anesthesia and cpr
TRANSCRIPT

Anesthesia and Cardio-Pulmonary Resuscitation
Lecture 1
Department Anesthesiology and Intensive Care
The head of a department: I.Titov, DrPh.

The themes of practical training
1. Cardiopulmonary resuscitation. Symptoms of clinical death. Safar’s triple manoeuvre. Breathing.
2. Cardiopulmonary resuscitation. Chest compression. Complications of the CPR.
3. Anesthesia. Local anesthesia.
4. Anesthesia. General anesthesia.

Part I: Anesthesia
The word is derived from the Greek words an, which means “without” and aithesia which means “feeling”
The use of medical anesthesia was first reported in 1846
The development of anesthesia has made today’s modern surgical techniques possible

History of Anesthesia
1771-Karl Scheel & Joseph Priestly
- discovery of O2
1772-Joseph Priestly - discovery of N2O

History of Anesthesia


1846-Dr. William T.G. Morton First anesthesia specialist Oct. 16, 1846 - Ether Day
at Harvard Medical School
Oliver Wendell Holmes suggested the name
"Anesthesia"

History of anesthesia
Ether synthesized in 1540 by CordusEther used as anesthetic in 1842 by Dr.
Crawford W. LongEther publicized as anesthetic in 1846 by
Dr. William MortonChloroform used as anesthetic in 1853 by
Dr. John Snow
History of anesthesia
Endotracheal tube discovered in 1878Local anesthesia with cocaine in 1885Thiopental first used in 1934Curare first used in 1942 - opened the
“Age of Anesthesia”

History of anesthesia


Part I: Anesthesia
All methods of anesthesia divides into two large groups:
local Elimination of painful sensation from a specific part of the body
without loss of consciousness
general Drug-induced depression of CNS to prevent all perception of
sensation during a procedure or surgery
Part I: Anesthesia. Local anesthesia.
Local anesthesia: topical block local infiltrationnerve block – intercostal anesthesia, brachial
plexus blocks, peripheral nerve block of the arm, etc.
spinal anesthesiaepidural anesthesia caudal anesthesia

Part I: Anesthesia. Local anesthesia.
A local anesthetic is an agent that interrupts pain impulses in a specific region of the body without a loss of patient consciousness.
Normally, the process is completely reversible -- the agent does not produce any residual effect on the nerve fiber.
Cocaine
South American Indians used to induce euphoria, reduce hunger, and increase work tolerance in sixth century

Part I: Anesthesia. Local anesthesia.
The first local anesthetic was Cocaine which was isolated from coca leaves by Albert Niemann in Germany in the 1860s.
The very first clinical use of Cocaine was in 1884 by Sigmund Freud who used it to wean a patient from morphine addiction. It was Freud and his colleague Karl Kollar who first noticed its anesthetic effect.
Kollar first introduced it to clinical ophthalmology as a topical ocular anesthetic. Also in 1884, Dr. William Stewart Halsted was the first to describe the injection of cocaine into a sensory nerve trunk to create surgical anesthesia.
Cocaine remains popular in medicine today, but only as a topical anesthetic, because of its unique vasoconstrictive properties.

Part I: Anesthesia. Local anesthesia.
All local anesthetics are weak bases, classified as tertiary amines.
Typical structure of local Anesthetic Molecule

Part I: Anesthesia. Local anesthesia.


Part I: Anesthesia. Local anesthesia.
Ester Amide
CocaineProcaine (Novocaine) (1905)
Benzocaine (1900)
Tetracaine (1930)
Chloroprocaine (1952)
Lidocaine (Xylocaine) (1944)
Mepivacaine (1957)
Prilocaine (1960)
Bupivacaine (1963)
Ropivacaine (1995)

Part I: Anesthesia. Local anesthesia.
Esters are hydrolyzed in plasma by pseudo-cholinesterase. One of the by-products of metabolism is paraaminobenzoic acid, the common cause of allergic reactions seen with these agents.
Amides are metabolized in the liver to inactive agents. True allergic reactions are rare.

Part I: Anesthesia. Local anesthesia.
Local anesthetics work to block nerve conduction by reducing the influx of sodium ions into the nerve cytoplasm.
Sodium ions cannot flow into the neuron, thus the potassium ions cannot flow out, thereby inhibiting the depolarization of the nerve.
If this process can be inhibited for just a few Nodes of Ranvier along the way, then nerve impulses generated downstream from the blocked nodes cannot propagate to the ganglion.

Part I: Anesthesia. Local anesthesia.Topical anesthesia.
Cream “EMLA”
10% lidocaine solution

Part I: Anesthesia. Local anesthesia.
Injection of local anesthetic around a peripheral nerve
Can be used for anesthesia during surgery or for post-op pain relief
Examples: ankle block for foot surgery, supraclavicular block for post-operative pain control after shoulder surgery

Part I: Anesthesia. Local anesthesia.
Spinal anesthesia.

Part I: Anesthesia. Local anesthesia.
A local anesthetic agent (lidocaine or bupivacaine) is injected into the subarachnoid space- Spinal anesthesia is also known as a subarachnoid block
Blocks sensory and motor nerves, producing loss of sensation and temporary paralysis

Part I: Anesthesia. Local anesthesia.
Possible Complications of Spinal Anesthesia Hypotension Post-dural puncture headache (“Spinal
headache”) caused by leakage of spinal fluid through the puncture hole in the dura - can be treated by blood patch
“High Spinal”- can cause temporary paralysis of respiratory muscles. Patient will need ventilatory support until block wears off

Part I: Anesthesia. Local anesthesia. Epidural anesthesia.
Local anesthetic agent is injected through an intervertebral space into the epidural space.
May be administered as a one-time dose, or as a continuous epidural, with a catheter inserted into the epidural space to administer anesthetic drug
Part I: Anesthesia. Local anesthesia. Systemic toxicity.
Adverse effects of local anestheticsAllergic reactions
Mild or severeSystemic toxicity
Most often due to accidental intravascular injection
Lightheadedness, visual changes, muscular twitching, seizures, coma,
Arrhythmias, cardiac depression

Part I: Anesthesia. Local anesthesia. Systemic toxicity.
Essentially all systemic toxic reactions associated with local anesthetics are the result of over-dosage leading to high blood levels of the agent given. Therefore, to avoid a systemic toxic reaction to a local anesthetic, the smallest amount of the most dilute solution that effectively blocks pain should be administered.

Part I: Anesthesia. General anesthesia
General anesthesia (narcosis)
Inhalation A. Noninhalation
Intravenous (IV)
Intramuscular (IM)
Rectal Oral

Part I: Anesthesia. General anesthesia
Effects of general anesthesia:
1. Hypnosis (sleep) and Amnesia
2. Analgesia
3. Loss of reflexes
4. Muscle relaxation
5. Neurovegetative protection Effects produced by depression of the
CNS & blocking pain stimuli at the level of the cerebral cortex

Perioperative — begins with decision to have surgery, lasts until patient is transferred to operating room
Intraoperative — extends from admission to surgical department to transfer to recovery room
Postoperative — lasts from admission to recovery room to complete recovery from surgery
Three Phases of Perioperative Period

Part I: Anesthesia. General anesthesiaThe stages of anesthesia
Preparation: physical examanation (Informed Consent Information)
premedicationAnesthesia: Stages of anesthesia Induction — from administration of anesthesia to
ready for incision Maintenance — from incision to near completion
of procedure Emergence — starts when patient emerges from
anesthesia and is ready to leave operating room

Informed Consent Information Description of procedure and alternative
therapies Underlying disease process and its natural
course Name and qualifications of person performing
procedure Explanation of risks and how often they occur Explanation that patient has the right to refuse
treatment or withdraw consent

Part I: Anesthesia. General anesthesia
Anesthesia Monitoring Devices:Electrocardiograph (EKG or ECG)Pulse oximeter (SpO2 and HR)
Blood pressure monitor Temperature probe

Part I: Anesthesia. General anesthesiaInhalation Anesthesia. Effects of general anesthesia:
1. Analgesia
2. Hypnosis (sleep)
and Amnesia
3. Loss of reflexes
4. Muscle relaxation
5. Neurovegetative protection
Nitrous Oxide
Halothane
Isoflurane
Desflurane
Sevoflurane
Enflurane

Part I: Anesthesia. Inhalation Anesthesia.Nitrous Oxide Prepared by Priestly in 1776 Anesthetic properties described by Davy in 1799 Characterized by inert nature with minimal metabolism Colorless, odorless, tasteless, and does not burn Simple linear compound Not metabolized Only anesthetic agent that is inorganic Major difference is low potency MAC value is 105% Weak anesthetic, powerful analgesic Needs other agents for surgical anesthesia Low blood solubility (quick recovery)

Part I: Anesthesia. Inhalation Anesthesia.
Nitrous Oxide Minimal effects on heart rate and blood pressure May cause myocardial depression in sick
patients Little effect on respiration Safe, efficacious agent Manufacturing impurities toxic Hypoxic mixtures can be used Large volumes of gases can be used Beginning of case: second gas effect End of case: diffusion hypoxia
Part I: Anesthesia. Inhalation Anesthesia.Halothane Synthesized in 1956 by Suckling Halogen substituted ethane Volatile liquid easily vaporized, stable, and nonflammable Most potent inhalational anesthetic MAC of 0.75% Efficacious in depressing consciousness Very soluble in blood and adipose Prolonged emergence Inhibits sympathetic response to painful stimuli Inhibits sympathetic driven baroreflex response (hypovolemia) Sensitizes myocardium to effects of exogenous catecholamines-- ventricular
arrhythmias Decreases respiratory drive-- central response to CO2 and peripheral to O2
Respirations shallow-- atelectasis Depresses protective airway reflexes
Depresses myocardium-- lowers BP and slows conduction Mild peripheral vasodilation

Part I: Anesthesia. Inhalation Anesthesia.Halothane Side Effects “Halothane Hepatitis” -- 1/10,000 cases
fever, jaundice, hepatic necrosis, death metabolic breakdown products are hapten-protein conjugates immunologically mediated assault exposure dependent
Malignant Hyperthermia-- 1/60,000 with succinylcholine to 1/260,000 without halothane in 60%, succinylcholine in 77%
Classic-- rapid rise in body temperature, muscle rigidity, tachycardia, rhabdomyolysis, acidosis, hyperkalemia, DIC most common masseter rigidity family history

Part I: Anesthesia. Inhalation Anesthesia. Malignant Hyperthermia (continued)
high association with muscle disorders autosomal dominant inheritance diagnosis--previous symptoms, increase CO2, rise in
CPK levels, myoglobinuria, muscle biopsy physiology--hypermetabolic state by inhibition of
calcium reuptake in sarcoplasmic reticulum treatment--early detection, d/c agents, hyperventilate,
bicarb, IV dantrolene (2.5 mg/kg), ice packs/cooling blankets, lasix/mannitol/fluids. ICU monitoring
Susceptible patients-- preop with IV dantrolene, keep away inhalational agents and succinylcholine

Part I: Anesthesia. General anesthesiaIntravenous Anesthesia. Effects of general anesthesia:
1. Analgesia
2. Hypnosis (sleep)
and Amnesia
3. Loss of reflexes
4. Muscle relaxation
5. Neurovegetative protection
Narcotic agonists
Ketamine
Thiopental
Propofol Diazepam
Etomidate Midazolam
Muscle RelaxantsDepolarizing – Succinylcholine
Nondepolarizing – Vecuronium
Droperidol

Part I: Anesthesia. Intravenous Anesthesia. First attempt at intravenous anesthesia by Wren
in 1656-- opium into his dog Use in anesthesia in 1934 with thiopental Many ways to meet requirements-- muscle
relaxants, opoids, nonopoids Appealing, pleasant experience
Thiopental Barbiturate Water soluble Alkaline Dose-dependent suppression of CNS activity--
decreased cerebral metabolic rate (EEG flat)

Part I: Anesthesia. Intravenous Anesthesia.
Thiopental Varied effects on cardiovascular system in
people-- mild direct cardiac depression-- lowers blood pressure-- compensatory tachycardia (baroreflex)
Dose-dependent depression of respiration through medullary and pontine respiratory centers
Noncompatibility Tissue necrosis--gangrene Tissue stores Post-anesthetic course

Etomidate Structure similar to ketoconozole Direct CNS depressant (thiopental) and GABA agonist Redistribution Little change in cardiac function in healthy and cardiac
patients Mild dose-related respiratory depression Decreased cerebral metabolism Pain on injection (propylene glycol) Myoclonic activity Nausea and vomiting (50%) Cortisol suppression
Part I: Anesthesia. Intravenous Anesthesia.

Ketamine
Structurally similar to PCP (phencyclidine) Interrupts cerebral association pathways --
“dissociative anesthesia” Stimulates central sympathetic pathways Characteristic of sympathetic nervous system
stimulation-- increase HR, BP, CO Maintains laryngeal reflexes and skeletal muscle
tone Emergence can produce hallucinations and
unpleasant dreams (15%)
Part I: Anesthesia. Intravenous Anesthesia.

Part I: Anesthesia. Intravenous Anesthesia.
Propofol
Rapid onset and short duration of actionMyocardial depression and peripheral
vasodilation may occur-- baroreflex not suppressed
Not water soluble-- painful (50%)Minimal nausea and vomiting
Part I: Anesthesia. Intravenous Anesthesia.
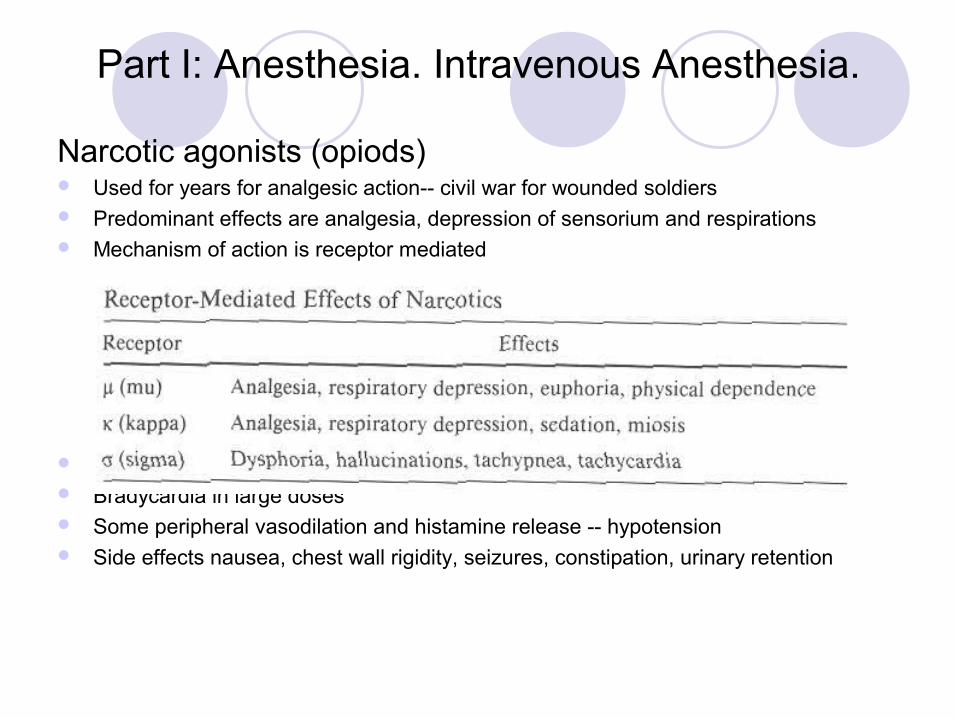
Narcotic agonists (opiods) Used for years for analgesic action-- civil war for wounded soldiers Predominant effects are analgesia, depression of sensorium and respirations Mechanism of action is receptor mediated
Minimal cardiac effects-- no myocardial depression Bradycardia in large doses Some peripheral vasodilation and histamine release -- hypotension Side effects nausea, chest wall rigidity, seizures, constipation, urinary retention

Part I: Anesthesia. Intravenous Anesthesia.
Narcotic agonists (opoids)
Meperidine (demerol), morphine, alfentanil, fentanyl, sufentanil. But morphine and fentanyl are commonly used.
Naloxone is pure antagonist that reverses analgesia and respiratory depression nonselectively-- acts 30 minutes, effects may recur when metabolized

Part I: Anesthesia. Intravenous Anesthesia.
Muscle Relaxants Current use of inhalational and previous intravenous agents do not fully provide
control of muscle tone First used in 1942-- many new agents developed to reduce side effects and lengthen
duration of action Mechanism of action occurs at the neuromuscular junction
Neuromuscular Junction

Part I: Anesthesia. Intravenous Anesthesia.Nondepolarizing Muscle Relaxants Competitively inhibit end plate nicotinic cholinergic
receptor Intermediate acting (15-60 minutes): atracurium,
vecuronium, mivacurium Long acting (over 60 minutes): pancuronium,
tubocurarine, metocurine Difference-- renal function Tubocurare-- suppress sympathetics, mast cell
degranulation Pancuronium-- blocks muscarinics Reversal by anticholinesterase-- inhibit
acetylcholinesterase neostigmine, pyridostigmine, edrophonium side effects muscarinic stimulation

Part I: Anesthesia. Intravenous Anesthesia.
Depolarizing Muscle Relaxants
Depolarize the end-plate nicotinic receptorSuccinylcholine used clinically
short duration due to plasma cholinesterase side effects-- fasiculations, myocyte rupture,
potassium extravasation, myalgias sinus bradycardia-- muscarinic receptor malignant hyperthermia

Part I: Anesthesia. General anesthesia

Part I: Anesthesia. General anesthesia
Part I: Anesthesia. General anesthesia Aspiration
Inhalation of GI contents & acids Results in mild respiratory status changes to sudden
death Pulmonary dysfunction
Hypoventilation Treated with increased oxygenation, reversal of drugs,
positive pressure ventilation
Postoperative anesthesia complications Respiratory: atalectasis, aspiration, pneumonia GI: Nausea, vomiting, decreased peristalsis,
paralytic ileus U: Urinary retention, kidney dysfunction

Part II. Cardiopulmonary resuscitation2005 International Consensus on
Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations was approved on November 2005.
A lot of regulations was changed.

Part II. Cardiopulmonary resuscitationSudden death Unexpected death of the patient, who is in
good general health condition. Appearance of the death within few hours from the onset of first symptoms of illness.
Cardiac sudden death.
Every tenth (third) of patients could be saved by proper life support.
Part II. Cardiopulmonary resuscitationLife For normal functioning all cells of the body
require oxygen. If oxygen is not provided, death of organism appears within 4..5 minutes.
Brain is the tissue most susceptible to anoxia (absence of oxygen).

Part II. Cardiopulmonary resuscitation
Process of the death
Is not a momentary but stepwise process, which can take certain
time.
Five steps of the death:
– Preagony
– Terminal pause
– Agony
– Clinical death (reversible injury)
Biological death (irreversible injury)

Part II. Cardiopulmonary resuscitationAgony is a stadium which preceeds to the death.
Function of vital organs is severly disturbed, and conditions required for survival of organism cannot be met.
Unconsciousness Blood pressure is undetectable No pulse on arteries
Clinical death: circulation stops completely and
that leads to the cessation of breathing and
nervous system activity.

Part II. Cardiopulmonary resuscitation
Symptoms of clinical death
No pulse on arteries (carotid or femoral)
Change of skin colour Unconsciousness Gasping, cessation of breathing Dilatation of eye pupils
Duration of clinical death is 3(5) minutes

Part II. Cardiopulmonary resuscitationBiological death is irreversible condition.
Metabolism of and functioning of vital organs has completely ceased. Organ damage is as extensive that resuscitation of the body is impossible.
Evident symptoms of the death: Rigor mortis Death spots on the body Drop of body temperature to the level of the
surrounding

Part II. Cardiopulmonary resuscitationCardiopulmonary Resuscitation – CPR
BLSBasic life support
Adult, pediatric
A(C)LSAdvanced (Cardiac) Life Support
Adult, pediatric
PRCPost-resuscitation care
Adult, pediatric

Part II. Cardiopulmonary resuscitation Adult BLS sequenceBasic life support consists of the following sequance
of actions:1. Make sure the victim, any bystanders, and you
are safe.2. Check the victim for a response (gently shake his
shoulders and ask loudly, “Sir. Or Ms., are you all right?”)
3 A. If he responds: Leave him in the position in which you find him
provided there is no further danger. Try to find out what is wrong with him and get
help if needed. Reassess him regularly.

Part II. Cardiopulmonary resuscitation Adult BLS sequence3 B. If he does not respond: Shout for help, call 911 (USA and Canada)
or 03 (Ukraine and Russian Fed) Turn the victim onto his back and then
open the airway using head tilt and chin lift:
- place your hand on his forehead and gently tilt head back.- with your fingertips under the point of the victim’s chin, lift the chin to open the airway.

Part II. Cardiopulmonary resuscitation Adult BLS sequence 4. Keep the airway open, look, listen, and
feel for normal breathing. Look for chest movement Listen at the victim’s mouth for breath
sounds. Feel for air on your cheekLook, listen and feel for no more than 10
sec to determine if the victim breathing normally. If you have any doubt whether breathing is normal, act as if it is not normal.

Safar’s triple manoeuvre Head tilt Jaw thrust Open mouth

Part II. Cardiopulmonary resuscitation Adult BLS sequence5 A. If he is breathing normally:• Turn him into the recovery position• Send or go for help, or call for an ambulance.• Check for continuated breathing.5 B. If he is not breathing normally:Ask someone to call for an ambulance. Kneel by the side of the victim. Pinch the soft part of the victim’s nose closed, using the
index finger and thumb of your hand on his forehead. Allows his mouth to open, but maintain chin tilt. Take a normal breath and place your lips around his mouth,
making sure that you have a good seal.

Recovery position
Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont)5B. Cont. Blow steadily into his mouth whilst watching for
his chest to rise; take about one second to make his chest rise as in normal breathing; this is an effective rescue breath.
Maintaining head tilt and chin lift, take your mouth away from the victim and watch for his chest to fall as air comes out.
Take another normal breath and blow into the victim’s mouth once more to give a total of two effective rescue breaths.
Give each rescue breath over 1 sec rather than 2 sec.

Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont)6. Check the victim’s pulse.6 A. If pulse on the carotid artery is not palpable –
begin chest compression. Place the heel of one hand in the centre of the
victim’s chest. Place the heel of your other hand on the top of
the first hand. Interlock the fingers of your hands and ensure
that pressure is not applied over the victim’s ribs. Do not apply any pressure over the upper abdomen or the bottom end of the bony sternum (breastbone).

Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont) Position yourself vertically above the victim’s
chest and, with your arms straight, press down on the sternum 4-5 cm.
After each compression, release all the pressure on the chest without losing contact between your hands and the sternum. Repeat at a rate of about 100 times a minute (a little less than 2 compressions a second).
Compression and release should take an equal amount of time.
Perform 30 compressions and after that open the airway again using head tilt and chin lift.

Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont) Perform 2 inflations. Then return your hands without delay to correct
position on the sternum and give a further 30 chest compressions.
Continue with the chest compressions and rescue breaths in the ratio of 30:2.
Stop to recheck the victim only if he starts breathing normally; otherwise do not interrupt resuscitation.

Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont)If your rescue breaths do not make the
chest rise as in normal breathing, then before your next attempt:
Сheck the victim’s mouth and remove any visible obstruction.
Recheck that there is adequate head tilt and chin lift.
Do not attempt more than two breaths each time before returning to chest compressions.

Part II. Cardiopulmonary resuscitation Adult BLS sequence (cont)If there is more than one rescuer present,
another should take over CPR about every 2 min to prevent fatigue. Ensure the minimum of delay during the changeover of rescuers.

Chain of survival
EARLY CPR
EARLY DEFIBRILLATION
EARLYACCESS
EARLY ADVANCED
CARE

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation

Part II. Cardiopulmonary resuscitation


Key - Life




