andrew d. schweitzer, md 1 jaspal r. singh, md 2 j. levi chazen, md 1 depts of radiology 1 and...
TRANSCRIPT

Andrew D. Schweitzer, MD1
Jaspal R. Singh, MD2
J. Levi Chazen, MD1
Depts of Radiology1 and Rehabilitation Medicine2
New York Presbyterian Hospital
Weill Cornell Medical Center
New York, NY
PERCUTANEOUS CT-GUIDED FACET JOINT SYNOVIAL CYST RUPTURE: SUCCESS WITH
REFRACTORY CASES AND TECHNICAL CONSIDERATIONS

DISCLOSURES
• ADS has no disclosures
• JRS is a consultant for Kimberly Clark and Physicians Pharmaceutical Solutions
• JLC has no disclosures

INTRODUCTION• Lumbar facet joint synovial cysts are an important
cause of low back pain• Occur at degenerated facet joints
• Percutaneous rupture of synovial cysts has been correlated with avoiding subsequent surgery in half of treated patients1
• In a series of 101 patients, in 19% of cases, cyst rupture could not be confirmed fluoroscopically1
1. Martha et al, The Spine Journal, 2009.

PURPOSE
• We describe the technique for CT-guided lumbar facet synovial cyst rupture with emphasis on technical considerations for success in refractory cases

PATIENTS• 11 consecutive patients with symptomatic
lumbar facet synovial cysts referred for percutaneous rupture
• 7 male, 4 female
• 5 were directly referred
• 6 had prior fluoroscopy-guided cyst drainage and/or rupture• None of the 6 had any relief with
fluoroscopy-guided intervention
• In one, facet joint could not be accessed under fluoroscopic guidance due to extensive osteophyte formation
Above: unsuccessful fluoroscopy-guided aspiration
Below: inability to access joint under fluoroscopy guidance due to extensive osteophytes
PATIENTS
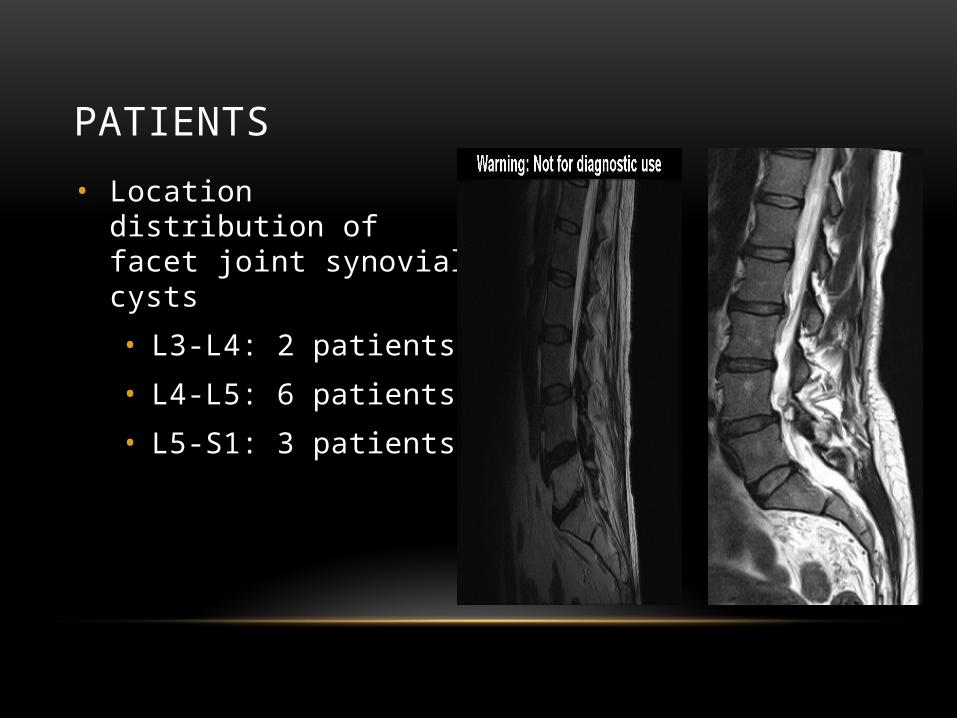
• Location distribution of facet joint synovial cysts
• L3-L4: 2 patients
• L4-L5: 6 patients
• L5-S1: 3 patients
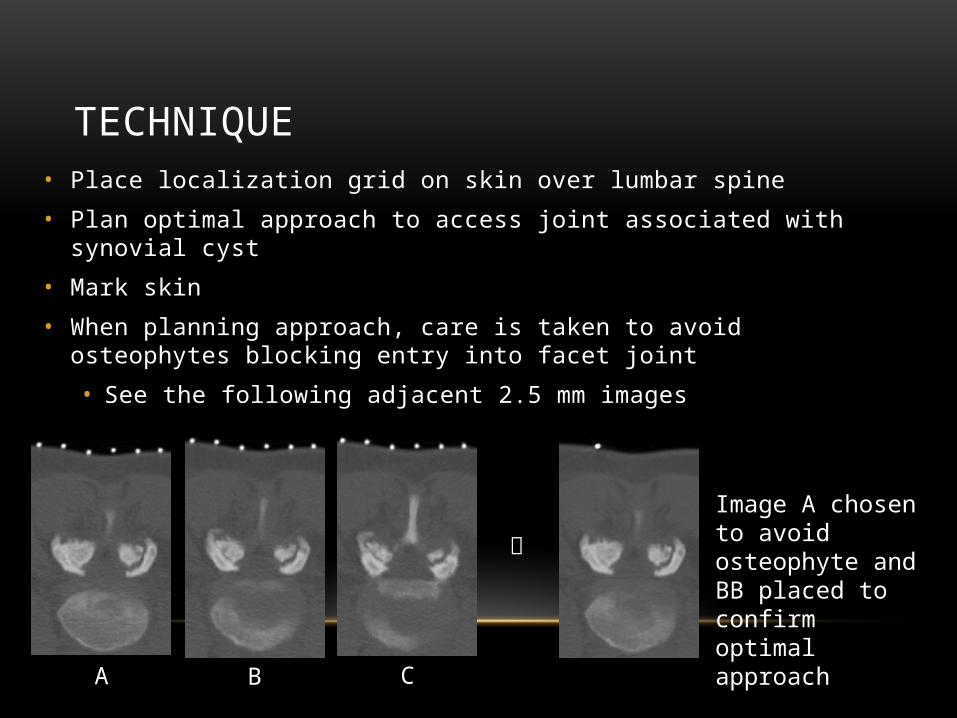
TECHNIQUE• Place localization grid on skin over lumbar spine
• Plan optimal approach to access joint associated with synovial cyst
• Mark skin
• When planning approach, care is taken to avoid osteophytes blocking entry into facet joint
• See the following adjacent 2.5 mm images
A B C
Image A chosen to avoid osteophyte and BB placed to confirm optimal approach

TECHNIQUE• Perform sterile preparation
• Administer moderate sedation (the process of cyst rupture usually exacerbates pain significantly)
• Anesthetize skin with 1% buffered lidocaine
• Under serial CT guidance, advance 22 gauge spinal needle into degenerated facet joint associated with the cyst
• Use bevel of spinal needle to guide direction and to get past osteophytes into joint capsule
Bevel directed laterally to get past osteophyte
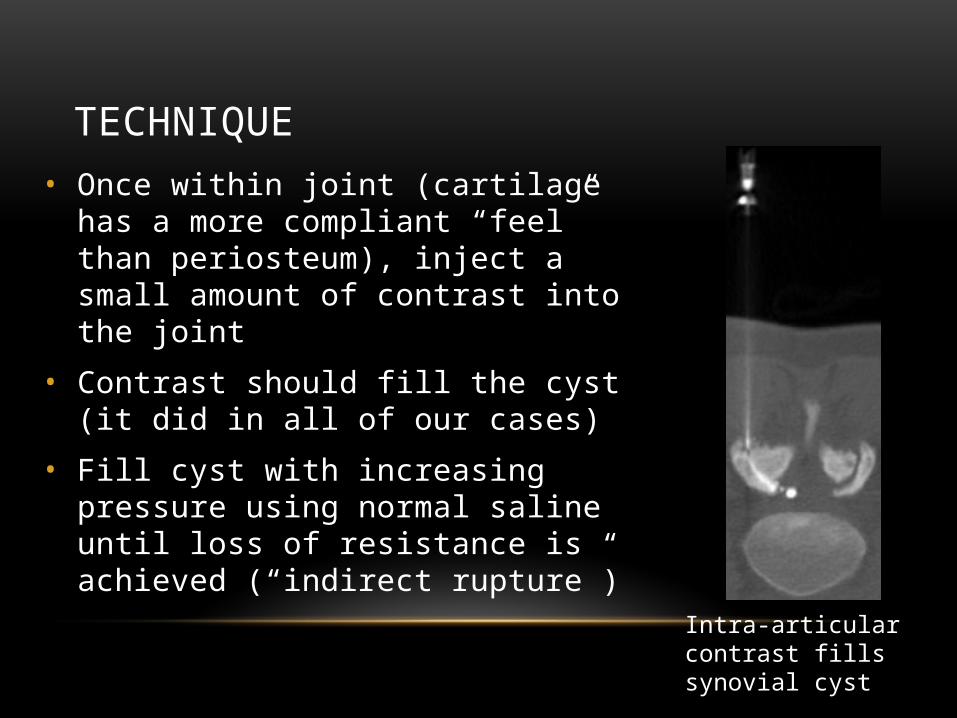
TECHNIQUE• Once within joint (cartilage has a more
compliant “feel” than periosteum), inject a small amount of contrast into the joint
• Contrast should fill the cyst (it did in all of our cases)
• Fill cyst with increasing pressure using normal saline until loss of resistance is achieved (“indirect rupture”)
Intra-articular contrast fills synovial cyst

TECHNIQUE• After CT confirmation of successful rupture,
inject steroid and local anesthetic mixture into joint• Some of steroid/anesthetic mixture will enter into
epidural space via new defect in synovial cyst
• In some cases, steroid/anesthetic mixture was administered directly into epidural space and/or transforaminally along exiting nerve root
Epidural contrast confirms rupture
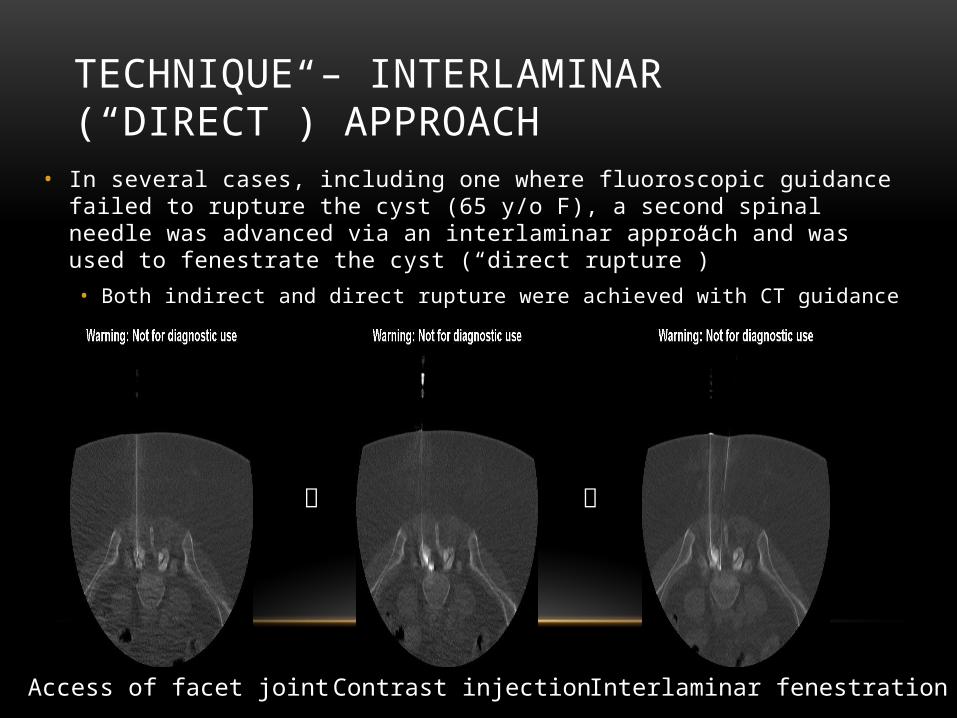
TECHNIQUE – INTERLAMINAR (“DIRECT”) APPROACH
• In several cases, including one where fluoroscopic guidance failed to rupture the cyst (65 y/o F), a second spinal needle was advanced via an interlaminar approach and was used to fenestrate the cyst (“direct rupture”) • Both indirect and direct rupture were achieved with CT guidance
Access of facet joint Contrast injection Interlaminar fenestration

RESULTS
• 10 of 11 patients underwent successful synovial cyst rupture confirmed by CT showing loss of cyst contour and dilute contrast in surrounding epidural space• One patient’s cyst could not be indirectly ruptured due to limited
access to facet joint from iliac crest • Interlaminar fenestration and cyst aspiration was performed in this
case and patient’s symptoms improved

RESULTS
• Clinical follow-up was available for 9 of 11 patients• Follow-up times ranged from 1.5 to 17 mo
• Among the 9 patients with clinical follow-up:• 7 (78 %) experienced significant relief or resolution of pain
• One of these patients had recurrent pain 5 mo after cyst rupture
• 2 (22%) did not experience significant symptom relief
• 5 of 6 patients with no relief after fluoroscopic procedures had symptom relief after the CT-guided rupture

RESULTS – CYST RESOLUTION
• One patient with cyst rupture and interlaminar fenestration had follow-up MRI showing resolution of synovial cyst
• Most patients did not have follow-up MRI as symptoms improved
1.5 mo later

SUMMARY OF TECHNICAL TIPS FOR SUCCESS IN REFRACTORY CASES
• CT provides much better anatomic detail than fluoroscopy for:
• Delineating barriers to joint access such as osteophytes
• Confirmation of intra-articular location
• Confirmation of cyst rupture
• Use bevel to direct needle into joint capsule
• Use moderate sedation so that patient can tolerate distention of cyst that occurs prior to rupture
• Significant hydrostatic pressure can be required to achieve rupture
• A smaller syringe filled with saline may be helpful
• Interlaminar fenestration (“direct rupture”) can be performed after cyst is filled with contrast
• Particularly in cases where cyst rupture cannot be achieved

CONCLUSION
• In cases refractory to fluoroscopy-guided drainage/rupture:
• CT-guided lumbar facet synovial cyst rupture can be successful both technically and in terms of symptom relief
THANK YOU