ancillary staff
TRANSCRIPT

Department of Nursing
Launchpad Orientation Manual
Ancillary Staff
2015
1

Launchpad Orientation Ancillary Staff
Table of Contents
Day 1
Ancillary Skills Day 1 Review ......................................................................... 5 Basic Care of Patients (Guideline) ................................................................. 8 Oral Hygiene:
Assisting Patient to Brush Teeth ...................................................... 12 Brushing Teeth ................................................................................ 13 Denture Care ................................................................................... 14
Personal Hygiene: Donning and Removing a Gown ...................................................... 16 Personal Hygiene – Bath or Shower ................................................ 17 Personal Hygiene – Bed Bath .......................................................... 18 CHG Bath Treatment with Mit ......................................................... 21 Shaving a Patient ............................................................................. 23
Infection Prevention: Standard and Transmission Based Precautions................................ 24
Transmission Based Precautions ......................................... 26 Disease/Conditions Requiring Precautions .......................... 35 Sequence for Donning Personal Protective Equipment (PPE) ................................................................. 52
Handwashing .................................................................................. 53 Removing Disposable Gloves .......................................................... 54
Day 2
Ancillary Skills Day 2 Review ....................................................................... 56 Admission, Transfer, and Discharging the Patient:
Admitting the Patient ...................................................................... 58 Rounding and Proactive Toileting .................................................... 59 Transferring the Patient .................................................................. 60 Discharging the Patient ................................................................... 61
2

Vital Signs and Patient Monitoring: Pulses .............................................................................................. 62 Taking Blood Pressure ..................................................................... 63 Taking the Respiratory Rate ............................................................. 64 Temperature Taking ........................................................................ 65 Pulse Oximeter ................................................................................ 66 EKG Lead II ...................................................................................... 67 EKG 12-Lead Recording ................................................................... 68 Recording Nasogastric Tube Drainage ............................................. 70
CAUTI Prevention: External Catheter Application .........................................................71
Skin Care for Incontinent Patients ............................................................... 72
Day 3
Ancillary Skills Day 3 Review ....................................................................... 74 Early and Progressive Mobility .................................................................... 78
Mobility Algorithm .......................................................................... 84 Criteria for PT Referral .................................................................... 85
Constant Observation Aide: Constant Observation Aide Algorithm ............................................. 86 Constant Observation Aide Report Sheet ........................................ 87 Constant Observation Aide Assignment and Documentation Sheet ............................................................................................... 90
Restraints .................................................................................................... 91 Pulmonary Hygiene (CPT, Cough) ................................................................ 94 Suction Canister Change ............................................................................. 96 Pain Observation—Unlicensed Assistive Personnel ..................................... 97
3

Ancillary Staff
Day 1 Skills
4

UCLA Health Launchpad Orientation
Under the direct supervision of the Registered Nurse, ancillary staff perform basic patient care skills, follows infection control practices, positions, transfers and transports patients, takes vital signs, collects specimens, accurately observes, reports and charts, performs range of motion and assists with feedings, self-care and elimination needs.
Day 1 Ancillary Staff Skills
IV/NGT 1. IV
a. Hand washing prior to touching IV site and tubing is critical to the prevention ofinfections.
b. Report to RN immediately: patient complaint of discomfort/pain, redness, swelling,drainage at insertion site, IV insertion site uncovered by dressing, and linedisconnection
2. Nasogastric Tubea. Accurate recording of nasogastric output amount (mark with black sharpie pen
time and date)b. Emptying of nasogastric drainage containerc. Report to RN immediately: coughing, SOB, changes in vital signs (including o2
sat), any change in external catheter length, and change in amount and color ofoutput.
d. The RN/LVN must assess placement of the NGT
3. Oral Care (regular and intubated patient)a. Report to RN any bleeding, loose teeth, sores or injury to the
mouth/gums/teeth.b. Independent patients/Dependent Non-ventilated patients:
i. Independent patients Brush teeth using soft-bristled toothbrush at leasttwice a day, preferably in the morning, before going to bed, and prn.
ii. Dependent Non- ventilated patients: Oral care should be performed Q8hand prn with suction toothbrush or foam swab. Patients withgastrostomy tubes or altered mental status should receive oral care aminimum of q4h.
5

c. For patients with bleeding tendencies, use foam swabs with hospitalrecommended oral care solution or toothpaste. Apply swab along tongue, teeth,cheek, and gums. (Rationale: Foam swabs are gentle to fragile tissues. Swabshelp to remove debris)
d. Ventilated Adult Patientsi. In the critical care setting, poor oral hygiene has been associated with
increased dental plaque accumulation, bacterial colonization of theoropharynx, and higher nosocomial infection rates, particularlyventilator-associated pneumonia (VAP)
ii. Oral hygiene should be performed Q2—4h and prniii. Brush teeth using suction toothbrush (foam swab is less effective) and
small amounts of hospital recommended oral care solution or sterilewater and alcohol-free antiseptic for approximately one to two minutes.Exert gentle pressure while moving in short horizontal or circularmotions. Gently brush the surface of the tongue.
iv. Follow with application of a water-based mouth moisturizer to tongue,teeth, cheeks, gums, and lips.
v. Oral hygiene needs of ventilated patients are under RN supervision perunit protocol and may be delegated to care partners and licensedvocational nurses (LVN).
4. Bathing (regular and CHG)a. Stress the importance of documentationb. Patient refusal—inform RN asapc. Daily Hygiene will be provided routinely with AM care, PM (H.S. Care) and as
neededd. CHG Bath
i. CHG bath treatments are initiated on all applicable patients within 24hours of admission.
ii. CHG bath treatment is performed at least once within a 24-hour periodon each patient unless contraindicated.
iii. The Registered Nurse is responsible for assessing the patient’s skin forany contraindications for a CHG bath treatment.
iv. The Registered Nurse is responsible for educating the patient on the useof CHG bath treatments as a standard unit treatment and providingpatient education information sheet as needed.
v. Assistive personnel such as Care Partners or Licensed Vocational Nursescan give CHG bath treatments with direction from the patient’s primaryRegistered Nurse.
a. 1:1 dilution (CHG : Water)b. Do not rinse off the CHGc. Do not use on the face, neck, or perineal area
6

vi. Contraindications for CHG Bath:a. Patients < 2 months of ageb. Patients with extensive and diffuse skin rashes, open extensive
weeping, or skin eruptions including varicella (more than onedermatome).
c. Patients with known allergies to CHG of hypersensitivity any otheringredients in the product.
d. Patient with burn greater than one dermatome or that includes ahigh percentage of disrupted body surface area.
e. Use in patients undergoing lumbar punctures or contact withmeninges (CHG is toxic to nerve tissues with direct contact)
5. Shaving (safety concern: bleeding, immunosuppression, and suicide risk)
During Medication Administration 1. ACCPs: Medication Ordering and Administration Process in CareConnect2. Isolation Precautions3. Handwashing and gloves4. Personal Protective Equipment5. Rounding 6Ps6. Proactive Toileting
7

BASIC CARE OF PATIENTS NUR-G1001
UCLA Department of Nursing General Care Nursing Guidelines
KKeeyy:: EEvviiddeennccee--bbaasseedd PPrraaccttiiccee RReeccoommmmeennddaattiioonnss RR ==RReesseeaarrcchh--bbaasseedd N = National Practice Guideline/ProtocolLL == LLiitteerraattuurree EE == EExxppeerrtt OOppiinniioonn//CCoonnsseennssuuss
UCLA Department of Nursing General Care Guidelines
Basic Care of Patients
PATIENT GOALS/OUTCOMES
1. Dignity, individuality, and cultural diversity will be respected in all aspects of patientcare.
2. All staff members will share responsibility to ensure that basic nursing care needswill be satisfied.
3. Patient’s care will be delivered in a compassionate, consistent, and timely mannerthroughout the hospitalization.
ASSESSMENT
1. Assess patient’s cultural, religious, spiritual needs or concerns during initialassessment.
2. Assess for skin, hygiene, and comfort needs during initial assessment and reassessas appropriate.
3. Assess for self care ability and opportunities for patient teaching.
INTERVENTIONS
1. Communicationa. Communicate with multidisciplinary team members (e.g. RN, LVNs, CPs, MDs,
Dietician, etc) at the beginning of the shift and as appropriate to ensurecontinuity of care
• Walking Rounds each shift• Verbal communication with team members
b. Establish a trusting relationship with patient• Introduce yourself (with a smile), and explain the role you will play in
their care.• Address patient by name• Make eye contact• Therapeutic Touch (e.g. touch patient's hand when speaking to
him/her) R1, R2
8
BASIC CARE OF PATIENTS NUR-G1001
UCLA Department of Nursing General Care Nursing Guidelines
c. Establish plan for the day (include family whenever possible) and involve patientin planning/directing and understanding their own care.
d. Conduct conversations appropriate to the patient when at the bedside caring forthe patient.
e. Ensure patient confidentiality
2. Ensure privacy, modesty, and dignity at all timesa. Be sensitive to modesty and ensure patient is well covered and unexposed.b. Pull curtains closed when working with patientc. Ensure privacy and warmth during bathingd. Respect and maintain dignity and individuality in your patient's caree. Close door when appropriatef. Knock prior to entering when door is closed or curtains are pulledg. Advocate for your patients in all aspects of their care.
3. Daily Hygiene will be provided routinely with AM care, PM (H.S. Care) and asneededa. AM Care will include the following each morning
• Oral hygiene (Brushing teeth and removing/brushing dentures, unlessoral care contraindicated) Q A.M. and document. R3, R4
• Hair Care (Brushing/combing) Q A.M. and PRN• Wash Hair (at least every week and PRN)• Total bath using Gentle Rain and warm water Q. A.M. - include peri-
care and catheter care• Completely removing Ted hose and sequential compression devices,
and wash feet• Incorporate ROM during Bath
Note: This is the most opportune time to conduct a full skin assessment as required for nursing documentation.
• Apply lotion to back, heels, elbows, friction/pressure points, dry areasQ A.M.
• Change Linen and Gown during a.m. care each morning
b. P.M. Care will include the following each evening - H.S. (Hour of SleepCare) will include:
• Oral Care (offer tooth brush or provide p.m. oral care)• Backrub/Lotion to bony/dry prominences R5, R6
• Change Gown at H.S.• Partial Linen Change (e.g. draw sheet change)• Provide Fresh Water at the bedside
4. General Care/Comfort Measuresa. Offer wash cloth before meals and after toiletingb. Ambulate as ordered/tolerated; all patients must ambulate with slippers. Be
sensitive to patient's modesty.
9

BASIC CARE OF PATIENTS NUR-G1001
UCLA Department of Nursing General Care Nursing Guidelines
c. Turn and position Q2 hour; float heels on all bed bound patients N1, use alift/turn sheet in order to prevent friction and/or shear.
d. Provide fresh drinking water as indicated at least BID (Q A.M. and Prior to H.S.)e. Meal trays must be accessible; provide assistance as neededf. Control and be conscious of the noise level R7
g. Use supportive aides (pillow,etc) to support the body
5. Bedside Environmenta. Call light, telephone, light cord, TV, urinal, tissue with disposal bag, glasses,
dentures, PCA Button within reachb. Inspect environment to ensure that all equipment/devices are clean, labeled and
in working order.c. Environment must be kept clean and neat - Notify Environmental services as
neededd. Remove unnecessary/surplus supplies, equipment, Linen, etc.
PATIENT/FAMILY EDUCATION
1. Collaborate with multidisciplinary team as appropriate to teach patient and familyabout aspects related to hygiene that relate to current condition.
RESOURCES: Unit based skin care resource nurses Unit based CNIV Unit Director Enterostomal Therapy (WOC) Service
REFERENCES:
KKeeyy:: RR == RReesseeaarrcchh--bbaasseedd NN == NNaattiioonnaall PPrraaccttiiccee GGuuiiddeelliinnee//PPrroottooccooll LL == LLiitteerraattuurree EE == EExxppeerrtt OOppiinniioonn//CCoonnsseennssuuss
R1 Heidt P. Effect of therapeutic touch on anxiety level of hospitalized patients Nursing Research 1981: 30: 32-37
R2 Olson M. Sneed N Anxiety and therapeutic touch. Issues Mental Health Nursing. 1995:16:97-108.
R3 Adams R. Qualified nurses lack adequate knowledge r/t oral health results in inadequate oral care of patients on medical wards. J Adv Nurs. 1996;24:552-560.
R4 Pearson LS. A comparison of the ability of foam swabs and tooth brushes to remove dental plaque: implications for nursing practice J Adv Nurs. 1996;23:62-69.
10

BASIC CARE OF PATIENTS NUR-G1001
UCLA Department of Nursing General Care Nursing Guidelines
R5 Fakouri C, Jones P. Relaxation Rx: Slow Stroke Back Rub. J Gerontol Nurs 1987:13(2)32-35.
R6 Richards KC. The effect of a back message and relaxation intervention on sleep. American Journal of Critical Care 1998: 13 (2) 42-48.
N1 Panel for the Prediction and Prevention of Pressure Ulcers in Adults. Pressure Ulcers in Adults: Prediction and Prevention. Clinical Practice Guideline, Number 3. AHCPR Publication No. 92-0047. Rickville, MD: Agency for Health Care Policy and Research, Public Health Service. U.S. Department of Health and Human Services. May 1992.
R7 Topf M. Effects of personal control over hospital noise on sleep. Research Nursing Health 1992;15;19-28.
REVIEWED: OCTOBER 2003, May 2007 Guidelines Committee
Contact Person(s): Linda Roof, RN, MPH
FORMS None
REVISION HISTORY Effective Date: October 2003 Review Date: May 2007 Revised Date: June 12, 2007
APPROVAL Heidi Crooks, RN, MA Sr. Assoc. Director of Operations and Patient Care Services UCLA Medical Center
11

Assisting Patient to Brush Teeth (UCLA)
Quicksheet
1. Assemble equipment needed:- Disposable gloves - Mouthwash (if permitted) - Emesis basin - Toothbrush - Toothpaste - Glass of cool water - Hand towel - Bed protector
2. Elevate the head of bed. Help patient into a comfortable position.3. Lower side rails and position over-bed table across patient's lap.4. Place emesis basin and glass of water on over-bed table.5. Place towel across patient's chest.6. Help patient brush teeth if needed.7. After patient has brushed his teeth:
- Push over-bed table to the foot of the bed. - Dispose of towel.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
12

Brushing Teeth (UCLA)
Quicksheet
1. Assemble equipment needed:- Disposable gloves - Mouthwash (if permitted) - Emesis basin - Toothbrush - Toothpaste - Glass of cool water - Hand towel - Bed protector
2. Elevate the head of bed. Help patient into a comfortable position3. Lower side rails and position over-bed table across patient's lap4. Place emesis basin and glass of water on over-bed table5. Place towel across patient's chest6. Help patient brush teeth if needed7. After patient has brushed his teeth:
- Push over-bed table to the foot of the bed
- Dispose of towel
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
13

Caring for Dentures (UCLA)
Quicksheet
1. Assemble equipment needed:- Disposable gloves - Tissues - Emesis basin - Toothbrush or denture brush - Toothpaste or powder - Denture cup
2. Allow the patient to clean dentures if able to do so. If the patient cannot:a. Put on gloves.b. Give tissue to patient.c. Ask patient to remove dentures.d. Assist, if necessary.
3. If patient cannot remove dentures:a. Ask patient to open mouth.b. Firmly grasp upper dentures. Gently ease down and forward and remove fromc. Firmly grasp lower dentures. Gently ease up and forward and remove from mouth.
4. Place dentures in denture cup or emesis basin with 2-3 inches of cool water. Take to bathroomor utility room. 5. Put toothpaste or tooth powder on toothbrush.
a. Place dentures in palm of hand and hold them under a gentle stream of warm water.b. Soak in a solution with a cleansing tablet before brushing, if necessary.c. Brush until all surfaces are clean.
6. Rinse dentures thoroughly under cold running water. Rinse denture cup.7. Place dentures in cup and take them to bedside.8. Assist patient to rinse mouth with mouthwash.9. Use a soft toothbrush or applicator to clean the mouth while dentures are out.10. Use tissue or gauze to hand the wet dentures to patient. Insert, if necessary.11. Remove and dispose of gloves according to facility policy.
12. Carry out each procedure completion action. Remember to wash your hands, reportcompletion of task, and document date, time, denture care, and patient reaction.
NOTE: Store dentures in a denture cup inside the bedside stand when not in use. Some patients prefer storing their dentures dry. Others prefer to store their dentures in a special solution.
14
NOTE: Dentures and Eyeglasses Dentures are artificial teeth that are removable. They must be cleaned. The patient may feel embarrassed about wearing dentures and even more so when seen after the dentures have been removed. Therefore, always provide privacy when dentures are to be removed and cleaned. When a patient wears dentures, it is your responsibility to:
- Use extreme care when handling dentures. - See that the dentures are kept clean. - See that the dentures are not lost or broken. - Store dentures safely when out of the patient's mouth. - Keep dentures in bedside stand. - Keep in container labeled with patient's name on the side. - Plastic dentures must be kept dry.
Eyeglasses and contact lenses need special care and attention. They should: - Be kept clean with special lens paper or soft, nonabrasive tissue. - Be stored in their container in the bedside stand when not in use. - Always be kept within easy reach of the patient.
Patients should be encouraged to wear dentures and glasses whenever possible.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
15

Donning and Removing a Gown (UCLA)
Quicksheet
1. Hold gown so that opening is in back. 2. Put one arm at a time through sleeves and pull up over shoulders. 3. Tie neck ties. 4. Wrap gown around waist, making sure back is completely covered. Tie waist strings. 5. To remove (takes gloves off first), untie waist strings. 6. Untie neck strings, bring them around shoulders so that gown is partially off shoulders. 7. Using dominant hand and grasping clean part of wristlet, pull sleeve wristlet over non-dominant hand. Use nondominant hand to pull sleeve wristlet over dominant hand. Must maintain clean surface to clean surface and dirty surface to dirty surface. 8. Grasp outside of gown through the sleeves at shoulders. Pull gown down over arms.
9. Hold gown shoulders in one hand and draw other hand out of gown, turn arm of gown inside out. Repeat with other hand
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
16

Personal Hygiene - Bath or Shower (UCLA)
Quicksheet
1. Assemble equipment needed.a) Liquid soapb) Washclothc) 2-3 bath towelsd) Bath blankete) Bath lotionf) Chair or stool beside shower or tubg) Bath or shower chair, as neededh) Patient's gown, robe, and slippersi) Bath mat
2. Help the patient put on robe and slippers.3. Escort patient to bathroom.4. Fill tub half full with water 95-105o F or adjust shower flow.5. Test the water with your wrist (should be warm).6. Place towel in the bottom of the tub to prevent patient from slipping (if nonskid strips are notpresent in tub). 7. Help the patient to undress. Give the male patient a towel to wrap around his waist.8. Position shower chair in tub or shower, if needed.9. Assist the patient into the tub or shower.10. Wash the patient's back.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
17

Personal Hygiene - Bed Bath (UCLA)
Quicksheet
1. Assemble equipment needed. a) Disposable gloves b) Washcloth c) 2-3 bath towels d) Bath blanket e) Bath lotion f) Bed linen g) Laundry bag or hamper h) Patient's gown i) Bath basin, the water should be 105o F j) Soap and soap dish or liquid soap k) Brush and comb l) Equipment for oral hygiene
2. Close the curtain to provide privacy. 3. Put towels on chair. 4. Place laundry hamper nearby. 5. Lower the back of the bed. 6. Lower side rails if permitted. 7. Loosen top bedclothes. 8. Remove and fold blanket and spread. 9. Place bath blanket over top sheet and remove sheet from under blanket. 10. Leave one pillow under patient's head. 11. Remove patient's night wear and place in laundry hamper. 12. If patient has an IV line.
a) Slip gown away from body toward arm with IV line in place. b) Gather gown at arm and slip downward over arm and line. c) Gather material of gown in one hand and slowly drawn gown over tip of fingers. d) With free hand, lift IV off of stand and slip gown over bottle. e) Remove gown. f) Replace IV bottle on stand.
13. Fill bath basin two-thirds full with water at 105o F. 14. Put on gloves if needed. 15. Form a mitten by folding washcloth around hand.
a) Wet washcloth. b) Wash eyes, using separate corners of cloth. c) Wipe from inside to outside corner. d) Do not use soap near eyes.
18

e) Do not use soap on face.
16. Rinse washcloth and apply soap if patient desires. Squeeze out excess water. 17. Wash and rinse patient's face, ears and neck well. Use towel to dry. 18. Expose patient's far arm. Protect bed with bath towel placed underneath arm.
a) Wash, rinse, and dry arm and hand. b) Repeat for other arm. c) Be sure axillae (armpits) are clean and dry. d) Apply deodorant and powder if patient requests them or needs them.
19. Care for hands and nails as necessary. Check with the nurse first to see if there are any special instructions. a) Place hands in basin of water. Wash each hand carefully. Rinse and dry. Push cuticle (base of fingernails) back gently with towel while wiping the fingers. 20. Put bath towel over patient's chest. Then fold blanket to waist.
a) Wash, rinse, and dry chest. b) Rinse and dry folds under breasts of female patient. c) Powder lightly.
21. Fold bath blanket down to pubic area. Wash, rinse, and dry abdomen. Fold bath blanket up to cover abdomen and chest. Slide towel out from under bath blanket. 22. Ask patient to flex knee, if possible. Fold bath blanket up to expose thigh, leg, and foot. Protect bed with bath towel.
a) Put bath basin on towel. b) Place patient's foot in basin. c) Wash and rinse leg and foot. d) When moving leg, support leg.
23. Lift leg and move basin to the other side of the bed. Dry leg and foot. Dry well between toes. 24. Repeat for other leg and foot. Take basin from bed before drying leg and foot. 25. Care for nails as necessary. 26. Apply lotion to feet of patient with dry skin. 27. If needed, change water and check for correct temperature. 28. Help patient to turn on side away from you. Help him to move toward the center of the bed. Place bath towel lengthwise next to patient's back.
- Wash, rinse and dry neck, back, and buttocks. - Use long, firm strokes when washing back.
29. A back rub is usually given at this time. 30. Help patient to turn on back. 31. Place a towel under the buttocks and upper legs. Place washcloth, soap, basin, and bath towel within convenient reach of the patient. Have patient complete bath by washing genitalia. Assist the patient, if necessary. If assisting a patient, always put on disposable gloves.
- For a female patient, wash from front to back, drying carefully. - For a male patient, be sure to carefully wash and dry penis, scrotum and groin area.
32. Carry out range of motion exercises as ordered.
19

33. Cover pillow with towel. Comb or brush hair.34. Discard towels and washcloth in laundry hamper.35. Provide clean gown. If the patient has an IV, check with the nurse before proceeding withsteps a through f. Find out if the gown is to (1) go over the arm with the IV or (2) remain off the arm and be draped over the shoulder (as with multiple IVs or an infusion pump). If situation #1 is the case, then:
a) Gather the sleeve on the IV side in one hand.b) Lift the bottle free of the stand.c) Slip the IV bottle through the sleeve from the inside and rehang.d) Guide the gown along the IV tubing to bed.e) Slip gown over hand.f) Position gown on infusion arm. Then insert opposite arm.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
20

CHG Treatment with 2% CHG and Bath Mitt - UCLA
Quicksheet CHG Treatment with 2% CHG and Bath Mitt 1. Screen patient for appropriateness for CHG bath. Hold if history of CHG hypersensitivity or other contraindication
2. Gather supplies: bath basin, hospital-approved bathing product that is compatible with CHG [(e.g. EasiCleanse bathing wipes or Gentle Rain). DO NOT USE: dispenser soap or soap provided by patient/family, towels, kit with 2% CHG and cloth mitt, clean gown, clean bed linen. 3. Wash out basin with soap and water before using.
4. Perform hand hygiene and apply clean gloves
5. Offer patient opportunity to void in bedpan or urinal if patient does not have an in-dwelling Foley catheter. 6. Remove patient’s gown and cover patient with blanket.
7. Bathe patient with soap and water. Use hospital-approved bathing product that is compatible with CHG [(e.g. EasiCleanse bathing wipes or Gentle Rain. Use Baza clean for incontinence care). 8. Dry patient 9. Moisten cloth mitt with 2% CHG solution and wipe on patient from neck down. Reapply as needed to cover the following areas: (a) Arms (b) Neck/chest (c) Abdomen (d) Legs (e) Back (f) Buttocks (Foley care OK) *AVOID EYES, EARS, MUCOUS MEMBRANES AND DRESSINGS.* 10. Pay special attention to axilla, groin, skin folds, nails, regions between digits. 11. Uncover area being cleansed. Keep rest of patient covered with blanket. 12. DO NOT RINSE CHG FROM SKIN 13. Apply hospital-approved skin moisturizer (Sween 24) to dry skin. 14. Replace gown and make patient’s bed if indicated. 15. Check function and position of external devices (indwelling tubes, catheters, lines; braces, TEDS, SCDs).
21

This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
16. Clean and replace bathing equipment Discard basins that remain visibly soiled 17. Perform hand hygiene 18. Document completion of CHG bath treatment in EHR: Daily cares/safety> Hygiene>CHG
22
Shaving a Patient (UCLA)
Quicksheet
1. Assemble equipment needed:- Disposable gloves - Electric shaver or safety razor - Shaving lather or an electric preshave lotion - Basin of water (115o F) - Face towel - Mirror - Aftershave lotion or powder
2. Put on disposable gloves.3. Place face towel across patient's chest.4. Moisten face and apply lather.5. Starting in front of the ear:
a. Hold skin taut.b. Bring razor down over cheek toward chin.c. Repeat until lather on cheek is removed and area has been shaved.d. Repeat on other cheek.e. Shave chin carefully.f. Ask patient to raise chin. Shave neck area on each side, bringing razor up toward chin.g. Use firm, short strokes.h. Rinse razor frequently.
6. Lather neck area and stroke up toward the chin in a similar manner.7. Wash face and neck. Dry thoroughly.8. Apply aftershave lotion or powder, if desired.9. If the skin is nicked:
a. Apply pressure directly over the area.b. Apply an antiseptic.c. Report incident to nurse.
10. Remove disposable gloves.NOTE:
- Use the patient's own shaving equipment if possible. Otherwise, use disposable, one-use safety razors. - If the patient is receiving anticoagulants, a special procedure may be required. For example, an electric razor provides the greatest safety. Check with your R.N. for the proper procedure. - If oxygen is being given, it may be possible to discontinue it during this procedure. Consult your R.N.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
23

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
1
STANDARD AND TRANSMISSION BASED PRECAUTIONS
PURPOSE
The purpose of this policy is to provide guidance on when and how to use Standard and Transmission Based Precautions.
SCOPE
This policy applies to UCLA Health System staff at Ronald Reagan, Santa Monica UCLA Medical Center and Orthopaedic Hospital, and Resnick Neuropsychiatric Hospital responsible for using Standard and Transmission Based Precautions.
POLICY
I. STANDARD PRECAUTIONS
Standard Precautions are designed to prevent transmission of blood borne pathogens (BBP) and other healthcare associated organisms. Use of Standard Precautions reduces the risk of transmission of microorganisms from both recognized and unrecognized sources. Standard Precautions include: hand hygiene, use of personal protective equipment (PPE), respiratory hygiene/cough etiquette and safe injection practices.
A. Hand Hygiene 1. Wash hands with alcohol-based hand rub or soap and water prior to
and following direct contact with the patient including their skin, mucous membranes, body fluids, the environment or equipment including contaminated patient-care items or surfaces. (See Policy HS IC 001 Hand Hygiene).
B. PPE PPE is defined by OSHA as “specialized clothing or equipment worn by an employee for protection against infectious materials.” Examples of PPE items include: gloves, masks, gowns, face shields and eyewear. (See the CDC’s sequence for donning and removing PPE, Appendix A.)
1. Wear PPE when there is risk of exposure to blood or other potentiallyinfectious material (OPIM). E.g. wear a fluid-resistant barrier gownwhen clothes are likely to be contaminated with blood or OPIM. Wearmask and eye protection during procedures that are likely to generatesplashes or sprays of blood or OPIM.
24

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
2
2. Remove and discard PPE prior to leaving the patient care area (e.g.inpatient room, treatment room). (See California OSHA standards:http://www.dir.ca.gov/title8/5193.HTML)
3. Practice hand hygiene immediately after removing PPE. Gloves arenot a substitute for hand hygiene.
4. PPE is single use. Do not use the same PPE (gloves included) ondifferent patients.
C. Safe Injection Practices Safe injection practices are part of Standard Precautions and are aimed at maintaining basic levels of patient safety and provider protection. The following are CDC recommended guidelines for safe injection practices. (See the CDC’s http://www.cdc.gov/hai/
The following recommendations apply to the use of needles, cannulas that replace needles, and, where applicable intravenous delivery systems.
1. Use aseptic technique to avoid contamination of sterile injectionequipment.
2. Do not administer medications from a syringe to multiple patients.Needles, cannulae and syringes are sterile, single-use items; theyshould not be reused for another patient or to access a medication orsolution that might be used for a subsequent patient.
3. Use fluid infusion and administration sets (i.e., intravenous bags,tubing and connectors) for one patient only and dispose appropriatelyafter use. Consider a syringe or needle/cannula contaminated once ithas been used to enter or connect to a patient's intravenous infusionbag or administration set.
4. Use single-dose vials for parenteral medications whenever possible.
5. Do not administer medications from single-dose vials or ampules tomultiple patients or combine leftover contents for later use.
6. If multidose vials must be used, both the needle or cannula andsyringe used to access the multidose vial must be sterile.
7. Do not keep multidose vials in the immediate patient treatment areaand store in accordance with the manufacturer's recommendations;discard if sterility is compromised or questionable.
8. Do not use bags or bottles of intravenous solution as a commonsource of supply for multiple patients.
25
STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
3
9. Provider protections, which are guided by Standard Precautionsprinciples, are covered in Policy IC 006 Exposure Control Plan forBloodborne Pathogens.
D. Special Precautions for Lumbar Procedures 1. In addition to skin antisepsis and wearing sterile surgical gloves, wear
a surgical mask when placing a catheter or injecting material into the spinal canal or subdural space (i.e., during myelograms, lumbar puncture and spinal or epidural anesthesia).
E. Respiratory Hygiene/Cough Etiquette 1. Respiratory hygiene/cough etiquette is a key component of Standard
Precautions. (See Policy HS IC 005 Airborne Disease Transmission Policy.)
F. Ambulatory Services 1. Consistent with the 2011 CDC Guide to Infection Prevention in
Outpatient Settings, safe delivery of care is based primarily upon elements of Standard Precautions and represents the minimum infection prevention expectations for safe care in ambulatory care settings.
II. TRANSMISSION BASED PRECAUTIONSTransmission Based Precautions are used in addition to Standard Precautionswhen there is known potential for spreading germs. Transmission BasedPrecautions include Airborne, Droplet, Contact and Contact/Spore (Tables 1-4,respectively). Each set of precautions are targeted specifically at how organismsare usually transmitted.
A. Initiating Transmission Based Precautions
1. A nurse may place a patient on precautions without a physician orderbased on assessment of signs, symptoms, infection status, ormicrobiology results. The nurse shall indicate the appropriate isolationstatus in the electronic medical record.
2. Use Transmission Based Precautions in addition to Standard Precautions.E.g. If a precautions sign indicates that you are to use a surgical maskonly, also use gloves if exposure to blood or OPIM is anticipated.
3. Practice hand hygiene and don PPE as indicated by the precautions sign.
4. Use a private room when available. When a private room is not available,a patient who requires Contact or Contact/Spore Precautions may beplaced in a room with another patient who has colonization or infectionwith the same microorganism but with no other infection (i.e., cohorting).
26

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
4
5. If a patient has diseases that require two or more types of precautions,post signage for each precaution type. E.g., if patient has carbapenem-resistant Enterobacteriaceae (CRE) and C. difficile, post both the redContact Precautions sign and the pink Contact/Spore Precautions sign.
6. Refer to Tables 5 and 6 for known or suspected diseases or conditionsand the types of precautions required.
B. Discontinuing Transmission Based Precautions
Discontinuing Transmission Based Precautions should be done withcareful consideration and with input from Clinical Epidemiology andInfection Prevention so that patients, staff, and visitors are not exposed tocommunicable diseases.
1. Evaluate the patient for appropriateness of discontinuingTransmission Based Precautions. Refer to Table 6. ContactClinical Epidemiology and Infection Prevention for assistance ifneeded.
2. Follow the organism—specific process for discontinuingtransmission-based precautions outlined in Table 6.
C. Ambulatory Services:
1. Transmission Based Precautions shall be utilized in ambulatorysettings in the manner described in Tables 1 – 4.
Table 1
AIRBORNE
PRECAUTIONS All Patients
Key Elements Use in addition to Standard Precautions.
Hand Hygiene Clean hands upon entering room and upon leaving room.
PPE
Wear a fit-tested respirator (N-95 mask or higher). Note that visitorsare not fit-tested, but rather are provided with masks of approximatesize.
Dispose of all PPE before leaving the patient care area. Dispose ofmask in Negative Pressure Isolation Room (NPIR) NPIR anteroomwith door to inpatient room closed.PPE is single use.
For Varicella (chickenpox), disseminated zoster, or measles (rubeola): If you are immune to varicella or measles, you do not need to wear
respiratory protection. If you are susceptible (i.e., non-immune), or unaware of your status.
you shall not be assigned to care for or visit the patient. However, if you must enter the room, wear a fit-tested respiratory (N-95 mask or higher). Note that visitors are not fit-tested, but rather are provided with masks of approximate size.
27

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
5
Room
Assignment
Use a NPIR. Please refer to the list of available NPIRs for patients requiring Airborne Precautions in Policy HS 8614.
Keep door closed at all times, including when the patient is out ofroom.
Minimize unnecessary entry into the room. If NPIR availability is limited, priority should be given to patients with
known or suspected tuberculosis or measles.
Precautions
Signs Post the Airborne Precautions sign outside the room where clearly
visible.
Visitors
Staff shall instruct visitors on hand hygiene and Airborne Precautions. Visitors shall follow Airborne Precautions as outlined above. Visitors
shall be provided with an N95 respirator of approximate size.
Staff shall provide patient and visitor with the education sheet, Patientand Visitor Instructions for Patients on Isolation Precautions, Form#11246.
Staff shall refer to the patient education sheet, Isolation Precautions:Nurse Education Instruction, Form #11249.
Patient
Transport
Limit the transport of the patient outside of their room. If transport is necessary, place a surgical mask on the patient. Notify the receiving department that Airborne Precautions are
required. Practice hand hygiene before and after transporting the patient.
Room
Cleaning
Use standard practices. Keep the room door(s) closed for at least one hour after the patient
has left the room and wear an N95 mask when entering the room.
Ambulation Patient should only leave room for necessary treatment, e.g. radiology or surgery. Patient shall wear a surgical mask for the entire duration they are outside the room
Discharge
Upon discharge, close room for 1 hour before admitting next patient. This allows ample time for air exchange. Healthcare workers may enter the room during this time, however they must don an N95 mask and the door must stay closed.
28

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
6
Table 2
DROPLET
PRECAUTIONS
All Patients
Key Elements Use in addition to Standard Precautions.
Hand Hygiene Clean hands upon entering room and upon leaving room.
PPE
Wear disposable surgical mask on entry to the patient room. Dispose of all PPE before leaving the room. PPE is single use.
Room
Assignment
Use a private room. Cohort patients with the same germ in thesame room if private room not available.
If patient must be placed in an open bed unit: Visibly separate the patient bed by curtain and place the
Droplet Precautions sign where clearly visible. Maintain at least 3 feet between the patient on Droplet
Precautions and other patients and visitors.Precautions
Signs
Post the Droplet Precautions sign outside the room where clearly visible.
Visitors
Staff shall instruct visitors on hand hygiene and DropletPrecautions.
Visitors shall follow Droplet Precautions as outlined above. Staff shall provide patient and visitor with the education sheet,
Patient and Visitor Instructions for Patients on IsolationPrecautions, Form #11246.
Staff shall refer to education sheet, Isolation Precautions:Nurse Education Instruction, Form #11249.
Patient
Transport
Limit the transport of the patient outside of their room. If transport is necessary, place surgical mask on patient. Notify the receiving department that Droplet Precautions are
required. Practice hand hygiene before and after transporting the patient.
Room Cleaning Use standard practices.
Ambulation
Patients on Droplet Precautions are encouraged to stay in theirroom.
Patient shall wear a surgical mask for the entire duration theyare outside the room.
29

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
7
Table 3
CONTACT
PRECAUTIONS
Inpatient Outpatient
Interventional Areas
Key Elements Use in addition to Standard Precautions.
Hand Hygiene Clean hands upon entering room and upon leaving room.
Clean hands before and after each patient encounter.
PPE
Wear gown and gloves onentry to patient room.
Dispose of all PPE beforeleaving the room.
PPE is single use.
Wear gloves and gowns whenexposure to blood and bodyfluids, mucous membranes, non-intact skin or potentially infectiousmaterial is anticipated (i.e.,Standard Precautions).
Dispose of all PPE before leavingthe patient care area.
PPE is single use.
Room
Assignment
Use private room. Cohort patients with the same germ in the same room if private room not available. If patient must be placed in an open bed unit, visibly separate the patient bed by curtain.
Visibly separate the patient bed by curtain or door.
Precautions
Signs
Post the Contact Precautions sign outside the room where clearly visible.
Use the red Contact Precautions sign to communicate isolation status in areas with increased risk of exposure to infectious materials, i.e., interventional areas such as surgery center.
Visitors
Visitors are not required toadhere to ContactPrecautions. However,visitors are required topractice StandardPrecautions including handhygiene and PPE as neededto reduce the risk ofexposure.
Visitors are not required to adhere to Contact Precautions. However, visitors are required to practice Standard Precautions including hand hygiene and PPE as needed to reduce the risk of exposure.
Patient
Transport
Practice hand hygiene before and after transporting the patient. Notifyreceiving department that Contact Precautions are required.
Cover wounds and contain body fluids. Ensure inpatients wear a clean gown and clean their hands before
leaving their room. When possible, transport a patient in a wheelchair or stretcher rather
than in their bed. Cover the wheelchair or stretcher with clean linen before seating the
patient. Wipe the wheelchair or stretcher with hospital-approved disinfectant
30

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
8
wipes after transporting the patient.
Patient Care
Equipment
Dedicate the use of equipment (e.g., stethoscope, blood pressure cuff) toa single patient.
Use single-patient disposable items whenever possible. Disinfect reusable patient care equipment using the hospital-approved
disinfectant before use on another patient.Room
Cleaning Use standard practices.
Ambulation See Criteria for Ambulating Patients on Contact Precaution, Form #10910.
Table 4
CONTACT/SPORE
PRECAUTIONS
Inpatient Outpatient
Interventional Areas
Key Elements Use in addition to Standard Precautions.
Hand Hygiene
Clean hands with alcohol-based hand rub or soap and water upon entering the room. Soap and water must be used when exiting the room.
Clean hands with alcohol-based hand rub or soap and water before each patient encounter. Soap and water must be used after each encounter.
PPE
Wear gown and gloves onentry to patient room.
Dispose of all PPE beforeleaving the room.
PPE is single use.
Wear gloves and gowns whenexposure to blood and bodyfluids, mucous membranes,non-intact skin or potentiallyinfectious material isanticipated.
Dispose of all PPE beforeleaving the patient care area.
PPE is single use.
Room Assignment
Use private room. Cohortpatients with the same germin the same room if privateroom not available.
If patient must be placed inan open bed unit, visiblyseparate the patient bed bycurtain.
Visibly separate the patient bedby curtain or door.
Precautions Signs Post the Contact/Spore Precautions sign outside the room where clearly visible.
Use the Contact/Spore Precautions sign to communicate isolation status in areas with increased risk of exposure to infectious materials, e.g. surgery center).
31
STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
9
Visitors
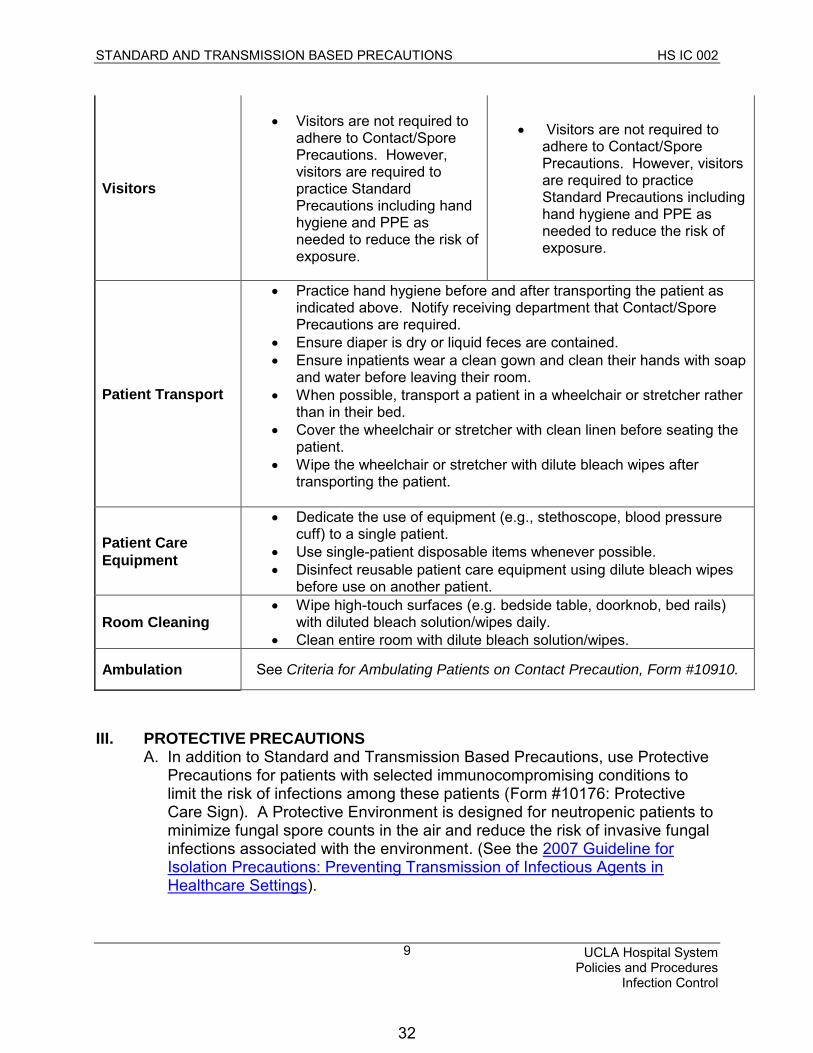
Visitors are not required toadhere to Contact/SporePrecautions. However,visitors are required topractice StandardPrecautions including handhygiene and PPE asneeded to reduce the risk ofexposure.
Visitors are not required toadhere to Contact/Spore Precautions. However, visitors are required to practice Standard Precautions including hand hygiene and PPE as needed to reduce the risk of exposure.
Patient Transport
Practice hand hygiene before and after transporting the patient asindicated above. Notify receiving department that Contact/SporePrecautions are required.
Ensure diaper is dry or liquid feces are contained. Ensure inpatients wear a clean gown and clean their hands with soap
and water before leaving their room. When possible, transport a patient in a wheelchair or stretcher rather
than in their bed. Cover the wheelchair or stretcher with clean linen before seating the
patient. Wipe the wheelchair or stretcher with dilute bleach wipes after
transporting the patient.
Patient Care
Equipment
Dedicate the use of equipment (e.g., stethoscope, blood pressurecuff) to a single patient.
Use single-patient disposable items whenever possible. Disinfect reusable patient care equipment using dilute bleach wipes
before use on another patient.
Room Cleaning Wipe high-touch surfaces (e.g. bedside table, doorknob, bed rails)
with diluted bleach solution/wipes daily. Clean entire room with dilute bleach solution/wipes.
Ambulation See Criteria for Ambulating Patients on Contact Precaution, Form #10910.
III. PROTECTIVE PRECAUTIONSA. In addition to Standard and Transmission Based Precautions, use Protective
Precautions for patients with selected immunocompromising conditions to limit the risk of infections among these patients (Form #10176: Protective Care Sign). A Protective Environment is designed for neutropenic patients to minimize fungal spore counts in the air and reduce the risk of invasive fungal infections associated with the environment. (See the 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings).
32

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
10
B. Protective Precautions may include:
Use of private room No live plants or fresh cut flowers No raw fruit or vegetables No rectal procedures (e.g. temperature)
C. Department or service specific protocols shall be utilized for high-risk patients. The Heart Transplant service utilizes Form #312758 and the Lung Transplant service utilizes Form #10106.
IV. INPATIENT BEHAVIORAL HEALTH
Staff who work in inpatient units in Resnick Psychiatric Hospital are required toadhere to Transmission Based Precautions with the following modifications:
For Contact or Contact/Spore Precautions, PPE is required only whenthere is reasonable risk of exposure to potentially infectious material (e.g.draining Foley bag, changing diaper, toileting).
33

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
11
TABLE 5. CLINICAL SYNDROMES OR CONDITIONS WARRANTING EMPIRIC PRECAUTIONS
PENDING CONFIRMATION OF DIAGNOSIS
Clinical Syndrome or Condition1
Potential Pathogens2
Empiric Precautions
Diarrhea
acute diarrhea with a likely infectious cause in an incontinent or diapered patient Enteric pathogens3 Contact
diarrhea in an adult with a history of recent antibiotic use Clostridium difficile Contact/Spore
Meningitis Neisseria meningitidis Hemophilus influenzae Droplet
Rash or exanthems
generalized, cause unknown, petechial/ecchymotic with fever Neisseria meningitidis Droplet
vesicular varicella Airborne/ Contact
maculopapular with coryza and fever Rubeola (measles) Airborne Respiratory infections
cough/fever/upper lobe pulmonary infiltrate Mycobacterium tuberculosis Airborne
paroxysmal or severe, persistent cough during periods of pertussis activity Bordetella pertussis Droplet
respiratory infections, particularly bronchiolitis and croup in infants and young children
Respiratory syncytial or Parainfluenza virus
Droplet/Contact, prolonged shedding may occur in immunocompromised patients. Longer duration may be necessary in high-risk populations.
Cystic Fibrosis (CF)
Contact for all CF patients regardless of B. cepacia status per Nur-HS G1036.
Skin or wound infection
abscess or draining wound that cannot be covered
Staphylococcus aureus, Group A streptococcus Contact
1Patients with the syndrome or conditions listed below may have atypical signs or symptoms (e.g. pertussis in neonates and adults may not have paroxysmal or severe cough). The
34

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
12
clinician’s index of suspicion should be guided by the prevalence of specific conditions in the community, as well as clinical judgment. 2The organisms listed under the column “Potential Pathogens” are not intended to represent the
complete or even most likely diagnoses, but rather possible etiologic agents that require additional precautions beyond Standard Precautions until they can be ruled out. 3These pathogens include enterohemorhagic Escherichia coli 0157:H7, Shigella, hepatitis A, and rotavirus.
TABLE 6. DISEASE/CONDITIONS
REQUIRINGPRECAUTIONS
DISEASE/CONDITION PRECAUTIONS COMMENTS Abscess Draining, major Draining, minor or limited
Contact Standard
Until drainage stops
Acinetobacter, resistant to meropenem Contact Duration of hospitalization and for each readmission. There is no clearance process for this class of organisms.
Acinetobacter, sensitive t to meropenem Standard AIDS/HIV infection Standard Actinomycosis Standard Adenovirus Droplet/Contact Duration of Illness,
prolonged shedding may occur in immunocompromised patients. Longer duration of isolation may be necessary in high-risk populations.
Amebiasis Standard Anthrax
Aerosolizable spore-containing powder Non-intact skin with draining lesions
Standard Airborne/Contact Contact
Ascariasis Standard Aspergillosis Pulmonary & other sites Wound
Standard Airborne/Contact Duration of illness,
precautions if massive soft tissue infection with copious drainage and repeated irrigations.
Babesiosis Standard Bed bugs Contact Duration of hospitalization.
Refer to HS 1441.
35

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
13
Blastomycosis,NorthAmerican, cutaneous or pulmonary
Standard
Bocavirus Contact Duration of illness Botulism Standard Bronchiolitis (see respiratory infections in infants and young children) Brucellosis (Undulant, Malta, Mediterranean fever)
Standard
Burkholderia cepacia in CF patients
Burkholderia cepacia that is multidrug resistant
Contact
Contact/Droplet
Duration of hospitalization and for each readmission. Do not cohort with non colonized CF patients.
Campylobacter gastroenteritis Diapered or incontinent
Standard Contact Duration of illness
Candidiasis, all forms including mucocutaneous
Standard
Carbapenem-resistant Enterobacteriaceae(CRE)
Contact Duration of hospitalization and for each readmission. There is no clearance process for this class of organisms.
Cat-scratch fever (benign inoculation lymphoreticulosis)
Standard
Cellulitis, uncontrolled drainage Contact Until drainage stops Chancroid (soft chancre) Standard Chickenpox (varicella) Airborne /Contact Minimum of 5 days after
onset of rash and until all lesions are crusted.
Chickenpox (varicella) exposure Exposed susceptible patients
Exposed susceptible staff
Airborne/Contact
N/A
Place on isolation from day 8-21 from exposure. If immunoglobulin given, continue until day 28 after exposure.
Exposed staff, refer to policy HS IC 7402.
Chlamydia trachomatis (any site) Standard Cholera Diapered or incontinent
Standard Contact Duration of illness
Closed-cavity infection (any) Standard Clostridium botulinum Standard Clostridium difficile (i.e. “C. diff”) Contact/Spore Duration of hospitalization.
Patients who test positive at any time during their
36

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
14
hospitalization must remain on Contact/Spore Precautions until discharge, even if their room location changes. Patients with a history of C. difficile do not need to be isolated upon admission unless they are exhibiting signs of active illness and/or C. difficile is suspected. Contact Clinical Epidemiology for further questions/evaluation.
Clostridium perfringens food poisoning or wound
Standard
Colorado tick fever Standard Congenital rubella Contact Until 12 mo of age Coccidiodomycosis (valley fever) Standard Conjunctivitis, bacterial (ANY) Standard Conjunctivitis, viral (acute hemorrhagic) Contact Duration of illness Coronavirus (non-SARS) i.e., 229E, HKUI, NL63, OC43
Droplet/ Contact
Duration of illness
Coronavirus (SARS), SARS-CoV
Airborne/ Contact
Call Clinical Epidemiology. Duration of Illness plus 10 days after resolution of fevers, provided respiratory symptoms are absent or improving.
Coxsackie virus Diapered or incontinent
Standard Contact
Duration of illness
Creutzfeldt-Jakob disease Standard Call Clinical Epidemiology Some tissues require special disposal/cleaning..
Croup Adults Infants and Children
Standard Contact
Duration of Illness
Cryptococcosis Standard Cryptosporidiosis Diapered or incontinent
Standard Contact
Duration of Illness
Cysticercosis Standard Cytomegalovirus infection Standard No additional precautions
for pregnant healthcare workers
Decubitus ulcer, major infected
Contact
37

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
15
minor or limited Standard Dengue fever Standard Diarrhea, infection suspected Contact Duration of illness or
hospitalization (depends on organism).
Diphtheria, cutaneous Contact Until off antibiotic therapy and two cultures taken 24 hr. apart are negative
Diphtheria, pharyngeal Droplet Until off antibiotic therapy and two cultures from both nose and throat taken 24 hr. apart are negative
Ebola viral hemorrhagic fever Airborne/Contact Call Clinical Epidemiology. Duration of Illness
Echnococcosis (hydatidosis) Standard Echovirus (enterovirus) Diapered or incontinent
Standard Contact Duration of illness
Encephalitis
Eastern Encephalitis Western Encephalitis Venezuelan equine encephalomyelitis St. Louis encephalitis California encephalitis
Standard
Enteroviral Illness (coxsackie, echovirus, enterovirus) Diapered or incontinent
StandardContact Duration of Illness
Endometritis Standard Enterobacter species, resistant to meropenem
Contact Duration of hospitalization and for each readmission. There is no clearance process for this class of organisms.
Enterobiasis (Pinworm disease, oxyuriasis)
Standard
Epiglottitis, caused by H. influenzae Droplet Until 24 hrs after initiation effective therapy
Epstein-Barr virus infection, including infectious mononucleosis
Standard
Erythema infectiosum (see Parvovirus B19) Droplet Duration of Illness. Duration of hospitalization for immunocompromised patients.
Escherichia coli, resistant to meropenem Contact Duration of hospitalization and for each readmission
Escherichia coli, sensitive to meropenem Standard Escherichia coli gastroenteritis Diapered or incontinent
Standard Contact
38

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
16
Duration of illness unless E. coli is resistant to meropenem (see above).
Food Poisoning (any) Standard Furunculosis-staphylococcal Infants and young children Contact Duration of Illness Gangrene (Gas gangrene) Standard Giardia lamblia Diapered or incontinent
Standard Contact Duration of illlness
German Measles (rubella)
Congenital rubella
Droplet
Contact
Until 7 days after onset of rash
Until 1 year of age, unless 2 clinical cultures obtained 1 month apart after 3 months of age are negative
Gonococcal ophtalmia neonatorum Standard Gonorrhea Standard Granuloma inguinale (donovanosis, granuloma venereum)
Standard
Guillain-Barre syndrome Standard Hand, foot, and mouth disease (enterovirus) Diapered or incontinent
Standard Contact
Duration of Illness Haemophilus influenza serotype b (Hib)
Meningitis
Other invasive bacteremia, epiglottitis, septic arthritis, osteomyelitis, pericarditis, cellulitis
Pneumonia Infant and children
Adult
Droplet
Droplet
Droplet
Standard
Until 24 hours after effective therapy
Until 24 hours after effective therapy
Until 24 hours after effective therapy
Hantavirus pulmonary syndrome Standard
Helicobacter pylori Standard
Hemorrhagic fevers (for example Lassa,Ebola, Marburg, Crimean-Congo fever)
Airborne/Contact Call Clinical Epidemiology immediately. Duration of Illness.
Hepatitis, Type A, adults Type A, diapered or incontinent
Standard Contact Children < 3 years, use
39
STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
17
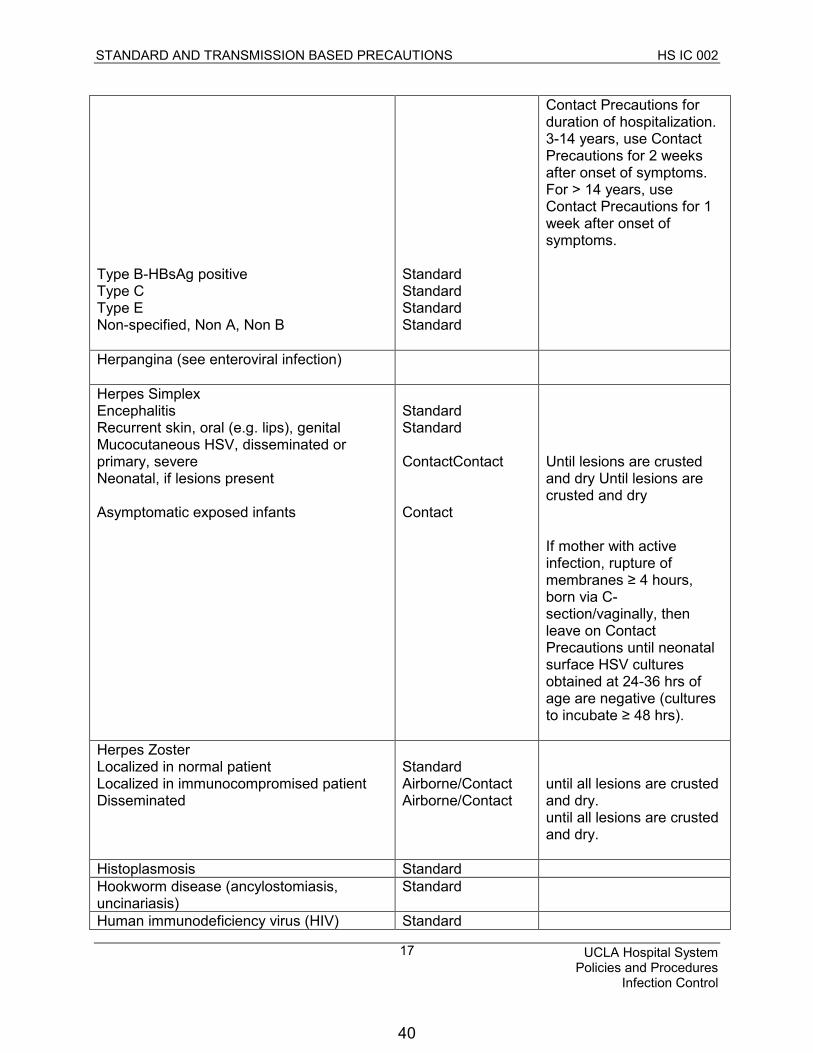
Type B-HBsAg positive Type C Type E Non-specified, Non A, Non B
Standard Standard Standard Standard
Contact Precautions for duration of hospitalization. 3-14 years, use Contact Precautions for 2 weeks after onset of symptoms. For > 14 years, use Contact Precautions for 1 week after onset of symptoms.
Herpangina (see enteroviral infection)
Herpes Simplex Encephalitis Recurrent skin, oral (e.g. lips), genital Mucocutaneous HSV, disseminated or primary, severe Neonatal, if lesions present
Asymptomatic exposed infants
Standard Standard
ContactContact
Contact
Until lesions are crusted and dry Until lesions are crusted and dry
If mother with active infection, rupture of membranes ≥ 4 hours,born via C-section/vaginally, then leave on Contact Precautions until neonatal surface HSV cultures obtained at 24-36 hrs of age are negative (cultures to incubate ≥ 48 hrs).
Herpes Zoster Localized in normal patient Localized in immunocompromised patient Disseminated
Standard Airborne/Contact Airborne/Contact
until all lesions are crusted and dry. until all lesions are crusted and dry.
Histoplasmosis Standard Hookworm disease (ancylostomiasis, uncinariasis)
Standard
Human immunodeficiency virus (HIV) Standard
40

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
18
infection Human metapneumovirus Droplet + Contact Duration of Illness Impetigo Contact Until 24 Hours after
effective therapy Infectious mononucleosis Standard Influenza
Influenza A or B, human (includes H1N1)
Droplet Duration of Illness, prolonged shedding may occur in immunocompromised patients. Longer duration of isolation may be necessary for high-risk populations.
Kawasaki syndrome Standard Klebsiella pneumoniae, resistant to meropenem (CRE)
Contact Duration of hospitalization and for each readmission. There is no clearance process for this class of organisms.
Klebsiella pneumoniae, sensitive to meropenem
Standard
Lassa fever Airborne/Contact Call Clinical Epidemiology immediately. Duration of Illness.
Legionnaires’ disease /Legionella Standard Leprosy Standard Leptospirosis Standard Lice (pediculosis) Contact Until 24 Hours after
effective therapy. Refer to HS 1441.
Listeriosis Standard Lyme disease Standard Lymphocytic choriomeningitis Standard Lymphogranuloma venereum Standard Malaria Standard Marburg virus disease Airborne/Contact Call Clinical Epidemiology
Immediately. Duration of Illness.
Measles (rubeola), all presentations Airborne Call Clinical Epidemiology Immediately. Four days after onset of rash or duration of illness in immunocompromised patients.
Meliodiosis, all forms Standard Meningitis, bacterial
41

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
19
H. flu and N. meningitidis
S. pneumonia (pneumococcus), listeria
Droplet
Standard
Until 24 Hours after effective therapy
Meningitis, viral, aseptic, fungal Standard Treat all meningitis as bacterial until viral diagnosis is confirmed
Meningitis (Haemophilus influenza) Droplet Duration of illness
Metapneumovirus, human Droplet/Contact Duration of Illness Methicillin-resistant Staphylococcus aureus(MRSA) infection or colonization
Draining wounds
Standard
Contact
Duration of illness
Molluscum contagiosum Standard Monkeypox/Monkeypox virus Airborne/Contact Airborne Precautions until
smallpox excluded. Contact Precautions until all lesions are crusted.
Mucormycosis Standard Multidrug-resistant organisms, infection or colonization
Contact May require Contact Precautions. Call Clinical Epidemiology.
Mumps (infectious parotitis) Droplet Until 5 days after onset of parotid swelling. Longer duration may be necessary in high-risk populations.
Mycobacteria, nontuberculosis (atypical) any site
Standard
Mycoplasmal pneumonia Droplet Duration of illness Necrotizing entercolitis Standard Nocardiosis Standard Norovirus gastroenteritis Contact Duration of Illness Orf Standard Parainfluenza virus infection Contact Duration of Illness.
Prolonged shedding may occur in immunocompromised patients. Longer duration of isolation may be necessary in high-risk populations.
Parvovirus B19 (erythema infectiosum) Droplet Duration of Illness, Duration of hospitalization for immunocompromised patients
Pertussis (whooping cough) Droplet Until after 5 days of effective therapy
Pharyngitis in infants and young children
42

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
20
caused by: Adenovirus Orthomyxoviridae Epstein-Barr virus Herpes simplex virus
Streptococcal disease (group A streptococcus)
Droplet/Contact Droplet Droplet Droplet/Contact
Droplet
Duration of Illness. Prolonged shedding may occur in immunocompromised patients. Longer duration of isolation may be necessary.
Until 24 hours after initiation of appropriate antibiotics
Pinworm infection (Enterobius) Standard Plague Bubonic
Pneumonic (Yersinia petis)
Standard
Droplet
Call Clinical Epidemiology Immediately
Until 48 hours of effective therapy
Pleurodynia Adults
Children, infants Standard Contact Duration of Illness
Pneumonia
Adenovirus
Bacterial not listed elsewhere
Burkholderia Cepacia in CF patients
Chlamydia
Fungal
Haemophilus influenzae Adults Infants and children (any age)
Meningococcal
Pneumococcus (S. pneumoniae)
Pneumocystis carinii
Staphylococcus aureus
Droplet/Contact
Standard
Contact
Standard
Standard
Standard Droplet
Droplet
Standard
Standard
Standard
Duration of Illness
Do not cohort with non colonized CF patients
Until 24 hours after effective therapy
Until 24 hours after effective therapy
Do not cohort with
43

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
21
Streptococcus, Group A (any age group)
Viral Adults Infants, Children, Immunocompromised Adults
Droplet Standard Contact
immunocompromised patient. Until 24 hrs after effective therapy Duration of illness
Poliomyelitis Contact Duration of illness Pseudomonas aeruginosa, resistant to all aminoglycosides
Contact Duration of hospitalization and for each readmission. There is no clearance process for this class or organisms.
Pseudomonas aeruginosa, sensitive to all aminoglycosides (
Standard organisms.
Psittacosis (ornithosis) Standard Q fever Standard Rabies Standard Rat-bite fever (Streptobacillus moniformis disease, Spirillum minus disease)
Standard
Relapsing fever Standard Respiratory syncytial virus (RSV)
Droplet/Contact
Duration of illness, prolonged shedding may occur in immunocompromised patients. Longer duration of isolation may be necessary.
Reye’s syndrome Standard Rheumatic fever Standard Rhinovirus Droplet Duration of illness Rickettsialpox (vesicular rickettsiosis) Standard Ringworm (dermatophytosis, dermatomycosis, tinea)
Standard
Ritter’s disease (staphylococcal scalded skin syndrome)
Contact Duration of illness
Rocky Mountain spotted fever Standard Roseola infantum (exanthum subitum) Standard Rotavirus Diapered or incontinent
Standard Contact
Duration of illness. Prolonged shedding may occur in immunocompromised patients. Longer duration
44

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
22
of isolation may be necessary.
Rubella (German Measles)
Congenital rubella
Droplet
Contact
Until 7 days after onset of rash
Until 1 year of age, unless 2 clinical cultures obtained 1 month apart after 3 months of age are negative
Salmonella species (including S. typhi) Diapered or incontinent Typhoid fever
Standard Contact Contact
Duration of illness Contact Precautions should be continued until 3 cultures, performed 48 hr after stopping antibiotics, are negative
SARS (Severe Adult Respiratory Syndrome) Airborne/Contact Call Clinical Epidemiology. Duration of illness plus 10 days after resolution of fevers, provided respiratory symptoms are absent or improving.
Scabies Contact Until 24 hrs after effective therapy. Refer to HS 1441.
Schistosomiasis (bilharziasis) Standard Shigella species Diapered or incontinent Standard
Contact Duration of Illness Shingles (see Herpes zoster or Zoster) Sporotrichosis Standard Spirillium minus disease (rat-bite fever) Standard Staphylococcal disease (S. aureus) Skin, wound, or burn Major Minor or limited Enterocolitis Adult Children, infants, incontinent
MRSA Pneumonia Scalded skin syndrome (Ritter’s) Toxic shock syndrome
Contact Standard
Standard Contact
Standard Standard Contact Standard
Duration of illness
Duration of illness
Duration of illness
Streptobacillus moiliformis disease (rat-bite fever)
Standard
45

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
23
Streptococcal disease (group A Streptococcus)
Skin, wound, burn
Endometritis (pleural sepsis) Pharyngitis in infants and young children Pneumonia in infants and young children Scarlet fever in infants and young children Serious invasive disease
Contact
Standard Droplet Droplet Droplet Droplet
Until 24 hrs after effective therapy
Until 24 hrs after effective therapy Until 24 hrs after effective therapy
Streptococcal disease (group B Streptococcus), neonatal
Standard
Streptococcal disease (not group A or B) unless covered elsewhere
Standard
Strongyloidiasis Standard Syphilis Skin and mucous membrane, including congenital, primary secondary Latent (tertiary) and seropositivity without lesions
Standard
Tapeworm disease Hymenolepis nana
Taenia solium (pork) Other
Standard Standard Standard
Tetanus Standard Tinea (fungus infection dermatophytosis, dermatomycosis, ringworm)
Standard
Toxoplasmosis Standard Toxic shock syndrome (staphylococcal disease)
Standard
Trachoma, acute Standard Trench mouth (Vincent’s angina) Standard Trichinosis Standard Trichomoniasis Standard Trichuriasis (whipworm disease) Standard Tuberculosis
Extrapulmonary Extrapulmonary, draining lesion
(including scrofula)
Pulmonary, confirmed or suspected
Laryngeal disease, confirmed orsuspected
Extrapulmonary, meningitis
Standard
Airborne/Contact
Airborne
Airborne
Standard
Patients with extrapulmonary TB infection should be assessed for concurrent pulmonary infection.
Keep on Airborne
Precautions until 3
negative AFB smears are
obtained; no sooner than
q8h apart (with one early
AM specimen), or patient
46

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
24
PPD or serology test positive with no
evidence of current pulmonary disease
Standard
is cleared by Pulmonary
or Infectious Disease
Attending. Note that if
the patient has been
reported to LA County
TB Control, patient may
require longer duration
of isolation. Consult
Clinical Epidemiology. Typhoid (Salmonella typhi) fever (see gastroenteritis) Diapered or incontinent
Standard Contact
Duration of illness
Typhus, endemic and epidemic Standard Urinary tract infection (including pyelonephritis), with or without urinary catheter
Standard
Vaccinia virus (smallpox vaccine), including conjunctivitis, rash, encephalitis
Contact Duration of illness/ Call Clinical Epidemiology. This includes all patients who had recent (< 30 days) smallpox vaccination or close contact with a person who received a smallpox vaccination.
Vancomycin resistant enterococci (VRE) Standard Varicella (chickenpox) Exposed susceptible patients Exposed susceptible staff
Airborne/Contact Airborne/Contact N/A
Minimum of 5 days and until all lesions are crusted. Susceptible individuals should not enter the room if immune caregivers are available. Place on Airborne/Contact Precautions from day 8-21 from exposure. If immunoglobulin given, continue until day 28 after exposure. Exposed staff, refer to HS IC 7402.
Vibrio parahaemolyticus Diapered or incontinent
Standard Contact
Duration of illness
Vincent’s angina (trench mouth) Standard Viral diseases Respiratory (if not covered elsewhere)
47

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
25
Adults Infants and young children
Standard Contact Duration of illness
Whooping cough (pertussis) Droplet Until 5 days after effective therapy
Wound infections Major Minor or limited
Contact Standard
Duration of Illness
Yellow fever Standard Yersinia entercolitica gastroenteritis Standard Zoster (varicella-zoster) Localized in immunocompromised patient, disseminated
Localized in normal patient
Airborne/ Contact
Standard
Susceptible individuals should not enter the room. Use Airborne/Contact Precautions until all lesions are crusted.
Susceptible individuals should not enter the room
Zygomycosis (phycomycosis, mucormycosis)
Standard
48

STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
26
APPENDIX A
SEQUENCE FOR DONNING AND REMOVING PPE
49
STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
27
FORMS & POLICIES
Policy HS IC 001 Hand Hygiene
Policy HS IC 005 Airborne Disease Transmission Policy
Policy HS IC 006 Exposure Control Plan for Bloodborne Pathogens
Policy HS 8614 Negative and Positive Pressure Rooms
Policy HS IC 7402 Varicella (Chickenpox/Zoster) Exposure Management
Policy HS 1441 Prevention, Containment and Management of Patients withInsect Infestation
Form 10910 Criteria for Ambulating Patients on Contact Precaution
Form 11249 Isolation Precautions: Nurse Education Instruction
Form 11246 Patient and Visitor Instructions for Patients on Isolation Precautions
REFERENCES
2007 Guideline for Isolation Precautions: Preventing Transmission of InfectiousAgents in Healthcare Settingshttp://www.cdc.gov/hicpac/2007ip/2007isolationprecautions.html
Standards Presentation California Occupational Safety and Health StandardsBoard Proposed State Standard, Title 8, Division 1, Chapter 4http://www.dir.ca.gov/oshsb/atdproptext.pdf
2011 Centers for Disease Control and Prevention Guide to Infection Preventionin Outpatient Settings
http://www.cdc.gov/HAI/pdfs/guidelines/standatds-of-ambulatory-care-7-2011.pdf
Centers for Disease Control and Prevention Sequence for Donning andRemoving PPE Poster
http://www.cdc.gov/HAI/pdfs/ppe/ppeposter1322.pdf
CONTACT: Medical Directors, Clinical Epidemiology and Infection Prevention, RR UCLAMC and SM UCLA MC & OH
REVISION HISTORY
Effective Date: April 1997 (Combined with HS IC 003 – June 30, 2014)
Review Date: March 1998, February 2000, October 2001, April 2002, January 2003, July 2003, April 2004, November 2, 2004, September 29, 2005, September 5, 2006, March 2008, April 24, 2008, August, 2008, September 2009, February 2010,
50
STANDARD AND TRANSMISSION BASED PRECAUTIONS HS IC 002
UCLA Hospital System Policies and Procedures
Infection Control
28
August 25, 2010, January 25, 2012, September 26, 2012, February 26, 2014, (Exec.Comm - March 31, 2014)
Revision Date: September 30, 2010, February 29, 2012, October 31, 2012, June 30, 2014
APPROVAL
David Feinberg, MD Associate Vice Chancellor and CEO UCLA Hospital System
Kevin M. Shannon, MD Chief of Staff Ronald Reagan UCLA Medical Center
Denise Sur, MD Chief of Staff Santa Monica - UCLA Medical Center and Orthopaedic Hospital
Stephen Chen, MD Chief of Staff Resnick Neuropsychiatric Hospital at UCLA
51
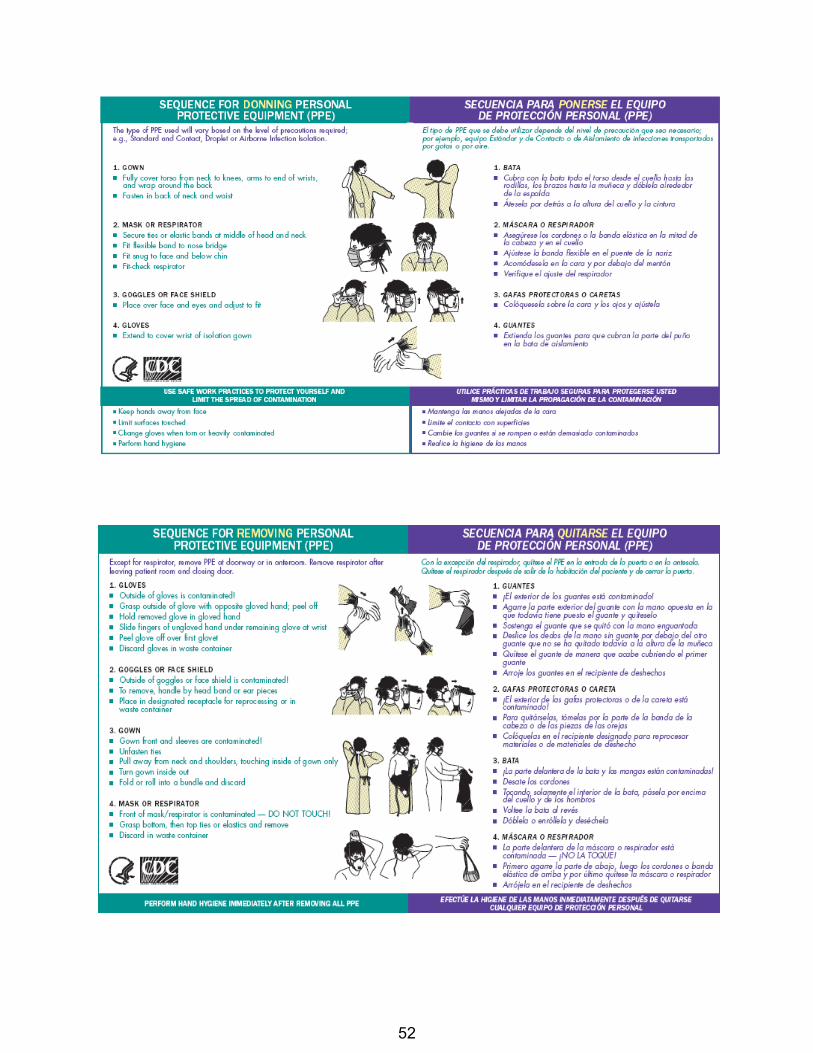
52

Handwashing (UCLA)
Quicksheet
Soap and Water 1. Wets hands and use approved soap2. Rubs hands vigorously at least 15 sec3. Rinses with running lukewarm water4. Keeps fingers pointed down5. Dry hands well6. Discards paper towel7. Turns off faucet with dry paper towel
Alcohol Based Sanitizers For touch dispenser method:
1. Hits the dispenser once2. Dips fingers into cupped filled hands3. Spreads around hands with friction until completely dissolved
For touch less dispenser method: 1. Places palm of hand under dispenser2. Dips fingers into cupped filled hands
3. Spreads around hands with friction until completely dissolved
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
53

Removing Disposable Gloves (UCLA)
Quicksheet
1. Wash hands before donning gloves.2. Put on gloves pulling up over wrists.3. Remove first glove by pulling from the outside of wrist, turning glove inside out.4. Remove second glove by reaching inside wrist with fingers and turning inside out over thefirst glove. 5. Discard gloves.
6. Wash hands.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
54

Ancillary Staff
Day 2 Skills
55

Day 2 Ancillary Staff Skills CLABSI:
1. Hand washing prior to touching CVC site and IV tubing is critical to the prevention of infections.
2. Observation of CVC Dressing a. Report to RN: redness, swelling, drainage at insertion site (signs of infection), line
disconnection) 3. Observation of the insertion procedure and stopping the insertion attempt if aseptic
technique is broken (unless it is an emergency situation).
Blood Administration: Assistive Staff’s Role with Blood Administration 1. The MD, RN, Perfusionist, Nurse Anesthetist or IV-Certified LVN transfusionist is
responsible for administering the blood products, taking the patient’s vital signs, maintaining the infusion, and observing for signs and symptoms of transfusion reaction.
2. Full set of Vital Signs are taken before and after the transfusion (blood pressure, temperature, pulse, and respiration rate).
3. Additional vital signs are recorded as ordered by the MD or at the care taker’s (RN/LVN) discretion.
4. Report any change in patient’s condition to the RN. a. Frequent signs and symptoms— Less serious:
i. Chills and fever. ii. Backache or other aches and pains.
iii. Hives and itching. b. Frequent signs and symptoms—More serious:
i. Blood-cell destruction (hemolysis) causing shortness of breath, severe headache, chest or back pain and blood in the urine.
CAUTI: 1. Facts about CAUTI
a. About 95% of UTIs occur when bacteria ascend the urethra to the bladder b. Up to 69% of CAUTI may be PREVENTABLE c. CAUTI is the leading cause of secondary hospital-acquired blood stream
infections d. The risk of a UTI increases 5% each day the urinary catheter remains in place
2. CAUTI Prevention is largely impacted by the work that Care Partners do: a. Assist with:
i. repositioning, ii. elimination needs,
iii. Walking, transports, etc. iv. Emptying Foley drainage v. Report any changes to the RN
56

3. Urinary catheter care and maintenance: a. Proper Maintenance
i. Use standard precautions and hand hygiene when handling catheter or drainage system.
ii. Meatal care with soap and water every shift and PRN iii. Start from meatal area outward towards catheter iv. Perineal care after each bowel movement
b. Maintain unobstructed urinary flow: i. Check for kinks and dependent loops in catheter tubing
ii. Maintain drainage bag below level of bladder at all times iii. Avoid reflux: Keep urinary drainage bag below level of area being
drained. Teach patient to do the same. c. Maintain a sterile closed drainage system
4. Notify RN for: a. Distention and retention b. Dribbling and leaks c. Changes in appearance in:
i. urine – i.e. color, clots, tissue, mucous plugs. ii. Foley – breaks in catheter set up
iii. securement device iv. surrounding skin – redness, swelling, drainage v. Patient reports of pain
Skin Care and Pressure Ulcer Prevention 1. Introduction of wound service (when to consult) 2. Skin Care Products: bathing, incontinent care, skin folds 3. Pressure Ulcer Prevention and Treatment
a. Pressure Ulcers present on admission—what to do b. Hospital-acquired pressure ulcers
4. Review of Skin Care/Wound Care Guideline (with products, boots, and specialty beds) 5. Bed Making Standard 6. Ostomy (stool and urine) 7. Ancillary Skills: Wound Care, and simple clean dressing changes
57
Admitting the Patient (UCLA)
Quicksheet
1. Assemble the following equipment: - Equipment for urine specimen - Tempa Dot - Flowsheets - Stethoscope - Scale - Blood pressure cuff and manometer
2. Identify the patient both by asking the name and checking the identification bracelet. - Introduce yourself
3. Provide privacy with curtain. 4. Help the patient to undress and put on a hospital gown or night clothes from home. 5. Check the patient's vital signs, weight, and height. 6. Help the patient get into bed. Adjust side rails as needed. 7. If the patient is wearing any jewelry or has valuables that were not left at the cashier's office: a. Make a list of them and check with R.N. regarding placement. 8. Collect a urine specimen if necessary. a. Assist the patient as necessary. b. Allow patient to use the bathroom, if ambulatory, or offer the bedpan or urinal. 9. Pour the specimen from the bedpan into the specimen bottle. Put on the cap. Label the specimen correctly. 10. Start the admission form including:
- Observations - Vital signs (TPR, BP, height, weight) - Allergies - Medications being taken - Food preferences and dislikes
11. Orient the patient to the unit by explaining: - Visiting hours - How to use the phone and/or television - Facility routines
- When meals and refreshments are provided
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
58

Rounding (UCLA)
Quicksheet
KEY ELEMENTS MET 1. Knocks on patient door and enters patient room.2. Uses hand gel or washes hands upon entering room.3. Greets patient by using patient’s preferred name.4. Introduces self- (If pt has not called RN, LVN, CCP by name thatshift). 5. Explains scheduled tasks and then performs them (Ex: Assessment,medication administration, etc…). 6. Individually addresses the 6 P’s (Pain, Personal Needs, Position,Placement, Prevention of Falls, and Pumps) with meaningful patient interaction. 7. Conducts environmental assessment (Urinal/commodechecked/emptied, IV pole and tubing checked, white board updated w/appropriate contacts-RN, CP, MD, etc….) 8. Asks pt if there is anything they may need before RN or CCP leavesthe room and responds to requests appropriately. 9. Explains when they or other team members will return.10. Uses hand gel or washes hands upon exiting the room.11. Documents the round in CareConnect.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
59

Transferring the Patient (UCLA)
Quicksheet
1. Determine the unit.2. Get the necessary vehicle (wheelchair, stretcher, or patient's own bed).3. Transfer equipment with the patient as needed.4. Assemble the equipment needed:
- Patient's chart - Flowsheets - Medications - Other equipment, supplies.
5. Gather all patient's belongings together.6. Assist the patient to put on robe and slippers if ambulatory. Assist patient into wheelchair. Ifbed is used, pull the side rails up. 7. Transport patient and belongings to new unit.8. Assist staff in helping patient into bed. Assist in putting away patient's belongings and helpingpatient to become settled.
9. Give any transferred medications, flowsheets, and chart to nurse in charge.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
60

Discharging the Patient (UCLA)
Quicksheet
1. Help the patient to dress, if necessary.
2. Collect the patient's personal belongings.a. Pack, if necessary.b. Make sure that all of the patient's belongings have been removed from the closet andbedside stand. c. Check to see if medications or other equipment are to go home with the patient.d. Verify that the patient has received discharge instructions from the nurse, physician, ordischarge coordinator.
3. Help patient into wheelchair.
4. Take patient to the discharge entrance of the facility.a. Help patient to transfer safely into the vehicle.
5. Return wheelchair.
6. Return to patient unit.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
61

Pulses (UCLA)
Quicksheet
PERIPHERAL 1. Palpate arteries with middle three (3) fingers. 2. Count for 30 sec. and multiply by two: if pulse is irregular, count for full minute. 3. Record rate and rhythm. RADIAL 1. Palpate radial artery using pads of middle three (3) fingers of your hand.
a. Palpate over inner surface of wrist directly over radius. b. Press artery against bone and gradually release pressure.
2. Count pulse for 30 sec., if regular, and multiply x 2; Take apical pulse if irregular and count for 60 sec. APICAL 1. Place stethoscope over apex of heart at left midclavicular line, 5-6 intercostal space. 2. Count for one minute.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
62

Taking Blood Pressure (UCLA)
Quicksheet
Alert Contraindications: Do not put the cuff on limbs with DVT, grafts, ischemic changes, AV fistula, AV graft, PICC line site, Peripheral IV site with IV infusing, trauma, or incisions. If Dinamap is being used please note the following:• One BP cuff per patient and keep in patient room If Patient is in any Isolation, use disposable stethoscope
1. Choose appropriate sized cuff.2. Wrap the cuff snugly and smoothly around the upper part of the arm, about 1-2 inches abovethe antecubital space with the center of the bladder over the brachial artery. See diagram for other sites. 3. Palpate the brachial artery (just medial to the midline).4. Place stethoscope on the medial antecubital space.5. Place earpieces in ears.6. Close valve on manometer pump.7. Inflate to approximately 160-180.8. Read at eye level.9. Deflate cuff ~ 2 mm Hg/sec; do not re-pump totally deflating cuff.10. Note first and last sounds.11. Completely deflate cuff.12. Remove cuff and compare reading with previous reading.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
63

Taking the Respiratory Rate (UCLA)
Quicksheet
1. Count rise and fall of the chest without the patient noticing. 2. Count for 30 sec and multiply x2.
3. If respirations irregular, count for 60 sec., noticing pattern and depth.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
64

Temperature Taking (UCLA)
Quicksheet
1. Gather equipment: Tempa-Dot 2. Tear off single thermometer along perforation. 3. Remove from wrapper. FOR ORAL: 1. Place thermometer far back under tongue. 2. Instruct patient to press tongue down on thermometer with mouth closed. 3. Wait at least 60 seconds. 4. Remove thermometer and wait about 10 sec. for dots to stabilize. 5. Read temperature from last blue dot. 6. Discard thermometer. FOR AXILLARY 1. Expose the axilla; if damp, pat dry. 2. Place the thermometer in the axilla. 3. Lay the patient's arm across their chest to hold thermometer in place. 4. Leave in place 3 minutes (adults and children). 5. Remove and read last blue dot after 10 seconds.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
65
Pulse Oximeter (UCLA)
Quicksheet
1. Explains the application of the Pulse Oximeter probe2. Gathers Equipment:
· Pulse Oximeter machine (Stand alone; DASH or Solar monitor)· Pulse Oximeter cable· Pulse Oximeter probe
3. Application:· Assures that the nail is free of polish (if applicable)· Places probe on any finger/toe
4. Turns on pulse Oximeter machine5. Records pulse oximetry result
Immediately reports to RN if pulse Oximeter reading is <93% or out of range for patient
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
66

EKG Lead II (UCLA)
Quicksheet
1. Place patient in supine position.
2. Apply leads to all four extremeties between wrists/elbows & knees/ankles.
3. Connect power cord
4. Turn power switch on.
5. Set lead selector to standard.
6. Position stylus to center of paper.
7. Set EKG paper speed for a routine EKG at 25mm/sec.
8. Push standardize button to check sensitivity: The 1cm. standardization is normal.
9. Set lead dial to appropriate lead and run for 3 to 6 seconds per lead. Move lead selector dial toobtain all desired leads. Mark each lead with the machine marker.
10. Stop recording and move lead selector to standard.11. Turn off power switch.
12. Disconnect the electrodes from the patient. Wipe electrode paste off patient's chest &extremities.
13. Label EKG strip(s) with patient's name, date, time, room #, & level of chest pain ifappropriate.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
67

EKG 12-Lead Recording
Quicksheet
1. Tells patient about procedure.
2. Inputs all patient information correctly.
3. Places patient in supine position.
4. Asks patient to lie still and try to relax.
5. Prepares skin as follows:a. Shaves hair for each electrode site if appropriate.b. Rubs each electrode site thoroughly with alcohol.c. Mark each electrode site with a felt tip pen – as appropriate.
6. Standard 12-lead electrode placement:
a. Places the chest electrode (V1-V6) as seen in picture at the back of competency.b. Places the limb electrode RA & LA (avoid the bony area).c. Places the limb electrode RL & LL (avoid the bony area).
7. Makes sure that all lead wires are well connected to the 12-lead EKG machine.
8. Pushes standardized button to check sensitivity: The 1cm. standardization is normal.
9. Presses the on/off key; then the screen will display “Pat. Info, rhythm, 25mm/s”
10. Next, selects Pat.Info by pressing key 1 or 2, then prompt will appear:a. “patient last name:” PRINTs the patient last name then presses ENTER.b. Another prompt will appear “patient first name.” PRINTs the patient first name thenpresses ENTER. c. Next prompt will appear “patient ID number”. TYPES patient ID number, then pressesENTER.
11. Presses STOP key to skip all other patient information prompts, then the home screen willappear “Pat.Info, Rhythm, 25mm/s”.
12. Presses the RECORD ECG key “12”, then the screen will display “Acquiring Data”, then“ECG Acquisition complete”.
13. Prompts will appear to “change gain” from 10/mv to 2.5, or 10, or 20 mv. Presses NO unlessotherwise indicated. Yes No
68

14. Prompt will appear “Analyzing ECG” then “Printing reports” and one copy comes out
15. The following prompt will appear “number of extra copies:” TYPES your copies number,then presses ENTER. Then, prompts will show “processing ECG”.
16. After completion, makes 1 extra copy.
17. Files copy in chart.
18. Places requisition and 1 copy in EKG drawer.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
69

Recording Nasogastric Tube Drainage (UCLA)
Quicksheet
1. Put on clean gloves.2. Mark the volume of new drainage on the suction canister.3. Note 8 hour volume and color.4. Remove gloves.5. Wash hands.6. Record volume of NGT drainage on patient’s I&O sheet.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
70

External Catheter Application (UCLA)
Quicksheet
1. Assemble equipment needed- basin of warm water - washcloth and towel - disposable gloves - bed protector - external urine collection appliance (exact size)
2. Arrange equipment on over-bed table3. Lower side rail, lower bed sheets to the foot of the bed4. Place bed protector under the patient's legs and hips5. Expose genital area6. Put on disposable gloves7. Wash meatus and penile shaft with soap and water. Rinse thoroughly, then dry completely.*8. Apply catheter from meatus to distal end of penis as per manufacturer's instructions.9. Remove excess pubic hear from the penis or trim with a pair of blunt scissors (with patient'spermission). 10. Unroll the sleeve onto the penis and discard plastic collar.11. Check that catheter is evenly applied i.e. without any wrinkles.12. With patient's permission, trim pubic hair that becomes entangled in the unrolled portion ofthe catheter. Ensure that the external catheter is not too tight which can cause penile circulation to be compromised. 13. Connect external catheter to either urinary drainage or leg bag. The urine collection bagshould always be below bladder level.
14. Remove disposable glove and wash hands.
NOTE: *Do not use lotions. -Once catheter in place do not attempt to reposition it -If the penis was erect during the application, check the seal of the catheter after the penis becomes flaccid -If adhesion of the catheter is a problem, ask the RN for additional problem solving solutions. -The leg bag, tubing, and straps are reusable. The leg bag and extension tubing should be cleaned daily. The straps may be washed and air dried.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
71

Skin Care for Incontinent Patients (UCLA)
Quicksheet
1. Assembles supplies:a) Clean linensb) Warm water, mild soap, a washcloth, a towel, and toilet tissue
2. Provides for privacy3. Positions the bed4. Removes the soiled linen
a. Washes the soiled skin with warm water and mild soapb. Rinses the soap off the skin thoroughly
- Female patients go from front to back - Male patients, withdraw foreskin before cleaning
c. Ensures that the un-cleaned skin folds are checked5. Pats the skin dry carefully with the bath towel6. Applies ointment, lotion, or powder to the patient's buttocks7. Puts a clean gown on the patient and makes the bed8. Removes the soiled materials
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
72
Ancillary Staff
Day 3 Skills
73

Day 3 Ancillary Staff Skills
Fall Prevention and Restraints Ancillary Staff Skills: Progressive Early Mobility
1. The RN will assess ability to tolerate mobilizationa. Cardiovascular: tachycardia, bradycardia, orthostatic hypotension ICU patients
may require 10 minutes to stabilize in an upright position.b. Pulmonary: shortness of breath (SOB)c. Muscular/skeleton: weakness, fatigue, strength (lower extremities equal or not)d. Paine. Neurologic status: lethargic, sedated, agitated, able to follow commandsf. Psychosocial/emotional: depression, anxietyg. Co morbidities may affect mobility: e.g. arthritis, coronary obstructive pulmonary
disease (COPD), neuropathy2. The RN will assess use of or need for assistive/functional devices such as the following,
utilize safe patient handling of supplies as necessary.a. Orthotics: e.g. prosthetics,b. Assistive devices: cane, walker, wheelchair, gait beltc. Hearing aid, eye glassesd. Gait belt, abdominal binder, helmet
3. Preparation:a. Assist patient to mobilize (unless mobility is contraindicated).b. Plan early in shift for the approximate time of mobility with the patientc. Limit the time a patient is in a single positiond. Active or Passive range of motion ROM should be performed for all patients at
least twice per shift and as needed (prn)4. Report to the nurse any concerns from the patient about mobility (pain, fear, anxiety)5. Patient preparation:
a. Assist with toileting before or place diaper if neededb. Empty drains and clamp nasogastric tube/gastric tube (NGT/GT) if possiblec. Provide clean gownd. Instruct patient on proper hand hygienee. Consider isolation needs: see Infection Control policy HS IC 002 Standard
Transmission Based Precautions and Forms Portal #10910 on ContactPrecautions.
f. Have patient wear functional devices: hearing aids, glasses.g. Prepare assistive device and place near to patient prior to mobility.h. Place brace or other supportive devices such as helmet on, if ordered.i. Dangle at bedside, assess for dizziness or lightheadedness.j. Check orthostatic blood pressures as needed. If abnormal, notify MD/designee
prior to ambulation.k. Place proper foot wear.
74

Respiratory Ancillary Staff Skills: performed under the direction and supervision of the RN
1. Chest Physiotherapya. Percussing the chest with cupped hands or percussor cups mechanically
dislodges thick, tenacious secretions from the bronchial walls.b. For patients with continuous tube feedings, feeds are stopped for the duration
of therapy then restarted afterwards.c. RN to obtain a MD/designee (house officer, nurse practitioner, physician
assistant) order which may include the frequency, duration, and target lungareas.
d. Chest percussion is performed every 4 hours or as per MD/designee’s order. Inintubated patients, chest percussion is done every 2 - 4 hours until extubation orper MD/designee’s order. In post-surgical patients begin chest percussion onpost-operative day 1 (or post-extubation, whichever comes first).
e. Percussion is performed 50-60 times per minute over each lung field for 3-5minutes.
f. During and after percussion, instruct patient to take deep breaths and cough. Ifthe patient is intubated or has an ineffective cough, consider suctioning thepatient after the chest percussion, if necessary.
g. Avoid percussion over recent surgical incision, within 2 hours after meals, andwhen a ventilator change has recently been made.
2. Deep Breathing and Coughinga. Position patient in a chair or in semi-Fowler position if in bed.b. Have patient exhale through their mouth; lips partially pursed, while contracting
abdominal muscles inward.3. Coughing
a. See Pulmonary Hygiene (Directed Cough (DC), Huff Cough (HC), & ChestPhysiotherapy (CPT) (UCLA)
b. Directed coughing aims to mimic effective, spontaneous cough in patients whoare unable to initiate cough independently.
c. Instruct the patient to take a deep breath and hold the breath. Using abdominalmuscle, cough with a single exhalation.
d. Take several relaxed breaths before the next cough effort.e. For patients who have had abdominal or thoracic surgery, instruct patients to
place hand or pillow over the incision site and apply gentle pressure whilecoughing. Caregiver may assist with incision support during coughing. Beware ofchest tubes during care to prevent dislodgement.
4. Incentive Spirometera. If tolerated, position patient sitting upright or leaning slightly forward.b. Instruct patient to exhale completely through mouth and place lips tightly
around the mouthpiece.c. Breathe in as slowly and deeply as possible maintaining a constant even
inhalation. Upon maximal inspiration, hold breath for at least 3 seconds thenexhale normally.
75

d. Repeat this technique 10 times per hour while awake. Have the patient rest andtake a few normal breaths in between exercises to prevent hyperventilation.
e. When the patient finishes with the 10 exercises, instruct the patient to take adeep breath and cough 2 to 3 times. If patient feels pain while coughing, havepatient hold a pillow or rolled-up blanket against the affected area of pain andapply pressure as they cough.
f. Refer to product guide for the minimum target inspiratory capacity.5. Oral suctioning6. Suction Canister Change
Pain Ancillary Staff Skills: 1. Pain Observation
a. The nursing assistant spends a significant amount of time with the patient andfamily, and plays an important role in pain management. When the patient or familyreports pain or pain is observed, the nursing assistant must report it to the nurse,who can evaluate the patient and revise the plan of care.
b. The nurse needs to be consulted before a nursing assistant begins any of thefollowing methods of pain relief.
i. Breathing techniquesii. Application of heat/cold
iii. Aromatherapyiv. Gentle massage (back, hand, foot)
2. The nurse may suggest that the nursing assistant help the patient and/or family withone of the following methods to treat pain as described in the plan of care. Some ofthese treatments may need instruction from the nurse before the nursing assistantbegins them.
i. Repositioningii. Distraction (pets, social support, quiet listening, laughter, reminiscing)
iii. Prayer or spiritual readingiv. Music
3. Monitoring patient with PCAa. The PCA Pump contains a specific opioid (pain medication) such as Fentanyl,
Morphine, Dialudid. The patient has the liberty to press the button to relievethemselves from pain. The patient is the ONLY one allowed to press the button.
b. These strong pain medications from the PCA pump can have severe side effects ifnot monitored properly such as:
i. Decreased Respirationsii. Low Blood Pressure
iii. Loss of Consciousnessiv. Itchingv. Difficulty urinating
vi. Deathc. Make sure to notify your RN immediately if any of these signs are noted.
76

d. Report to the RN if:i. You are having a difficult time waking patient up
ii. There are any abnormal vital signsiii. Especially if patient’s respirations are less than 10 per minuteiv. If the patient seems to be confused or acting strangely.
e. RNs can delegate vital sign frequency to the CCPs as needed.i. Starting a PCA: every 15 minutes x 4 (1 hour)
ii. Then every 2 hours x 4, then every 4 hours.
77

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
Key: Evidence-based Practice Recommendations
R= Research
N= National Practice Guideline/Protocol
L= Literature (non-Research)
E= Expert Opinion/Consensus
UCLA Department of Nursing
General Care Nursing Guidelines
EARLY AND PROGRESSIVE MOBILITY
SCOPE This guideline applies to the adult inpatient population at the Ronald Reagan UCLA Medical Center (RRUCLAMC) and Santa Monica UCLA Medical Center (SMUCLAMC) and Orthopaedic Hospital.
PATIENT GOALS/OUTCOMES I. The patient will maintain optimal function. II. The patient will have positive outcomes such as improved physical functioning,
enhanced well-being, shorter length of stay and decrease incidence of delirium. III. The patient will experience fewer complications of immobility such as venous
thrombembolism (VTE), pulmonary embolism (PE), pressure ulcer, nosocomial pneumonia, diminished quality of life, greater dependence, new institutionalization, or death R1 L1-4.
ASSESSMENT
I. Perform mobility assessment in the electronic health record (EHR)A. On admission document
i. Prehospital baselineii. Current level of mobilityiii. Consider a physical therapy (PT) evaluation for any deviation from
patient‟s pre-hospital baseline mobility status. (see Appendix B:„Criteria for PT Referral‟)
B. Every shift and as necessary i. If level of mobility declines consistently over a 2 day period,
consider obtaining an order for PT reevaluation if medically stable. ii. Obtain MD/designee (house officer, nurse practitioner, physician
assistant) order (to increase)(consider removal) activity/mobility as appropriate unless any of the following criteria are present: a. Unstable trauma with head/spine injuries or lower extremity
fractures b. Unstable neurological/muscular disorder R2
c. Active bleeding
78

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
d. Sub-therapeutic internalized normalized ratio (INR) forpatients with VTE or supratherapeutic INR >4.0, check withMD/designee E1
e. Symptomatic hypo/hypertensionf. Unstable cardiac/respiratory statusg. Presence of behavioral condition(s) which present a danger
to the patient and/or staffh. Relative Contraindications for the Intensive Care Unit (ICU)
per patient condition and unit standard L5
i. Femoral arterial/venous sheathii. Continuous Renal Replacement Therapy (CRRT)iii. Transvenous pacemakeriv. Superficially closed wounds
II. Assess ability to tolerate mobilization, consider the followingA. Cardiovascular: tachycardia, bradycardia, orthostatic hypotension ICU
patients may require 10 minutes to stabilize in an upright position L6. B. Pulmonary: shortness of breath (SOB) C. Muscular/skeleton: weakness, fatigue, strength (lower extremities equal or
not) D. Pain E. Neurologic status: lethargic, sedated, agitated, able to follow commands F. Psychosocial/emotional: depression, anxiety G. Co morbidities may affect mobility: e.g. arthritis, coronary obstructive
pulmonary disease (COPD), neuropathy
III. Assess the use of or need for assistive/functional devices such as the following,utilize safe patient handling of supplies as necessary.A. Orthotics: e.g. prosthetics, B. Assistive devices: cane, walker, wheelchair, gait belt C. Hearing aid, eye glasses D. Gait belt, abdominal binder, helmet
IV. Leaving the nursing unitA. See HS 1350 Leaving the Nursing Unit - Inpatients (Remaining on
Hospital Grounds) B. See HS 1382 Monitored Patients; Transportation of which refers to
patients taken off a monitor C. Considerations for patients leaving the ICU
i. Appropriate equipment for patient mobility off the unit.ii. Number of staff needed, length of time, unit patient flow;iii. Note: cardiac chair cannot be utilized for transport
INTERVENTIONS I. Preparation
79

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
A. Assist patient to mobilize (unless mobility is contraindicated). i. Plan early in shift for the approximate time of mobility with the
patient E 2
ii. Limit the time a patient is in a single position E 2
iii. Active or Passive range of motion ROM should be performed for allpatients at least twice per shift and as needed (prn) R3,4
B. Address any concerns from the patient about mobility (pain, fear, anxiety) i. Educate on benefits of mobilityii. Premedicate with pain med as needed
C. Patient preparation: i. Assist with toileting before or place diaper if neededii. Empty drains and clamp nasogastric tube/gastric tube (NGT/GT) if
possibleiii. Provide clean gowniv. Instruct patient on proper hand hygiene
D. Consider isolation needs: see Infection Control policy HS IC 002 Standard Transmission Based Precautions and Forms Portal #10910 on Contact Precautions E3
E. Have patient wear functional devices: hearing aids, glasses. F. Prepare assistive device and place near to patient prior to mobility. G. Place brace or other supportive devices such as helmet on, if ordered. H. Dangle at bedside, assess for dizziness or lightheadedness. I. Check orthostatic blood pressures as needed. If abnormal, notify
MD/designee prior to ambulation. J. Place proper foot wear.
II. See the Early/Progressive Mobility Algorithm (Appendix A) L7
III. Documentation and Hand offA. Document in electronic health record (EHR) B. Hand off report: Communicate patient activity order and tolerance.
PATIENT/FAMILY EDUCATION
I. Educate on benefits of mobility and complications related to immobility II. Family training on bed mobility, transfer and walking as needed
III. Address safety issues like fallsIV. Based on their learning needs, provide them with resources e.g. handouts L8
STAFF/FAMILY RESOURCES
I. Mosby Nursing Skills on UCLA Intranet A. Ambulation Aids: Measuring and Fitting B. Ambulation (Pediatric) C. Ambulation Aids: Patient Education
II. UCLA Forms Portal – search using key word “falls prevention” , “exercise,” “gaittraining”:, “rehab” will display adult and pediatric forms:
80

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
16185 Fall Prevention/Promoting Mobility: How to Transfer and Walk a Patient Using a Gait Belt https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayoutRootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view
16186 Fall Prevention/Promoting Mobility: Mobility Assessment https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayout RootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view
16187 Fall Prevention/Promoting Mobility: Walker Measurement and Gait with Front -Wheeled Walker https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayoutRootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view
16188 Fall Prevention/Promoting Mobility: Lower Extremity Strengthening Exercise Program https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayoutRootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view
Exercise (multiple forms) https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayoutRootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view i. Lower ext strengthening exercise programii. Flexed-pivot transferiii. Stand-pivot transferiv. Lower extremity passive range of motionv. Upper extremity passive range of motionvi. Bed exercise programvii. Lower extremity strengthening exercise program
Gait Training:( multiple forms) https://forms.mednet.ucla.edu/tag.118afa338346b877.render.userLayoutRootNode.uP?uP_sparam=focusedTabID&focusedTabID=66&uP_sparam=mode&mode=view
REFERENCES
KKeeyy:: RR == RReesseeaarrcchh--bbaasseedd NN == NNaattiioonnaall PPrraaccttiiccee GGuuiiddeelliinnee//PPrroottooccooll LL == LLiitteerraattuurree EE == EExxppeerrtt OOppiinniioonn//CCoonnsseennssuuss
81

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
R1 Gustafsson, U., Hausel, J., Thorell, A., Ljungqvist, O., Soop, & M. Nygren, J. (2011). Adherence to the enhanced recovery after sugery protocol and outcomes after colorectal cancer surgery. Archives of Surgery, 146(5) 571-577.
R2 Winkelman C, et al.(2012) Examining the positive effects of exercise in intubated adults in ICU: A prospective repeated measures clinical study. Intensive CritCare Nurse doi:10.1016/j.iccn.2012.02.007
R3 Zomorodi, M. Topley, D. and McAnaw, M. (2012). Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU. Critical Care Researchand Practice. Volume 2012, Article ID 964547, doi:10.1155/2012/964547
R4 Morris, P.,Goad, A., Thompson, C., Taylor,K., Harry, B., Passmore, L., Ross, A.,Anderson, L., Baker, S., Sanchez, M., Penley, L., Howard, A., Dixon, L., Leach, S., Small, R., Hite, R.D., Haponik, E. (2008).Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 36(8) DOI: 10.1097/CCM.0b013e318180b90e
L1 Schweinberger, M. & Roukis, T. (2010). Effectiveness of instituting a specific bed protocol in reducing complications associated with bed rest. Journal of Foot &Ankle Surgery, 49, 340-347.
L2 Pashikanti, L. & Von Ah, D. (2012). Impact of early mobilization protocol on the medical-surgical inpatient population. Clinical Nurse Specialist, 87-94
L3 Graf, C. (2006). Functional decline in hospitalized older adults. American Journalof Nursing, 106(1) 58-67.
L4 Blumenstein, M.S. (2007 Early ambulation after acute deep vein thrombosis: Is it safe? Journal of Pediatric Oncology Nursing, 24(6) pp 309-313
L5 Winkleman, C. (2011). Ambulating with pulmonary artery or femoral catheters in place. Critical Care Nurse;31:70-73 doi: 10.4037/ccn2011556
L6 Vollman KM (2010). Introduction to progressive mobility. Critical Care Nurse Supplement:. 30 (2) pp 3-5. ISSN: 0279-5442 PMID: 20360443 CINAHL AN: 2010630583
L7 Danos, T. Pattison, S., Eppling, J., Carbajal, CR, Block, D, D‟Gerolamo, T.(2011). Focus on rehab: A team approach: Ensuring the safety, well-being, and positive outcomes of hospitalized mobility patients. Rehab Management, retrieved from http://www.rehabpub.com/issues/articles/2011-09_03.asp
L8 Perme, C. & Chandrashekar, R. (2009). Early mobility and walking program for patients in intensive care units: creating a standard of care. AmericanAssociation of Critical Care Nurses, 18, 212-221.
82

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
E1 UCLA Anticoagulation Clinic (2012)
E2 Clinical Practice Council, Med/Surg Subgroup#2 (2012)
E3 UCLA Infection Control (2010) HS IC 002 Standard Transmission Based Precautions aand Contact Precautions on Forms Portal # 10910
E4 UCLA Physical Therapy Department (2012)
CONTACT Clinical Practice Council, Medical/Surgical Group 2 (2012); Critical Care Subgroup (2013)
KEYWORDS
Mobility, Ambulation, Physical Therapy
REVISION HISTORY
Effective Date: December 11, 2012 Review Date: November 2013 Revised Date: December 10, 2013
APPROVAL
Heidi Crooks, RN, MA Sr. Assoc. Director of Operations and Patient Care Services Chief Nursing Officer UCLA Health System
83

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
APPENDIX A
MOBILITY ALGORITHM L7
Perform Functional Screen on Admission, q Shift, and as needed (PRN) Check Activity Order Verify order/obtain order if none
Reposition q2hrs Perform range of motion (ROM) exercises
Yes No, or Bed Rest Ordered
No
Can patient sit upright with support?
Yes
Dangle at bedside for 5-10 min. TID Up to cardiac chair BID Reposition q2 hrs Obtain PT order if appropriate
No
Can patient sit upright unsupported?
Yes
Dangle at bedside for 5-10 min. three times a day (TID) Up to cardiac chair twice a day (BID) Reposition q2 hrs Obtain PT order if appropriate
Can patient transfer
No
Yes, with 1-2 person assist
Up in chair for meals Bedside commode for toileting If needed contact Lift Team or use assistive device Obtain PT order if appropriate
No
Can patient ambulate?
Yes Ambulate with assistance or assistive device
84

EARLY AND PROGRESSIVE MOBILITY Nur-HS G1030
UCLA Department of Nursing General Care Nursing Guidelines
APPENDIX B: Criteria for PT Referral E4
Routine Referral
Request Urgent Referral if
1. Patient‟s functional ability has declined from baseline (i.e. bed mobility, transfers,ambulation)
2. AND and patient is medically stable
3. Patient requires family/caregiver training for assistance with transfers, mobility,positioning, range of motion and/or use of new assistive deviceAND/OR use of new assistive device
4. Particular diagnosis or condition calls for a PT evaluation
Patient awaiting PT consult for immediate DC from the inpatient setting
85

CONSTANT OBSERVATION REQUEST FORM & ALGORITHM Directions: This request form must be completed and sent to the staffing office by 4:00AM/PM - The algorithm must be completed every shift! - Must check a box under each step - Reassess safety needs and interventions every shift! - Must assess for metabolic/organic/physiological causes every shift!
UCLA Form #165030 Rev. (10/14) Page 1 of 1
STEP 1 5150 or 5250 Psych Hold (gravely disabled may be excluded) Recommended by Psych Child on Hospital Hold/Munchausen by proxy
YES Clinical Care Partner
NO
STEP 2 Self-discontinuation on lines, tubes, drains Agitation/high potential for injury to self Behavioral Restraints NO
No further action needed.
YES
STEP 3 Family available for constant observation No Yes
Family assessed and education to safety plan for patient.
STEP 4 Family agreed to provide private duty nurse No Yes
Send Family to Admissions Office
STEP 5
Would a Nursing Volunteer be appropriate? No Yes
Nursing Volunteer available in the unit? Yes Assign Nursing Volunteer. No Go to STEP 6
STEP 6 Try all Restraint Alternatives (per restraint policy) Restraint Alternatives effective? No Yes
Continue Restraint Alternatives
STEP 7
Use Restraints: No
Reason: ______________________________________ Yes
Follow Restraint Policy – Restraint Effective? Yes – Continue with Restraint Policy No
STEP 8
Restraint ineffectiveness due to: Increased agitation Lines pulled Injury to self Other: __________________________
Primary Organic/Metabolic Etiology: Encephalopathy Delirium tremens Steroid induced psychoses Psychoses Narcotic/Anesthetic side effects Other: _____________________
STEP 9
The Charge Nurse will make the final determination of the need for constant observation based on the Constant Observation algorithm (must be done every shift).
Patient Label/Patient Info:
Charge Nurse: X Unit: Nursing Volunteer Used? (YES)
Float Team CCP Used? (YES) Unit Based CCP Used? (YES)
DAY or NIGHT Shift:
86

CONSTANT OBSERVATION AIDE
UCLA Form #10407 Rev. (10/10) Page 1 of 4
Instructions: The primary RN will highlight the condition that relates to her/his pt and review information with the Constant Observation Aide. The Constant Observation Aide will implement the recommended intervention and check those interventions that the pt responds to best. These interventions will be communicated to the primary RN and the oncoming Constant Observation Aide to promote continuity of care and optimize pt outcome. The Constant Observation Aide should report any changes in pt condition to primary RN.
CARING FOR THE PATIENT WITHDRAWING FROM SUBSTANCE ABUSE: Observe for the following behaviors: Report any changes to RN. 1. Restlessness/ irritability/anxiety/agitation2. Nausea/vomiting3. Elevated temperature/ B/P & pulse/Insomnia/nightmares4. Impaired concentration/memory & judgment/ increased sensitivity to noise/Paranoid
Delusions/Hallucinations (auditory, visual, or tactile)/Delirium (disorientation to time,place and/or situation)
5. Grand mal seizuresGoal for treatment: Increase the patient’s comfort, decrease the risk of seizures and delirium and keep the patient safe. Therapeutic Interventions:
1. Really listen / Make good eye contact, be empathic and supportive e.g.” How difficultthat must be”, “I understand” “Sounds like you have a lot to deal with”
2. Demonstrate acceptance and genuine interest / Do not give advice or bedisapproving/ be aware of any prejudices or stereotypes you may have
3. Check every shift and after visitors for contraband (sharps, drugs, alcohol) and Referto General Therapeutic Interventions on CCP Assignment & DocumentationSheet).
CARING FOR THE AGITATED PATIENT: Observe for the following behaviors: Signs of increasing agitation:
1. Restlessness/ Irritability that does not respond to reassurance, redirection, ordistraction
2. Anxiety/ Fear/ Poor judgment/Anger/3. Verbal threats/Yelling/and/or Combativeness (hitting, pinching, kicking).4. If any of these behaviors occur notify your RN.
Therapeutic Interventions: (Also refer to General Therapeutic Interventions on CCP Assignment & Documentation Sheet )
1. Know your patient / Intervene early2. Ask them about their family, work, interests/Focus on the patient not the task3. Get the person’s attention, make eye contact, and speak directly to the person4. Tell the patient what you are planning before performing the task5. Keep directions simple, clear and one step at a time6. Speak slowly especially if you have an accent7. Give them tasks easily accomplished so they may feel successful8. Supervise and prompt with ADL’s9. Realize their need for humor, dignity, privacy, and socialization10. Really listen to what they are saying and do not interrupt
87

UCLA Form #10407 Rev. (10/10) Page 2 of 4
11. If your patient becomes frustrated decrease your demands and give a breaka. Do not take their anger personallyb. Do not get into a power strugglec. Don’t shout, confront, try to reason, argue or touch an agitated patientd. Give them space while attempting to reassuree. Be aware of the danger for yourself and the patientf. If they calm down, ask the RN if you can walk them or move them to chair/
Use music, books and magazines to provide meaningful activities.12. Demonstrate acceptance and genuine interest—compliment them / help them to see
you are an ally13. Tell them in calm, reassuring tone who you are and what your role is and ask, “How
can I help?”/ Ask if they have pain, offer snacks, offer bathroom every 2-3 hours14. Remind them they are in the hospital and they will be safe15. Decrease environmental stimuli (if noisy in the hall, close the door).
CARING FOR THE SUICIDAL PATIENT: Take all threats of suicide seriously! Observe for the following behaviors:
1. Expressing thoughts of suicide2. Describing a plan to injure or kill self3. Conversation that centers around death4. Increased energy5. Talking about giving away possessions6. Refusing medical care7. Attempting to conceal harmful objects
Therapeutic Interventions: 1. Provide safe environment2. Patient is on a strict I:I and must be in vision of the CCP at all times (door must be
partially open when patient in Bathroom)3. Check environment every shift and after visitors for harmful objects or personal
medications, if found remove from immediate environment and inform RN4. Communicate caring and concern5. Encourage patient to talk about their feelings—do not give advice or judge6. Offer meaningful activities such as music, cards, books or magazines.7. Refer to General Therapeutic Interventions on CCP Assignment and
Documentation Sheet.
CARING FOR THE PATIENT WITH SCHIZOPHRENIA: Core problems: Anxiety, Depression, Difficulty expressing needs, Inability to learn from Experience. Observe for the following behaviors:
1. Auditory Hallucinations: voices talking about the patient, commands that tell thepatient to do something harmful or dangerous.
2. Visual Hallucinations: Visions can be terrifying or pleasant.3. Delusions: Believing that someone is trying to harm them, steal from them.4. Agitation.
Therapeutic Interventions: (Also refer to General Therapeutic Interventions) 1. Each shift search area for sharps, glass, personal medication or weapons2. If you are anxious or frightened the patient will be anxious and frightened3. Establish a trusting relationship/ Be patient, show acceptance and actively listen4. Do not argue with the patient about differences in perceptions
88
UCLA Form #10407 Rev. (10/10) Page 3 of 4
5. When hallucinations occur, do not leave the patient alone6. Respond to the patient’s underlying feelings rather than the illogical nature of the
delusion, “ you seem anxious (fearful, angry) can you talk about it?” 7. Do not agree with delusions / Do not attempt a logical explanation8. If you feel they are responding to “internal stimuli”, you can ask. “Are you hearing
voices—what are they telling you”, “I do not hear them, but I know you do”, reassure“You will be safe here in the hospital”
9. Set firm limits on dangerous or aggressive behavior, in a calm, but firm tone, holdingup your hand, “ You must stop that behavior“
89

UCLA Form #10407 Rev. (10/10) Page 4 of 4
CLINICAL CARE PARTNER ASSIGNMENT AND DOCUMENTATION SHEET DATE: (Use form for shift report and return to RN before you leave unit)
NOTIFY THE R.N. IMMEDIATELY FOR THE FOLLOWING VITAL SIGNS SYSTOLIC B/P : more than ____ or less than ____ or DIASTOLIC B/P : more than _____ or less than _____, PULSE: more than ____ less than -
_____ TEMP: more than _____
RN: Discuss any special needs with Clinical Care Partner
ASSIGNED STAFF:____________________________/ ____________________________PATIENT______________________Room #__________ CCP RN
Reason for sitter: ____________________________ _________IMPAIRMENTS: N/A Vision Hearing Communication___________________ Medical Psychiatric
FUNCTIONAL STATUS (ADL’s): (I) Independent (A) Assist (D) Dependent: Bathing _____Dressing, ____Toileting _____(if A or D offer toileting every 2-3 hours), Transfer ______________ Ambulation___________Ambulate every__________ Walker Cane Continent Incontinent Special Diet____________ Fall Risk: Y N Restraints: Y N Assess and document per policy/Guideline
Dentures__________ Hearing Aid(s)_______Glasses_________ SKIN INTEGRITY: good fair poor N/A Area of skin breakdown _________________ Interventions: N/A __________________________ SCHEDULED TESTS (inform patient of test and time)_______________________________________________ PATIENT SPECIAL NEEDS: _______________________________________ _____________________________________________________________________________________________________________________________________ Suicidal Patients: Do not leave the patient at anytime/patient must always be in your vision CCP CHECK DURING EVERY SHIFT: PT.WRISTBAND ON: Always use two identifiers Safe environment check: Remove anything the patient could harm themselves with e.g. mirrors, glass, weapons, tourniquet, razor, personal medications and give to the RN PATIENT BELONGINGS LABELED: Check that Hearing aids, dentures and glasses are in place MANAGE ENVIRONMENT: Keep free of clutter, keep noise to a minimum and be aware of safety issues. CCP OBSERVE & DOCUMENT DURING SHIFT: B/P, Pulse, Temp, RR, UOP, and BM. Report to RN any change in pt’s condition. Effective Interventions: _______________________________________
GENERAL THERAPEUTIC INTERVENTIONS: 1. Know your patient and what they are able to do2. Introduce yourself and explain your role / Sit near the patient3. Assist with meals PRN/ Offer snacks4. Encourage meaningful activities (e.g. cards, magazines, books, newspaper, music)/engage in meaningful conversation e.g.: Ask them about themselves, their
family, their work, and hobbies5. Actively listen with good eye contact, be empathic and supportive: “I understand”, “How frustrating for you”, “How difficult that must be”, “I see, go on”6. Demonstrate an attitude of acceptance, tolerance and genuine interest7. Compliment and offer genuine praise/ understand their losses and how it affects them8. Recognize their need for humor, dignity and socialization9. Do not give advice10. CHOOSE BATTLES WISELY/ DON’T GET INTO POWER STRUGGLES/ DON’T TAKE THINGS PERSONALLY (if they are angry, try to
understand the cause of their anger)11. Be aware of your non-verbal behavior: facial expressions, arms folded, hands on hips12. Provide limit setting that is firm but not punitive.
90

Restraints (UCLA)
Quicksheet
1. Describes indications for restraint use per RestraintPolicy.
2. Describes differences between medical surgicalrestraint and behavioral restraint and appropriate order sets for each.
3. States type of restraints (medical surgical vsbehavioral) as it relates to agitation scale.
4. Describes components of a physician’s order and ofphysician documentation.
5. Describes the process of advisement to patient andfamily required by policy.
6. Describes restraint alternatives (physiologic,psychologic considerations and environmental modifications) and least restrictive interventions to be attempted prior to restraint application.
7. Describes conditions in which Side Rails would beconsidered a “Restraint” and potential risks associated with bed rail entrapment.
8. Describes required nursing observation, monitoringand documentation per policy for med/surgical and behavioral restraints.
a) Medical Surgical Restraints: Q2 hours, check signsof injury, LOC, circulation, sensory and motor, release (CSM); Release with ROM, position change, hygiene, elimination, hydration, nutrition, and reassessment of need to continue restraints. b) Behavioral Restraints: Continuous Observation
of patient with Q15 minute documentation of safety checks, signs of injury, LOC, CSM; and Q2 hour documentation of release, ROM, reassessment, hygiene, elimination, hydration, nutrition, position change; and need to continue restraints
91

9. States when MD initial and continuation orders:• Medical Surgical - each calendar day;• Behavioral – patient must be evaluated by MD
within 1 hour of restraint application;thereafter, every 4 hrs adults; every 2 hrs for 9-17 yrs; every 1 hr for < 9 yrs).
10. Discusses the individualized plan of care (based onRestraint Guideline for Care) for patients in restraints and where to document in Notes section of CareConnect.
11. States special precautions for pregnant patientsgreater than 20 weeks gestation.
12. States conditions for Reporting of Restraint PatientDeaths.
13. Removes restraints Q2 hours for ROM, hydration,toileting, turning, protective skin care measures (e.g., placement of soft-care mattress, elbow/heel protectors, sheepskin, etc.).
14. Demonstrates correct application of med/surgrestraints (vest, soft restraints, using a “slip” knot to non-moveable part of bed.
15. Describes the process for admitting a patient from theER in Hard Leather Restraints
a. Locked Hard Restraints (that require keys)are NOT to be used in the inpatient setting – They must be replaced with Tuff Cuff Quick Release restraints when admitted to the floor.
b. Order “Tuff Cuffs” (blue for wrists) and (redfor ankle) from CENTRAL SUPPLY
c. Have Tuff Cuffs available at bedside whenpatient arrives from ER.
d. Security officer(s) will escort the Patient to theinpatient unit from the ER and assist the RN in replacing the “Locked” Hard Restraints with the “Tuff Cuff” Quick Release type restraints
92

e. Attaches “quick release” buckles to non-moveable part of bed (Tuff Cuff restraints (blue – wrists; red-ankles)
f. Ensures quick release Tuff Cuff restraints aresecure prior to security officer leaving the nursing unit.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
93

Pulmonary Hygiene (Directed Cough (DC), Huff Cough (HC), & Chest Physiotherapy (CPT) (UCLA)
Quicksheet
KEY ELEMENTS MET 1. Verbalizes knowledge on when to avoid percussion (i.e. over recentsurgical incision, recent ventilator setting changes and within 2hrs of meal consumption) 2. Receives orders to perform DC, HC and or CPT (Orders state:frequency, duration and target lung areas) 3. Assesses for Pain. If pain present, administers appropriate medication.4. Gathers the necessary equipment.(i.e. handheld percussion device,pillows, oral care supplies) 5. Confirms oral suction set up available and ready for use6. Explains the procedure to the patient and family7. If patient has nasogastric/gastric tube feeds, stops feeding for duration oftherapy 8. Washes hands and dons gloves9. Positions patient appropriately (i.e. upright-sitting at edge of bed orlaterally if pt is unable to sit up) 10. CPT:
-Following positioning: If using percussion device, displaces gown or clothing so that areas to be percussed are bare. If using cupped hands or if skin is compromised, covers areas to be percussed with gown or towel. -Percusses 50-60 times/min over the lungs target area for 3-5 minutes. If dyspnea occurs, stop, and notify MD and/or RN.
After therapy: Instructs patient to deep breath and cough to attempt to clear secretions. If patient is intubated the secretions are suctioned 11. Directed Cough:
Instructs patient to take a deep breath, then hold the breath, using abdominal muscles to force air against a closed glottis
Instructs the patient to cough two to three times during exhalation, contracting abdominal muscles inward
Instructs patient to take several relaxed breaths before the next cough effort 12. Huff Cough (for patients with history of lung disease):
94

-Places patient in high fowler position;
-Teaches patient to place palms of hands on rib cage
-Instructs the patient to take a slow, deep breath, hold it for 2 seconds, contract expiratory muscles, open mouth and say “HUFF” several times while exhaling.
Instructs patient to take several relaxed breaths before the next cough effort.
13. Provides oral hygiene after any type of pulmonary hygiene.
14. Documents in EHR : date/time of type of pulmonary physiotherapy,sputum color, amount, odor, viscosity of secretions, presence or absence of blood, side effects and patient’s tolerance of treatment.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
95

Suction Canister Change (UCLA)
Quicksheet
1. Use universal precautions in all contact with body fluids.2. Change suction container PRN or 72 hours.3. Remove suction container from wall vacuum source.4. Empty fluid in waste disposal site.5. Dispose container in dirty trash container.
6. Remove eye protectors, mask and gloves.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
96

UAP (Unlicensed Assistive Personnel) Pain Management (UCLA)
Quicksheet
1. Define pain.2. Utilize a pain intensity measurement tool appropriate to age and cognitive status (i.e., 0-10rating scale, smiley faces). 3. Determine level of pain:
No pain = 0 Mild 1 – 3 Moderate 4 – 6 Severe 7 – 10
Report to RN greater or equal to 4 (moderate pain and severe pain). 4. Ask about pain with:
• Vital Signs• Activity• Ambulating• Pre-Procedure• Post-Procedure
5. Recognize and inform R.N. on patient controlled analgesia pump.• Pump alarms• Leaking or disconnected tubing• Red and swollen I.V. site• Patient complains of pain at I.V. site
6. Recognize and inform R.N. on Epidural Analgesia pump.• Pump alarms• Leaking or disconnected tubing• Loose or soiled back dressing• Patient complains of pain and back discomfort
7. Document pain scale on vital signs flow sheet in EHR.
This content has been modified from its original form by the customer. Original material Copyright © 2006 - 2015 Elsevier Inc. All Rights Reserved.
97