to follow
59 9% of LBW babies admitted in KMC
Average days of stay in KMC ward
8 N/A
From the results above, the sum of babies discharged, babies who died, babies absconded
and babies lost to follow exceeds the number of babies admitted at the KMC site by 61 (9%).
This shows that the site does not keep proper records of KMC services. There is demand for
KMC services in the region as almost half 1,183 (54%) of newborn babies were LBW .

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 54
17. PERFORMANCE ASSESSMENT FOR TANGA REGION
17.1. BASIC INFORMATION ON TANGA KMC UNIT
The KMC services in Tanga region are provided at the Bombo Regional Hospital. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 17-1: Basic Information on Tanga KMC Unit
Item Description
Name of health facility
Bombo Regional Hospital
Type of health facility
Hospital
Location Tanga Region, Tanga Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 20 health workers received formal KMC training, 2
KMC master trainers
Health providers working in KMC
unit/ward
5 nurses in the maternity ward working on rotational basis. 2 are trained in KMC and 3 are not
Health providers followed up after
training
2
17.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, two (2) external supervision exercises were done on 30th March
2012 (during year 4) and on 29th January 2013 (during year 5). No supervision visits were
done in Tanga during year 1, 2 and 3.
17.2.1. First Supervision Visit on 30th March 2012
The performance of the KMC unit at Tanga during the first supervision visit was evaluated as
very good with a performance score of 92%. The KMC team was noted to be very committed
to their work and was making efforts ensure that everyone visiting the site got a message on
the KMC concept. It was also observed that there was a lot of support from the hospital
management team. Out of all the 19 KMC sites, Tanga is the only site where KMC services
have been institutionalized. There is a lot of sharing and learning through continuous
education, a session held every month and includes all staff, medical and nurses students
including Intern doctors.
17.2.2. Second Supervision Visit on 29th January 2013
During the second visit, it was assessed that the performance was still good although it had
dropped to 82% from the previous 92% assessed during the first visit. Despite the drop in
assessed performance, the HMT was still very supportive in delivering KMC services. The
hospital team appreciated the assessment exercise which they termed as participatory,
supportive and helpful. The assessment exercise made them gain knowledge and skills on
KMC services which they would use to improve areas where gaps were identified. Several
gaps were identified that led to the drop, most of which were associated with inadequate
knowledge and skills of health workers to provide quality KMC services. These gaps are
listed below:

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 55
Inadequate space for KMC services.
Low understanding level of some mothers resulting to failure in adhering to
KMC practice
Shortage of trained personnel for KMC unit
Lack of utensils for cleaning and storing feeding cups.
Lack of essential equipments/supplies for use in KMC. e.g. oxygen
concentrator, digital weighing scale were out of order, electric kettle, gowns,
shoes and basins
It was unfortunate that at the time of concluding the assessment, the MOI/C and the HMT
were not available for feedback and discussion on the way forward to address the identified
gaps. The MOI/C and the HMT were in a series of meetings with the Regional
Commissioner.
17.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Tanga KMC unit scored an average performance of 87% as
shown in the table below:
Table 17-2: Average Performance for Tanga KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 2 2 2.0
2 KMC services are institutionalized in the facility 3 2 2.5
3 The provider prepares the mother and the baby for KMC 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 2 2.5
5 The provider monitors the baby receiving KMC correctly 3 2 2.5
6 Infection prevention and control practices are adhered 2 2 2.0
7 The mother of the baby receiving KMC and her family are supported
2 3 2.5
8 The baby is discharged from the facility according to guidelines
3 2 2.5
9 The baby receives regular follow ups 3 3 3.0
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 3 2 2.5
13 Monitoring and evaluation of KMC services 3 3 3.0
Total Score 36 32 34.0
Percentage 92% 82% 87%
17.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE TANGA FACILITY
During the project period, 1,908 newborn babies were admitted at the neonatal and/or the
postnatal wards. Out of this, 460 (24%) were admitted in the KMC ward as shown in the
table below.
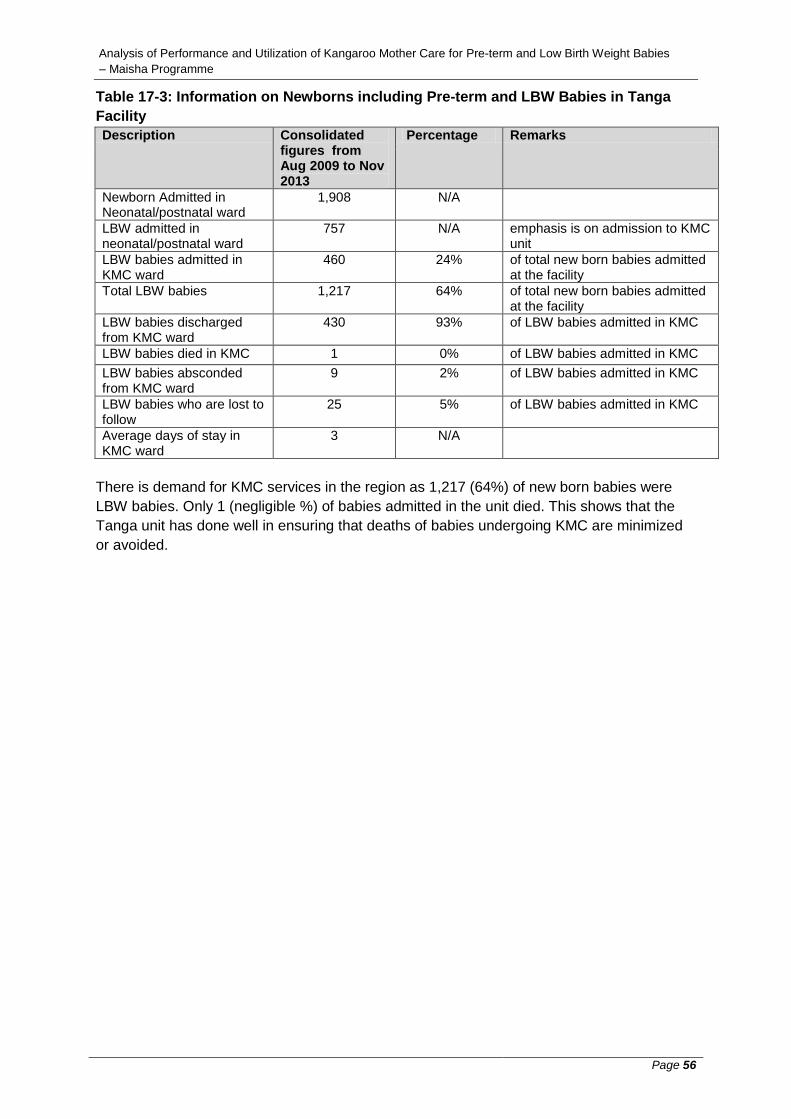
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 56
Table 17-3: Information on Newborns including Pre-term and LBW Babies in Tanga
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
1,908 N/A
LBW admitted in neonatal/postnatal ward
757 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
460 24% of total new born babies admitted at the facility
Total LBW babies 1,217 64% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
430 93% of LBW babies admitted in KMC
LBW babies died in KMC 1 0% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
9 2% of LBW babies admitted in KMC
LBW babies who are lost to follow
25 5% of LBW babies admitted in KMC
Average days of stay in KMC ward
3 N/A
There is demand for KMC services in the region as 1,217 (64%) of new born babies were
LBW babies. Only 1 (negligible %) of babies admitted in the unit died. This shows that the
Tanga unit has done well in ensuring that deaths of babies undergoing KMC are minimized
or avoided.
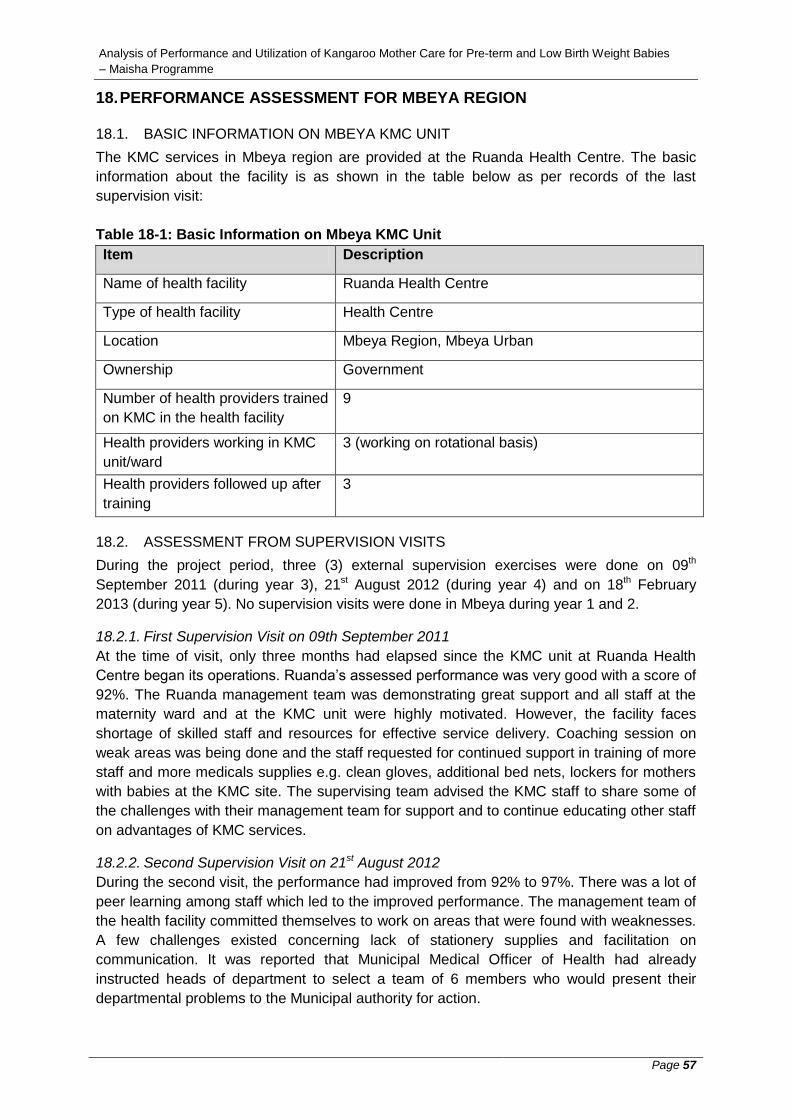
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 57
18. PERFORMANCE ASSESSMENT FOR MBEYA REGION
18.1. BASIC INFORMATION ON MBEYA KMC UNIT
The KMC services in Mbeya region are provided at the Ruanda Health Centre. The basic
information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 18-1: Basic Information on Mbeya KMC Unit
Item Description
Name of health facility
Ruanda Health Centre
Type of health facility
Health Centre
Location Mbeya Region, Mbeya Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
9
Health providers working in KMC
unit/ward
3 (working on rotational basis)
Health providers followed up after
training
3
18.2. ASSESSMENT FROM SUPERVISION VISITS
During the project period, three (3) external supervision exercises were done on 09th
September 2011 (during year 3), 21st August 2012 (during year 4) and on 18th February
2013 (during year 5). No supervision visits were done in Mbeya during year 1 and 2.
18.2.1. First Supervision Visit on 09th September 2011
At the time of visit, only three months had elapsed since the KMC unit at Ruanda Health
Centre began its operations. Ruanda’s assessed performance was very good with a score of
92%. The Ruanda management team was demonstrating great support and all staff at the
maternity ward and at the KMC unit were highly motivated. However, the facility faces
shortage of skilled staff and resources for effective service delivery. Coaching session on
weak areas was being done and the staff requested for continued support in training of more
staff and more medicals supplies e.g. clean gloves, additional bed nets, lockers for mothers
with babies at the KMC site. The supervising team advised the KMC staff to share some of
the challenges with their management team for support and to continue educating other staff
on advantages of KMC services.
18.2.2. Second Supervision Visit on 21st August 2012
During the second visit, the performance had improved from 92% to 97%. There was a lot of
peer learning among staff which led to the improved performance. The management team of
the health facility committed themselves to work on areas that were found with weaknesses.
A few challenges existed concerning lack of stationery supplies and facilitation on
communication. It was reported that Municipal Medical Officer of Health had already
instructed heads of department to select a team of 6 members who would present their
departmental problems to the Municipal authority for action.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 58
18.2.3. Third Supervision Visit on 18th February 2013
Performance assessment during the third supervision visit showed that the KMC services
were performing well at a score of 95%. Most of the gaps identified in previous visits had
already been addressed. The unit was warm and very clean, all four beds were occupied,
and services were being offered as required. The management team appreciated that the
exercise was very participatory and have promised to work further on areas that were still
found with some weaknesses.
18.2.4. Average Performance from the three Supervision Visits
Based on the three visits, the Mbeya KMC unit scored an average performance of 95% as
shown in the table below:
Table 18-2: Average Performance for Mbeya KMC Unit
No. Performance Area 1st Visit
2nd Visit
3rd Visit
Average
1 KMC physical setting 2 3 3 2.7
2 KMC services are institutionalized in the facility 3 3 3 3.0
3 The provider prepares the mother and the baby for KMC
3 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 3 3 3.0
5 The provider monitors the baby receiving KMC correctly
3 3 3 3.0
6 Infection prevention and control practices are adhered 3 3 3 3.0
7 The mother of the baby receiving KMC and her family are supported
3 3 3 3.0
8 The baby is discharged from the facility according to guidelines
3 3 3 3.0
9 The baby receives regular follow ups 3 3 3 3.0
10 KMC readmission criteria 3 3 3 3.0
11 Discontinuation of babies from KMC 3 3 3 3.0
12 KMC services are known to the community 2 3 1 2.0
13 Monitoring and evaluation of KMC services 2 2 3 2.3
Total Score 36 38 37 37.0
Percentage 92% 97% 95% 95%
18.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE MBEYA FACILITY
During the project period, no data was available on the number of new born babies admitted
at the neonatal and/or the postnatal wards. There were 199 LBW babies admitted in the
KMC ward, and out of this, 143 (72%) were discharged, 2 (1%) died, none absconded and 2
(1%) were lost to follow up as shown in the table below.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 59
Table 18-3: Information on Newborns including Pre-term and LBW Babies in Mbeya
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage
Remarks
Newborn Admitted in Neonatal/postnatal ward
0 N/A
LBW admitted in neonatal/postnatal ward
57 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
199 N/A
Total LBW babies 256 N/A
LBW babies discharged from KMC ward
143 72% of LBW babies admitted in KMC
LBW babies died in KMC 2 1% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
0 0% of LBW babies admitted in KMC
LBW babies who are lost to follow
2 1% of LBW babies admitted in KMC
Average days of stay in KMC ward
4 N/A
Only 2 (1%) of babies admitted in the unit died. This shows that the unit has done well in
ensuring that deaths of babies undergoing KMC are minimized or avoided. However, from
the above results, 52 (26%) of babies admitted at the KMC site were not accounted for. This
shows that the site does not keep proper records of KMC services.
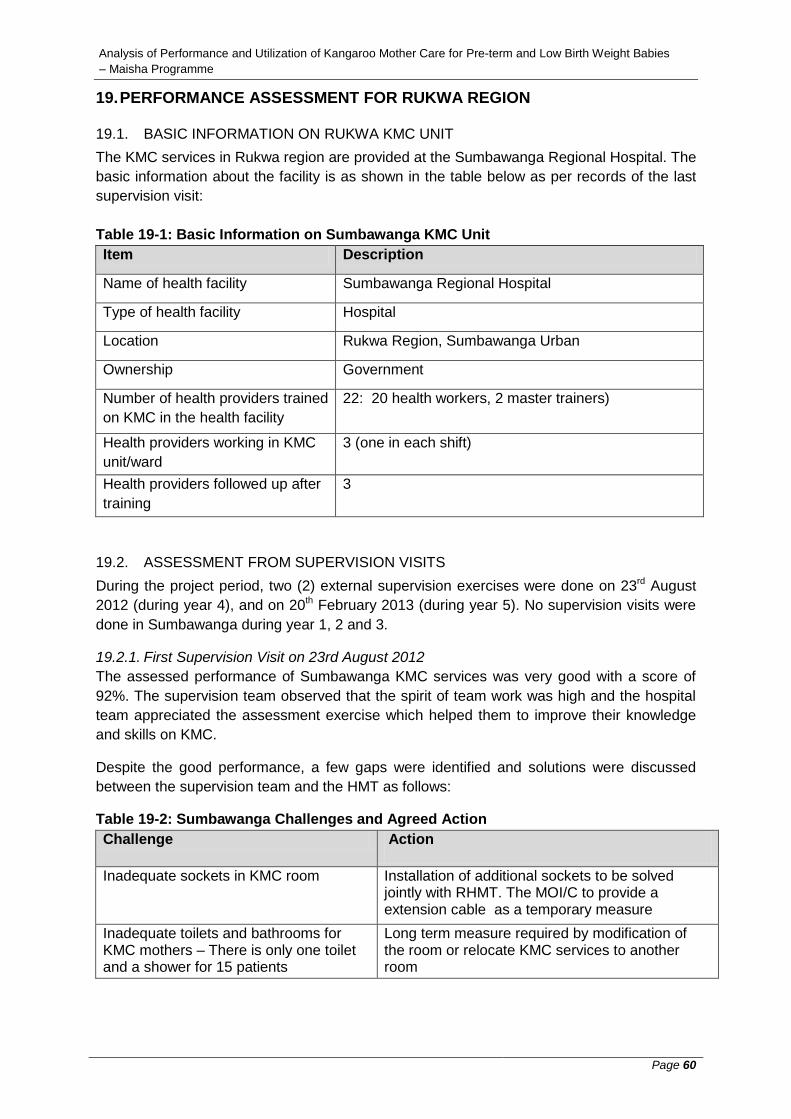
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 60
19. PERFORMANCE ASSESSMENT FOR RUKWA REGION
19.1. BASIC INFORMATION ON RUKWA KMC UNIT The KMC services in Rukwa region are provided at the Sumbawanga Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 19-1: Basic Information on Sumbawanga KMC Unit
Item Description
Name of health facility
Sumbawanga Regional Hospital
Type of health facility
Hospital
Location Rukwa Region, Sumbawanga Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
22: 20 health workers, 2 master trainers)
Health providers working in KMC
unit/ward
3 (one in each shift)
Health providers followed up after
training
3
19.2. ASSESSMENT FROM SUPERVISION VISITS During the project period, two (2) external supervision exercises were done on 23rd August
2012 (during year 4), and on 20th February 2013 (during year 5). No supervision visits were
done in Sumbawanga during year 1, 2 and 3.
19.2.1. First Supervision Visit on 23rd August 2012
The assessed performance of Sumbawanga KMC services was very good with a score of
92%. The supervision team observed that the spirit of team work was high and the hospital
team appreciated the assessment exercise which helped them to improve their knowledge
and skills on KMC.
Despite the good performance, a few gaps were identified and solutions were discussed
between the supervision team and the HMT as follows:
Table 19-2: Sumbawanga Challenges and Agreed Action
Challenge Action
Inadequate sockets in KMC room Installation of additional sockets to be solved jointly with RHMT. The MOI/C to provide a extension cable as a temporary measure
Inadequate toilets and bathrooms for KMC mothers – There is only one toilet and a shower for 15 patients
Long term measure required by modification of the room or relocate KMC services to another room

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 61
Inadequate support on secretarial and communication services from HMT
To be discussed during the therapeutic committee meeting which is a forum to discuss and solve hospital matters
There is no system to track mothers who are lost to follow up due to distance
To be discussed during the therapeutic committee meeting which is a forum to discuss and solve hospital matters
Lack of awareness on KMC concept at community as far as peripheral level
Issue to be discussed this with the RHMT
19.2.2. Second Supervision Visit on 20th February 2013
In the second assessment, the performance dropped from the previously recorded 92% in
the first assessment to 72%. General performance was not pleasing and through a question
and answer session, it was observed that the level of understanding of KMC guidelines by
KMC team was still low. This resulted to failure by the team to provide quality KMC services
in areas of pre and post counseling, documentation of the neonates’ information, criteria for
admission, discharge and follow up not adhered to and posters with advocacy messages
related to the three KMC elements (positioning, support and feeding) not utilized.
Communication barrier still existed because some of the responsible key staff were not
aware of the visit despite notification letters sent by the MoHSW to the RMO about the visit.
The KMC room was spacious and well ventilated but needed an additional heater due to the
cold weather. The room thermometer was not in place to measure room temperature.
Gaps previously identified in the first visit still persisted. There were inadequate toilets and
bathrooms for KMC mothers, there was no system to track mothers who were lost to follow
up and there was no awareness on KMC concept at community level. During the feedback
meeting, the Deputy MOI/C urged every member of staff especially those who received
formal KMC training to play their role in supporting provision of quality KMC services. The
KMC focal person was requested to improve the overall management of the KMC unit with
special focus on documentation of neonates’ information. The staff working at the unit were
requested to be pro active in seeking assistance from the KMC master supervisors or master
trainers.
19.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Rukwa KMC unit scored an average performance of 85% as
shown in the table below:
Table 19-2: Average Performance for Rukwa KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 2 3 2.5
2 KMC services are institutionalized in the facility 3 3 3.0
3 The provider prepares the mother and the baby for KMC 3 3 3.0
4 The provider ensures that the baby is fed correctly 3 2 2.5
5 The provider monitors the baby receiving KMC correctly 3 1 2.0
6 Infection prevention and control practices are adhered 3 2 2.5
7 The mother of the baby receiving KMC and her family are supported
3 1 2.0
8 The baby is discharged from the facility according to guidelines
3 3 3.0
9 The baby receives regular follow ups 3 3 3.0

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 62
10 KMC readmission criteria 3 3 3.0
11 Discontinuation of babies from KMC 3 3 3.0
12 KMC services are known to the community 2 2 2.0
13 Monitoring and evaluation of KMC services 2 1 1.5
Total Score 36.0 30.0 33.0
Percentage 92% 77% 85%
19.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE RUKWA FACILITY
During the project period, there were 233 LBW babies admitted in the KMC ward, and out of
this, 163 (70%) were discharged, 33 (14%) died, 4 (2%) absconded and 22 (9%) were lost to
follow up as shown in the table below.
Table 19-3: Information on Newborns including Pre-term and LBW Babies in Rukwa
Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage
Remarks
Newborn Admitted in Neonatal/postnatal ward
366 N/A
LBW admitted in neonatal/postnatal ward
203 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
233 64% of total new born babies admitted at the facility
Total LBW babies 436 119% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
163 70% of LBW babies admitted in KMC
LBW babies died in KMC 33 14% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
4 2% of LBW babies admitted in KMC
LBW babies who are lost to follow
22 9% of LBW babies admitted in KMC
Average days of stay in KMC ward
4 N/A
However, from the above results, 11 (5%) of babies admitted at the KMC ward were not
accounted for. The sum of LBW babies admitted at the KMC ward and the
neonatal/postnatal wards also exceeds the total number of newborns admitted at the
hospital. This shows that the site does not keep proper records of KMC services. The
number of children who died is also quite significant and the KMC staff together with the
hospital management should establish the causes and address them to stop further deaths.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 63
20. PERFORMANCE ASSESSMENT FOR KILIMANJARO REGION
20.1. BASIC INFORMATION ON KILIMANJARO KMC UNIT The KMC services in Kilimanjaro region are provided at the Mawenzi Regional Hospital. The
basic information about the facility is as shown in the table below as per records of the last
supervision visit:
Table 20-1: Basic Information on Kilimanjaro KMC Unit
Item Description
Name of health facility
Mawenzi Regional Hospital
Type of health facility
Hospital
Location Kilimanjaro Region, Moshi Urban
Ownership
Government
Number of health providers trained
on KMC in the health facility
31: 29 health workers had formal KMC training, 2
master trainers)
Health providers working in KMC
unit/ward
3
Health providers followed up after
training
2
20.2. ASSESSMENT FROM SUPERVISION VISITS During the project period, two (2) external supportive supervision visits were done on 26th
July 2012 (during year 4), and on 21st May 2013 (during year 5). No supervision visits were
done in Kilimanjaro during year 1, 2 and 3.
20.2.1. First Supervision Visit on 26th July 2012
Although the physical outlook of the KMC unit was very good with adequate space, well
arrangement and clean, the assessed performance was not good. The KMC site scored 58%
with many gaps being identified. The KMC staff seemed not to have adequate knowledge
and skills on provision of quality KMC services. Other challenges identified are:
Mothers lost to follow up due to lack of tracking system
Poor cleaning and storage of feeding cups
Electrical wall sockets were not enough
The hospital does not provide food for patients. As a result mothers admitted
at the KMC unit tend to request for early discharge.
Staff allocated to work in the KMC unit are not trained
The hospital management promised to provide a TV for recreation but no
follow up was done.
20.2.2. Second Supervision Visit on 21st May 2013
In the second visit, the physical set up and general cleanliness of the unit was still very good
and the unit met all the requirements for provision of KMC services. The unit had adequate
space, good ventilation and was well arranged. The assessed performance improved from
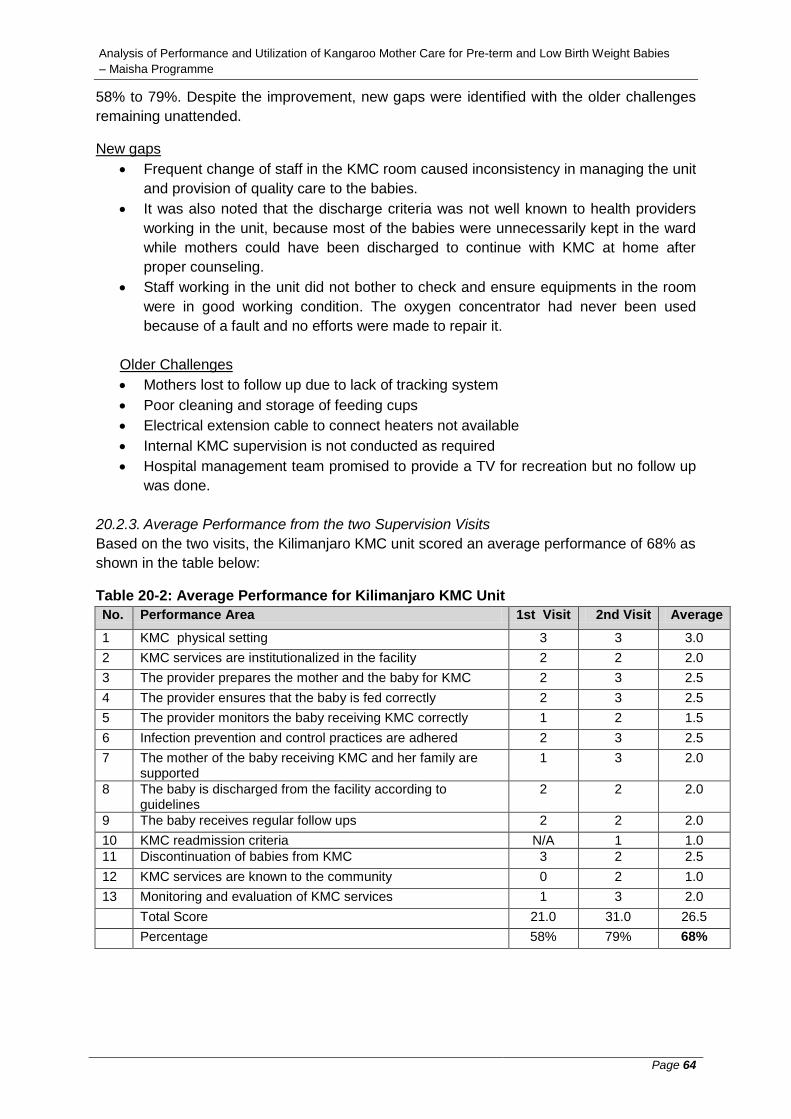
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 64
58% to 79%. Despite the improvement, new gaps were identified with the older challenges
remaining unattended.
New gaps
Frequent change of staff in the KMC room caused inconsistency in managing the unit
and provision of quality care to the babies.
It was also noted that the discharge criteria was not well known to health providers
working in the unit, because most of the babies were unnecessarily kept in the ward
while mothers could have been discharged to continue with KMC at home after
proper counseling.
Staff working in the unit did not bother to check and ensure equipments in the room
were in good working condition. The oxygen concentrator had never been used
because of a fault and no efforts were made to repair it.
Older Challenges
Mothers lost to follow up due to lack of tracking system
Poor cleaning and storage of feeding cups
Electrical extension cable to connect heaters not available
Internal KMC supervision is not conducted as required
Hospital management team promised to provide a TV for recreation but no follow up
was done.
20.2.3. Average Performance from the two Supervision Visits
Based on the two visits, the Kilimanjaro KMC unit scored an average performance of 68% as
shown in the table below:
Table 20-2: Average Performance for Kilimanjaro KMC Unit
No. Performance Area 1st Visit 2nd Visit Average
1 KMC physical setting 3 3 3.0
2 KMC services are institutionalized in the facility 2 2 2.0
3 The provider prepares the mother and the baby for KMC 2 3 2.5
4 The provider ensures that the baby is fed correctly 2 3 2.5
5 The provider monitors the baby receiving KMC correctly 1 2 1.5
6 Infection prevention and control practices are adhered 2 3 2.5
7 The mother of the baby receiving KMC and her family are supported
1 3 2.0
8 The baby is discharged from the facility according to guidelines
2 2 2.0
9 The baby receives regular follow ups 2 2 2.0
10 KMC readmission criteria N/A 1 1.0
11 Discontinuation of babies from KMC 3 2 2.5
12 KMC services are known to the community 0 2 1.0
13 Monitoring and evaluation of KMC services 1 3 2.0
Total Score 21.0 31.0 26.5
Percentage 58% 79% 68%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 65
20.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE KILIMANJARO FACILITY
During the project period, there were 167 LBW babies admitted in the KMC ward, and out of
this, 129(77%) were discharged, 7(4%) died, 1(1%) was absconded and 1(1%) was lost to
follow as shown in the table below.
Table 20-3: Information on Newborns including Pre-term and LBW Babies in
Kilimanjaro Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
330 N/A
LBW admitted in neonatal/postnatal ward
167 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
167 51% of total new born babies admitted at the facility
Total LBW babies 334 101% of total new born babies admitted at the facility
LBW babies discharged from KMC ward
129 77% of LBW babies admitted in KMC
LBW babies died in KMC 7 4% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
1 1% of LBW babies admitted in KMC
LBW babies who are lost to follow
1 1% of LBW babies admitted in KMC
Average days of stay in KMC ward
9 N/A
However, from the above results, 29 (17%) of babies admitted at the KMC ward were not
accounted for. The sum of LBW babies admitted at the KMC ward and the
neonatal/postnatal wards also exceeds the total number of newborns admitted at the
hospital. This shows that the site does not keep proper records of KMC services.

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 66
21. PERFORMANCE ASSESSMENT FOR DAR ES SALAAM REGION
21.1. BASIC INFORMATION ON DAR ES SALAAM KMC UNIT The KMC services in Dar es Salaam region are provided at the Mbagala Rangi Tatu Health
Centre. The basic information about the facility is as shown in the table below as per records
of the last supervision visit:
Table 21-1: Basic Information on Dar es Salaam KMC Unit
Item Description
Name of health facility
Mbagala Rangi Tatu Health Centre
Type of health facility
Health Centre
Location Dar es salaam Region, Temeke Municipality
Ownership
Government
Number of health providers trained
on KMC in the health facility
6: 4 trained under MAISHA and 2 health workers by
CCBRT
Health providers working in KMC
unit/ward
3 (working on a rotation basis)
Health providers followed up after
training
2
21.2. ASSESSMENT FROM SUPERVISION VISITS During the project period, only one (1) external supervision exercise was done on 01st
November 2012 (during year 5). No supervision visits were done in Dar es Salaam during
year 1, 2, 3 and 4.
The assessed performance was very good with the KMC unit scoring 95%. The assessment
exercise was carried out in a participatory and supportive manner. The spirit of team work
was high at the site. A better performance would have been achieved if more support from
the health centre management was extended to the KMC team.
A number of challenges were also identified as follows:
Inadequate toilets and bathrooms for KMC mothers. There is only one toilet and a
shower for 8 patients
Mothers demand early discharge due to lack of food
Mothers look untidy with casual clothes; they need 3 uniforms per patient and
napkins
No clothe line within the laundry, the lining space is outside
There is shortage of staff.
The is lack of awareness on KMC concept at the local level in the community
Since only one external supervision exercise was done, it can be assumed that the average
performance for the unit is 95% as shown in the table below:
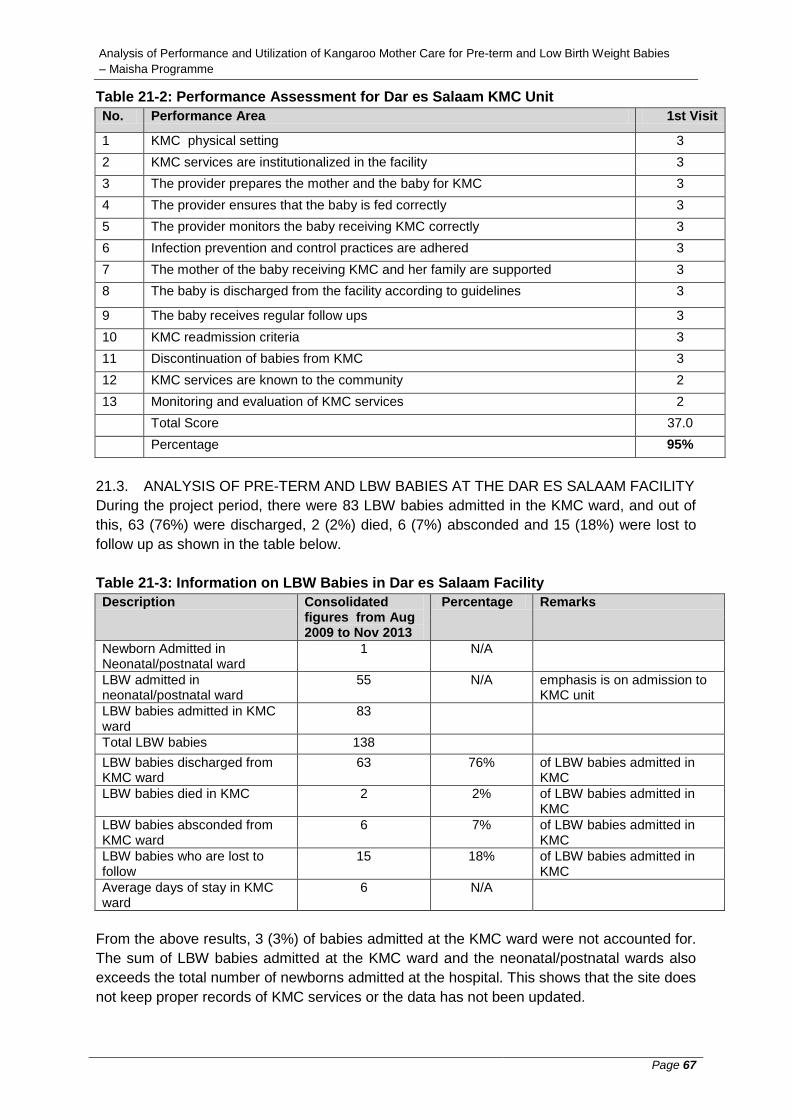
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 67
Table 21-2: Performance Assessment for Dar es Salaam KMC Unit
No. Performance Area 1st Visit
1 KMC physical setting 3
2 KMC services are institutionalized in the facility 3
3 The provider prepares the mother and the baby for KMC 3
4 The provider ensures that the baby is fed correctly 3
5 The provider monitors the baby receiving KMC correctly 3
6 Infection prevention and control practices are adhered 3
7 The mother of the baby receiving KMC and her family are supported 3
8 The baby is discharged from the facility according to guidelines 3
9 The baby receives regular follow ups 3
10 KMC readmission criteria 3
11 Discontinuation of babies from KMC 3
12 KMC services are known to the community 2
13 Monitoring and evaluation of KMC services 2
Total Score 37.0
Percentage 95%
21.3. ANALYSIS OF PRE-TERM AND LBW BABIES AT THE DAR ES SALAAM FACILITY
During the project period, there were 83 LBW babies admitted in the KMC ward, and out of
this, 63 (76%) were discharged, 2 (2%) died, 6 (7%) absconded and 15 (18%) were lost to
follow up as shown in the table below.
Table 21-3: Information on LBW Babies in Dar es Salaam Facility
Description Consolidated figures from Aug 2009 to Nov 2013
Percentage Remarks
Newborn Admitted in Neonatal/postnatal ward
1 N/A
LBW admitted in neonatal/postnatal ward
55 N/A emphasis is on admission to KMC unit
LBW babies admitted in KMC ward
83
Total LBW babies 138
LBW babies discharged from KMC ward
63 76% of LBW babies admitted in KMC
LBW babies died in KMC 2 2% of LBW babies admitted in KMC
LBW babies absconded from KMC ward
6 7% of LBW babies admitted in KMC
LBW babies who are lost to follow
15 18% of LBW babies admitted in KMC
Average days of stay in KMC ward
6 N/A
From the above results, 3 (3%) of babies admitted at the KMC ward were not accounted for.
The sum of LBW babies admitted at the KMC ward and the neonatal/postnatal wards also
exceeds the total number of newborns admitted at the hospital. This shows that the site does
not keep proper records of KMC services or the data has not been updated.
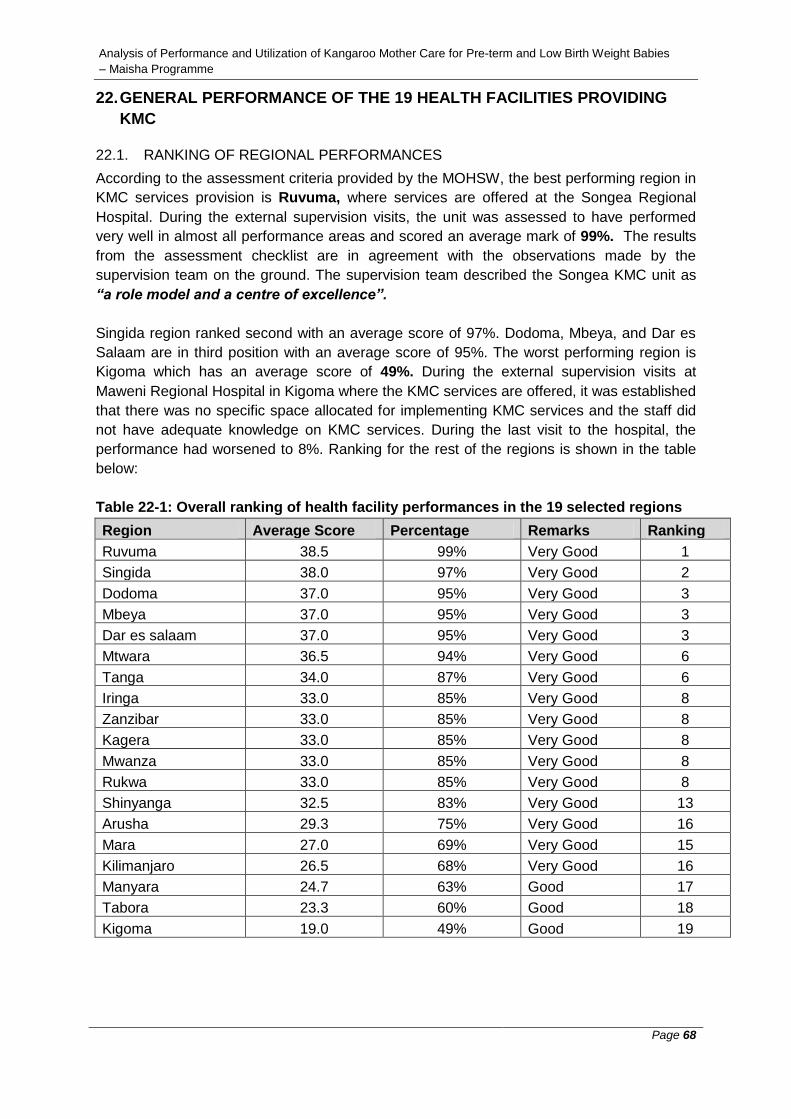
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 68
22. GENERAL PERFORMANCE OF THE 19 HEALTH FACILITIES PROVIDING
KMC
22.1. RANKING OF REGIONAL PERFORMANCES
According to the assessment criteria provided by the MOHSW, the best performing region in
KMC services provision is Ruvuma, where services are offered at the Songea Regional
Hospital. During the external supervision visits, the unit was assessed to have performed
very well in almost all performance areas and scored an average mark of 99%. The results
from the assessment checklist are in agreement with the observations made by the
supervision team on the ground. The supervision team described the Songea KMC unit as
“a role model and a centre of excellence”.
Singida region ranked second with an average score of 97%. Dodoma, Mbeya, and Dar es
Salaam are in third position with an average score of 95%. The worst performing region is
Kigoma which has an average score of 49%. During the external supervision visits at
Maweni Regional Hospital in Kigoma where the KMC services are offered, it was established
that there was no specific space allocated for implementing KMC services and the staff did
not have adequate knowledge on KMC services. During the last visit to the hospital, the
performance had worsened to 8%. Ranking for the rest of the regions is shown in the table
below:
Table 22-1: Overall ranking of health facility performances in the 19 selected regions
Region Average Score Percentage Remarks Ranking
Ruvuma 38.5 99% Very Good 1
Singida 38.0 97% Very Good 2
Dodoma 37.0 95% Very Good 3
Mbeya 37.0 95% Very Good 3
Dar es salaam 37.0 95% Very Good 3
Mtwara 36.5 94% Very Good 6
Tanga 34.0 87% Very Good 6
Iringa 33.0 85% Very Good 8
Zanzibar 33.0 85% Very Good 8
Kagera 33.0 85% Very Good 8
Mwanza 33.0 85% Very Good 8
Rukwa 33.0 85% Very Good 8
Shinyanga 32.5 83% Very Good 13
Arusha 29.3 75% Very Good 16
Mara 27.0 69% Very Good 15
Kilimanjaro 26.5 68% Very Good 16
Manyara 24.7 63% Good 17
Tabora 23.3 60% Good 18
Kigoma 19.0 49% Good 19

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 69
22.2. PERFORMANCE PER GRADING CRITERIA
According to the assessment criteria provided by the MOHSW, 16 regions (84%) performed
“very good”, 3 (16%) performed “good” while none performed “weak” as shown in the
summarized assessment table below:
Table 22-2: Performance per Grading Criteria
Assessment Score No. of Regions Percentage
Very Good 67-100% 16 84%
Good 33-66% 3 16%
Weak Below 33% 0 0%
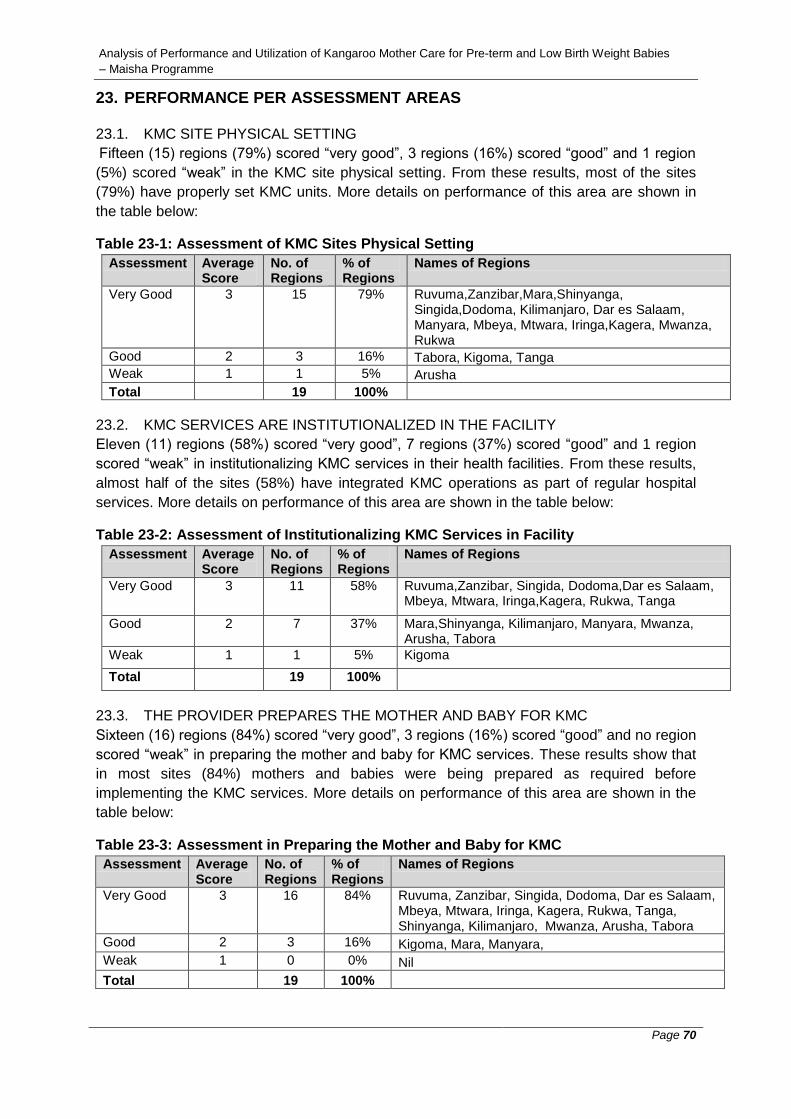
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 70
23. PERFORMANCE PER ASSESSMENT AREAS
23.1. KMC SITE PHYSICAL SETTING
Fifteen (15) regions (79%) scored “very good”, 3 regions (16%) scored “good” and 1 region
(5%) scored “weak” in the KMC site physical setting. From these results, most of the sites
(79%) have properly set KMC units. More details on performance of this area are shown in
the table below:
Table 23-1: Assessment of KMC Sites Physical Setting
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 15 79% Ruvuma,Zanzibar,Mara,Shinyanga, Singida,Dodoma, Kilimanjaro, Dar es Salaam, Manyara, Mbeya, Mtwara, Iringa,Kagera, Mwanza, Rukwa
Good 2 3 16% Tabora, Kigoma, Tanga
Weak 1 1 5% Arusha
Total 19 100%
23.2. KMC SERVICES ARE INSTITUTIONALIZED IN THE FACILITY
Eleven (11) regions (58%) scored “very good”, 7 regions (37%) scored “good” and 1 region
scored “weak” in institutionalizing KMC services in their health facilities. From these results,
almost half of the sites (58%) have integrated KMC operations as part of regular hospital
services. More details on performance of this area are shown in the table below:
Table 23-2: Assessment of Institutionalizing KMC Services in Facility
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 11 58% Ruvuma,Zanzibar, Singida, Dodoma,Dar es Salaam, Mbeya, Mtwara, Iringa,Kagera, Rukwa, Tanga
Good 2 7 37% Mara,Shinyanga, Kilimanjaro, Manyara, Mwanza, Arusha, Tabora
Weak 1 1 5% Kigoma
Total 19 100%
23.3. THE PROVIDER PREPARES THE MOTHER AND BABY FOR KMC
Sixteen (16) regions (84%) scored “very good”, 3 regions (16%) scored “good” and no region
scored “weak” in preparing the mother and baby for KMC services. These results show that
in most sites (84%) mothers and babies were being prepared as required before
implementing the KMC services. More details on performance of this area are shown in the
table below:
Table 23-3: Assessment in Preparing the Mother and Baby for KMC
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 16 84% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Kagera, Rukwa, Tanga, Shinyanga, Kilimanjaro, Mwanza, Arusha, Tabora
Good 2 3 16% Kigoma, Mara, Manyara,
Weak 1 0 0% Nil
Total 19 100%
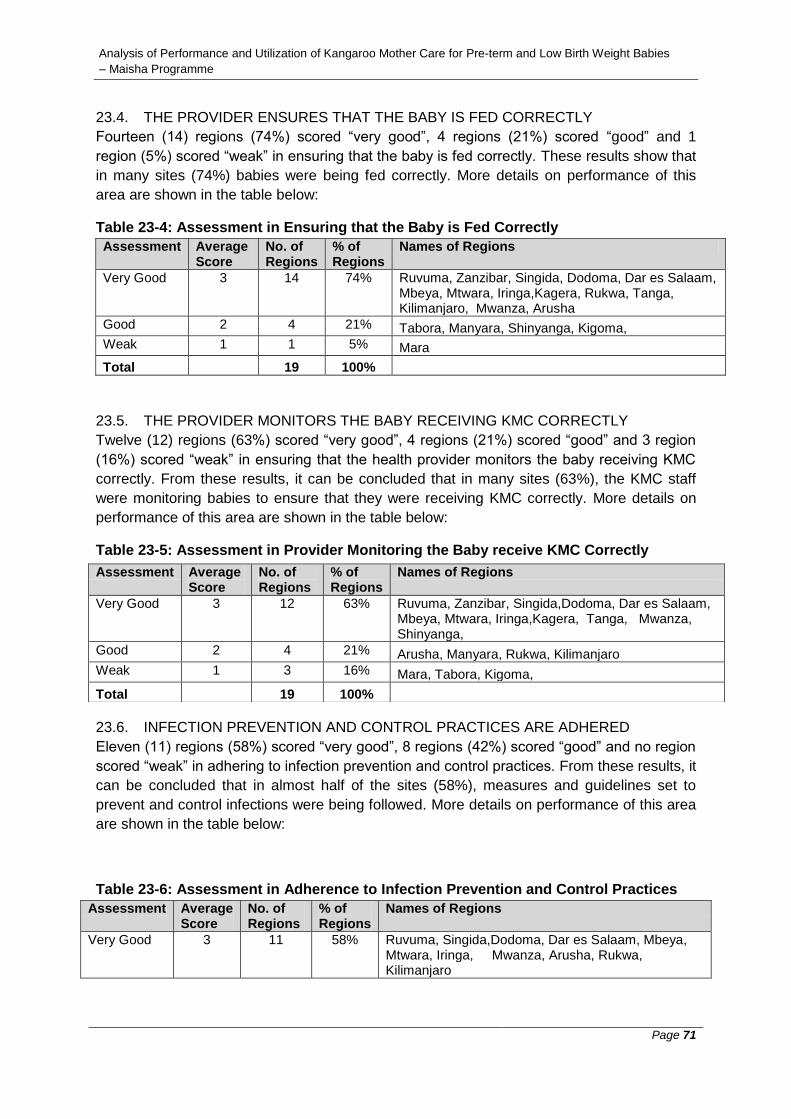
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 71
23.4. THE PROVIDER ENSURES THAT THE BABY IS FED CORRECTLY
Fourteen (14) regions (74%) scored “very good”, 4 regions (21%) scored “good” and 1
region (5%) scored “weak” in ensuring that the baby is fed correctly. These results show that
in many sites (74%) babies were being fed correctly. More details on performance of this
area are shown in the table below:
Table 23-4: Assessment in Ensuring that the Baby is Fed Correctly
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 14 74% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa,Kagera, Rukwa, Tanga, Kilimanjaro, Mwanza, Arusha
Good 2 4 21% Tabora, Manyara, Shinyanga, Kigoma,
Weak 1 1 5% Mara
Total 19 100%
23.5. THE PROVIDER MONITORS THE BABY RECEIVING KMC CORRECTLY
Twelve (12) regions (63%) scored “very good”, 4 regions (21%) scored “good” and 3 region
(16%) scored “weak” in ensuring that the health provider monitors the baby receiving KMC
correctly. From these results, it can be concluded that in many sites (63%), the KMC staff
were monitoring babies to ensure that they were receiving KMC correctly. More details on
performance of this area are shown in the table below:
Table 23-5: Assessment in Provider Monitoring the Baby receive KMC Correctly
23.6. INFECTION PREVENTION AND CONTROL PRACTICES ARE ADHERED
Eleven (11) regions (58%) scored “very good”, 8 regions (42%) scored “good” and no region
scored “weak” in adhering to infection prevention and control practices. From these results, it
can be concluded that in almost half of the sites (58%), measures and guidelines set to
prevent and control infections were being followed. More details on performance of this area
are shown in the table below:
Table 23-6: Assessment in Adherence to Infection Prevention and Control Practices
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 11 58% Ruvuma, Singida,Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Mwanza, Arusha, Rukwa, Kilimanjaro
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 12 63% Ruvuma, Zanzibar, Singida,Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa,Kagera, Tanga, Mwanza, Shinyanga,
Good 2 4 21% Arusha, Manyara, Rukwa, Kilimanjaro
Weak 1 3 16% Mara, Tabora, Kigoma,
Total 19 100%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 72
Good 2 8 42% Manyara, Mara, Tabora, Kigoma, Zanzibar,Kagera,Shinyanga,Tanga
Weak 1 0 0%
Total 19 100%
23.7. THE MOTHER & HER FAMILY ARE SUPPORTED
Twelve (12) regions (63%) scored “very good”, 6 regions (32%) scored “good” and 1 region
(5%) scored “weak” in the performance area of mother and her family being supported by
health providers in carrying out KMC. From these results, it can be concluded that in many
sites (63%), the mothers and their families were being supported by the KMC staff to carry
out KMC services properly. More details on performance of this area are shown in the table
below:
Table 23-7: Assessment on the Mother and her Family being supported
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 12 63% Ruvuma, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Mwanza, Mara, Tabora, Kagera,Tanga
Good 2 6 32% Manyara, Arusha, Kigoma, Rukwa, Zanzibar, Kilimanjaro
Weak 1 1 5% Shinyanga
Total 19 100%
23.8. THE BABY IS DISCHARGED ACCORDING TO GUIDELINES
Fifteen (15) regions (79%) scored “very good”, 4 regions (21%) scored “good” and no region
scored “weak” in discharging a baby from the KMC facility according to guidelines. From
these results, it can be concluded that many sites (79%) were discharging babies from KMC
units as required. More details on performance of this area are shown in the table below:
Table 23-8: Assessment in discharging the Baby from the Facility
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 15 79% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Kagera, Rukwa, Tanga, Mwanza, Arusha, Shinyanga, Mara,
Good 2 4 21% Tabora, Kigoma, Kilimanjaro, Manyara,
Weak 1 0 0% Nil
Total 19 100%
23.9. THE BABY RECEIVES REGULAR FOLLOW UPS
Fifteen (15) regions (79%) scored “very good”, 3 regions (16%) scored “good” and 1 region
(5%) scored “weak” in discharging a baby from the KMC facility according to guidelines.
From these results, it can be concluded that many sites (79%) were making regular follow
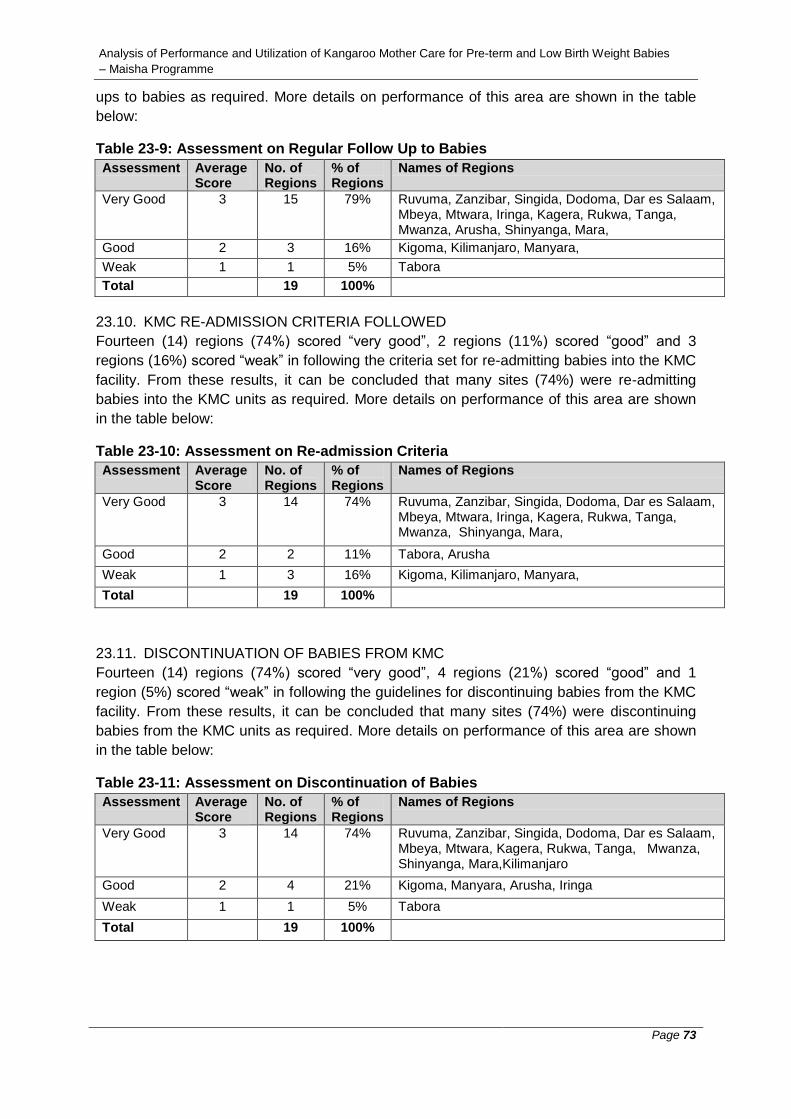
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 73
ups to babies as required. More details on performance of this area are shown in the table
below:
Table 23-9: Assessment on Regular Follow Up to Babies
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 15 79% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Kagera, Rukwa, Tanga, Mwanza, Arusha, Shinyanga, Mara,
Good 2 3 16% Kigoma, Kilimanjaro, Manyara,
Weak 1 1 5% Tabora
Total 19 100%
23.10. KMC RE-ADMISSION CRITERIA FOLLOWED
Fourteen (14) regions (74%) scored “very good”, 2 regions (11%) scored “good” and 3
regions (16%) scored “weak” in following the criteria set for re-admitting babies into the KMC
facility. From these results, it can be concluded that many sites (74%) were re-admitting
babies into the KMC units as required. More details on performance of this area are shown
in the table below:
Table 23-10: Assessment on Re-admission Criteria
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 14 74% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Iringa, Kagera, Rukwa, Tanga, Mwanza, Shinyanga, Mara,
Good 2 2 11% Tabora, Arusha
Weak 1 3 16% Kigoma, Kilimanjaro, Manyara,
Total 19 100%
23.11. DISCONTINUATION OF BABIES FROM KMC
Fourteen (14) regions (74%) scored “very good”, 4 regions (21%) scored “good” and 1
region (5%) scored “weak” in following the guidelines for discontinuing babies from the KMC
facility. From these results, it can be concluded that many sites (74%) were discontinuing
babies from the KMC units as required. More details on performance of this area are shown
in the table below:
Table 23-11: Assessment on Discontinuation of Babies
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 14 74% Ruvuma, Zanzibar, Singida, Dodoma, Dar es Salaam, Mbeya, Mtwara, Kagera, Rukwa, Tanga, Mwanza, Shinyanga, Mara,Kilimanjaro
Good 2 4 21% Kigoma, Manyara, Arusha, Iringa
Weak 1 1 5% Tabora
Total 19 100%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 74
23.12. KMC SERVICES ARE KNOWN TO THE COMMUNITY
Only 3 regions (16%) scored “very good”, 6 regions (32%) scored “good” and 10 regions
(53%) scored “weak” in creating awareness on KMC services to the neighbouring local
communities and the public at large. From these results, it can be deduced that the KMC
concept is not well known to the local communities. Almost half of the sites (53%) scored
less than 33% as shown in the table below:
Table 23-11: Assessment on Awareness of KMC Services
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 3 16% Ruvuma, Singida, Tanga
Good 2 6 32% Dar es Salaam, Mbeya, Mtwara, Rukwa, Mwanza, Shinyanga
Weak 1 10 53% Tabora, Arusha, Zanzibar, Dodoma, Kagera, Iringa, Mara, Kilimanjaro, Manyara, Kigoma
Total 19 100%
23.13. MONITORING AND EVALUATION OF KMC SERVICES
Only 7 regions (37%) scored “very good”, 10 regions (53%) scored “good” and 2 regions
(11%) scored “weak” in the area of Monitoring and Evaluation (M&E) of KMC services. From
these results, it can be deduced that many KMC sites do not know the importance of M&E.
There is also a possibility that they do not have skills and knowledge to conduct M&E. More
details of performance in this area are shown in the table below:
Table 23-11: Assessment on Monitoring and Evaluation
Assessment Average Score
No. of Regions
% of Regions
Names of Regions
Very Good 3 7 37% Ruvuma, Singida, Tanga, Mara, Shinyanga, Mtwara, Dodoma
Good 2 10 53% Dar es Salaam, Mbeya, Rukwa, Mwanza, Arusha, Zanzibar, Kagera, Iringa, Kilimanjaro, Manyara
Weak 1 2 11% Kigoma, Tabora
Total 19 100%
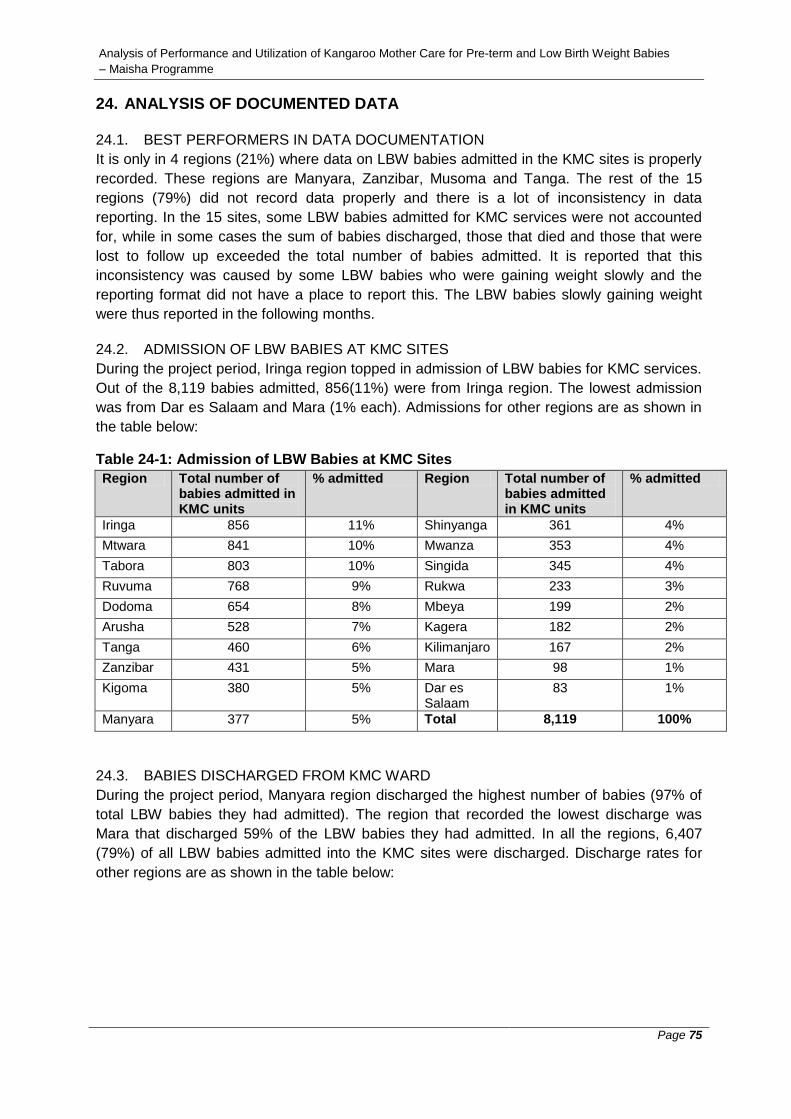
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 75
24. ANALYSIS OF DOCUMENTED DATA
24.1. BEST PERFORMERS IN DATA DOCUMENTATION
It is only in 4 regions (21%) where data on LBW babies admitted in the KMC sites is properly
recorded. These regions are Manyara, Zanzibar, Musoma and Tanga. The rest of the 15
regions (79%) did not record data properly and there is a lot of inconsistency in data
reporting. In the 15 sites, some LBW babies admitted for KMC services were not accounted
for, while in some cases the sum of babies discharged, those that died and those that were
lost to follow up exceeded the total number of babies admitted. It is reported that this
inconsistency was caused by some LBW babies who were gaining weight slowly and the
reporting format did not have a place to report this. The LBW babies slowly gaining weight
were thus reported in the following months.
24.2. ADMISSION OF LBW BABIES AT KMC SITES
During the project period, Iringa region topped in admission of LBW babies for KMC services.
Out of the 8,119 babies admitted, 856(11%) were from Iringa region. The lowest admission
was from Dar es Salaam and Mara (1% each). Admissions for other regions are as shown in
the table below:
Table 24-1: Admission of LBW Babies at KMC Sites
Region Total number of babies admitted in KMC units
% admitted Region Total number of babies admitted in KMC units
% admitted
Iringa 856 11% Shinyanga 361 4%
Mtwara 841 10% Mwanza 353 4%
Tabora 803 10% Singida 345 4%
Ruvuma 768 9% Rukwa 233 3%
Dodoma 654 8% Mbeya 199 2%
Arusha 528 7% Kagera 182 2%
Tanga 460 6% Kilimanjaro 167 2%
Zanzibar 431 5% Mara 98 1%
Kigoma 380 5% Dar es Salaam
83 1%
Manyara 377 5% Total 8,119 100%
24.3. BABIES DISCHARGED FROM KMC WARD
During the project period, Manyara region discharged the highest number of babies (97% of
total LBW babies they had admitted). The region that recorded the lowest discharge was
Mara that discharged 59% of the LBW babies they had admitted. In all the regions, 6,407
(79%) of all LBW babies admitted into the KMC sites were discharged. Discharge rates for
other regions are as shown in the table below:

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 76
Table 24-2: Discharge of Babies from KMC Sites
Region LBW babies admitted to KMC units
Total Discharged from KMC
% discharged
Region LBW babies admitted to KMC units
Total Discharged from KMC
% discharged
Singida 345 348 N/A Arusha 528 407 77%
Manyara 377 366 97% Dar es Salaam
83 63 76%
Dodoma 654 617 94% Mbeya 199 143 72%
Tanga 460 430 93% Mwanza 353 251 71%
Kagera 182 153 84% Rukwa 233 163 70%
Shinyanga 361 300 83% Tabora 803 557 69%
Zanzibar 431 346 80% Ruvuma 768 530 69%
Kigoma 380 303 80% Iringa 856 581 68%
Mtwara 841 662 79% Mara 98 58 59%
Kilimanjaro 167 129 77% Total 8,119 6,407 79%
24.4. DEATH OF BABIES AT KMC SITES
During KMC implementation period, Mara and Zanzibar regions had the highest number of
babies succumbing to death. The two regions recorded 18% and 17% respectively, of the
total number of Pre-term and LBW babies they had admitted in their sites. Regions that
recorded low number of deaths are Tanga (negligible %), Shinyanga (1%), Mbeya (1%),
Arusha (1%), Manyara (1%) and Singida(1%). A total of 8,119 LBW babies were admitted in
all sites and out of this, 446 (5%) died. It is reported that the deaths were related to asphyxia
due to suffocation as a result of poor feeding, pneumonia hypothermia, infections, congenital
malaria, hypoglycemia and bleeding from mouth and nose. Death rates for the other regions
are as shown in the table below:
Table 24-3: Death of Babies at KMC Sites
Region Total number of babies admitted in KMC units
Babies who died in KMC units
% of babies who died in KMC units
Mara 98 18 18%
Zanzibar 431 72 17%
Rukwa 233 33 14%
Mwanza 353 43 12%
Kagera 182 17 9%
Ruvuma 768 61 8%
Kigoma 380 24 6%
Tabora 803 47 6%
Dodoma 654 33 5%
Mtwara 841 39 5%
Kilimanjaro 167 7 4%
Iringa 856 28 3%
Dar es Salaam 83 2 2%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 77
Singida 345 5 1%
Manyara 377 5 1%
Arusha 528 6 1%
Mbeya 199 2 1%
Shinyanga 361 3 1%
Tanga 460 1 0%
Total 8,119 446 5%
24.5. MOTHERS ABSCONDED WITH THEIR PRE-TERM AND LBW BABIES FROM KMC
WARD
During the project period Singida, Manyara and Mbeya KMC sites did not have any cases of
absconded babies. Mara, Kagera and Dar es Salaam sites had the highest number of
absconded babies equal to 7% of all the babies they had admitted. In all the regions, 173
(2%) of all LBW babies admitted into the KMC sites were absconded. Rates for absconded
babies for other regions are as shown in the table below:
Table 24-4: Abscondees at KMC Sites
Regions Babies admitted to KMC
Abscondees
% absconded Regions Babies admitted to KMC
Aabscondees
% absconded
Singida 345 0 0% Tanga 460 9 2%
Manyara 377 0 0% Mwanza 353 9 3%
Mbeya 199 0 0% Ruvuma 768 22 3%
Shinyanga 361 1 0% Tabora 803 30 4%
Iringa 856 4 0% Kigoma 380 15 4%
Kilimanjaro 167 1 1% Mtwara 841 34 4%
Dodoma 654 6 1% Mara 98 7 7%
Arusha 528 5 1% Kagera 182 13 7%
Zanzibar 431 7 2% Dar es Salaam
83 6 7%
Rukwa 233 4 2% Total 8,119 173 2%
24.6. BABIES LOST TO FOLLOW UP
During the project period Singida, Manyara Kagera, Dodoma and Zanzibar KMC sites had the
lowest number of babies lost to follow (1% and below) of the LBW babies they had admitted
into their facilities. Tabora had the highest number of babies lost to follow, recording 54(30%)
of all the babies they had admitted into the KMC unit. In all the regions, 440(5%) of all LBW
babies admitted into the KMC sites were lost to follow. Rates for babies lost to follow for other
regions are as shown in the table below:
Table 24-5: Babies Lost to Follow up
Regions Babies admitted to KMC
Babies lost to follow
% lost to follow up
Regions Babies admitted to KMC
Babies lost to follow up
% lost to follow
Singida 345 1 0% Kigoma 460 25 5%
Mara 528 2 0% Tanga 353 30 8%
Kagera 167 1 1% Rukwa 654 59 9%
Dodoma 431 4 1% Mtwara 233 22 9%
Zanzibar 199 2 1% Kilimanjaro 768 75 10%
Ruvuma 841 14 2% Mbeya 380 48 13%
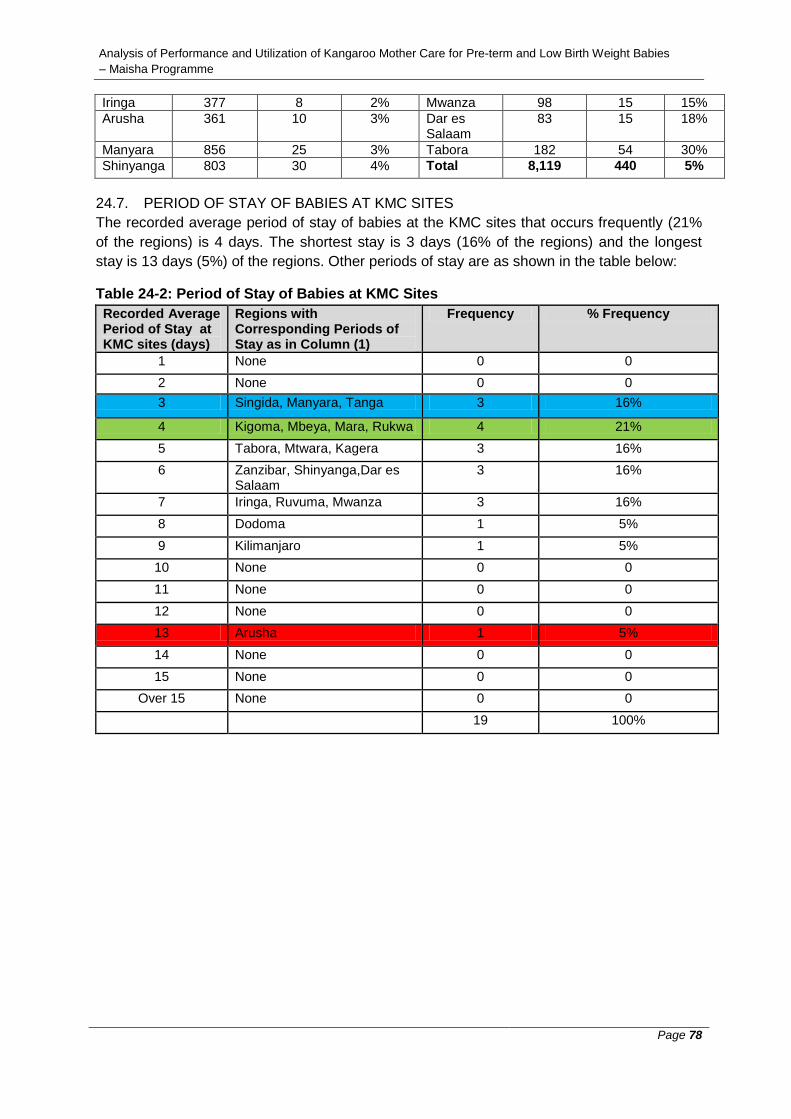
Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 78
Iringa 377 8 2% Mwanza 98 15 15%
Arusha 361 10 3% Dar es Salaam
83 15 18%
Manyara 856 25 3% Tabora 182 54 30%
Shinyanga 803 30 4% Total 8,119 440 5%
24.7. PERIOD OF STAY OF BABIES AT KMC SITES
The recorded average period of stay of babies at the KMC sites that occurs frequently (21%
of the regions) is 4 days. The shortest stay is 3 days (16% of the regions) and the longest
stay is 13 days (5%) of the regions. Other periods of stay are as shown in the table below:
Table 24-2: Period of Stay of Babies at KMC Sites
Recorded Average Period of Stay at KMC sites (days)
Regions with Corresponding Periods of Stay as in Column (1)
Frequency % Frequency
1 None 0 0
2 None 0 0
3 Singida, Manyara, Tanga 3 16%
4 Kigoma, Mbeya, Mara, Rukwa 4 21%
5 Tabora, Mtwara, Kagera 3 16%
6 Zanzibar, Shinyanga,Dar es Salaam
3 16%
7 Iringa, Ruvuma, Mwanza 3 16%
8 Dodoma 1 5%
9 Kilimanjaro 1 5%
10 None 0 0
11 None 0 0
12 None 0 0
13 Arusha 1 5%
14 None 0 0
15 None 0 0
Over 15 None 0 0
19 100%

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 79
25. CONCLUSION AND RECOMMENDATIONS
25.1. CONCLUSION
The initiative by MAISHA Programme to implement the KMC project in collaboration with SC
is quite commendable and has received great support from all stakeholders; the MOHSW,
respective health facilities and the beneficiaries. The project has seen many lives of babies
saved under facility based KMC and many service providers have been trained on the
provision of KMC services to make the KMC concept sustainable. The supervision exercises
have largely been described as participatory, supportive and educative by the service
providers.
Generally the performance of the 19 sites is good, although there are similar and recurrent
challenges in many of the sites. If these challenges are addressed in time, better services will
be realized. According to the assessment criteria in the monitoring tool, 16 regions (84%)
performed “very good”, 3 (16%) performed “good” while none performed “weak”.
The demand for KMC services in the 19 sites is quite high. Many of the neonates admitted to
the health facilities were pre-term with LBW. For instance, in Manyara region, 97% of all
newborns were pre-term and LBW. Many other regions had LBW babies accounting for more
than 50% of all newborn babies admitted in the respective health facilities.
25.2. RECOMMENDATIONS
From the analysis of the supportive supervision reports and the consolidated data on pre-
term and LBW babies at all the 19 sites, the following recommendations were made:
The grading system for awarding of marks in the assessment criteria for
performance areas prepared by the MOHSW (monitoring checklist) for use during
supervision exercises should be reviewed. Some supervision reports indicate that
the marks scored by some sites do not reflect the actual situation on the ground.
The sites scored high marks than they deserved. These reports are those for
Iringa (3rd visit), Kigoma (2nd visit), Kagera (1st visit) and Musoma (1st visit). The
current grading system has 3 categories with intervals of 33 marks, which
apparently lumps many sites in one category. The number of categories could be
increased to lower the interval of marks in order to segregate the sites accordingly
as per actual performance.
More efforts are needed to increase awareness on KMC services. In many sites, it
is evident that the neighbouring local communities are not aware of these
services. Only 3 regions (16%) scored “very good” in creating awareness on KMC
services.
More efforts are also needed in educating and training of staff working in KMC
units on M&E. From the analysis of performance reports, only 7 regions (37%)
scored “very good” in the area of M&E of KMC services.
There is need to sensitize the KMC staff and the HMT to keep proper records of
KMC services and also improve the reporting format. The data provided in many

Analysis of Performance and Utilization of Kangaroo Mother Care for Pre-term and Low Birth Weight Babies
– Maisha Programme
Page 80
sites is inconsistent. Some LBW babies admitted for KMC services were not
accounted for, while in some sites the sum of babies discharged, those that died
and those that were lost to follow up exceeded the total number of babies
admitted.
Other areas that need joint efforts between the MOHSW and the HMTs are
provision of adequate space for KMC services (in sites where space is a problem)
and provision of food to admitted mothers to address the problem of mothers
seeking early discharge.

Sample Checklist 1
ANNEX 1: SAMPLE CHECKLIST
Background information
1. Read this checklist carefully before filling 2. Write the answer by putting a tick in the corresponding box or on the space
provided 3. Provide an appropriate feedback if required
Name of Health Facility: ......................................................................................... Number of health providers trained on KMC in the health facility: ..................................
o Working in KMC Unit/ward: .......................................................................
o How many were followed up after training: ................................................
District: ................................................................................................................................ Region: ................................................................................................................................ Type of Health Facility
Hospital
Health Centre Ownership
o Government o Faith based o Private o Others (explain): ________________________________________
Location: Urban: Rural:
Names of Supervisors:
1. ............................................................................................................................. 2. ............................................................................................................................. 3. .............................................................................................................................. 4. ............................................................................................................................... 5........................................................................................................................ 6............................................................................................................................. 7..............................................................................................................................
Supervision date: ........................................................................................................
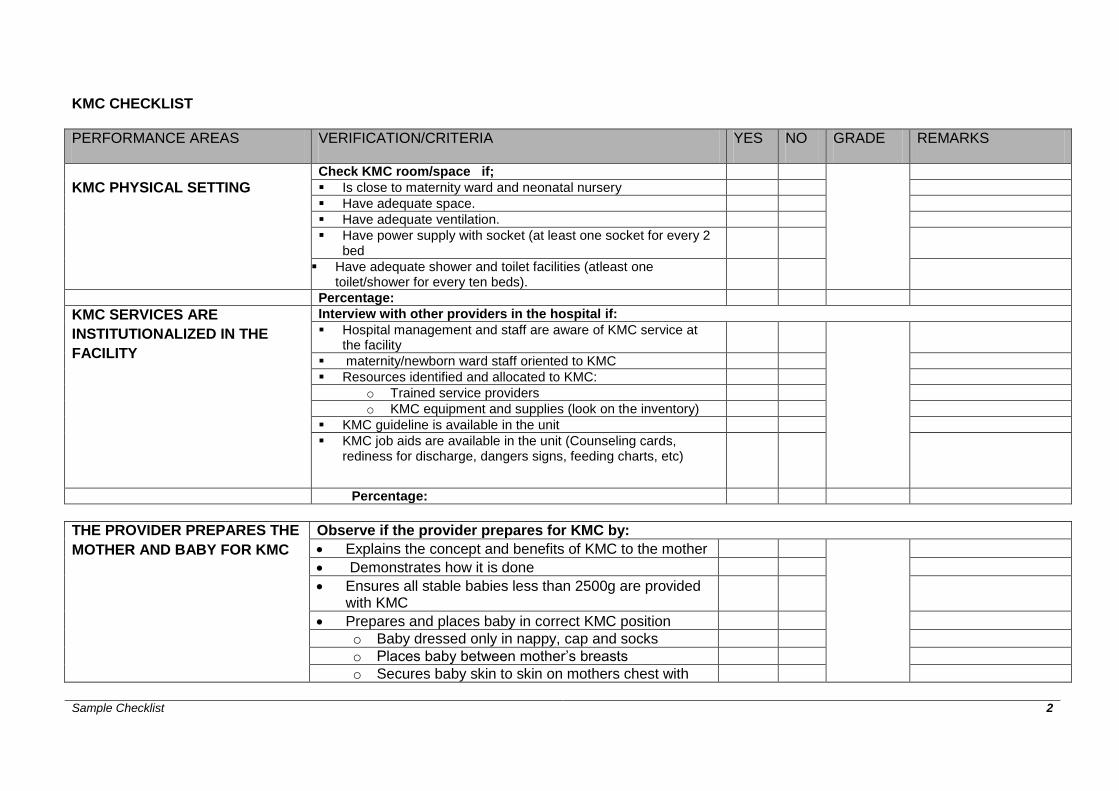
Sample Checklist 2
KMC CHECKLIST
PERFORMANCE AREAS VERIFICATION/CRITERIA YES NO GRADE REMARKS
KMC PHYSICAL SETTING
Check KMC room/space if;
Is close to maternity ward and neonatal nursery
Have adequate space.
Have adequate ventilation.
Have power supply with socket (at least one socket for every 2 bed
Have adequate shower and toilet facilities (atleast one toilet/shower for every ten beds).
Percentage:
KMC SERVICES ARE
INSTITUTIONALIZED IN THE
FACILITY
Interview with other providers in the hospital if:
Hospital management and staff are aware of KMC service at the facility
maternity/newborn ward staff oriented to KMC
Resources identified and allocated to KMC:
o Trained service providers
o KMC equipment and supplies (look on the inventory)
KMC guideline is available in the unit
KMC job aids are available in the unit (Counseling cards, rediness for discharge, dangers signs, feeding charts, etc)
Percentage:
THE PROVIDER PREPARES THE
MOTHER AND BABY FOR KMC
Observe if the provider prepares for KMC by:
Explains the concept and benefits of KMC to the mother
Demonstrates how it is done
Ensures all stable babies less than 2500g are provided with KMC
Prepares and places baby in correct KMC position
o Baby dressed only in nappy, cap and socks
o Places baby between mother’s breasts
o Secures baby skin to skin on mothers chest with

Sample Checklist 3
appropriate wrapper/local cloth
Instruct mother / care giver the following:
o Wear open front top
o Keep baby in upright position
o Ensure continuous skin to skin contact (may be intermittent when appropriate to circumstances)
o Sleep in slanted half sitting position to maintain baby upright
Percentage:
THE PROVIDER ENSURES THAT
THE BABY IS FED CORRECTLY
Observe if the provider
Ensures babies are fed as per schedule(look on the feeding charts)
Ensure proper attachment during breastfeeding.
Babies are breastfed or fed EBM by cup/NGT or Fed alternatively by cup or NGT
Encourages exclusive breastfeeding for 6 months
Calculates feeds using guidelines for volume of feeds required per day based on age and weight of baby
Percentage:
THE PROVIDER MONITORS THE
BABY RECEIVING KMC
CORRECTLY
Observe if the provider:
Ensures baby is in continuous skin to skin position
Registers baby and records details in KMC register
Monitors and records vital signs every 12 hours, and more frequently when required (temperature, respiration).
Records feeds given as per schedule
Takes baby’s daily weight to monitor growth
Percentage:
INFECTION PREVENTION AND
CONTROL
Observe if the mother/Care taker:
Washes her hands with clean running water and soap
o Before and after feeding baby

Sample Checklist 4
o Before and after changing nappies
o After attending toilet
Cleans all cups and feeding utensils before and after use and stored in covered clean container.
Ensures baby’s umbilical cord is kept clean and dry
Takes bath appropriately and puts on clean cloths
Cleans/wipes baby daily with warm water and soft cloths (“head to toe”)
Ensures baby wears clean and dry nappies
Percentage:
THE MOTHER AND HER FAMILY
ARE SUPPORTED
Observe if the provider:
Integrates another family member into care, as appropriate
Discusses and helps mother with any problems related to KMC positioning
Discusses and helps mother with feeding and care of the baby
Encourages mother to continue KMC
Encourages mother/family member to express concerns and ask questions
Percentage: 80%
THE BABY IS DISCHARGED
FROM THE FACILITY
ACCORDING TO GUIDELINES
o Baby has gained weight and has a minimum weight of 1500g
o Continous weight gain of at least 15 gm per day for three consecutive days.
o KMC position is well tolerated by baby and mother
o Has no danger sign
o Mother is confident and competent breast feeding and/or feeding expressed breast milk
o Mother accepts KMC method and is willing to continue with KMC at home

Sample Checklist 5
Mother can get support from relatives at home and she is willing to come back for followup visits
Percentage:
PERFORMANCE AREAS VERIFICATION/CRITERIA YES NO GRADE REMARKS
THE BABY RECEIVES REGULAR
FOLLOW UPS
Observe if the provider:
Ensures follow up of babies after discharge is done o Every week for babies weighing between 1500g, and 1800g o Every 2 weeks for babies weighing >1800g o For any other medical indication
Ensures baby is immunized according to EPI guidelines
Weighs the baby
take history from mother/guardian If KMC is continuing at home, continuous or intermitent and duration of skin-to-skin contact
How baby is feeding or being fed
If baby has any danger signs and continues educating the mother on danger signs
If baby is showing any signs of intolerance to KMC (baby too active and uncomfortable in KMC position)
Performs a physical assessment of the baby
Discusses experiences/problems mother may have in continuing KMC and gives support
Praise the mother/care taker and encourages mother/family to continue KMC as needed
Schedules the next visit as relevant x
KMC RE-ADMISSION CRITERIA
Check KMC records for last 3-6 months: check 3 cases of re-admision
Readmits baby to health facility (according to national guidelines):if baby has:
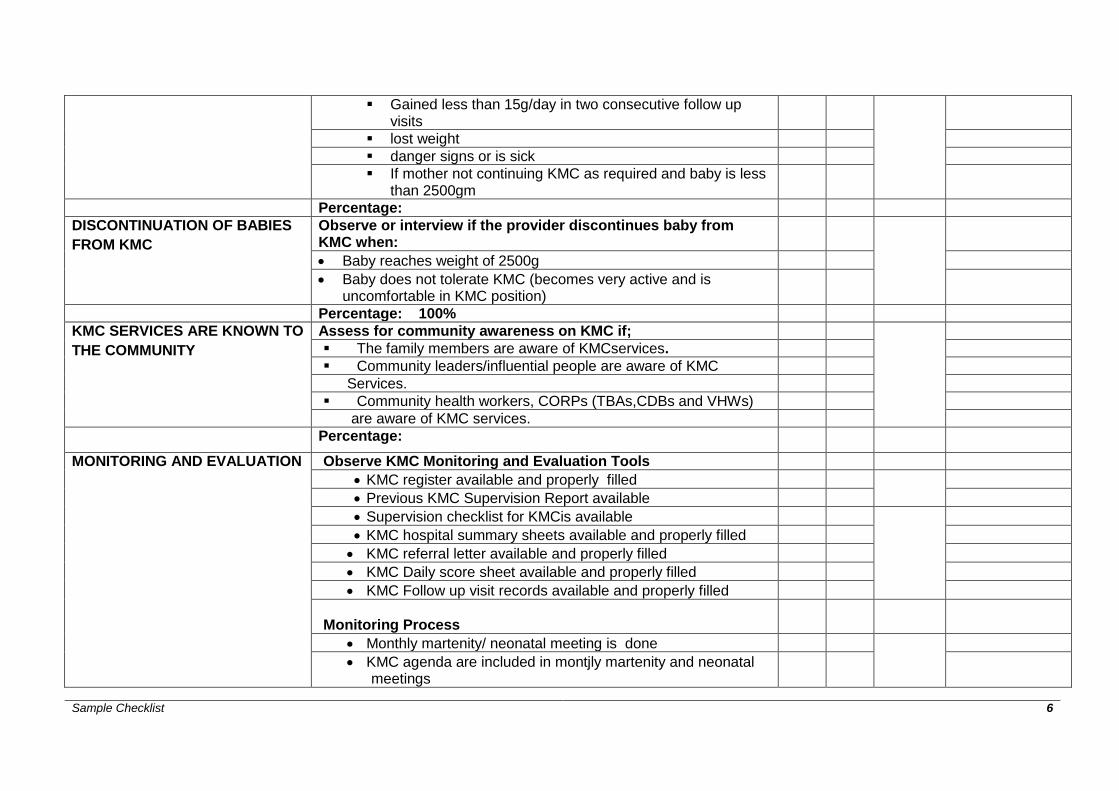
Sample Checklist 6
Gained less than 15g/day in two consecutive follow up visits
lost weight
danger signs or is sick
If mother not continuing KMC as required and baby is less than 2500gm
Percentage:
DISCONTINUATION OF BABIES
FROM KMC
Observe or interview if the provider discontinues baby from KMC when:
Baby reaches weight of 2500g
Baby does not tolerate KMC (becomes very active and is uncomfortable in KMC position)
Percentage: 100%
KMC SERVICES ARE KNOWN TO
THE COMMUNITY
Assess for community awareness on KMC if;
The family members are aware of KMCservices.
Community leaders/influential people are aware of KMC
Services.
Community health workers, CORPs (TBAs,CDBs and VHWs)
are aware of KMC services.
Percentage:
MONITORING AND EVALUATION
Observe KMC Monitoring and Evaluation Tools
KMC register available and properly filled
Previous KMC Supervision Report available
Supervision checklist for KMCis available
KMC hospital summary sheets available and properly filled
KMC referral letter available and properly filled
KMC Daily score sheet available and properly filled
KMC Follow up visit records available and properly filled
Monitoring Process
Monthly martenity/ neonatal meeting is done
KMC agenda are included in montjly martenity and neonatal meetings

Sample Checklist 7
KMC monthly Reports available
Percentage: 40%

Sample Checklist 8
SUMMARY OF KMC SUPORTIVE SUPERVISION FACILITY: …………………………………………………………………………..
PERFOMANCE AREA SCORE REMARKS(Very Good, Good, Poor)
KMC PHYSICAL SETTING
KMC SERVICES ARE INSTITUTIONALIZED IN THE FACILITY
THE PROVIDER PREPARES THE MOTHER AND BABY FOR KMC
THE PROVIDER ENSURES THAT THE BABY IS FED CORRECTLY
THE PROVIDER MONITORS THE BABY RECEIVING KMC CORRECTLY
INFECTION PREVENTION AND CONTROL PRACTICES ARE ADHERED
THE MOTHER OF THE BABY RECEIVING KMC AND HER FAMILY ARE SUPPORTED
THE BABY IS DISCHARGED FROM THE FACILITY ACCORDING TO GUIDELINES
THE BABY RECEIVES REGULAR FOLLOW UPS
KMC READMISSION CRITERIA
DISCONTINUATION OF BABIES FROM KMC
KMC SERVICES ARE KNOWN TO THE COMMUNITY
MONITORING AND EVALUATION OF KMC SERVICES
TOTAL SCORE X
PERCENTAGE: (X/39 x100) =